Embed Size (px)
Citation preview

129
J.F. Loring & S.E. Peterson (eds): Human Stem Cell Manual, Second edition. DOI: © 2013 Elsevier Inc. All rights reserved.2012
http://dx.doi.org/10.1016/B978-0-12-385473-5.00009-6
CHAPTER 9
Victoria L. Glenn, John P. Schell, Eyitayo S. Fakunle, Ronald Simon, and Suzanne E. Peterson
EDITOR’S COMMENTARYSince human embryonic stem cell (hESC) lines were first reported in 1998, dozens of laboratories have been studying their remarkable properties of self-renewal and differentiation potential. In 2007, remarkably similar cells, called induced pluripotent stem cells (iPSCs), were generated by tran-sient expression of reprogramming factors in human dermal fibroblasts. hESCs and iPSCs both self-renew and can differentiate into widely diverse cell types, and there is now considerable debate about which pluripotent cells are preferable for particular research and clinical studies. While hESCs have been in laboratories for much longer and researchers have more expe-rience in their culture and characterization, there are several reasons why iPSCs may find a wider range of uses. Since hESCs are not generated from living individuals, there is no clinical information associated with them; for example, as models for studying human genetic disease, hESCs are limited to those derived from embryos that have been screened using prenatal genetic diagnostics. Given that most diseases cannot be identified prenatally, this limits the utility of these cells for disease modeling. Although there are now hundreds of hESC lines available to researchers, they are still dominated by particular ethnicities, which will likely limit their use for drug screen-ing and toxicology applications as well as immunological matching for cell therapy.
Over the past several years, we have been building collections of iPSCs for three purposes: collections for studies of human genetic disease, collections of ethnically diverse cells for screens of drug toxicity, and collections for spe-cific cell transplantation therapies. We have chosen dermal fibroblasts derived from skin biopsies as the most practical source of cells for reprogramming. This chapter describes methods we developed for producing and banking fibroblasts from donor skin biopsies.
Isolation of Human Dermal Fibroblasts from Biopsies

CHAPTER 9: Isolation of Human Dermal Fibroblasts from Biopsies130
OVERVIEWAlthough new methods for generating iPSCs have been a hot topic for the past several years, less attention has been focused on the cells being repro-grammed. Fibroblasts have been the most common source of reprogram-mable cells, probably because there are several resources that have already banked fibroblasts from both diseased and normal donors. However, there is a growing need for primary cells that are not available from a company or a somatic cell bank. When considering banking their own collections of somatic cells for reprogramming, researchers need to consider which somatic cell type would be the best for their particular application. Over the years, a number of different somatic cell types have been successfully reprogrammed into iPSCs with varying efficiency, including fibroblasts, keratinocytes from hair and skin, various cells from the blood, and urothelial cells from urine (Aasen, 2009; Stadtfeld, 2010; Zhou, 2011). Each cell type has different advan-tages and disadvantages. For example, isolating keratinocytes from the outer root sheath of hair does not require a physician’s assistance, is painless for the donor, and the cells reprogram with high efficiency. However, primary keratinocytes do not expand well nor do they recover well after cryopreserva-tion. Blood is fairly easy to acquire but the reprogramming efficiency is low and since normal blood cells do not proliferate well in vitro, there is limited potential for banking cells for further reprogramming. In our lab, we have generated a number of iPSC lines using different types of primary cells that we isolated ourselves. We have weighed the pros and cons of each cell type and have found that human dermal fibroblasts (HDF) are the most robust cell type for reprogramming purposes with the fewest drawbacks.
In this chapter we present reliable techniques for isolating HDFs from a skin punch biopsy. Note that before any experimentation begins proper approval must be obtained from an IRB (institutional review board; see Chapter 38). This will involve the generation of an appropriate informed consent docu-ment that must be signed by each donor. Biopsies must be performed by a licensed medical practitioner in a clinical setting.
Isolation of HDFs begins by performing a 3 mm punch biopsy with local anesthesia, usually on the inner forearm or shoulder of the donor. Before iso-lation of the cells, it is important to keep the biopsy specimen submerged in ice-cold fibroblast medium containing an antibiotic and antimycotic. This is critical because the skin naturally harbors a variety of native bacteria and microorganisms on its surface that can lead to contamination. The tissue sam-ple is then cut into pieces and enzymatically digested. Cells and minced tissue are plated on fibronectin-coated tissue culture plates and allowed to settle and grow. Once the fibroblasts have become confluent, they are trypsinized and passaged to larger flasks for expansion, cryobanking, and experimentation.

Procedure 131
PROCEDUREIt is important to use sterile technique throughout this protocol. For best results, process the biopsy immediately after it is taken. Alternatively, biop-sies can last for a few days if they are kept in fibroblast medium on ice. If biopsies are shipped from a remote location make sure they are kept on ice continuously.
1. In a laminar flow hood, remove the 3 mm punch biopsy from the conical tube in which it was transported to the lab using sterile forceps.
2. Transfer the biopsy to a 60 mm dish containing 5 mL of 13 PBS with Penicillin/Streptomycin and Primocin to wash (Figure 9.1).
3. Transfer the biopsy to a new 60 mm dish containing only a small volume of PBS with Penicillin/Streptomycin and Primocin. Using forceps and very sharp scissors cut the tissue into approximately 10–15 equally sized small pieces (Figure 9.2).
n NoteIt is very important to use sharp scissors to cut the tissue. Do not shred or tear the tissue. Also, 10–15 pieces are appropriate for a 3 mm biopsy. If you are using larger biopsies, scale up the number of pieces to cut. n
4. Make up collagenase B solution immediately before use (See Recipes).5. Gather the pieces together in a clump and use forceps to transfer them
to a 1.5 mL microfuge tube. Make sure that the pieces are transferred to the bottom of the tube where they will come into contact with the collagenase B solution added in the next step.
FIGURE 9.1A 3 mm punch biopsy.

CHAPTER 9: Isolation of Human Dermal Fibroblasts from Biopsies132
n NoteThis step can be frustrating because sometimes the tissue sticks to the for-ceps or to the top of the microfuge tube. It is easiest to transfer the pieces in a clump rather than individually. Be patient. n
6. Add 1 mL of sterile filtered collagenase B to the microfuge tube. Make sure the pieces of tissue are completely covered.
7. Place the tube in a 37°C incubator. 8. About once each hour, gently agitate the tissue pieces in the tube, being
careful not to let any pieces stick to the side of the tube above the collagenase B solution.
9. After 3–6 hours, spin the tube at 1150 g for 5 minutes.10. Carefully pipette off the supernatant, making sure not to disturb the
pellet.11. Resuspend the pellet in 1 mL of fibroblast medium, pipetting up and
down several times to ensure that the pellet is broken up as much as possible.
n NoteFibroblast medium is fine for use in this protocol. However, specialty media designed for fibroblasts will generate higher cell yields. We recom-mend the fibroblast medium from ScienCell or Cell N Tec. n
12. Transfer the cell suspension to one fibronectin-coated well of a 12-well plate (see Recipes).
FIGURE 9.2Hold the biopsy with forceps (right) and cut it into 10–15 pieces with scissors (left).

Procedure 133
n NoteUnder a phase contrast microscope, many isolated cells should be appar-ent (Figure 9.3). There may also be a few larger pieces of tissue. n
13. Incubate the cells at 37°C, 5% CO2.14. Leave the plate undisturbed for 2–3 days, then examine it under the
microscope, looking for small patches of attached cells (Figure 9.4). 15. Add 1 mL of medium to the well without aspirating the original medium.16. Two days later, aspirate all the medium and replace it with 1 mL of
fibroblast medium.
FIGURE 9.3Skin biopsy plated after 5 hours of incubation in collagenase B.
FIGURE 9.4Skin biopsy 3 days after plating on fibronectin. Note the dark attached fibroblast cells.
CHAPTER 9: Isolation of Human Dermal Fibroblasts from Biopsies134
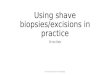
17. Change the medium every other day. You should have nice outgrowth by 1 week (Figure 9.5).
18. When the well is confluent (Figure 9.6), trypsinize the cells and transfer them to a larger flask.
n NoteMost biopsies will be ready to passage in 1–2 weeks. We typically passage one 12-well plate well into a T25 flask and then expand from there for banking and reprogramming. n
FIGURE 9.5Skin biopsy dissociated in collagenase B and grown on fibronectin for 1 week.
FIGURE 9.6Confluent well of fibroblasts from a skin biopsy. The cells are ready to be passaged into a T25 flask.

Procedure 135
n NoteOccasionally, contaminating non-fibroblast cells are seen in the original biopsy well (Figure 9.7). These cells are more resistant to trypsinization so monitor the cells during the trypsinization process and stop it when only the fibroblasts are detached. Even if some contaminating cells persist past the first trypsinization, they will be out-competed by the fibroblasts quickly. n
Passaging HDFs
1. Aspirate the medium from the 12-well plate well. 2. Rinse with 1 mL PBS. 3. Add 0.5 mL 0.05% Trypsin-EDTA. 4. Place the plate under a microscope and monitor the cells every minute
or so. 5. When the fibroblasts have come off but the contaminating cell types still
remain attached, add 0.5 mL of fibroblast medium to the well. 6. Pipette the cells up and down and transfer to a 15 mL conical tube. 7. Spin the tube at 200 g for 5 minutes. 8. Carefully remove the supernatant and resuspend the cells in 5 mL of
fibroblast medium. 9. Add the cell suspension to a T25 flask (does not need to be coated with
fibronectin) and return it to the incubator. Check cell growth in 2 days and do not disturb for at least 24 hours after passaging to ensure cell attachment to the flask.
n NoteKeep antibiotics and antimycotics in the medium only for the first week or two of culture. n
FIGURE 9.7Skin biopsy culture with contaminating non-fibroblast cell types. These cell types can easily be removed during the first trypsinization and will eventually be outcompeted by the fibroblasts.

CHAPTER 9: Isolation of Human Dermal Fibroblasts from Biopsies136
10. Replace the medium every 2 days until the flask becomes confluent, then passage again. Split the cells at a 1:3 ratio (e.g. T25 flask into T75 flask, T75 flask into T175 flask).
11. Cryopreserve at least two vials of cells before they are cultured antibiotic-free.
12. Make a larger cryobank after the cells have been cultured without antibiotics for a week and have been mycoplasma tested.
ALTERNATIVE PROCEDURESAlthough the first fibroblast isolation protocol described in this chapter is robust, this alternative protocol may also be used. Cells usually take longer to reach confluency using this protocol.
1. Pipette off the medium the biopsy was transported in, being careful not to aspirate the biopsy.
2. Rinse the biopsy 2 times in 13 PBS with Penicillin/Streptomycin and Primocin by manual pipetting.
3. Add 2–5 mL sterile filtered dispase at 2 units/mL (in PBS with Primocin and Penicillin/Streptomycin) and incubate at 4°C for 18 hours.
4. Rinse the biopsy twice in 13 PBS with Penicillin/Streptomycin and Primocin by manual pipetting.
5. Prepare one 12-well plate well per biopsy:n With a sterile needle, etch the bottom of one well of a 12-well plate
in a cross-hatched pattern.n Dilute 12 μL of bovine fibronectin (1 mg/mL stock) in 800 μL of
PBS and add to the etched well and incubate at room temperature for 45 minutes. Wash once with PBS before use.
6. In a laminar flow hood, transfer the biopsy to a 60 mm culture dish containing 1–2 mL 13 PBS (with Penicillin/Streptomycin and Primocin) to keep it from drying out.
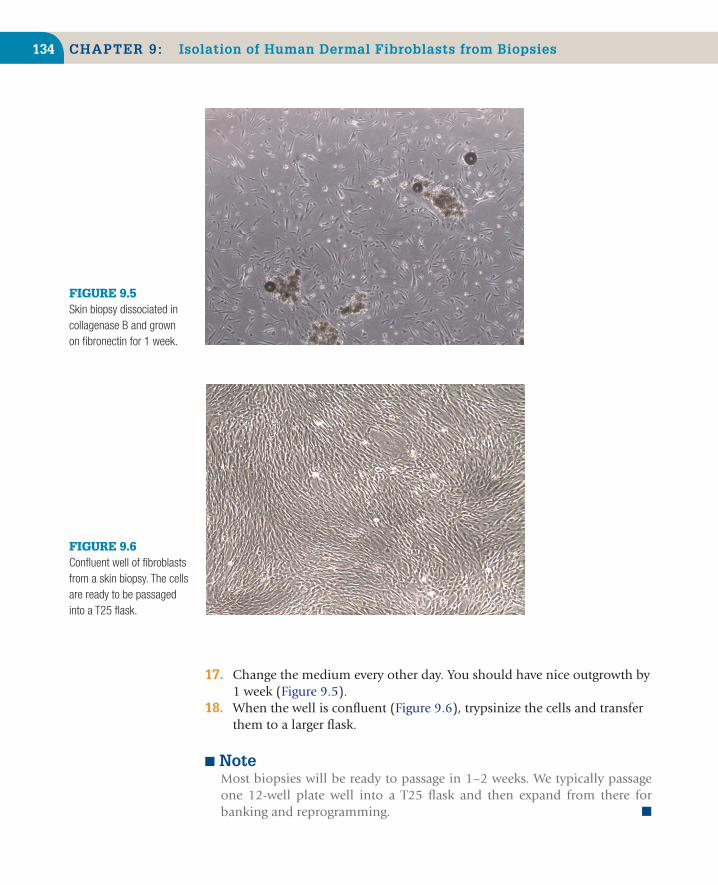
7. Using sterile instruments, separate the dermis and epidermis (Figure 9.8).n Use larger forceps with a flat broad end to hold the dermal layer
(Figure 9.8A).n Hold epidermal layer using thin forceps with pointed tips
(Figure 9.8A).n Pull to separate. It should come apart very easily (Figure 9.8B).
8. Transfer dermal tissue to a 35 mm dish and add 2 mL of AccuMax™.
n NoteThe epidermal layer may be discarded at this point or it can be used to iso-late keratinocytes. n
Alternative Procedures 137
9. Using two pairs of sterile dissecting scissors (one in each hand), manually dissociate tissue repeatedly for 3 minutes.
10. Transfer the 35 mm dish containing tissue in AccuMax to a 37°C incubator for 20 minutes.
11. Remove the dish from the incubator and transfer the contents of the dish to a 15 mL conical tube.
12. Neutralize AccuMax by adding fibroblast medium, bringing the total volume to 15 mL.
13. Spin down by centrifugation for 5 minutes at 200 g.14. Carefully aspirate the supernatant and resuspend in 2 mL of fibroblast
medium.15. Transfer the cell suspension to a prepared well of a 12-well plate and
place in a CO2 incubator at 37°C.16. Optional: Spin the plate at 2100 g for 5 minutes at room temperature in
order to help the cells adhere to the substratum.
n NoteOnce plated, do not remove from the incubator for 2 days (do not even touch the dish) to allow the larger undigested tissue to settle and allow cells to migrate out. n
17. Add 1 mL of fibroblast medium to the well on day 3; handle the plate gently to avoid dislodging the cells.
n NoteAt this point, some of the pieces of tissue should have attached to the etched areas in the wells (Figure 9.9). n
(A) (B)
FIGURE 9.8Separation of the dermal and epidermal layers. (A) Hold the dermal layer with large forceps that have a broad tip and the epidermal layer with pointed tipped forceps. (B) Pull the two layers apart. They should separate easily.

CHAPTER 9: Isolation of Human Dermal Fibroblasts from Biopsies138
18. On day 5, medium may be collected and biopsy fragments that did not attach may be seeded onto a new well.n Prepare a new well of the 12-well plate by etching and coating with
fibronectin.n Pipette up the medium from the original well and put it in a 15 mL
conical tube (there will be pieces of the biopsy which did not attach to the plate in this medium).
n Add 2 mL of fibroblast medium to the original well.n Bring up the volume in the 15 mL conical tube to 10 mL with
fibroblast medium. Spin at 200 g for 5 minutes, aspirate and resuspend in 2 mL of fibroblast medium.
n Add 2 mL of cell suspension to the new (etched and coated) well (on the same plate if possible). Treat the new well the same as the original biopsies – do not disturb for 2 days, and change medium on the same schedule.
19. Change the medium on the cells every other day until the well is confluent.
n NoteThis protocol is much more variable in regard to when the cells will start to grow out of the tissue. Outgrowths can sometimes be seen as early as 1 week but other times it may take several weeks. n
PITFALLS AND ADVICEManual DissociationWhen manually dissociating the biopsy into smaller pieces, make clean cuts. Minimizing tearing and shredding of the tissue will greatly improve primary
FIGURE 9.9Skin biopsy 2 days after harvest. Pieces of tissue from the biopsy tend to attach to the plate in the etched areas.

Reagents and Supplies 139
cell outgrowth from the dissociated tissue. To generate the cleanest cuts, make sure that the scissors you use are sharp enough to cleanly slice rather than shred the tissue.
Enzyme ExposureWhen using enzymes to dissociate tissue or to detach cells for passaging it is important not to leave the cells in active enzymes for longer than necessary. Enzymes used for cell culture work by breaking down connecting proteins and matrix components, such as collagen, but can begin to act on the cellular membrane proteins if given enough time. Serum used in culture medium can be used to decrease enzyme activity to prevent cell death.
ContaminationSince many microbes can live on human skin, it is important to test your fibroblasts for contaminants before cryobanking them. Remove the Primocin and Penicillin/Streptomycin from the medium 1–2 weeks after plating the cells and watch for bacteria and fungi (see Chapter 4). In addition, it is important to test your fibroblasts for mycoplasma (see Chapter 4).
EQUIPMENTn Class II biosafety cabinetn Tissue culture incubator, 37°C, 5% CO2n Inverted phase contrast microscope with 43, 103, and 203 objectivesn Dissecting microscope with Dark Field Transillumination and 0.8–4.53
rangen Tabletop centrifugen Scale capable of measuring in mgn Access to 4°C, 20°C, 80°C, and cryogenic freezersn Pipette aid and micropipetters, p-2, p-20, p-200, and p-1000 μL
REAGENTS AND SUPPLIESRecommended Reagents and Supplies
Item Supplier Catalog # Note
Dulbecco’s Phosphate-Buffered Saline (DPBS) without Calcium and Magnesium
Life Technologies 14190-250
Dispase Life Technologies 17105-041Costar 12-Well Clear TC-Treated Multiple Well Plates, Sterile
Corning 3512

CHAPTER 9: Isolation of Human Dermal Fibroblasts from Biopsies140
Item Supplier Catalog # Note
Sterile conical tubes, 50 mL Corning 430291Sterile conical tubes, 15 mL Corning 430053Bovine Fibronectin Calbiochem 341631Collagenase B Roche 11088807001DMEM GlutaMAX™ Life Technologies 10566-016MEM NEAA Life Technologies 11140-050Fetal Bovine Serum Gemini 900-108 10% total volumePenicillin/Streptomycin Life Technologies 15140 10 μL per 1 mL of
medium or PBSPrimocin InvivoGen Ant-pm-1 2 μL per 1 mL of
medium or PBS500 mL Vacuum Filter/Storage Bottle System, sterile low protein binding 0.22 μm pore, 33.2 cm2 PES membrane
Corning 431097
0.22 μm syringe filter Millipore SLGP033RS10 mL syringe BD 30960460 mm dish Sarstedt 83.1801Micro dissecting scissors World Precision
Instruments501263-G
Thumb dressing forceps Roboz RS-81221.5 mL microfuge tube Eppendorf 0223632040.05% Trypsin-EDTA Life Technologies 25300-054T25 flask Corning 430168T75 flask Corning 430641T175 flask Corning 431080Sterile needle and syringe BD 309569AccuMax Stemgent 01-0007Fibroblast Medium Sciencell 2301Fibroblast Medium Cell nTec CnT-05
RECIPESPreparation of Fibroblast Medium1. To make 500 mL:
Sterile filtern 445 mL DMEM with GlutaMAXn 50 mL FBS (Fetal Bovine Serum)n 5 mL MEM NEAA (Non-Essential Amino Acids).
2. Once filtered, aliquot medium for use in 50 mL conical tubes.3. Add Primocin and Penicillin/Streptomycin to the aliquot.

141Reading List
n NoteMaintain primary fibroblast cultures in Primocin and Penicillin/Streptomycin for only the first couple of weeks to prevent contamination. n
Preparation of Bovine Fibronectin Coated Wells1. Coat one well of a 12-well plate (1 well per biopsy) with bovine
fibronectin.2. For each well, dilute 12 μL of bovine fibronectin (1 mg/mL stock) in 800 μL of PBS and add to the well.
3. Allow the plate to incubate at room temperature for 45 minutes.4. Wash well once with PBS just prior to plating the cells
n NoteAliquot fibronectin to avoid repeated freeze thaw cycles. n
Preparation of Collagenase B1. Make up collagenase B immediately before use.2. Collagenase B is used at 2 units/mL; however, units of activity can vary
between lots so be sure to check the lot specifications prior to use.3. Bring collagenase B to room temperature before opening the container.4. Once at room temperature, measure the appropriate amount needed
(make 1 mL per biopsy).5. Add PBS and collagenase B to a conical tube.6. Sterile filter mixture into a sterile 15 mL conical tube with a 0.22 μm filter
and a 10 mL syringe.
READING LISTAasen, T., Belmonte, J.C., 2010. Isolation and cultivation of human keratinocytes from skin
or plucked hair for the generation of induced pluripotent stem cells. Nat. Protoc. 5 (2), 371–382.
Stadtfeld, M., Hochedlinger, K., 2010. Induced pluripotency: History, mechanisms, and applica-tions. Genes. Dev. 24 (20), 2239–2263.
Zhou, T., Benda, C., Duzinger, S., Huang, Y., Li, X., Li, Y., et al., 2011. Generation of induced pluripotent stem cells from urine. J. Am. Soc. Nephrol. 22 (7), 1221–1228.







![Intrinsic Radiosensitivity of Normal Human Fibroblasts and ... · (CANCER RESEARCH 52. 6348-6352. November 15. 1992] Intrinsic Radiosensitivity of Normal Human Fibroblasts and Lymphocytes](https://img.pdfslide.us/doc/110x75/60cc08f35a119f051502c1e0/intrinsic-radiosensitivity-of-normal-human-fibroblasts-and-cancer-research.jpg)