Embed Size (px)
Citation preview
HUN 3403 Wk3 D2b
Chapter 15 Adolescent Nutrition:Conditions and Interventions
Introduction
• Behaviors & nutrition concerns impacting significant numbers of youth are addressed including:– Overweight & obesity– Competitive sports– Substance use & abuse– Eating disorders– Hypertension & hyperlipidemia– Chronic health conditions
Overweight and Obesity
• Prevalence of overweight adolescents has nearly doubled during the past two decades
• Factors most likely to be causes of increase in overweight and obesity– Environmental factors– Genetic factors
Overweight and Obesity
• Additional factors contributing to the increase include:– Having one or more overweight parents– From a low income family– African American, Hispanic, American Indian or
Native Alaskan descent– Having a condition that limits mobility– Inadequate physical activity– Diets high in calories, sugars, & fat

Assessing Weight Status
• BMI for age & gender is used to assess weight status– BMI ≥85th to <95% are “overweight”– BMI ≥95% are “obese”– Wt status assessed by plotting growth
curve charts on the next slide
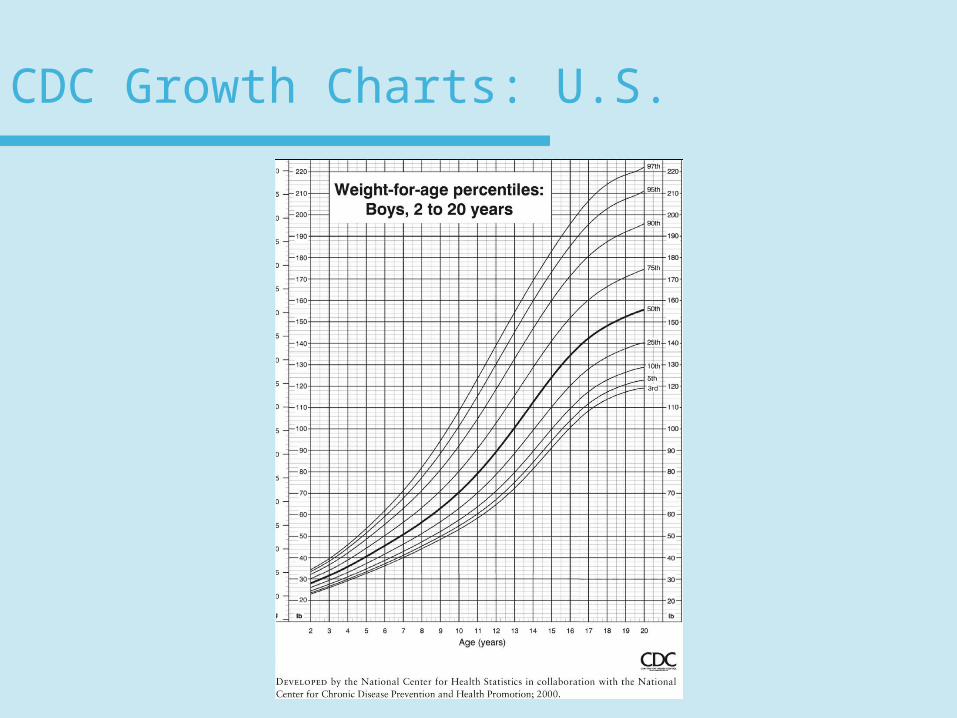
CDC Growth Charts: U.S.
Health Implications of Adolescent Overweight
• Range of complications associated with being overweight include:– Hypertension– Dyslipidemia– Insulin resistance or type 2 diabetes
mellitus– Sleep apnea– Hypoventilation disorders
Health Implications of Adolescent Overweight
• Range of complications associated with being overweight include (cont.):– Orthopedic problems– Hepatic disease– Body image disturbances– Low self esteem
Assessment and Treatment of Adolescent Overweight and Obesity
• Screen all adolescents for wt-for-ht annually
• Those at-risk for overweight require in-depth medical assessments
• Recommendations based on physical growth & presence of medical complications
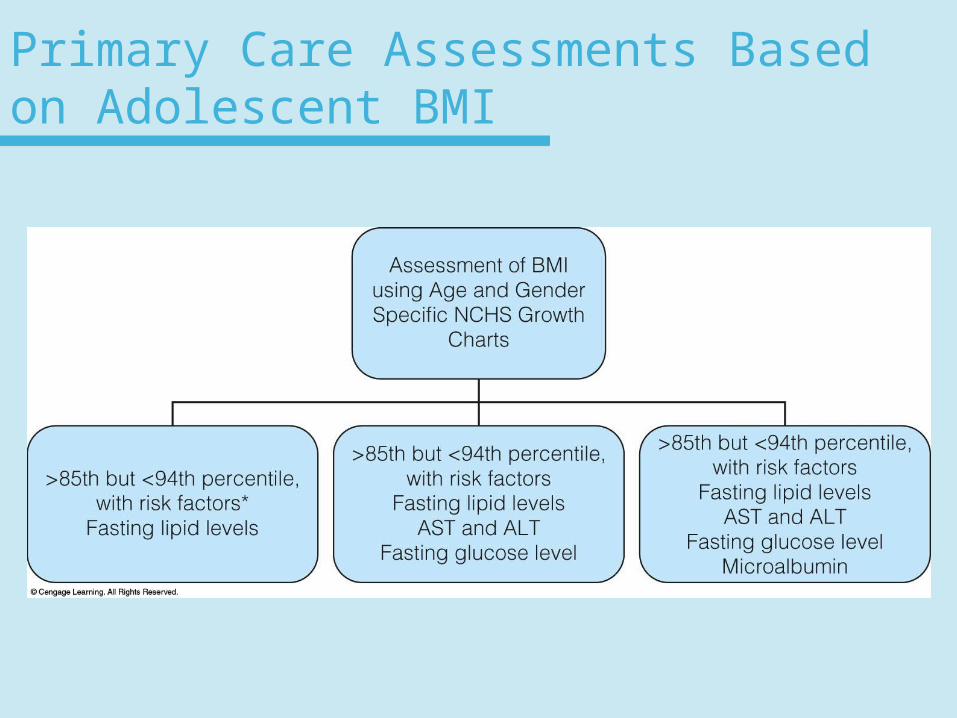
Primary Care Assessments Based on Adolescent BMI
National Guidelines for Weight Management Therapy
1. Prevention plus– BMI >85th but <95th without co-morbidity
conditions– Level of treatment builds upon
• Basic nutrition• Physical activity
– Goal• Promote health• Prevent disease
National Guidelines for Weight Management Therapy
2. Structured weight management– Same behaviors as stage 1– More structured
• Screen time is limited to <1 hour per day• Emphasize nutrient-dense foods• Minimize energy-dense foods
National Guidelines for Weight Management Therapy
3. Comprehensive multidisciplinary intervention
– Same behavioral goals as stage 2– More structured eating– More structured physical activity plan– Designed to lead to negative caloric
balance
National Guidelines for Weight Management Therapy
4. Tertiary care intervention– Appropriate with severely obese youth or those
who have significant, chronic co-morbidity conditions
– Level of treatment provided through a tertiary wt management center
– Diet and activity counseling with behavior modifications
National Guidelines for Weight Management Therapy
4. Tertiary care intervention (cont.)– Treatments may include
• Meal replacement• A very low energy diet• Medication• Surgery may be implemented
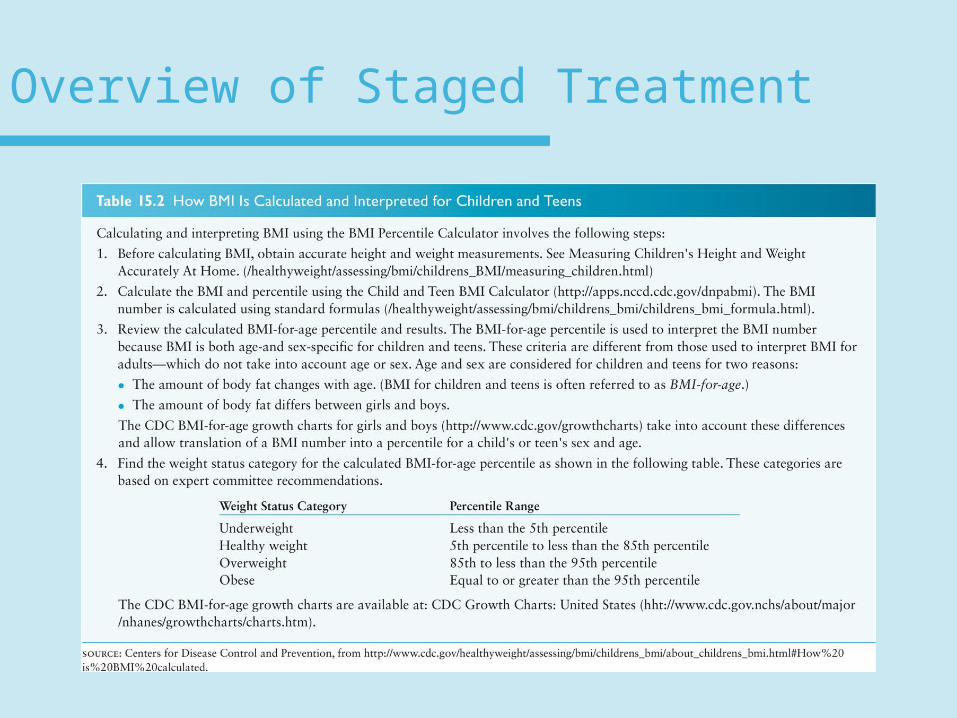
Overview of Staged Treatment
Management of Severely Obese Adolescents
• Rapid weight loss may be medically necessary
• Intensive medical supervision required with the following:– Very-low-calorie diets or protein-sparing
modified fasts – Appetite suppressants or other drugs– Bariatric surgery
Bariatric Surgery and Severely Obese Adolescents
• Performed only if obesity has medical comorbidities
• Adolescent must have completed growth spurt and have either:– BMI >35 with major complications or– BMI >50 with minor complications
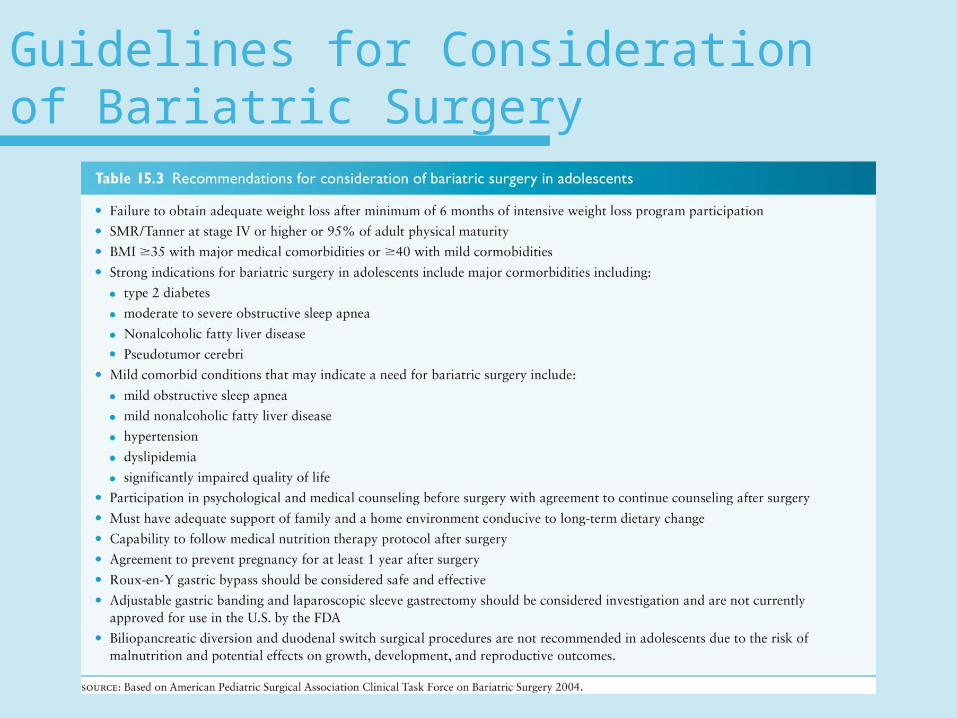
Guidelines for Consideration of Bariatric Surgery
Supplement Use
• Vitamin & Mineral Supplements:• National data - >1/3 adolescents use Vitamin-
Mineral supplements• Most common supplements are
– Vitamin C – Calcium – Iron– Vitamin E– B-vitamin complex
Supplement Use
• Vitamin & Mineral Supplements:• Prevalence of supplement use:
– Positively correlated with • Household income• High food-security status• Some form of health insurance• Parental education
– Adolescents who take supplements tend to consume a more nutritionally adequate diet than those who don’t
Supplement Use
• Herbal Remedies:• Few data available on herbal use• Reasons for taking them include:
– Weight loss– Treatment of ADD – To increase energy and stamina
• More studies needed on herb use since many herbs have potentially dangerous side effects
Supplement Use
• Ergogenic Supplements Used by Teens– 4% of adolescents report taking illegal steroids
• Most common in males• Use peaks during 9th grade • May be taken orally, injected, or as a patch• Few high school athletic programs test
athletes for ergogenic supplement use
Anabolic-androgenic Steroids
• Used to increase LBM & strength• Linked to infertility, hypertension, physeal
closure, depression, aggression, & increased risk of atherosclerosis– Two commonly used steroids that are precursors
of testosterone & estrogen are:• Androstenedione (Andro)— controlled substance• DHEA (Dehydroepiandrosterone) widely available as
supplements
Anabolic-androgenic Steroids
• Claims for taking DHEA and Andro
• While not scientifically proven, claimed to:– Reduce body fat– Decrease insulin resistance– Increase immune system function & LBM– Decrease risk of osteoporosis
Anabolic-androgenic Steroids
• Risks of taking DHEA and Andro
• Possible Side effects:– Gynecomastia (breast enlargement)– Prostate enlargement– Hirsuitism (facial hair in females)
Growth Hormone
• Benefit of growth hormone:– Decrease subcutaneous fat– Strengthen ligaments and tendons
• Side effects include:– Physeal closure– Hyperlipidemia– Glucose intolerance– Myopathy
Creatine
• Sold as supplement to increase LBM
• Naturally formed in liver & kidneys
• Main dietary sources are meats
• Studies show mixed results on benefits
• Side effects are numerous
• Chronic use may be associated with renal damage
Ephedra
• Was banned as OTC supplement in 2004
• Does increase BMR but no known benefits to athletic performance
• Side effects include cardiac arrhythmia, hypertension, increased risk of myocardial infarction, cerebral vascular accidents, & death
Nutrition for Adolescent Athletes
• More than half of U.S. adolescents report playing one or more sports– 62% of males– 50% of females
• Nutrition concerns include:– Fluid & hydration– Carbohydrate loading – High-protein diets
Nutritional Considerations for Physically Active Adolescents
• High levels of activity combined with growth & development increase needs for energy, protein & certain vitamins & minerals
• Nutrient needs higher during intense training & competition seasons
• Monitor changes in body weight to assess for adequate energy and nutrient intake
Considerations for Assessing Nutrient Needs for Adolescent Athletes
1. What sport(s) are engaged in & duration of competition season(s)?
2. What is the level of competition? (Recreational, competitive, or highly competitive)
3. What kind of training does adolescent engage in?
Considerations for Assessing Nutrient Needs for Adolescent Athletes
4. Does the athlete typically sweat profusely or lose body weight during competition?
5. Does athlete follow a special diet or take supplements to improve athletic performance? The type, amount and frequency of supplement use should be noted and counseling provided as necessary.
Nutritional Considerations for Physically Active Adolescents
• Competitive athletes may need 500-1500 additional calories per day
• Protein should supply no more than 30% of calories in the diet
• Special concern for vegetarian athletes or restricted caloric intake to maintain a particular weight
Dietary Recommendations for Adolescent Athletes
• Follow MyPlate guidelines– May need upper limit of food group servings
because of increased energy needs
• Eat pre-event meal at least 2-3 hours prior to exercise
• Post-event meals should contain 400-600 calories & be high in complex carbs & adequate non-caffeinated fluids
Dietary Recommendations for Adolescent Athletes
• Avoid foods high in fat, protein & dietary fiber for at least 4 hours before event
• Increased risk of bone fractures make adequate calcium intake important
Fluids and Hydration
• Reasons adolescents are at risk for dehydration:– Young adolescents do not regulate body
temperatures well– Ignore physiological signs of fluid loss– May be unaware of need for fluids
• All athletes should be counseled on fluid needs
Fluids and Hydration
• Fluid recommendations:– 6-8 oz fluids prior to exercise– 4-6 oz every 15-20 minutes during activity– ≥8 oz following exercise– Not more than 16 oz in 30 minutes to avoid
nausea
Special Dietary Practicesof Adolescent Athletes
• Carbohydrate loading– Used with endurance athletes such as
distance runners– Consists of high-carb diet to increase
glycogen stores combined with resting prior to athletic event
Special Dietary Practices of Adolescent Athletes
• High-protein diets– May consist of 3-4 times the DRI– Should be discouraged because:
• Protein foods typically high in total & saturated fats
• Protein & fat may delay digestion & absorption, limiting total energy available for activity
• More water required for protein breakdown which increases dehydration risk
Substance Use
• Use of substances can affect nutritional status– Tobacco increases Vitamin C needs– Alcohol replaces nutritious foods and
beverages– Illicit drugs may increase risk for
disordered eating behaviors
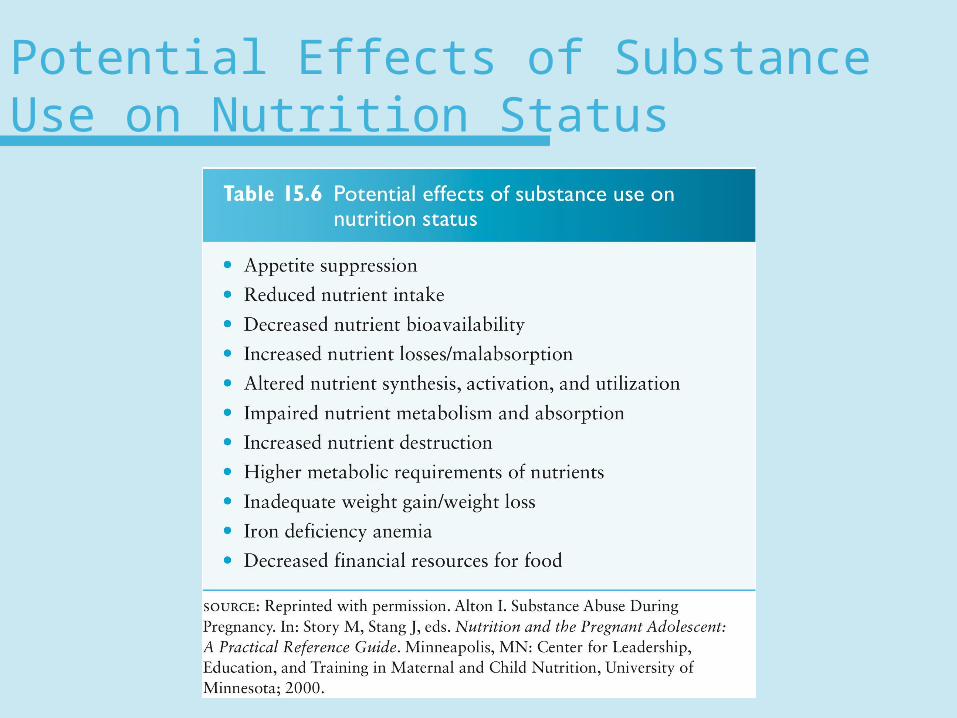
Potential Effects of Substance Use on Nutrition Status
Iron-Deficiency Anemia
• Iron-deficiency anemia is the most common nutritional deficiency
• Risk factors for iron deficiency:– Rapid growth intake iron- or vitamin C-rich foods– Vegan diets– Caloric restriction, meal skipping– Participation in strenuous or endurance sports– Heavy menstrual bleeding
Iron-Deficiency Anemia
• Effects of iron deficiency on adolescents:– Delayed or impaired growth & development– Fatigue– Increased susceptibility to infection– Depressed immune system– Impaired physical performance & endurance– Increased susceptibility to lead poisoning
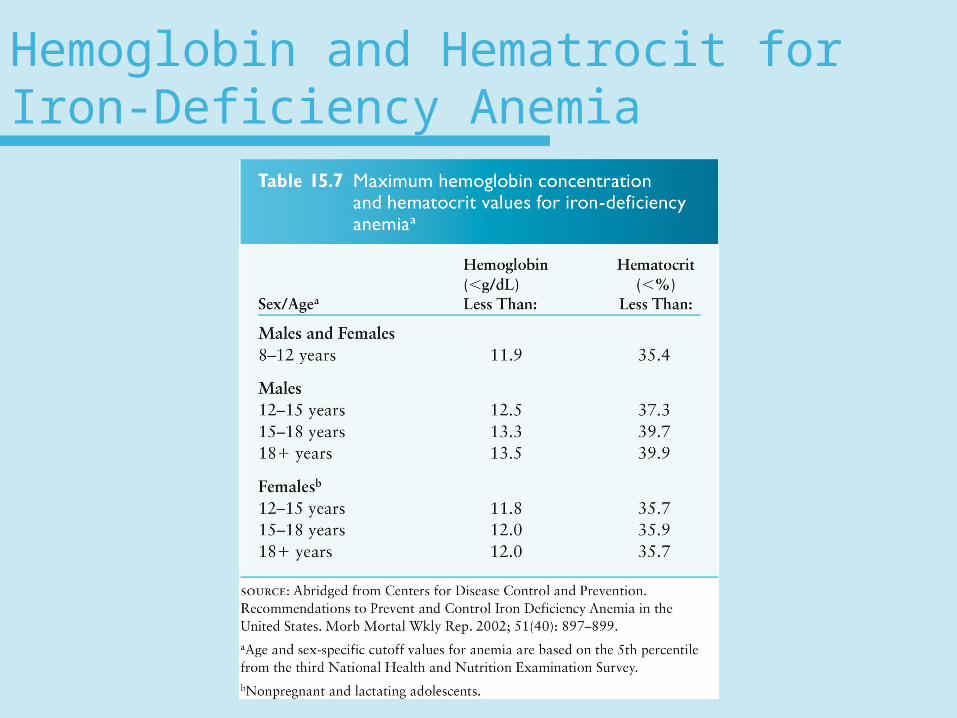
Hemoglobin and Hematrocit for Iron-Deficiency Anemia
Treatment of Iron-Deficiency Anemia
• Treatment includes:– Increase intake of foods rich in iron &
vitamin C– Iron supplements
• Under age 12—60 mg/day• Over age 12—60 (males) to 120 (females)
mg/day
Side Effects of Iron Supplements
• Common side effects include constipation , nausea, cramps– Reduce side effects by
• Taking small, frequent doses• Take with meals
– Factors iron absorption include • Calcium supplements • Dairy products• Coffee, Tea• High-fiber foods
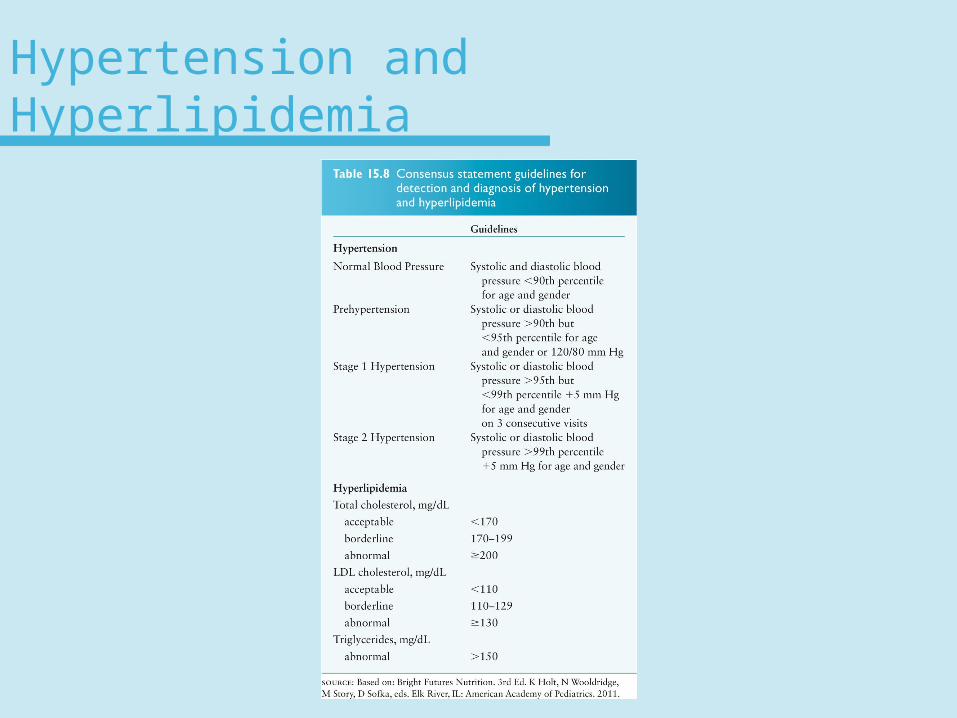
Hypertension and Hyperlipidemia
Risk Factors for Hypertension
• Family history of hypertension
• High sodium intake
• Overweight
• Hyperlipidemia
• Inactive lifestyle
• Tobacco use
Nutrition Counseling for Hypertension
• Decrease sodium intake• Limit fat to 30% of calories• Consume adequate fruits, vegetables,
whole grains, & low-fat dairy• Weight loss if overweight• Dietary recommendations should be
encouraged even if meds are prescribed
Hyperlipidemia
• ~1 in 4 adolescents have elevated cholesterol• Risk factors include:
– Family history– Cigarette smoking– Overweight– Hypertension– Diabetes– Physically inactive
Dietary Recommendations to Reduce Hyperlipidemia
• <35% calories from total fat
• <10% calories from saturated fat
• Cholesterol intake ≤300 mg/day
• Adequate fruits, vegetables, grains, & low-fat dairy
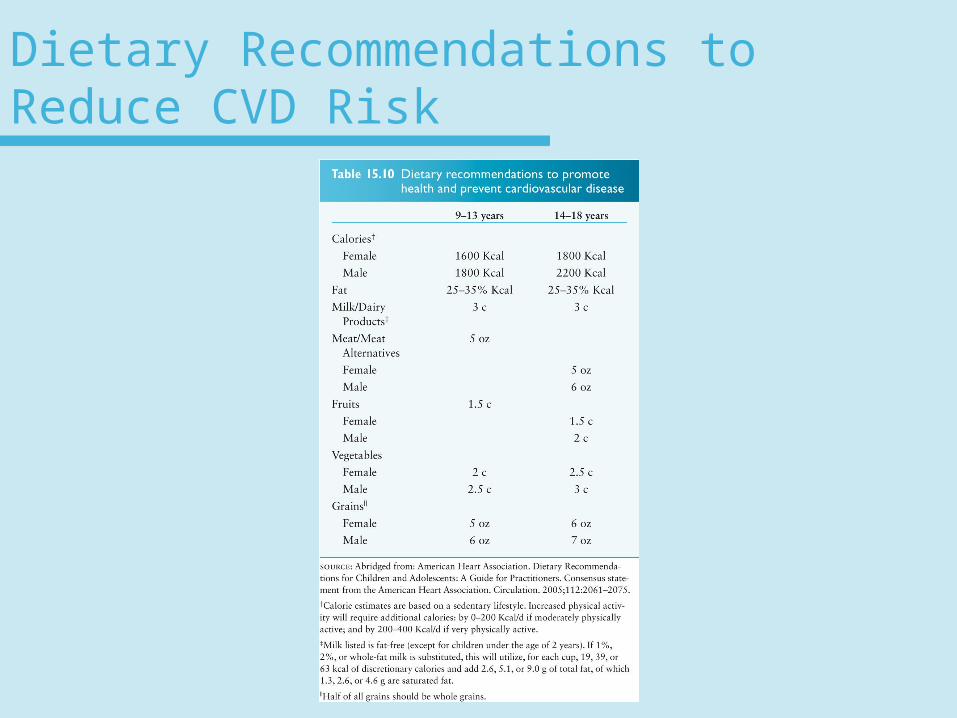
Dietary Recommendations to Reduce CVD Risk
Children & Adolescents with Chronic Health Conditions
• About 18% of children & adolescents have a chronic condition or disability
• Condition may put person at risk for nutrition problems related to:– Altered consumption, digestion or
absorption – Biochemical imbalances– Psychological stress– Environmental factors
Children & Adolescents with Chronic Health Conditions
• Common nutrition problems with special health care needs:– Altered energy and nutrient needs– Delayed growth– Oral-motor dysfunction– Elimination problems– Drug/nutrient interactions– Appetite disturbances– Unusual food habits– Dental caries, gum disease
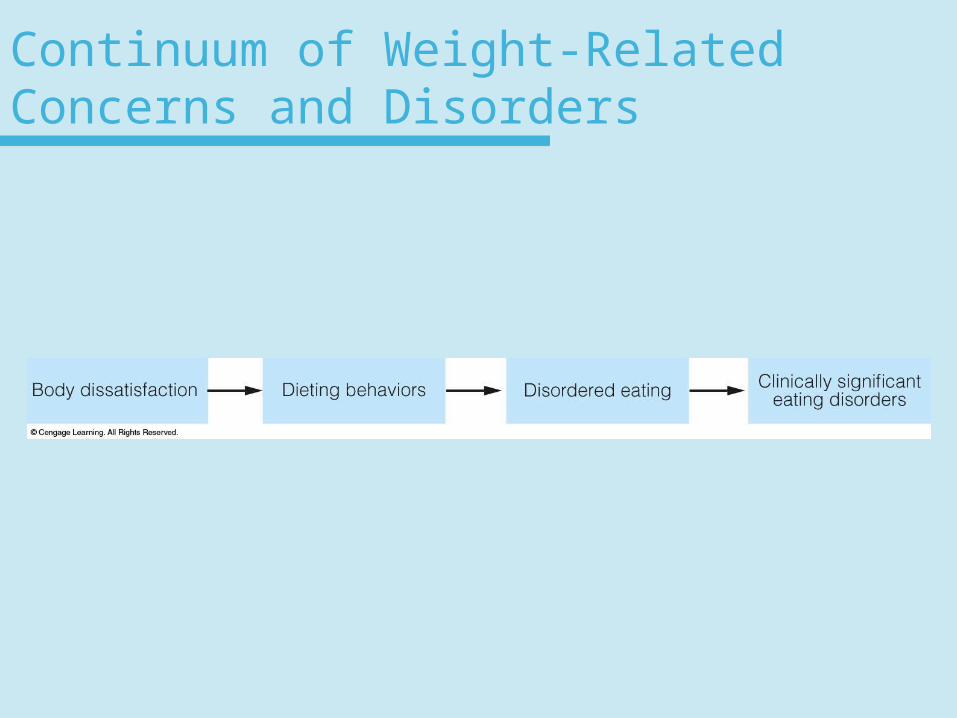
Continuum of Weight-Related Concerns and Disorders
Dieting Behaviors
• Dieting most common in Hispanic females followed by white females
• Dieting & unhealthy wt control behaviors may increase chance of future overweight or obesity
• Effective nutrition messages should focus on lifestyle changes
• Adolescents with low levels of body satisfaction are more likely to use unhealthy weight control behaviors & participate in less physical activity
Disordered Eating Behaviors
• Anorexic or bulimic behaviors—with less frequency or intensity=unable to do a formal diagnosis
• Most frequently used behaviors– Vomiting– Laxatives– Fasting or extreme dieting– Excessive exercise
Three Main Eating Disorders
• Anorexia nervosa– Characterized by extreme wt loss, poor
body image, & irrational fears of wt gain & obesity
• Bulimia nervosa– Characterized by recurrent episodes of
rapid uncontrolled eating of large amounts of food in a short period of time frequently followed by purging
Three Main Eating Disorders
• Binge-eating disorder– Characterized by periodic binge eating not
followed by vomiting or use of laxatives
Prognosis for People with Anorexia Nervosa
• ~10% to 15% die from the disease• Deaths related to
– Weakened immune system– Gastric ruptures– Cardiac arrhythmia– Heart failure– Suicide
Prognosis for People with Anorexia Nervosa
• Early diagnosis & treatment improves chances for recovery
• Recovery rates – <50% fully recover– ~33% show improvement– ~20% chronically affected
Prognosis for People with Bulimia Nervosa
• ~2-3% die from disease• Recovery rates
– ~48% full recovery
– ~26% improvement
– ~26% chronicity
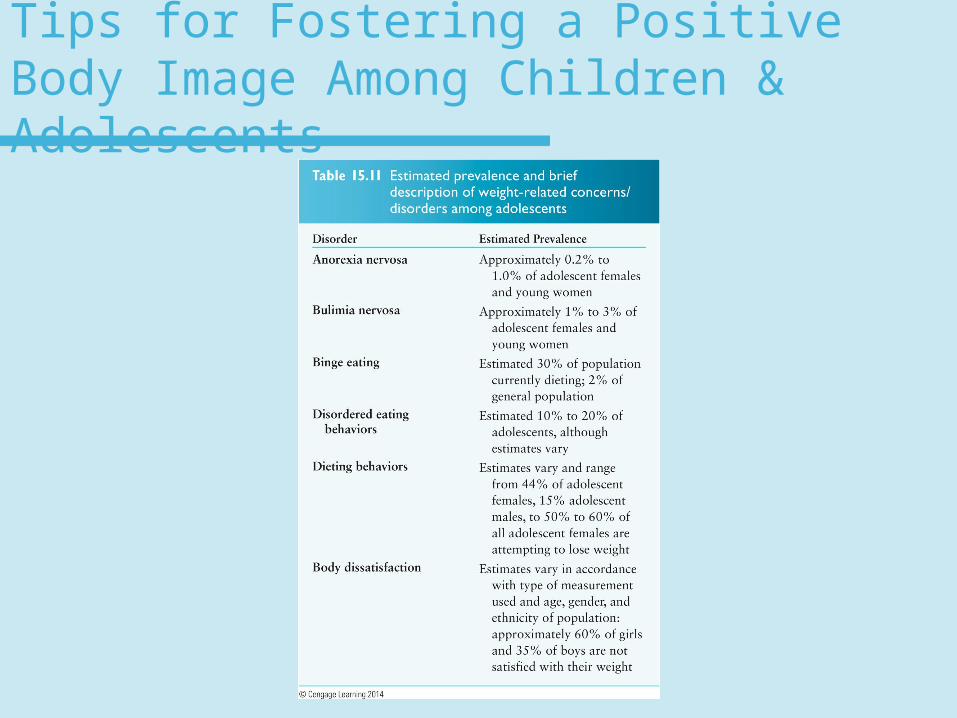
Tips for Fostering a Positive Body Image Among Children & Adolescents
Etiology of Eating Disorders
• Environmental factors:– Media Influences– Societal and cultural norms– Food availability and accessibility
• Family factors:– Family dynamics
• Weight-related behaviors of parents and siblings• Feeding behaviors reinforced during childhood and
adolescence
Etiology of Eating Disorders
• Interpersonal factors:– Peer norms and behaviors– Abuse experiences
• Personal factors:– Biological– Psychological– Knowledge, attitudes and behaviors
Treating Eating Disorders
• A multidisciplinary team approach
• Team may consist of– Physician– Dietitian– Nurse– Psychologist– Psychiatrist
Treating Eating Disorders
• Goal of eating-disorder treatment programs– Restore body weight– Improve social and emotional well-being– Normalize eating behaviors
Treating Eating Disorders
• Core components of programs:– Treatment of medical comorbidities– Restoration of body weight to normal– Nutrition education & counseling– Individualized psychotherapy– Family therapy– Group therapy
Eating Disorders Among Adolescents: Summing It Up
• Eating disorders—a continuum ranging from body dissatisfaction to clinically significant eating disorders
• Parents, peers, educators, & health care providers should take an important role to help decrease prevalence of eating disorders
Preventing Eating Disorders
• Programs that focus on changing weight-related attitudes of youth & promoted healthy weight-control strategies were found to be more effective
• Effects have lasted up to 2 years
Preventing Eating Disorders
• Characteristics of successful eating disorder prevention programs:– Target high-risk groups– Target adolescents > 15 years of age– Information provided by trained
interventionists– Multiple sessions– Integrated interactive learning










![Oct09 Wk3 Dwb[1]](https://img.pdfslide.us/doc/110x75/54bbb7be4a795937768b460c/oct09-wk3-dwb1.jpg)

















