Embed Size (px)
DESCRIPTION
HIV pandemic continues to evolve Global Prevalence of HIV stabilise at 0.8% 25 million died of HIV 33 million living with HIV/ AIDS Every day: 4,900 die of HIV/AIDS 7,100 new HIV infection 3,200 on HAART : 2.6 million new infection 2 million died of HIV/ AIDS (1.7 million
Citation preview

Human Immune Deficiency Virus Infection
Dr Huda Taha Sep 2015

EpidemiologyVirologyNatural HistoryDiagnosisTransmissionHIV pregnancy

• HIV pandemic continues to evolve• Global Prevalence of HIV stabilise at 0.8%• 25 million died of HIV• 33 million living with HIV/ AIDS
• Every day: 4,900 die of HIV/AIDS 7,100 new HIV infection 3,200 on HAART
• 2009-2010: 2.6 million new infection 2 million died of HIV/ AIDS (1.7 million<15 Year old)
• 4 million receive HAART in Africa (50,000 in 2002)• 1 million pregnant women on HAART

100,000 people are living with HIV, quarter are unaware of their infection (16,000 in 1990)
2010-2011; 6660 new diagnoses of HIV
37 English PCT/ HIV prevalence >2:1000
1:5 HIV+ >50 Year old

“HIV in the UK” report
• Infection acquired within the UK almost doubled/ exceed those acquired abroad
• In the last 10 years, the biggest increases in people living with diagnosed HIV, East of England, the West Midlands and the North East.
• 2010 over 3000 gay men were diagnosed with HIV: 1 in 20 gay men are now infected with HIV nationally 1 in 10 in London
• Universal testing

HIV is a Lentivirus a member of the Retrovirus family
HIV infects vital cells in the human immune system such as helper T cells (specifically CD4+ T cells), macrophages and dendritic cells

Natural history
HIV vs AIDSAcquisition of Infection Primary HIV infection Asymptomatic HIV infection Early symptomatic infection Late symptomatic infection Advance HIV disease

1200
1100
1000
900
800
700
600
500
400
300
200
100
0
1:512
1:256
1:128
1:64
1:32
1:16
1.8
1.4
1.2
0
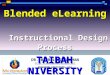
Weeks Years0 3 6 9 1 2 3 4 5 6 7 8 9 10 1112
CD
4+T
Cel
ls/m
m3
Plas
ma
Vir
emia
Titr
e
Primaryinfection
Possible acute HIV syndrome. Wide dissemination of virusSeeding of lymphoid organs
Clinical latency
Death
Opportunisticdiseases
Constitutionalsymptoms(
)
()
Natural History of HIV Infection

HIV infectionin pregnant women

Case 1
Conceiving on HAART;;

Use of antiretroviral therapy in pregnancy
Should continue HAART

Case 2Case 2
Naïve to HAART: mother needs ART for herself

Use of antiretroviral therapy in pregnancy
Commence treatment as soon as possible
NRTIs plus third agent ( NNRTI or PI)
Consider third trimester TDM

Case 3Case 3
Naïve to HAART: mother does not need HAART for herself

Use of antiretroviral therapy in pregnancy
All women should have commenced ART by week 24 preg.
NRTIs plus PI

Case 4
Late-presenting woman not on treatment

Use of antiretroviral therapy in pregnancy
After 28 weeks should commence HAART without delay
Unknown VL or >100 000 HAART plus Raltegravir
Untreated woman presenting in labour ; HAART plus Raltegravir
IV zidovudine for the duration of labour and delivery.

Women presenting ROM without a documented HIV result must be recommended to have an urgent HIV test
A reactive/positive test must be acted upon immediately with initiation of the interventions for prevention of PMTCT without waiting for further/ formal serological confirmation.

Case 5
Untreated women; CD-4 count ≥ 350 cells/ml and VL <50 copies/mL (confirmed on a separate assay)

Elite controllers
Can be treated with zidovudine monotherapy or with HAART
Can aim for a vaginal delivery
Should exclusively formula feed their infant

HIV in Pregnancy
ANC Testing ANC Testing Sexual Health Sexual Health Preconception and fertility managementPreconception and fertility managementMDT & documentationMDT & documentationPsychosocial issuesPsychosocial issuesAZT monotherapy AZT monotherapy vsvs CART CARTHIV testing in childrenHIV testing in childrenBreast feedingBreast feeding

STI screening
Recommended for pregnant women newly diagnosed with HIV.
Suggested for HIV-positive women already engaged in care
Genital tract infections should be treated according to BASHH guidelines.

Laboratory monitoring
Routine Antenatal investigationsHIV resistance testing Post short course treatment a further resistance test recommendedCD-4 count Viral load 2–4 weeks after commencing HAART

LFT at initiation of HAART and then at each antenatal visit.
If not achieved VL <50 copies/mL at 36 weeks the following interventions are recommended:
- Review adherence and concomitant medication - Perform resistance test if appropriate - Consider therapeutic drug monitoring - Optimise to best regimen - Consider intensification

ART postpartum
Continue HAART if CD4 count < 350 cells/ml 350-500 co- infection with Hep C or Hep B > 500 if sero-discordant or co morbidity
Can consider continuing between 350-350 even if no co morbidities

Infant testing
HIV DNA PCR (or HIV RNA testing) During the first 48 hours and prior to hospital discharge 6 weeks of age 12 weeks of age On other occasions if additional risk (breast-feeding)
HIV antibody testing for seroreversion should be done at age 18 months

Psychosocial issues
Antenatal HIV care should be delivered by a multidisciplinary team (MDT)

ThanksThanks
Suggested site:
WWW.BHIVA.org