Embed Size (px)
Citation preview
Huntsman Cancer Institute Eighth Annual
Hematology Review
A review of advances in benign and malignant hematology
Saturday, February 24, 2018

Contents Introduction ................................................................................................................................................................................... 1
Accreditation ................................................................................................................................................................................. 2
Speaker and Planning Committee Disclosure Summary ............................................................................................. 3
Grant Support ................................................................................................................................................................................ 5
Instructions for Claiming and Printing Your Certificate ............................................................................................. 6
Agenda.............................................................................................................................................................................................. 7
Faculty .............................................................................................................................................................................................. 8
Growing UP: Treatment of Young Adults with ALL ................................................................................................................ 9 Wendy Stock, MD
Update on Coagulation ........................................................................................................................................................................ 31 George Rodgers, MD, PhD
Multiple Myeloma: A Year in Review .................................................................................................................................. 41 Douglas Sborov, MD
New Therapeutic Options for AL Amyloidosis........................................................................................................................... 56 Tibor Kovacsovics, MD
Acute Leukemias .................................................................................................................................................... 70 Paul Shami, MD
Cancer Survivorship .............................................................................................................................................................................. 84 Paul Thielking, MD; Rachel Montague, APRN, FNP-C; Brighton Loveday, APRN, ANP-BC; Jacyln Piper-Williams, APRN, FNP-C
Differential Diagnosis of Polycythemias and New Clinical Data on Ph-negative MPNs ....................................... 108 Josef Prchal, MD
Advances in the Treatment of Lymphoma and CLL ............................................................................................................... 124 Martha Glenn, MD

Huntsman Cancer Institute
Eighth Annual Hematology Review
Salt Lake City, Utah
Welcome to the eighth Huntsman Cancer Institute Annual Hematology Review. The goal of this course is to provide a comprehensive review and update on the state-of- the-art management of benign and malignant hematologic diseases. This academic course will provide an opportunity t o learn about new approaches for the diagnosis, prognostication, treatment, and care of these diseases.
The lectures are provided by speakers with expertise in each covered discipline. We welcome your feedback regarding the organization and content. This will help us in planning future meetings.
Course Director
Paul J. Shami, MD
Professor, Division of Hematology and Hematologic Malignancies Huntsman Cancer Institute
University of Utah Salt L ake City, Utah
This conference is supported by an educational grant from Novartis.
Exhibitors include: Adaptive Biotech, Amgen, ARIAD, Brisol-Myers Squibb, Genentech, Gilead, Incyte, Janssen Biotech, Merck, Onyx, Pfizer, Novartis and Takeda
Huntsman Cancer Institute Eighth Annual Hematology Review 1

Huntsman Cancer Institute 8th Annual Hematology Review February 24, 2017
Huntsman Cancer Institute – Eccles Auditorium
Accreditation: The University of Utah School of Medicine is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians.
AMA Credit: The University of Utah School of Medicine designates this live activity for a maximum of 7.0 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Nondiscrimination and Disability Accommodation Statement: The University of Utah does not exclude, deny benefits to or otherwise discriminate against any person on the basis of race, color, national origin, sex, disability, age, veteran’s status, religion, gender identity/expression, genetic information, or sexual orientation in admission to or participation in its programs and activities. Reasonable accommodations will be provided to qualified individuals with disabilities upon request, with reasonable notice. Requests for accommodations or inquiries or complaints about University nondiscrimination and disability/access policies may be directed to the Director, OEO/AA, Title IX/Section 504/ADA Coordinator, 201 S President’s Circle, RM 135, Salt Lake City, UT 84112, 801-581-8365 (Voice/TTY), 801-585-5746 (Fax).
Acknowledgment of Commercial Support: We would like to thank the following commercial interest company for the generous grant in support of our conference: Novartis.
Huntsman Cancer Institute Eighth Annual Hematology Review 2
Instructions for Course Coordinators:
Copy & paste the information below into an email. This will go to all participants registered for your course. This information MUST be given to participants before your course begins. If it does not go out before your course as an email, this information must be printed and given to every participant.
Please include [email protected] in your email so we have documentation this was sent. Please have a few hard copies on hand at your course to give to any ‘walk-ins’.
Please feel free to add any additional information to this email (parking instructions, directions, etc.).
Thank you for registering for the:
8th Annual HCI Hematology Course February 24th, 2018
HCI
Accreditation: The University Of Utah School Of Medicine is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians.
AMA Credit: The University of Utah School of Medicine designates this live activity for a maximum of 7.00 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
NONDISCRIMINATION AND DISABILITY ACCOMMODATION STATEMENT: The University of Utah does not exclude, deny benefits to or otherwise discriminate against any person on the basis of race, color, national origin, ethnicity, sex, disability, age, veteran’s status, religion, gender identity, gender expression, genetic information, or sexual orientation in admission to or participation in its programs and activities. Reasonable accommodations will be provided to qualified individuals with disabilities upon request, with reasonable notice. Requests for accommodations or inquiries or complaints about University nondiscrimination and disability/access policies may be directed to the Director, OEO/AA, Title IX/Section 504/ADA Coordinator, 201 S President’s Circle, RM 135, Salt Lake City, UT 84112, 801-581-8365 (Voice/TTY), 801-585-5746 (Fax).
Speaker and Planning Committee Disclosure Summary: The University Of Utah School Of Medicine Continuing Medical Education Office meets the ACCME expectations regarding the identification and resolution of conflicts of interest that arise from financial relationships with commercial interests.
Financial relationships are those relationships in which the individual benefits by receiving a salary, royalty, intellectual property rights, consulting fee, honoraria, ownership interest (e.g., stocks, stock
Huntsman Cancer Institute Eighth Annual Hematology Review 3

options or other ownership interest, excluding diversified mutual funds), or other financial benefit. Financial benefits are usually associated with roles such as employment, management position, independent contractor (including contracted research), consulting, speaking and teaching, membership or advisory committees or review panels, board membership, and other activities from which remuneration is received, or expected. We consider relationships of the person involved in the CME activity to include financial relationships of a spouse or partner.
Everyone in control of content, including all speakers and planners are expected to disclose any relevant financial relationships in any amount within the past 12 months. Speakers are also expected to openly disclose intent to discuss any off-label, experimental, or investigational use of drugs, devices, or equipment in their presentations.
No one in The University of Utah Continuing Medical Education Office in control of content for the course has any relevant financial relationship with commercial products or services discussed during this conference.
Your Name Role Role Role
Relevant Financial Relationships
Commercial Interest & Role/Nature of Relationship
Nicole Felkel Planner No
Wendy Stock Speaker Yes pfizer, advisory board; jazz, advisory boardDeidre Moore Planner NoMartha Glenn Planner Speaker No
Paul Shami Planner Speaker Moderator Yes Pfizer - Advisory Board Meeting.Sarah Stice-Goff Planner NoMarie Asay Planner No
George Rodgers Speaker Yes Novartis-consultingPaul Thielking Speaker NoJosef Prchal Speaker NoBrighton Loveday APRN Planner Speaker NoRachel Montague Planner Speaker No
Tibor Kovacsovics Speaker YesProthena, research support; Janssen, research support
Douglas W Sborov MD MS Speaker NoJaclyn Piper-Williams Speaker No
Huntsman Cancer Institute Eighth Annual Hematology Review 4

HUNTSMAN CANCER INSTITUTE EIGHTH ANNUAL HEMATOLOGY REVIEW
A REVIEW OF ADVANCES IN BENIGN AND MALIGNANT HEMATOLOGY
SPONSORED BY The Division of Hematology and Hematologic Malignancies, Department of Internal Medicine,
and Huntsman Cancer Institute, University of Utah
GRANT SUPPORT NOVARTIS
Huntsman Cancer Institute Eighth Annual Hematology Review 5

Instructions for Course Coordinators:
Copy & paste the instructions below into an email. This will need to go to all participants once your course is complete. Include [email protected] in your email so we have documentation that this has been sent. Have a few hard copies on hand at your course to give to any registrants who might request this.
The link below will ask participants to complete an evaluation of your course, as well as claim their credit for participating. If participants do not “claim their credit, they will not be awarded the credit and will not receive a certificate.
Please feel free to add any additional information to your email.
8th Annual HCI Hematology Course February 24th, 2018
HCI Thank you for your participation in our course! Please complete the short course evaluation by following the link below. The evaluation should take less than 5 minutes.
Once you complete the evaluation, the link will prompt you to claim your CME credit for this course. Thank you!
Instructions for Claiming Credit and Printing Your Certificate:
(Note: There will be a series of screens please follow the directions on each screen).
1. To complete a short evaluation, claim your credit and print your course certificate please go tothe following link:
http://goo.gl/nrJKrN
2. When prompted enter your email address. If you are a new user, select “new user” andcomplete some short identifying information about yourself.
3. Enter the password; if you do not have a password you will be able to create one.4. Enter the following CME Activity code: 438135. Complete the short evaluation6. Enter the number of credits commensurate with your participation in the activity, up to 7.00
which is the number of AMA PRA Category 1 Credit(s)TM credits this activity is certified for.7. If you encounter any problems please call the UUCME office at 801-581-6886.
Huntsman Cancer Institute Eighth Annual Hematology Review 6

Huntsman Cancer Institute Seventh Annual Hematology Review Huntsman Cancer Institute Eccles Auditorium
February 24, 2018
Agenda
7:15 a.m. Registration and Breakfast
7:55 a.m. Welcome Paul J. Shami, MD
8:00 a.m. ALL AYA Wendy Stock, MD Keynote Speaker
9:00 a.m. Coagulation George Rodgers, MD, PhD
9:45 a.m. Break
10:00 a.m. Multiple Myeloma Douglas Sborov, MD
10:45 p.m. Amyloidosis Tibor Kovacsovics, MD
11:30 a.m. Acute Leukemias Paul Shami, MD
12:15 p.m. Lunch
1:15 p.m. Survivorship Rachel Montague, APRN Brighton Loveday, APR Jaclyn Piper-Williams APRN Paul Thielking, MD
2:45 p.m. Break
3:00 p.m. MPD Josef Prchal, MD
3:45 p.m. Lymphoma Martha Glenn, MD
4:30 p.m. Wrap-up and Evaluations Paul J. Shami, MD
Huntsman Cancer Institute Eighth Annual Hematology Review 7

Faculty
Keynote Speaker: Wendy Stock, MD Anjuli Seth Nayak Professor in Leukemia, University of Chicago School of Medicine
Martha Glenn, MD Professor, Division of Hematology and Hematologic Malignancies, University of Utah
Tibor Kovacsovics, MD Professor, Division of Hematology and Hematologic Malignancies, University of Utah
Brighton Loveday, APRN Rachel Montague, APRN Jaclyn Piper-Williams, APRN Nurse Practitioners, Supportive Oncology and Survivorship, Huntsman Cancer Institute
Josef Prchal, MD Professor, Division of Hematology and Hematologic Malignancies, University of Utah
George Rodgers, MD, PhD Professor, Division of Hematology and Hematologic Malignancies, University of Utah
Douglas Sborov, MD, MS Assistant Professor, Division of Hematology and Hematologic Malignancies, University of Utah
Paul Shami, MD Professor, Division of Hematology and Hematologic Malignancies, University of Utah
Paul Thielking, MD Assistant Professor, Department of Psychiatry, University of Utah
Huntsman Cancer Institute Eighth Annual Hematology Review 8
Huntsman Cancer Institute Eighth Annual
Hematology Review
Growing UP: Treatment of Young Adults with ALL
Wendy Stock, MD
Huntsman Cancer Institute Eighth Annual Hematology Review 9

Growing UP: Treatment of Young Adults with ALL
Striving towards PRECISION MEDICINEImproving Outcomes
Wendy Stock, MDUniversity of Chicago Medicine
Disclosures
• Research funding: Sigma Tau (Baxalta)
• Advisory Boards: Amgen, Pfizer, SeattleGenetics
• Honoraria: Up to Date
• Service honoraria:, NCI (CTEP leukemiasteering committee), American Society ofHematology
Jim Nachman, 2011
“Pediatricians know best!”……how to treat ALL!”
Huntsman Cancer Institute Eighth Annual Hematology Review 10
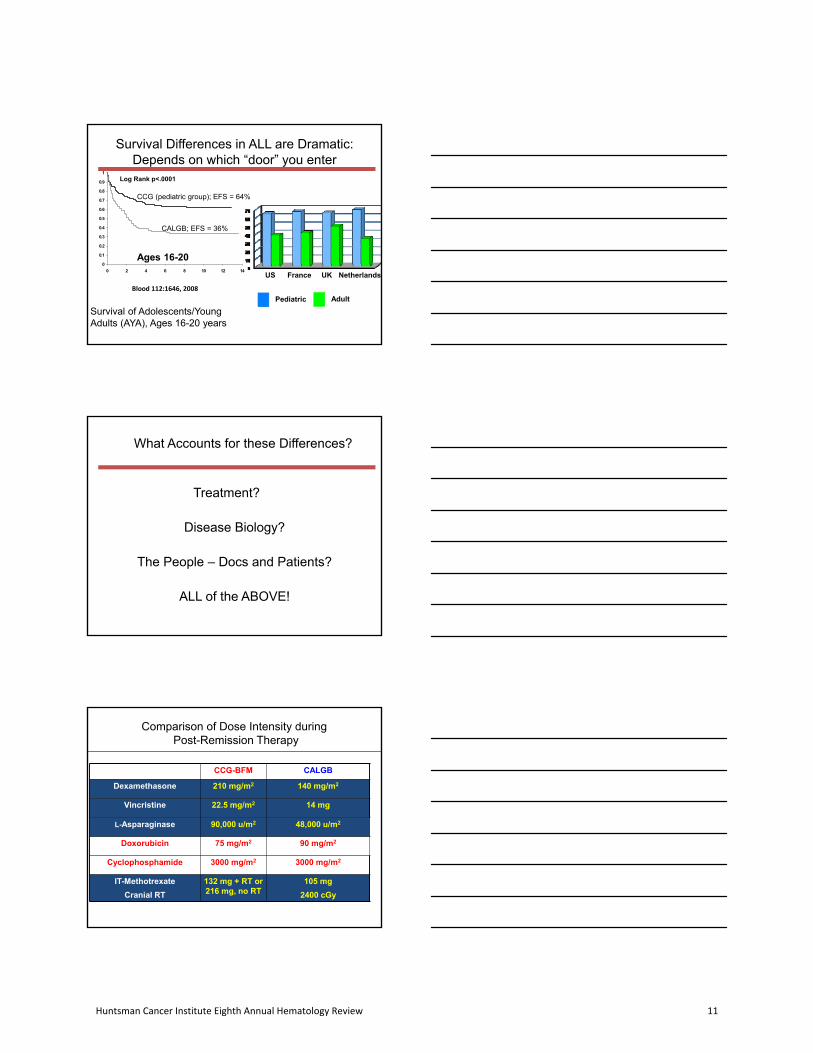
Survival Differences in ALL are Dramatic: Depends on which “door” you enter
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 2 4 6 8 10 12 14
Log Rank p<.0001
Ages 16-20
Pediatric Adult
US France NetherlandsUK
CCG (pediatric group); EFS = 64%
CALGB; EFS = 36%
Survival of Adolescents/Young Adults (AYA), Ages 16-20 years
Blood 112:1646, 2008
Pediatric Adult
What Accounts for these Differences?
Treatment?
Disease Biology?
The People – Docs and Patients?
ALL of the ABOVE!
Comparison of Dose Intensity duringPost-Remission Therapy
CCG-BFM CALGB
Dexamethasone 210 mg/m2 140 mg/m2
Vincristine 22.5 mg/m2 14 mg
L-Asparaginase 90,000 u/m2 48,000 u/m2
Doxorubicin 75 mg/m2 90 mg/m2
Cyclophosphamide 3000 mg/m2 3000 mg/m2
IT-Methotrexate
Cranial RT
132 mg + RT or 216 mg, no RT
105 mg
2400 cGy
Huntsman Cancer Institute Eighth Annual Hematology Review 11

Cytogenetics of ALL as Function of Patient Age
Moorman et al, Brit J Haemat 10.1111,1365, 2008
????
Proportion of Patients Treated at NCICCC/COG Sites
63% 63%
70%74%
34%30%
51%
42%
10% 8%12%
16%
0%
10%
20%
30%
40%
50%
60%
70%
80%
NHL HL ALL AML
1‐14y 15‐21y 22‐39y
p<0.0001
Wolfson J et al, Cancer Epidemiol Biomarkers Prev; 26(3); 312–20. ©2017
Goals of US Intergoup Trial (10403)
• Estimate feasibility and DFS using a successful COG regimen in adult cooperative group setting in USA– Flow sheets to evaluate compliance with doses/schedule ofchemotherapy
• Obtain insights into age‐specific molecular pathogenesis and toidentify prognostic markers– MRD studies: characterize patients likely to relapse– Partnership with COG/St. Jude for GWAS studies
• New knowledge of psycho‐social and socio‐economic issues of AYA population – Patient survey at three treatment time‐points
Huntsman Cancer Institute Eighth Annual Hematology Review 12
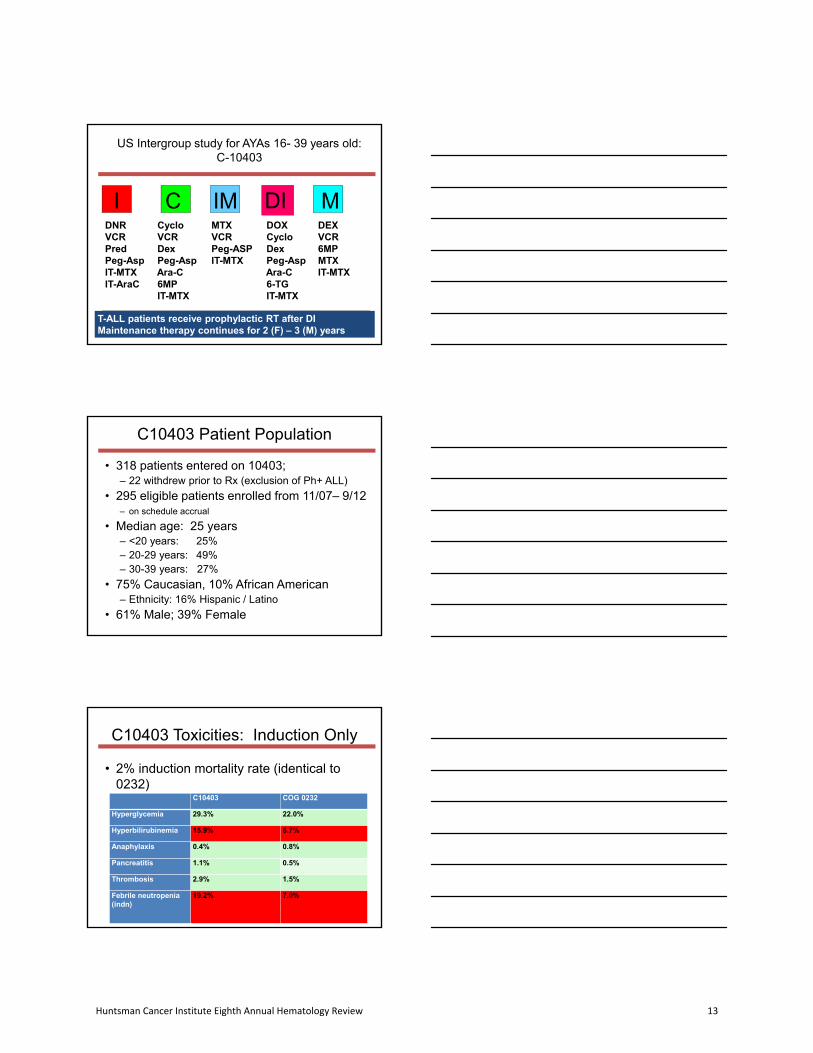
US Intergroup study for AYAs 16- 39 years old: C-10403
I DIC MIM
T-ALL patients receive prophylactic RT after DIMaintenance therapy continues for 2 (F) – 3 (M) years
DNRVCRPredPeg-AspIT-MTXIT-AraC
CycloVCRDexPeg-AspAra-C6MPIT-MTX
MTXVCRPeg-ASPIT-MTX
DOXCycloDexPeg-AspAra-C6-TGIT-MTX
DEXVCR6MPMTXIT-MTX
Accrual completed on 9/15/12 (n = 300)
C10403 Patient Population
• 318 patients entered on 10403;– 22 withdrew prior to Rx (exclusion of Ph+ ALL)
• 295 eligible patients enrolled from 11/07– 9/12– on schedule accrual
• Median age: 25 years– <20 years: 25%– 20-29 years: 49%– 30-39 years: 27%
• 75% Caucasian, 10% African American– Ethnicity: 16% Hispanic / Latino
• 61% Male; 39% Female
C10403 Toxicities: Induction Only
• 2% induction mortality rate (identical to0232)
C10403 COG 0232
Hyperglycemia 29.3% 22.0%
Hyperbilirubinemia 15.9% 6.7%
Anaphylaxis 0.4% 0.8%
Pancreatitis 1.1% 0.5%
Thrombosis 2.9% 1.5%
Febrile neutropenia (indn)
19.2% 7.0%
Huntsman Cancer Institute Eighth Annual Hematology Review 13

No significant differences in toxicity at later time‐points in treatment
Hepatic 10403 0232
Liver failure 1.0 1.9
ALT 50.0 48.7
AST 30.2 22.2
Bilirubin 22.9 24.7
Pancreatitis 4.2 3.8
Low overall treatment related mortality of 3%; identical to COGAALL0232 AYAs
10403: Event‐free and Overall Survival
All Patients
3 yr EFS = 61%
3 year OS = 73%
Obesity Associated with Poor Survival
p = 0.0003
Huntsman Cancer Institute Eighth Annual Hematology Review 14
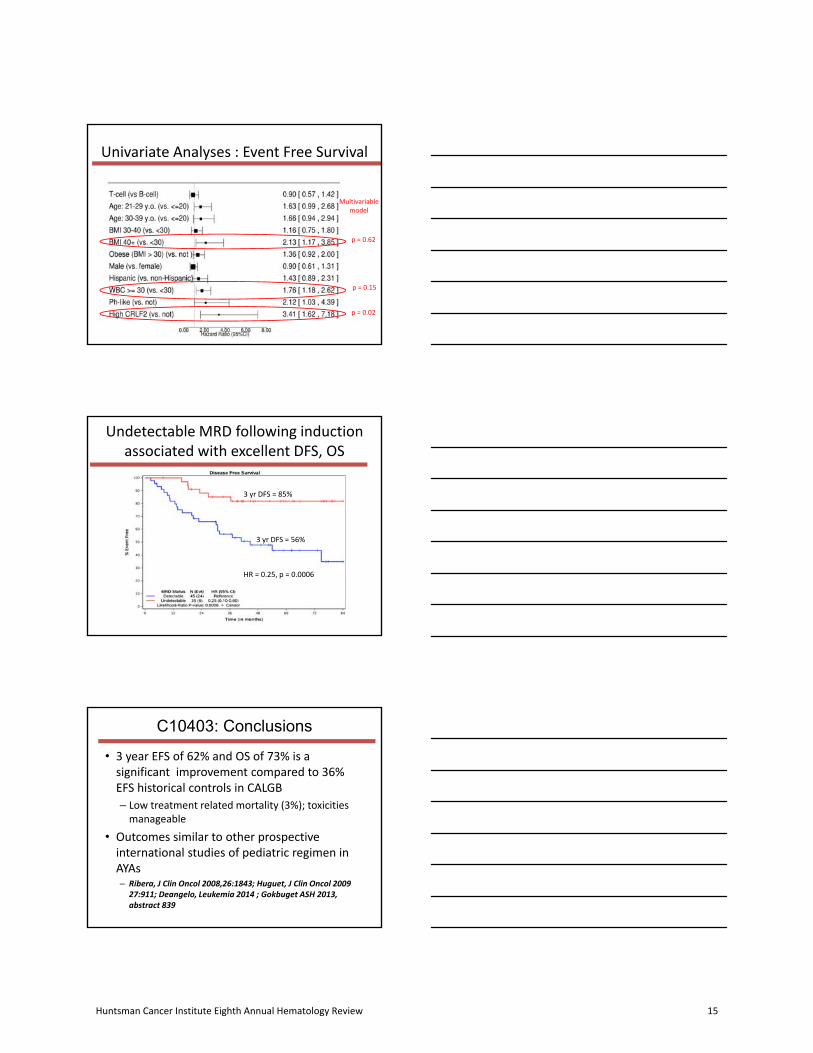
Multivariable model
p = 0.62
p = 0.02
p = 0.15
Univariate Analyses : Event Free Survival
Undetectable MRD following induction associated with excellent DFS, OS
HR = 0.25, p = 0.0006
3 yr DFS = 85%
3 yr DFS = 56%
C10403: Conclusions
• 3 year EFS of 62% and OS of 73% is asignificant improvement compared to 36%EFS historical controls in CALGB
– Low treatment related mortality (3%); toxicities manageable
• Outcomes similar to other prospectiveinternational studies of pediatric regimen inAYAs – Ribera, J Clin Oncol 2008,26:1843; Huguet, J Clin Oncol 2009
27:911; Deangelo, Leukemia 2014 ; Gokbuget ASH 2013, abstract 839
Huntsman Cancer Institute Eighth Annual Hematology Review 15
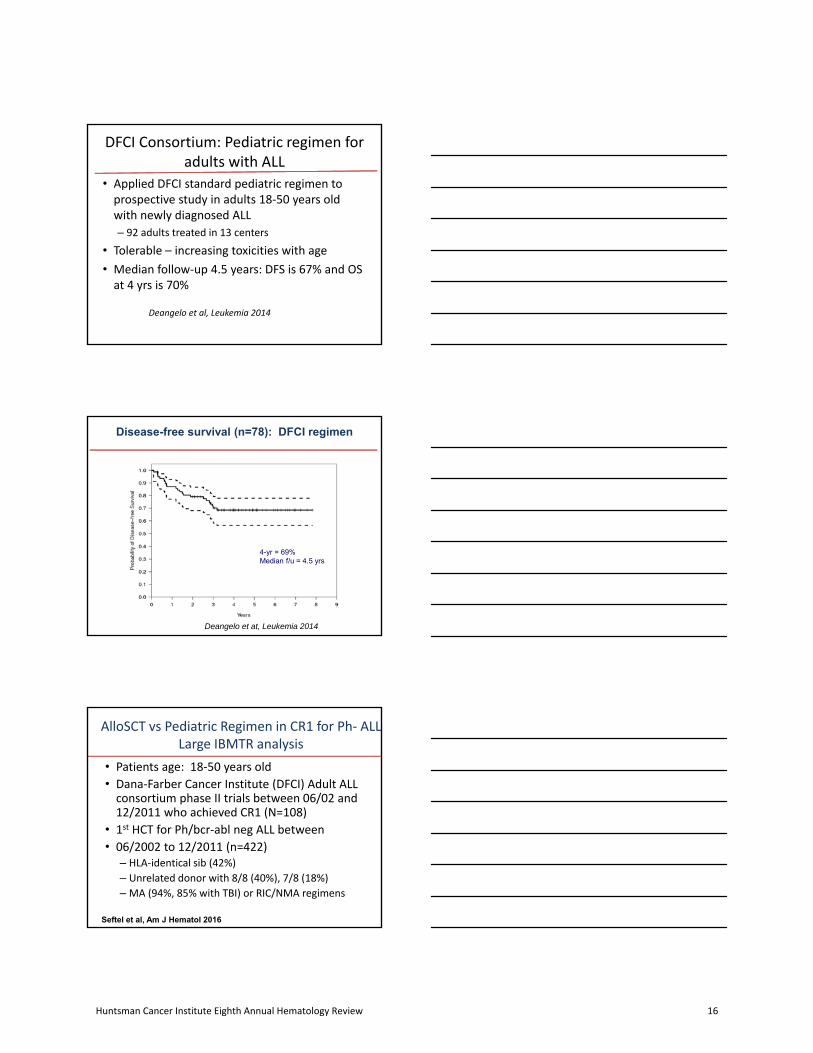
DFCI Consortium: Pediatric regimen for adults with ALL
• Applied DFCI standard pediatric regimen toprospective study in adults 18‐50 years oldwith newly diagnosed ALL
– 92 adults treated in 13 centers
• Tolerable – increasing toxicities with age
• Median follow‐up 4.5 years: DFS is 67% and OSat 4 yrs is 70%
Deangelo et al, Leukemia 2014
Disease-free survival (n=78): DFCI regimen
4-yr = 69%Median f/u = 4.5 yrs
Deangelo et at, Leukemia 2014
AlloSCT vs Pediatric Regimen in CR1 for Ph‐ ALLLarge IBMTR analysis
• Patients age: 18‐50 years old
• Dana‐Farber Cancer Institute (DFCI) Adult ALLconsortium phase II trials between 06/02 and12/2011 who achieved CR1 (N=108)
• 1st HCT for Ph/bcr‐abl neg ALL between
• 06/2002 to 12/2011 (n=422)– HLA‐identical sib (42%)
– Unrelated donor with 8/8 (40%), 7/8 (18%)
– MA (94%, 85% with TBI) or RIC/NMA regimens
Seftel et al, Am J Hematol 2016
Huntsman Cancer Institute Eighth Annual Hematology Review 16
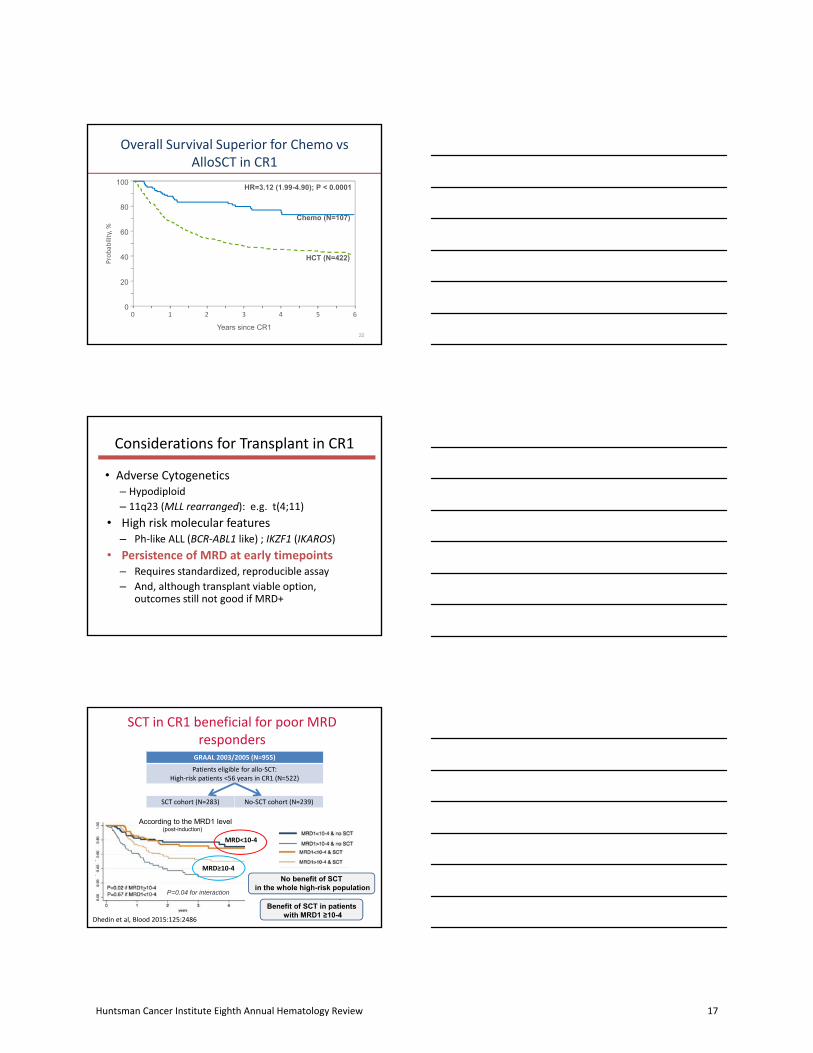
Overall Survival Superior for Chemo vsAlloSCT in CR1
22
100
0
20
40
60
80
Probab
ility, %
Years since CR1
HR=3.12 (1.99-4.90); P < 0.0001
Chemo (N=107)
HCT (N=422)
0 2 64 531
Considerations for Transplant in CR1
• Adverse Cytogenetics– Hypodiploid
– 11q23 (MLL rearranged): e.g. t(4;11)
• High risk molecular features– Ph‐like ALL (BCR‐ABL1 like) ; IKZF1 (IKAROS)
• Persistence of MRD at early timepoints– Requires standardized, reproducible assay
– And, although transplant viable option, outcomes still not good if MRD+
SCT in CR1 beneficial for poor MRD responders
GRAAL 2003/2005 (N=955)
Patients eligible for allo‐SCT:High‐risk patients <56 years in CR1 (N=522)
SCT cohort (N=283) No‐SCT cohort (N=239)
Dhedin et al, Blood 2015:125:2486
P=0.04 for interaction
According to the MRD1 level(post-induction)
Benefit of SCT in patientswith MRD1 ≥10-4
No benefit of SCTin the whole high-risk population
MRD<10‐4
MRD≥10‐4
Huntsman Cancer Institute Eighth Annual Hematology Review 17
NEXT STEPS: INTEGRATING NEW TREATMENT STRATEGIES, NEW BIOLOGIC INSIGHTS
The melding of biology and therapy
What’s Next for AYA ALL ?
• Integrate biology/new targets: Eradicate MRD– Antibodies/Targeted kinase inhibitors/CAR‐Ts
• Rituximab – GRAALL Phase III trial : EFS and OS advantage
• Blinatumomab (frontline for older adults – E1910)
– Can addition of inotuzumab ozogamycin (InO) eradicate MRD and improve survival in AYA ALL?
– Can novel antibodies also improve outcome of patients with Ph‐like ALL?
– Use 10403 backbone and add new targeted therapies to eradicate MRD
• Insights, adjustments to reduce toxicities
•Patients with newly-diagnosed previouslyuntreated Ph-negative B-cell precursor (BCP)ALL 18-59 years old
– With ≥ 20% bone marrow non-Burkitt ALL blasts
•Positive for CD20 expression– Defined as 20% or more CD20+ leukemic blasts
•Patients could receive allogeneic transplant inCR1
Phase III Trial of Intensive BFM-like regimen+\- Rituximab: GRAALL-R 2005
Maury et al, NEJM 2016
Huntsman Cancer Institute Eighth Annual Hematology Review 18

Improved EFS for CD20+ ALL: GRAALL‐R
• After censoring at SCT in CR1: HR, 0.59 [0.37-0.93]; p= 0.021
Median follow-up, 30 months
Maury et al, NEJM 9.16
Inotuzumab Phase III trial: INOVATE
Ara‐C=cytarabine; FLAG=fludarabine/ara‐C/granulocyte colony‐stimulating factor; HIDAC=high‐dose ara‐C; Ph=Philadelphia chromosome
• Relapsed/refractory CD22+ ALL
• Due for salvage 1 or 2 therapy
• Ph– or Ph+
1:1 Randomization(N=326)
Inotuzumab ozogamicin (InO)
•Starting dose 1.8 mg/m2/cycle
•0.8 mg/m2 on day 1;0.5 mg/m2 on days 8 and 15 of a 21–28 day cycle (≤6 cycles)
Standard of Care (SOC)
• FLAG or
• Ara‐C plus mitoxantrone or
• HIDAC
• ≤4 cycles
Stratifications:
• Duration of 1st remission ≥12 vs <12 mo
• Salvage 2 vs 1
• Aged ≥55 y vs <55 y
326 patients randomized at 117 sites in 19 countries (INO‐VATE ALL; NCT01564784)
InO dose was reduced to 1.5 mg/m2/cycle once the patient achieved CR/CRi
Kantarjian et al, N Engl J Med, 6/2016
Inotuzumab vs Standard of CareINOVATE: Relapsed ALL
InO Standard of care1-Sided P Value
Na 109 96
CR/CRi,% (95% CI)
80.7 (72−88) 33.3 (24−44) <0.0001
CR 35.8 (27−46) 19.8 (12−29) 0.0056
CRi 45.0 (35−55) 13.5 (7−22) <0.0001
MRD-negativity among responders, n (%) [95% CI]
CR/CRi 69/88 (78.4) [68−87] 9/32 (28.1) [14−47] <0.0001
CR 35/39 (89.7) [76−97] 6/19 (31.6) [13−57] <0.0001
CRi 34/49 (69.4) [55−82] 3/13 (23.1) [5−54] 0.0034Kantarjian et al, NEJM, 2016
Huntsman Cancer Institute Eighth Annual Hematology Review 19

A041501 for AYAs 18-39: Opened to accrual fall 2017
Ph‐negCD22+16‐40
C10403Induction
R
NoINO
2 Cycles INO
C10403Consol.Maint.
Stratification*:Age
LDA‐cardCD20
Primary Endpoint:3‐yr EFS
*Based on GRAALL data , we will incorporate rituximab in non‐random fashion for all CD20+ patients
US Intergroup study for AYA: A041501 Randomized Phase III trial
I DIC MIM
*CD20+ Patients will Receive Rituximab with C, IM, DIMaintenance therapy continues for 2 (F) – 3 (M) years
DNRVCRDexPeg-AspIT-MTXIT-AraC
CycloVCRDexPeg-AspAra-C6MPIT-MTX
Rituximab
MTXVCR
Peg-ASPIT-MTX
Rituximab
DOXCycloDexPeg-AspAra-C6-TGIT-MTXRituximab
DEXVCR6MPMTXIT-MTX
Inotuzumab
Can we reduce treatment toxicity?
• More work needed to optimize PEG‐aspdosing in AYAs with ALL– Reduce dose but still achieve adequate depletion?
• May be most important during induction cycle• Cap dose?
• Obesity related toxicity
– Important insights will be obtained in the A041501 from study of asparaginase levels
• Now routinely available as CLIA/CAP approved test
• Will also detect silent inactivation if it occurs
Huntsman Cancer Institute Eighth Annual Hematology Review 20

Pharmacogenomics
• Pharmacogenomics: genetic polymorphismsaffect metabolism, impact toxicity– Myelosuppression – TPMT (6-MP)
– Osteonecrosis (glucocorticoids, asparaginase)• Karol et al, Blood 127;2016
– Pancreatitis -CPA2 (glucocorticoids,asparaginase)
• Liu et al, J Clin Oncol 34; 2015– Hepatotoxicity –SOD2 (asparaginase)
• Alachkar et al, Pharmacogenomics J. 2016, PMID27019981
– Neuropathy CEP72 (vincristine)• Diouf et al JAMA. 2015;313(8):815‐23
An Inherited Genetic Variant in CEP72 Promoter Predisposes to Vincristine‐Induced Peripheral Neuropathy in Adults with ALL
Clinical Pharmacology & Therapeuticspages 391‐395, 16 NOV 2016 DOI: 10.1002/cpt.506http://onlinelibrary.wiley.com/doi/10.1002/cpt.506/full#cpt506‐fig‐0001
‐CEP72 involved in mitotic spindle formation
‐CEP72 risk allele (T) results in decreased CEP72 expression
‐Knockdown of CEP72 results in increased sensitivity to vincristine (iPS model)
IMPLICATION‐Suggests that it may be possible to reduce dose of vincristine, decrease neuro‐tox, without compromise of efficacy
The rs4880 SOD2 SNP genotype frequencies in adults with ALL:CC genotype is associated with higher rates of hepatotoxicity
Alachkar et al, Pharmacogenomics 2017, 17:274
CC genotype is more common among self‐reported Hispanic ethnicity
Huntsman Cancer Institute Eighth Annual Hematology Review 21

Modulating Asparaginase Toxicity?
• Pilot study of 41 pts (median age of 43);– 15 received reduction in Peg‐Asp dosing with goal of achieving therapeutic asparaginase level and assessment of hepatic toxicity
• Dose ‐ 1000U/m2 IV vs standard dose of 2750U/m2
– Further dose reduction to 500 U/m2 if BMI>30, Age> 50,Baseline LFT abnormalities, Diabetes
• Goal was ≥ 0.1 IU/mL, measured weekly after dose• 80% achieved therapeutic levels with lower dose• Overall, trend towards decreased hepatotoxicity with
significant decrease in grade 3/4 hyperbilirubinemia– Occurred in 12 (46%) standard dose vs 1 (7%), p=0.014
Streck et al, ASCO 2017
BCR‐ABL1 like or Ph1‐like ALL:Important, new biological Subset
• 26 year old man: New diagnosis of ALL
• B‐ALL; CD19+,CD10+, Tdt+; 28% circulatinglymphoblasts
• Cytogenetics, 46 XY
• Initial CSF – clear
• Induction according to 10403
• Induction course uncomplicated
• Day 14 marrow: hypocellular (10%), with residualALL (40‐50% Tdt+)
• Day 28 marrow……..
(BM biopsy, Images courtesy of Dr. SandeepGurbuxani, UChicago)
Post‐induction Bone Marrow Biopsy
Day 29 of Induction:
Hypercellular Marrow
Gross Residual Disease
Huntsman Cancer Institute Eighth Annual Hematology Review 22

Discovery of Novel Subset of ALL:“BCR‐ABL1‐Like” or “Ph‐like” ALL
• “Ph‐like” ALL or “BCR‐ABL1‐like” ALL:– ≥ 10‐15% childhood ALL– Gene expression profile similar to BCR‐ABL1 ALL
• den Boer, Lancet Oncol 2009:10
– Very poor treatment outcome • Mullighan NEJM 2009; Harvey/Chen Blood 2010;
Loh, Blood 2013
– 50% have CRLF2 alterations, the majority have JAK mutations
– Remaining 50% have cryptic translocations or small deletions in genes encoding tyrosine kinases or genes deregulating kinase signaling: ABL1/2, CSF1R, EPOR, IL7R, JAK2, PDGFRB
• Roberts, Cancer Cell 2012
21 3 87654
0 1 2 3 4 5 6
0.0
0.2
0.4
0.6
0.8
1.0
Years
Pro
ba
bili
ty o
f RF
S
Kinase Fusions Retain Intact Tyrosine Kinase domains: Targets!
Childhood H
R
Adolesc
ent (
16-2
1 yr
s)
Young adult
(21-
39 y
rs)
% c
ases
Kathryn Roberts, NEJM, 2014
High proportion of JAK alterations in AYA Ph‐like ALL
Kinase gene TKI % of children % of AYAs
ABL1, ABL2, CSFR1, PDGFRB
Dasatinib 17% 6‐9%
CRLF2, JAK2, EPOR,IL2RB, TSLP
JAK2 inhibitor 68% 74‐87%
Others Crizotinib, TYK2 inhibitor, FAK inhibitor, unknown
15% 6‐17%
Huntsman Cancer Institute Eighth Annual Hematology Review 23

BCR-ABL1 like signature occurs in 28% of 10403 patients and is associated with poor EFS
3 yr OS = 81%
3 yr OS = 63%
Aberrant CRLF2 associated with worse outcomes among Ph‐like ALL
CRLF2 Subgroup of Ph‐like ALL:Worst Outcomes
Ph‐like ALL
Courtesy, Nitin Jain
Huntsman Cancer Institute Eighth Annual Hematology Review 24

Gene Expression “Chip” Identifies Ph‐Like ALL
• The COG (Willman et al) developed a CLIA‐approved adaptable screening assay to identifyPh+‐like ALL using 8 gene “chip array”
Reshmi et al, Blood. 2017 Jun 22;129(25):3352-3361.
Event-Free Survival Overall Survival
Ph+‐like
Not Ph+‐like
Current diagnostic pipeline for Ph‐like cases at UChicago
Flow cytometry for CRLF2 expression
FISH panel for Ph‐like associated most recurrent rearrangements
Chromosomal Microarray Analysis
Targeted RNA seq (not ready for prime time)Yap et al, Leukemia and Lympohoma, 58, 2017
Ph‐like ALL FISH panel: UChicago(3’ regions of the genes are involved in fusion event)
• CRLF2 break‐apart probe (Kreatech)
• IGH break‐apart probe (Vysis)
• ABL2 break‐apart probe (Empire genomics)
• CSF1R break‐apart probe (Empire)
• PDGFRB break‐apart probe (Vysis)
• JAK2 break‐apart probe (Kreatech)
• BCR/ABL1 (Vysis) – NUP214‐ABL
Expected pattern: break‐apart of a fusion signal in case of translocation or loss of 5’region signal in case of intrachromosomal deletions
CRLF2 Break-apart
Courtesy, G. Raca, M. Sukhanova
Huntsman Cancer Institute Eighth Annual Hematology Review 25
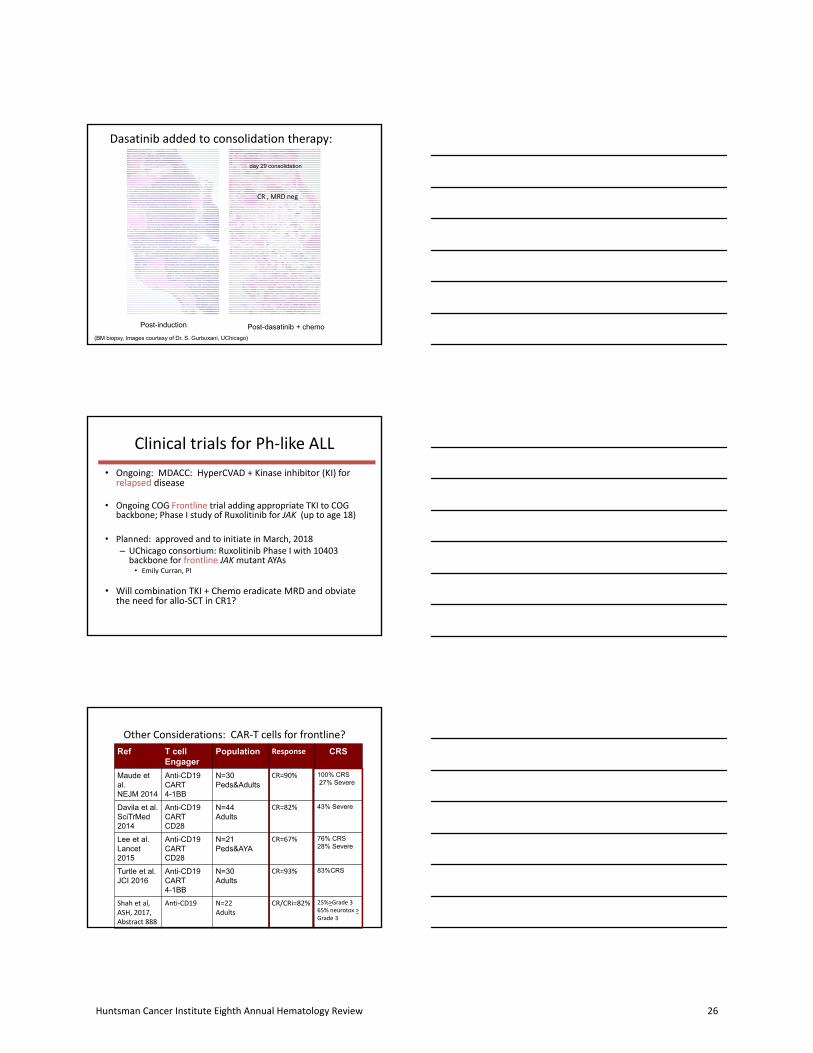
Post-induction Post-dasatinib + chemo
(BM biopsy, Images courtesy of Dr. S. Gurbuxani, UChicago)
day 29 consolidation
Dasatinib added to consolidation therapy:
CR , MRD neg
Clinical trials for Ph‐like ALL
• Ongoing: MDACC: HyperCVAD + Kinase inhibitor (KI) forrelapsed disease
• Ongoing COG Frontline trial adding appropriate TKI to COG backbone; Phase I study of Ruxolitinib for JAK (up to age 18)
• Planned: approved and to initiate in March, 2018– UChicago consortium: Ruxolitinib Phase I with 10403 backbone for frontline JAK mutant AYAs
• Emily Curran, PI
• Will combination TKI + Chemo eradicate MRD and obviatethe need for allo‐SCT in CR1?
Other Considerations: CAR‐T cells for frontline?
Ref T cellEngager
Population Response CRS
Maude et al.NEJM 2014
Anti-CD19CART4-1BB
N=30Peds&Adults
CR=90% 100% CRS27% Severe
Davila et al.SciTrMed2014
Anti-CD19CARTCD28
N=44Adults
CR=82% 43% Severe
Lee et al.Lancet 2015
Anti-CD19CARTCD28
N=21Peds&AYA
CR=67% 76% CRS28% Severe
Turtle et al.JCI 2016
Anti-CD19CART4-1BB
N=30Adults
CR=93% 83%CRS
Shah et al,ASH, 2017,Abstract 888
Anti‐CD19 N=22Adults
CR/CRi=82% 25%>Grade 365% neurotox >Grade 3
Huntsman Cancer Institute Eighth Annual Hematology Review 26
Overcoming Treatment Resistance: Targeting Survival Pathways
Phase I Trial of Venetoclax/Navitoclax +/‐ Chemotherapy for Relapsed Refractory ALL in children and young adults up to age 45 years
44 year old man: Resistant to 10403 induction, Resistant to Blinatumomab, Resistant to Inotuzumab, Finally CR with CAR‐T followed by MRD alloSCT‐ RELAPSE day 150 post allo‐SCT and enrolled on Phase I trial of Venetoclax/Navitoclax
Pre‐treatment: 11/27/17 Day 8: 12/12/17 Day 36: 1/9/18
CREATION OF YOUNG ADULT CANCER CLINIC
Providing comprehensive care for the young adult with cancer
The AYA Psyche and Adherence
• Lower levels of well‐being than patients withcancer in other age groups
– Higher levels of isolation, depression
• Nonadherence in adolescents and youngadults with cancer are high, ranging from 27‐60%
– Associated with higher rates of morbidity and lower survival rates
– 39% considered stopping treatment
Kroenke et al, JCO 22:1849, 2004; Kondryn et al; Lancet Oncology 12:100, 2011; Bleyer et al, CA Cancer J Clin 57;242, 2007; Kondryn et al Psychooncology 18; 1327, 2009
Huntsman Cancer Institute Eighth Annual Hematology Review 27

“It takes a village”: Creation of AYA clinic
GOALS:
• Comprehensivetherapeutic, physical andpsychosocial support;improved patient well-being and alliance withmedical team
• Improving treatmentcompliance leading tobetter outcomesTrevino et al, JCO 31; 1683,2013
UCHICAGO AYA TEAM 2017
AYA Clinic InitiativesStudy of post‐traumatic stress in AYA patients completing treatment for malignancies
‐Lori Muffly, MD; Cancer, 2016
Study of risky behaviors in AYA receiving treatment
‐Tara Henderson,MD
Piloting tools for assessment of the patient/caregiver (MD/Nursing) “alliance” and treatment complicance
37
17
29
11
35
31
27
12
0 10 20 30 40 50
AnyImpairment
Anxiety
Depression
PTSD
% Impaired
On‐Treatment
Early Survivor
P= 0.99
P= 0.89
P= 0.21
P= 0.84
Frequency of Psychological Impairments Amongst AYAs with Hematologic Malignancies
Muffly et al, Cancer 2016
Huntsman Cancer Institute Eighth Annual Hematology Review 28

Treatment should be at site with expertise in ALL management
• ALL regimens: Compliance, adherence is key– Arduous regimens– More than three years of treatment
• Requires expertise on part of health care team• Requires appropriate support, motivation forpatient and their caregivers
• Emerging data support improved outcomes whenAYAs with ALL treated at NCI cancercenter/cooperative group sites– J Wolfson et et al, Cancer Epidemiol Biomarkers Prev;2017, 26(3); 312–20.
Summary: Treatment of ALL in Young Adults
• Progress made when patients enrolled onclinical trials
• Clinical expertise required
• Psycho‐social support crucial
– Adherence, compliance facilitated
• Exciting time for future progress!
– Building upon a successful “backbone” with addition of novel agents
Thanks to our patients – they are our inspiration
Huntsman Cancer Institute Eighth Annual Hematology Review 29

Faculty/FellowsAndy Artz, MDJane Churpek, MDEmily Curran, MDMichael Drazer, MDLucy Godley, MD, PhDAndrew Hantel, MDTara Henderson, MDSatya Kosuri, MDRichard Larson, MDHongtao Liu, MD, PhDJennifer McNeer, MDToyosi Odenike, MDWendy Stock, MDMichael J. Thirman, MDJoe Wynne, MD, PhDRandy Knoebel, PharmDJenn Anderson, PharmD
HematopathologyJohn Anastasi, MDJason Cheng, MDSandeep Gurbuxani, MD, PhDElizabeth Hyjek, MDGarish Venkataraman, MDJames W. Vardiman, MDDan Arber, MD
Clinical SpecialistsNancy Glavin, RNPeggy Green, RNRebecca Pape, APNJean Ridgeway, APNLauren Ziskind, APNStock LabNoreen Fulton, BSHouda Alachkar, PhDBart Eisfelder, PhD
Cytogenetics and Molecular Genetics
Michelle M. Le Beau, PhDMegan McNerney, MD,PhDY. Lynn Wang, MD, PhD
Madina Sukhanova, PhDJeremy P. Segal, MD, PhD
The Leukemia Program: UC Medicine
ClinicalResearch GroupHowie Weiner, LeaderKristy Johnson, BAMelissa Fridstein, BABelen Aguado, BSChris Ott, BSJudith Murray, BAAlliance LeukemiaRichard Stone, MDJohn Byrd, MD Clara Bloomfield, MDECOG: Selina Luger MDSWOG: Anjali Advani MDCOG/St. JudeCharles Mullighan, MDMary Relling, PharmDBill Evans, PharmDCheryl Willman, MDRichard Harvey, PhDI-Ming Chen, DVM, MS
Huntsman Cancer Institute Eighth Annual Hematology Review 30
Huntsman Cancer Institute Eighth Annual
Hematology Review
Update on Coagulation
George Rodgers, MD
Huntsman Cancer Institute Eighth Annual Hematology Review 31

UPDATE ON COAGULATION
George M. Rodgers, MD
TOPICS
• NOACs vs LMWH in cancer-associated VTE
• Incidental VTE in cancer patients
• Thrombocytopenia in pregnancy
• Thrombopoietic drugs
• Cost analysis
• Benefit-risk comparison
• Chemotherapy – induced thrombocytopenia
• A novel treatment for hemophilia
TRIAL OF EDOXABAN VS LMWH IN CANCER VTE
• LMWH is considered to be treatment of choice
• Guidelines recommend six months LMWH therapy
• A NOAC (edoxaban) was compared with LMWH (dalteparin) in cancer VTE for 12 months of therapy
• 1050 patients in total randomized; 525 patients per group
• Non-inferiority trial; primary outcome – composite of first recurrent VTE or major bleeding event over 12 months
• 53% of patients had metastatic disease
Raskob GE, et al. ASH LBA-6, 2017 (NEJM 2017)
Huntsman Cancer Institute Eighth Annual Hematology Review 32

TRIAL OF EDOXABAN VS LMWH IN CANCER VTE
Raskob GE, et al. ASH LBA-6, 2017 (NEJM 2017)
Recurrent VTE
Major Bleeding
TRIAL OF EDOXABAN IN CANCER PATIENTS WITH VTE
• Rate of recurrent VTE lower with edoxaban (p = 0.09)
• Rate of major bleeding higher with edoxaban (p = 0.04)
• Frequency of severe major bleeding was similar with both drugs
• Major bleeding in edoxaban group was primarily GI, in patients with GI cancer
• Mortality from any cause was similar with both drugs
Raskob GE, et al. ASH LBA-6, 2017
Huntsman Cancer Institute Eighth Annual Hematology Review 33

RIVAROXABAN VS LMWH IN CANCER VTE
• A prospective British trial compared rivaroxaban vs dalteparin in cancer VTE between 2013-2016
• 203 patients in each treatment arm; 59% had metastatic disease
• 53% had incidental PE; 47% had symptomatic PE or DVT
• After six months treatment, VTE recurrence rates were: 11% dalteparin; 4% rivaroxaban
• Major bleeding rates were similar: 3% dalteparin; 4% rivaroxaban
• A larger phase III trial is pending
Young A, et al. ASH abstract #625, 2017
REAL-WORLD EFFICACY AND SAFETY OF RIVAROXABAN IN CANCER PATIENTS WITH
VTE
• US Truven Market Scan claims data and NCI-SEER data: cancer patients who developed VTE and were prescribed rivaroxaban were identified
• 949 patients were started on rivaroxaban following their index VTE
• The 180-day cumulative incidence estimate was 4% for recurrent VTE, 2.7% for major bleeding, and 11% for mortality
• These results are similar to prior studies using LMWH therapy
Kohn CG, et al. ASH abstract #3717
REAL-WORLD EFFICACY AND SAFETY OF RIVAROXABAN IN CANCER PATIENTS WITH VTE
Kohn CG, et al. ASH abstract #3717
Huntsman Cancer Institute Eighth Annual Hematology Review 34

INCIDENTAL VTE IN CANCER PATIENTS
• Approximately, 50% of VTE events in cancer patients are found incidentally
• In general, the prognosis of incidental VTE in cancer patients is similar to that of symptomatic VTE with comparable high rates of recurrent VTE
• Clot location may determine whether anticoagulation is necessary
Di Nisio M, Carrier M. 2017 ASH Education Book, p. 121
INCIDENTAL VTE IN CANCER PATIENTS
Di Nisio M, Carrier M. 2017 ASH Education Book, p. 121
THROMBOCYTOPENIA IN PREGNANCY
Cines DB, Levine LD. 2017 ASH Education Book, p. 144
Huntsman Cancer Institute Eighth Annual Hematology Review 35

THROMBOCYTOPENIA IN PREGNANCY
Practical Points
• Gestational thrombocytopenia is not apparent before mid-second trimester
• First trimester thrombocytopenia is likely to be ITP
• Platelet counts in GT rarely are less than 50,000/mcL
• GT does not respond to steroids or IvIgG
• ITP is the most common cause of platelet count below 50,000/mcL in first or second trimesters
• Preeclampsia is the most common cause of a platelet count below 50, 000/mcLin third trimester
Cines DB, Levine LD. 2017 ASH Education Book, p. 144
TREATMENT OF ITP IN PREGNANCY
• Guidelines suggest a minimum platelet count of 80,000/mcL for neuraxialanesthesia
• Steroids are preferred later in pregnancy; daily prednisone is preferred overpulse dexamethasone because of placental transfer concerns
• If treatment is necessary early in pregnancy, IvIgG is recommended
• Romiplostim has been used in anecdotal cases
• Pregnancy-associated TTP or aHUS should be treated with plasma exchange or eculizumab, respectively
Cines DB, Levine LD. 2017 ASH Education Book, p. 144
CATARACT INCIDENCE IN ITP PATIENTS TREATED WITH ELTROMBOPAG
• Clinical trials with eltrombopag reported cataract development or worsening in 7% of both treated and placebo patients
• An eltrombopag extension trial looked at the long-term risks of cataracts
• The rate of cataract development was low (9%) and no higher than that expected in a general adult population with other risk factors (steroid use, diabetes, and smoking)
WONG RSM, ET AL. ASH ABSTRACT # 1053, 2017
Huntsman Cancer Institute Eighth Annual Hematology Review 36

A COST-CONSEQUENCE MODEL: ELTROMBOPAG VS ROMIPLOSTIM
IN PEDIATRIC ITP PATIENTS
• Data was extracted from phase III clinical trials – platelet count response, bleeding events, and adverse events. Costs include
drugs and administration, routine care, rescue medications, bleeding-related
adverse events, mortality.
Tremblay G, et al . ASH abstract # 2146, 2017; Tremblay G, et al. ASH abstract # 3410, 2017
BENEFIT-RISK COMPARISON IN ITP PATIENTS RECEIVING ELTROMBOPAG OR
ROMIPLOSTIM
• Electronic data from 26 hospitals was analyzed to compare adult ITP patients treated with two drugs
• The proportion of patients who experienced bleeding events, rescue medication use, platelet transfusions, and adverse events were calculated overthe first 12 months of treatment
• Incidence proportions of patients with all bleeding events, rescue medication use, and most adverse events were lower in patients receiving eltrombopag
• Eltrombopag appears to have advantages over romiplostim in ITP
Forsythe A, et al. ASH abstract # 3409, 2017
BENEFIT-RISK COMPARISON IN ITP PATIENTS RECEIVING
ELTROMBOPAG OR ROMIPLOSTIM
Forsythe A, et al. ASH abstract # 3409, 2017
*
*
*
*
*
Huntsman Cancer Institute Eighth Annual Hematology Review 37

ROMIPLOSTIM FOR CHEMOTHERAPY-INDUCED THROMBOCYTOPENIA
• Chemotherapy-induced thrombocytopenia (CIT) may delay or cause dose-reduction of treatment
• First prospective trial of romiplostim in CIT
• Phase II open-label trial of solid tumor patients with at least four weeks ofthrombocytopenia (<100,000/mcL) despite dose-reduction or delay in chemotherapy
• Two groups: romiplostim vs observation
• 40 patients, approximately 90% had metastatic disease; 55% had GI cancer
• Observation arm was discontinued after interim analysis
Soff GA, et al. ASH abstract #289, 2017
ROMIPLOSTIM FOR CHEMOTHERAPY-INDUCED
THROMBOCYTOPENIA
Results
• Of 32 romiplostim up-front patients, 84% corrected thrombocytopenia within three weeks
• Mean effective romiplostim dose was 2.5 mcg/kg
• Four of 32 romiplostim patients experienced thrombosis (all VTEs); all had metastatic or locally-advanced pancreas, colorectal, or liver cancer
Soff GA, et al. ASH abstract #289, 2017
THROMBOPOIETIC DRUGS
Nursing Aspects
• Eltrombopag (Promacta®)
Oral; 25-75 mg daily
Adverse events- Liver toxicity, thrombosis, rebound thrombocytopenia
Monitoring- Platelet counts and LFTs
• Romiplostim (Nplate®)
S.C. ;1-10 mcg/kg weekly
Adverse events- 10% patients have variable PK, thrombosis, rebound
thrombocytopenia
Monitoring- Platelet counts
When these drugs are discontinued, consider “bridging therapy” with steroids or IVIgG to avoid rebound thrombocytopenia and bleeding
Huntsman Cancer Institute Eighth Annual Hematology Review 38

A NOVEL TREATMENT FOR HEMOPHILIA A
Standard Hemophilia A Therapy
• Patients without inhibitors – factor VIII replacement
• Patients with inhibitors – immune tolerance therapy
“bypass therapy” – factor VIIₐ
Huntsman Cancer Institute Eighth Annual Hematology Review 39

A NOVEL TREATMENT FOR HEMOPHILIA A
• Emicizumab is now approved to treat hemophilia patients with inhibitors
• Larger trials are ongoing in non-inhibitor patients
• Additional “non-factor” therapies for hemophilia are under investigation
SUMMARY
• For cancer-associated VTE patients, edoxaban and rivaroxaban are goodtreatment options (vs LMWH)
• Most cancer patients with incidental VTE should be anticoagulated
• Thrombopoietic drugs
• Eltrombopag has advantages over romiplostim
• Early clinical trial data with romiplostim to treat chemotherapy-induced thrombocytopenia is encouraging
• Emicizumab is a breakthrough therapy for hemophilia A patients
Huntsman Cancer Institute Eighth Annual Hematology Review 40

Huntsman Cancer Institute Eighth Annual
Hematology Review
Multiple Myeloma: A Year in Review
Douglas Sborov, MD
Huntsman Cancer Institute Eighth Annual Hematology Review 41

8th ANNUAL HCI HEMATOLOGY UPDATE
Multiple myeloma: A year in review
Douglas W. Sborov, MD MSAssistant Professor
Division of Hematology & Hematologic MalignanciesUniversity of Utah – Huntsman Cancer Institute
24-Feb-2018
8th ANNUAL HCI HEMATOLOGY UPDATE
• No financial disclosures
Disclosures
8th ANNUAL HCI HEMATOLOGY UPDATE
• Newly diagnosed MM (NDMM)– Transplant ineligible not fit for RVd
– Transplant eligible
• Relapsed refractory MM (RRMM)– Carfilzomib- and Daratumumab-based regimens
– New promising therapeutics• CAR-T, BiTE, and SINE
Outline
Huntsman Cancer Institute Eighth Annual Hematology Review 42
8th ANNUAL HCI HEMATOLOGY UPDATE
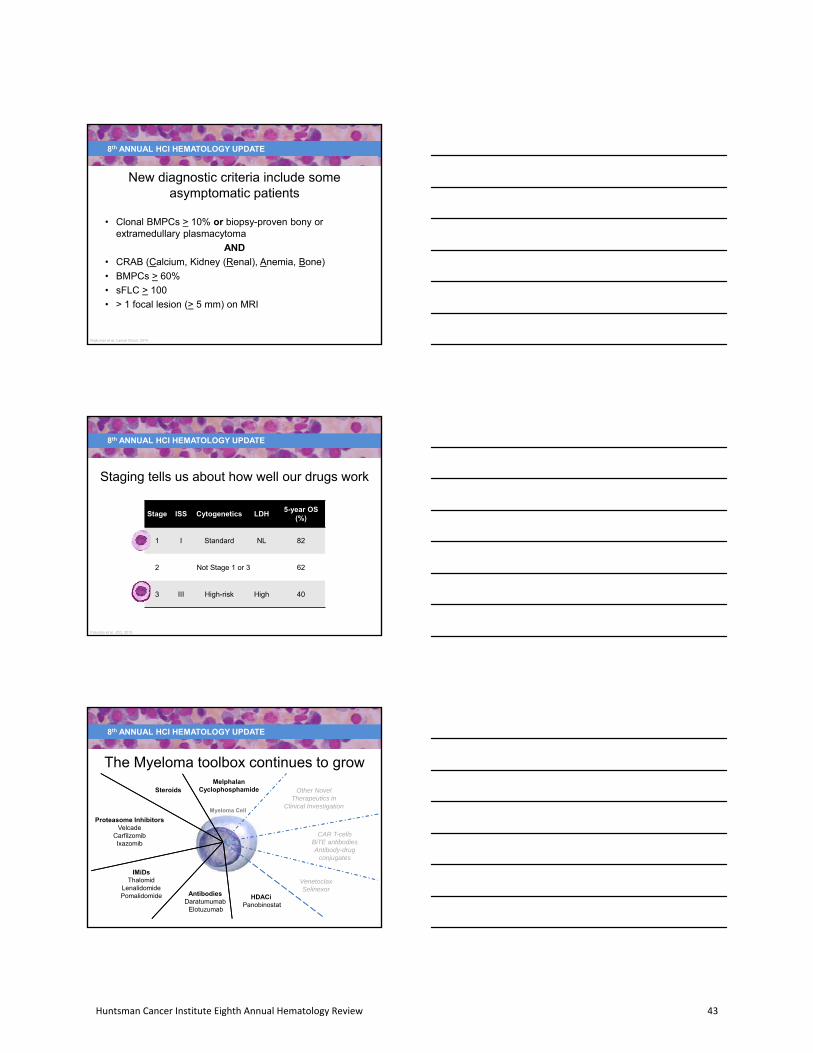
• Clonal BMPCs > 10% or biopsy-proven bony orextramedullary plasmacytoma
AND
• CRAB (Calcium, Kidney (Renal), Anemia, Bone)
• BMPCs > 60%
• sFLC > 100
• > 1 focal lesion (> 5 mm) on MRI
New diagnostic criteria include some asymptomatic patients
Rajkumar et al, Lancet Oncol, 2014
8th ANNUAL HCI HEMATOLOGY UPDATE
Staging tells us about how well our drugs work
Stage ISS Cytogenetics LDH5-year OS
(%)
1 I Standard NL 82
2 Not Stage 1 or 3 62
3 III High-risk High 40
Palumbo et al, JCO, 2015
8th ANNUAL HCI HEMATOLOGY UPDATE
Steroids
Proteasome InhibitorsVelcade
CarfilzomibIxazomib
IMiDsThalomid
LenalidomidePomalidomide Antibodies
DaratumumabElotuzumab
VenetoclaxSelinexor
CAR T-cellsBiTE antibodiesAntibody-drug
conjugates
Other Novel Therapeutics in
Clinical InvestigationMyeloma Cell
The Myeloma toolbox continues to growMelphalan
Cyclophosphamide
HDACiPanobinostat
Huntsman Cancer Institute Eighth Annual Hematology Review 43

8th ANNUAL HCI HEMATOLOGY UPDATE
NDMM – A simple treatment algorithm
VRd or clinical trial
Transplant ineligible unable to tolerate SOC
VRd lite
Transplant eligible
AutoHSCT
Maintenance
Rd
8th ANNUAL HCI HEMATOLOGY UPDATE
FIRST line treatment of elderly or frail patients
Rd Continuous REVLIMID + low-dose dexarm (n = 535) until progression
Rd18 arm REVLIMID + low-dose dex(n = 541) up to 18 cycles
MPT arm Melphalan + prednisone + (n = 547) thalidomide up to 12 cycles
Ra
nd
om
izat
ion
Benboubker et al, NEJM, 2014
8th ANNUAL HCI HEMATOLOGY UPDATE
Continuous Rd is safe and effective
Benboubker et al, NEJM, 2014
Outcome Rd continuous Rd18 MPT
Safety (G3/4)> 1 AE
NeutropeniaInfection
DVT +/- PE
85%28%29%8%
80%26%22%6%
89%45%17%5%
ResponseORR
> VGPR75%44%
73%43%
62%28%
SurvivalPFS
3-year OS4-year OS
25.5 m70%59%
20.7 m66%56%
21.2 m62%51%
SPMs 3% 6% 5%
Compared to MPT, continuous Rd significantly improves PFS and reduces the risk of death without compromising safety and tolerability
Huntsman Cancer Institute Eighth Annual Hematology Review 44
8th ANNUAL HCI HEMATOLOGY UPDATE
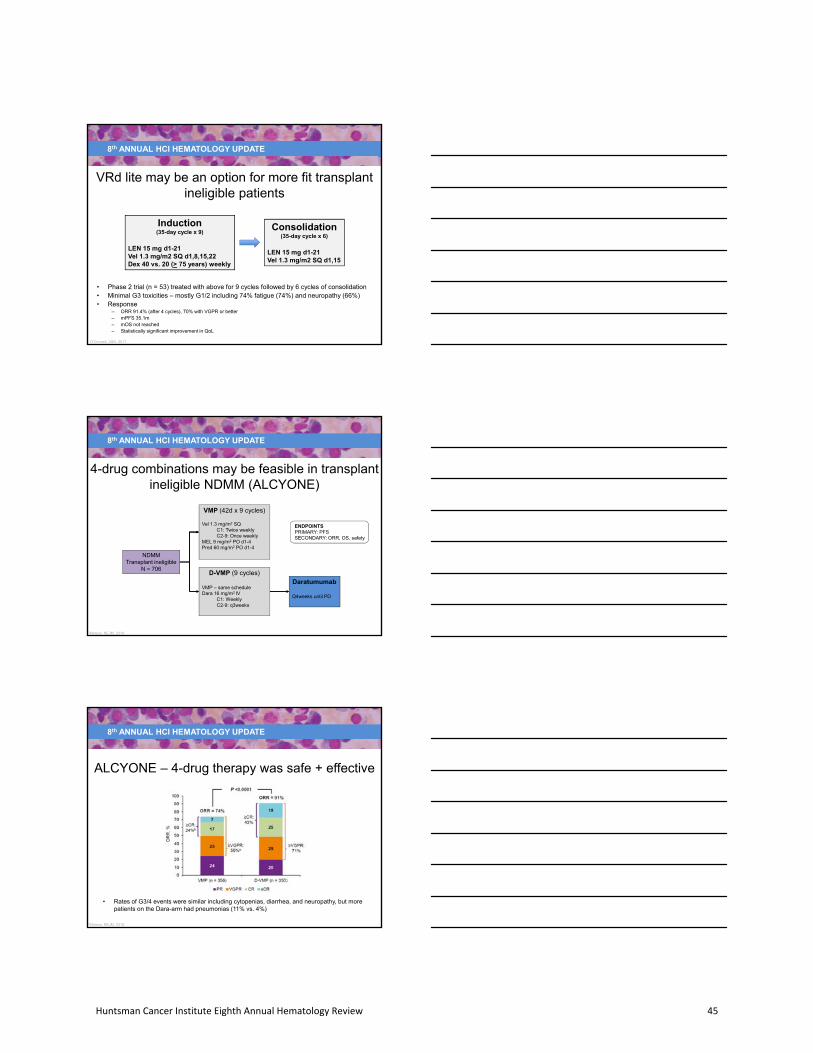
VRd lite may be an option for more fit transplant ineligible patients
Induction(35-day cycle x 9)
LEN 15 mg d1-21Vel 1.3 mg/m2 SQ d1,8,15,22Dex 40 vs. 20 (> 75 years) weekly
• Phase 2 trial (n = 53) treated with above for 9 cycles followed by 6 cycles of consolidation• Minimal G3 toxicities – mostly G1/2 including 74% fatigue (74%) and neuropathy (66%)• Response
– ORR 91.4% (after 4 cycles), 70% with VGPR or better– mPFS 35.1m– mOS not reached– Statistically significant improvement in QoL
Consolidation(35-day cycle x 6)
LEN 15 mg d1-21Vel 1.3 mg/m2 SQ d1,15
O’Donnell, ASH, 2017
8th ANNUAL HCI HEMATOLOGY UPDATE
4-drug combinations may be feasible in transplantineligible NDMM (ALCYONE)
3Mateos, NEJM, 2018
NDMMTransplant ineligible
N = 706
VMP (42d x 9 cycles)
Vel 1.3 mg/m2 SQC1: Twice weeklyC2-9: Once weekly
MEL 9 mg/m2 PO d1-4Pred 60 mg/m2 PO d1-4
D-VMP (9 cycles)
VMP – same scheduleDara 16 mg/m2 IV
C1: WeeklyC2-9: q3weeks
Daratumumab
Q4weeks until PD
ENDPOINTSPRIMARY: PFSSECONDARY: ORR, OS, safety
8th ANNUAL HCI HEMATOLOGY UPDATE
ALCYONE – 4-drug therapy was safe + effective
3Mateos, NEJM, 2018
• Rates of G3/4 events were similar including cytopenias, diarrhea, and neuropathy, but more patients on the Dara-arm had pneumonias (11% vs. 4%)
Huntsman Cancer Institute Eighth Annual Hematology Review 45

8th ANNUAL HCI HEMATOLOGY UPDATE
VRd is SOC for all fit patients: SWOG S0777
NDMM s intent for immediate autoHSCT
Rd (n=232)
LEN 25 mg D1-21Dex 40 mg weekly
[6 x 28-day cycles]
VRd (n=242)
LEN 25 mg D1-14Dex 20 mg Vel 1.3 mg/m2 D1,4,8,11
[8 x 21-day cycles]Rd
LEN 25 mg D1-21Dex 40 mg weekly
[24‐day cycles until PD, unacceptable toxicity, or withdrawl of consent]
MAINTENANCE
Stratified by ISS & intent to transplant
INDUCTION
ENDPOINTSPRIMARY: PFSSECONDARY: ORR, OS, safety
Durie et al, Lancent Oncology, 2016
8th ANNUAL HCI HEMATOLOGY UPDATE
VRd + Rev maintenance is tolerated and significantly improves outcomes in NDMM
Durie et al, Lancent Oncology, 2016
Outcome VRd (n = 241) Rd (n = 226) p-value
Safety (G3/4 AE)Neurologic
PainInfection
GISPM
802934522
249
31174
ResponseORR
VGPR or better81.5%43.5%
71.5%31.8%
SurvivalPFSOS
43 m75 m
30 m64 m
p = 0.0018p = 0.0125
8th ANNUAL HCI HEMATOLOGY UPDATE
• KRd– P2 trials show exceptional activity1,2
– Ongoing randomized ENDURANCE trial – KRd vs VRd
• 4 drug combinations– VRd +/- Daratumumab (GRIFFIN)3
– KRd +/- Daratumumab4
– VRd +/- Elotuzumab5
We can likely do better than VRd induction… KRd or 4-drug induction
1Korde et al, JAMA Onc, 2015; 2Jakubowiak et al, Blood, 2012; 3Voorhes, ASH, 2017; 4XXXX, ASH, 2017; 5Usman et al, BCJ, 2015;
Huntsman Cancer Institute Eighth Annual Hematology Review 46
8th ANNUAL HCI HEMATOLOGY UPDATE
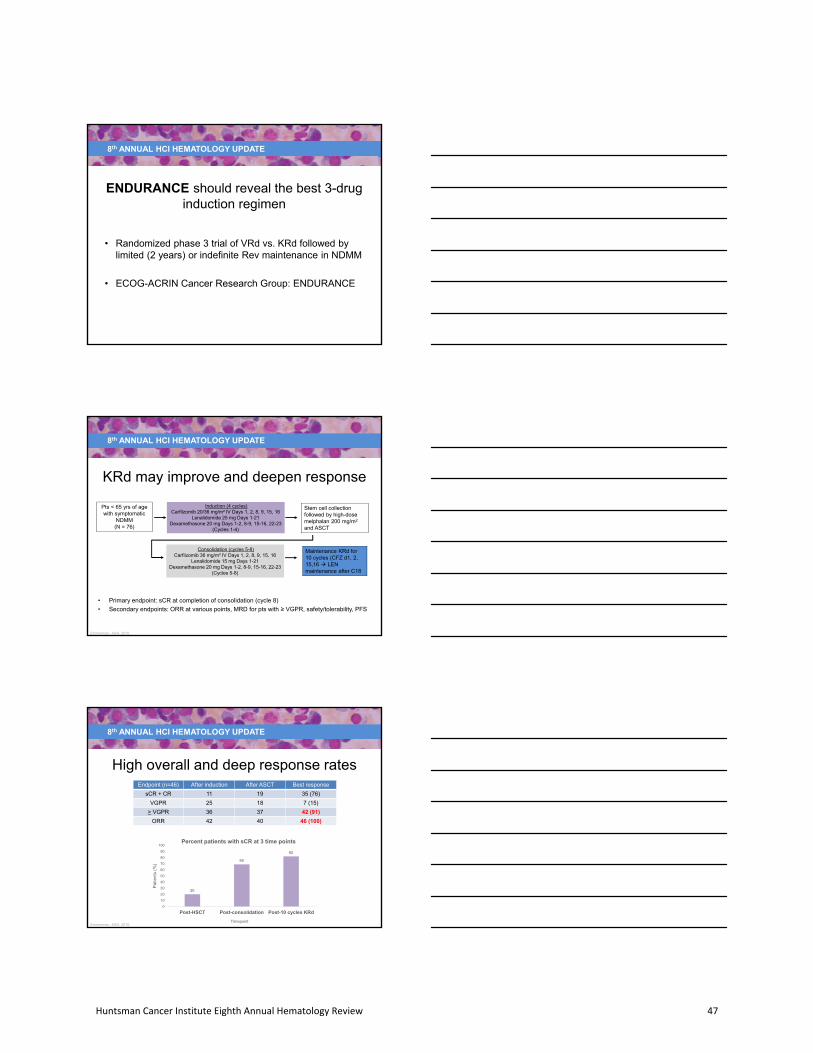
• Randomized phase 3 trial of VRd vs. KRd followed by limited (2 years) or indefinite Rev maintenance in NDMM
• ECOG-ACRIN Cancer Research Group: ENDURANCE
ENDURANCE should reveal the best 3-drug induction regimen
8th ANNUAL HCI HEMATOLOGY UPDATE
KRd may improve and deepen response
Pts < 65 yrs of agewith symptomatic
NDMM(N = 76)
Induction (4 cycles)Carfilzomib 20/36 mg/m² IV Days 1, 2, 8, 9, 15, 16
Lenalidomide 25 mg Days 1-21Dexamethasone 20 mg Days 1-2, 8-9, 15-16, 22-23
(Cycles 1-4)
Stem cell collection followed by high-dose melphalan 200 mg/m2
and ASCT
Consolidation (cycles 5-8)Carfilzomib 36 mg/m² IV Days 1, 2, 8, 9, 15, 16
Lenalidomide 15 mg Days 1-21Dexamethasone 20 mg Days 1-2, 8-9, 15-16, 22-23
(Cycles 5-8)
Maintenance KRd for 10 cycles (CFZ d1, 2, 15,16 LEN maintenance after C18
• Primary endpoint: sCR at completion of consolidation (cycle 8)
• Secondary endpoints: ORR at various points, MRD for pts with ≥ VGPR, safety/tolerability, PFS
Zimmerman, ASH, 2016
8th ANNUAL HCI HEMATOLOGY UPDATE
High overall and deep response rates
Zimmerman, ASH, 2016
Endpoint (n=46) After induction After ASCT Best response
sCR + CR 11 19 35 (76)
VGPR 25 18 7 (15)
> VGPR 36 37 42 (91)
ORR 42 40 46 (100)
20
69
82
0
10
20
30
40
50
60
70
80
90
100
Post-HSCT Post-consolidation Post-10 cycles KRd
Pat
ient
s (%
)
Timepoint
Percent patients with sCR at 3 time points
Huntsman Cancer Institute Eighth Annual Hematology Review 47

8th ANNUAL HCI HEMATOLOGY UPDATE
RVd +/- Daratumumab (P2 - GRIFFIN)
Voorhes, ASH, 2017
• Safety run-in: DLTs (n=3) included fatigue, gastroenteritis, and pneumonitis and hypotension• No new safety signals with 4-drug treatment
NDMMTransplant eligible
N ~ 200
RVd (4 – 21d cycles)
Vel 1.3 mg/m2 SQ d1,4,8,11LEN 25 mg d1-4Dex 40 mg weekly
D-RVd (4 cycles)
RVd – same scheduleDara 16 mg/m2 IV weekly
AutoHSCT
AutoHSCT
RVd x 2
Same schedule
D-RVd x 2
RVd – same scheduleDara 16 mg/m2 d1
Revlimid d1-2110 mg 15 mg
Revlimid + Dara q56 day
INDUCTION CONSOLIDATION MAINTENANCE
8th ANNUAL HCI HEMATOLOGY UPDATE
• Phase 1b study (n = 22) NDMM
• ORR 100% including > VGPR 90%; all patients alive at 1-year
• No new safety signals
KRd +/- Daratumumab
Chari, ASH, 2017
KRd + Daratumumab(13 – 28d cycles)
CFZ weekly20 mg/m2 C1D170 mg/m2 thereafter
LEN 25 mg d1-21Dex 40 mg weeklyDaratumumab 16 mg/m2 IV weekly
10091
57
43
0
10
20
30
40
50
60
70
80
90
100
> PR > VGPR > CR sCR
Best response (n=21)
8th ANNUAL HCI HEMATOLOGY UPDATE
Transplant remains standard of care
RVRd x 3 cycles VRd x 3 cycles
AutoHSCT
VRd x 2 cycles
LEN 12 months
VRd x 5 cycles
LEN 12 months
Attal et al, NEJM, 2017
IFM / DFCI 2009
Huntsman Cancer Institute Eighth Annual Hematology Review 48

8th ANNUAL HCI HEMATOLOGY UPDATE
IFM / DFCI 2009 trial
Attal et al, NEJM, 2017
Outcome VRd (n = 350) AutoHSCT (n = 350) p-value
CR rate by treatment phase (%)
After inductionAfter AutoHSCT or consolidation
End of maintenance
456976
477885
0.870.03
< 0.001
Response (%)VGPR or betterMRD negative
7765
8879
0.001< 0.001
mTTP / mPFS 36 m 50 m < 0.001
4 year OS (NR) 82% 81% 0.87
Autologous transplant was associated with significantly increased TTP and PFS but no benefit in OS
8th ANNUAL HCI HEMATOLOGY UPDATE
Single autoHSCT is SOC: P3 STaMINA trial
Eligible pts ≤ 70(N = 758)
Single ASCT (n=257)LEN Maintenance until PD
10 mg qday x 3 cycles 15 mg/day
Consolidation (n=254)VEL 1.3 mg/m² D1,4,8,11
LEN 15 mg D1-15Dex 40 mg D1,8,154 – 28-day cycles
LEN Maintenance until PD10 mg qday x 3 cycles
then 15 mg/day
Tandem ASCT (n=247)Melphalan 200 mg/m²
AutoHSCTMEL 200 mg/m2
• Primary endpoint: PFS at 38 mos
• Secondary endpoints: OS, ORR, CR conversion rate, safety, infections, tx-related mortality, QoL
Stadtmauer, ASH abstract, 2016
8th ANNUAL HCI HEMATOLOGY UPDATE
No significant difference in PFS or OS between the 3 arms
Stadtmauer, ASH abstract, 2016
PFS100
80
60
40
20
0
PF
S (
%)
0 12 24 38
Months From Randomization
OS100
80
60
40
20
0
OS
(%
)
0 12 24 38Months From Randomization
Huntsman Cancer Institute Eighth Annual Hematology Review 49

8th ANNUAL HCI HEMATOLOGY UPDATE
Revlimid maintenance leads to improved survival
Holstein et al, Lancet, 2017
• Revlimid– CALGB 100104
• Randomized phase 3 trial in 460 patients
• mTTP 57.3m vs. 28.9m (p < 0.0001)
• mOS 113.8m vs. 84.1m (p = 0.0004)
• 5 year OS was 76% vs. 64%
– Meta-analysis (CALGB 100104, IFM 2005-2,GIMEMA RV-209) demonstrated OS with LEN in all
• 26% reduction in risk of death
• Estimated 2.5 year OS benefit
8th ANNUAL HCI HEMATOLOGY UPDATE
Relapsed and refractory myeloma (RRMM)Progressive
disease
Off treatment*On maintenance*
Frail or indolentFit
IF REVLIMID MAINTENANCE
KPd, DVd DVd
IF VELCADE MAINTENANCE
DRd DRd or IRd
Frail or indolentFit
KRd or DRd DRd, DVd, ERd, IRd
* Always consider clinical trial; salvage autoHSCT for patients not previously transplanted; 2nd autoHSCT if > 18 months off treatment or > 36 months response on post-transplant maintenance
8th ANNUAL HCI HEMATOLOGY UPDATE
Daratumumab-, Carfilzomib-, and Pomalidomide-based regimens
Huntsman Cancer Institute Eighth Annual Hematology Review 50

8th ANNUAL HCI HEMATOLOGY UPDATE
Daratumumab + Revlimid or Velcade + Dex
Dimopoulos, NEJM, 2016; Palumbo, NEJM, 2016
POLLUXDRd vs. Rd [P3 (n=569)]
> 1 prior lines of therapy
CASTOR DVd vs. Vd[P3 (n=498)]
> 1 prior lines of therapy
RA
ND
OM
IZA
TIO
NR
AN
DO
MIZ
AT
ION
RdLEN days 1-21 + weekly Dex
DRdDara qweek x 8 q2w for 16 w monthly
LEN days 1-21 + weekly Dex
DVdDara qweek x 10 q3w for 24 w monthly
VEL days 1, 4, 8, 11 + Dex
VdVEL days 1, 4, 8, 11 + Dex
8th ANNUAL HCI HEMATOLOGY UPDATE
Daratumumab: POLLUX and CASTOR trials
Dimopoulos, NEJM, 2016; Palumbo, NEJM, 2016; Spencer, ASH, 2017; Dimopoulos, ASH, 2017
POLLUX CASTOR
Response DRd Rd p‐value DVd Vd p‐value
ORR 93% 76% p < 0.001 84% 63% p < 0.001
> VGPR 81% 49% p < 0.001 62% 29% p < 0.001
12 m PFS 83% 60% p < 0.0001 62% 29% p < 0.0001
MRD negativity (10‐4) 29% 8% p < 0.0001 13.5% 2.8% p < 0.0001
8th ANNUAL HCI HEMATOLOGY UPDATE
Daratumumab: POLLUX and CASTOR trials
Dimopoulos, NEJM, 2016; Palumbo, NEJM, 2016
POLLUX CASTOR
Most common G3/4 AE DRd Rd DVd Vd
Neutropenia 51.9% 27% 12.8% 4.2%
Anemia 12.4% 19.6% 14.4% 16.0%
Thrombocytopenia 12.7% 13.5% 45.3% 32.9%
Febrile neutropenia 5.7% 2.5%
Diarrhea 5.3% 3.2% 3.7% 1.3%
Fatigue 6.4% 2.5% 4.5% 3.4%
Infusion reactions*Any gradeGrade 3
47.7%5.3%
45.3%8.6%
Huntsman Cancer Institute Eighth Annual Hematology Review 51

8th ANNUAL HCI HEMATOLOGY UPDATE
Daratumumab + Pomalidomide + Dex (DPd)
DPd(28d cycles)
Daratumumab 16 mg/m2 IV Weekly C1-2Biweekly C3-6Monthly until PD
POM 4 mg d1-21Dex 40 mg weekly
• P1b (EQQLEUS) – DPd in patients (n = 103) treated with > 2 prior lines• AE profile similar to Pd with more neutropenia and infusion reactions• Time to response 1 – 3 months• mPFS 8.8m, mOS 17.5m
Chari, Blood, 2017
8th ANNUAL HCI HEMATOLOGY UPDATE
Daratumumab + Carfilzomib + Dex (DKd)
DKd(28d cycles)
Daratumumab 16 mg/m2 IV Weekly C1-2Biweekly C3-6Monthly until PD
CFZ 20/70 mg/m2 weeklyDex 40 mg weekly
Lonial, ASH, 2017
• P1b – DKd in patients (n=85),treated with 1-3 prior lines
• MC AE cytopenias, HTN
• No changes in mLVEF
• ORR 84%, 56% > VGPR
8th ANNUAL HCI HEMATOLOGY UPDATE
Carfilzomib + Revlimid + Dex (KRd) - ASPIRE
Endpoint KRd Rd
sCR + CR 31.8% 9.3%
mPFS 26.1m 16.6m
OS 48.3m 40.4m
ORR 42 40
KRd is associated with improved QoL
RRMM1-3 prior lines
N = 792
Rd
LEN 25 mg D1-21Dex 40 mg weekly
KRd
CFZ 20/27 d1,2,8,9,15,16LEN 25 mg d1-21Dex 40 mg weekly
After C12 – CFZ d1,2,15,16After C16 – CFZ stopped
Stewart, ASH, 2017
Huntsman Cancer Institute Eighth Annual Hematology Review 52
8th ANNUAL HCI HEMATOLOGY UPDATE
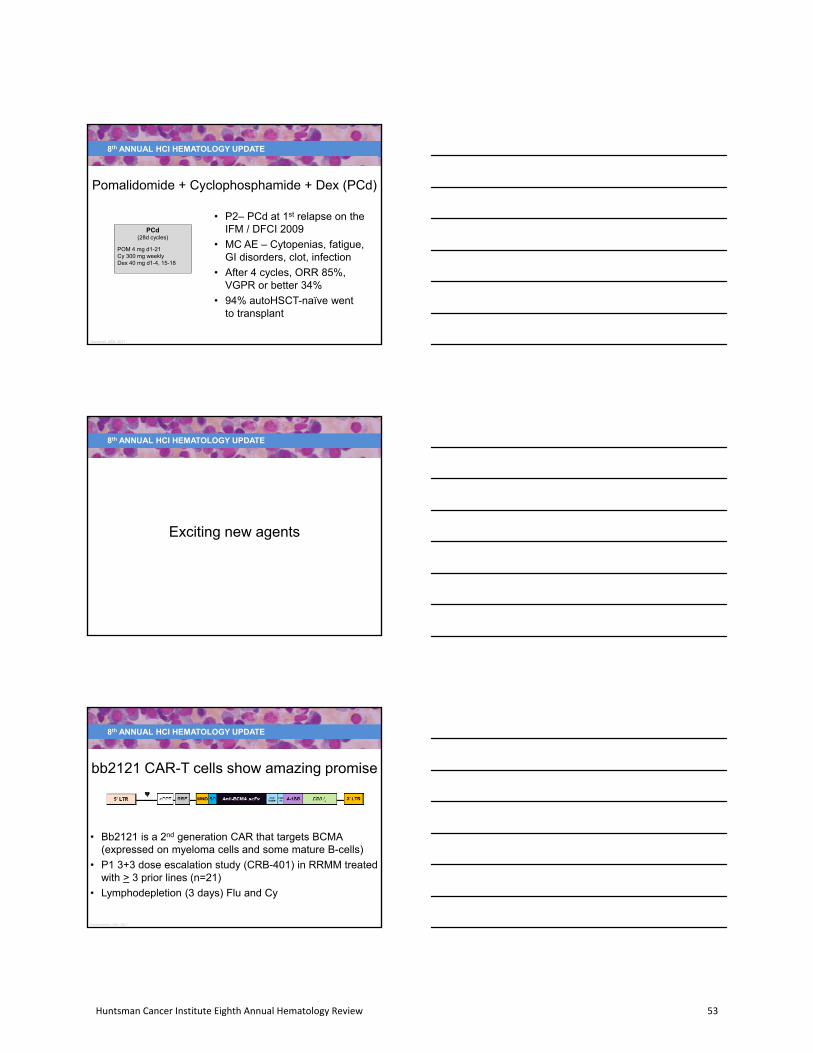
Pomalidomide + Cyclophosphamide + Dex (PCd)
PCd(28d cycles)
POM 4 mg d1-21Cy 300 mg weeklyDex 40 mg d1-4, 15-18
• P2– PCd at 1st relapse on theIFM / DFCI 2009
• MC AE – Cytopenias, fatigue,GI disorders, clot, infection
• After 4 cycles, ORR 85%,VGPR or better 34%
• 94% autoHSCT-naïve wentto transplant
Gardenet, ASH, 2017
8th ANNUAL HCI HEMATOLOGY UPDATE
Exciting new agents
8th ANNUAL HCI HEMATOLOGY UPDATE
bb2121 CAR-T cells show amazing promise
• Bb2121 is a 2nd generation CAR that targets BCMA (expressed on myeloma cells and some mature B-cells)
• P1 3+3 dose escalation study (CRB-401) in RRMM treatedwith > 3 prior lines (n=21)
• Lymphodepletion (3 days) Flu and Cy
Kochenderfer, ASH, 2017
Huntsman Cancer Institute Eighth Annual Hematology Review 53

8th ANNUAL HCI HEMATOLOGY UPDATE
bb2121 CAR-T cells
AEOveralln (%)
> G3n (%)
CRS 15 (71) 2 (10)
Neurotoxicity 5 (24) 0
Neutropenia 18 (86) 18 (86)
Thrombocytopenia 11 (52) 9 (43)
Anemia 14 (67) 12 (57)
27
6
47
33
27
56
0
20
40
60
80
100
04 MAY 2017 (N=15) 02 OCT 2017 (N=18)
ORR
CR/sCR
VGPR
PR
• 5 deaths – PD (3), cardiac arrest (1), MDS p treatment stopped (1)• ORR 94%, > VGPR 89%• MRD negative in 90% of evaluable patients• P2 KarMMa is open
Kochenderfer, ASH, 2017
8th ANNUAL HCI HEMATOLOGY UPDATE
• Humanized anti-BCMA IgG monoclonal antibody conjugated to the cytotoxic agent monomethyl auristatin-F - kills MM cells via ADC, ADCC, immune directed cell death, BCMA receptor signaling inhibition
• DREAMM-1 (Driving Excellence in Approaches to Multiple Myeloma)
• RRMM with at least 3 prior lines of treatment
BCMA antibody drug conjugate – GSK2857916
Trudel, ASH, 2017
8th ANNUAL HCI HEMATOLOGY UPDATE
Antibody-drug conjugate GSK2857916
Trudel, ASH, 2017
n (%)N = 35
Any Grade > G3
Thrombocytopenia 20 (57) 12 (34)
Vision blurred 16 (46) 0
Dry eye 12 (34) 1 (3)
Anemia 10 (29) 5 (14)
Nausea 8 (23) 0
Photophobia 8 (23) 0
Fever 8 (23) 0
Fatigue 7 (20) 0
RESPONSE
• ORR 60%
• In part 2, 51% of patientshad VGPR or better
• mPFS 7.9m
Huntsman Cancer Institute Eighth Annual Hematology Review 54

8th ANNUAL HCI HEMATOLOGY UPDATE
• Questions?
• Please do not hesitate to contact me:– [email protected]
Thank you
8th ANNUAL HCI HEMATOLOGY UPDATE
• Diagnosis and staging of multiple myeloma
• Common side effects associated with SOC and experimental regimens
• Understanding the differences between induction, relapsed, andexperimental treatments
RN considerations
Huntsman Cancer Institute Eighth Annual Hematology Review 55
Huntsman Cancer Institute Eighth Annual
Hematology Review
New Therapeutic Options for AL Amyloidosis
Tibor Kovacsovics, MD
Huntsman Cancer Institute Eighth Annual Hematology Review 56

New therapeutic options for AL amyloidosis
Tibor Kovacsovics, MDUtah Amyloidosis Program
Division of Hematology and Hematologic MalignanciesHuntsman Cancer Institute andUniversity of Utah
Utah Amyloidosis Program
Disclosures
• Research support:
‐ Janssen
‐ Prothena
• Off label use: all medications described in thistalk; there are no FDA approved drugs for ALamyloidosis
Outline
• diagnostic algorithm
• novel prognostic scores
• therapy:
‐ chemotherapy approaches
‐ transplant
• Direct amyloidosis targeting:
‐ agents destabilizing amyloid fibrils: doxicyclin
‐ monoclonal antibodies: NED001
Huntsman Cancer Institute Eighth Annual Hematology Review 57

Amyloidosis: a protein misfoldingdisease
• Amyloidosis is a protein disease, which resultsfrom the accumulation into amyloid fibrils ofmisfolded precursor proteins
• There are about 30 different amyloidosisprecursors proteins
• The amyloidosis accumulate into amyloidfibrils, which have a beta pleated sheet
The cascade of molecular events leading to amyloidosis.
Giampaolo Merlini et al. JCO 2011;29:1924-1933
©2011 by American Society of Clinical Oncology
Most Common Amyloidosis Types
PRECURSOR PROTEIN AMYLOIDOSIS TYPE SITE OF SYNTHESIS
Monoclonal light chain AL, acquired Bone marrow plasma cells
Mutant transthyretin TTR, hereditary Liver
WT transthyretin SSA (senile), acquired Liver
SAP AA (reactive), acquired Liver
LECT ALECT2, hereditary Liver
Huntsman Cancer Institute Eighth Annual Hematology Review 58

Mechanism of amyloid organ toxicity
• Mass effect in most organs
• Direct toxicity of AL light chains on the heart:
‐ discrepancy between the amount of amyloiddeposits in the heart and the level of heartfailure
‐direct toxicity of light chains in differentmodels
‐mediation by reactive oxygen species or bythe MAP kinase pathway
Clinical Presentation
CARDIAC RENAL NEURO GI MSK
Heart failureNephrotic syndrome
Polyneuropathy Hepatomegaly Shoulder pad
Conduction abnormalities
Peripheral edema
Autonomic dysfunction
Gastroparesis Macroglossia
Diarrhea Arthropathy
Malabsorption
Organ involvement varies with amyloidosis type
AMYLOID TYPE HEART KIDNEY LIVER PNS
AL amyloidosis ++ ++ + +
TTR amyloidosis ++ + ‐ ++
SSA (WT‐TTR) ++ ‐ ‐ ‐
AA (reactive) + ++ + ‐
Huntsman Cancer Institute Eighth Annual Hematology Review 59
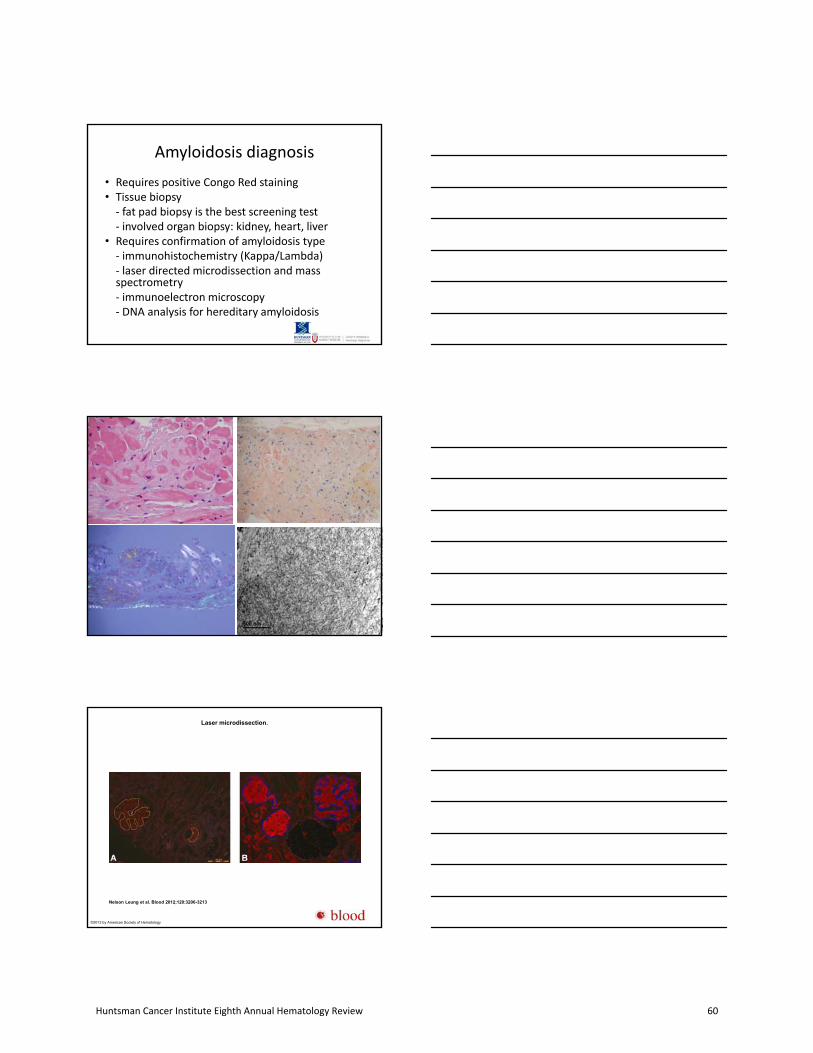
Amyloidosis diagnosis
• Requires positive Congo Red staining• Tissue biopsy‐ fat pad biopsy is the best screening test‐ involved organ biopsy: kidney, heart, liver
• Requires confirmation of amyloidosis type‐ immunohistochemistry (Kappa/Lambda)‐ laser directed microdissection and massspectrometry‐ immunoelectron microscopy‐ DNA analysis for hereditary amyloidosis
Laser microdissection.
Nelson Leung et al. Blood 2012;120:3206-3213
©2012 by American Society of Hematology
Huntsman Cancer Institute Eighth Annual Hematology Review 60
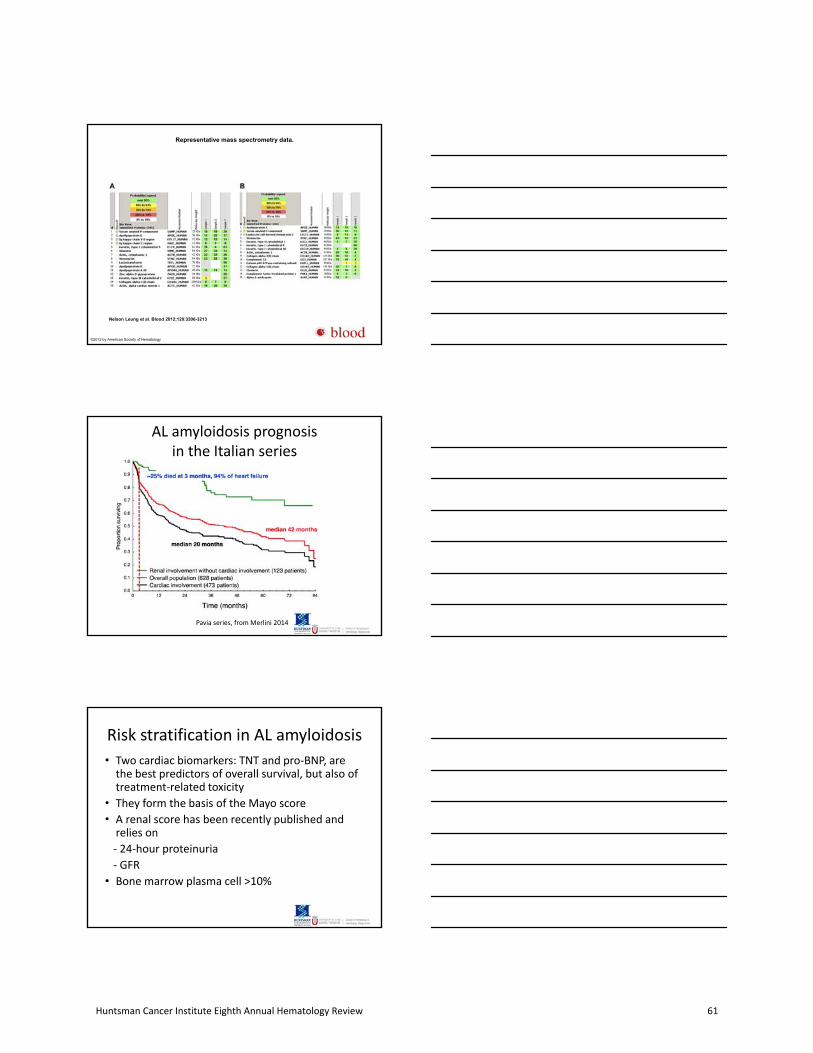
Representative mass spectrometry data.
Nelson Leung et al. Blood 2012;120:3206-3213
©2012 by American Society of Hematology
AL amyloidosis prognosis in the Italian series
Pavia series, from Merlini 2014
Risk stratification in AL amyloidosis
• Two cardiac biomarkers: TNT and pro‐BNP, arethe best predictors of overall survival, but also oftreatment‐related toxicity
• They form the basis of the Mayo score
• A renal score has been recently published andrelies on
‐ 24‐hour proteinuria
‐ GFR
• Bone marrow plasma cell >10%
Huntsman Cancer Institute Eighth Annual Hematology Review 61

Risk stratification in AL amyloidosisMayo score
Dispenzieri, J Clin Oncol 22:3751, 2004
Risk stratification in renalAL amyloidosis
Palladini et al, Blood 124:2235, 2014
Therapeutic strategy in AL amyloidosis
• Reduction of free light chain burden byeradicating the plasma cells with anti‐myelomastrategies‐ standard dose chemotherapy‐ stem cell transplantation
• Overall survival correlates with quality ofhematologic response
• Organ function improves slowly• Limitations: toxicity, especially with transplantand in patient with poor heart function
Huntsman Cancer Institute Eighth Annual Hematology Review 62
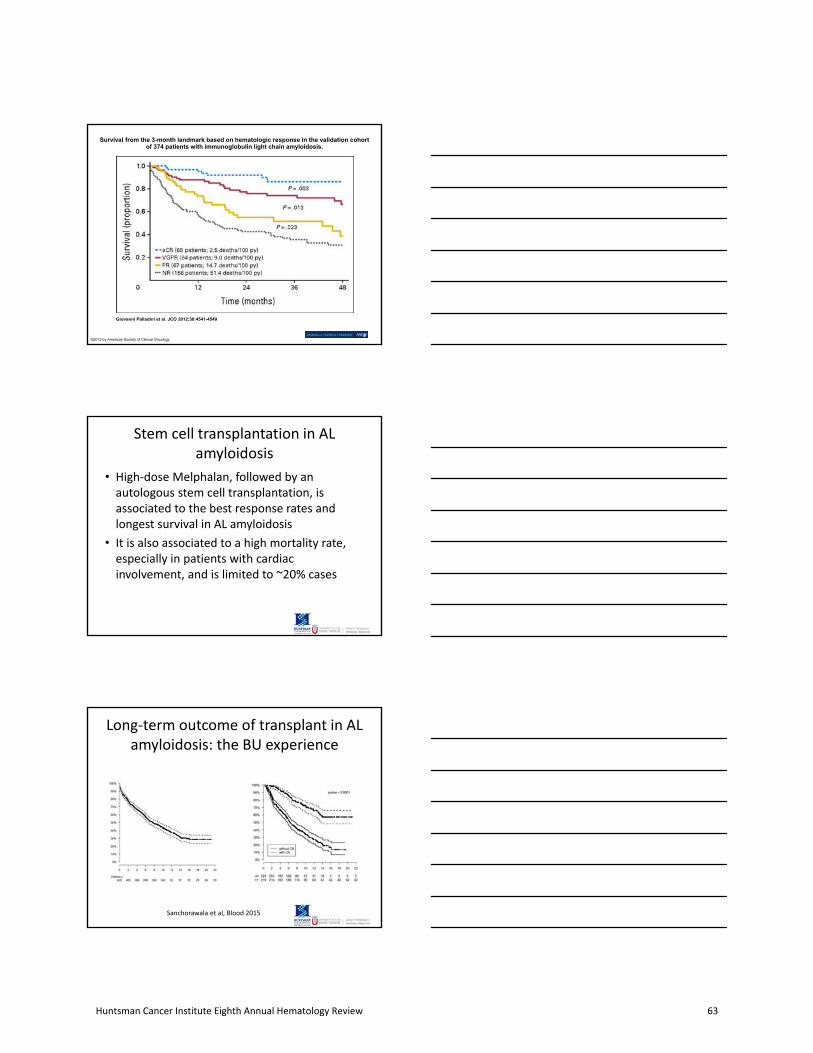
Survival from the 3-month landmark based on hematologic response in the validation cohort of 374 patients with immunoglobulin light chain amyloidosis.
Giovanni Palladini et al. JCO 2012;30:4541-4549
©2012 by American Society of Clinical Oncology
Stem cell transplantation in AL amyloidosis
• High‐dose Melphalan, followed by anautologous stem cell transplantation, isassociated to the best response rates andlongest survival in AL amyloidosis
• It is also associated to a high mortality rate,especially in patients with cardiacinvolvement, and is limited to ~20% cases
Long‐term outcome of transplant in AL amyloidosis: the BU experience
Sanchorawala et al, Blood 2015
Huntsman Cancer Institute Eighth Annual Hematology Review 63

Impact of Mayo score on transplant‐related mortality
Gertz et al, Bone Marrow Transplantation 2013
Probabilities of (A) early mortality and (B) overall survival (OS) in light-chain amyloidosis after transplantation for all three time cohorts.
Anita D'Souza et al. JCO doi:10.1200/JCO.2015.62.4015
©2015 by American Society of Clinical Oncology
Trends in (A) overall survival (OS) for cardiac light-chain amyloidosis (AL); (B) OS for renal, noncardiac AL; (C) early mortality (EM) based on center experience; and (D) time trends in
improvement in EM among centers.
Anita D'Souza et al. JCO doi:10.1200/JCO.2015.62.4015
©2015 by American Society of Clinical Oncology
Huntsman Cancer Institute Eighth Annual Hematology Review 64

Chemotherapy
• Chemotherapy approaches have evolved overtime
• Melphalan‐Dexamethasone has been astandard for a long time
• Bortezomib‐based regimens are associated todeep and rapid responses, and represent anew standard
• CyBorD (Cyclophosphamide‐Bortezomib‐Dexamethasone) is the regimen of choice
Survival of 230 patients with AL amyloidosis treated with CyBorD.
Giovanni Palladini et al. Blood 2015;126:612-615
©2015 by American Society of Hematology
Transplant vs chemotherapy
• Transplant:
‐ pro: Deeper responses, long follow up
‐ con: high mortality rate
• Modern chemotherapy regimens:
‐ deep responses, low mortality
‐ durability of responses unknown
Huntsman Cancer Institute Eighth Annual Hematology Review 65

Mayo clinic algorith for AL amyloidosis management
Chemotherapy options for relapsed amyloidosis
• Ongoing clinical trials (relapse):
‐ Carfilzomib
‐ Izaxomib
‐ Bendamustine‐Dexamethasone
‐ Daratumumab
Novel approaches targeting the amyloid fibrils
• Chemotherapy: Daratumumab
• Anti amyloid agents:
‐ disruptors of amyloid fibrils: Doxicylin
‐ monoclonal antibodies targeting SAP, acomponent of the amyloid fibril
‐ NEOD001
Huntsman Cancer Institute Eighth Annual Hematology Review 66
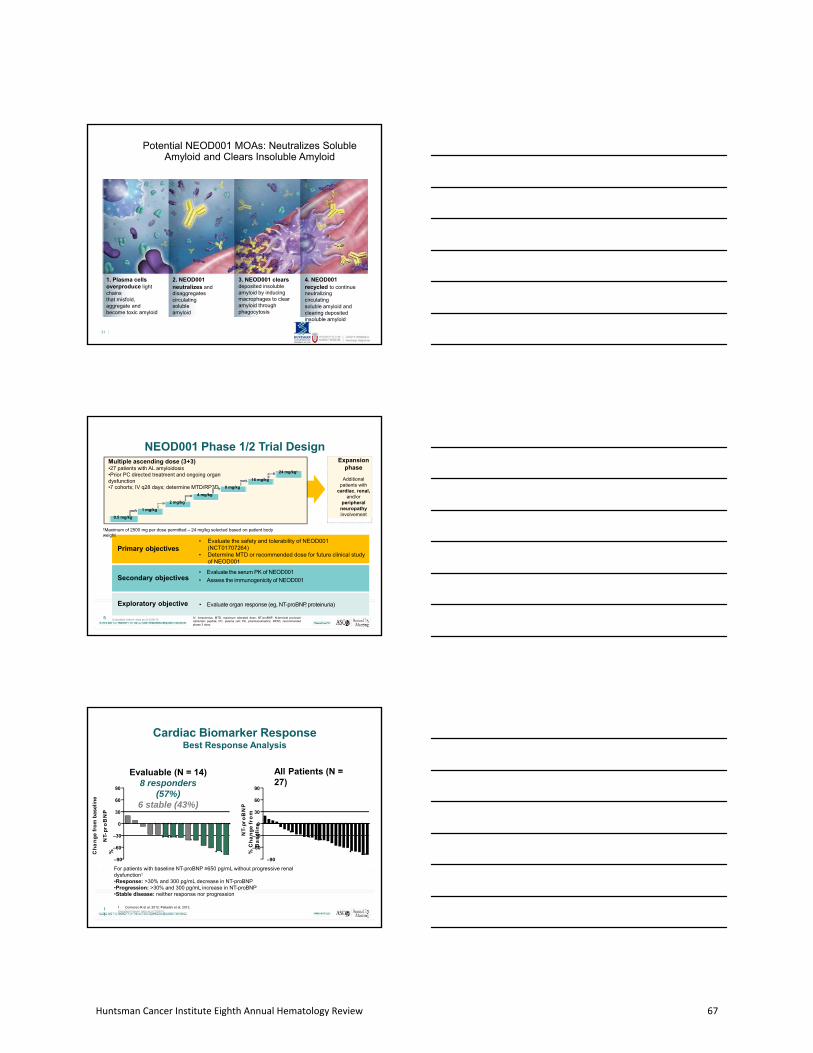
Potential NEOD001 MOAs: Neutralizes Soluble Amyloid and Clears Insoluble Amyloid
1. Plasma cells overproduce lightchainsthat misfold, aggregate and become toxic amyloid
31
2. NEOD001neutralizes and disaggregatescirculating solubleamyloid
3. NEOD001 clears deposited insoluble amyloid by inducing macrophages to clear amyloid through phagocytosis
4. NEOD001recycled to continue neutralizing circulatingsoluble amyloid andclearing deposited insoluble amyloid
NEOD001 Phase 1/2 Trial Design
Primary objectives• Evaluate the safety and tolerability of NEOD001
(NCT01707264)• Determine MTD or recommended dose for future clinical study
of NEOD001
Secondary objectives
Exploratory objective • Evaluate organ response (eg, NT-proBNP, proteinuria)
• Evaluate the serum PK of NEOD001
• Assess the immunogenicity of NEOD001
Expansion phase
Additional patients with
cardiac, renal, and/or
peripheral neuropathy involvement
Multiple ascending dose (3+3)•27 patients with AL amyloidosis•Prior PC directed treatment and ongoing organ dysfunction•7 cohorts; IV q28 days; determine MTD/RP3D
†Maximum of 2500 mg per dose permitted – 24 mg/kg selected based on patient body weight
24 mg/kg†
16 mg/kg
8 mg/kg
4 mg/kg
0.5 mg/kg
1 mg/kg
2 mg/kg
IV, intravenous; MTD, maximum tolerated dose; NT-proBNP, N-terminal pro-brainnatriuretic peptide; PC, plasma cell; PK, pharmacokinetics; RP3D, recommendedphase 3 dose.
5 Unaudited interim data as of 2/28/15
Cardiac Biomarker ResponseBest Response Analysis
–90 –90
For patients with baseline NT-proBNP ≥650 pg/mL without progressive renal dysfunction1
•Response: >30% and 300 pg/mL decrease in NT-proBNP•Progression: >30% and 300 pg/mL increase in NT-proBNP•Stable disease: neither response nor progression
Evaluable (N = 14)8 responders
(57%)6 stable (43%)
All Patients (N = 27)
–60
–30
0
30
60
90
NT-
pro
BN
P%C
ha
ng
efr
om
bas
elin
e
–60
1. Comenzo R et al, 2012; Palladini et al, 2012.Unaudited interim data as of 2/28/15
11
–30
0
30
60
90
NT-
pro
BN
PC
ha
ng
efr
om
B
as
eli
ne
%
Huntsman Cancer Institute Eighth Annual Hematology Review 67

Renal Biomarker ResponseBest Response Analysis
For patients with baseline proteinuria ≥0.5 g/24 hours1
• Response: >30% decrease in proteinuria or a decrease in proteinuria to <0.5 g/24 hours inthe absence of renal progression
• Progression: >25% worsening in eGFR• Stable disease: neither response nor progression
All Patients (N =24)
Evaluable (N = 15)9 responders (60%)
6 stable (40%)100
80
60
40
20
0
–20
–40
–60
–80
–100
Pro
tein
uri
a
%C
ha
ng
efr
om
Ba
se
lin
e 100
80
60
40
20
0
–20
–40
–60
–80
–100
1. Palladini et al. 2014.Unaudited interim data as of 2/28/1513
Pro
tein
uri
afr
om
Ba
se
lin
e%
Ch
an
ge
Baseline NT-proBNP = 3312 Best NT-proBNP = 1275 (-61.5%)Time since last hematologic response = 9.63 months
Patient Case ProfilesImproved and Sustained Response Over Time
Cardiac Renal
Baseline protein = 5129Best protein level= 1241 (-76%)Time since last hematologic response = 40.33 months
60 60
30 30
0 0
–30 – 30
–60 – 60
–90 – 900 2 4 6 8 10 12 14 16 18
NEOD001 Treatment, month
90 90120403
%C
han
ge
inB
ase
line
0 2 4 6 8 10 12 14
NEOD001 Treatment, month
110601
35 Unaudited interim data as of 2/28/15
Phase 3: The Vital Study (NCT02312206)Patients must be treatment naive and have a confirmed diagnosis of AL amyloidosis with cardiac involvement
Eligibility Criteria• ≥18 years old• Treatment naive• Confirmed new diagnosis of
AL amyloidosis• Cardiac involvement
• NT-proBNP ≥650 pg/mL
Key Exclusion Criteria
• Non-AL amyloidosis
• Diagnostic criteria for symptomatic multiplemyeloma
• NT-proBNP >8500 pg/mL Primary end point: Time to composite of all-cause mortality or cardiac hospitalizationKey Secondary end points: SF-36 (QoL), 6MWT, cardiac, renal, nerve, and hepatic response
N = 236
NEOD001 (24 mg/kg IV) + SOCn = 118
Placebo (normal saline IV) + SOCn = 118
Every 28 days for up to 42 monthsEvent-based timeline
QoL, quality of life; 6MWT, Six-Minute Walk Test.
Huntsman Cancer Institute Eighth Annual Hematology Review 68

Conclusions
• diagnostic accuracy is essential
• novel prognostic scores
• therapy:
‐ chemotherapy approaches
‐ transplant
• novel anti amyloidosis agents:
‐ agents destabilizing amyloid fibrils: doxicyclin
‐ monoclonal antibodies: NED001
Utah Amyloidosis Program
Services
1. Hematology - Chemotherapy and Stem Cell Transplant
2. Cardiology - Heart Failure
3. Nephrology - Renal Failure
4. Neurology - Polyneuropathy
Regional Referral Center
Huntsman Cancer Institute Eighth Annual Hematology Review 69

Huntsman Cancer Institute Eighth Annual
Hematology Review
Acute Leukemias
Paul Shami, MD
Huntsman Cancer Institute Eighth Annual Hematology Review 70

Acute Leukemias
Paul J. Shami, M.D.
Division of Hematology and Hematologic Malignancies
Huntsman Cancer Center
University of Utah
Outline
• AML drugs approved in 2017:
- Midostaurin
- Liposomal Daunorubicin/Cytarabine (CPX-351)
- Gemtuzumab Ozogamicin
- Enasidenib
• ALL drug approved in 2017:
- Inotuzumab Ozogamicin
Acute Myeloid Leukemia- 21,380 new cases in 2017.- 10,590 deaths in 2017.- 26.9% 5-year survival.- Disease involving mainly middle aged and elderly.
- Therapeutic backbone of cytarabine/anthracyclinedeveloped around 40 years ago.
- Transplant limited to a minority of patients- Hypomethylating agents for frail patients- Most of the therapeutic advances up to this point were
due to improved supportive care.
THINGS CHANGED IN 2017!
Huntsman Cancer Institute Eighth Annual Hematology Review 71

FLT3 Overview• Type III transmembrane receptor tyrosine kinase
– Other subfamily members include KIT, FMS, and PDGFR-α/ 1
• FLT3 is highly expressed on hematopoietic progenitors and is required for proliferation and differentiation of myeloid progenitorcell.
• Mutations in the FLT3 gene cause constitutive activation of the FLT3 receptor.
• ITD and TKD mutations are found in about 30% of AML patients.
• ITD mutations are associated with a worse prognosis.
Midostaurin
• Multikinase inhibitory activity.
• Targets include PKC, PDGFR, CDK1, KIT, VEGFR.
• Inhibitor of FLT-3.
• Synergy with cytotoxic chemotherapy.
• Phase Ib study established safety when combinedwith standard AML chemotherapy.
5/ M‐PKC‐
Huntsman Cancer Institute Eighth Annual Hematology Review 72
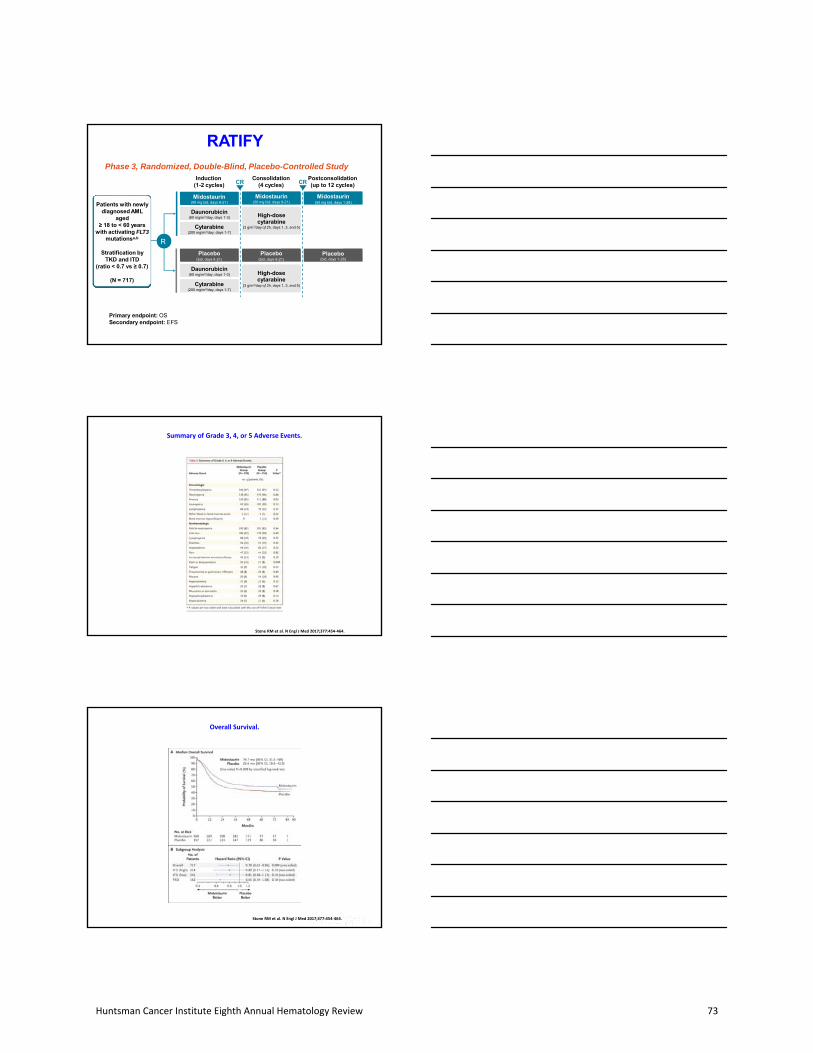
RATIFYPhase 3, Randomized, Double-Blind, Placebo-Controlled Study
Primary endpoint: OSSecondary endpoint: EFS
Postconsolidation(up to 12 cycles)
Midostaurin(50 mg bid, days 1-28)
Placebo(bid, days 1-28)
Cytarabine(200 mg/m2/day, days 1-7)
Daunorubicin(60 mg/m2/day, days 1-3)
Midostaurin(50 mg bid, days 8-21)
Placebo(bid, days 8-21)
Cytarabine(200 mg/m2/day, days 1-7)
Daunorubicin(60 mg/m2/day, days 1-3)
High-dose cytarabine
(3 g/m2/day q12h, days 1, 3, and 5)
Consolidation(4 cycles)
Midostaurin(50 mg bid, days 8-21)
High-dosecytarabine
(3 g/m2/day q12h, days 1, 3, and 5)
Placebo(bid, days 8-21)
Induction(1-2 cycles) CR CR
R
Patients with newly diagnosed AML
aged≥ 18 to < 60 years
with activating FLT3mutationsa,b
Stratification by TKD and ITD
(ratio < 0.7 vs ≥ 0.7)
(N = 717)
Stone RM et al. N Engl J Med 2017;377:454‐464.
Summary of Grade 3, 4, or 5 Adverse Events.
Stone RM et al. N Engl J Med 2017;377:454‐464.
Overall Survival.
Huntsman Cancer Institute Eighth Annual Hematology Review 73
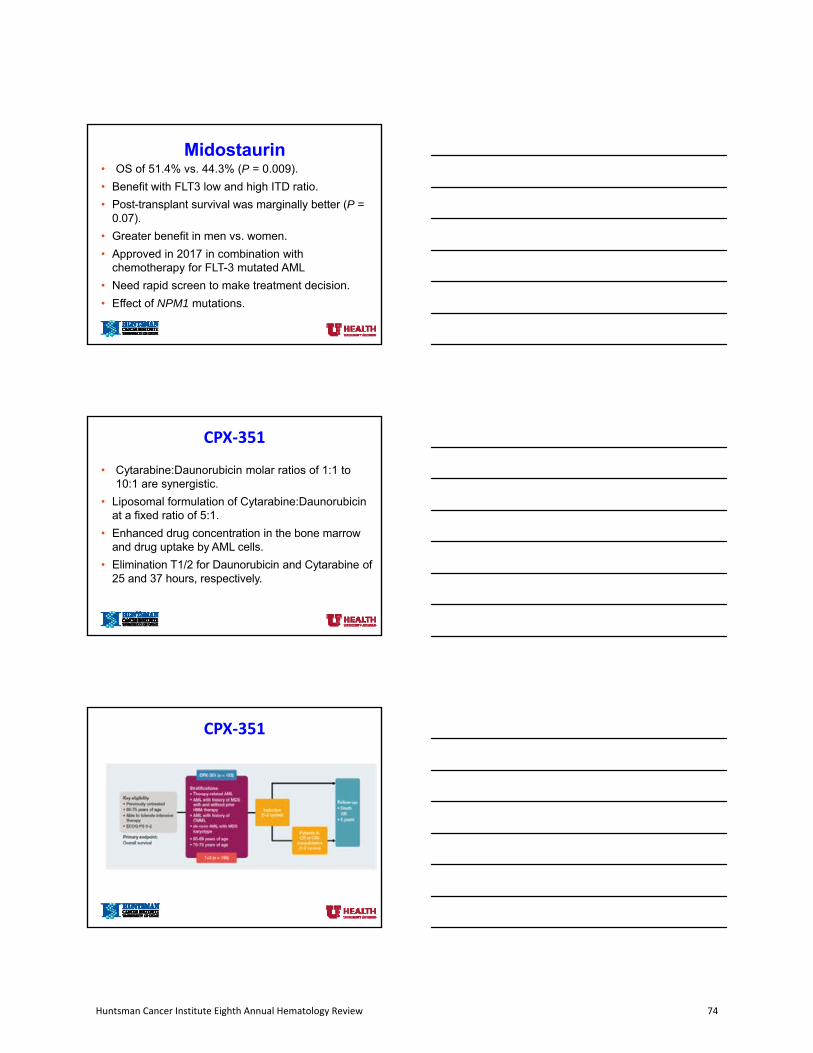
Midostaurin• OS of 51.4% vs. 44.3% (P = 0.009).
• Benefit with FLT3 low and high ITD ratio.
• Post-transplant survival was marginally better (P =0.07).
• Greater benefit in men vs. women.
• Approved in 2017 in combination withchemotherapy for FLT-3 mutated AML
• Need rapid screen to make treatment decision.
• Effect of NPM1 mutations.
CPX‐351
• Cytarabine:Daunorubicin molar ratios of 1:1 to10:1 are synergistic.
• Liposomal formulation of Cytarabine:Daunorubicinat a fixed ratio of 5:1.
• Enhanced drug concentration in the bone marrowand drug uptake by AML cells.
• Elimination T1/2 for Daunorubicin and Cytarabine of25 and 37 hours, respectively.
CPX‐351
Huntsman Cancer Institute Eighth Annual Hematology Review 74

CPX‐351
CPX‐351• Higher CR rate than 7+3 (47.7 vs. 33.3%) in patients with
antecedent hematologic disorders or t-AML.• Higher OSrate than 7+3 (9.56 vs. 5.95 months) in patients
with antecedent hematologic disorders or t-AML.• Longer cytopenias than 7+3.• FDA-approved for t-AML and AML with MDS-related
changes.• Younger patients and t-AML were not studied in the pivotal
trial.• Morphologic definition of MLD is subjective to a certain
extent.• Cytogenetic information may not be available at the time
of treatment decision.
Gemtuzumab Ozogamicin (GO)
• Antibody drug conjugate, directed at CD33 and linked to calicheamycin.
• Approved in 2000 for relapsed AML in olderpatients.
• Drug taken off in 2010 after findings in a SWOG randomized trial.
• European studies completed after withdrawalshowed benefit in subgroups of patients.
Huntsman Cancer Institute Eighth Annual Hematology Review 75

ALFA-0701 trial
• Phase 3 trial of the ALFA group in patients 55‐70.
• N=280.
• Design: patients with de novo AML randomized to 7+3 ± fractionated GO.
• Study showed same response rate but lowerrelapse risk in GO arm, especially in patients withfavorable risk AML (CBF AML).
Castaigne et al, Lancet 379:1508, 2012
ALFA-0701 trial
Castaigne et al, Lancet 379:1508, 2012
Hills meta-analysis
• Meta‐analysis of 4 randomized trials.
• GO in newly diagnosed AML in combination withchemotherapy.
• N=3325.
• Findings:
‐ the optimal dose of Mylotarg is 3 mg, in single or fractionated doses.
‐ CR rate is not increased but relapse risk is reduced.
‐ maximal benefit observed in favorable risk AML.
Hills et al, Lancet Oncol 15:986, 2014
Huntsman Cancer Institute Eighth Annual Hematology Review 76
Hills et al, Lancet Oncol 15:986, 2014
Hills meta-analysis
Hills et al, Lancet Oncol 15:986, 2014
Overall survival according to cytogenetic risk category
Gemtuzumab Ozogamicin (GO)• Only 50% of the calicheamicin payload is conjugated to the
Ab, raising concerns about toxicity and competition betweenunconjugated Ab and conjugated Ab.
• VOD is a concern, particularly if given close to transplant.
• Fractionated dosing improves safety profile withoutcompromising efficacy.
• FDA re‐approved the drug at a lower fractionated dose in 2017 with a broad spectrum of indications (newly diagnosed,R/R, combined with chemotherapy, single agent.
• Dosing and safety of fractionated GO in combination withHiDAC consolidation regimens needs to be established.
Huntsman Cancer Institute Eighth Annual Hematology Review 77

• IDH1 and IDH2 are enzymes of the citric acid cycle.
• Mutant IDH1 and IDH2 (mIDH1 and mIDH2) occurs in 8 and 12% ofpatients with AML.
• Result is production of 2-HG, which alters DNA methylation and leadsto a block in cellular differentiation.
• Enasidenib (AG-221) is a selective, oral, potent inhibitor of mIDH2 enzyme.
• Enasidenib induces differentiation of leukemic cells.
Isocitrate Dehydrogenase (IDH) Mutations as a Target in AML
22
EnasidenibPhase 1/2 Study Design
• Patients with relapsed/refractory AML (239) and mIDH2.
• Dose range of 50 – 650 mg/day.
• Dose of 100 mg/day selected for expansion cohort.
• Generally well tolerated.
• Grade 3 – 4 AEs included hyperbilirubinemia (12%).
• Differentiation syndrome (7%).
Stein et al, Blood 130(6):722; 2017
EnasidenibPhase 1/2 Study Design
• CR/CRi 26.6%.
• PR and morphologic leukemia-free state 12%.
• Median duration of response of 5.6 months.
• Overall Survival of 9.3 months.
• OS of 19.7 months if CR achieved.
• No marrow aplasia observed.
Stein et al, Blood 130(6):722; 2017
Huntsman Cancer Institute Eighth Annual Hematology Review 78

Evolution of response during treatment of responding patients (n = 71).
Eytan M. Stein et al. Blood 2017;130:722-731
©2017 by American Society of Hematology
Morphologic evidence of myeloid differentiation during enasidenib treatment.
Eytan M. Stein et al. Blood 2017;130:722-731
©2017 by American Society of Hematology
Mean (± standard error) platelet count, absolute neutrophil count, hemoglobin, and bone marrow blasts over time in patients with relapsed/refractory AML treated with enasidenib.
Eytan M. Stein et al. Blood 2017;130:722-731
©2017 by American Society of Hematology
Huntsman Cancer Institute Eighth Annual Hematology Review 79

Overall survival.
Eytan M. Stein et al. Blood 2017;130:722-731
©2017 by American Society of Hematology
Enasidenib
• Differentiation rather than cytotoxic effect.
• Prolonged time for optimal response.
• Differentiation syndrome – Treat promptly with steroids.
• FDA approved in 2017 for R/R AML with mIDH2.
• Role in the first-line setting to be determined.
Stein et al, Blood 130(6):722; 2017
Venetoclax
• BCL2 inhibitor with modest single agent activity in AML (19% CR/CRi).
• Combined with hypomethylating agents or low dose cytarabine in elderly patients who are not eligible for intensive therapy.
• CR/CRi of 62 – 68%.
• 12-months survival of 50 – 70%.
• NOT FDA approved for this indication.
• Stay tuned.
Huntsman Cancer Institute Eighth Annual Hematology Review 80

AML 2018
• No longer one size fits all.
• Choices of therapies depending on multiple factors: history, chromosomal rearrangement, molecular findings.
• It is critically important to obtained comprehensive chromosomal and molecular studies in a timely fashion.
• More agents are coming.
• Cost of newly approved agents is a significant issue.
• Optimal management of MRD is still an open question.
AMLNCCN 2017
AML- NCCN 2018
Huntsman Cancer Institute Eighth Annual Hematology Review 81
Newly Diagnosed non-APL AML Fit for InductionHCI 2018
• Obtain molecular studies as soon as possible.
• Clinical trial preferred.
• CBF leukemia: Chemotherapy + GO.
• FLT3-mutated AML: Chemotherapy + Midostaurin followed by transplant if feasible.
• Secondary AML: CPX-351 followed by transplant if feasible.
ALLInotuzumab Ozogamicin (IO)
• CD22 is expressed on 90% of B-cell ALL cells.
• IO is a humanized anti-CD22 antibody conjugated to Calicheamicin.
• Adults (326) with R/R B-cell ALL randomize to IO vs. standard intensive chemotherapy.
• CR rate of 80.7% vs. 29.4% (P < 0.001).
• Median PFS of 5.0 vs. 1.8 months (P < 0.001).
• Median OS of 7.7 vs. 6.7 months (P = 0.04).
• VOD of 11% vs 1%.
• FDA approved in 2017 for R/R B-cell ALL.
Kantarjian et al, NEJM 375:740; 2016
Acute LeukemiaNursing Considerations
• It will often take longer to make treatment decisions for AML.
• Patients may be sent home without therapy pending results of molecular studies.
• During that time more intensive outpatient monitoring will be required with interventions that could include transfusions. During that time watch for any indication to re-admit the patient, especially infections (fever, etc…) and bleeding.
• Watch for liver toxicity, particularly VOD (abnormal liver function tests, jaundice, weight gain, ascites) with GO and IO.
• Watch for differentiation syndrome with enasidenib (fever, SOB, oxygen requirement).
• CPX-351 is associated with longer cytopenias than standard 7+3.
Huntsman Cancer Institute Eighth Annual Hematology Review 82

Suggested Reading
• Wei AH and Tiong IS. Blood 130(23):2469-2474;2017.
• Kantarjian et al. NEJM 375(8):740-753, 2016.
Acknowledgement
• Tibor Kovacsovics
Huntsman Cancer Institute Eighth Annual Hematology Review 83
Huntsman Cancer Institute Eighth Annual
Hematology Review
Cancer Survivorship
Paul Thielking, MD Rachel Montague, APRN, FNP-C
Brighton Loveday, APRN, ANP-BC Jaclyn Piper-Williams, APRN, FNP-C
Huntsman Cancer Institute Eighth Annual Hematology Review 84

Cancer SurvivorshipHCI Supportive Oncology & Survivorship Team
Paul Thielking, MD Brighton Loveday, APRN, ANP‐BCRachel Montague, APRN, FNP‐C Jaclyn Piper‐Williams, APRN, FNP‐C
HCH Supportive Oncology Team
Learning Objectives
Upon completion of this presentation, participants will be able to:
Identify the members and role of the Supportive Oncology team here at HCH
Define “survivorship” in cancer patients, with particular attention to those with hematologic cancers
Discuss the role of a Survivorship Care Plan
Describe the complex medical and psychosocial needs of survivors and ways to attend to those needs
Discuss some of the most common sequelae of cancer treatment
Huntsman Cancer Institute Eighth Annual Hematology Review 85

Survivorship – Who are “survivors”
National Coalition for Cancer Survivorship4
– Starting at the point of diagnosis and for the balance of life
ASCO Functional Definition3
– Individuals who have successfully completed curative treatment or those who have transitioned to maintenance or prophylactictherapy (acute, extended, permanent)
NCI & NCCN (National Comprehensive Cancer Network)6
– An individual is considered a cancer survivor from the time of diagnosis through the balance of his or her life. Family members, friends, and caregivers are also impacted.
Survivorship – Who are “survivors”
American Cancer Society1
Any person with a history of cancer, from the time of diagnosis through the remainder of their life
Three phases of “survival”: Time from diagnosis to end of initial treatment
Transition from treatment to extended survival
Long‐term survival
Encompasses a range of cancer experiences and trajectories
May be difficult to define in hematologic cancers where the “treatment” phase is more long‐term…
American Cancer Society, 2016
Huntsman Cancer Institute Eighth Annual Hematology Review 86
Survivorship ‐ What
Primary or secondary cancer prevention
Surveillance for cancer recurrence
Health promotion (intervention)
Symptom management of common and long‐term late effects (coordination)
Assessment of late psychosocial and medicaleffects
Survivorship ‐ Where
• Everywhere!
• Clinical settings – outpatient, inpatient,community
• Primary oncology team responsible forproviding Survivorship Care Plan which is thensupplied to community based care teams (PCP,specialists, etc)
• Once completed, found under “TreatmentSummary” in Problem List in EPIC
Survivorship ‐ When
Defined time period group specific
Generally within first year followingcompletion of treatment and transitioning into “surveillance” or “remission” phase
Acute/initial, extended, long‐term
Huntsman Cancer Institute Eighth Annual Hematology Review 87

Survivorship ‐ Why
As of January 1, 2016, more than 15.5 million cancer survivors in the U.S.1
– Expected to be 20.3 million by 2026– More than the populations of NYC, Houston, and Chicago combined
Longer lifespans, increasing survival rates At least 50% of survivors suffer late effects of cancer –
most commonly pain, depression, fatigue Survivors are remarkably resilient, but may have to
make physical, emotional, social, and spiritual adjustments to their lifestyle – in other words, to find a “new normal.”
Survivorship ‐ Why
Quality of life (QOL) is a broad multidimensional concept that considers a person’s physical, emotional, social, and spiritual well‐being
Individuals who have a history of more invasive and aggressive treatments tend to report poorer functioning and QOL
Healthy behaviors hugely important for survivors –nutrition, physical activity, smoking cessation, etc
Cancer not only affects survivors but also their family members and close friends
Role of Survivorship Care Plans
In 2006, IOM issued a report recommending that every cancer patient receive an individualized plan1
American College of Surgeons sets standards for percentage of delivered survivorship care plans – current goal is >50% ofeligible patients (reduced from 75%)2
Designed to provide patients and their clinicians with a treatment summary, information about possible late and long‐term effects, follow‐up care/surveillance guidelines,recommendations for healthy living, delineation of oncologist/PCP roles and timing of transfer of care if needed, and identification of supportive resources3
Huntsman Cancer Institute Eighth Annual Hematology Review 88
Example of Survivorship Care Plan
NCCN, 2018
References1. American Cancer Society. Cancer Treatment & Survivorship Facts & Figures 2016‐
2017. Atlanta: American Cancer Society; 2016.2. American College of Surgeons. (2017, December 13). Important information
regarding CoC Survivorship Care Plan Standard. Retrieved fromhttps://www.facs.org/quality‐programs/cancer/news/survivorship.
3. American Society of Clinical Oncology. (2018). About survivorship. Retrieved fromhttps://www.cancer.net/survivorship/about‐survivorship.
4. Center for Disease Control and Prevention. (2017). Cancer Survivorship. Retrieved from http://www.cdc.gov/cancer/survivorship/.
5. National Coalition for Cancer Survivorship. (2018). https://www.canceradvocacy.org/.
6. National Comprehensive Cancer Network. (2018). NCCN guidelines version 2.2017 survivorship. Retrievedhttps://www.nccn.org/professionals/physician_gls/pdf/survivorship.pdf.
7. Taylor, K., DipOnc, G., & Monterosso, L. (2015, May). Survivorship Care Plans and Treatment Summaries in Adult Patients With Hematologic Cancer: An Integrative Literature Review. In Oncology nursing forum (Vol. 42, No. 3).
Depression
and
Anxiety
Huntsman Cancer Institute Eighth Annual Hematology Review 89

Depression ‐ Prevalence1,2
Depression ‐ (DSM‐IV)3
Five or more of the following symptoms during a2‐week period with a change in functioning. Atleast one of the symptoms of either depressedmood or loss of interest/pleasure
– Depressed mood– Diminished interest– Weight loss/gain or appetite changes– Insomnia/hypersomnia– Psychomotor agitation/retardation– Fatigue/ loss of energy– Feelings of worthlessness/guilt– Diminished ability to think/concentrate– Recurrent thoughts of death
Depression ‐ Diagnosis4
“Exclusive” approaches attempt to exclude symptoms that overlap with physical illness such as fatigue or weight loss. Endicott proposed focusing on hopelessness, helplessness, worthlessness, guilt instead of somatic symptoms in cancer patients.
Anhedonia could be due to decreased functional status
Inclusive approaches include all symptoms in DSM. Risk of over‐diagnosis of depression in medically ill is small.
Benefits of treatment outweigh risks associated withfailure to treat.
Huntsman Cancer Institute Eighth Annual Hematology Review 90

Depression ‐ Assessment 1,4
Instruments validated and used often inmedically ill Hospital Anxiety and Depression Scale Patient Health Questionnaire (PHQ‐9) Single item “are you depressed?”
Two item “have you been depressed, and haveyou lost interest or pleasure?”
Beck Depression Inventory Hamilton Depression Scale
Depression ‐ Treatment1,5,6
Challenging if life expectancy is limited
Psychotherapy
Individual, Group, Family
Depression ‐ SSRIs
Paroxetine
Fluoxetine
Sertraline
Citalopram
Escitalopram
Huntsman Cancer Institute Eighth Annual Hematology Review 91
Depression ‐ SNRIs
Venlafaxine
Duloxetine
Depression ‐ Atypical Antidepressants
Buproprion
Mirtazapine
Olanzapine
Ketamine
Depression‐Tricyclic Antidepressants
Desipramine
Nortriptyline
Amitriptyline
Imipramine
Huntsman Cancer Institute Eighth Annual Hematology Review 92

Psychostimulants7
Methylphenidate is most commonly prescribed.
Augmentation therapy for depression
Counteracts sedation associated with opioid use.
CNS malignancies – may enhance cognitivefunction, stamina, motivation.
May help fatigue with neurodegenerativediseases and HIV.
Psychostimulants5,7
Methylphenidate is most commonly prescribed.
Augmentation therapy for depression
Counteracts sedation associated with opioid use.
CNS malignancies – may enhance cognitivefunction, stamina, motivation.
May help fatigue with neurodegenerativediseases and HIV.
Prognosis < 6 Months5
*Consider referral to psychiatrist if patient has suicidal ideation, treatment resistant depression, diagnostic uncertainty
Huntsman Cancer Institute Eighth Annual Hematology Review 93

Prognosis > 6 Months5
*patient preference, prior response to meds, primary relative response to meds, anticipated side effects, co‐occurring conditions, potential drug interactions, cost.**augmenting options include bupropion (Wellbutrin), buspirone (Buspar), T3 (Cytomel), lithium.
Anxiety8
Symptoms thought to occur in up to 70% ofmedically ill patients
Adjustment Disorder, Panic Disorder, GeneralizedAnxiety Disorder, PTSD most common
Distress may be related to physical, psychological,social, spiritual, practical, end‐of‐life, and lossissues
Fear of uncontrolled symptoms or dependency
Anxiety ‐ Treatment
Care Tenor Treating patients with compassion, respect, dignity.
Compassionate, patient‐centered care Frequent meetings with team, opportunity to be involved in decisions, information about diagnosis and prognosis, psychological support for patient and family
Combination of pharmacologic and non‐pharmacologic approaches usually is mosteffective
Huntsman Cancer Institute Eighth Annual Hematology Review 94

Anxiety ‐ Psychotherapy
Psychotherapies for Anxiety Supportive psychotherapy (emphatic, compassionate, non‐judgmental listening) CBT (focus on modifying dysfunctional thoughts, feelings, behaviors) Interpersonal Therapy (focus on role of social dysfunction in creating or maintaining distress)
Psychotherapies for Palliative Care Managing Cancer and Living Meaningfully (CALM) Dignity Therapy (Chochinov) Meaning Centered Therapy (Breitbart)
Anxiety ‐ Complementary Therapies
Music Therapy
Relaxation Training
Acupuncture
Meditation
Mind Body Skills Group
Aromatherapy
Massage
Art Therapy
Anxiety ‐ Other Interventions
Exercise
Decreased caffeine and alcohol consumption
Sleep hygiene
Psycho‐education
Huntsman Cancer Institute Eighth Annual Hematology Review 95

Anxiety ‐ Pharmacologic Interventions
SSRIs are drug of choice
SNRIs
Neuropathic Pain
Mirtazapine
Sedating
Buspirone
Anxiety ‐ Pharmacologic Interventions
Benzodiazepines– Very short acting
• Midazolam 0.5‐5 mg/hr infusion
– Short acting • Lorazepam 0.5‐2 mg bid PO, SL, IV, IM
– Intermediate • Chlordiazepoxide 10‐50 mg tid‐qid PO, IM
– Long Acting • Clonazepam 0.25‐3 mg qd‐bid PO.
• Diazepam 2‐10 mg qd‐bid PO, IV, IM, PR
Anxiety ‐ Pharmacologic Interventions
Other Anxiolytics
– Trazodone 25 mg q 1 hr, NTE 500 mg in 24 hr
– Gabapentin 100 mg q 1 hr, NTE 3600 mg in 24 hr
– Hydroxyzine 25‐100 mg q 6 hrs
– Lyrica
Huntsman Cancer Institute Eighth Annual Hematology Review 96

References
1. Ali Abbas AA, Wagle KC, et al. Depression in terminally ill patients: dilemmas in diagnosis and treatment. Journal of Pain and Symptom Management. May, 2013. 45(5);926‐933
2. Walker J, Hansen CH, et al. Prevalence of depression in adults with cancer: a systematic review. Ann Oncol.2013;24(4):895‐900.
3. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders.4th ed., 2000
4. Klopstein KG, Marin DB. How does one assess for psychiatric illness in patients with advanced disease? Evidence‐based practice of palliative medicine.2013. Chapter 35.176‐180.
5. Irwin SA, Block S. What treatments are effective for depression in the palliative care setting? Evidence Based Palliative Medicine. 2013. Chapter 33.
6. Strouse TB. Psychopharmacologic treatment of depression in patients with cancer: a 2013 update. FOCUS The Journal of Lifelong Learning in Psychiatry. Fall 2013; 482‐498.
7. Prommer E. Methylphenidate: established and expanding roles in symptoms management. American Journal of Hospice and Palliative Medicine. 2012;29(6:):483‐490.
8. Irwin SA, Montross, LP, Chochiov HM. What treatments are effective for anxiety in patients with serious illness? Evidence Based Palliative Medicine. 2013. Chapter 34.
Pain
Management
Part of a Bigger Picture
Majority of cancer patients will experience acutepain related to procedures, interventions, orcomplications
30‐50% of patients require opioid therapy forchronic pain during antineoplastic therapy, up to90% in those with advanced disease
Huntsman Cancer Institute Eighth Annual Hematology Review 97

Acetaminophen & NSAIDs
Effective for mild nociceptive or visceral cancer‐related pain
May be used as monotherapy, or in combinationwith opioids
Opioid‐sparing
NSAID contraindications: history of PUD, concurrent corticosteroid use, bleeding history,renal insufficiency, thrombocytopenia, orconcurrent anticoagulant use
NSAIDs Celecoxib
– Only available selective COX‐2 inhibitor in the US– Does not affect platelet aggregation, safer for concurrent anticoagulation or if
thrombocytopenic– ↓ GI toxicity, ↑ cardiovascular toxicity– May be cost‐prohibitive
Meloxicam– 7.5mg dose may be safely used with concurrent anticoagulation or
thrombocytopenia– Typically more affordable than celecoxib
Naproxen– ↓ Cardiovascular toxicity, ↑ GI toxicity– OTC and Rx strengths
* Consider addition of PPI for gastroprotection
Neuropathic Pain Gabapentinoids
– First line treatment in pts without co‐occurring depression– Pregabalin has simplified dosing but typically requires prior‐authorization– Gabapentin is typically less cost‐prohibitive, has large range of dosing– No known drug‐drug interactions– Most common side effects are somnolence and mental cloudiness
Duloxetine– Specifically studied in CIPN, analgesia noted at 30‐60mg daily– First line treatment if concurrent depression and CIPN– May be cost‐prohibitive
TCAs– Amitriptyline is least tolerated, has most bothersome side effect profile, ↑
anticholinergic– Nortriptyline and Desipramine have less side effects at lower doses– May also help with sleep– Affordable, on $4 drug list– Use with caution in elderly population
Huntsman Cancer Institute Eighth Annual Hematology Review 98

Topical Agents Diclofenac ‐ NSAID
– Voltaren gel 1%, must be applied 3‐4 times/daily• Best for localized nociceptive pain of superficial joints, non‐neuropathic
– Flector patch 1.3%, applied BID• Useful for musculoskeletal pain• May be cost‐prohibitive
Capsaicin– Derived from the chili pepper– Depletes substance P from afferent C fibers– Available OTC in cream or low‐dose patch– Weak to moderate analgesic effect for neuropathic pain– Most common side effect is burning at administration site
Lidocaine– 5% patches available with Rx only, may be cost‐prohibitive– 4% patches are OTC, more affordable– Available in creams, ointments, and gels for local pain relief, more affordable option– Weak evidence to support benefit for neuropathic pain– Clinical experience indicates modest benefit with limited side effects
Opioid Therapy
High dose = > 90mg OME Goal for gradual reduction of opioid therapy over time, due
to risks associated with chronic opioid use Opioids are first line for cancer‐related pain during active
cancer treatment, but not recommended for long‐term use Long‐term use is associated with fatigue, low testosterone,
immune suppression, dental problems due to decreased salivary gland production, physical and emotional dependence, addiction and opioid‐induced hyperalgesia.
Recommend use of adjunctive and alternative treatments in longer term survivorship
Opioid Therapy
Short‐acting opioids are indicated for acute painsyndromes– Tramadol, Norco, Morphine, Oxycodone, Hydromorphone
Long‐acting formulations are reserved forchronic management, not for first‐line therapy– MS Contin, Fentanyl Patch, OxyContin
– Cost may be prohibitive with certain agents
Consider move to long‐acting opioids if OME >90mg
Huntsman Cancer Institute Eighth Annual Hematology Review 99

Clinical Pearls
Avoid Morphine products with renal insufficiency– Oxycodone, Fentanyl, Hydromorphone safer options
Always consider adjunctive medications for opioid‐sparing benefits
Consideration for Interventional Pain evaluation– Neurolysis, corticosteroid injections, Intrathecal Pain Pump,
lidocaine infusion
Recommend regular Controlled Substance Database reviewof each patient, both in clinic and inpatient– Limit number of prescribers if possible
Always put your patients on a bowel regimen– Senna‐S and Miralax are first‐line agents
References
1. Portenoy, R. K., & MZ, A. E. (2010). Cancer pain management: General principles and risk management for patients receiving opioids. Uptodate.
2. Portenoy, R. K., Ahmed, E., & Keilson, Y. Y. (2012). Cancer pain management: use of acetaminophen and nonsteroidal anti‐inflammatory drugs. UpToDate, 18.
3. Portenoy, R. K., Ahmed, E., & Keilson, Y. Y. (2017). Cancer pain management: Adjuvant analgesics (coanalgesics). UpToDate.(Accessed on April 25, 2016.).
4. Portenoy, R. K., & Dhingra, L. K. (2017). Overview of cancer pain syndromes.
Cancer‐Related Fatigue
and
Wellness Services
Huntsman Cancer Institute Eighth Annual Hematology Review 100

Cancer‐Related Fatigue (CRF)
Fatigue is a common problem in cancer patients, both in those being actively treated and in cancer survivors.
CRF profoundly affects quality of life (QOL) of both patients and their families.
It is routinely identified by patients as one of the most distressing symptoms associated with cancer and its treatment.
Treatment of CRF is one of the major symptoms the supportive care focuses on.
Guidelines from Groups
ASCO Encourage all patient to engage in a moderate level of physical activity
after cancer treatment (eg, 150 minutes of moderate aerobic exercise such as fast walking, cycling, or swimming) per week with an additional 2‐3 strength training (such as wt. lifting) sessions per week unless contraindicated.
Walking programs are generally safe for most cancer survivors.
Survivors are at a higher risk of injury (those living with neuropathy, cardiomyopathy, or other long‐term effects of therapy) and patients with severe fatigue interfering with function should be referred to a PT or exercise specialist.
Guidelines from Groups
NCCN Provide information about patterns of fatigue during and after treatment (conservation, pacing, peak energy times).
Make use of local resources to increase exercise (Cancer centers, community programs focused on survivors).
For patients with fatigue interfering with function, consider referral to a physical therapist or physiatrist
Psychosocial interventions recommended (CBT, nutrition consultation, sleep hygiene, acupuncture, etc).
Consider psychostimulants
Huntsman Cancer Institute Eighth Annual Hematology Review 101

Impact on Quality of Life
Survivors of allo‐HSCT are at high risk for treatment‐related adverse events that may worsen physical capacity and may induce fatigue and disability.
Exercise capacity was reduced in most allo‐HSCT long‐term survivors1
– Because reduced exercise capacity was associated with fatigue, disability and decrease in QOL, recommendation was made for exercise testing in every patient who reports fatigue and disability.
1 Dirou, S., Chambellan, A., Chevallier, P., Germaud, P., Lamirault, G., Gourraud, P. A., ... & Peterlin, P. (2017).
Huntsman Cancer Institute Eighth Annual Hematology Review 102
Role of Exercise Programs
Supervised or prescribed exercise programs can reduce or reverse declines in physical fitness seen during and after medical treatment in cancer survivors2
Exercise programs increase strength, decrease fatigue.
Supervised exercise has been consistently shown to be safe in this population and is recommended by the National Comprehensive Cancer Network (NCCN) and the American College of Sports Medicine (ACSM) among others.
2 Marker, R. J., Cox‐Martin, E., Jankowski, C. M., Purcell, W. T., & Peters, J. C. (2017)
HCH Wellness Program ‐ Mission
To empower people affected by cancer to improve their quality of life, reduce treatment side effects, and increase strength for daily living through movement in a supportive atmosphere
HCH Wellness Program ‐ Overview
Physical assessments
Personalized exercise prescriptions
Supervised Individual training
Group Training sessions
Community‐based activities such as road biking, hiking, and
rowing
Many classes for patients, caregivers, and staff
Telemedicine Visits
Huntsman Cancer Institute Eighth Annual Hematology Review 103

Impact of Physical Activity
Improvements in: Fatigue Nausea Pain Insomnia/Sleep Depression Anxiety Quality of Life Emotional Wellbeing Cardiovascular Fitness Muscle Strength Body Composition And much more…
Mind‐Body Interventions
Mindfulness‐based stress reduction
Mind Body Skills Group here at Huntsman
Yoga
Acupuncture
Touch therapy, massage
Music therapy
Relaxation, Reiki and QiGong
Mindfulness‐Based Stress Reduction
There is evidence from randomized trials that mindfulness‐based approaches may relieve fatigue in cancer survivors.
In the largest trial, 229 women with early‐stage breast cancer after surgery, chemo, and radiotherapy were randomly assigned to an 8‐week program of mindfulness‐based stress reduction or usual care.
The intervention group had significant improvements at 8 wks.
3 Escalante, C.P. (2017)
Huntsman Cancer Institute Eighth Annual Hematology Review 104

Yoga
There is some evidence from randomizedtrials that mind‐body approaches such as yogamay improve sleep quality and fatigue.
– Four of the five trials have enrolled cancer survivors.
In the largest trial, 410 patients with breast cancer. After four weeks, yoga participants demonstrated greater improvements compared with baseline in global sleep quality, greater reduction in daytime dysfunction and reduced use of sleep medications.
3 Escalante, C.P. (2017)
Acupuncture
Benefits of acupuncture for CRF are unclear.
Major problem with interpreting study results is the lack of a sham acupuncture control group; at least in the setting of non‐cancer disease such as chronic pain, both acupuncture and sham acupuncture have been shown to have much greater efficacy than no treatment – suggesting a strong placebo effect.
Benefit from acupuncture has been suggested in at least four randomized trials, some conducted in cancer survivors and some in patients receiving active treatment.
3 Escalante, C.P. (2017)
Acupuncture
In the largest trial, 302 patients with non‐metastatic breast cancer who completed chemotherapy and were experiencing at least moderate fatigue were randomly assigned to usual care with and without acupuncture.– The usual care received a booklet with info about fatigue and its
management, while the acupuncture group received both the booklet and a once weekly treatment by an acupuncturist for 6 weeks.
– Acupuncture was of significant benefit, with an estimated difference in the week 6 general fatigue score and also significantly improved other fatigue aspects including physical and mental fatigue, anxiety and depression, and QOL.
3 Escalante, C.P. (2017)
Huntsman Cancer Institute Eighth Annual Hematology Review 105

Pharmacologic Management
For patients with severe fatigue during cancer therapy in whom non‐pharmacologic methods are not helpful, and anemia and other medical conditions and symptoms causing fatigue are controlled, a therapeutic trial of a psychostimulant or other wakefulness agent is suggested.– Methylphenidate, dexmethylphenidate, modafinil
Benefit for psychostimulants in patients with CRF was suggested in a year 2010 Cochrane review of five trials(four used methylphenidate).– There was a small but statistically significant improvement in
fatigue score relative to placebo.
References
1. Dirou, S., Chambellan, A., Chevallier, P., Germaud, P., Lamirault, G., Gourraud, P. A., ... & Peterlin, P. (2017). Deconditioning, fatigue and impaired quality of life in long‐term survivors after allogeneic hematopoietic stem cell transplantation. Bone marrow transplantation, 1.
2. Marker, R. J., Cox‐Martin, E., Jankowski, C. M., Purcell, W. T., & Peters, J. C. (2017). Evaluation of the effects of a clinically implemented exercise program on physical fitness, fatigue, and depression in cancer survivors. Supportive Care in Cancer, 1‐9.
3. Escalante, C.P. Cancer‐related fatigue:Treatment. 2017 December. Retrieved on 2/1/18 fromUpToDate; https://www.uptodate.com/contents/cancer‐related‐fatigue‐treatment
Understand all of our patients are at high risk for depression,
anxiety, pain, sleep disturbances, anorexia, fatigue, and many more
challenges throughout the course of cancer treatment and into
survivorship. Be sure to frequently assess not only the physical but
also the mental, emotional, and spiritual well‐being of your
patients and their families.
Encourage patients to explore services of the Wellness Center for
Power Program, complementary therapies, and other modalities
for ensuring quality of life. There are many here at HCH!
Feel free to contact SOS, both inpatient and outpatient, for
additional support with symptom management and coping needs
Nursing Considerations
Huntsman Cancer Institute Eighth Annual Hematology Review 106

Thank you!
Huntsman Cancer Institute Eighth Annual Hematology Review 107

Huntsman Cancer Institute Eighth Annual
Hematology Review
Differential Diagnosis of Polycythemias and New Clinical
Data on Ph-negative MPNs
Josef Prchal, MD
Huntsman Cancer Institute Eighth Annual Hematology Review 108

Differential Diagnosis of Polycythemias and new clinical data on Ph-negative MPNs.
Josef Prchal and Tsewang Tashi, University of Utah, Salt Lake City
Josef T. Prchal – Conflict of Interest
• Advisory Boards:
Agios ‐ “Therapy of Pyruvate Kinase Deficiency”. Not related to this topic
Ctibiopharma–” Phase 2 Study of Pacritinib, JAK2 inhibitor”. Will not discuss here.
Classification of Polycythemias/Erythrocytoses• Primary Polycythemias
• Due to acquired or congenital mutations expressed within hematopoietic progenitors causing increased proliferation/decreased apoptosis
Polycythemia Vera ‐acquiredPrimary Familial and Congenital Polycythemia (PFCP)‐inherited, autosomal dominant
• Secondary PolycythemiasDue to circulating factors driving erythropoiesis, e.g., erythropoietin
Hemoglobin mutations, 2,3 BPG deficiency
• Chuvash Polycythemia—inherited hypoxia sensing defects(& HIF2a and PHD2)
• Acquired Compensatory Physiological “Polycythemia”; in contrast natives of high altitude developing genetic determinants permitting adaptation to extreme hypoxia; Tibetans & Ethiopians versus Andean natives(Quechua and Aymara).
Huntsman Cancer Institute Eighth Annual Hematology Review 109
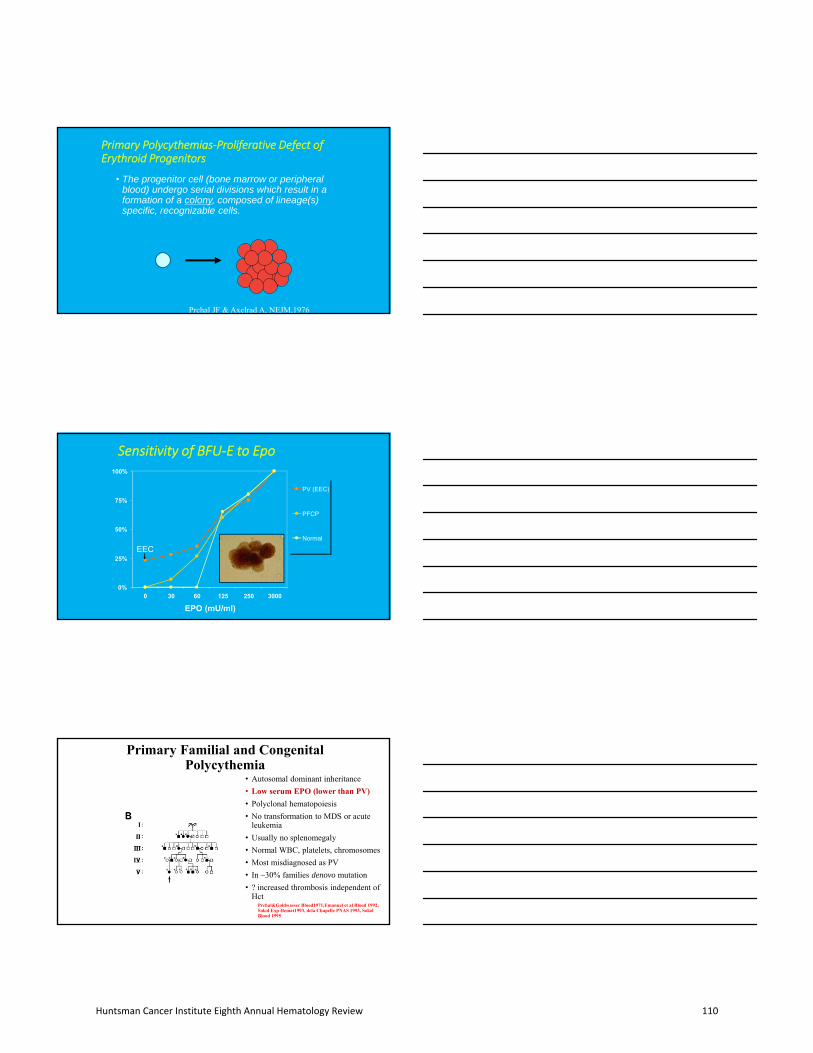
Primary Polycythemias‐Proliferative Defect of Erythroid Progenitors
• The progenitor cell (bone marrow or peripheralblood) undergo serial divisions which result in aformation of a colony, composed of lineage(s)specific, recognizable cells.
Prchal JF & Axelrad A, NEJM,1976
Sensitivity of BFU‐E to Epo
0%
25%
50%
75%
100%
0 30 60 125 250 3000
EPO (mU/ml)
PV (EEC)
PFCP
Normal
EEC
Primary Familial and Congenital Polycythemia
• Autosomal dominant inheritance
• Low serum EPO (lower than PV)
• Polyclonal hematopoiesis
• No transformation to MDS or acute leukemia
• Usually no splenomegaly
• Normal WBC, platelets, chromosomes
• Most misdiagnosed as PV
• In ~30% families denovo mutation
• ? increased thrombosis independent of Hct
Prchal&Goldwasser Blood1971,Emanuel et al Blood 1992, Sokol Exp Hemat1993, dela Chapelle PNAS 1993, SokolBlood 1995
Huntsman Cancer Institute Eighth Annual Hematology Review 110

STAT-5
Erythropoietin Receptor (EPOR)Primary familial and congenital polycythemia (PFCP)
STAT-5 HCPNegative Regulatory Domain
HCP
PO4 PO4
HCP
JAK-2 JAK-2
Secondary Polycythemias/ErythrocytosesHigh oxygen affinity hemoglobins and low 2,3DPG
Hb Oxygen Dissociation CurveHigh and Low Affinity Hbs
• Polycythemia associated Hbs
• Different phenotypes associated w:– Alpha globin– Beta globin– Gamma globin mutations
• Easy screen for from venous blood: N. Agarwal:Int J Med Sci. 2007 Oct 4;4(4):232-6
If you cannot get Hb/O2 dissociation curve
• ANNALS OF INTERNAL MEDICINE: ORIGINAL RESEARCH |1 MAY 1976
• Detection of Mutant Hemoglobins with Altered Affinity for Oxygen: ASimplified Technique
• MARSHALL A. LICHTMAN, M.D.; MARION S. MURPHY, B.S.; JOHN W.ADAMSON, M.D.
pO2(venous) 65
pH(venous) 7.378
sO2(venous) 89.8
p50= 28.32
Original Formula Converted by Excel
Huntsman Cancer Institute Eighth Annual Hematology Review 111

Hypoxia Sensing• EPO expression upregulated by hypoxia ~300
• HRE (Hypoxia Responsive element): oligo 16‐merGCCCTACGTGCTGTCTCACACAGCCTGTCTGACCICTCGACCTACCGGCC
• Many HRE in the genomes
• HIFs (Hypoxia Inducible Factors) ; HIF‐1, HIF‐2, HIF‐3
• Bind to HRE
• HIFs- dimers of hypoxia responsive) a and b
subunits
• HIF-1 ubiquitously expressed
• ~3% of genes controlled by HIF-1
• HIF-2 -tissue specific expression
Hypoxia Sensing
Hypoxia
HIF-1
CGTG
HIF -1HIF-1
EPO
VEGF
Glut1, PGK
Transferrin
…VHL
Normoxia
O2 O2
O2
O2
O2O2
OH
HIF-1
Pro.H
Fe
Degradation
HIF-1
Chuvash Polycythemia
• >100 pts with endemic polycythemia, most previously diagnosed and treated as PV
• Sib-pair analysis • 79 families, 339 siblings• 111 affected siblingsautosomal recessive inheritance
• Polyakovaʼs thesis rejected because of use of genetic methodology in then Soviet Union
• My lab: high EPO, normal p50, no linkage with EPO & EPOR
Lydia AndreyevnaPolyakova, MDDoctoral Thesis, 1977 Chuvash State UniversityCheboksary, Russia
Huntsman Cancer Institute Eighth Annual Hematology Review 112
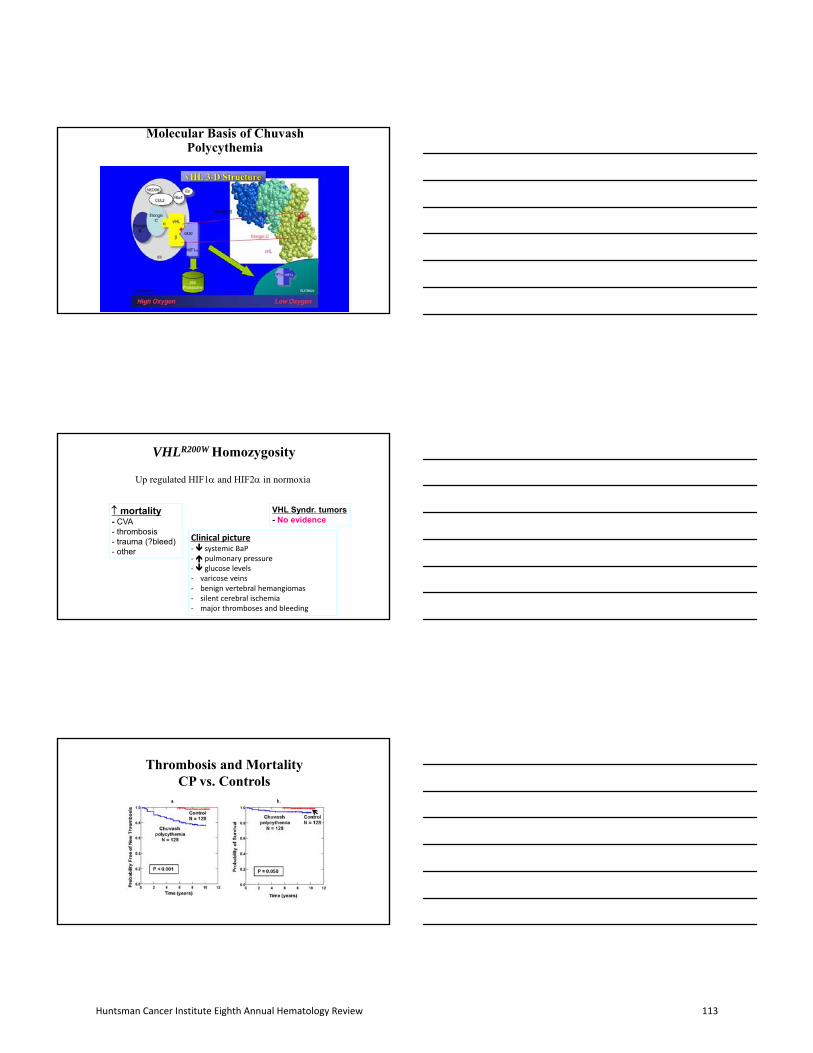
Molecular Basis of Chuvash Polycythemia
VHLR200W Homozygosity
Up regulated HIF1 and HIF2 in normoxia
mortality- CVA- thrombosis- trauma (?bleed)- other
VHL Syndr. tumors- No evidence
Clinical picture‐ systemic BaP‐ pulmonary pressure‐ glucose levels‐ varicose veins‐ benign vertebral hemangiomas‐ silent cerebral ischemia‐ major thromboses and bleeding
Thrombosis and MortalityCP vs. Controls
a. b.
Huntsman Cancer Institute Eighth Annual Hematology Review 113
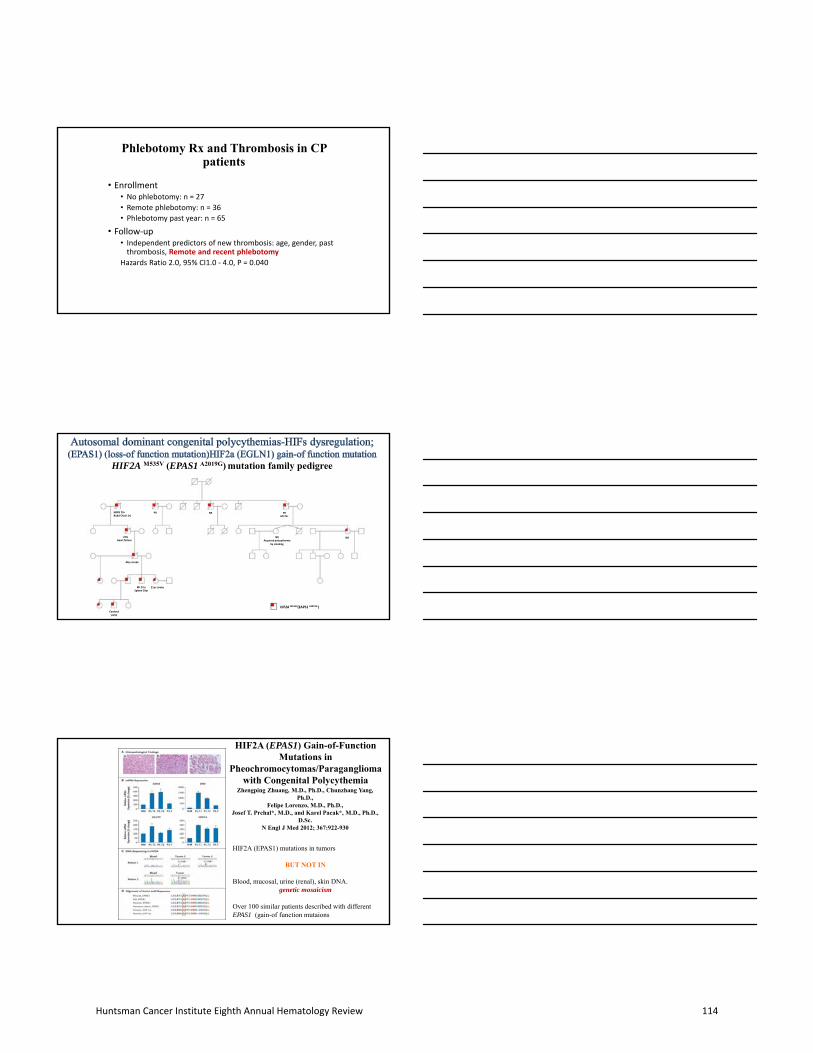
Phlebotomy Rx and Thrombosis in CP patients
• Enrollment• No phlebotomy: n = 27
• Remote phlebotomy: n = 36
• Phlebotomy past year: n = 65
• Follow‐up• Independent predictors of new thrombosis: age, gender, past thrombosis, Remote and recent phlebotomy
Hazards Ratio 2.0, 95% CI1.0 ‐ 4.0, P = 0.040
HIF2A M535V (EPAS1 A2019G) mutation family pedigree
HIF2A M535V(EAPS1 A2019G )
21yr stroke MI 27yr Spleen 29yr
Cerebral palsy
44yr stroke
+70sHeart failure
NR Acquired polycythemia
by smoking
PR NR PR MI 70+
NRPR 70+ Budd‐Chairi (+)
NR
Zhengping Zhuang, M.D., Ph.D., Chunzhang Yang, Ph.D.,
Felipe Lorenzo, M.D., Ph.D., Josef T. Prchal*, M.D., and Karel Pacak*, M.D., Ph.D.,
D.Sc.N Engl J Med 2012; 367:922-930
Peptide Sequencing in Samples Obtained from the Patients.
HIF2A (EPAS1) mutations in tumors
BUT NOT IN
Blood, mucosal, urine (renal), skin DNA. genetic mosaicism
Over 100 similar patients described with different EPAS1 (gain-of function mutaions
HIF2A (EPAS1) Gain-of-Function Mutations in
Pheochromocytomas/Paragangliomawith Congenital Polycythemia
Huntsman Cancer Institute Eighth Annual Hematology Review 114

Classical Myeloproliferative Disorders-Neoplasms(MPN)
• Chronic Myelogenous Leukemia -
increased leukocytes
• Polycythemia Vera- increased
erythrocytes; most common MPD
• Primary Myelofibrosis (PMF)-
variable increased or decreased
blood cells
• Essential Thrombocythemia-
increased platelets
• Acquired mutation in a
hematopoietic stem cell
• Clonal hematopoiesis
• Variable proliferation of
granulocytes, red cells and/or
platelets
• Variable rate of transformation to
incurable acute leukemias
2016 revised WHO classification for Myeloid Malignancies
Acute
Chronic
Acute Myeloid Leukemia
Myelodysplastic Syndromes
MPN/MDS
Myeloid/Lymphoid neoplasms associated with eosinophilia and with PDGFRa,PDGFRb,FGFR1 or
PCM1‐JAK2
Myeloproliferative Neoplasms
Mastocytosis
• Chronic Myeloid Leukemia (CML)• Chronic Neutrophilic Leukemia (CNL)• Polycythemia Vera (PV)• Essential Thrombocythemia (ET)• Primary Myelofibrosis
• Pre‐fibrotic – early stage• Overt fibrotic stage
• Chronic Eosinophilic Leukemia, NOS• MPN ‐ Unclassifiable
Arber D et al, Blood, 2016
Chronic Myelogenous Leukemia
Before Targeted Therapy
• Proliferation of granulocytes
• All stages of granulocyte maturation in peripheral blood
• Platelets may be elevated
• Splenomegaly, frequent
• Almost invariable transformation to fatal acute leukemia; ~2.5yrs after Dx
Huntsman Cancer Institute Eighth Annual Hematology Review 115
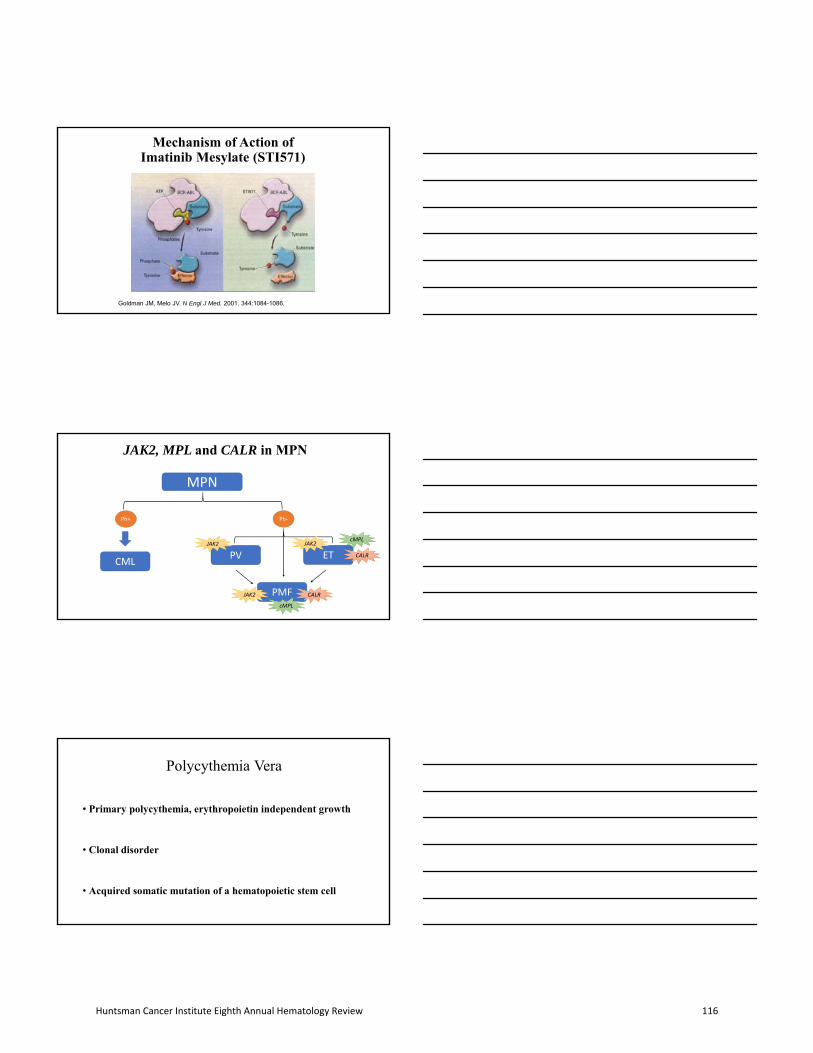
Mechanism of Action of Imatinib Mesylate (STI571)
Goldman JM, Melo JV. N Engl J Med. 2001. 344:1084-1086.
MPN
CMLPV ET
PMF
Ph+ Ph‐
JAK2
JAK2
JAK2cMPL
CALR
CALR
cMPL
JAK2, MPL and CALR in MPN
Polycythemia Vera
• Primary polycythemia, erythropoietin independent growth
• Clonal disorder
• Acquired somatic mutation of a hematopoietic stem cell
Huntsman Cancer Institute Eighth Annual Hematology Review 116
JAK2V617F mutation
• Gene encodes a cytoplasmic tyrosine kinase essential for erythroid maturation
• This mutation causes substitution of phenylalanine for valine at position 617
• The mutation occurs in “the pseudo-kinase (negative regulatory)domain” which leads to a gain of function mutation
• This increases JAK2 activity and leads to cytokine-independent cell line growth
• BUT not specific: 98% of PV, 60% of PMF, 50% E&, and in chronic neutrophilic leukemia and MDS-RS with high platelets
PV ComplicationsSymptoms
Aquagenic pruritusErythromelalgia
ThrombosesCorrelates with WBCNo correlation with increased platelet count.Correlated with JAK2 V617F allelic burden???effect of Hct
MyelofibrosisLeukemia
in most instances JAK2 V617F negative?same clone as PV from clonal pre- JAK2 V617F cells?
Erythromelalgia
Huntsman Cancer Institute Eighth Annual Hematology Review 117

Thrombosis in MPN
Arterial
Venous, including
unusual sites(BCS, PVT,
CVT)
MicrovascularErythromelalgia
HA, visual disturbance, TIA
At initial presentation11-25% in ET pts12 to 39% in PV pts
Risk persists after diagnosisPV:3.8/100 person yrsET:1.9/100 person yrs
Clear impact on prognosis
ET and PV management largely influenced by vascular risk
Falanga et al, Seminars in Thrombosis and Hemostasis 2014
Diagnostic Criteria (WHO) for PV
2016• Major Criteria
1. Hgb > 16.5 g/dl (Hct >49%) in men or 16 g/dl (Hct>48%) in women
2. Bone marrow biopsy – hypercellular for age with panmyelosis and pleomorphic mature megakaryocytes
3. Presence of JAK2 mutations
• Minor Criteria1. Low serum Erythropoietin
• Requires all 3 major or first 2 major + the minor
• Caveat – if sustained erythrocytosis, JAK2 positive and low EPO, then BMmay not be needed
Silver R et al, Blood, 2008
2008• Major Criteria
1. Hgb > 18.5 g/dl in men or 16.5 g/dl in women
2. Presence of JAK2 mutations
• Minor Criteria1. Bone marrow biopsy – hypercellular
for age with panmyelosis2. Low serum Erythropoietin3. Endogenous erythroid colonies
• Requires both major and 1 minor OR first major and 2 minor
Arber D et al, Blood, 2016
Summary – 2016 revision in MPN• Decreased Hb/Hct threshold for PV
• but BM morphology as one of the major criteria
• Addition of CALR mutation for ET and PMF
• Distinction of Prefibrotic PMF as a separate entities
Limitations:
• How to interpret the historical data?
• Overlap between ET and pre‐PMF?
• MDS with fibrosis versus PMF?
Huntsman Cancer Institute Eighth Annual Hematology Review 118
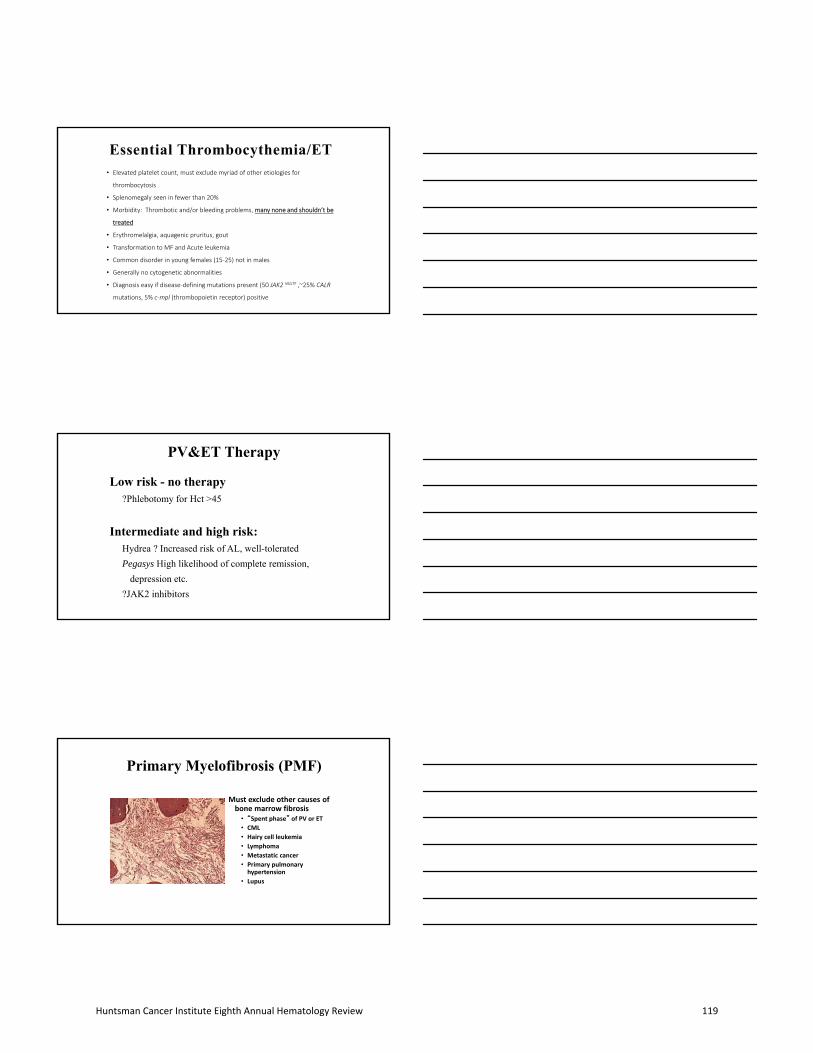
• Elevated platelet count, must exclude myriad of other etiologies for
thrombocytosis
• Splenomegaly seen in fewer than 20%
• Morbidity: Thrombotic and/or bleeding problems, many none and shouldn’t be
treated
• Erythromelalgia, aquagenic pruritus, gout
• Transformation to MF and Acute leukemia
• Common disorder in young females (15‐25) not in males
• Generally no cytogenetic abnormalities
• Diagnosis easy if disease‐defining mutations present (50 JAK2 V617F ,~25% CALR
mutations, 5% c‐mpl (thrombopoietin receptor) positive
PV&ET Therapy
Low risk - no therapy?Phlebotomy for Hct >45
Intermediate and high risk:Hydrea ? Increased risk of AL, well-tolerated
Pegasys High likelihood of complete remission,
depression etc.
?JAK2 inhibitors
Primary Myelofibrosis (PMF)
Must exclude other causes of bone marrow fibrosis
• “Spent phase” of PV or ET
• CML
• Hairy cell leukemia
• Lymphoma
• Metastatic cancer
• Primary pulmonary hypertension
• Lupus
Huntsman Cancer Institute Eighth Annual Hematology Review 119
“Teardrop” Cells/ Dacrocytes
JAK2, MPL and CALR in MPN
Kampfl et al, NEJM, 2013
Huntsman Cancer Institute Eighth Annual Hematology Review 120
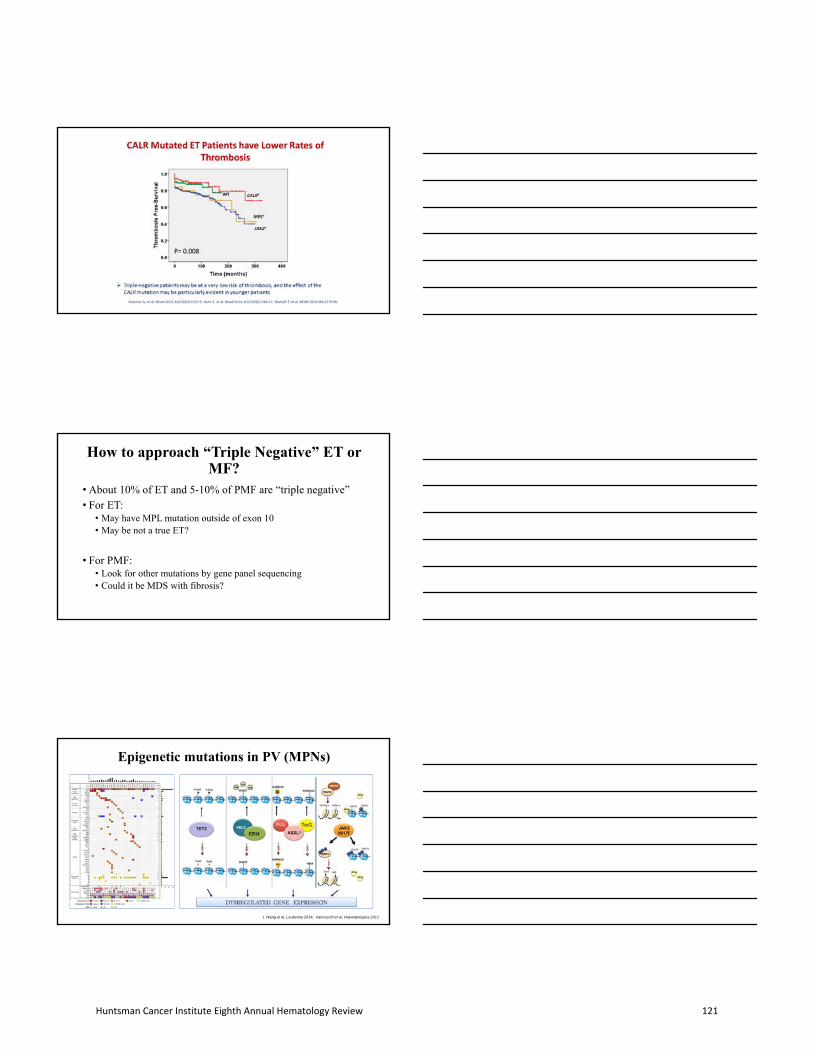
How to approach “Triple Negative” ET or MF?
• About 10% of ET and 5-10% of PMF are “triple negative”
• For ET:• May have MPL mutation outside of exon 10• May be not a true ET?
• For PMF:• Look for other mutations by gene panel sequencing• Could it be MDS with fibrosis?
Epigenetic mutations in PV (MPNs)
L Wang et al, Leukemia 2014; Vannucchi et al, Haematologica 2011
Huntsman Cancer Institute Eighth Annual Hematology Review 121

Diagnostic Criteria (WHO 2016)ET
• Major Criteria1. Sustained platelet count > 450 K/mcl
for atleast 2 months2. Bone marrow: primarily
megakaryocytic proliferation, with very rare reticulin fibrosis (grade 1)
3. No evidence of other myeloid neoplasms
4. Presence of JAK2, CALR or cMPL
• Minor Criterion1. Presence of clonal marker or no
evidence of reactive thrombocytosis
• Requires all major or first 3 major +the minor
Arber D et al, Blood, 2016
Overt‐PMF
• Major Criteria1. Bone marrow: Megakaryocytic atypia
with reticulin fibrosis grade 2 or 3; 2. Exclude other myeloid neoplasm3. Presence of JAK2, CALR, cMPL or other
clonal marker, OR absence of reactivefibrosis
• Minor Criterion1. Anemia (not due to other conditions)2. Leukocytosis > 11 K/mcl3. Leukoerythroblastosis4. Elevated LDH5. Splenomegaly
• Requires all major and 1 minor
ET Subtype: Prefibrotic MF
• Elevated peripheral blood platelet count
• Hypercellular marrow with increased megakaryocytes with atypicalclustering
• No fibrosis, no splenomegaly
• Rapid progression to myelofibrosis
Peripheral blood Bonemarrow
Photomicrographs courtesy Dr. Mohamed Salama
ET vs Prefibrotic PMF vs Overt PMF – what is different?
Barbui et al, JCO 2011; Mudireddy et al, ASH 2016
Huntsman Cancer Institute Eighth Annual Hematology Review 122

Acknowledgments
Thanks to:
Patients and their families
Nurses & Research coordinators
Funding
NIH‐MPD Consortium
Leukemia & Lymphoma Foundation
Huntsman Cancer Institute Eighth Annual Hematology Review 123

Huntsman Cancer Institute Eighth Annual
Hematology Review
Advances in the Treatment of Lymphoma and CLL
Martha Glenn, MD
Huntsman Cancer Institute Eighth Annual Hematology Review 124

Martha Glenn, MD
Feb 24, 2018
Advances in the Treatment of Lymphoma and CLL
Highlights
• CAR T cell therapy for DLBCL
• CLL combinations
• Advanced HL BV for 1st line
Objectives
• CAR T cell therapy for DLBCL
– Understand use of CAR T cell in treatment of relapsed/refractory DLBCL, including limitations and outcomes
• Advanced HL BV for 1st line
– Evaluate results of PhIII Echelon trial
• CLL combinations
– Review results of Ph III MURANO trial for RR CLL
– Compare results of early PhI/II trials of non‐chemotherapy approaches for 1st line and RR CLL
Huntsman Cancer Institute Eighth Annual Hematology Review 125
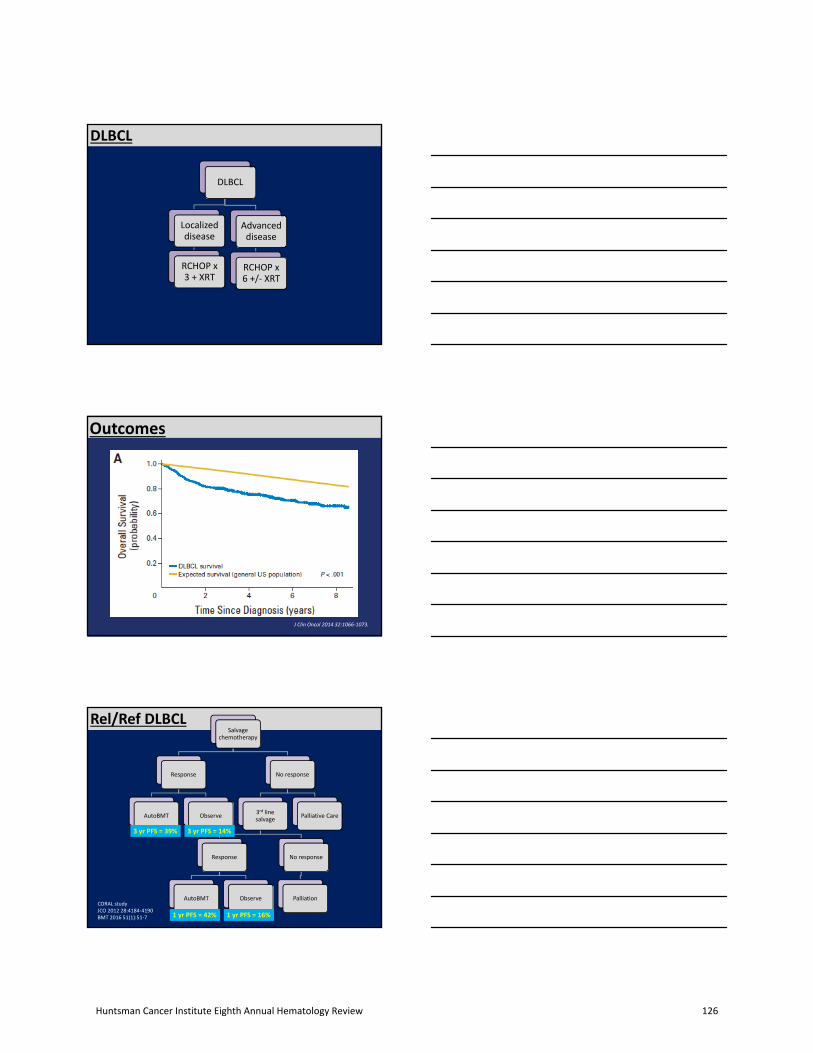
DLBCL
DLBCL
Localized disease
RCHOP x 3 + XRT
Advanced disease
RCHOP x 6 +/‐ XRT
Outcomes
J Clin Oncol 2014 32:1066‐1073.
Rel/Ref DLBCLSalvage
chemotherapy
Response
AutoBMT Observe
No response
3rd line salvage
Response
AutoBMT Observe
No response
Palliation
Palliative Care
3 yr PFS = 39% 3 yr PFS = 14%
CORAL studyJCO 2012 28:4184‐4190BMT 2016 51(1):51‐7 1 yr PFS = 42% 1 yr PFS = 16%
Huntsman Cancer Institute Eighth Annual Hematology Review 126

Rel/Ref DLBCLSalvage
chemotherapy
Response
AutoBMT Observe
No response
3rd line salvage
Response
AutoBMT Observe
No response
Palliation
Palliative Care
3 yr PFS = 39% 3 yr PFS = 14%
CORAL studyJCO 2012 28:4184‐4190BMT 2016 51(1):51‐7 1 yr PFS = 42% 1 yr PFS = 16%
Refractory DLBCL
• “Outcomes in refractory DLBCL: results from theinternational SCHOLAR‐1 Study”
– Blood 2017; 130(16): 1800‐1808
• Outcome from start of salvage treatment forrefractory disease
• Data sources
– 2 PhIII studies for RR DLBCL
• CORAL and LY.12
– 2 observational cohorts
• MDA for relapsed DLBCL
• Iowa/Mayo lymphoma database
Refractory DLBCL
Huntsman Cancer Institute Eighth Annual Hematology Review 127

Selection Bias in RR DLBCL trials
Sarah C. Rutherford, and John P. Leonard Blood 2017;130:1778-1779
©2017 by American Society of Hematology
Refractory DLBCL: Scholar‐1 Study
• Benchmarking validity for prospective trials
– Median age = 55 yr
– Male = 64%
– ECOG 1‐2 = 73%
– Stage III/IV = 72%
– 28% primary refractory
– 49% refractory to salvage
– 22% early relapse after auto BMT
Refractory DLBCL: Scholar‐1 Study
Outcome
ORR 26%
CR 7%
PR 18%
Med OS 6.3 mos
2 yr OS 20%
CR then auto Med OS >6 yrs
Huntsman Cancer Institute Eighth Annual Hematology Review 128

Refractory DLBCL: OS
http://www.headaround.com/car‐t‐cell‐immunotherapy‐diagram/
antiCD19 CAR T cell products
Names DevelopersCompany
Co‐stim signalVector
Trial Names FDA approval
KTE‐C19Axicabtagene ciloleucel(axi cel)YescartaNEJM 2017 377:2531‐44
NCIKite now Gilead
CD28Retroviral
“ZUMA1” Ref DLBCL and tL
CTL019TisagenleucleucelKymriahNEJM 2017 377:2545‐54
UnivPennNovartis
4‐1BBLentiviral
“Juliet” B ALL (< 26 yo)
JCAR017Lisocabtagene maraleucel(liso cel)Blood 2017 abst 581
FHCRC/MSKCCJUNO now Celgene
4‐1BBLentiviral
“TranscendNHL”
Huntsman Cancer Institute Eighth Annual Hematology Review 129
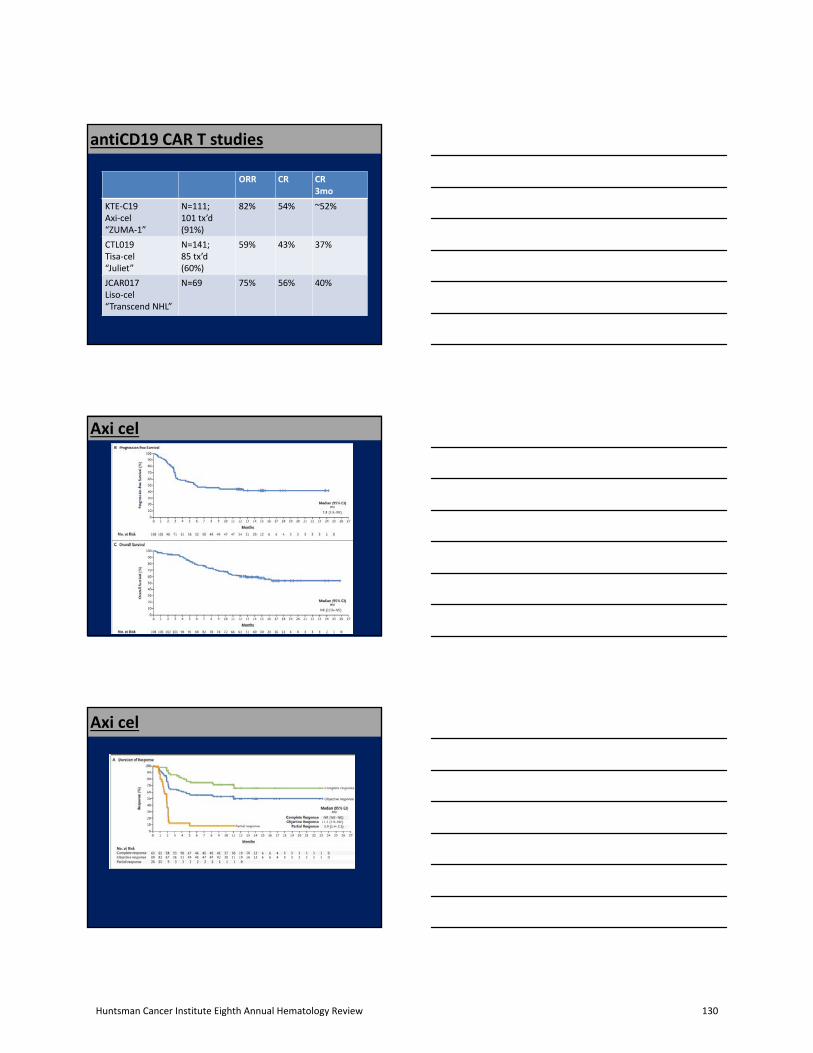
antiCD19 CAR T studies
ORR CR CR3mo
KTE‐C19Axi‐cel“ZUMA‐1”
N=111; 101 tx’d(91%)
82% 54% ~52%
CTL019Tisa‐cel“Juliet”
N=141;85 tx’d(60%)
59% 43% 37%
JCAR017Liso‐cel“Transcend NHL”
N=69 75% 56% 40%
Axi cel
Axi cel
Huntsman Cancer Institute Eighth Annual Hematology Review 130

Tisa cel
Tisa cel
JCAR
Huntsman Cancer Institute Eighth Annual Hematology Review 131

• CRS– Fever, hypotension, tachycardia, hypoxia
• Neurotoxicity– Mild cognitive dysfunction to encephalopathy– Early signs: difficulty with word finding, calculation, handwriting
• Cytopenias– Neutropenia, anemia, thrombocytopenia– May be prolonged in 20‐30%
• Neutropenic Fever
Toxicity
ToxicityApprox RateGr3/4
Onset
CRS 35‐95%5‐17%
D2‐3~5 days
Neurotoxicity 20‐64%13‐34%
D5‐7~10+ days
Cytopenias ANC 41‐93%Hct 38‐66%Plts 29‐58%
Neutropenic Fever 36%
Tocilizumab given in 10‐45%Steroids in 0‐27%CRS/NT seen most in Axi‐cel
• Axi cell $373,000• CTL019 $475,000• Estim $1,000,000 per pt treated
“Health systems and Financial Implications of Offering CAR T Therapies” Silver ASH2017 • Mark up 110% (for in‐pt infusion; no toxicitymanagement)– Total charge $524,300
• Medicare payment = $86,836
• Mark up 400%– Total charge $1,606,000
• Medicare payment = $303,176
Cost
Huntsman Cancer Institute Eighth Annual Hematology Review 132

Refractory DLBCL: OS
Very rough estimate CART tx
Historical benchmark
• CR at 3 months seems to predict for durableresponses
– Roughly 40% reach this point
• Setting realistic expectations
– Selection bias
• Slower disease growth
• Excellent health despite RR DLBCL– ECOG 0‐1
– Expensive
– Considerable toxicity
CAR T Tx for Ref DLBCL: Summary
Adv’d HL
• ABVD x 6 cycles– 5 yr PFS = 53%; 5 yr OS = 66%
• EscBEACOPP x 6– 5yr PFS 89; 5 yr OS 95%
• Response adapted approach– ABVD PET2 neg, ABVD or AVD x 4
• 3 yr PFS 84%; 3 yr OS 97%
– ABVD PET2 POS, escBEACOPP x4• 3 yr PFS 67%; OS 88%
Huntsman Cancer Institute Eighth Annual Hematology Review 133

Brentuximab Vedotin Mechanism of Axn
Brentuximab vedotin (SGN-35) ADC
ADC binds to CD30
MMAE disruptsMicrotubule network
ADC-CD30 complex traffics to lysosome
MMAE is released
Apoptosis
G2/M cellcycle arrest
anti-CD30 monoclonal antibodyprotease-cleavable linkermonomethyl auristatin E (MMAE), potent antitubulin agent
Brentuximab Vedotin Mechanism of Axn
Brentuximab vedotin (SGN-35) ADC
ADC binds to CD30
MMAE disruptsMicrotubule network
ADC-CD30 complex traffics to lysosome
MMAE is released
Apoptosis
G2/M cellcycle arrest
anti-CD30 monoclonal antibodyprotease-cleavable linkermonomethyl auristatin E (MMAE), potent antitubulin agent
Single agent efficacy in RR HL post AutoBMT:CR 34%ORR 75%
Adv’d HL: ECHELON‐1
• “Brentuximab Vedotin with Chemotherapy forStage III or IV Hodgkin’s Lymphoma”
– Connors et al NEJM 2018: 378:331‐44
RANDOMIZATION
AAVD x 6
ABVD x 61334 pts
Primary Endpoint:2 yr PFS
Huntsman Cancer Institute Eighth Annual Hematology Review 134
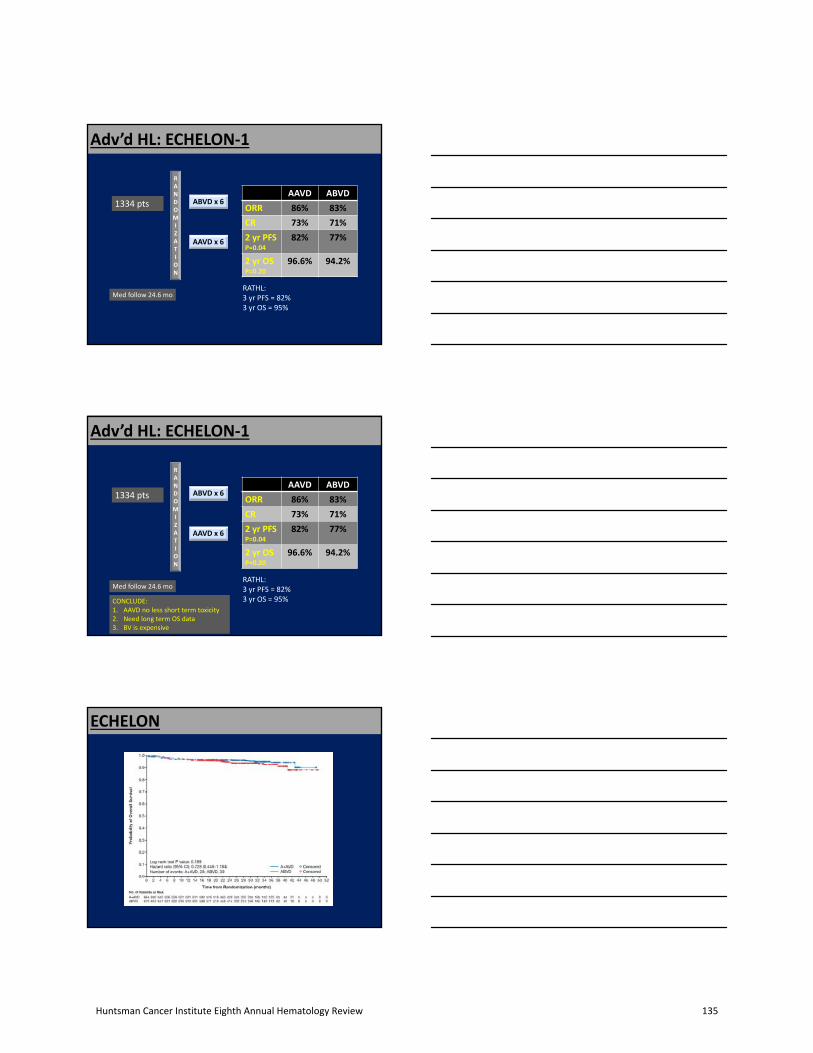
Adv’d HL: ECHELON‐1
RANDOMIZATION
AAVD x 6
ABVD x 61334 pts
Med follow 24.6 mo
AAVD ABVD
ORR 86% 83%
CR 73% 71%
2 yr PFSP=0.04
82% 77%
2 yr OSP=0.20
96.6% 94.2%
RATHL:3 yr PFS = 82%3 yr OS = 95%
Adv’d HL: ECHELON‐1
RANDOMIZATION
AAVD x 6
ABVD x 61334 pts
Med follow 24.6 mo
AAVD ABVD
ORR 86% 83%
CR 73% 71%
2 yr PFSP=0.04
82% 77%
2 yr OSP=0.20
96.6% 94.2%
RATHL:3 yr PFS = 82%3 yr OS = 95%CONCLUDE:
1. AAVD no less short term toxicity2. Need long term OS data3. BV is expensive
ECHELON
Huntsman Cancer Institute Eighth Annual Hematology Review 135

Chronic lymphocytic leukemia
• MURANO trial RR CLL VR vs BR
• Venetoclax + Ibrutinib RR CLL
• Venetoclax + Ibrutinib + ObinutuzumabUpfront
• Venetoclax + Obinutuzumab Upfront
• “VR is superior to BR in RR CLL—results frominterim analysis of PhIII MURANO study”
– Seymour et al ASH2017 LBA‐2
RANDOMIZATION
BR x 6
VR x 6 389 ptsRR CLL V 2 yr
max
Primary Endpoint:Investigator Response
Assessement
Med follow 24 mo
RR CLL: MURANO
RR CLL: MURANO
ORR CR
VR 93% 26%
BR 68% 8%
OS benefit:HR 0.48 (CI 0.25‐0.90)
(P<0.0001)
Huntsman Cancer Institute Eighth Annual Hematology Review 136

RR CLL: Venetoclax/Ibrutinib
• “Initial Results of IBR + VEN in RR CLL(CLARITY): High rates of OR, CR and MRDeradications following 6 months of therapy”
– Hillmen et al ASH 2017
TX stopped if MRD neg x as long as took to get MRD
negIBR + VENIBR
X 2 mo
Primary Endpoint:BM MRD p 12 mo
MRD assess6, 12,24 mo
0 2 8
RR CLL: Venetoclax/Ibrutinib
• “Initial Results of IBR + VEN in RR CLL(CLARITY): High rates of OR, CR and MRDeradications following 6 months of therapy”
– Hillmen et al ASH 2017
IBR + VENIBR
X 2 mo
Primary Endpoint:BM MRD p 12 mo
MRD assess6, 12,24 mo
0 2 8
25 pts 50 pts TX stopped if MRD neg x as long as took to get MRD
neg
RR CLL: Venetoclax/Ibrutinib
IBR + VENIBR
X 2 mo
Primary Endpoint:BM MRD p 12 mo
MRD assess6, 12,24 mo
0 2 8
25 pts 50 pts TX stopped if MRD neg x as long as took to get MRD
neg
• ORR = 100%
• CR = 60%
• MRD neg = 28%
Huntsman Cancer Institute Eighth Annual Hematology Review 137
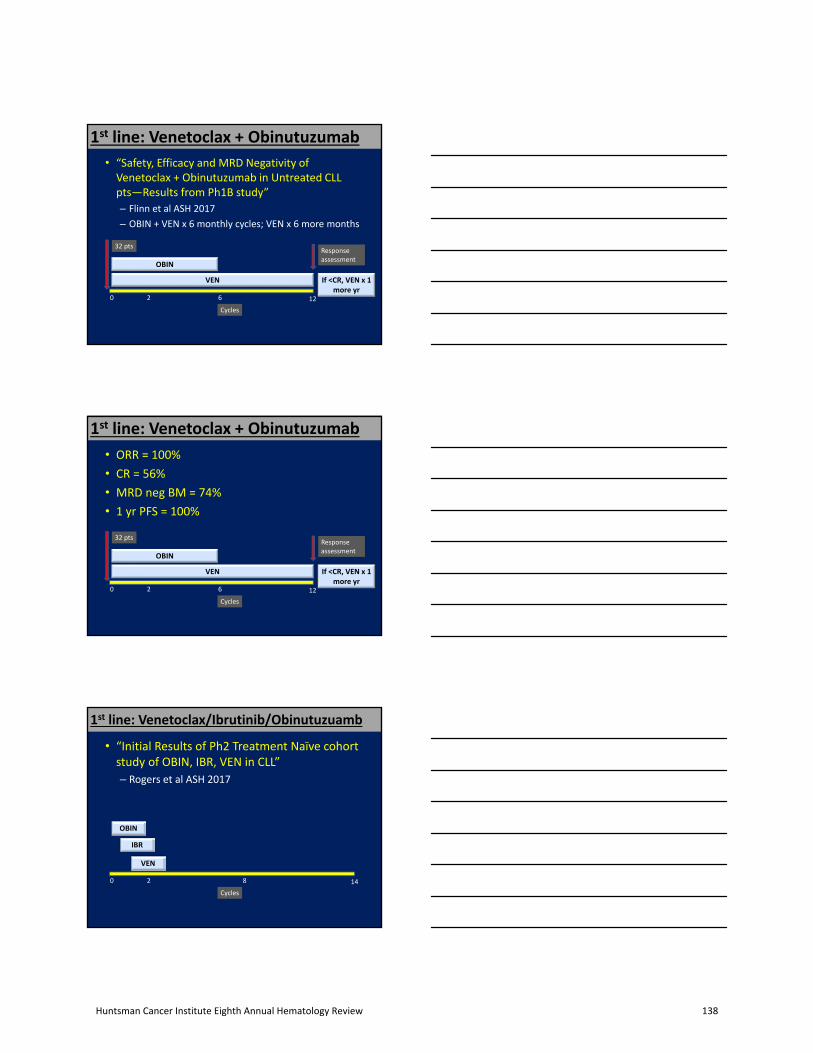
1st line: Venetoclax + Obinutuzumab
• “Safety, Efficacy and MRD Negativity ofVenetoclax + Obinutuzumab in Untreated CLLpts—Results from Ph1B study”
– Flinn et al ASH 2017
– OBIN + VEN x 6 monthly cycles; VEN x 6 more months
12
VEN
OBIN
Cycles
0 2 6
If <CR, VEN x 1 more yr
Response assessment
32 pts
1st line: Venetoclax + Obinutuzumab
• ORR = 100%
• CR = 56%
• MRD neg BM = 74%
• 1 yr PFS = 100%
12
VEN
OBIN
Cycles
0 2 6
If <CR, VEN x 1 more yr
Response assessment
32 pts
1st line: Venetoclax/Ibrutinib/Obinutuzuamb
• “Initial Results of Ph2 Treatment Naïve cohortstudy of OBIN, IBR, VEN in CLL”
– Rogers et al ASH 2017
14
IBR
VEN
OBIN
Cycles
0 2 8
Huntsman Cancer Institute Eighth Annual Hematology Review 138

1st line: Venetoclax/Ibrutinib/Obinutuzuamb
• “Initial Results of Ph2 Treatment Naïve cohortstudy of OBIN, IBR, VEN in CLL”
– Rogers et al ASH 2017
14
IBR
VEN
OBIN
Cycles
0 2 8
Response assessment23 pts
25 pts
14
IBR
VEN
OBIN
Cycles
0 2 8
Response assessment23 pts
25 pts
• ORR = 100%
• CR = 50%
• MRD neg = 58%
1st line: Venetoclax/Ibrutinib/Obinutuzuamb
14
IBR
VEN
OBIN
Cycles
0 2 8
Response assessment23 pts
25 pts
• ORR = 100% (100%)
• CR = 50% (56%)
• MRD neg = 58% (74%)
1st line: Venetoclax/Ibrutinib/Obinutuzuamb
Huntsman Cancer Institute Eighth Annual Hematology Review 139

CLL‐‐summary
• RR CLL
– Venetoclax + Rituximab improves RR, PFS and OS over BR after previous CIT
• Venetoclax approval is for 17pDEL RR CLL currently
– Venetoclax + Ibrutinib with response (MRD) adapted discontinuation is promising
• 1st line
– Venetoclax + Obinutuzumab is promising
• Unclear that adding IBR adds increased efficacy
Current clinical trials at HCI• FL/iNHL
– Ph1/2 intratumoral injection of G100 (TLR4 agonist) +/‐ pembrolizumab– IMMU‐114 (humanized anti‐HLA DR Ab) Ph1
• MCL– Ibrutinib maintenance after frontline tx– IMMU‐114– Ibrutinib + selinexor (Selective inhibitor of Nuclear export)
• DLBCL– IMMU‐114– Ibrutinib + selinexor– SGN CD19B (anti‐CD19 ADC with DNA‐crosslinking drug payload SGD‐
1882))– Nivolumab + IDO inhibitor Ph I– BET (transcriptional activator) inhibitor Ph I/II (in MYC de‐regulated)
lymphoma)
• Information/Referrals – New pt coordinator: Laura Peay 801‐585‐6906– http://healthcare.utah.edu/huntsmancancerinstitute/clinical‐
trials/find‐clinical‐trials‐at‐hci/
Huntsman Cancer Institute Eighth Annual Hematology Review 140





























