Embed Size (px)
Citation preview

HW5: In-Vitro Diagnostics Clinical Needs, MethodsComparison and Engineering Mechanisms BetweenStandard-of-Care and Point-of-Care for Infectious
Diseases
Bryan Felix, Ewnet Gebrehiwot, and Scott Hansen
August 21, 2019
Abstract
A comparison of clinical needs, methods and engineering mechanisms were com-pleted between the standard of care (SOC) and Point of care (POC) diagnostics forinfectious diseases. Infectious diseases are one of the leading deaths in developing coun-tries such as Africa and Regions of Asia. Malaria, Tuberculosis and HIV/AIDS wereselected for the assessment and the findings were a shared clinical needs and benefitsin developing ’better, faster and cheaper’ POC. ELISA and LFA were compared indetail in their methods and engineering mechanisms in detecting infectious diseasesto achieve high sensitivity and quicker results response time. In the case of LFAs,sensitivity remains an issue since it is difficult to detect small amounts of antigens.Engineering approaches to modify the nanoparticles and time scale of LFAs increasetest sensitivity by increasing reaction rates and keeping flow rates from being too high.
1

1 Introduction
Infectious Diseases are caused by bacteria, viruses, fungi or parasites [14]. These are commu-nicable diseases either from one person to another, bites from insects or animals or ingestingof contaminated food or water [14]. Infectious diseases are #9 for 1.6% of total U.S. YLD(Years Lived with Disability) and #10 for 2.6% of Global YLD [24]. However, infectiousdiseases are the #1 cause of death in Sub-Saharan Africa and Various Regions of Asia [25].These countries have low-income, limited resource, high population and overall lack of healthcare and infrastructure that promotes infectious diseases to wide spread easily and not getproper treatments. This leads to millions of people dying every year and transmission andsurvival of the disease not only locally but worldwide compromising the overall health stateof the world.
Considering the limitations of resource limited countries (RLC), it is essential to comeup with a medical and engineering solutions to reduce and eliminate the epidemic nature ofinfectious diseases. One of the ways to achieve such impact is having high sensitive, easy touse, less maintenance and cost-effective in-vitro diagnostics testing that is suitable for RLCsetting [23]. There are two types of in-vitro diagnostics; one is laboratory based microscopyand immunosorbent assay (ELISA) detection methods for antibodies, antigen or protiens,referred to as Standard of Care (SOC). The second type is rapid diagnostic testing based onlateral flow assay (LFA) color band detection methods on an oral swab strip, finger pricksfor blood or urine markers, referred to as Point-of-Care (POC).
On the following sections, the clinical needs of three infectious diseases (Malaria, Tuber-culosis and HIV/AIDS) are discussed followed by the current diagnostic methods and resultsassessment utilized by these three infectious diseases. The mechanisms of SOC and POCwill be discussed in the subsequent sections, which includes a discussion on the engineeringprinciples and newly emerging technologies such as nanodiagnostics impact in improvingPOC in particular.
2 Clinical Needs
Out of the long list of infectious diseases, Malaria, Tuberculosis and HIV/AIDS were selectedto assess their clinical needs for in-vitro diagnostics especially for their POC needs. All ofthem have similar themes of clinical needs with some specific needs based on the diseasesseverity and characteristics. Table 1 below attempts to summaries the clinical needs findingsas it pertains to POC.
Table 1: Clinical Needs Summary
2

The shared benefits for developing POC for these diseases lies in early detection resultingin reduced transmission, improved treatment outcomes and reduced health care costs [20].Especially, in resource limited countries (Africa and parts of Asia), early detection of thediseases will directly impact in saving millions of lives every year, increase life expectancyand quality of life. The following sections will discuss brief background on the infectiousdiseases, disease type characteristics and highlights the unmet clinical needs.
2.1 Malaria
Malaria is caused by plasmodium parasites through the bites of infected female Anophelesmosquitoes called ”malaria vectors” [9]. 92% of malaria cases and 93% of malaria deathshappen in Sub-Saharan Africa [9]. Two out of the five parasite species that cause malariain humans, P. falciparum and P.vivax are the deadliest. After the first symptoms such asfever, headache and chills, especially if the P. falciparum is not treated within 24 hours, themalaria can progress and often can lead to death [9].
For a non-immune individual, it takes up to 10-15 days to start having the first symptoms[9]. Although, the best option is prevention by using insecticide-treated mosquito nets andindoor residual spraying, it might not be possible to prevent or even be aware of the presenceof the mosquitoes in most cases. Therefore, there is a clinical need of early detection andtreatment of malaria to reduce disease and prevent deaths. Early detection would be possibleby increasing sensitivity and specificity to detect low level parasites that hasn’t developedto first symptom [10].
According to World Heath Organization (WHO), the total funding for malaria con-trol/elimination is near US3.1billion in 2017 [9], which shows the seriousness of the diseasesand the need for a cost-effective and value-adding diagnosis for early detection. A parasite-based diagnostic testing is recommended to confirm the parasitological within 30minutes orless before administrating treatment [9].
Figure 1 below show vector control, preventive vaccines, diagnostics, drug treatment atvarious stages of Malaria disease progression. Knowing the different stages of the progressionhelps with formulating an analyte to detect the infection before the first symptoms appearsafter 10-15 days.
3

Figure 1: Malaria treatment stages including vaccines, drug and diagnostics from [10]
Malaria seems to have a well advanced disease state understanding and robust RDTwithin 30 minutes or less results. The one area with an unmet need on the diagnostics isfinding an early detectable biomarker with in the window of the first 10-15 days to expeditethe early detection process and reduce transmission.
4

2.2 Tuberculosis
Tuberculosis (TB) is one of the top 10 causes of death worldwide and it is caused by bac-teria called Mycobacterium Tuberculosis that usually attack the lungs [9, 11]. TB is highlycontagious through air when a person coughs, sneezes or talks. 72% of the TB cases are inAfrica followed by India cases of 27% [12].
There are two types of TB, first latent TB that is inactive form of the disease and is nottransmittable, however, 5-15% population with latent TB have a chance of falling ill withactive TB. The second type is active TB disease which may begin with a mild symptoms ofcough, fever, night sweats and weight loss for months. Due to its slow progress of illness,people can delay care and result in transmitting the disease to other people [9]. If nottreated properly, 45% of HIV-negative people with TB and nearly all HIV-positive peopledie because of the TB [9].
The commonly used rapid diagnostic test (Xpert MTB/RIF) has been in use since 2010,which detects TB and resistance to the treatment drug [9]. The diagnosis takes 2 hoursand it is a recommended initial test by WHO. One of the clinical challenges with TB isdiagnosing multi-drug resistance especially drug-resistant TB since it is complex and expen-sive [9]. Therefore, the clinical needs for TB diagnosis is in the ability to detect multipledrug resistance technology, cost-effect and faster Point of Care (POC) type of diagnostics.
Figure 2 below shows the research need for TB Assay that is mainly focused on under-standing the assay and accurately detecting it. One of the main need for TB is the abilityto multiplex by detecting not only the bacteria’s antigen/antibodies but also by detectinghow much the person is drug resistant to various TB treatments.
5

Figure 2: Point of Care (POC) Consideration for TB-LAM Assay and in General from [13]LAM Stands for Lipoarabinomannan, it is an antigen from the cell wall lipopolysaccharide.
TB can initially be confused with colds and flu symptoms that misleads people fromseeking treatment quickly. In addition, the current POC for TB does that 2 hours and needto complete multiple tests for the bacteria and drug resistance. All these inconveniences maynot encourage people to seek diagnosis and treatment until the TB has progressed. Easy touse home based POC could encourage people to take the test more readily than the currentsituation.
2.3 HIV/AIDS
The Human Immunodeficiency Virus (HIV) targets the immune system and weakens people’sdefence system against infections and other disease types [9]. Gradually, the virus cause theinfected individuals to become immunodeficient and make the individual vulnerable to a widerange of diseases [9]. The progressed stage of HIV infection is Acquired ImmunodeficiencySyndrome (AIDS). In the past two decades, 38% of HIV related deaths reduced becauseof the lifelong antiretroviral therapy (ART); currently 59% of adults and 52% of childrenrecieve ART. Two Thirds of the population who lives with HIV is in Africa.
The rapid diagnostics tests (RDT) such as serological tests detect the presence or absenceof antibodies or antigen in response to the virus [9]. Therefore, HIV is not directly detecteddirectly. Furthermore, it takes up to 28 days to develop the antibodies that can be detectedby the RDT and it is the highest time to transmit the virus to other individuals [9].
The clinical need for HIV diagnosis is a search for effective analyte with antigen or RNAto for an early detection of HIV [14]. Furthermore, considering only 75% of the people with
6

HIV know their status, more access to cheaper and easy to use POC is needed to diagnosemore people who do not know their status yet [9]. The other clinical need is for infants bornto mothers living with HIV who needs virological testing (faster by detecting the virus or partof it directly) instead of serological testing (takes time to detect the antibodies/antigen) [14].
The critical question for HIV is how early can it be detected. Hurt et. al. [15] outlinesthis time for detection will depend on 1) the target being detected, 2) when the target ispresent following infection, 3) the concentration of target in the specimen, 4) the volume ofspecimen tested, and 5) the test’s lower limit of target detection.
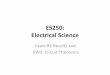
Figure 3 below shows how the virological testing (HIV RNA) has much faster detec-tion time (approximately 10 days) compared to commonly used serological testing (Anti-body/antigen, which takes up to 30 days). For HIV/AIDS, the ability to detect earlier withthe most effective and accurate bio-marker is important. Currently, the detection time forHIV is increasing as we move from detecting proteins (greater than 30 days) to detectingantibodies (Approx. 30 days) to antigens (approx. 20 days) to virus(approx. 10 days).
7

Figure 3: Serological vs. Virological testings detection time from [15] NAT stands for NucelicAcid Testing, which is testing of host cell to detect any RNA modification caused by theHIV, p24 is an antigen associated with HIV, IgM and IgG are antibodies associated withHIV. Western Bolt is highly sensitive, multi step and protein based test.
Given the lack of cure and highly transmissions nature of HIV/AIDS, a lot of goodadvancement has been made in the last 30-35 years. Although, the number of HIV infectedpeople has decreased and due to the use of ART sustained, there are 25% of infected butunaware people that can be an agent in continuing the transmission. This rises the unmetneed of easy to use home-based POC for resource limited countries would be essential. Oncea person is diagnosed positive, multiple level of repetitive diagnostic testing is executed tocomplete the diagnosis. This calls a need to consolidate the multiple testing to a single orreduced step but highly sensitive POC.
8

2.4 Diagnostic Methods Comparison: SOC vs. POC Discussion
What we observe from the three infectious diseases discussed above (i.e. Malaria, Tubercu-losis and HIV/AIDS) the traditional diagnostic methods of microscopy is used hand in handwith the Rapid Diagnostics Testing (RDT). The common drawbacks in the standard careof microscopy-related diagnosis is the need of significant laboratory testing time, laboratoryinfrastructure and trained staff and relatively expensive because of testing time, personneltraining and equipment maintenance [21]. On the other hand, the microscopy-related diag-nosis tend to have high sensitivity, accuracy of results and ability to handle multiple testingat once (multiplexing).
In parallel, the common benefit in RDT diagnosis is the cost-effectiveness and quickerresponse time leading to early detection and faster treatment options. In the meantime,this POC can be less sensitive in detection, may not be widely accessible in resource-limitedcountries and result in false negative results that can be misleading in taking the earlytreatment options.
Table 2 below compares the diagnostic methods between SOC and POC for Malaria,Tuberculosis and HIV/AIDS. The findings confirm most of the common themes of pros andcons, however, there are some contrary results shown such as lower sensitivity for MalariaSOC but high sensitivity for TB POC. Also Malaria’s SOC and POC has little to no costdifference. The main reason for the contrary results could be due to the disease severity leveland the resource-limited nature of the countries where these diseases are being treated.
Table 2: Diagnostic Methods Comparison
For instance Malaria, where 92% of the people with the disease lives in Africa, the typeof the SOC and POC is going to be greatly compromised of quality and standard becauseof the resource-limited nature of the African countries. SOC for Malaria does not havethe specificity to picking up Malaria parasites only so it does pick up other types of regionalparasites [19]. As some literature [20,22,23] pointed out the POC design criteria for resource-limited countries (RLC) would have to be different than developed countries. Besides cost,which is not the sole problem of RLC , the ease of use and less maintenance are also criticalneeds for accessibility and usability of POC in RLC. [23].
In the meantime, the search for novel and advanced analyte and detection modalitiesare also important as extensively discussed on Kim et al. [20]. For example, the HIV/AIDSPOC is always looking for the most effective biomarker to detect the virus present as earlyas possible as depicted on Figure 3 in HIV/AIDS Section above.
9

The promise of nanoparticles to improve analytical sensitivity of diagnostic assays [20]might be at its early technology development stage, however, can impact POC all aroundthe world by promoting high sensitivity for early detection of infectious diseases while main-taining cost effective and easy to use. The following sections will discuss further into themechanisms and engineering analysis of the two most common diagnostic methods of SOC(ELISA) and POC (LFA).
3 Enzyme-linked Immunosorbent Assay: ELISA
ELISA (acronym for enzyme-linked immunosorbent assay) is a technique for antigen detec-tion. It is commonly used to measure antibodies, antigens, proteins, and glycoproteins inbiological samples. Given that the methods are highly reproducible and inexpensive it isa common choice for large scale sample testing. Other benefits of using ELISA are clear;we direct the reader to the chart in Figure (6) for a further reference. ELISA methodswork on the principle that enzymes are capable of reacting with substrates multiple timesbefore decaying. Thus, a weak signal from an antigen can be enhanced. Parting from animmobilized target, enzyme-labeled antibodies are added and cultured so that they form anantibody-antigen complex. Later, an enzyme substrate is added and the enzyme productis quantified (see Figure 5). Although many variations of Elisa exist (see Figure 4), suchas direct, indirect, competitive, sandwich, among others, the steps involved are analogous.Broadly the relevant stages involved are [5]:
1. Adsorption of antigen or antibody to the plastic solid phase
2. Addition of the test sample and subsequent reagents
3. Incubation of reactants
4. Separation of bound and free reactants by washing
5. Addition of enzyme-labeled reagent
6. Addition of enzyme detection system (color development)
7. Visual or spectrophotometric reading of the assay
10

Figure 4: Different ELISA formats. Taken from [6]
Figure 5: Direct ELISA method. Taken from [4]
11

Figure 6: Features of ELISA. Taken from [5]
Depending on the test to be performed, ELISA methods might not be adequate. Itssensitivity is in the femto- to nano-molar range. Moreover quantification of results mightrequire specialized instruments which might be expensive depending on their sensitivity.Then, specific antigen or antibodies reagents, and long hours of cultivation might be abarrier for particular samples [7].
3.1 Mathematical Model and governing equations
We proceed to describe the governing equation in a 3-Dimensional space, as it is the case inmicro-plate well assays. For simplicity we assume that the well has a cylindrical geometrywith diameter equal to 3mm, and height equal to 10 mm. We denote by Ω the inside of thewell, by ∂Ω the boundaries, and by Γ the bottom of the well (See figure 7).
12

Ω@Ω
Γ
1.5 mm
10mm
Figure 7: Typical geometry of a well
Here, we focus on the direct assay technique (see Figure 5). Thus, parting from an assaywith an established concentration of antigens at Γ, we describe the two steps:
1. addition enzyme-labeled antibodies, and
2. addition of enzyme substrates.
We will assume that the intermediate steps are conducted in such a way that, the steadystate of process 1 is independent from step 2 above.
3.1.1 Step 1: Addition of enzyme-labeled antibodies
Let [P ] denote the concentration of (without loss of generality) proteins of interest to bedetected; [A] the concentration of enzyme labeled antibodies; and [E] the functional enzymecomplex AP . Now, consider the chemical process:
A+ Pk1k2E. (1)
We presume this reaction can only take place near the surface Γ. Specifically we fix ` = 10nmto be the minimum distance from Γ at which the reaction takes place. Then, the generalform of the reaction diffusion process is given by
∂
∂t[A] =DΓ∆Γ[A]− k1`[A][P ] + k2[E] ∈ Γ (2)
∂
∂t[E] =DΓ∆Γ[E] + k1`[A][P ]− k2[E] ∈ Γ (3)
∂
∂t[P ] =DΩ∆Ω[P ] ∈ Ω (4)
13

where Di is the diffusion coefficient in the respective domain, and ∆ = ∇2 is the Laplace-Beltrami operator in the appropriate domain. To the above we impose the following bound-ary conditions
DΩ∂
∂n[P ] =− k1`[A][P ] + k2[E] ∈ Γ (5)
∂
∂n[P ] =0 ∈ ∂Ω\Γ (6)
∂
∂n[A] =
∂
∂n[E] = 0 ∈ ∂Γ (7)
where ∂n is to be taken as the outward normal vector of the respective domain.
3.1.2 Step 2: Addition of enzyme substrates
We assume that that the species of step 1 have been cultivated and washed as to leave asteady state concentration of enzyme-labeled antibodies at the surface Γ. Now, let [S] denotethe concentration of the enzyme substrate, [C] the concentration of the complex ES, andlet [S∗] be the concentration of the enzyme product. A version of enzyme kinetics is givenby the chemical reaction
E + Sr1r2C
r3→ E + S∗. (8)
Analogous to the derivation for governing equations in step 1, we presume that the substrateand its product diffuse freely on the medium. Moreover, as we did before, the enzymaticreactions are restricted to an area near the boundary Γ. Then the governing equations areof the form:
∂
∂t[E] =DΓ∆Γ[E]− r1`[E][S] + (r2 + r3)[C] ∈ Γ (9)
∂
∂t[S] =DΩ∆Ω[S] ∈ Ω (10)
∂
∂t[C] =DΓ∆Γ[C] + r1`[E][S]− (r2 + r3)[C] ∈ Γ (11)
∂
∂t[S∗] =DΩ∆Ω[S∗] ∈ Ω (12)
(13)
together with the following boundary conditions
DΩ∂
∂n[S] =− r1`[E][S] + r2[C] ∈ Γ (14)
DΩ∂
∂n[S∗] =r3[C] ∈ Γ (15)
∂
∂n[S] =
∂
∂n[S∗] = 0 ∈ ∂Ω\Γ (16)
∂
∂n[E] =
∂
∂n[C] = 0 ∈ ∂Γ (17)
14

Figure 8: Taken from [27]
0.2 0.4 0.6 0.8 1.0Distance(cm)
100
200
300
400
Time (hours)Difussion time
Figure 9: Diffusion time
3.1.3 Paramters and the Damkohler number
It has been found that at 20C the diffusion coefficient of human IgG in 10-times-dilutedserum is (4.4 ± 0.2)×10−7cm2s−1, while the diffusion coefficient of rabbit anti-human IgGin a purified preparation is (2.9 ± 0.2) ×10−7cm2s−1 [26]. Moreover, binding rates for IgGhave been theoretically estimated in a studies such as [27]. Their results are summarizedin Figure 8. Observe that the diffusion time (τ = L2/2D) for a well of 1cm (as in 7) isabout 20 days. A plot of the time to diffusion is show in Figure 9. Thus, it is unrealisticto allow the labeled antibodies to diffuse from the top. In fact, the standard protocol forELISA requires the solutions to be added directly into the wells [28]. Thus we will computethe Damkhohler number as defined in [29] by
Da = kCn−10 τ
where k is the kinetic constant, C0 is the initial concentration of the reagent, n is the order ofthe reaction, and τ is the residence time. For the residence time here we assume is the timeit takes the reagent to diffuse a length larger that the reaction domain defined by ` = 10nm.Explicitly, taking k to be the maximum among the kinetic rates provided in 8, we get
Da = kCn−10 τ = 5.26× 10−4C0.
Note that the units of k are M−1s−1. Thus, in order for Da to be less than 0.01 we requirethe initial concentration of the reagents to be of the order
C0 < 20M
which is reasonable. With this at hand, we know that the kinetics will be the limitingparameters of the reaction. Thus, in the next section, we will proceed by assuming thatdiffusion in negligible, and we will reduce the system.
15

3.1.4 Lumped system for captured analyte and steady state analysis
As discussed in the previous subsection diffusion plays a minor role in our model. Thus,to analyze the steady state of analytes we will reduce the model in section 3.1.1 . Tobegin, we presume that diffusion gradients are negligible and derive a lumped model for theconcentration profiles. We define the mean concentration of P as
P (t) =1
|Ω|
∫Ω
P (t, x) dx.
Then, taking the derivative with respect to time we get
d
dtP =
1
|Ω|
∫Ω
∂
∂tP (t, x) dx =
1
|Ω|
∫Ω
DΩ∆ΩP dx.
By using the divergence theorem we have
d
dtP =
1
|Ω|
∫∂Ω
DΩ∇Pn · ds =1
|Ω|
∫Γ
−k1`[A][P ] + k2[E] ds.
Assuming that the concentrations of P,A, and E are constant across the bottom surface Γwe have that
d
dtP =
1
|Ω|(−k1`[A][P ] + k2[E])
∫Γ
ds =|Γ||Ω|
(−k1`[A][P ] + k2[E]).
In an analogous manner we deduce mean concentrations for A and E. We have
d
dtA =
1
|Γ|
∫Γ
∂
∂t[A] (18)
=1
|Γ|
∫γ
−k1`[A][P ] + k2[E] ds (19)
=1
|Γ|(−k1`[A][P ] + k2[E])
∫Γ
ds (20)
=− k1`[A][P ] + k2[E]. (21)
Finally, for E,
d
dtE =
1
|Γ|
∫Γ
∂
∂t[E] (22)
=1
|Γ|
∫γ
k1`[A][P ]− k2[E] ds (23)
=1
|Γ|(k1`[A][P ]− k2[E])
∫Γ
ds (24)
=k1`[A][P ]− k2[E]. (25)
16

Thus, our lumped system satisfies
d
dtP =|Γ||Ω|
(−k1`[A][P ] + k2[E]) (26)
d
dtA =− k1`[A][P ] + k2[E] (27)
d
dtE =k1`[A][P ]− k2[E]. (28)
Note that the equations reveal the following conservation laws
C1 =[A]0 + [E]0, (29)
C2 =|Γ||Ω|
[E]0 + [P ]0. (30)
Now we proceed to find the analytical solution of the steady state using the parametersshown in Table 3.
Parameter value units|Γ| π(0.015)2 cm2
|Ω| π(0.015)2 cm3
k1 3.29× 104 M−1s−1
k2 2.9× 10−4 s−1
` 1× 10−6 cm[A]0 C1 M[P ]0 C2 M[E]0 0 M
Table 3: Parameters used
Our variable of interest [E] reaches steady state at
3.04× 10−7(√
(−1.65× 106C1 + 1.65× 106C2 + 149)2 + 9.8× 108C1 (31)
+1.65× 106C1 + 1.65× 106C2 + 149)
(32)
A plot of the steady state concentration of [E] for severl choices of C1 and C2 is shown inFigure 10
17

Figure 10: Steady state concentration of [E] for several choices of [A]0 = C1 and [P ]0 = C2
4 Lateral Flow Assay
Lateral flow assays (LFAs) are simple diagnostic tools that can detect specific biomolecules.They are fast, inexpensive, easy to use, and protable [1]. LFAs have made fast, point-of-care diagnostics a reality for many conditions that would typically require long laboratorytesting. Sensitivity remains an issue with LFAs, but this is being addressed by the growingfield of thermal contrast techniques [1]. Though they lack sensitivity, LFAs rely on a robustmechanism of action for diagnosis when their is sufficient antigen present.
LFAs consist of four main components: 1) A sample pad, 2) a conjugation pad, 3) a ni-trocellulose membrane test region, and 4) an absorbent pad [1,2]. The sample pad is dippedinto the specimen of interest and is pulled through the nitrocellulose membrane throughcapillary action. The conjugation pad contains antibody-coated gold nanoparticles (GNPs).The antibodies are specific to the antigen of interest, which will then bind to the GNP. Thenext stage of the LFA is where detection occurs. The test line is coated with antibodiesthat target the antigen on the GNP complex as it flows through the device. The antibodiesbind the antigen, thus stopping the GNP complex form progressing through the device. Theaccumulation of GNPs in the test section signals the presence of the particular antigen ofinterest. The control strip ensures that the GNPs and antibodies are working correctly. Ifthis line is not visible during the assay, it is unreliable because the nanoparticles could bedefective or there was some other malfunction with the device. The absorbent pad is thefinal destination for the GNPs as they flow through the LFA.
18

Figure 11: Schematic of a typical lateral flow assay [2]. LFAs are typically composed of asample pad, a conjugation pad, a test region, and an absorption pad.
Figure 12: LFAs utilize antibody-coated GNP to bind the antigen of interest and subse-quently bind to the monoclonal antibodies bound to the surface of the membrane.
Figure 13: When the Peclet number is too large (Pe >> 1), GNPs do not have enough timeto diffuse to the capture antibody before being carried away by the flow. LFAs with smallerPeclet numbers allow sufficient time for diffusion to the capture antibody for binding.
19

Figure 14: At high concentrations, LFA test signal experiences a hook effect, resulting in aregression of the signal.
The intensity of the test region visual signal is indicative of the concentration of theanalyte. Figure 14 shows a representative curve of the intesnsity signal as the concentrationof the analyte increases. At most concentrations, the intensity follows a fairly predictablepattern-increasing concentration leads to a stronger signal. However, at very high concentra-tions the signal undergoes a high dose hook effect and the signal begins to decrease. Ideally,all of the GNP complexes would bind to antibodies bound to the test strip region. At highconcentrations, the antibodies bound to the test strip are increasingly filled. This makesit more difficult for conjugated antibodies bound to the antigen to bind them. Therefore,due to the high concentration, conjugated antibodies in the fluid phase bind to one another.With the antigen already bonded on both sides, the GNPs pass through the test regionwithout contributing to the signal. The signal will then be lower than expected at highconcentrations.
GNP capture is a crucial aspect in determining the sensitivity of LFAs. Poor GNPcapture will make for an ineffective LFA. Therefore, GNP capture must be optimized forproper performance of the LFA. Velocity, diffusion, and reaction rates all play a role in GNPcapture. These parameters can be defined using the Peclet number (Equation 33) and theDamkohler number (Equation 34).
Pe =UR
D(33)
Da =kCR
D(34)
L
V= τ (35)
√Dτ = Ldiff (36)
The Peclet number is the ratio of convection to diffusion of a system. For LFAs, Pecletnumbers less than one, where diffusion dominates convection, are desirable. This corre-
20

sponds to the low convection region on the left hand side of Figure 15. When diffusiondominates, there is an increase in transit time that allows for the GNP reporters to diffuseaway from the streamline and bind to the capture antibodies. In order to decrease the timeto make a reading, Pe is usually much larger than one and diffusion becomes the rate limitingstep [3]. This can be demonstrated by calculating a residence time as found in Equation 35and comparing to the diffusion length scale from Equation 36. We used previously reportedvalues of 0.2 mm/s, 10e-11 m2/s, and 2mm for the velocity, diffusivity, and length of thetest strip as an example. Applying Equation 35 yields a residence time of 10s. Using thisresult in Equation 36 yields a diffsuion length of 31.6µm. Within the 10 second time frame,particles under 31.6µm would be able to bind to the capture antibody by diffusing across thestreamline. This provides a good balance of both speed and signal strenght, both of whichare important components in the design of LFAs.
Reaction rate goes hand in hand with convection as a reduced velocity will increase thetime for reactions to occur. The Damkohler number, defined by Equation 34, provides aratio of the reaction rate constant to diffusion. Reaction is the rate limiting step, whichmeans that higher Da numbers are preferable [3]. Larger reaction rates and, thus, largerDamkohler numbers would lead to better binding. This corresponds to the large Damkohlernumbers on the right hand side of Figure 16, where reaction rate dominates diffusion. Whentaking both the Peclet number and the Damkohler number into account, the ideal LFA wouldhave a small Peclet number and a larger Damkohler number. This means that convection isdominated by diffusion, which is dominated by reaction.
Figure 15: Plot of Peclet number (Equation 33) as a function of velocity and diffusivity.
21

Figure 16: Plot of Damkohler number (Equation 34) as a function of the reaction ratecoefficient and diffusivity.
With the importance of GNP capture in mind, there are certain methods that shouldtheoretically maximize the chances of the GNP binding to the membrane. One thing thatcan be in order to increase the size of the nanoparticle. This has the benefit of increasingthe number of surface antibodies on the GNP and making capture more likely [3]. This,coupled with the fact that their absorption and scattering profiles make larger GNPs morereadily detectable [3]. As mentioned earlier, slowing down the flow allows the GNPs to havemore time to bind to the capture antibodies. A third and final method to maximize bindingwould be to change the shape of the nanoparticle to a geometry such as a rod with a highsurface area to volume ratio. The larger surface area would serve a similar purpose as usinga larger particle in that there are more available binding sites for the capture antibody tocome into contact with.
Nanoparticle size is a critical parameter in designing LFAs. 30nm is a common sizefor GNPs used in these types of systems. However, larger particles can help improve thesignal as we have already addressed. However, the benefits of increasing the size of theGNP eventually cease to outweigh the costs. Zhan et al [3] found that a functional limitis reached at around 100nm. Due to their larger size, they have a much larger Damkohlernumber, which means that the reaction rate will be limited by the slower diffusion of thelarger particle. Practically, it is also very expensive to make larger and larger nanoparticlesas it requires more gold and many more antibodies [3]. Eventually, settling becomes an issueif the size of the GNP gets to be too large. In this case, the GNP will settle within the poresof the membrane before before reaching the test line. It has been estimated that GNPsaround 400nm would not follow the streamline, but rather settle before reaching the teststrip [3]. This effect lowers the accuracy of the device and makes detection of the analytemore difficult. Therefore, GNPs must be designed in such a way so as to maximize theirlikelihood of capture through modifications to their size and shape without becoming solarge that test accuracy is compromised.
22

5 Conclusions
Three infectious diseases, Malaria, Tuberculosis and HIV/AIDS have been assessed for theirclinical needs and benefits of diagnostic testing especially POC. There are a number ofshared clinical needs such as early detection, high sensitivity and quicker results responsetime. The shared benefits of developing POC are reduced disease transmission, improvedtreatment outcomes and reduced health care costs. Furthermore, the benefits for resourcelimited countries quadruples by saving lives, increasing life expectancy and quality of life.
The comparison between SOC and POC diagnostic methods showed currently, utilizedtogether. Unless in some cases, SOC are highly sensitive but takes long time and needtrained personnel and infrastructure. On the other had, POC take less time to get results,are easy to use but lack the sensitivity of SOC.
In our analysis for ELISA assays we proved that the steady state profile of the enzyme-labeled antibody depends only on the kinetics of the chemical reaction. Moreover, we graph-ically showed that the steady state depends linearly in the initial concentration of trappedantibody and initial concentration of enzyme-labeled antibody. We give reasonable parame-ters ranges for which the analysis is valid. Moreover, we provided a constructive method forfinding the steady state values parting from a lumped assumption.
In our evaluation of lateral flow assays, we demonstrated that small Peclet numbers, wherediffusion dominates convection, and large Damkohler numbers, where reaction dominatesdiffusion, are most effective. In reality, though, these are not always attainable parameters.Peclet numbers are often much higher than one so that the assay can be performed ina matter of minutes. This limitation reduces signal strength due to the speed at whichthe GNPs are passing by the test strip. Sensitivity remains a significant roadblock to thedevelopment and adoption of fast POC diagnostic tests. Thermal contrast utilizing GNPsis one approach that is being developed to increase LFA sensitivity to small amounts ofantigen even when visible detection shows a negative result. Fast, POC diagnostic assayshave a massive potential to change healthcare. Their speed, affordability, and ease of usestreamline diagnostics, resulting in earlier diagnoses and better outcomes.
23

References
[1] Qin Z, Chan WCW, Boulware DR, Akkin T, Butler EK, Bischof JC. ”SignificantlyImproved Analytical Sensitivity of Lateral Flow Immunoassays by Using Thermal Con-trast.” Angew. Chem. 2012. 124:4434-4437.
[2] https://www.dcndx.com/lateral-flow-rapid-diagnostic-test/
[3] Zhan L, Guo S, Song F, Gong Y, Xu F, Boulware DR, McAlpine M, Chan W, BischofJC. ”The Role of Nanoparticle Design in Determining Analytical Performance of LateralFlow Immunoassays.” Nano Lett. 2017. 17:7207-7212.
[4] https://www.aatbio.com/resources/faq-frequently-asked-questions/What-is-a-Direct-ELISA
[5] John R. Crowther, Methods in Molecular Biology, The ELISA Guidebook. Second Edi-tion. Humana Press, a part of Springer Science + Business Media, LLC 2009.
[6] https://www.thermofisher.com/us/en/home/life-science/protein-biology/protein-biology-learning-center/protein-biology-resource-library/pierce-protein-methods/overview-elisa.html
[7] Kim, Jisung, et al. ”State of diagnosing infectious pathogens using colloidal nanomate-rials.” Biomaterials 146 (2017): 97-114.
[8] Baish, James W. ”Microvascular heat transfer.” The Biomedical Engineering Handbook,2 (2000): 98-1.
[9] https://www.who.int/news-room/fact-sheets/detail/malaria andhttps://www.who.int/en/news-room/fact-sheets/detail/tuberculosis andhttps://www.who.int/news-room/fact-sheets/detail/hiv-aids
[10] DCK, FO and TW, malERA: An updated research agenda for diagnostics, drugs, vac-cines, and vector control in malaria elimination and eradication. The malERA RefreshConsultative Panel on Tools for Malaria Elimination. 2017.
[11] https://medlineplus.gov/tuberculosis.html
[12] https://www.tbfacts.org/tb-statistics/
[13] Lawn, Stephen D. Point-of-care detection of lipoarabinomannan (LAM) in urine forfiagnosis of HIV-associated tuberculosis: a state of the art review. 2012.
[14] https://www.mayoclinic.org/diseases-conditions/hiv-aids/diagnosis-treatment/drc-20373531
[15] Hurt, Christopher B, et al. Selecting an HIV Test: A Narrative Review for Cliniciansand Researchers. 2017
24

[16] Zulfiqar, Hafiza Fizzah, et al. HIV Diagnosis and Treatment through Advanced Tech-nologies. 2017.
[17] https://www.cdc.gov/tb/publications/factsheets/pdf/xpertmtb-rifassayfactsheet-final.pdfhttps://www.cdc.gov/malaria/diagnosis treatment/diagnostic-tools.html
[18] Lu, Chunling, et al. A Systemic Review of Reported Cost for Smear and Culture Testsduring Multidrug-Resistant Tuberculosis Treatment. 2013.
[19] Wongsrichanalai, Chansuda, et al. A Review of Malaria Diagnostic Tools: Microscopyand Rapid Diagnostic Test (RDT). 2007.
[20] Kim, Jisung et al. State of disgnosing infectious pathogens using colloidal nanomaterials.2017.
[21] Drancourt, Michel, et al. THe Point-of-Care Laboratory in Clinical Microbiology. 2016.
[22] Juupiel, Desmond et al. Improving the Accessibility and Efficiency of Point-of-Care Di-agnostics Services in Low-and Middle-Income Countries: Lean and Agile Supply ChainManagement. 2017.
[23] Drain, Paul K. et al. Evaluating Diagnositic Point-of-Care Tests in Resource-LimitedSettings. 2014.
[24] https://www.nimh.nih.gov/health/statistics/global/global-leading-categories-of-diseases-disorders-ylds.shtml
[25] https://ourworldindata.org/burden-of-disease
[26] Pokric, Biserka, and Zvonimir Pucar. ”The two-cross immunodiffusion technique: Dif-fusion coefficients and precipitating titers of IgG in human serum and rabbit serumantibodies.” Analytical biochemistry 93 (1979): 103-114.
[27] Saha, K., F. Bender, and E. Gizeli. ”Comparative study of IgG binding to proteins Gand A: nonequilibrium kinetic and binding constant determination with the acousticwaveguide device.” Analytical chemistry 75.4 (2003): 835-842. APA
[28] https://www.thermofisher.com/us/en/home/references/protocols/cell-and-tissue-analysis/elisa-protocol/general-elisa-protocol.html#prot4
[29] https://en.wikipedia.org/wiki/Damkhler-numbers
25