Embed Size (px)
Citation preview

FL81077NM20-1 Page 1
Humana Insurance Company offers Plans A, F, High Deductible F, G, High Deductible G and NBenefit Chart of Medicare Supplement Plans Sold on or After January 1, 2020NOTICE TO BUYER: This policy may not cover all of the costs associated with medical care incurred by the buyer during the period of coverage. The buyer is advised to review carefully all policy limitations.
Benefits Plans Available to All Applicants
Medicare first eligible before 2020
only+ A B D G1 K L M N C F1
Medicare Part A Coinsurance and hospital coverage (up to an additional 365 days after Medicare benefits are used up)
¸ ¸ ¸ ¸ ¸ ¸ ¸ ¸ ¸ ¸
Medicare Part B Coinsurance or Copayment ¸ ¸ ¸ ¸ 50% 75% ¸
¸copays apply3
¸ ¸
Blood (first three pints) ¸ ¸ ¸ ¸ 50% 75% ¸ ¸ ¸ ¸Part A Hospice Care Coinsurance or Copayment ¸ ¸ ¸ ¸ 50% 75% ¸ ¸ ¸ ¸Skilled Nursing Facility Coinsurance N/A N/A ¸ ¸ 50% 75% ¸ ¸ ¸ ¸Medicare Part A Deductible N/A ¸ ¸ ¸ 50% 75% 50% ¸ ¸ ¸Medicare Part B Deductible N/A N/A N/A N/A N/A N/A N/A N/A ¸ ¸Medicare Part B Excess Charges N/A N/A N/A ¸ N/A N/A N/A N/A N/A ¸Foreign Travel Emergency (up to plan limits) N/A N/A ¸ ¸ N/A N/A ¸ ¸ ¸ ¸Out of Pocket Limit in 2021 2 N/A N/A N/A N/A $6,2202 $3,110 2 N/A N/A N/A N/A
Note: A ¸ means 100% of the benefit is paid. +Only applicants first eligible for Medicare before January 1, 2020 may purchase Plans C, F, and high deductible F. This chart shows the benefits included in each of the standard Medicare supplement plans. Some plans may not be available. Every company must make Plan "A" available.1 Plans F and G also have a high deductible option which require first paying a plan deductible of $2,370 before the plan begins to pay. Once the
plan deductible is met, the plan pays 100% of covered services for the rest of the calendar year. High deductible Plans F and G do not cover the separate Foreign travel emergency deductible. High Deductible Plan G does not cover the Medicare Part B deductible. However, high deductible plans F and G count your payment of the Medicare Part B deductible toward meeting the plan deductible.
2 Plans K and L pay 100% of covered services for the rest of the calendar year once you meet the out-of-pocket yearly limit. 3 Plan N pays 100% of the Part B coinsurance, except for a copayment of up to $20 for some office visits and up to a $50 copayment for
emergency room visits that do not result in an inpatient admission.
Page 2 FL81077NM20-1
Basic Benefits Hospitalization – Part A coinsurance plus coverage for 365 additional days after Medicare benefits end. Medical Expenses – Part B coinsurance (generally 20% of Medicare-approved expenses) or copayments for hospital outpatient services. Plans K, L and N require insureds to pay a portion of Part B coinsurance or co-payments. Blood – First three pints of blood each year. Hospice - Part A coinsurance.
Premium Information We, Humana Insurance Company, can only raise your premium if we raise the premium for all policies like yours in the state of Florida. Premium amounts are available for a monthly payment mode only.
Read your policy very carefully This is only an outline describing your policy's most important features. The policy is your insurance contract. You must read the policy itself to understand all of the rights and duties of both you and your insurance company.
Right to return policy If you find that you are not satisfied with your policy, you may return it to:
Humana Insurance Company Attn: Medicare Enrollments P.O. Box 14168 Lexington, KY 40512-4168
If you send the policy back to us within 30 days after you receive it, we will treat the policy as if it had never been issued and return all of your payments.
Notice Neither Humana Insurance Company nor its agents are connected with Medicare. This Outline of Coverage does not give all the details of Medicare coverage. Contact your local Social Security Office or consult the "Medicare & You" handbook for more details. Use this outline to compare benefits and premiums among policies.
Policy replacement If you are replacing another health insurance policy, do NOT cancel it until you have actually received your new policy and are sure you want to keep it.
FL81077NM20-1 Page 3
Complete answers are very important When you fill out the application for the new policy, and it is NOT an "Open Enrollment or Guaranteed Issue status application," be sure to answer truthfully and completely all questions about your medical and health history. The policy is issued on the basis that the answers to all questions and all information shown in the application are correct and complete. The company may cancel your policy and refuse to pay any claims if you make misstatements, leave out or falsify important information. Review the application carefully before you sign it. Be certain that all information has been properly recorded. To review "Open Enrollment" timeframes please go to the following link on the Medicare.gov website: https://www.medicare.gov/supplement-other-insurance/when-can-i-buy-medigap/when-can-i-buy-medigap.html

Page 4 FL81077NM20-1
Premium Rating Area ClassificationUse this page to identify your rating area for assistance in determining your monthly premium. Please locate your county below.
Area 1: (Premium rates begin on page Broward, Miami-Dade, Palm Beach
Area 2: (Premium rates begin on page Baker, Bay, Brevard, Charlotte, Clay, Collier, Duval, Hernando, Hillsborough, Indian River, Lake, Lee, Manatee, Martin, Nassau, Okaloosa, Orange, Osceola, Pasco, Pinellas, St. Johns, St. Lucie, Sarasota, Seminole, Volusia
Area 3: (Premium rates begin on page Alachua, Bradford, Calhoun, Citrus, Columbia, DeSoto, Dixie, Escambia, Flagler, Franklin, Gadsden, Gilchrist, Glades, Gulf, Hamilton, Hardee, Hendry, Highlands, Holmes, Jackson, Jefferson, LaFayette, Leon, Levy, Liberty, Madison, Marion, Monroe, Okeechobee, Polk, Putnam, Santa Rosa, Sumter, Suwannee, Taylor, Union, Wakulla, Walton, Washington
5)
10)
15)
FL81077NM20-1 Page 5
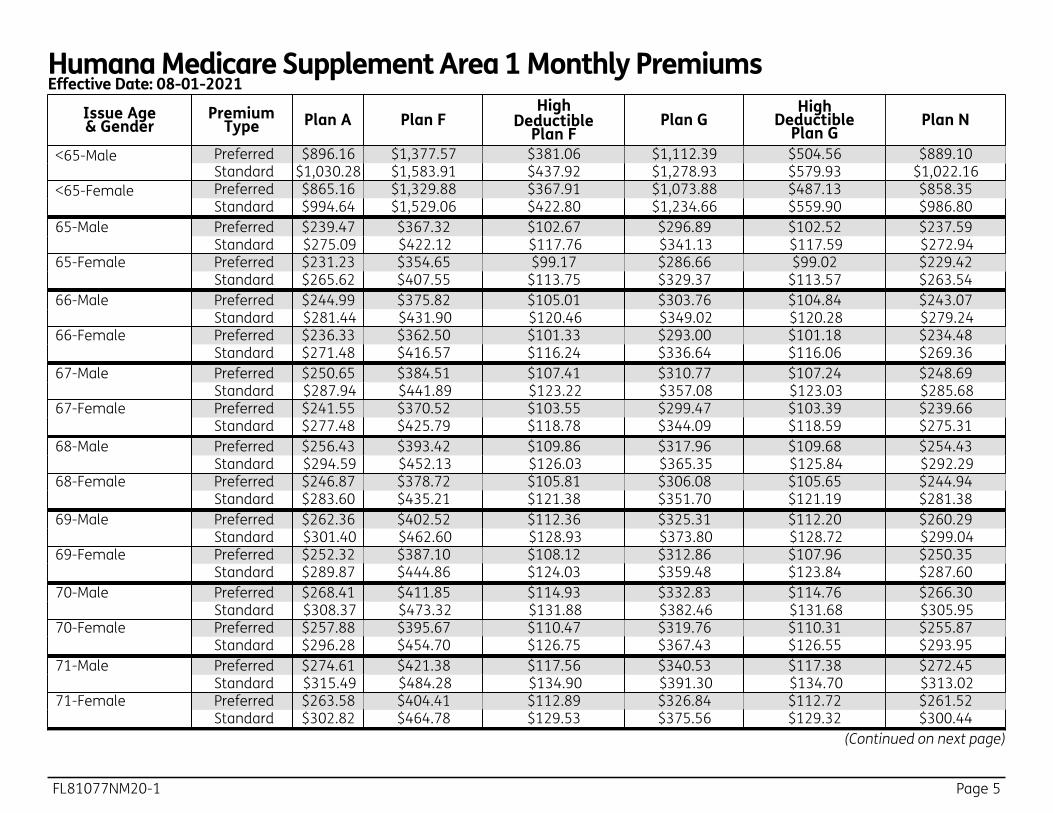
Humana Medicare Supplement Area 1 Monthly PremiumsEffective Date: 08-01-2021
Issue Age & Gender
Premium Type Plan A Plan F
High Deductible
Plan FPlan G
High Deductible
Plan GPlan N
<65 -Male Preferred $896.16 $1,377.57 $381.06 $1,112.39 $504.56 $889.10 Standard $1,030.28 $1,583.91 $437.92 $1,278.93 $579.93 $1,022.16
<65 -Female Preferred $865.16 $1,329.88 $367.91 $1,073.88 $487.13 $858.35 Standard $994.64 $1,529.06 $422.80 $1,234.66 $559.90 $986.80
65 -Male Preferred $239.47 $367.32 $102.67 $296.89 $102.52 $237.59 65-Male Standard $275.09 $422.12 $117.76 $341.13 $117.59 $272.94 65 -Female Preferred $231.23 $354.65 $99.17 $286.66 $99.02 $229.42 65-Female Standard $265.62 $407.55 $113.75 $329.37 $113.57 $263.54 66 -Male Preferred $244.99 $375.82 $105.01 $303.76 $104.84 $243.07 66-Male Standard $281.44 $431.90 $120.46 $349.02 $120.28 $279.24 66 -Female Preferred $236.33 $362.50 $101.33 $293.00 $101.18 $234.48 66-Female Standard $271.48 $416.57 $116.24 $336.64 $116.06 $269.36 67 -Male Preferred $250.65 $384.51 $107.41 $310.77 $107.24 $248.69 67-Male Standard $287.94 $441.89 $123.22 $357.08 $123.03 $285.68 67 -Female Preferred $241.55 $370.52 $103.55 $299.47 $103.39 $239.66 67-Female Standard $277.48 $425.79 $118.78 $344.09 $118.59 $275.31 68 -Male Preferred $256.43 $393.42 $109.86 $317.96 $109.68 $254.43 68-Male Standard $294.59 $452.13 $126.03 $365.35 $125.84 $292.29 68 -Female Preferred $246.87 $378.72 $105.81 $306.08 $105.65 $244.94 68-Female Standard $283.60 $435.21 $121.38 $351.70 $121.19 $281.38 69 -Male Preferred $262.36 $402.52 $112.36 $325.31 $112.20 $260.29 69-Male Standard $301.40 $462.60 $128.93 $373.80 $128.72 $299.04 69 -Female Preferred $252.32 $387.10 $108.12 $312.86 $107.96 $250.35 69-Female Standard $289.87 $444.86 $124.03 $359.48 $123.84 $287.60 70 -Male Preferred $268.41 $411.85 $114.93 $332.83 $114.76 $266.30 70-Male Standard $308.37 $473.32 $131.88 $382.46 $131.68 $305.95 70 -Female Preferred $257.88 $395.67 $110.47 $319.76 $110.31 $255.87 70-Female Standard $296.28 $454.70 $126.75 $367.43 $126.55 $293.95 71 -Male Preferred $274.61 $421.38 $117.56 $340.53 $117.38 $272.45 71-Male Standard $315.49 $484.28 $134.90 $391.30 $134.70 $313.02 71 -Female Preferred $263.58 $404.41 $112.89 $326.84 $112.72 $261.52 71-Female Standard $302.82 $464.78 $129.53 $375.56 $129.32 $300.44
(Continued on next page)

Page 6 FL81077NM20-1
Humana Medicare Supplement Area 1 Monthly PremiumsEffective Date: 08-01-2021
Issue Age & Gender
Premium Type Plan A Plan F
High Deductible
Plan FPlan G
High Deductible
Plan GPlan N
72 -Male Preferred $280.95 $431.13 $120.25 $348.41 $120.08 $278.75 72-Male Standard $322.80 $495.50 $137.99 $400.36 $137.78 $320.25 72 -Female Preferred $269.40 $413.37 $115.36 $334.06 $115.18 $267.30 72-Female Standard $309.51 $475.08 $132.36 $383.87 $132.15 $307.09 73 -Male Preferred $287.44 $441.12 $123.00 $356.46 $122.82 $285.19 73-Male Standard $330.26 $507.00 $141.16 $409.63 $140.94 $327.67 73 -Female Preferred $275.35 $422.51 $117.87 $341.44 $117.70 $273.18 73-Female Standard $316.35 $485.59 $135.27 $392.36 $135.05 $313.86 74 -Male Preferred $294.09 $451.34 $125.81 $364.71 $125.62 $291.78 74-Male Standard $337.89 $518.73 $144.39 $419.11 $144.17 $335.24 74 -Female Preferred $281.43 $431.87 $120.46 $348.99 $120.27 $279.22 74-Female Standard $323.34 $496.35 $138.22 $401.05 $138.01 $320.81 75 -Male Preferred $300.87 $461.79 $128.70 $373.14 $128.51 $298.52 75-Male Standard $345.71 $530.75 $147.71 $428.82 $147.48 $342.99 75 -Female Preferred $287.64 $441.43 $123.09 $356.72 $122.90 $285.38 75-Female Standard $330.49 $507.35 $141.25 $409.92 $141.03 $327.90 76 -Male Preferred $307.84 $472.49 $131.65 $381.78 $131.44 $305.42 76-Male Standard $353.71 $543.06 $151.10 $438.75 $150.87 $350.94 76 -Female Preferred $293.99 $451.21 $125.79 $364.60 $125.60 $291.69 76-Female Standard $337.80 $518.58 $144.35 $418.99 $144.13 $335.15 77 -Male Preferred $314.95 $483.44 $134.67 $390.62 $134.46 $312.47 77-Male Standard $361.88 $555.66 $154.56 $448.91 $154.33 $359.05 77 -Female Preferred $300.49 $461.20 $128.53 $372.67 $128.34 $298.14 77-Female Standard $345.26 $530.07 $147.52 $428.26 $147.29 $342.56 78 -Male Preferred $322.23 $494.63 $137.76 $399.66 $137.54 $319.70 78-Male Standard $370.26 $568.54 $158.11 $459.31 $157.87 $367.35 78 -Female Preferred $307.13 $471.42 $131.35 $380.91 $131.15 $304.72 78-Female Standard $352.91 $541.82 $150.76 $437.76 $150.53 $350.13 79 -Male Preferred $329.68 $506.10 $140.91 $408.91 $140.69 $327.09 79-Male Standard $378.83 $581.71 $161.75 $469.95 $161.50 $375.85 79 -Female Preferred $313.92 $481.85 $134.23 $389.34 $134.03 $311.45 79-Female Standard $360.71 $553.83 $154.06 $447.44 $153.83 $357.87
(Continued on next page)
FL81077NM20-1 Page 7
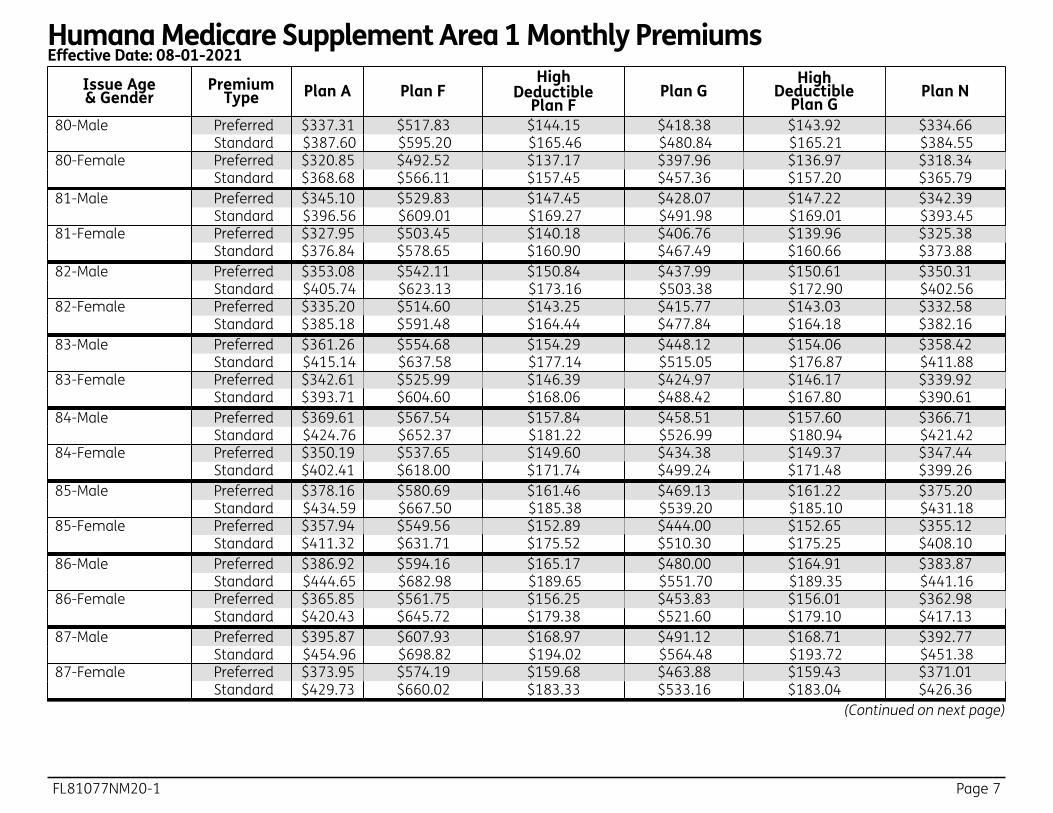
Humana Medicare Supplement Area 1 Monthly PremiumsEffective Date: 08-01-2021
Issue Age & Gender
Premium Type Plan A Plan F
High Deductible
Plan FPlan G
High Deductible
Plan GPlan N
80 -Male Preferred $337.31 $517.83 $144.15 $418.38 $143.92 $334.66 80-Male Standard $387.60 $595.20 $165.46 $480.84 $165.21 $384.55 80 -Female Preferred $320.85 $492.52 $137.17 $397.96 $136.97 $318.34 80-Female Standard $368.68 $566.11 $157.45 $457.36 $157.20 $365.79 81 -Male Preferred $345.10 $529.83 $147.45 $428.07 $147.22 $342.39 81-Male Standard $396.56 $609.01 $169.27 $491.98 $169.01 $393.45 81 -Female Preferred $327.95 $503.45 $140.18 $406.76 $139.96 $325.38 81-Female Standard $376.84 $578.65 $160.90 $467.49 $160.66 $373.88 82 -Male Preferred $353.08 $542.11 $150.84 $437.99 $150.61 $350.31 82-Male Standard $405.74 $623.13 $173.16 $503.38 $172.90 $402.56 82 -Female Preferred $335.20 $514.60 $143.25 $415.77 $143.03 $332.58 82-Female Standard $385.18 $591.48 $164.44 $477.84 $164.18 $382.16 83 -Male Preferred $361.26 $554.68 $154.29 $448.12 $154.06 $358.42 83-Male Standard $415.14 $637.58 $177.14 $515.05 $176.87 $411.88 83 -Female Preferred $342.61 $525.99 $146.39 $424.97 $146.17 $339.92 83-Female Standard $393.71 $604.60 $168.06 $488.42 $167.80 $390.61 84 -Male Preferred $369.61 $567.54 $157.84 $458.51 $157.60 $366.71 84-Male Standard $424.76 $652.37 $181.22 $526.99 $180.94 $421.42 84 -Female Preferred $350.19 $537.65 $149.60 $434.38 $149.37 $347.44 84-Female Standard $402.41 $618.00 $171.74 $499.24 $171.48 $399.26 85 -Male Preferred $378.16 $580.69 $161.46 $469.13 $161.22 $375.20 85-Male Standard $434.59 $667.50 $185.38 $539.20 $185.10 $431.18 85 -Female Preferred $357.94 $549.56 $152.89 $444.00 $152.65 $355.12 85-Female Standard $411.32 $631.71 $175.52 $510.30 $175.25 $408.10 86 -Male Preferred $386.92 $594.16 $165.17 $480.00 $164.91 $383.87 86-Male Standard $444.65 $682.98 $189.65 $551.70 $189.35 $441.16 86 -Female Preferred $365.85 $561.75 $156.25 $453.83 $156.01 $362.98 86-Female Standard $420.43 $645.72 $179.38 $521.60 $179.10 $417.13 87 -Male Preferred $395.87 $607.93 $168.97 $491.12 $168.71 $392.77 87-Male Standard $454.96 $698.82 $194.02 $564.48 $193.72 $451.38 87 -Female Preferred $373.95 $574.19 $159.68 $463.88 $159.43 $371.01 87-Female Standard $429.73 $660.02 $183.33 $533.16 $183.04 $426.36
(Continued on next page)
Page 8 FL81077NM20-1
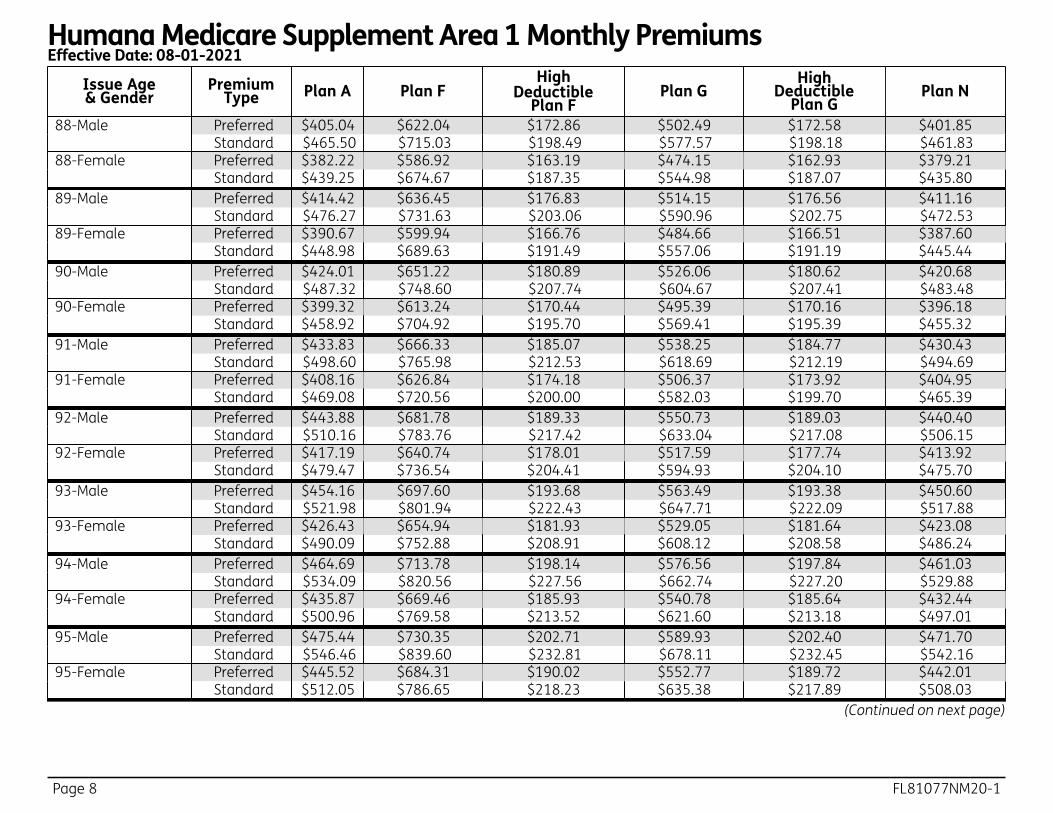
Humana Medicare Supplement Area 1 Monthly PremiumsEffective Date: 08-01-2021
Issue Age & Gender
Premium Type Plan A Plan F
High Deductible
Plan FPlan G
High Deductible
Plan GPlan N
88 -Male Preferred $405.04 $622.04 $172.86 $502.49 $172.58 $401.85 88-Male Standard $465.50 $715.03 $198.49 $577.57 $198.18 $461.83 88 -Female Preferred $382.22 $586.92 $163.19 $474.15 $162.93 $379.21 88-Female Standard $439.25 $674.67 $187.35 $544.98 $187.07 $435.80 89 -Male Preferred $414.42 $636.45 $176.83 $514.15 $176.56 $411.16 89-Male Standard $476.27 $731.63 $203.06 $590.96 $202.75 $472.53 89 -Female Preferred $390.67 $599.94 $166.76 $484.66 $166.51 $387.60 89-Female Standard $448.98 $689.63 $191.49 $557.06 $191.19 $445.44 90 -Male Preferred $424.01 $651.22 $180.89 $526.06 $180.62 $420.68 90-Male Standard $487.32 $748.60 $207.74 $604.67 $207.41 $483.48 90 -Female Preferred $399.32 $613.24 $170.44 $495.39 $170.16 $396.18 90-Female Standard $458.92 $704.92 $195.70 $569.41 $195.39 $455.32 91 -Male Preferred $433.83 $666.33 $185.07 $538.25 $184.77 $430.43 91-Male Standard $498.60 $765.98 $212.53 $618.69 $212.19 $494.69 91 -Female Preferred $408.16 $626.84 $174.18 $506.37 $173.92 $404.95 91-Female Standard $469.08 $720.56 $200.00 $582.03 $199.70 $465.39 92 -Male Preferred $443.88 $681.78 $189.33 $550.73 $189.03 $440.40 92-Male Standard $510.16 $783.76 $217.42 $633.04 $217.08 $506.15 92 -Female Preferred $417.19 $640.74 $178.01 $517.59 $177.74 $413.92 92-Female Standard $479.47 $736.54 $204.41 $594.93 $204.10 $475.70 93 -Male Preferred $454.16 $697.60 $193.68 $563.49 $193.38 $450.60 93-Male Standard $521.98 $801.94 $222.43 $647.71 $222.09 $517.88 93 -Female Preferred $426.43 $654.94 $181.93 $529.05 $181.64 $423.08 93-Female Standard $490.09 $752.88 $208.91 $608.12 $208.58 $486.24 94 -Male Preferred $464.69 $713.78 $198.14 $576.56 $197.84 $461.03 94-Male Standard $534.09 $820.56 $227.56 $662.74 $227.20 $529.88 94 -Female Preferred $435.87 $669.46 $185.93 $540.78 $185.64 $432.44 94-Female Standard $500.96 $769.58 $213.52 $621.60 $213.18 $497.01 95 -Male Preferred $475.44 $730.35 $202.71 $589.93 $202.40 $471.70 95-Male Standard $546.46 $839.60 $232.81 $678.11 $232.45 $542.16 95 -Female Preferred $445.52 $684.31 $190.02 $552.77 $189.72 $442.01 95-Female Standard $512.05 $786.65 $218.23 $635.38 $217.89 $508.03
(Continued on next page)
FL81077NM20-1 Page 9
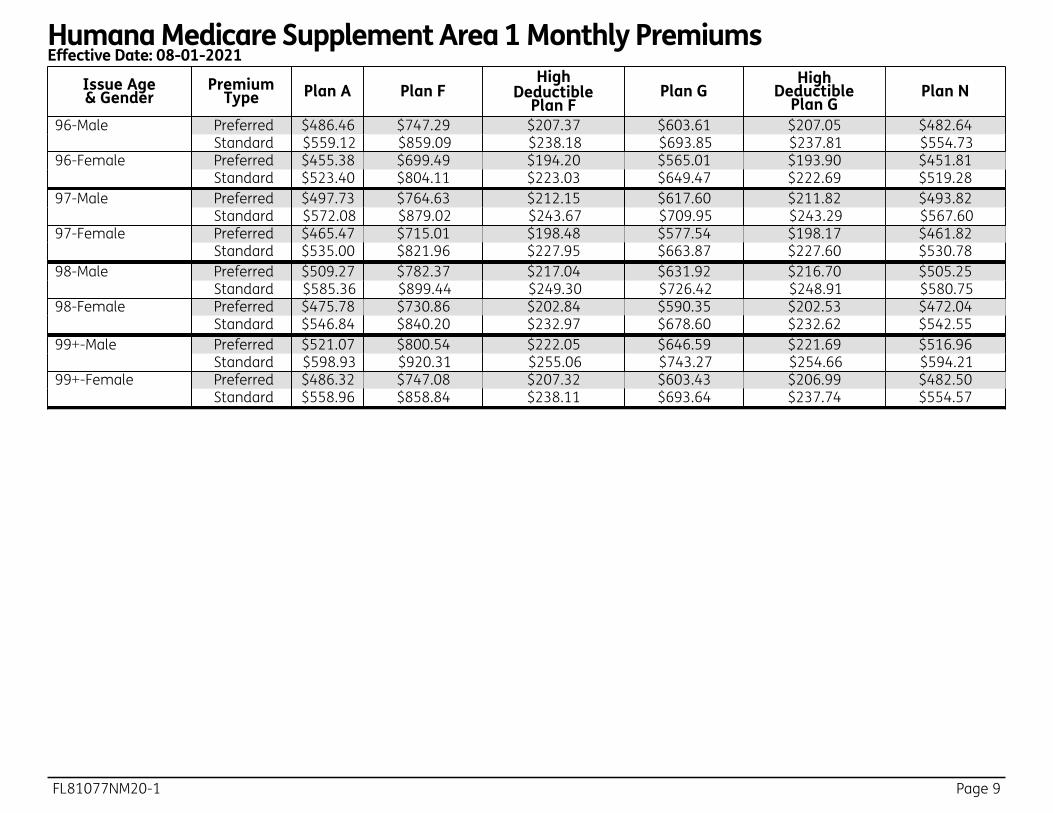
Humana Medicare Supplement Area 1 Monthly PremiumsEffective Date: 08-01-2021
Issue Age & Gender
Premium Type Plan A Plan F
High Deductible
Plan FPlan G
High Deductible
Plan GPlan N
96 -Male Preferred $486.46 $747.29 $207.37 $603.61 $207.05 $482.64 96-Male Standard $559.12 $859.09 $238.18 $693.85 $237.81 $554.73 96 -Female Preferred $455.38 $699.49 $194.20 $565.01 $193.90 $451.81 96-Female Standard $523.40 $804.11 $223.03 $649.47 $222.69 $519.28 97 -Male Preferred $497.73 $764.63 $212.15 $617.60 $211.82 $493.82 97-Male Standard $572.08 $879.02 $243.67 $709.95 $243.29 $567.60 97 -Female Preferred $465.47 $715.01 $198.48 $577.54 $198.17 $461.82 97-Female Standard $535.00 $821.96 $227.95 $663.87 $227.60 $530.78 98 -Male Preferred $509.27 $782.37 $217.04 $631.92 $216.70 $505.25 98-Male Standard $585.36 $899.44 $249.30 $726.42 $248.91 $580.75 98 -Female Preferred $475.78 $730.86 $202.84 $590.35 $202.53 $472.04 98-Female Standard $546.84 $840.20 $232.97 $678.60 $232.62 $542.55 99 +-Male Preferred $521.07 $800.54 $222.05 $646.59 $221.69 $516.96 99-Male Standard $598.93 $920.31 $255.06 $743.27 $254.66 $594.21 99 +-Female Preferred $486.32 $747.08 $207.32 $603.43 $206.99 $482.50 99-Female Standard $558.96 $858.84 $238.11 $693.64 $237.74 $554.57
Page 10 FL81077NM20-1
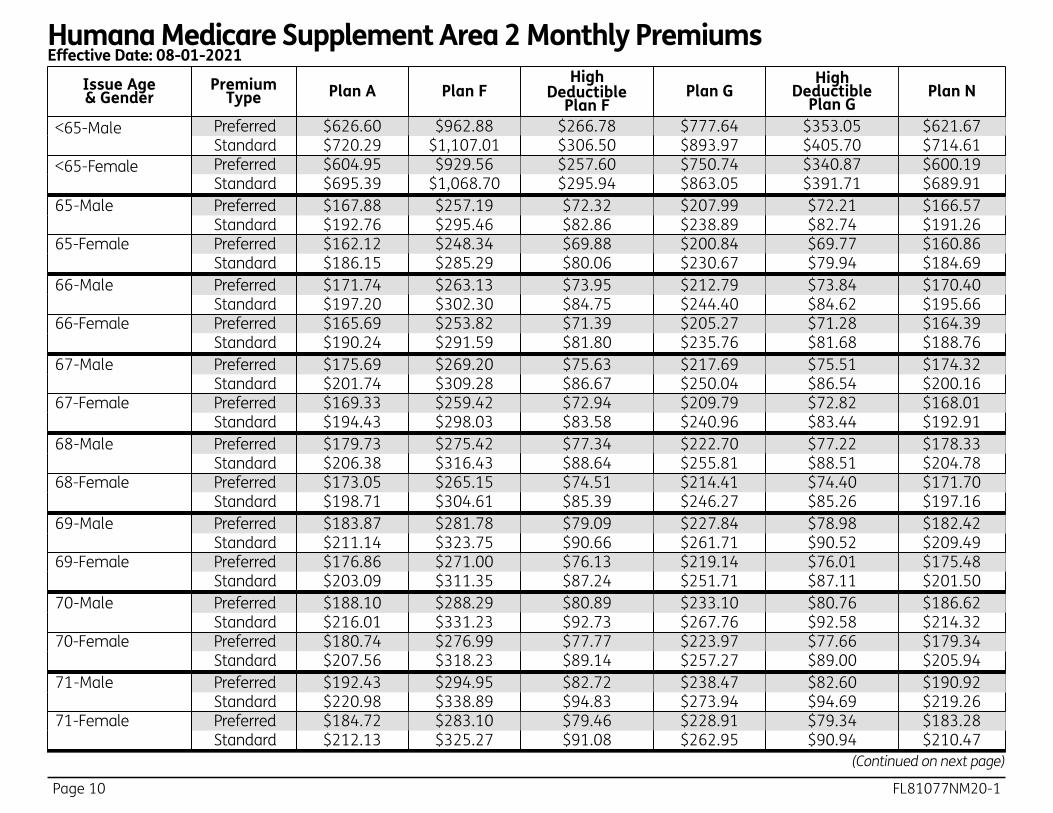
Humana Medicare Supplement Area 2 Monthly PremiumsEffective Date: 08-01-2021
Issue Age & Gender
Premium Type Plan A Plan F
High Deductible
Plan FPlan G
High Deductible
Plan GPlan N
<65-Male Preferred $626.60 $962.88 $266.78 $777.64 $353.05 $621.67 Standard $720.29 $1,107.01 $306.50 $893.97 $405.70 $714.61
<65-F emale Preferred $604.95 $929.56 $257.60 $750.74 $340.87 $600.19 Standard $695.39 $1,068.70 $295.94 $863.05 $391.71 $689.91
65 -Male Preferred $167.88 $257.19 $72.32 $207.99 $72.21 $166.57 99-Male Standard $192.76 $295.46 $82.86 $238.89 $82.74 $191.26 65-Female Preferred $162.12 $248.34 $69.88 $200.84 $69.77 $160.86 99- Female Standard $186.15 $285.29 $80.06 $230.67 $79.94 $184.69 66 -Male Preferred $171.74 $263.13 $73.95 $212.79 $73.84 $170.40 99-Male Standard $197.20 $302.30 $84.75 $244.40 $84.62 $195.66 66-Female Preferred $165.69 $253.82 $71.39 $205.27 $71.28 $164.39 99- Female Standard $190.24 $291.59 $81.80 $235.76 $81.68 $188.76 67 -Male Preferred $175.69 $269.20 $75.63 $217.69 $75.51 $174.32 99-Male Standard $201.74 $309.28 $86.67 $250.04 $86.54 $200.16 67-Female Preferred $169.33 $259.42 $72.94 $209.79 $72.82 $168.01 99- Female Standard $194.43 $298.03 $83.58 $240.96 $83.44 $192.91 68 -Male Preferred $179.73 $275.42 $77.34 $222.70 $77.22 $178.33 99-Male Standard $206.38 $316.43 $88.64 $255.81 $88.51 $204.78 68-Female Preferred $173.05 $265.15 $74.51 $214.41 $74.40 $171.70 99- Female Standard $198.71 $304.61 $85.39 $246.27 $85.26 $197.16 69 -Male Preferred $183.87 $281.78 $79.09 $227.84 $78.98 $182.42 99-Male Standard $211.14 $323.75 $90.66 $261.71 $90.52 $209.49 69-Female Preferred $176.86 $271.00 $76.13 $219.14 $76.01 $175.48 99- Female Standard $203.09 $311.35 $87.24 $251.71 $87.11 $201.50 70 -Male Preferred $188.10 $288.29 $80.89 $233.10 $80.76 $186.62 99-Male Standard $216.01 $331.23 $92.73 $267.76 $92.58 $214.32 70-Female Preferred $180.74 $276.99 $77.77 $223.97 $77.66 $179.34 99- Female Standard $207.56 $318.23 $89.14 $257.27 $89.00 $205.94 71 -Male Preferred $192.43 $294.95 $82.72 $238.47 $82.60 $190.92 99-Male Standard $220.98 $338.89 $94.83 $273.94 $94.69 $219.26 71-Female Preferred $184.72 $283.10 $79.46 $228.91 $79.34 $183.28 99- Female Standard $212.13 $325.27 $91.08 $262.95 $90.94 $210.47
(Continued on next page)
FL81077NM20-1 Page 11
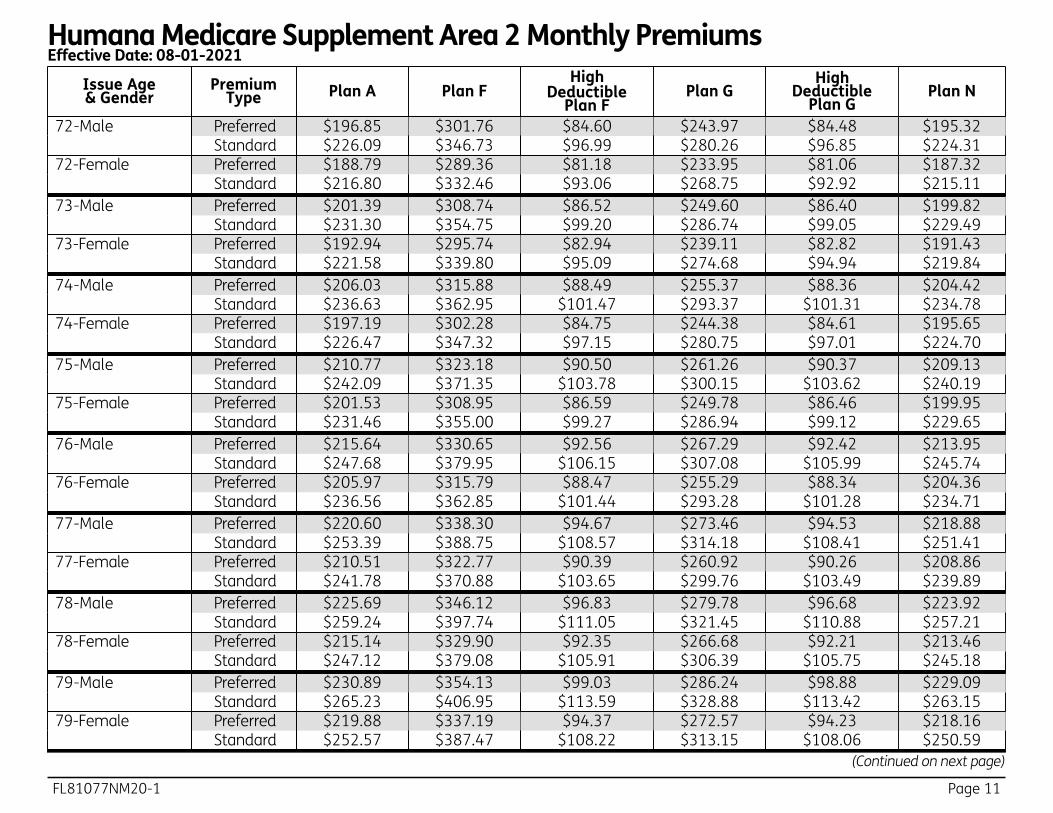
Humana Medicare Supplement Area 2 Monthly PremiumsEffective Date: 08-01-2021
Issue Age & Gender
Premium Type Plan A Plan F
High Deductible
Plan FPlan G
High Deductible
Plan GPlan N
72 -Male Preferred $196.85 $301.76 $84.60 $243.97 $84.48 $195.32 99-Male Standard $226.09 $346.73 $96.99 $280.26 $96.85 $224.31 72-Female Preferred $188.79 $289.36 $81.18 $233.95 $81.06 $187.32 99- Female Standard $216.80 $332.46 $93.06 $268.75 $92.92 $215.11 73 -Male Preferred $201.39 $308.74 $86.52 $249.60 $86.40 $199.82 99-Male Standard $231.30 $354.75 $99.20 $286.74 $99.05 $229.49 73-Female Preferred $192.94 $295.74 $82.94 $239.11 $82.82 $191.43 99- Female Standard $221.58 $339.80 $95.09 $274.68 $94.94 $219.84 74 -Male Preferred $206.03 $315.88 $88.49 $255.37 $88.36 $204.42 99-Male Standard $236.63 $362.95 $101.47 $293.37 $101.31 $234.78 74-Female Preferred $197.19 $302.28 $84.75 $244.38 $84.61 $195.65 99- Female Standard $226.47 $347.32 $97.15 $280.75 $97.01 $224.70 75 -Male Preferred $210.77 $323.18 $90.50 $261.26 $90.37 $209.13 99-Male Standard $242.09 $371.35 $103.78 $300.15 $103.62 $240.19 75-Female Preferred $201.53 $308.95 $86.59 $249.78 $86.46 $199.95 99- Female Standard $231.46 $355.00 $99.27 $286.94 $99.12 $229.65 76 -Male Preferred $215.64 $330.65 $92.56 $267.29 $92.42 $213.95 99-Male Standard $247.68 $379.95 $106.15 $307.08 $105.99 $245.74 76-Female Preferred $205.97 $315.79 $88.47 $255.29 $88.34 $204.36 99- Female Standard $236.56 $362.85 $101.44 $293.28 $101.28 $234.71 77 -Male Preferred $220.60 $338.30 $94.67 $273.46 $94.53 $218.88 99-Male Standard $253.39 $388.75 $108.57 $314.18 $108.41 $251.41 77-Female Preferred $210.51 $322.77 $90.39 $260.92 $90.26 $208.86 99- Female Standard $241.78 $370.88 $103.65 $299.76 $103.49 $239.89 78 -Male Preferred $225.69 $346.12 $96.83 $279.78 $96.68 $223.92 99-Male Standard $259.24 $397.74 $111.05 $321.45 $110.88 $257.21 78-Female Preferred $215.14 $329.90 $92.35 $266.68 $92.21 $213.46 99- Female Standard $247.12 $379.08 $105.91 $306.39 $105.75 $245.18 79 -Male Preferred $230.89 $354.13 $99.03 $286.24 $98.88 $229.09 99-Male Standard $265.23 $406.95 $113.59 $328.88 $113.42 $263.15 79-Female Preferred $219.88 $337.19 $94.37 $272.57 $94.23 $218.16 99- Female Standard $252.57 $387.47 $108.22 $313.15 $108.06 $250.59
(Continued on next page)

Page 12 FL81077NM20-1
Humana Medicare Supplement Area 2 Monthly PremiumsEffective Date: 08-01-2021
Issue Age & Gender
Premium Type Plan A Plan F
High Deductible
Plan FPlan G
High Deductible
Plan GPlan N
80 -Male Preferred $236.22 $362.33 $101.29 $292.85 $101.13 $234.37 99-Male Standard $271.35 $416.37 $116.18 $336.49 $116.01 $269.23 80-Female Preferred $224.73 $344.65 $96.42 $278.59 $96.28 $222.97 99- Female Standard $258.14 $396.05 $110.59 $320.08 $110.41 $256.12 81 -Male Preferred $241.67 $370.70 $103.60 $299.63 $103.44 $239.78 99-Male Standard $277.61 $426.01 $118.84 $344.27 $118.66 $275.44 81-Female Preferred $229.69 $352.27 $98.52 $284.74 $98.37 $227.89 99- Female Standard $263.84 $404.81 $113.00 $327.16 $112.83 $261.77 82 -Male Preferred $247.24 $379.28 $105.97 $306.55 $105.81 $245.30 99-Male Standard $284.03 $435.87 $121.56 $352.23 $121.38 $281.80 82-Female Preferred $234.75 $360.06 $100.67 $291.03 $100.52 $232.92 99- Female Standard $269.66 $413.77 $115.47 $334.39 $115.29 $267.55 83 -Male Preferred $252.95 $388.06 $108.38 $313.63 $108.22 $250.97 99-Male Standard $290.59 $445.97 $124.34 $360.38 $124.15 $288.31 83-Female Preferred $239.93 $368.03 $102.86 $297.46 $102.71 $238.05 99- Female Standard $275.62 $422.94 $118.00 $341.78 $117.81 $273.45 84 -Male Preferred $258.79 $397.05 $110.86 $320.89 $110.69 $256.76 99-Male Standard $297.31 $456.30 $127.19 $368.72 $126.99 $294.98 84-Female Preferred $245.22 $376.17 $105.10 $304.03 $104.94 $243.30 99- Female Standard $281.70 $432.29 $120.57 $349.34 $120.39 $279.50 85 -Male Preferred $264.76 $406.23 $113.39 $328.31 $113.22 $262.69 99-Male Standard $304.18 $466.87 $130.10 $377.25 $129.90 $301.79 85-Female Preferred $250.63 $384.49 $107.40 $310.75 $107.23 $248.67 99- Female Standard $287.92 $441.87 $123.21 $357.06 $123.02 $285.67 86 -Male Preferred $270.88 $415.64 $115.98 $335.90 $115.80 $268.75 99-Male Standard $311.21 $477.68 $133.08 $385.98 $132.87 $308.76 86-Female Preferred $256.16 $393.00 $109.75 $317.62 $109.58 $254.16 99- Female Standard $294.29 $451.65 $125.91 $364.96 $125.71 $291.98 87 -Male Preferred $277.13 $425.26 $118.63 $343.67 $118.45 $274.96 99-Male Standard $318.41 $488.75 $136.13 $394.91 $135.92 $315.91 87-Female Preferred $261.82 $401.69 $112.14 $324.64 $111.97 $259.76 99- Female Standard $300.78 $461.65 $128.66 $373.03 $128.46 $298.43
(Continued on next page)

FL81077NM20-1 Page 13
Humana Medicare Supplement Area 2 Monthly PremiumsEffective Date: 08-01-2021
Issue Age & Gender
Premium Type Plan A Plan F
High Deductible
Plan FPlan G
High Deductible
Plan GPlan N
88 -Male Preferred $283.53 $435.11 $121.35 $351.61 $121.16 $281.31 99-Male Standard $325.77 $500.08 $139.26 $404.05 $139.04 $323.20 88-Female Preferred $267.59 $410.59 $114.59 $331.81 $114.41 $265.49 99- Female Standard $307.43 $471.88 $131.48 $381.29 $131.28 $305.02 89 -Male Preferred $290.09 $445.18 $124.12 $359.75 $123.93 $287.81 99-Male Standard $333.29 $511.67 $142.45 $413.41 $142.23 $330.68 89-Female Preferred $273.50 $419.68 $117.09 $339.16 $116.91 $271.35 99- Female Standard $314.23 $482.33 $134.36 $389.72 $134.15 $311.76 90 -Male Preferred $296.79 $455.50 $126.96 $368.07 $126.77 $294.46 99-Male Standard $341.01 $523.52 $145.72 $422.98 $145.49 $338.33 90-Female Preferred $279.54 $428.97 $119.66 $346.65 $119.47 $277.35 99- Female Standard $321.17 $493.01 $137.31 $398.35 $137.09 $318.65 91 -Male Preferred $303.64 $466.06 $129.88 $376.59 $129.67 $301.27 99-Male Standard $348.89 $535.66 $149.06 $432.78 $148.82 $346.16 91-Female Preferred $285.72 $438.47 $122.27 $354.32 $122.09 $283.48 99- Female Standard $328.27 $503.93 $140.31 $407.17 $140.10 $325.69 92 -Male Preferred $310.66 $476.85 $132.85 $385.31 $132.64 $308.23 99-Male Standard $356.97 $548.08 $152.48 $442.80 $152.24 $354.17 92-Female Preferred $292.03 $448.18 $124.95 $362.15 $124.76 $289.74 99- Female Standard $335.53 $515.10 $143.39 $416.18 $143.17 $332.89 93 -Male Preferred $317.85 $487.90 $135.89 $394.22 $135.68 $315.36 99-Male Standard $365.22 $560.78 $155.98 $453.05 $155.74 $362.35 93-Female Preferred $298.48 $458.10 $127.69 $370.16 $127.49 $296.14 99- Female Standard $342.95 $526.51 $146.53 $425.40 $146.31 $340.26 94 -Male Preferred $325.20 $499.20 $139.01 $403.35 $138.80 $322.64 99-Male Standard $373.68 $573.79 $159.56 $463.55 $159.31 $370.74 94-Female Preferred $305.07 $468.24 $130.48 $378.35 $130.28 $302.68 99- Female Standard $350.54 $538.18 $149.75 $434.81 $149.52 $347.78 95 -Male Preferred $332.71 $510.77 $142.20 $412.69 $141.98 $330.10 99-Male Standard $382.32 $587.09 $163.22 $474.28 $162.98 $379.32 95-Female Preferred $311.81 $478.62 $133.34 $386.73 $133.13 $309.36 99- Female Standard $358.29 $550.10 $153.04 $444.43 $152.80 $355.48
(Continued on next page)
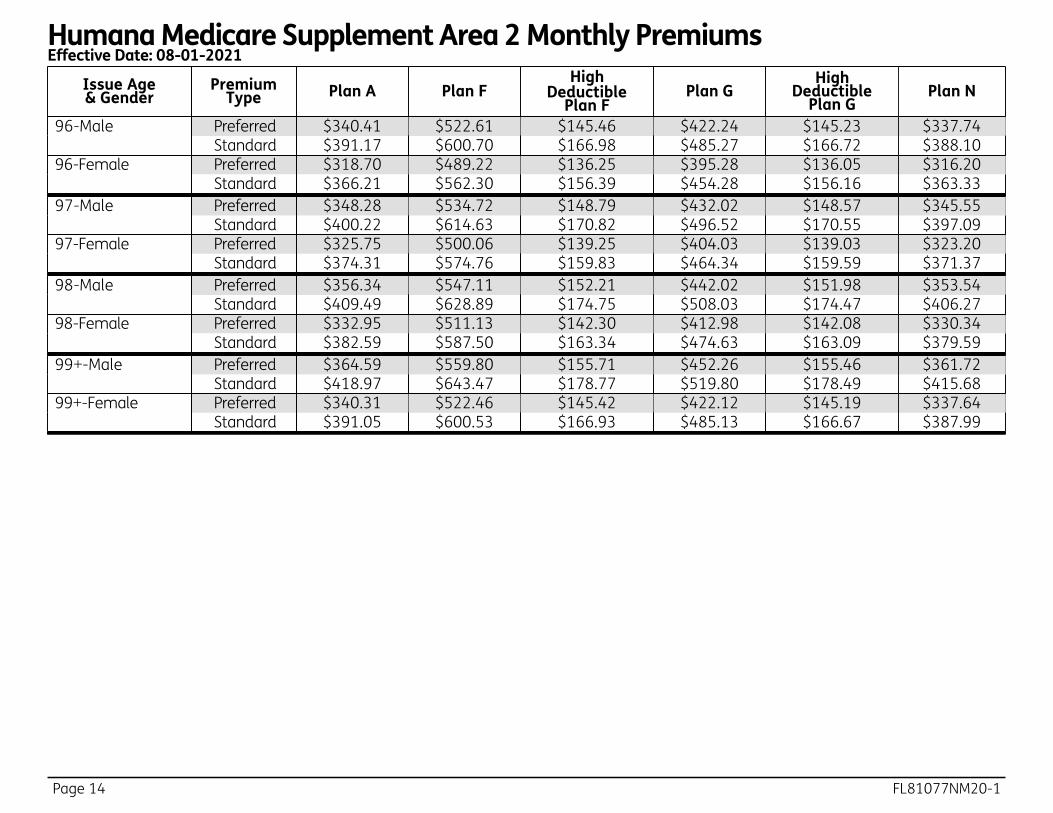
Page 14 FL81077NM20-1
Humana Medicare Supplement Area 2 Monthly PremiumsEffective Date: 08-01-2021
Issue Age & Gender
Premium Type Plan A Plan F
High Deductible
Plan FPlan G
High Deductible
Plan GPlan N
96 -Male Preferred $340.41 $522.61 $145.46 $422.24 $145.23 $337.74 99-Male Standard $391.17 $600.70 $166.98 $485.27 $166.72 $388.10 96-Female Preferred $318.70 $489.22 $136.25 $395.28 $136.05 $316.20 99- Female Standard $366.21 $562.30 $156.39 $454.28 $156.16 $363.33 97 -Male Preferred $348.28 $534.72 $148.79 $432.02 $148.57 $345.55 99-Male Standard $400.22 $614.63 $170.82 $496.52 $170.55 $397.09 97-Female Preferred $325.75 $500.06 $139.25 $404.03 $139.03 $323.20 99- Female Standard $374.31 $574.76 $159.83 $464.34 $159.59 $371.37 98 -Male Preferred $356.34 $547.11 $152.21 $442.02 $151.98 $353.54 99-Male Standard $409.49 $628.89 $174.75 $508.03 $174.47 $406.27 98-Female Preferred $332.95 $511.13 $142.30 $412.98 $142.08 $330.34 99- Female Standard $382.59 $587.50 $163.34 $474.63 $163.09 $379.59 99 +-Male Preferred $364.59 $559.80 $155.71 $452.26 $155.46 $361.72 99-Male Standard $418.97 $643.47 $178.77 $519.80 $178.49 $415.68 99+-Female Preferred $340.31 $522.46 $145.42 $422.12 $145.19 $337.64 99- Female Standard $391.05 $600.53 $166.93 $485.13 $166.67 $387.99
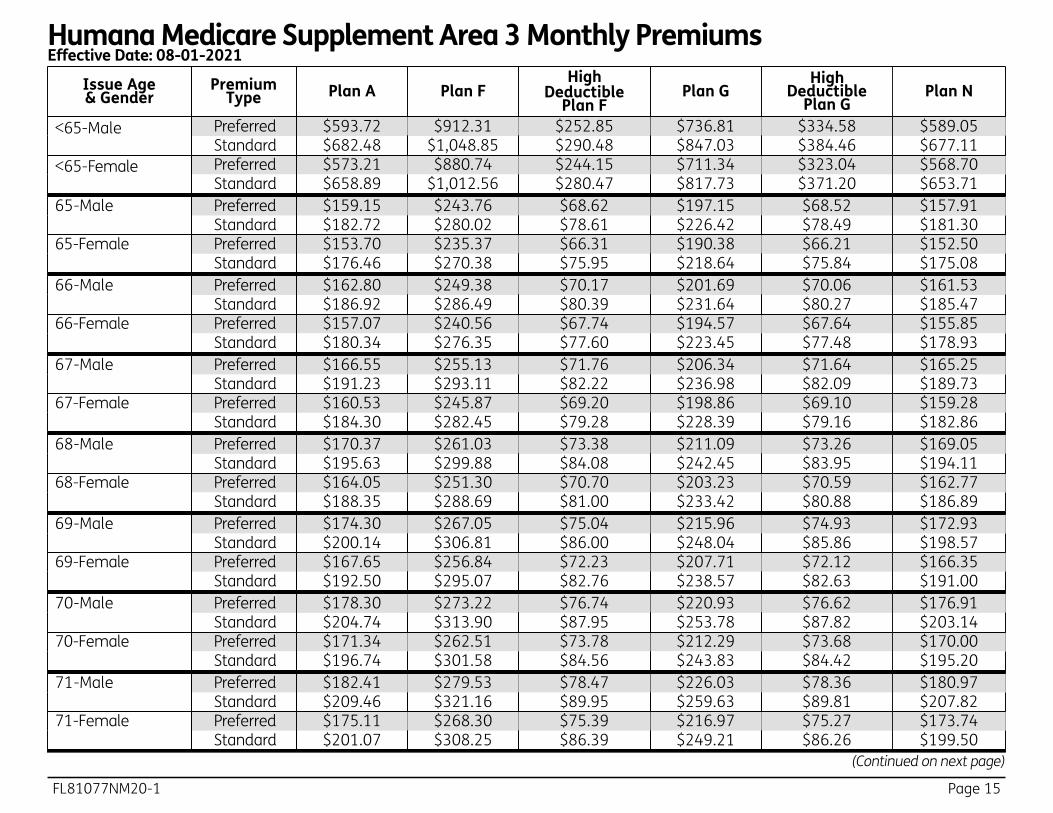
FL81077NM20-1 Page 15
Humana Medicare Supplement Area 3 Monthly PremiumsEffective Date: 08-01-2021
Issue Age & Gender
Premium Type Plan A Plan F
High Deductible
Plan FPlan G
High Deductible
Plan GPlan N
<65-Male Preferred $593.72 $912.31 $252.85 $736.81 $334.58 $589.05 Standard $682.48 $1,048.85 $290.48 $847.03 $384.46 $677.11
<65-F emale Preferred $573.21 $880.74 $244.15 $711.34 $323.04 $568.70 Standard $658.89 $1,012.56 $280.47 $817.73 $371.20 $653.71
65 -Male Preferred $159.15 $243.76 $68.62 $197.15 $68.52 $157.91 99-Male Standard $182.72 $280.02 $78.61 $226.42 $78.49 $181.30 65-Female Preferred $153.70 $235.37 $66.31 $190.38 $66.21 $152.50 99- Female Standard $176.46 $270.38 $75.95 $218.64 $75.84 $175.08 66 -Male Preferred $162.80 $249.38 $70.17 $201.69 $70.06 $161.53 99-Male Standard $186.92 $286.49 $80.39 $231.64 $80.27 $185.47 66-Female Preferred $157.07 $240.56 $67.74 $194.57 $67.64 $155.85 99- Female Standard $180.34 $276.35 $77.60 $223.45 $77.48 $178.93 67 -Male Preferred $166.55 $255.13 $71.76 $206.34 $71.64 $165.25 99-Male Standard $191.23 $293.11 $82.22 $236.98 $82.09 $189.73 67-Female Preferred $160.53 $245.87 $69.20 $198.86 $69.10 $159.28 99- Female Standard $184.30 $282.45 $79.28 $228.39 $79.16 $182.86 68 -Male Preferred $170.37 $261.03 $73.38 $211.09 $73.26 $169.05 99-Male Standard $195.63 $299.88 $84.08 $242.45 $83.95 $194.11 68-Female Preferred $164.05 $251.30 $70.70 $203.23 $70.59 $162.77 99- Female Standard $188.35 $288.69 $81.00 $233.42 $80.88 $186.89 69 -Male Preferred $174.30 $267.05 $75.04 $215.96 $74.93 $172.93 99-Male Standard $200.14 $306.81 $86.00 $248.04 $85.86 $198.57 69-Female Preferred $167.65 $256.84 $72.23 $207.71 $72.12 $166.35 99- Female Standard $192.50 $295.07 $82.76 $238.57 $82.63 $191.00 70 -Male Preferred $178.30 $273.22 $76.74 $220.93 $76.62 $176.91 99-Male Standard $204.74 $313.90 $87.95 $253.78 $87.82 $203.14 70-Female Preferred $171.34 $262.51 $73.78 $212.29 $73.68 $170.00 99- Female Standard $196.74 $301.58 $84.56 $243.83 $84.42 $195.20 71 -Male Preferred $182.41 $279.53 $78.47 $226.03 $78.36 $180.97 99-Male Standard $209.46 $321.16 $89.95 $259.63 $89.81 $207.82 71-Female Preferred $175.11 $268.30 $75.39 $216.97 $75.27 $173.74 99- Female Standard $201.07 $308.25 $86.39 $249.21 $86.26 $199.50
(Continued on next page)
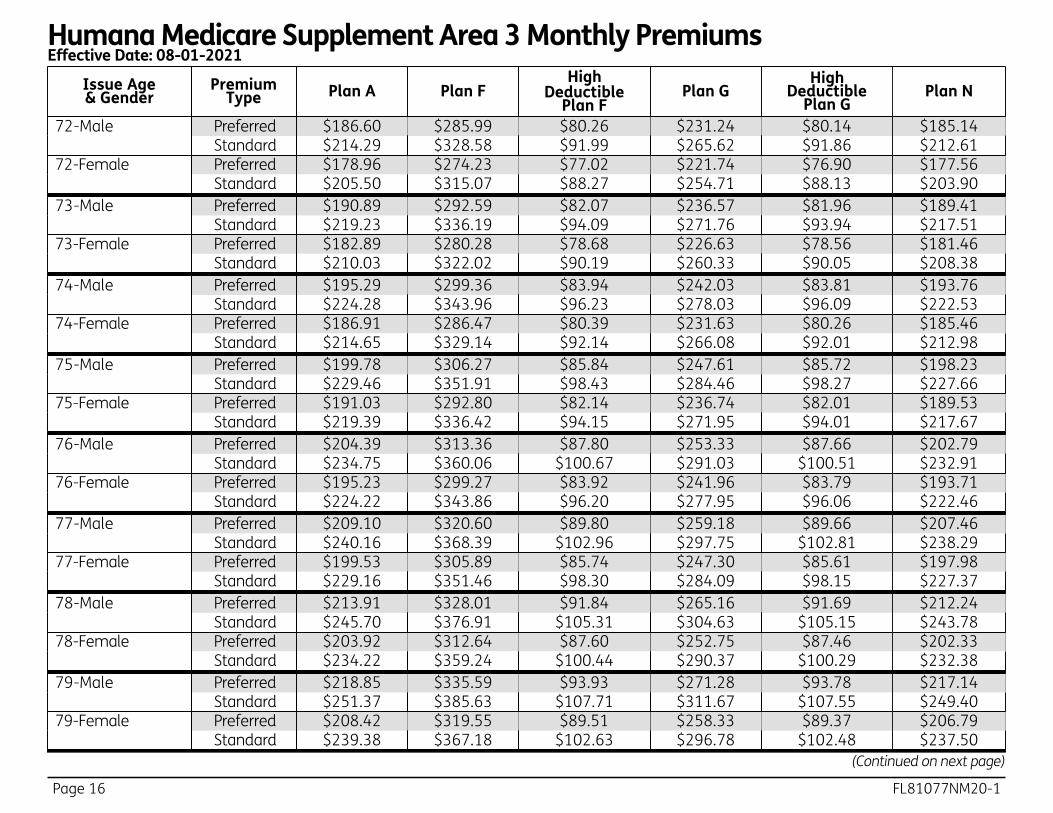
Page 16 FL81077NM20-1
Humana Medicare Supplement Area 3 Monthly PremiumsEffective Date: 08-01-2021
Issue Age & Gender
Premium Type Plan A Plan F
High Deductible
Plan FPlan G
High Deductible
Plan GPlan N
72 -Male Preferred $186.60 $285.99 $80.26 $231.24 $80.14 $185.14 99-Male Standard $214.29 $328.58 $91.99 $265.62 $91.86 $212.61 72-Female Preferred $178.96 $274.23 $77.02 $221.74 $76.90 $177.56 99- Female Standard $205.50 $315.07 $88.27 $254.71 $88.13 $203.90 73 -Male Preferred $190.89 $292.59 $82.07 $236.57 $81.96 $189.41 99-Male Standard $219.23 $336.19 $94.09 $271.76 $93.94 $217.51 73-Female Preferred $182.89 $280.28 $78.68 $226.63 $78.56 $181.46 99- Female Standard $210.03 $322.02 $90.19 $260.33 $90.05 $208.38 74 -Male Preferred $195.29 $299.36 $83.94 $242.03 $83.81 $193.76 99-Male Standard $224.28 $343.96 $96.23 $278.03 $96.09 $222.53 74-Female Preferred $186.91 $286.47 $80.39 $231.63 $80.26 $185.46 99- Female Standard $214.65 $329.14 $92.14 $266.08 $92.01 $212.98 75 -Male Preferred $199.78 $306.27 $85.84 $247.61 $85.72 $198.23 99-Male Standard $229.46 $351.91 $98.43 $284.46 $98.27 $227.66 75-Female Preferred $191.03 $292.80 $82.14 $236.74 $82.01 $189.53 99- Female Standard $219.39 $336.42 $94.15 $271.95 $94.01 $217.67 76 -Male Preferred $204.39 $313.36 $87.80 $253.33 $87.66 $202.79 99-Male Standard $234.75 $360.06 $100.67 $291.03 $100.51 $232.91 76-Female Preferred $195.23 $299.27 $83.92 $241.96 $83.79 $193.71 99- Female Standard $224.22 $343.86 $96.20 $277.95 $96.06 $222.46 77 -Male Preferred $209.10 $320.60 $89.80 $259.18 $89.66 $207.46 99-Male Standard $240.16 $368.39 $102.96 $297.75 $102.81 $238.29 77-Female Preferred $199.53 $305.89 $85.74 $247.30 $85.61 $197.98 99- Female Standard $229.16 $351.46 $98.30 $284.09 $98.15 $227.37 78 -Male Preferred $213.91 $328.01 $91.84 $265.16 $91.69 $212.24 99-Male Standard $245.70 $376.91 $105.31 $304.63 $105.15 $243.78 78-Female Preferred $203.92 $312.64 $87.60 $252.75 $87.46 $202.33 99- Female Standard $234.22 $359.24 $100.44 $290.37 $100.29 $232.38 79 -Male Preferred $218.85 $335.59 $93.93 $271.28 $93.78 $217.14 99-Male Standard $251.37 $385.63 $107.71 $311.67 $107.55 $249.40 79-Female Preferred $208.42 $319.55 $89.51 $258.33 $89.37 $206.79 99- Female Standard $239.38 $367.18 $102.63 $296.78 $102.48 $237.50
(Continued on next page)
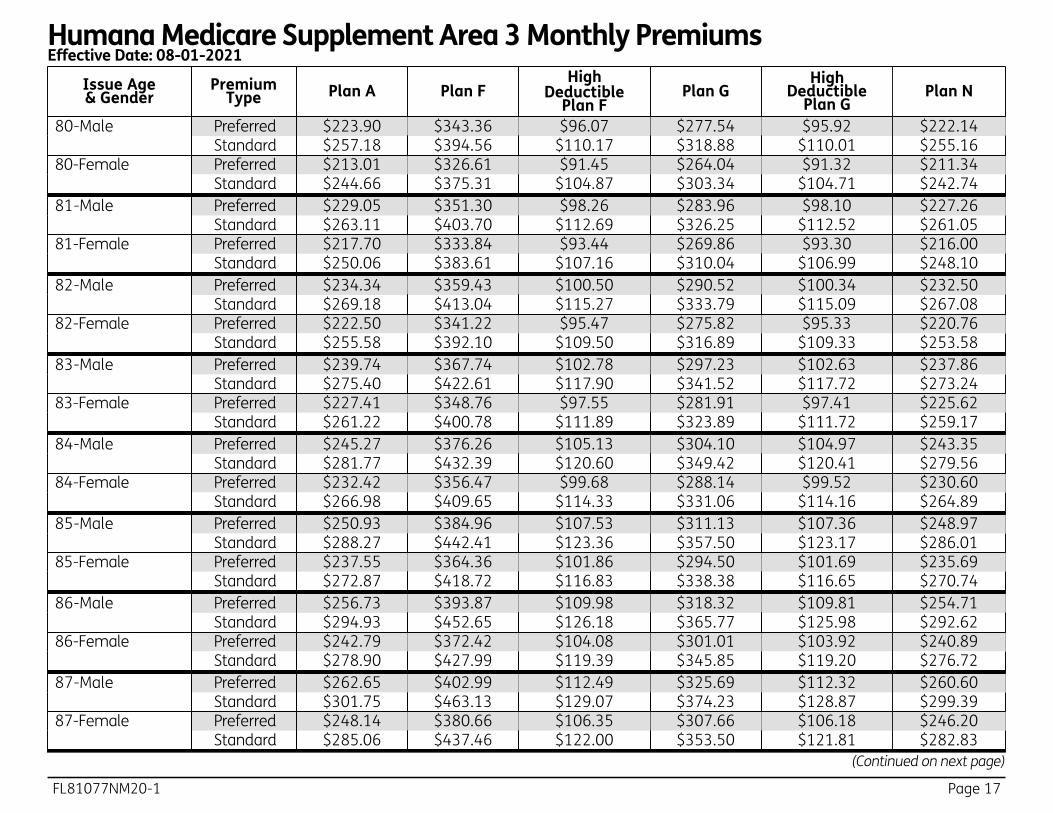
FL81077NM20-1 Page 17
Humana Medicare Supplement Area 3 Monthly PremiumsEffective Date: 08-01-2021
Issue Age & Gender
Premium Type Plan A Plan F
High Deductible
Plan FPlan G
High Deductible
Plan GPlan N
80 -Male Preferred $223.90 $343.36 $96.07 $277.54 $95.92 $222.14 99-Male Standard $257.18 $394.56 $110.17 $318.88 $110.01 $255.16 80-Female Preferred $213.01 $326.61 $91.45 $264.04 $91.32 $211.34 99- Female Standard $244.66 $375.31 $104.87 $303.34 $104.71 $242.74 81 -Male Preferred $229.05 $351.30 $98.26 $283.96 $98.10 $227.26 99-Male Standard $263.11 $403.70 $112.69 $326.25 $112.52 $261.05 81-Female Preferred $217.70 $333.84 $93.44 $269.86 $93.30 $216.00 99- Female Standard $250.06 $383.61 $107.16 $310.04 $106.99 $248.10 82 -Male Preferred $234.34 $359.43 $100.50 $290.52 $100.34 $232.50 99-Male Standard $269.18 $413.04 $115.27 $333.79 $115.09 $267.08 82-Female Preferred $222.50 $341.22 $95.47 $275.82 $95.33 $220.76 99- Female Standard $255.58 $392.10 $109.50 $316.89 $109.33 $253.58 83 -Male Preferred $239.74 $367.74 $102.78 $297.23 $102.63 $237.86 99-Male Standard $275.40 $422.61 $117.90 $341.52 $117.72 $273.24 83-Female Preferred $227.41 $348.76 $97.55 $281.91 $97.41 $225.62 99- Female Standard $261.22 $400.78 $111.89 $323.89 $111.72 $259.17 84 -Male Preferred $245.27 $376.26 $105.13 $304.10 $104.97 $243.35 99-Male Standard $281.77 $432.39 $120.60 $349.42 $120.41 $279.56 84-Female Preferred $232.42 $356.47 $99.68 $288.14 $99.52 $230.60 99- Female Standard $266.98 $409.65 $114.33 $331.06 $114.16 $264.89 85 -Male Preferred $250.93 $384.96 $107.53 $311.13 $107.36 $248.97 99-Male Standard $288.27 $442.41 $123.36 $357.50 $123.17 $286.01 85-Female Preferred $237.55 $364.36 $101.86 $294.50 $101.69 $235.69 99- Female Standard $272.87 $418.72 $116.83 $338.38 $116.65 $270.74 86 -Male Preferred $256.73 $393.87 $109.98 $318.32 $109.81 $254.71 99-Male Standard $294.93 $452.65 $126.18 $365.77 $125.98 $292.62 86-Female Preferred $242.79 $372.42 $104.08 $301.01 $103.92 $240.89 99- Female Standard $278.90 $427.99 $119.39 $345.85 $119.20 $276.72 87 -Male Preferred $262.65 $402.99 $112.49 $325.69 $112.32 $260.60 99-Male Standard $301.75 $463.13 $129.07 $374.23 $128.87 $299.39 87-Female Preferred $248.14 $380.66 $106.35 $307.66 $106.18 $246.20 99- Female Standard $285.06 $437.46 $122.00 $353.50 $121.81 $282.83
(Continued on next page)
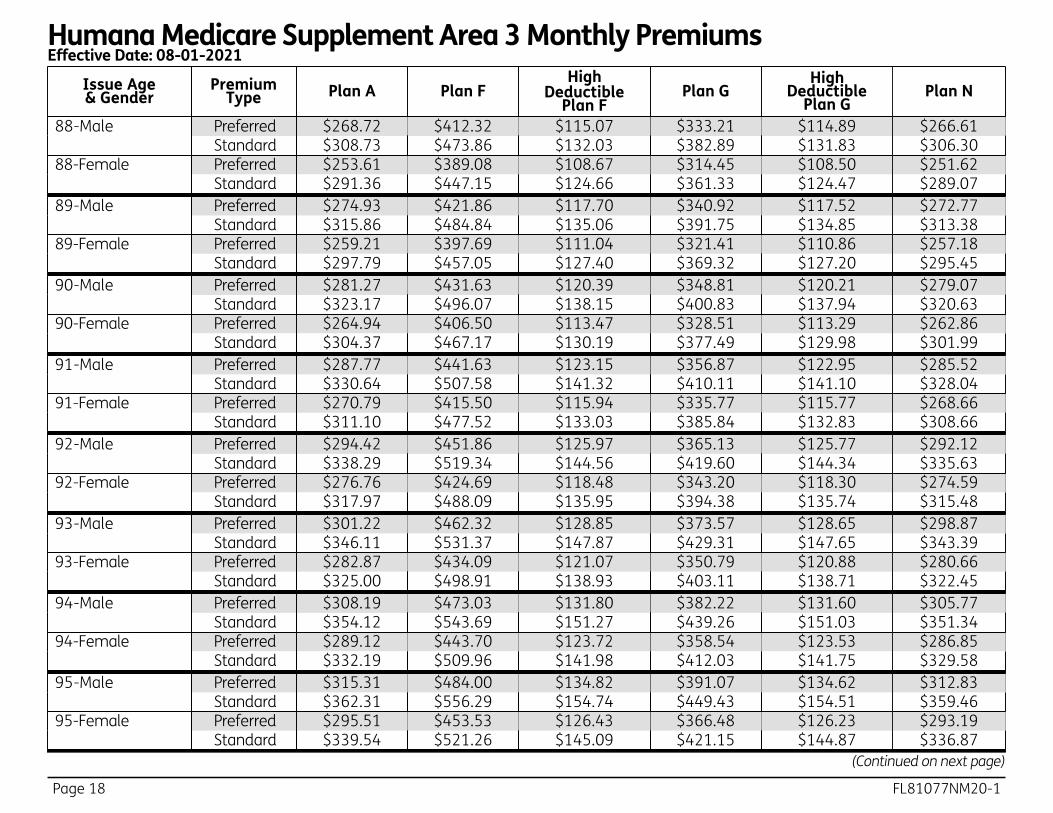
Page 18 FL81077NM20-1
Humana Medicare Supplement Area 3 Monthly PremiumsEffective Date: 08-01-2021
Issue Age & Gender
Premium Type Plan A Plan F
High Deductible
Plan FPlan G
High Deductible
Plan GPlan N
88 -Male Preferred $268.72 $412.32 $115.07 $333.21 $114.89 $266.61 99-Male Standard $308.73 $473.86 $132.03 $382.89 $131.83 $306.30 88-Female Preferred $253.61 $389.08 $108.67 $314.45 $108.50 $251.62 99- Female Standard $291.36 $447.15 $124.66 $361.33 $124.47 $289.07 89 -Male Preferred $274.93 $421.86 $117.70 $340.92 $117.52 $272.77 99-Male Standard $315.86 $484.84 $135.06 $391.75 $134.85 $313.38 89-Female Preferred $259.21 $397.69 $111.04 $321.41 $110.86 $257.18 99- Female Standard $297.79 $457.05 $127.40 $369.32 $127.20 $295.45 90 -Male Preferred $281.27 $431.63 $120.39 $348.81 $120.21 $279.07 99-Male Standard $323.17 $496.07 $138.15 $400.83 $137.94 $320.63 90-Female Preferred $264.94 $406.50 $113.47 $328.51 $113.29 $262.86 99- Female Standard $304.37 $467.17 $130.19 $377.49 $129.98 $301.99 91 -Male Preferred $287.77 $441.63 $123.15 $356.87 $122.95 $285.52 99-Male Standard $330.64 $507.58 $141.32 $410.11 $141.10 $328.04 91-Female Preferred $270.79 $415.50 $115.94 $335.77 $115.77 $268.66 99- Female Standard $311.10 $477.52 $133.03 $385.84 $132.83 $308.66 92 -Male Preferred $294.42 $451.86 $125.97 $365.13 $125.77 $292.12 99-Male Standard $338.29 $519.34 $144.56 $419.60 $144.34 $335.63 92-Female Preferred $276.76 $424.69 $118.48 $343.20 $118.30 $274.59 99- Female Standard $317.97 $488.09 $135.95 $394.38 $135.74 $315.48 93 -Male Preferred $301.22 $462.32 $128.85 $373.57 $128.65 $298.87 99-Male Standard $346.11 $531.37 $147.87 $429.31 $147.65 $343.39 93-Female Preferred $282.87 $434.09 $121.07 $350.79 $120.88 $280.66 99- Female Standard $325.00 $498.91 $138.93 $403.11 $138.71 $322.45 94 -Male Preferred $308.19 $473.03 $131.80 $382.22 $131.60 $305.77 99-Male Standard $354.12 $543.69 $151.27 $439.26 $151.03 $351.34 94-Female Preferred $289.12 $443.70 $123.72 $358.54 $123.53 $286.85 99- Female Standard $332.19 $509.96 $141.98 $412.03 $141.75 $329.58 95 -Male Preferred $315.31 $484.00 $134.82 $391.07 $134.62 $312.83 99-Male Standard $362.31 $556.29 $154.74 $449.43 $154.51 $359.46 95-Female Preferred $295.51 $453.53 $126.43 $366.48 $126.23 $293.19 99- Female Standard $339.54 $521.26 $145.09 $421.15 $144.87 $336.87
(Continued on next page)
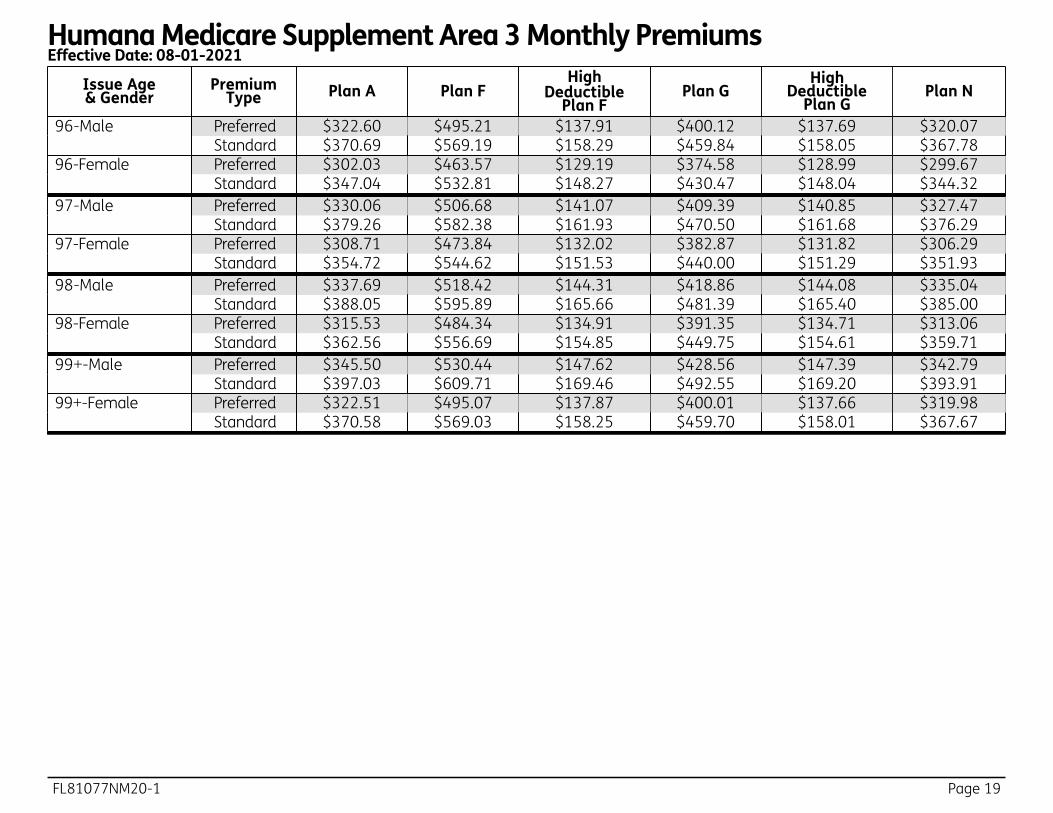
FL81077NM20-1 Page 19
Humana Medicare Supplement Area 3 Monthly PremiumsEffective Date: 08-01-2021
Issue Age & Gender
Premium Type Plan A Plan F
High Deductible
Plan FPlan G
High Deductible
Plan GPlan N
96 -Male Preferred $322.60 $495.21 $137.91 $400.12 $137.69 $320.07 99-Male Standard $370.69 $569.19 $158.29 $459.84 $158.05 $367.78 96-Female Preferred $302.03 $463.57 $129.19 $374.58 $128.99 $299.67 99- Female Standard $347.04 $532.81 $148.27 $430.47 $148.04 $344.32 97 -Male Preferred $330.06 $506.68 $141.07 $409.39 $140.85 $327.47 99-Male Standard $379.26 $582.38 $161.93 $470.50 $161.68 $376.29 97-Female Preferred $308.71 $473.84 $132.02 $382.87 $131.82 $306.29 99- Female Standard $354.72 $544.62 $151.53 $440.00 $151.29 $351.93 98 -Male Preferred $337.69 $518.42 $144.31 $418.86 $144.08 $335.04 99-Male Standard $388.05 $595.89 $165.66 $481.39 $165.40 $385.00 98-Female Preferred $315.53 $484.34 $134.91 $391.35 $134.71 $313.06 99- Female Standard $362.56 $556.69 $154.85 $449.75 $154.61 $359.71 99 +-Male Preferred $345.50 $530.44 $147.62 $428.56 $147.39 $342.79 99-Male Standard $397.03 $609.71 $169.46 $492.55 $169.20 $393.91 99+-Female Preferred $322.51 $495.07 $137.87 $400.01 $137.66 $319.98 99- Female Standard $370.58 $569.03 $158.25 $459.70 $158.01 $367.67

Page 20 FL81077NM20-1
Plan AMedicare (Part A) - Hospital Services - Per Benefit Period * A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and
have not received skilled care in any other facility for 60 days in a row.
Services Medicare Pays Plan Pays You Pay Hospitalization* Semiprivate room and board, general nursing and miscellaneous services and supplies First 60 days All but $1,484 $0 $1,484
(Part A deductible) 61st through 90th day All but $371 a day $371 a day $0 91st day and after:
while using 60 lifetime reserve days once lifetime reserve days are used:
All but $742 a day $742 a day $0
• additional 365 days $0 100% of Medicare eligible expenses
$0**
• beyond the additional 365 days $0 $0 All costs
Skilled Nursing Facility Care* You must meet Medicare's requirements, including having been in a hospital for at least three days and entered a Medicare-approved facility within 30 days after leaving the hospital First 20 days All approved
amounts $0 $0
21st through 100th day All but $185.50 a day
$0 Up to $185.50 a day
101st day and after $0 $0 All costs
Blood First three pints $0 Three pints $0 Additional amounts 100% $0 $0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy's "Core Benefits." During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
FL81077NM20-1 Page 21
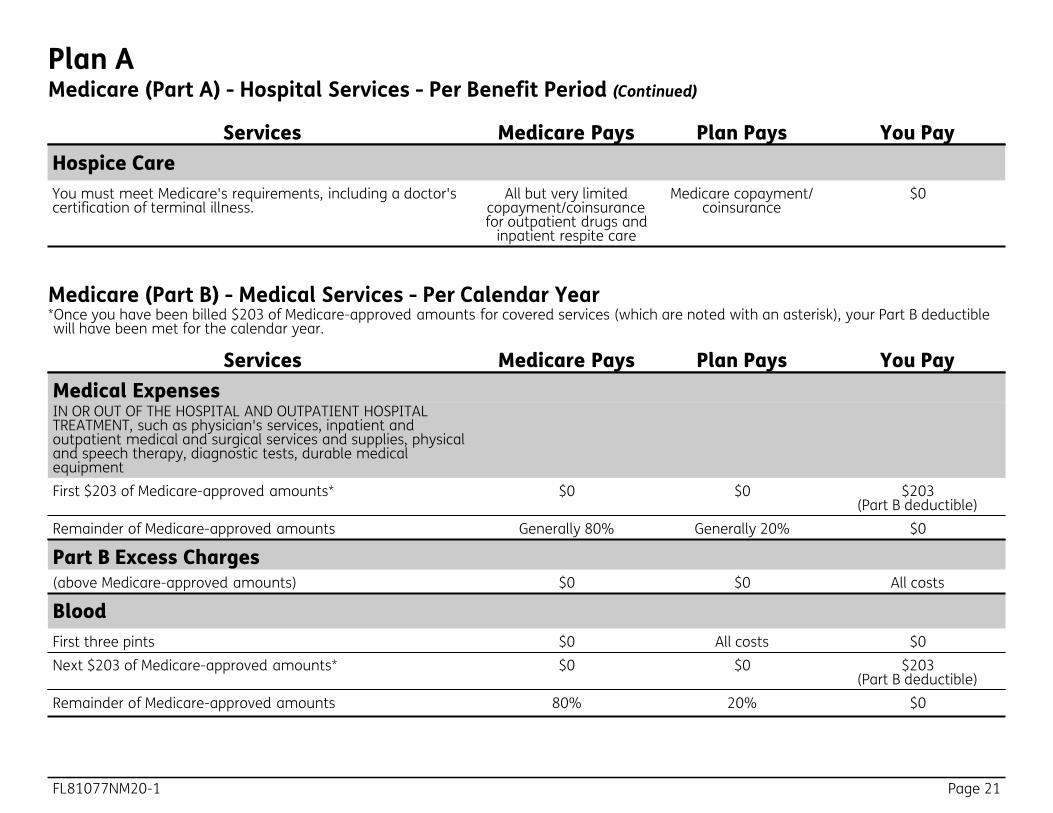
Plan AMedicare (Part A) - Hospital Services - Per Benefit Period (Continued)
Services Medicare Pays Plan Pays You Pay Hospice Care You must meet Medicare's requirements, including a doctor's certification of terminal illness.
All but very limited copayment/coinsurance for outpatient drugs and
inpatient respite care
Medicare copayment/ coinsurance
$0
Medicare (Part B) - Medical Services - Per Calendar Year
Services Medicare Pays Plan Pays You Pay Medical Expenses IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as physician's services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment First $203 of Medicare-approved amounts* $0 $0 $203
(Part B deductible) Remainder of Medicare-approved amounts Generally 80% Generally 20% $0
Part B Excess Charges (above Medicare-approved amounts) $0 $0 All costs
Blood First three pints $0 All costs $0 Next $203 of Medicare-approved amounts* $0 $0 $203
(Part B deductible) Remainder of Medicare-approved amounts 80% 20% $0
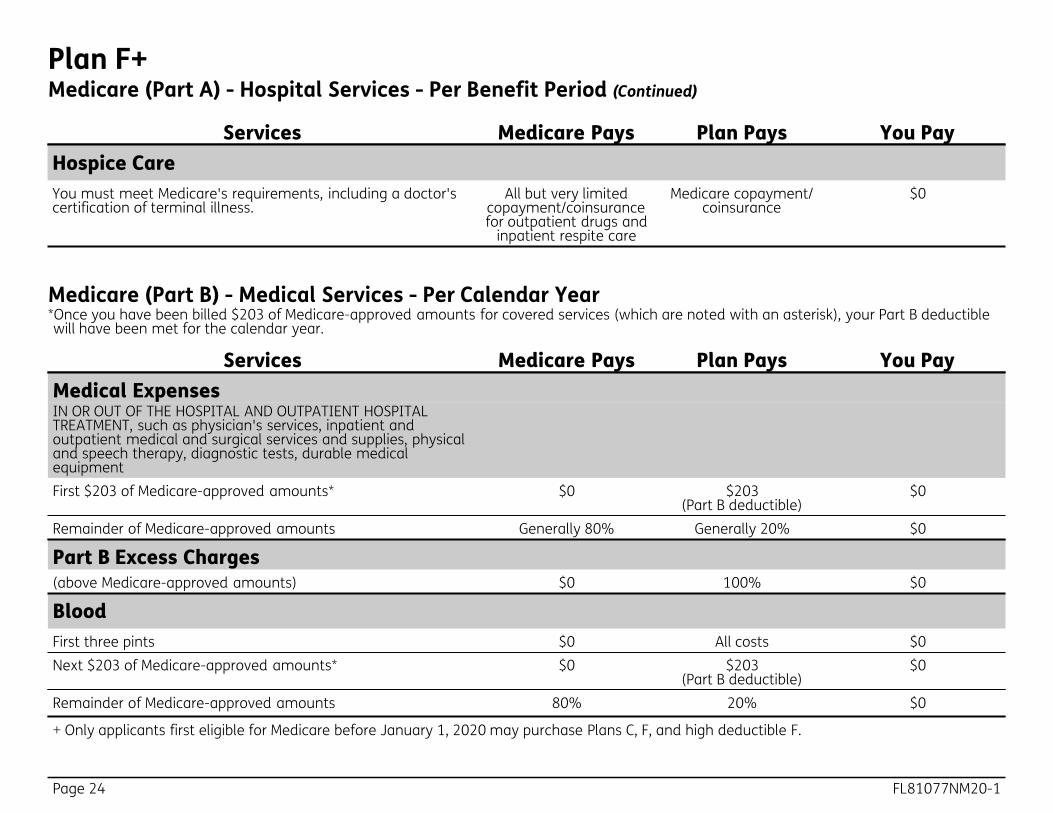
*Once you have been billed $203 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
Page 22 FL81077NM20-1
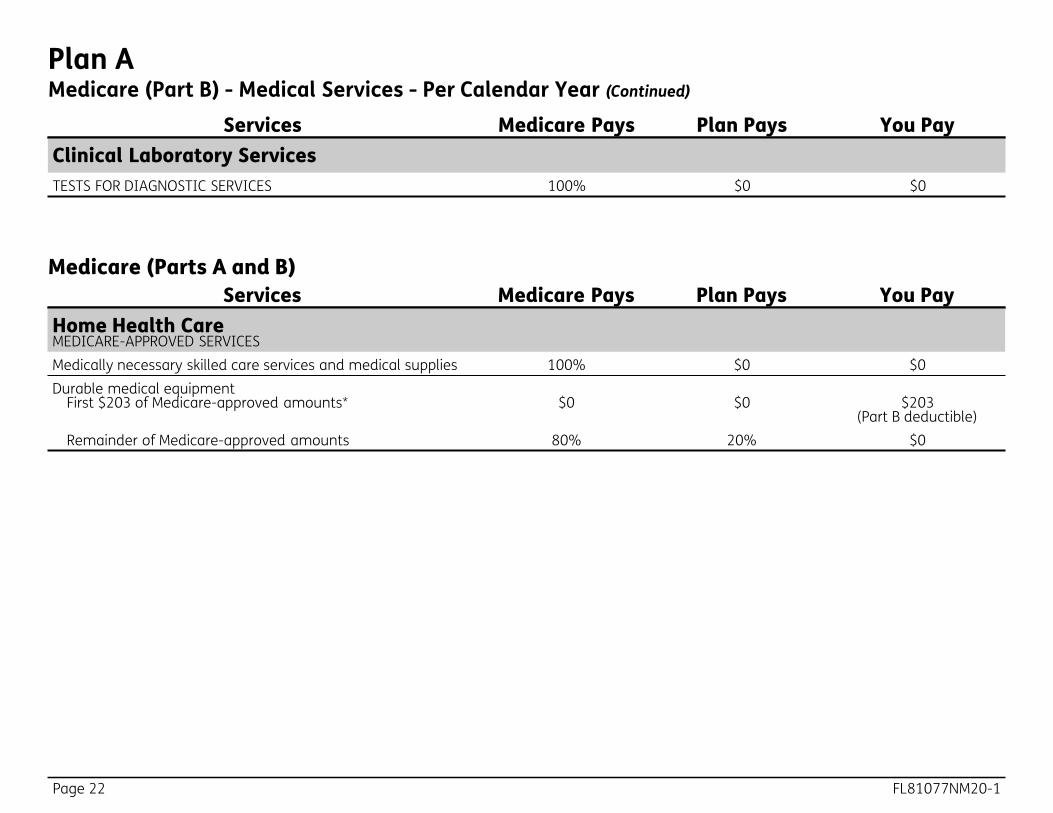
Plan AMedicare (Part B) - Medical Services - Per Calendar Year (Continued)
Services Medicare Pays Plan Pays You Pay Clinical Laboratory Services TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
Services Medicare Pays Plan Pays You Pay Home Health Care MEDICARE-APPROVED SERVICES Medically necessary skilled care services and medical supplies 100% $0 $0 Durable medical equipment
First $203 of Medicare-approved amounts* $0 $0 $203 (Part B deductible)
Remainder of Medicare-approved amounts 80% 20% $0
Medicare (Parts A and B)

FL81077NM20-1 Page 23
Plan F+Medicare (Part A) - Hospital Services - Per Benefit Period * A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and
have not received skilled care in any other facility for 60 days in a row.
Services Medicare Pays Plan Pays You Pay Hospitalization* Semiprivate room and board, general nursing and miscellaneous services and supplies First 60 days All but $1,484 $1,484
(Part A deductible) $0
61st through 90th day All but $371 a day $371 a day $0 91st day and after:
while using 60 lifetime reserve days once lifetime reserve days are used:
All but $742 a day $742 a day $0
• additional 365 days $0 100% of Medicare eligible expenses
$0**
• beyond the additional 365 days $0 $0 All costs
Skilled Nursing Facility Care* You must meet Medicare's requirements, including having been in a hospital for at least three days and entered a Medicare-approved facility within 30 days after leaving the hospital First 20 days All approved
amounts $0 $0
21st through 100th day All but $185.50 a day
Up to $185.50 a day
$0
101st day and after $0 $0 All costs
Blood First three pints $0 Three pints $0 Additional amounts 100% $0 $0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy's "Core Benefits." During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
+ Only applicants first eligible for Medicare before January 1, 2020 may purchase Plans C, F, and high deductible F.
Page 24 FL81077NM20-1
Plan F+Medicare (Part A) - Hospital Services - Per Benefit Period (Continued)
Services Medicare Pays Plan Pays You Pay Hospice Care You must meet Medicare's requirements, including a doctor's certification of terminal illness.
All but very limited copayment/coinsurance for outpatient drugs and
inpatient respite care
Medicare copayment/ coinsurance
$0
Services Medicare Pays Plan Pays You Pay Medical Expenses IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as physician's services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment First $203 of Medicare-approved amounts* $0 $203
(Part B deductible) $0
Remainder of Medicare-approved amounts Generally 80% Generally 20% $0
Part B Excess Charges (above Medicare-approved amounts) $0 100% $0
Blood First three pints $0 All costs $0 Next $203 of Medicare-approved amounts* $0 $203
(Part B deductible) $0
Remainder of Medicare-approved amounts 80% 20% $0
+ Only applicants first eligible for Medicare before January 1, 2020 may purchase Plans C, F, and high deductible F.
Medicare (Part B) - Medical Services - Per Calendar Year *Once you have been billed $203 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
FL81077NM20-1 Page 25
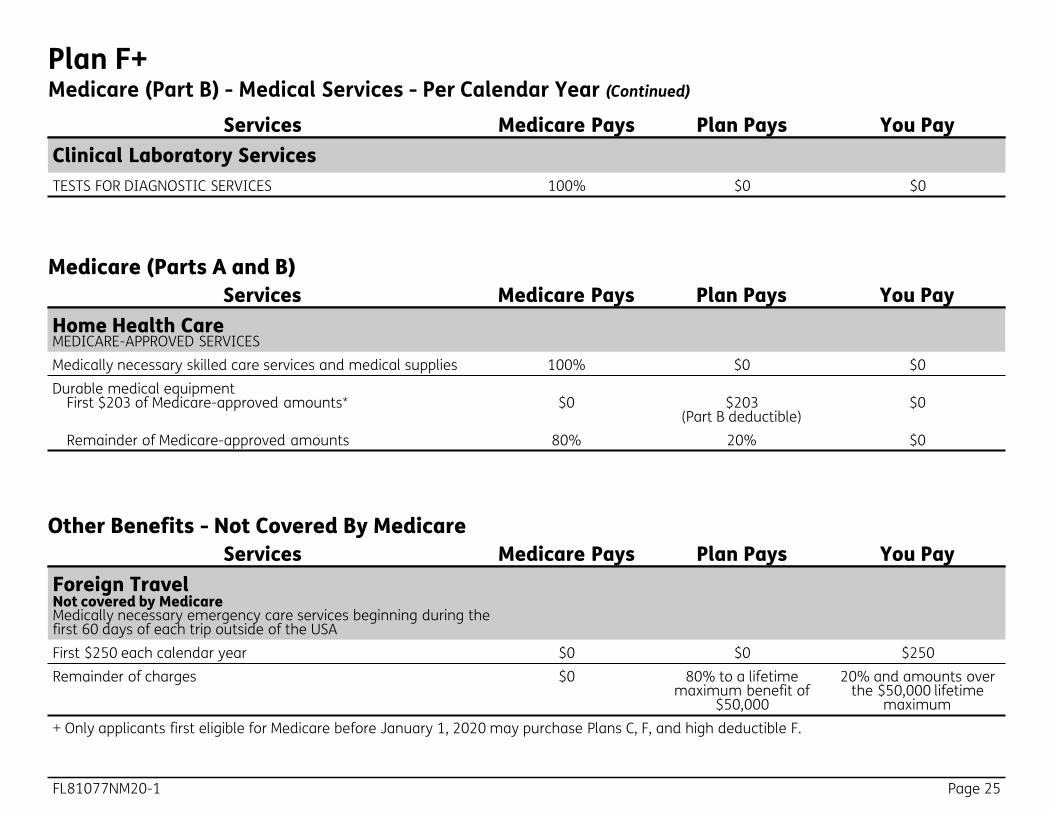
Plan F+Medicare (Part B) - Medical Services - Per Calendar Year (Continued)
Services Medicare Pays Plan Pays You Pay Clinical Laboratory Services TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
Services Medicare Pays Plan Pays You Pay Home Health Care MEDICARE-APPROVED SERVICES Medically necessary skilled care services and medical supplies 100% $0 $0 Durable medical equipment
First $203 of Medicare-approved amounts* $0 $203 (Part B deductible)
$0
Remainder of Medicare-approved amounts 80% 20% $0
Medicare (Parts A and B)
Services Medicare Pays Plan Pays You Pay Foreign Travel Not covered by Medicare Medically necessary emergency care services beginning during the first 60 days of each trip outside of the USA First $250 each calendar year $0 $0 $250 Remainder of charges $0 80% to a lifetime
maximum benefit of $50,000
20% and amounts over the $50,000 lifetime
maximum + Only applicants first eligible for Medicare before January 1, 2020 may purchase Plans C, F, and high deductible F.
Other Benefits - Not Covered By Medicare
Page 26 FL81077NM20-1
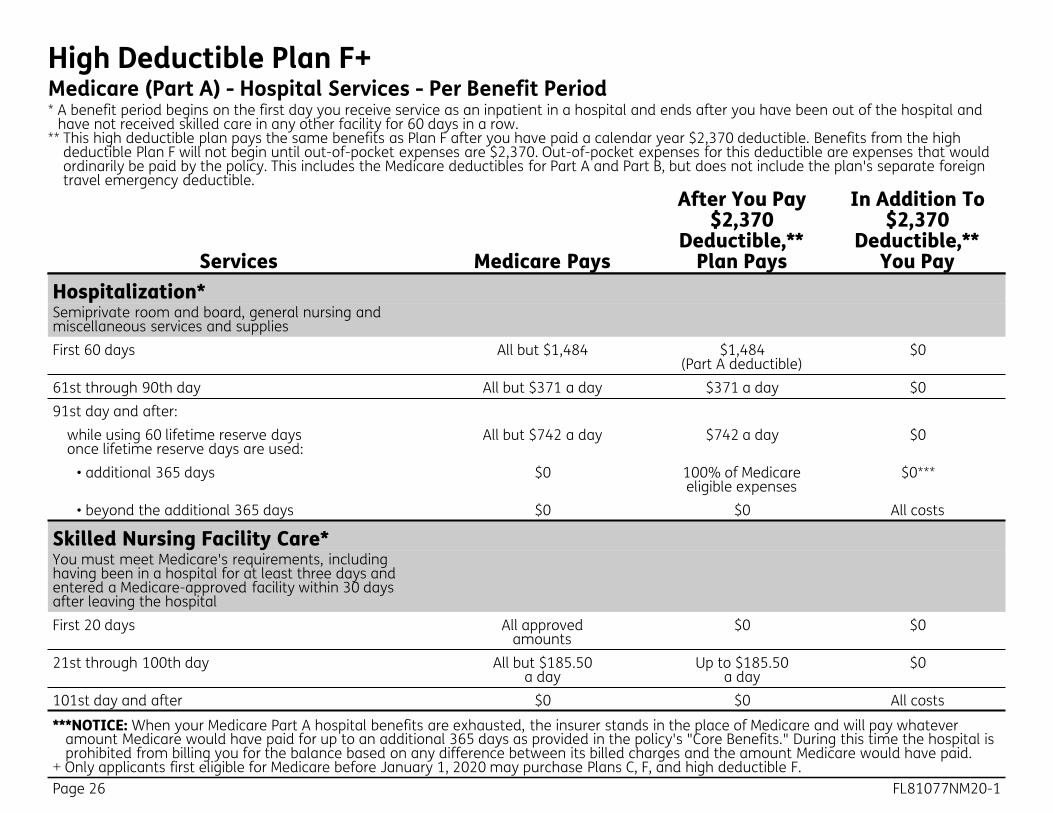
High Deductible Plan F+Medicare (Part A) - Hospital Services - Per Benefit Period * A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and
have not received skilled care in any other facility for 60 days in a row. ** This high deductible plan pays the same benefits as Plan F after you have paid a calendar year $2,370 deductible. Benefits from the high
deductible Plan F will not begin until out-of-pocket expenses are $2,370. Out-of-pocket expenses for this deductible are expenses that would ordinarily be paid by the policy. This includes the Medicare deductibles for Part A and Part B, but does not include the plan's separate foreign travel emergency deductible.
Services Medicare Pays
After You Pay $2,370
Deductible,** Plan Pays
In Addition To $2,370
Deductible,** You Pay
Hospitalization* Semiprivate room and board, general nursing and miscellaneous services and supplies First 60 days All but $1,484 $1,484
(Part A deductible) $0
61st through 90th day All but $371 a day $371 a day $0 91st day and after:
while using 60 lifetime reserve days once lifetime reserve days are used:
All but $742 a day $742 a day $0
• additional 365 days $0 100% of Medicare eligible expenses
$0***
• beyond the additional 365 days $0 $0 All costs
Skilled Nursing Facility Care* You must meet Medicare's requirements, including having been in a hospital for at least three days and entered a Medicare-approved facility within 30 days after leaving the hospital First 20 days All approved
amounts $0 $0
21st through 100th day All but $185.50 a day
Up to $185.50 a day
$0
101st day and after $0 $0 All costs
***NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy's "Core Benefits." During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
+ Only applicants first eligible for Medicare before January 1, 2020 may purchase Plans C, F, and high deductible F.
FL81077NM20-1 Page 27
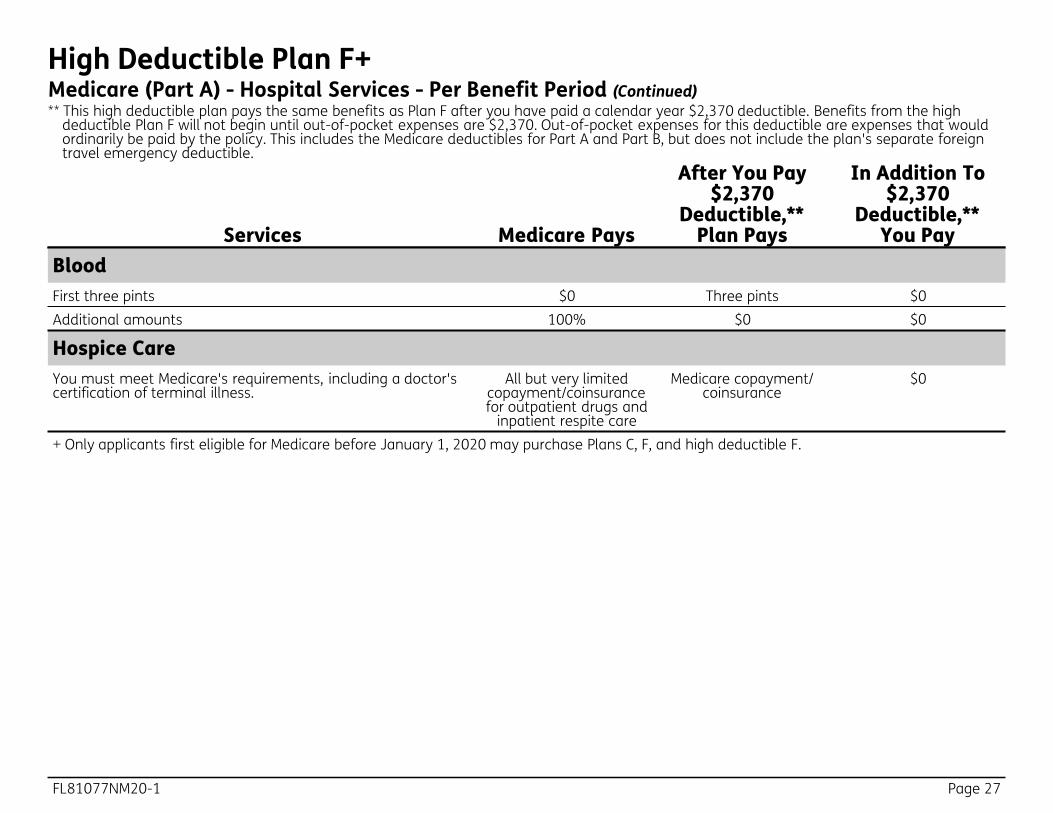
High Deductible Plan F+Medicare (Part A) - Hospital Services - Per Benefit Period (Continued) ** This high deductible plan pays the same benefits as Plan F after you have paid a calendar year $2,370 deductible. Benefits from the high
deductible Plan F will not begin until out-of-pocket expenses are $2,370. Out-of-pocket expenses for this deductible are expenses that would ordinarily be paid by the policy. This includes the Medicare deductibles for Part A and Part B, but does not include the plan's separate foreign travel emergency deductible.
Services Medicare Pays
After You Pay $2,370
Deductible,** Plan Pays
In Addition To $2,370
Deductible,** You Pay
Blood First three pints $0 Three pints $0 Additional amounts 100% $0 $0
Hospice Care You must meet Medicare's requirements, including a doctor's certification of terminal illness.
All but very limited copayment/coinsurance for outpatient drugs and
inpatient respite care
Medicare copayment/ coinsurance
$0
+ Only applicants first eligible for Medicare before January 1, 2020 may purchase Plans C, F, and high deductible F.
Page 28 FL81077NM20-1
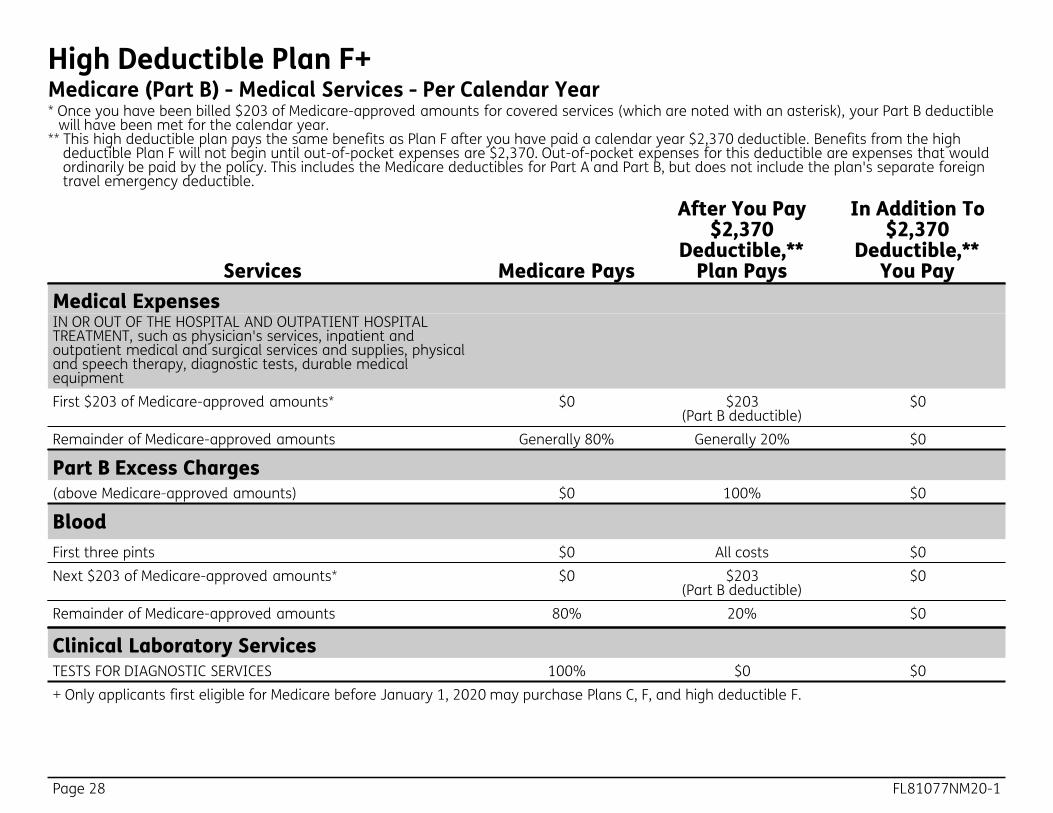
High Deductible Plan F+Medicare (Part B) - Medical Services - Per Calendar Year * Once you have been billed $203 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible
will have been met for the calendar year. ** This high deductible plan pays the same benefits as Plan F after you have paid a calendar year $2,370 deductible. Benefits from the high
deductible Plan F will not begin until out-of-pocket expenses are $2,370. Out-of-pocket expenses for this deductible are expenses that would ordinarily be paid by the policy. This includes the Medicare deductibles for Part A and Part B, but does not include the plan's separate foreign travel emergency deductible.
Services Medicare Pays
After You Pay $2,370
Deductible,** Plan Pays
In Addition To $2,370
Deductible,** You Pay
Medical Expenses IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as physician's services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment First $203 of Medicare-approved amounts* $0 $203
(Part B deductible) $0
Remainder of Medicare-approved amounts Generally 80% Generally 20% $0
Part B Excess Charges (above Medicare-approved amounts) $0 100% $0
Blood First three pints $0 All costs $0 Next $203 of Medicare-approved amounts* $0 $203
(Part B deductible) $0
Remainder of Medicare-approved amounts 80% 20% $0
Clinical Laboratory Services TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0 + Only applicants first eligible for Medicare before January 1, 2020 may purchase Plans C, F, and high deductible F.
FL81077NM20-1 Page 29
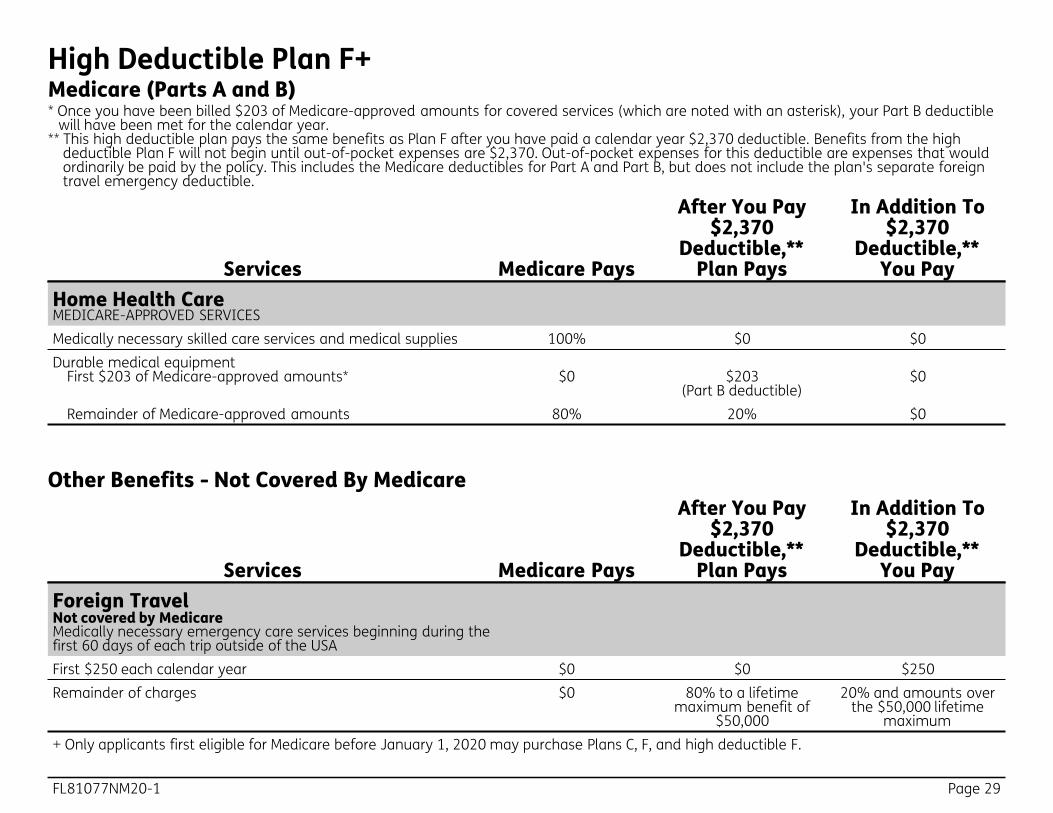
High Deductible Plan F+
Services Medicare Pays
After You Pay $2,370
Deductible,** Plan Pays
In Addition To $2,370
Deductible,** You Pay
Home Health Care MEDICARE-APPROVED SERVICES Medically necessary skilled care services and medical supplies 100% $0 $0 Durable medical equipment
First $203 of Medicare-approved amounts* $0 $203 (Part B deductible)
$0
Remainder of Medicare-approved amounts 80% 20% $0
Medicare (Parts A and B) * Once you have been billed $203 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible
will have been met for the calendar year. ** This high deductible plan pays the same benefits as Plan F after you have paid a calendar year $2,370 deductible. Benefits from the high
deductible Plan F will not begin until out-of-pocket expenses are $2,370. Out-of-pocket expenses for this deductible are expenses that would ordinarily be paid by the policy. This includes the Medicare deductibles for Part A and Part B, but does not include the plan's separate foreign travel emergency deductible.
Services Medicare Pays
After You Pay $2,370
Deductible,** Plan Pays
In Addition To $2,370
Deductible,** You Pay
Foreign Travel Not covered by Medicare Medically necessary emergency care services beginning during the first 60 days of each trip outside of the USA First $250 each calendar year $0 $0 $250 Remainder of charges $0 80% to a lifetime
maximum benefit of $50,000
20% and amounts over the $50,000 lifetime
maximum + Only applicants first eligible for Medicare before January 1, 2020 may purchase Plans C, F, and high deductible F.
Other Benefits - Not Covered By Medicare
Page 30 FL81077NM20-1
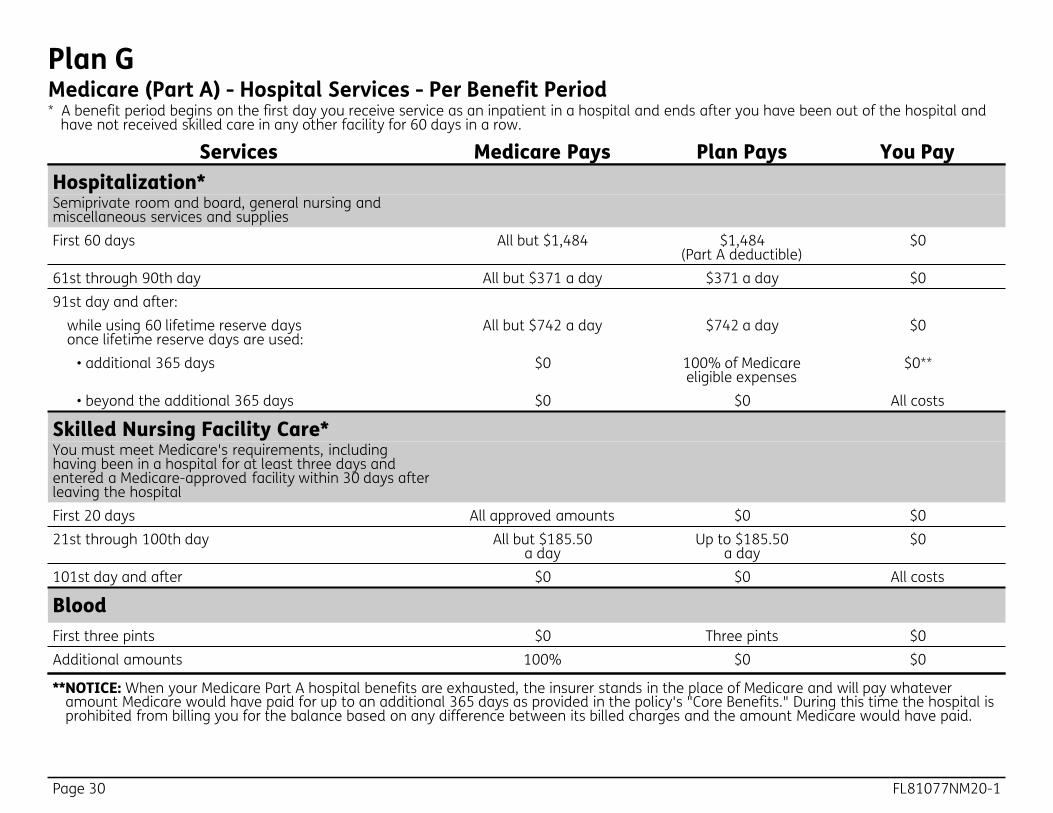
Plan GMedicare (Part A) - Hospital Services - Per Benefit Period * A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and
have not received skilled care in any other facility for 60 days in a row.
Services Medicare Pays Plan Pays You Pay Hospitalization* Semiprivate room and board, general nursing and miscellaneous services and supplies First 60 days All but $1,484 $1,484
(Part A deductible) $0
61st through 90th day All but $371 a day $371 a day $0 91st day and after:
while using 60 lifetime reserve days once lifetime reserve days are used:
All but $742 a day $742 a day $0
• additional 365 days $0 100% of Medicare eligible expenses
$0**
• beyond the additional 365 days $0 $0 All costs
Skilled Nursing Facility Care* You must meet Medicare's requirements, including having been in a hospital for at least three days and entered a Medicare-approved facility within 30 days after leaving the hospital First 20 days All approved amounts $0 $0 21st through 100th day All but $185.50
a day Up to $185.50
a day $0
101st day and after $0 $0 All costs
Blood First three pints $0 Three pints $0 Additional amounts 100% $0 $0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy's "Core Benefits." During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
FL81077NM20-1 Page 31
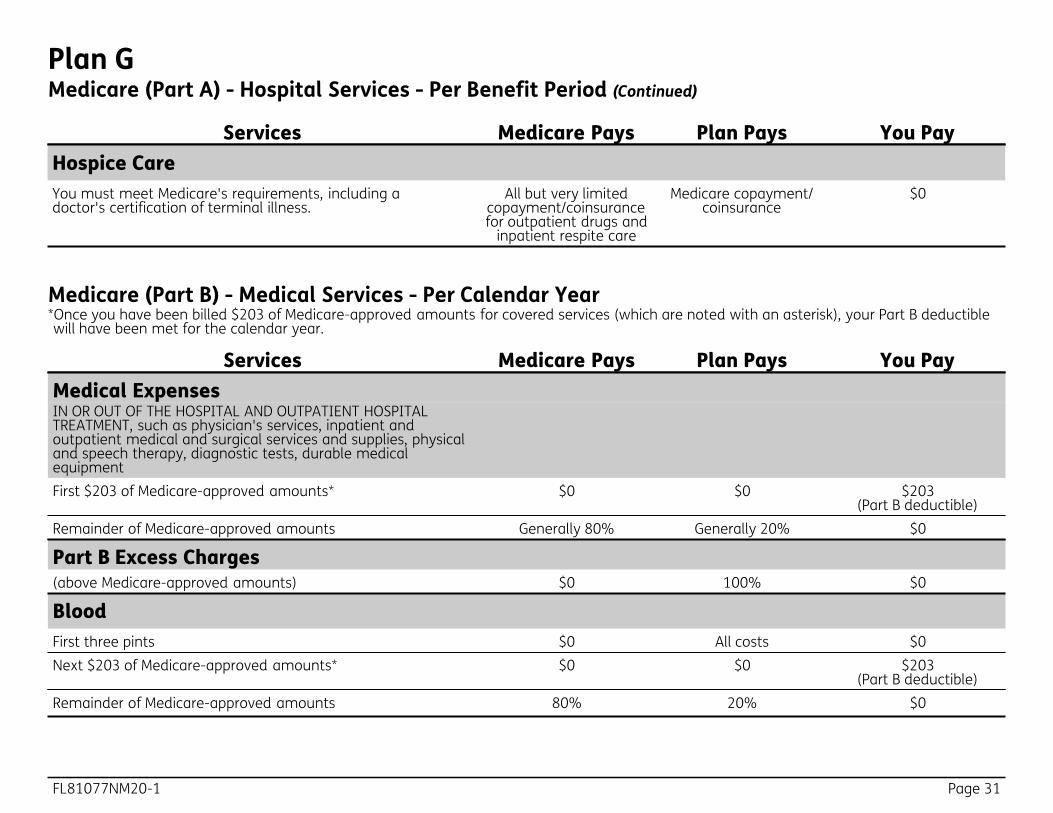
Plan GMedicare (Part A) - Hospital Services - Per Benefit Period (Continued)
Services Medicare Pays Plan Pays You Pay Hospice Care You must meet Medicare's requirements, including a doctor's certification of terminal illness.
All but very limited copayment/coinsurance for outpatient drugs and
inpatient respite care
Medicare copayment/ coinsurance
$0
Medicare (Part B) - Medical Services - Per Calendar Year
Services Medicare Pays Plan Pays You Pay Medical Expenses IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as physician's services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment First $203 of Medicare-approved amounts* $0 $0 $203
(Part B deductible) Remainder of Medicare-approved amounts Generally 80% Generally 20% $0
Part B Excess Charges (above Medicare-approved amounts) $0 100% $0
Blood First three pints $0 All costs $0 Next $203 of Medicare-approved amounts* $0 $0 $203
(Part B deductible) Remainder of Medicare-approved amounts 80% 20% $0
*Once you have been billed $203 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.

Page 32 FL81077NM20-1
Plan GMedicare (Part B) - Medical Services - Per Calendar Year (Continued)
Services Medicare Pays Plan Pays You Pay Clinical Laboratory Services TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
Services Medicare Pays Plan Pays You Pay Foreign Travel Not covered by Medicare Medically necessary emergency care services beginning during the first 60 days of each trip outside of the USA First $250 each calendar year $0 $0 $250 Remainder of charges $0 80% to a lifetime
maximum benefit of $50,000
20% and amounts over the $50,000 lifetime
maximum
Other Benefits - Not Covered By Medicare
Services Medicare Pays Plan Pays You Pay Home Health Care MEDICARE-APPROVED SERVICES Medically necessary skilled care services and medical supplies 100% $0 $0 Durable medical equipment
First $203 of Medicare-approved amounts* $0 $0 $203 (Part B deductible)
Remainder of Medicare-approved amounts 80% 20% $0
Medicare (Parts A and B)
FL81077NM20-1 Page 33
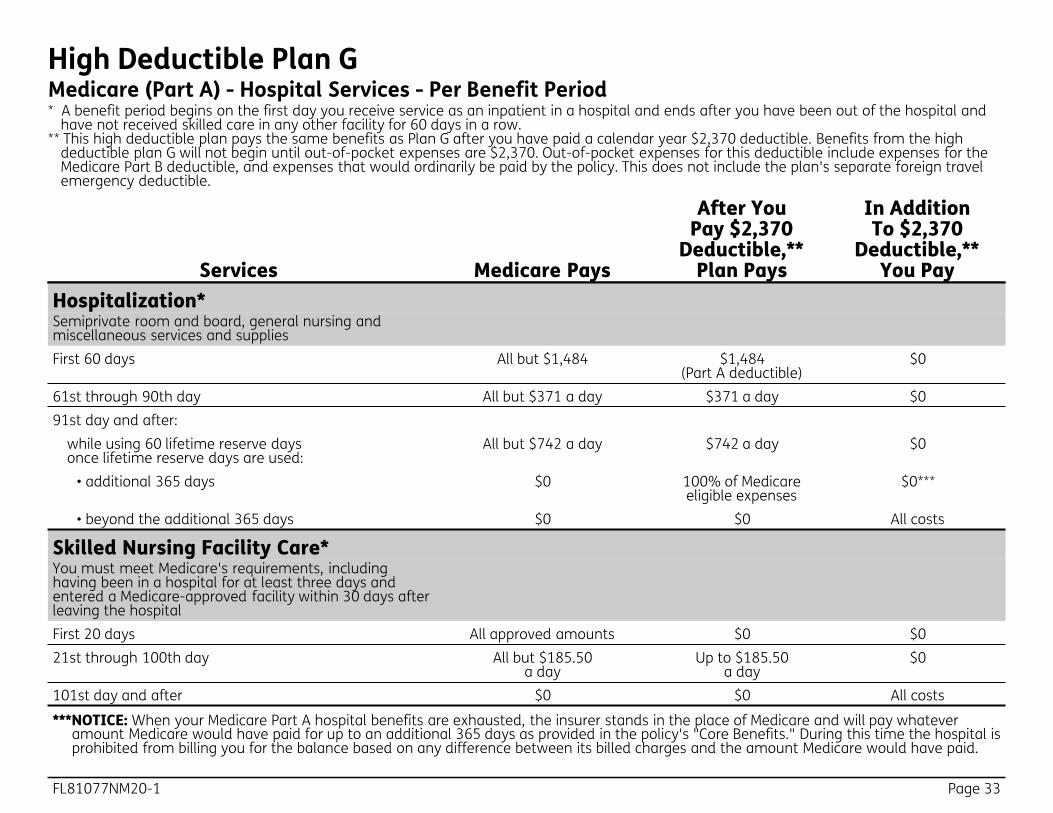
High Deductible Plan GMedicare (Part A) - Hospital Services - Per Benefit Period * A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and
have not received skilled care in any other facility for 60 days in a row. ** This high deductible plan pays the same benefits as Plan G after you have paid a calendar year $2,370 deductible. Benefits from the high
deductible plan G will not begin until out-of-pocket expenses are $2,370. Out-of-pocket expenses for this deductible include expenses for the Medicare Part B deductible, and expenses that would ordinarily be paid by the policy. This does not include the plan's separate foreign travel emergency deductible.
Services Medicare Pays
After You Pay $2,370
Deductible,** Plan Pays
In Addition To $2,370
Deductible,** You Pay
Hospitalization* Semiprivate room and board, general nursing and miscellaneous services and supplies First 60 days All but $1,484 $1,484
(Part A deductible) $0
61st through 90th day All but $371 a day $371 a day $0 91st day and after:
while using 60 lifetime reserve days once lifetime reserve days are used:
All but $742 a day $742 a day $0
• additional 365 days $0 100% of Medicare eligible expenses
$0***
• beyond the additional 365 days $0 $0 All costs
Skilled Nursing Facility Care* You must meet Medicare's requirements, including having been in a hospital for at least three days and entered a Medicare-approved facility within 30 days after leaving the hospital First 20 days All approved amounts $0 $0 21st through 100th day All but $185.50
a day Up to $185.50
a day $0
101st day and after $0 $0 All costs
***NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy's "Core Benefits." During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
Page 34 FL81077NM20-1
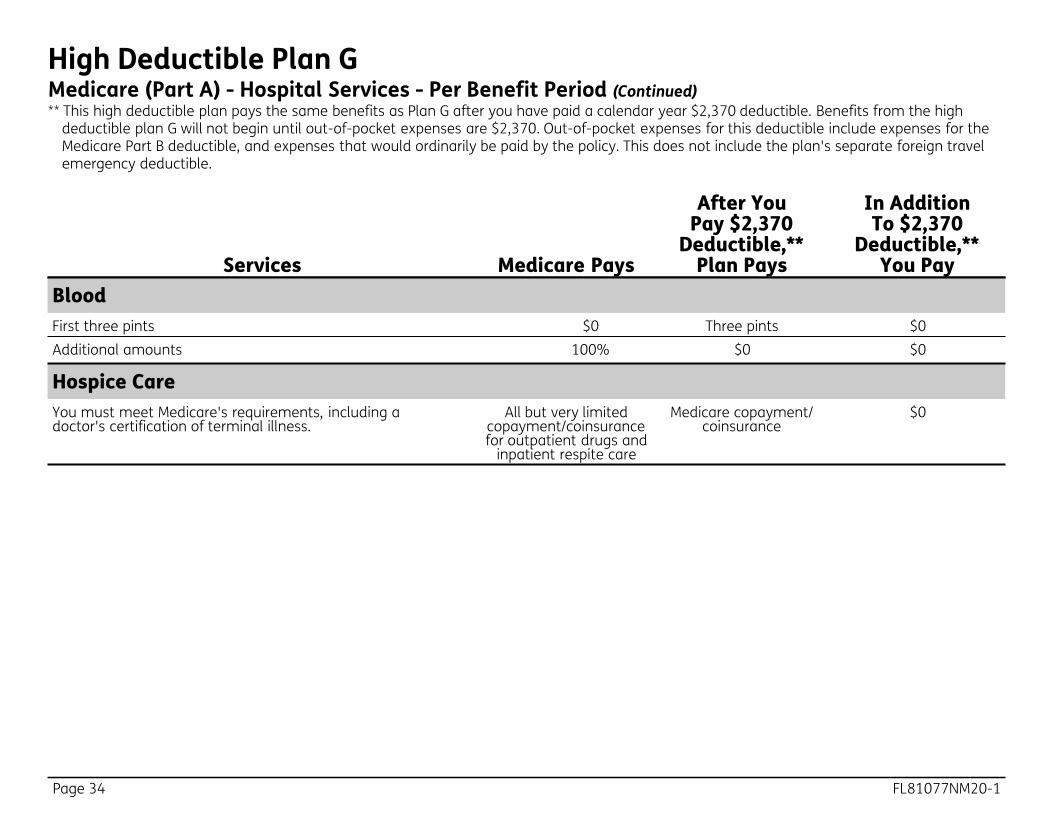
High Deductible Plan GMedicare (Part A) - Hospital Services - Per Benefit Period (Continued) ** This high deductible plan pays the same benefits as Plan G after you have paid a calendar year $2,370 deductible. Benefits from the high
deductible plan G will not begin until out-of-pocket expenses are $2,370. Out-of-pocket expenses for this deductible include expenses for the Medicare Part B deductible, and expenses that would ordinarily be paid by the policy. This does not include the plan's separate foreign travel emergency deductible.
Services Medicare Pays
After You Pay $2,370
Deductible,** Plan Pays
In Addition To $2,370
Deductible,** You Pay
Blood First three pints $0 Three pints $0 Additional amounts 100% $0 $0
Hospice Care You must meet Medicare's requirements, including a doctor's certification of terminal illness.
All but very limited copayment/coinsurance for outpatient drugs and
inpatient respite care
Medicare copayment/ coinsurance
$0
FL81077NM20-1 Page 35
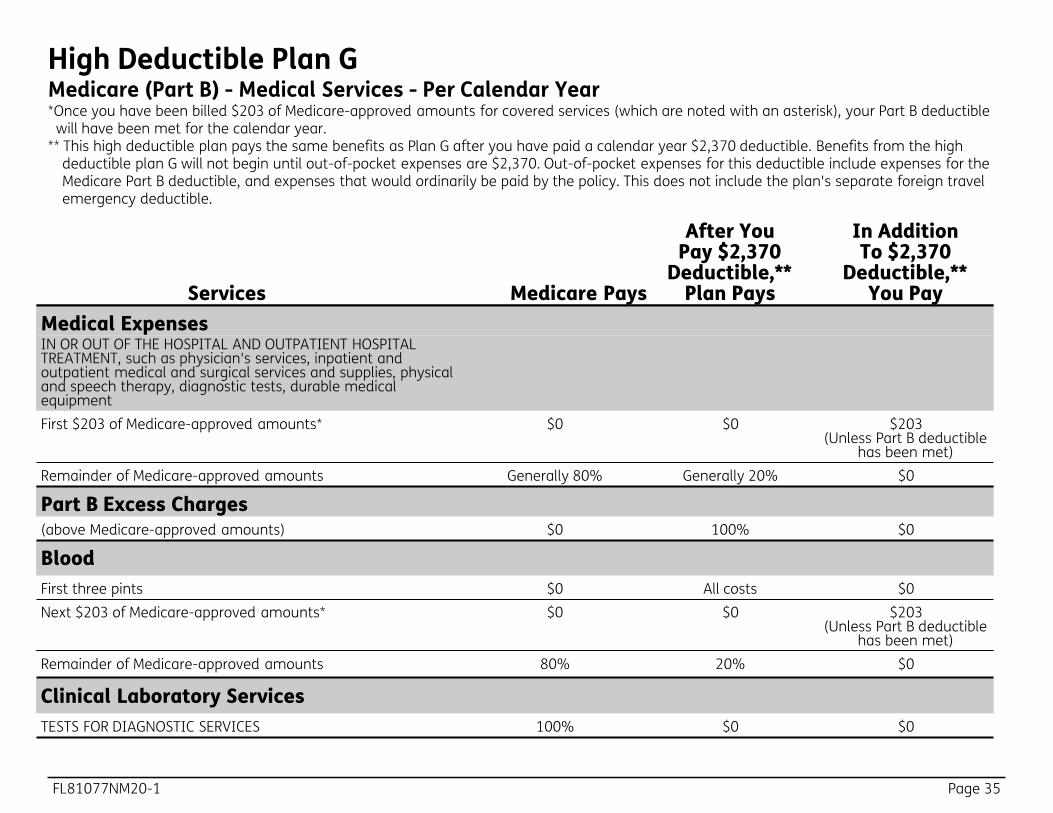
High Deductible Plan GMedicare (Part B) - Medical Services - Per Calendar Year *Once you have been billed $203 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible
will have been met for the calendar year. ** This high deductible plan pays the same benefits as Plan G after you have paid a calendar year $2,370 deductible. Benefits from the high
deductible plan G will not begin until out-of-pocket expenses are $2,370. Out-of-pocket expenses for this deductible include expenses for the Medicare Part B deductible, and expenses that would ordinarily be paid by the policy. This does not include the plan's separate foreign travel emergency deductible.
Services Medicare Pays
After You Pay $2,370
Deductible,** Plan Pays
In Addition To $2,370
Deductible,** You Pay
Medical Expenses IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as physician's services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment First $203 of Medicare-approved amounts* $0 $0 $203
(Unless Part B deductible has been met)
Remainder of Medicare-approved amounts Generally 80% Generally 20% $0
Part B Excess Charges (above Medicare-approved amounts) $0 100% $0
Blood First three pints $0 All costs $0 Next $203 of Medicare-approved amounts* $0 $0 $203
(Unless Part B deductible has been met)
Remainder of Medicare-approved amounts 80% 20% $0
Clinical Laboratory Services TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0

Page 36 FL81077NM20-1
High Deductible Plan GMedicare (Parts A and B) - Medical Services - Per Calendar Year *Once you have been billed $203 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible
will have been met for the calendar year. ** This high deductible plan pays the same benefits as Plan G after you have paid a calendar year $2,370 deductible. Benefits from the high
deductible plan G will not begin until out-of-pocket expenses are $2,370. Out-of-pocket expenses for this deductible include expenses for the Medicare Part B deductible, and expenses that would ordinarily be paid by the policy. This does not include the plan's separate foreign travel emergency deductible.
Services Medicare Pays
After You Pay $2,370
Deductible,** Plan Pays
In Addition To $2,370
Deductible,** You Pay
Home Health Care MEDICARE-APPROVED SERVICES Medically necessary skilled care services and medical supplies 100% $0 $0 Durable medical equipment
First $203 of Medicare-approved amounts* $0 $0 $203 (Unless Part B deductible
has been met) Remainder of Medicare-approved amounts 80% 20% $0
Services Medicare Pays
After You Pay $2,370
Deductible,** Plan Pays
In Addition To $2,370
Deductible,** You Pay
Foreign Travel Not covered by Medicare Medically necessary emergency care services beginning during the first 60 days of each trip outside of the USA First $250 each calendar year $0 $0 $250 Remainder of charges $0 80% to a lifetime
maximum benefit of $50,000
20% and amounts over the $50,000 lifetime
maximum
Other Benefits - Not Covered By Medicare
FL81077NM20-1 Page 37
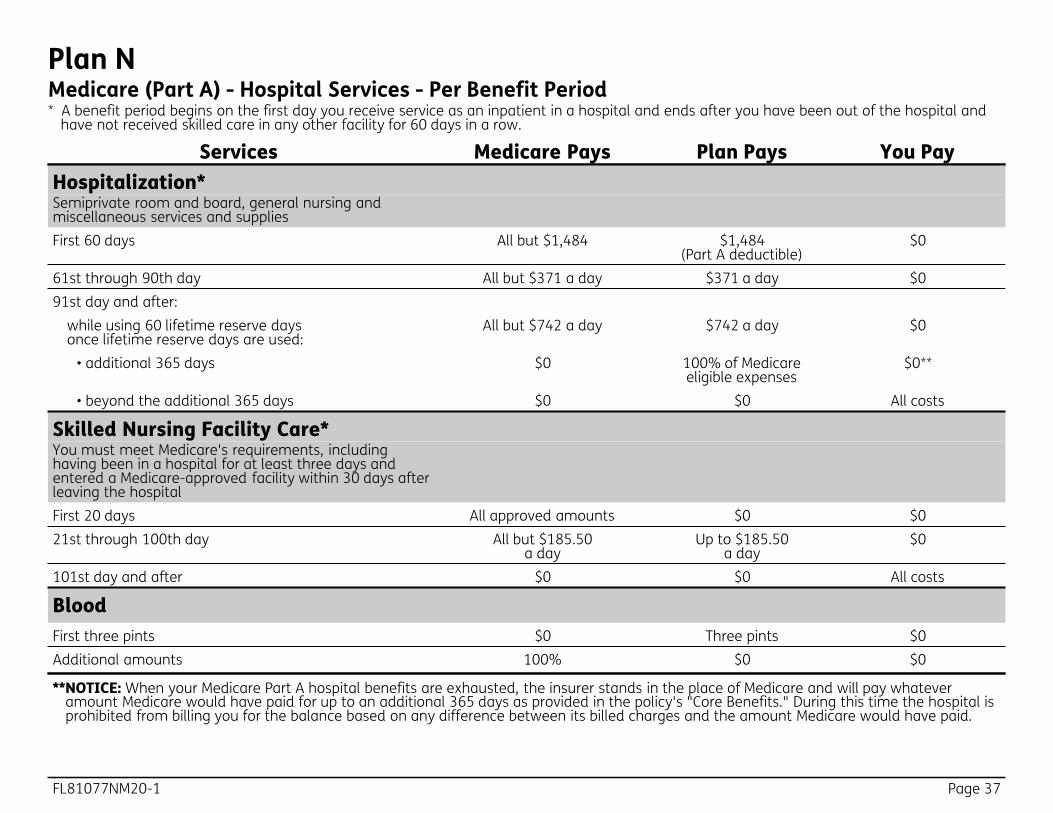
Plan NMedicare (Part A) - Hospital Services - Per Benefit Period * A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and
have not received skilled care in any other facility for 60 days in a row.
Services Medicare Pays Plan Pays You Pay Hospitalization* Semiprivate room and board, general nursing and miscellaneous services and supplies First 60 days All but $1,484 $1,484
(Part A deductible) $0
61st through 90th day All but $371 a day $371 a day $0 91st day and after:
while using 60 lifetime reserve days once lifetime reserve days are used:
All but $742 a day $742 a day $0
• additional 365 days $0 100% of Medicare eligible expenses
$0**
• beyond the additional 365 days $0 $0 All costs
Skilled Nursing Facility Care* You must meet Medicare's requirements, including having been in a hospital for at least three days and entered a Medicare-approved facility within 30 days after leaving the hospital First 20 days All approved amounts $0 $0 21st through 100th day All but $185.50
a day Up to $185.50
a day $0
101st day and after $0 $0 All costs
Blood First three pints $0 Three pints $0 Additional amounts 100% $0 $0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy's "Core Benefits." During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.

Page 38 FL81077NM20-1
Plan NMedicare (Part A) - Hospital Services - Per Benefit Period (Continued)
Services Medicare Pays Plan Pays You Pay Hospice Care You must meet Medicare's requirements, including a doctor's certification of terminal illness.
All but very limited copayment/coinsurance for outpatient drugs and
inpatient respite care
Medicare copayment/ coinsurance
$0
Medicare (Part B) - Medical Services - Per Calendar Year
Services Medicare Pays Plan Pays You Pay Medical Expenses IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as physician's services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment First $203 of Medicare-approved amounts* $0 $0 $203
(Part B deductible) Remainder of Medicare-approved amounts Generally 80% Balance, other than up
to $20 per office visit and up to $50 per
emergency room visit. The copayment of up to
$50 is waived if the insured is admitted to any hospital and the
emergency visit is covered as a Medicare
Part A expense.
Up to $20 per office visit and up to $50 per
emergency room visit. The copayment of up to
$50 is waived if the insured is admitted to any hospital and the
emergency visit is covered as a Medicare
Part A expense.
Part B Excess Charges (above Medicare-approved amounts) $0 $0 All costs
*Once you have been billed $203 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
FL81077NM20-1 Page 39
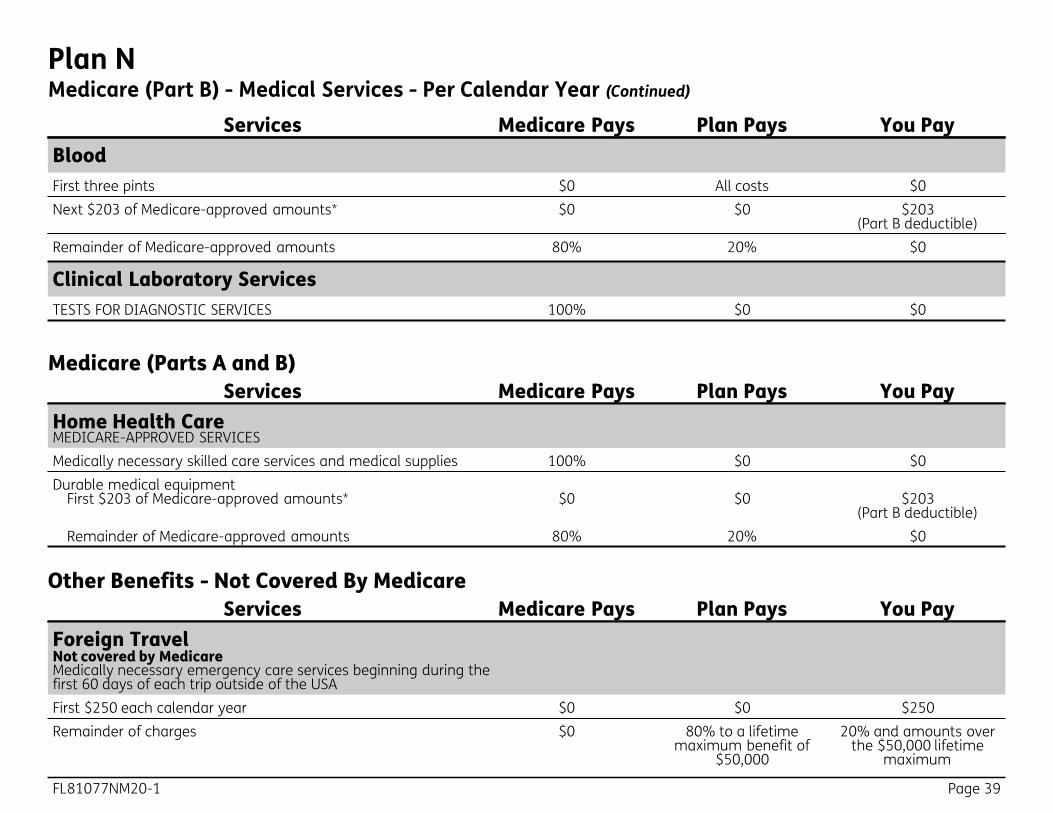
Plan NMedicare (Part B) - Medical Services - Per Calendar Year (Continued)
Services Medicare Pays Plan Pays You Pay Blood First three pints $0 All costs $0 Next $203 of Medicare-approved amounts* $0 $0 $203
(Part B deductible) Remainder of Medicare-approved amounts 80% 20% $0
Clinical Laboratory Services TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
Services Medicare Pays Plan Pays You Pay Home Health Care MEDICARE-APPROVED SERVICES Medically necessary skilled care services and medical supplies 100% $0 $0 Durable medical equipment
First $203 of Medicare-approved amounts* $0 $0 $203 (Part B deductible)
Remainder of Medicare-approved amounts 80% 20% $0
Medicare (Parts A and B)
Services Medicare Pays Plan Pays You Pay Foreign Travel Not covered by Medicare Medically necessary emergency care services beginning during the first 60 days of each trip outside of the USA First $250 each calendar year $0 $0 $250 Remainder of charges $0 80% to a lifetime
maximum benefit of $50,000
20% and amounts over the $50,000 lifetime
maximum
Other Benefits - Not Covered By Medicare
Page 40 FL81077NM20-1
Notes
FL81077NM20-1 Page 41
Notes

Important! ______________________________________________________________________________________________At Humana, it is important you are treated fairly. Humana Inc. and its subsidiaries do not discriminate or exclude people because of their race, color, national origin, age, disability, sex, sexual orientation, gender, gender identity, ancestry, marital status or religion. Discrimination is against the law. Humana and its subsidiaries comply with applicable Federal Civil Rights laws. If you believe that you have been discriminated against by Humana or its subsidiaries, there are ways to get help. • You may file a complaint, also known as a grievance:
Discrimination Grievances, P.O. Box 14618, Lexington, KY 40512-4618 If you need help filing a grievance, call 1-800-866-0581 or if you use a TTY, call 711.
• You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights electronically through their Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or at U.S. Department of Health and Human Services, 200 Independence Avenue, SW, Room 509F, HHH Building, Washington, DC 20201, 1-800-368-1019, 800-537-7697 (TDD). Complaint forms are available at https://www.hhs.gov/ocr/office/file/index.html.
• California residents: You may also call California Department of Insurance toll-free hotline number: 1-800-927-HELP (4357), to file a grievance.
Auxiliary aids and services, free of charge, are available to you. 1-800-866-0581 (TTY: 711)Humana provides free auxiliary aids and services, such as qualified sign language interpreters, video remote interpretation, and written information in other formats to people with disabilities when such auxiliary aids and services are necessary to ensure an equal opportunity to participate.
Language assistance services, free of charge, are available to you. 1-800-866-0581 (TTY: 711) Español (Spanish): Llame al número arriba indicado para recibir servicios gratuitos de asistencia lingüística.繁體中文 (Chinese): 撥打上面的電話號碼即可獲得免費語言援助服務。Tiếng Việt (Vietnamese): Xin gọi số điện thoại trên đây để nhận được các dịch vụ hỗ trợ ngôn ngữ miễn phí.한국어 (Korean): 무료 언어 지원 서비스를 받으려면 위의 번호로 전화하십시오 .Tagalog (Tagalog – Filipino): Tawagan ang numero sa itaas upang makatanggap ng mga serbisyo ng tulong sa wika nang walang bayad.Русский (Russian): Позвоните по номеру, указанному выше, чтобы получить бесплатные услуги перевода.Kreyòl Ayisyen (French Creole): Rele nimewo ki pi wo la a, pou resevwa sèvis èd pou lang ki gratis.Français (French): Appelez le numéro ci-dessus pour recevoir gratuitement des services d’aide linguistique.Polski (Polish): Aby skorzystać z bezpłatnej pomocy językowej, proszę zadzwonić pod wyżej podany numer.Português (Portuguese): Ligue para o número acima indicado para receber serviços linguísticos, grátis.Italiano (Italian): Chiamare il numero sopra per ricevere servizi di assistenza linguistica gratuiti.Deutsch (German): Wählen Sie die oben angegebene Nummer, um kostenlose sprachliche Hilfsdienstleistungen zu erhalten.日本語 (Japanese): 無料の言語支援サービスをご要望の場合は、上記の番号までお電話ください。
(Farsi) فارسیبرای دریافت تسهیلات زبانی بصورت رایگان با شماره فوق تماس بگیرید.
Diné Bizaad ЁNavajoЂ: W0dah7 b44sh bee hani’7 bee wolta’7g77 bich’9’ h0d77lnih 47 bee t’11 jiik’eh saad bee 1k1’1n7da’1wo’d66 nik1’adoowo[.
(Arabic) العر بيةالرجاء الاتصال بالرقم المبين أعلاه للحصول على خدمات مجانية للمساعدة بلغتك
GCHJV5REN 0220

Bla
nk
insi
de
bac
k co
ver.

Insu
red
by H
uman
a In
sura
nce
Com
pany
FL81
077N
M20
-1
821





























