Embed Size (px)
DESCRIPTION
http://www.kirklees.nhs.uk/fileadmin/documents/meetings/27_01_10/KPCT-10-22_Dementia_Strategy_-_10_Nov_09.pdf
Citation preview
This draft 10.11.09
-
Page 1 of 59
CONTENTS PAGE
NO
1. Foreword 2
2. Introduction 4
3. Vision for Dementia 7
4. Current Service Provision, Gaps and Action Plan 11
5. Financial Resources 16
6. Making it Happen 19
7. Bibliography 21
List of Appendices: 23
Appendix 1: National and Local Policy Context 24
Appendix 2: National Dementia Strategy – Objectives 29
Appendix 3: National and Local Data, Needs and Trends 32
Appendix 4: Summary of Key Priorities 43
Appendix 5: Kirklees Dementia Strategy Action Plan 45
8.
Appendix 6: What is Dementia?/Types of Dementia 58
9. Acknowledgements 59

This draft 10.11.09
-
Page 2 of 59
1. FOREWORD
1.1 Nationally and locally it is clear that dementia is one of the biggest challenges facing the health and social care economy. Although dementia can affect adults at any age, it is most common in older people becoming more prevalent with increasing age, but this does not mean it is a natural part of the ageing process or inevitable for all older people- a message we need to communicate more widely!.
1.2 The population of older people in Kirklees is rising steadily and dementia will impact on an increasing number of families, and increase the pressure on health and social care services. The current system needs to plan for this increased demand and provide better support for the many dementia suffers and their carers.
1.3 Our vision is for all people with dementia and their carers to continue to ‘live life to the full’ as described in the Vision for Older People in Kirklees (2008). To do this we will create an environment where people feel empowered to seek help early, know where to go for help and what services to expect, have access to the care and support that they would benefit from, and are confident that this care is of high quality, where the public and professionals are well informed and where fear and stigma associated with dementia has decreased.
1.4 Early diagnosis of, and intervention for, dementia are the keys to delaying admission to long term care and to helping people remain independent for longer. Making the diagnosis early means that there is the chance to prevent and plan for future problems and for people to benefit from positive interventions. Promoting healthy ageing, for example keeping people active and tackling social isolation, is important in delaying the onset and progression of dementia.
1.5 It is essential that we refocus investment in providing information about:
• the risk factors associated with dementia and the degree to which some dementias can be prevented;
• the symptoms of the disease and how to seek help and advice;
• low level support, at an earlier stage, to ensure people have the information they need to be able to plan and take greater control over their own lives.
1.6 We also know that accommodation choices for people with dementia are limited. Up to two thirds of people with dementia live in their own homes and want to remain there for as long as possible. At the later stages of the ‘journey’ finding quality residential and nursing care homes, which promote people’s independence and dignity can also be difficult. During the lifetime of this strategy we will aim to reduce premature admission to care homes and will explore opportunities to:

This draft 10.11.09
-
Page 3 of 59
• commission services which support people to stay in their own homes for longer;
• increase the range of accommodation choices for people with dementia, including extra care schemes;
and we will also:
• continue to influence the design of residential and nursing care home provision in the area to create environments which provide stimulation, enjoyment and dignified person centred care at the end of someone’s life.
1.7 It is important to recognise that delivery of this strategy cannot be achieved by one agency: Kirklees Council and Kirklees NHS along with our mental health partners, housing providers and voluntary and private sector providers must all work together to effect the changes that are needed to improve the lives of people affected by dementia and their families to make a real difference and ensure people receive the care and support that they need.
Keith Smith
Chair of the Older People’s Partnership Board

This draft 10.11.09
-
Page 4 of 59
2. INTRODUCTION
2.1 This document forms the Kirklees Joint Commissioning Strategy for Dementia 2009-2014. It is based on national guidance, set out in “Living well with dementia: A National Dementia Strategy” (2009), a local needs assessment and review of current provision, and has been developed by the Older People’s Partnership Board in partnership with Kirklees Adult Services, NHS Kirklees, The South West Yorkshire Partnership NHS Foundation Trust and third sector organisations.
2.2 The National Dementia Strategy (NDS) sets out the Government’s strategy for dementia over the next five years and brings together national priorities from a range of policy documents (described in Appendix 1 – National and Local Context).
2.3 Via the NDS the Government aims to ensure:
1. Improved public and professional awareness and understanding of dementia;
2. Earlier diagnosis and intervention;
3. A higher quality of care for people with dementia and their carers from diagnosis to end of life; and
identifies 17 objectives (set out in Appendix 2) which, when implemented largely at a local level, should result in significant improvements in the quality of services provided to people with dementia and should promote a greater understanding of the causes and consequences of dementia. Seven key priority outcomes have been highlighted that are likely to need focused attention for early delivery:
1. Early intervention and diagnosis for all;
2. Improved community personal support services;
3. Implementing the New Deal for Carers;
4. Improved quality of care for people with dementia in general hospitals;
5. Living well with dementia in care homes;
6. An informed and effective workforce for people with dementia; and
7. A Joint Commissioning Strategy for dementia.
2.4 The objectives identified within the NDS fit closely with what older people and relevant stakeholders have already told us are important to them and which have been incorporated into the Kirklees Older People’s Partnership Board’s “Vision for Older People in Kirklees – Living Life to the Full : Dementia Strategy” (see Figure 1 on page 6).
This draft 10.11.09
-
Page 5 of 59
2.5 National and local needs and trends have been analysed (see Appendix 3). Local dementia provision has been assessed against the NDS (see Section 4) and key priorities have been identified (set out in Appendix 4), from which an action plan has been developed (attached at Appendix 5) which aims to meet the objectives identified in the NDS and the key themes and priorities identified in the Older People’s Partnership Board’s Living Life to the Full Dementia Strategy.
2.6 This strategy, which should be viewed as a working document, aims to refocus investment in earlier diagnosis and intervention to improve outcomes for people with dementia and their carers to enable them to live life to the full, from diagnosis to end of life. It also aims to support people in the comfort and familiarity of their own environment by shifting care out of acute hospitals and reducing the number of people prematurely entering long term care.
2.7 A number of local policies, detailed in Appendix 1, will be significant in ensuring effective implementation of this strategy, particularly the Mental health Commissioning Strategy which will be reviewed later this year and the Carers Strategy currently in development. The actions within this strategy will therefore be jointly monitored through the Older People’s Partnership Board, the Mental Health Partnership Board and the Carers Strategy Group.

This draft 10.11.09
-
Page 6 of 59
Figure 1: Older People’s Partnership
Board - Living Life to the Full:
Dementia Strategy
• Improve public & professional awareness about dementia
• Provide good quality information about dementia and services available
• Ongoing support & advice
• Improve Carer Support
Ensure Diversity is provided
• Young onset dementia particularly within BME communities and people with a learning disability
• Earlier diagnosis
• Ensure Memory Services have adequate capacity
• Improve Care in General Hospital
• Improve End of Life Care
• Provide access to meaningful personalised activities
• Provide support to access mainstream activities
• Provide an informed and effective Workforce – all staff providing dementia care to be trained
• Improve Community Personal Support Services
• Improve Intermediate Care
• Provide access to assistive technology & telecare equipment
• Provide Peer Support
• Develop Learning networks
• Supported Housing- provide a range of options
• Improve the quality of care in care homes
DEMENTIA STRATEGY OBJECTIVES

This draft 10.11.09
-
Page 7 of 59
3. VISION FOR DEMENTIA
3.1 The Vision for Older People in Kirklees (2008)1 is the product of a comprehensive consultation with a range of stakeholders including Kirklees citizens, building on the work of the Older People’s Partnership Board and the Kirklees Council document “Improving the Quality of Life of Vulnerable Older People”. The vision is built around the kind of things that are important to older people in their everyday lives in Kirklees. We have used a ‘person centred’ approach which looks at how people want to live and what infrastructure and support they need in order to do so. We are trying to make sure that we do not attempt to fit people into services, but that we build support around people.
The vision and the themed areas of importance identified within the Older People’s Vision were reviewed by the Older People’s Partnership Board in March 2009 and it was agreed that these themes are equally as important for people experiencing dementia. Implementation of this strategy will therefore support achievement of the priorities and objectives contained within the Older People’s Partnership Board’s Vision for Older People, as illustrated at Figure 1 on page 6.
3.2 Our Vision for Dementia is that all people with dementia and their carers should be able to live life to the full. Achievement of the vision will encompass three areas in line with the NDS:
1. Encouraging help seeking and referral for diagnosis;
2. Making early diagnosis and treatment the rule rather than the exception;
3. The provision of good-quality care from diagnosis to end of life, in the community, hospital and care home.
1 http://www.kirklees.gov.uk/community/care-support/livelife/PDFFiles/visionForOlderPeople.pdf
Our vision is for all people with dementia and their carers to continue to ‘live life to the full’ from diagnosis to end of life. To do this we will create an environment where people:
• Are confident to seek help early;
• Know where to go for help and what services to expect;
• Have access to the care and support that they would benefit from and the quality of this care to be high;
• Know that the public and professionals are well informed and where the fear and stigma associated with dementia has decreased.

This draft 10.11.09
-
Page 8 of 59
3.3 Figure 2 below illustrates the care pathway and summarises the three themes of the National Dementia Strategy and the commissioning challenges.
Figure 2.
3.4 How will we achieve the vision? - There is a vast amount that can be done to improve and maintain the quality of life for Kirklees citizens with dementia and their families and partners will do this by:
• Challenging widespread defeatism that dementia is an inevitable consequence of the ageing process and that nothing can be done about it;
• Reducing the stigma that surrounds dementia and ensure that people with dementia are treated with dignity and respect - that the person is seen, not the diagnosis!;
• Promoting partnerships to improve earlier diagnosis and help seeking by locating responsibility for the diagnosis of mild and moderate dementia;
• Providing the right advice and information, at the right time;
• Focusing on remaining abilities and sustaining people’s independence for as long as possible;
• Providing access to high quality health and social care services, housing support and leisure activities when they are needed, to support people to live their preferred lifestyle and live well with dementia;

This draft 10.11.09
-
Page 9 of 59
• Implementing the Carers Strategy;
• Providing high quality end of life care;
• Ensuring that the workforce are trained to develop appropriate competencies and skills in dementia care and end of life care;
• Encouraging providers of services to develop dementia friendly environments incorporating appropriate design features both indoors and outdoors to improve way finding, support independence and improve quality of life.
3.5 What will we do? - As people’s needs and expectations are changing we need to change the way we respond to individuals accessing services and in the way we deliver services by:
• Re-focusing on prevention and encouraging people to behave in ways which will improve their health outcomes to reduce those risk factors associated with some dementias which we can do something about, for example:
> living a healthy lifestyle can reduce the risk of heart disease and stroke and may also reduce the risk of vascular dementia;
> reducing alcohol abuse can prevent or reduce alcohol related dementias such as Korsokoffs;
• Shifting investment from more costly acute interventions and refocusing on earlier diagnosis and intervention to improve outcomes for people with dementia and their carers;
• Educating and supporting people to self care for as long as possible, reducing reliance on the public sector;
• Focusing on wellbeing, meaningful occupation and physical activity;
• Engaging with housing providers and the third sector to provide lower level support to maximise independence and maintain skills for as long as possible;
• Providing access to enabling and rehabilitation services to maximise independence - people with dementia can still have rehabilitation potential and some skills can be relearned or new skills developed to compensate;
• Providing access to health and social care services at home to prevent avoidable admission to hospital;
• Guaranteeing a fast response for those leaving hospital or experiencing a crisis - including out of hours support;
• Developing specialist support for those people with complex needs and or long term health conditions such as diabetes, stroke, depression, incontinence, physical disabilities, terminal illness etc as well as dementia and other mental health concerns;

This draft 10.11.09
-
Page 10 of 59
• Supporting carers to enable people to be supported at home, for example through the provision of appropriate advice, information, respite care, education and peer support;
• Providing outcome-focused services which refer to the impacts or end results of services on a person’s life, aiming to achieve the aspirations, goals and priorities identified by service users;
• Giving people more choice and putting them in control of the services they receive, for example supporting more people with dementia to use direct payments and individualised budgets to direct their own care and service solutions.
3.6 Our principles - We believe we should:
• Listen to and involve people with dementia and their carers;
• Enable people to make informed choices and exercise choice and control over their lives;
• Give people time to make important decisions at difficult times and provide them with the best possible information to do so;
• Involve people in decisions about their lives;
• Support people in negotiating the “service maze” throughout the progression of their illness;
• Involve and support carers;
• Respect the dignity and privacy of people;
• Recognise individual differences;
• Provide integrated services.
3.7 How we will implement and deliver this vision is outlined in our action plan at Appendix 5.

This draft 10.11.09
-
Page 11 of 59
4. CURRENT SERVICE PROVISION, GAPS AND PRIORITIES
4.1 Currently in Kirklees diagnosis of dementia is made by a mental health professional usually after referral to the Memory Monitoring Service. However we know that diagnosis is low, only 40% of people are likely to have a diagnosis, so many people do not access specialist services. NHS Kirklees commission the South West Yorkshire Partnership NHS Foundation Trust (SWYPFT) to provide older people’s mental health treatment through a range of services including the Memory Monitoring Service, Community Mental Health Teams (CMHT), inpatient assessment and treatment, day services, intensive home treatment/assertive outreach, carer support through the Changes education programme and professional support via Care Home Liaison, Acute Hospital Liaison, Funded Nursing Care and Specialist Support and Management (Approved Mental Health Professionals and Psychologists).
4.2 Social care support is commissioned by Kirklees Council and is accessed if eligible following a community care assessment, this includes services such as home care, assistive technology, equipment and adaptations, day opportunities, respite care, residential care (most of which is purchased in the private sector), advice and information and signposting through Gateway to care and Gateway Workers. The Yorkshire and Humber Improvement Partnership2 identified that day care provision in Kirklees is in the highest 20% in England, homecare provision is slightly above the English median, and the numbers of people living in care homes (2.29% of population aged 65+) is just below the national median (2.33%).
4.3 The authors of Dementia UK (the report of a study by the London School of Economics, King's College London and the Alzheimer's Society) investigated the prescribing patterns for anti-dementia drugs and found that they varied across the Yorkshire and Humber region with Kirklees being close to the median value (at 2.1 prescriptions per person with dementia) for England and Wales (at 2.2).
4.4 The voluntary and community sector also provide a range of jointly commissioned support via organisations such as the Alzheimer’s Society, Age Concern, Anchor Trust, Crossroads for Carers and community organisations e.g St Andrews Support Group in North Kirklees.
2 www.yhip.org.uk- Dementia in Yorkshire and Humber- A Demographic Profile July 2009
This draft 10.11.09
-
Page 12 of 59
4.5 Some independent sector dementia services are now beginning to emerge to provide dedicated support to people with dementia and their carers to enable them to continue to live at home. These services can be commissioned privately or funded via direct payments and individual budgets
4.6 A comprehensive assessment of current service provision within Kirklees has been undertaken, and measured against the 17 objectives within the National Dementia Strategy.
4.7 The outcome of the review indicated that, although there is a range of assessment and community support services in Kirklees they are often focused at the general needs of older people and may not understand the specific needs of people experiencing dementias and the support needs of their carers. Service delivery, environmental design and staff skills and competencies within older age provision will be reviewed and services redesigned to achieve the objectives set out in this Strategy so that they can best provide care that meets individual need and best practice in dementia care.
4.8 Figure 3 on page 14 illustrates current services available in the dementia care pathway in Kirklees. Those highlighted in green are services currently being developed but not yet operational.
4.9 Figure 4 on page 15 summarises the priorities for Kirklees and illustrates where we want to be in the next 5 years.
4.10 Opportunities with agencies not traditionally seen as partners in dementia care will be explored and partnerships identified to commission improved outcomes for people, eg:
• Front line staff in the housing sector are in an excellent position to raise awareness and signpost people towards an early diagnosis, as well as providing housing related support to help people with dementia to stay in their homes for longer;
• Culture & Leisure services are well placed to improve access to physical activity and therapeutic interventions, which may delay progression of the disease and improve health and wellbeing.
4.11 The NHS Next Stage Review - NHS Yorkshire and the Humber - Report of Mental Health Clinical Pathway Group May 2008 identified as a development priority that:
“Dementia care services (are) required to be modernised with early access to memory assessment services supported by rapid access home and community orientated services aimed at supporting people in their own homes. This model allows people to be cared for within familiar environments maintaining their functioning for a longer time. It would also support nursing/residential care homes to care for people in later stage dementia and reduce hospital admissions”.
These priorities support the vision outlined within this strategy.
This draft 10.11.09
-
Page 13 of 59
4.12 NICE/SCIE guideline3 recommends therapies and treatments which we should integrate into new models of provision. These include:
• Structured group cognitive stimulation programmes in mild and moderate dementia;
• Alternative therapies for people with dementia and agitation such as aromatherapy, multi-sensory stimulation, therapeutic use of music/dance, animal assisted therapy, massage;
• Cognitive behaviour therapy for people with dementia who have depression/anxiety; this may include carers;
• Sensory stimulation therapies for anxiety, for example reminiscence therapy, multi-sensory stimulation, animal assisted therapy and exercise for people with dementia with depression/anxiety.
4.13 Following analysis of current provision and gaps we have outlined our commissioning priorities to meet the 17 objectives set out in the National Dementia Strategy and the themed outcomes and priorities set out in the Vision for Older People in Kirklees – Living Life to the Full: Dementia Strategy (Figure 1 on page 6). The key priorities are set out in Appendix 4 and the initial three year action plan drawn up to effect the change required is attached at Appendix 5.
3 National Institute for Health and Clinical Excellence and Social Care Institute for Excellence (2006) Dementia: Supporting People with Dementia and their Carers

This draft 10.11.09
-
Page 14 of 59
Figure 3: Dementia Care Pathway – Current Service Mapping in Kirklees 2009
Raising Awareness & Understanding
Early Diagnosis & Support
Living well with Dementia
End of Life
WORKFORCE COMPETENCIES/TRAINING: Safeguarding, Performance monitoring & Inspection
Living Life to the Full Guide Alzheimer’s Society national information e.g. Be Head Strong shared locally. Piloting Dementia Information Prescriptions. Kirklees Older People’s Network- public event
Primary Care- IAP Memory Services Alzheimer’s Contract
• Advice & Info
• Peer Support Advocacy – Cloverleaf Dementia Advisor Pilot- South Asian community focus
Community: Domiciliary care Intermediate Care access being developed Day Opportunities- some dementia places Community Support Workers Telecare & Equipment Housing- 10 extra care units planned Integrated services- eg continence services
Residential: Residential Care Homes & Respite Care EMI Care - 665 beds (res & nursing) Care Home Liaison
Care Management & Treatment Memory Services Community Mental Health Team inpatient beds
Acute Hospital Liaison Team
Y & H End of Life Strategy 2008
• Developing Domiciliary Care with specialist end of life care- Liverpool Care Pathway
Equipment services
EMI Nursing – 300 beds (4 homes achieved Gold Standards Framework accreditation)

This draft 10.11.09
-
Page 15 of 59
Clinical leads identified in all hospitals, care improved e.g pocket cards Environment, signage, design dementia friendly
Figure 4: Dementia Care Pathway – Priorities in Kirklees 2009- 2014
Joint public information campaign Living Life to the Full- use campaign to develop partnership work around self care. Improved wider staff awareness and understanding Improved GP awareness and increased referrals
Primary Care:
• Refresh H&SC dementia protocol
• Increased numbers earlier diagnosed
Memory Services- reviewed and capacity increased Increased peer support.- e.g. disease specific Expert Patients Programme and Looking After Me carers programme for dementia, new groups in the community Life history work developed widely
Community: Domiciliary care- all staff to have core skills/training Intermediate Care Pathway implemented Specialist Dementia Day Opportunities and access to mainstream activities Community Support Workers – service reviewed Telecare & Equipment Housing- extra care units more options Long Term Conditions and Stroke Strategy actions implemented Integrated services in place e.g. continence care Housing support services, Leisure services
Residential: Dementia leads in all homes EMI nursing beds Care Home Liaison input
Admiral nurse service in place Memory Service capacity increased Inpatient beds
Kirklees End of Life Strategy completed with action plan linked to dementia strategy
• Domiciliary Care with specialist end of life care using Liverpool Care Pathway
EMI Nursing beds
Gold Standards Framework implemented across all nursing and residential homes
Advanced care planning the norm.
Prescribing of anticipatory drugs the norm- pain relief
Preferred place of care the norm
End of Life
Living well with Dementia
Early Diagnosis & Support
Raising Awareness & Understanding
WORKFORCE COMPETENCIES/TRAINING: Safeguarding, Performance monitoring & Inspection

This draft 10.11.09
-
Page 16 of 59
8%
15%
41%
36%NHS
Social Services
Accommodation
Unpaid Care
5. FINANCIAL RESOURCES
5.1 Dementia costs the UK economy £17 billion a year and, in the next 30 years, the number of people with dementia in the UK will double to 1.4 million, with the costs trebling to over £50 billion a year.
5.2 Knapp et al 20075 suggested the breakdown of the distribution of dementia service costs, as illustrated in Figure 5 below.
Figure 5: Distribution of dementia service costs
5.2 The Dementia UK report4 commissioned by the Alzheimer’s Society calculated the overall costs of dementia in the UK, as £17.03 billion per annum, an average of £25,472 per person. This included care provided by formal agencies as well as the value of unpaid care provided by carers. Direct costs to the NHS and social care are currently estimated at £3.3 billion per year - this does not include ‘continuing care’ costs or care home costs. Dementia costs the health and social care economy more than cancer, heart disease and stroke combined!
5.3 The total cost per person per annum with dementia in the UK, in different settings, has been estimated as follows and includes unpaid care costs5 :
� People in the community with mild dementia- £14,540;
� People in the community with moderate dementia - 20,355
� People in the community with severe dementia- 28,527;
� People in care homes- £31,263.
4 Knapp et al (2007) Dementia UK: Report to the Alzheimer’s Society 5 www.alzheimers.org.uk

This draft 10.11.09
-
Page 17 of 59
5.4 Dementia service costs were broken down as follows:
� Over one third is due to informal care provided by unpaid carers and includes lost income for those carers who had to give up work - £6 billion;
� 15% of costs are incurred by Social Services;
� 8% of costs are incurred by the NHS;
� Accommodation costs, 41% - £7 billion of which, approximately 30%, will be self funded.
5.5 Funding for local dementia services is provided from two major statutory sources:
• NHS Kirklees
• Kirklees Council
These resources are used for both direct provision and commissioning of a wide variety of services. Kirklees Council currently spends approximately 17% of the older people’s budget (equating to approx £8.6m) on specialist dementia services. In addition people with dementia access mainstream generic services, which is therefore complex to calculate/apportion investment.
5.6 The local picture of need and the predicted rise in numbers of people with dementia in Kirklees is outlined in Appendix 3 and identifies where there is likely to be pressure for services and support.
5.7 This strategy sets out priorities to improve earlier diagnosis, intervention and reduce or delay the need for residential care. ‘Transforming the Quality of Dementia Care’6 set out the costs and benefits of expanding early diagnosis and intervention services for dementia and provides good evidence that establishing such services would lead to reduced use of residential care and would be clinically effective and cost effective to invest in such services. The report also suggested that savings would accrue from early diagnosis in terms of reduced use of acute hospital beds, by retention of admissions and facilitation of discharges. The financial case is strong if a strategic view over 4-10 years is adopted and there is a powerful argument for the prevention of institutionalisation and the positive effects that will be made on quality of life.
6Transforming the Quality of Dementia Care: Consultation on a National Dementia Strategy DoH 2008- Appendix 4.

This draft 10.11.09
-
Page 18 of 59
5.8 The DOH Impact Assessment of the NDS identified other savings opportunities in remodelling services, eg the report identified that 2.39 hours of psychiatrist time per patient can lead to a reduction in average hospital stay of 2.2 days and the National Audit Office estimated that people with dementia make up half of people who remain in hospital unnecessarily, average length of stay being 44% longer than an older person without dementia, it would seem pertinent to explore these opportunities.

This draft 10.11.09
-
Page 19 of 59
6. MAKING IT HAPPEN
6.1 This strategy sets out a wide range of commissioning priorities and actions outlined at Appendices 4 and 5.
6.2 In order to deliver the actions outlined in this commissioning strategy we have a number of working groups whose responsibility it is to ensure that we are moving closer towards our visions for services. The priorities and actions will be monitored through the Older People’s Partnership Board together with the Mental Health Partnership Board. A performance plan will ensure that every action is reported against during the year.
6.3 The Partnership Boards have a linked Executive Commissioning Group. The remit of these groups is to assist the Partnership Boards to set their strategic vision, ensure these visions are reflected in agency business plans, performance monitor their implementation and problem solve interagency issues, especially financial ones.
6.4 The Partnership Boards also have various sub-groups which work on particular aspects of the Board’s strategic vision for the future of services and which ensure that people who use services are closely involved in their planning and direction.
6.5 Diagram 6, page 19 shows how these various groups link together and highlights the roles each of them play in delivering this strategy.

This draft 10.11.09
-
Page 20 of 59
Local Public
Service Board for Adults and Healthier
Communities
Partnership Boards
Executive Commissioning
Groups
NHS
Kirklees
Board
Health Improvement Teams
Partnership Board Sub-groups
Integration Boards (eg Mental Health,
etc)
Council Cabinet
Formal decision making forums for
each partner agency
Senior Executive level partnership
forum for agreeing shared strategic
priorities:
Multi-agency stakeholder forums - their job is to develop
& agree shared strategic vision &
ensure all stakeholder input. One for each care group: MH, LD, OP, PSI/LTC, and Carers’ Strategy
Group
Multi-agency executive groups - tasked with
assisting the Partnership Boards to set their
strategic vision, translate vision into business /
action plans, performance monitor implementation,
problem solve interagency issues, esp financial ones.
Implementation groups tasked with delivering
the action plans, problem solving
interagency issues at an operational level, for
example:
Diagram 6: Making it Happen - responsibilities of the various interagency planning and working groups
Local Public
Service Board for Safer and
Stronger Communities

This draft 10.11.09
-
Page 21 of 59
7. BIBLIOGRAPHY
• Living well with dementia : A National Dementia Strategy (DoH 2009) http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_094058
• Improving services and support for older people with mental health problems (Age Concern 2007) http://www.mhilli.org/documents/Inquiryfinalreport-FULLREPORT.pdf
• Vision for Older People in Kirklees (2008) http://www.kirklees.gov.uk/community/care-support/livelife/PDFFiles/visionForOlderPeople.pdf
• Yorkshire and Humber Improvement Partnership (YHIP) Dementia in Yorkshire and Humber – A Demographic Profile (July 2009) http://www.yhip.org.uk/silo/files/dementia-in-yorkshire--humber--a-demographic-profile.pdf
• NICE/CSCI – Dementia: Supporting People with Dementia and their Carers (2006) http://www.nice.org.uk/guidance/cg42
• Knapp, M., Prince, (2007), The Prevalence and Economic Cost of Dementia in the UK, London, Kings College http://www.alzheimers.org.uk/site/scripts/documents_info.php?documentID=418&categoryID=200167&pageNumber=1
• POPPI – Projecting Older People Population Information System http://www.poppi.org.uk/index.php
• PANSI – Projecting Adult Social Care Needs and Service Information http://www.dhcarenetworks.org.uk/csed/Solutions/dfAndCapacityPlanning/pansi/
• Kirklees Joint Strategic Needs Assessment (JSNA) 2009 http://www.kirklees.nhs.uk/public-information/publications/reviews-and-assessments/
• Dementia UK http://alzheimers.org.uk/site/scripts/download_info.php?fileID=2
• Care Services Efficiency Delivery (Available from: http://www.poppi.org.uk), April ‘08
• National Audit Office (2007), Improving services and support for people with dementia, London, the Stationery Office
• Office of National Statistics, (2001), Population Census in England and Wales, ONS

This draft 10.11.09
-
Page 22 of 59
• The UK Inquiry Board (www.mhilli.org) (June 2006),Promoting Mental Health and Well Being in Later Life (Age Concern), London, Age Concern and the Mental Health FoundationTransforming the quality of dementia care: consultation on a National Dementia Strategy (DOH 2008)http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_085567.pdf
• Who cares? Information and support for the carers of people with dementia (DOH 2005) http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4123629.pdf
• Impact Assessment of National dementia Strategy Version 1.6 (DOH 2009) http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_094055.pdf
• Equality Impact Assessment of NDS (DOH 2009) http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_094054.pdf

This draft 10.11.09
-
Page 23 of 59
8. APPENDICES
Appendix 1: National and Local Context Appendix 2: National Dementia Strategy - Objectives Appendix 3: National and Local Needs and Trends Appendix 4: Summary of Key Priorities Appendix 5: Kirklees Dementia Strategy Action Plan Appendix 6: What is Dementia?

This draft 10.11.09
-
Page 24 of 59
APPENDIX 1
NATIONAL AND LOCAL CONTEXT
1. NATIONAL CONTEXT
1.1 “Living well with dementia: A National Dementia Strategy” (Department of Health, February 2009) brings together national priorities identified across a range of key policy documents:
• Forget Me Not (Audit Commission 2000) recognised that:
> Only one half of GPs believed it important to look actively for signs of dementia and make early diagnosis;
> GPs felt they did not receive sufficient training;
> There was a lack of clear information, advocacy and support for people with dementia and their families;
> There was insufficient specialist home care.
• National Service Framework for Older people (2001) included a chapter on mental health, considering dementia, advocating early diagnosis and intervention.
• Everybody’s Business (Department of Health and the Care Services Improvement Partnership 2005) set out the essentials for a service for older people’s mental health which included:
> Memory assessment services to enable early diagnosis;
> Integrated community mental health teams to support the management of people with dementia with complex symptoms.
• National Institute for Clinical Excellence (NICE)/Social
Care Institute for Excellence (SCIE) Clinical Guidance (2006), key recommendations included:
> Integrated working across agencies;
> Memory assessment services as a point of referral for diagnosis;
> Assessment and support for carers;
> Assessment and treatment of non-cognitive symptoms and behaviour that challenges;
> Dementia care training for all staff working with older people;
> Improvement of care for people with dementia in hospitals.
• Dementia UK Report (Alzheimer’s Society 2007) set out the numbers of people with dementia nationally and the costs associated with treatment and care. Its recommendations included:

This draft 10.11.09
-
Page 25 of 59
> Making dementia an explicit national health and social care priority;
> Improving the quality of services provided for people with dementia and their carers.
• Improving Services and Support for People with Dementia (The National Audit Office 2007) This report was critical about the quality of care for people with dementia and their carers. It advocated a ‘spend to save’ approach with up front investment in services for early diagnosis and intervention, improved specialist services, community services and care in general hospitals resulting in long term cost savings from the prevention of transition into care homes and decreased hospital stays. It also recognised:
> That the availability and size of specialist community mental health teams was variable;
> That the confidence of GPs spotting the symptoms of dementia was lower than it had been in 2000;
> The lack of support for carers;
> That overall services were not delivering value for money;
> That people were not being diagnosed early enough;
> That early intervention is needed to improve quality of life;
> That services in the community, care homes and end of life were not delivering support to people to live independently as long as possible in the place of their choosing.
1.2 The size of the population affected by dementia means that development of policies and services for people with dementia and their carers is significantly affected by the wider policy context. It is integral to the:
• “Putting People First” agenda;
• Implementation of the NHS Review “Your NHS, Your Future”; and sits along side other key Government policies including the:
• The Carers Strategy;
• Valuing People Now;
• The review of No Secrets (adult safeguarding);
• Transforming Adult Social Care;
• Lifetime Homes, Lifetime Neighbourhoods: A National Strategy for Housing in an Ageing Society;
• World Class Commissioning; and
• The Darzi Review.
1.3 NHS Operating Framework for 2009/10 - dementia has been included as one of the areas where the Department of Health will expect to see and monitor progress:

This draft 10.11.09
-
Page 26 of 59
“The national Dementia Strategy will be a comprehensive framework aimed at driving up standards of health and social care services to improve the quality of life and quality of care for people with dementia and their carers. PCTs will want to work with local authorities to consider how they could improve dementia services.”
2. LOCAL CONTEXT
2.1 In 2008, Kirklees Council commissioned a piece of research7 with focus groups of local people aged 65+, which highlighted concerns across all seven localities about people’s perceptions of dementia:
• Negative images of dementia - ‘nothing could be done for you’;
• Little recognition of the stages of dementia;
• Concern about managing risks at home;
• An expectation that you would need residential care, no awareness of alternatives;
• Dementia was seen almost unanimously by participants in the focus groups as ‘the end’.
This research has informed the development of the Kirklees Dementia Strategy.
2.2 Development of the End of Life Strategy for Yorkshire and the Humber (2008) identified that there is a lack of public awareness about end of life issues. Death and dying are not discussed and health services tend to focus on treatment and cure. Advance planning for end of life is not consistently undertaken so that patients’ preferred place of care and care choices are not always recorded to inform last days of life care. Patients’ preferences for place of care are not well met. The majority of patients (60%) indicated that they would wish to be cared for and die at home, however, only 18% of patients currently have this wish met. A recent bench mark audit of nursing home deaths in 2 homes in Kirklees identified that 50% of deaths were due to dementia and that the majority of these had not had anticipatory drugs prescribed. This evidence has also informed the development of the Kirklees Dementia Strategy.
2.3 The Council’s Ambitions and Key Improvement Priorities
Ensuring the wellbeing of adults and older people and reducing health inequalities are areas of strategic priority and focus for the Council’s political administration, ie to:
� Transform the delivery of adult social care to meet local needs and aspirations, emphasising quality provision;
� Support people to live independently, minimising the need for acute services and hospital admissions;
� Ensure effective safeguarding of vulnerable adults; 7 MRUK- focus group Exec Summary 2008

This draft 10.11.09
-
Page 27 of 59
� Address locality based health and social care inequalities;
� Ensure an adequate supply of new and improved homes;
� Tailor housing services to individual needs, supporting adult wellbeing and choice;
� Facilitate good quality neighbourhood and community services to support wellbeing and reduce social isolation;
� Improve the mental health and wellbeing of adults (and of children and young people);
� Support people with long term conditions to be more independent and make informed choices for their care;
� Improve access to high quality healthcare, especially in primary care serving communities with the worst health.
All of which Adult Services and partners are working towards and which are implicit in the Kirklees Dementia Strategy.
2.4 The strategies set out in the paragraphs below will be significant in ensuring effective implementation of the Kirklees Dementia Strategy:
• Kirklees Commissioning Strategy for Adults 2009-2012 - sets out local commissioning priorities in Kirklees.
• Kirklees Carers Strategy - currently being updated in line with the national strategy for carers.
• Kirklees Joint Mental Health Commissioning Strategy 2008-2011 – sets out the vision to maintain and improve the mental health and wellbeing of our local population. This strategy will be refreshed during 2009 to recognise the impact of dementia in later life and challenge the widespread defeatism which leads to the belief that dementia is an inevitable part of growing older and therefore nothing can be done.
• Kirklees Learning Disability Strategy – sets out the vision and commissioning strategy for people with learning disabilities in Kirklees. This strategy will recognise the need to provide services and support to people with learning disabilities who may experience young onset dementia.
• Kirklees Intermediate Care Programme- review of the current intermediate care pathway recognises that it must not exclude people with dementia and will challenge the false assumption that people with dementia cannot benefit from rehabilitation. It aims to provide in-reach into the place of residence during a crisis to prevent the need for hospital admission and to support people to return home rather than be admitted prematurely to residential care.
This draft 10.11.09
-
Page 28 of 59
• Kirklees Long Term Conditions Programme- aims to promote self care and improve the treatment and care of older people with long term conditions, for example diabetes, stroke, heart disease, cancer, some of which will also experience dementia and other mental health related conditions.
• Kirklees Adult Safeguarding Strategy- this multi-agency agreement for safeguarding adults aims to assist “vulnerable” adults to live a life that is free from abuse and neglect and which enables them to retain independence, wellbeing, dignity and choice.
• Dignity in care Agenda- promotes life history work and ensures that people with dementia are accorded the dignity and respect which underlies their value as a unique individual within the context of their past and present environment and social relationships.
• Kirklees Stroke Strategy – currently being developed to raise awareness of stroke prevention and improve services which help reduce incidence and minimise long term effect. The care pathway will ensure that people who develop vascular dementias are signposted to appropriate supports.

This draft 10.11.09
-
Page 29 of 59
APPENDIX 2
NATIONAL DEMENTIA STRATEGY - OBJECTIVES
Objective 1: Improving public and professional awareness and
understanding of dementia
Public and professional awareness and understanding of dementia to be improved and the stigma associated with it addressed. This should inform individuals of the benefits of timely diagnosis and care, promote the prevention of dementia, and reduce social exclusion and discrimination. It should encourage behaviour change in terms of appropriate help-seeking and help provision.
Objective 2: Good-quality early diagnosis and intervention for all
All people with dementia to have access to a pathway of care that delivers: a rapid and competent specialist assessment; an accurate diagnosis, sensitively communicated to the person with dementia and their carers; and treatment, care and support provided as needed following diagnosis. The system needs to have the capacity to see all new cases of dementia in the area.
Objective 3: Good-quality information for those with diagnosed dementia and their carers
To provide people with dementia and their carers with good-quality information on the illness, and on the services available. This is both at diagnosis and throughout the course of their care.
Objective 4: Enabling easy access to care, support and advice following diagnosis
A dementia adviser to facilitate easy access to appropriate care, support and advice for those diagnosed with dementia and their carers.
Objective 5: Development of structured peer support and learning networks
The establishment and maintenance of such networks will provide direct local peer support for people with dementia and their carers. It will also enable people with dementia and their carers to take an active role in the development and prioritisation of local services.
Objective 6: Improved community personal support services
The provision of an appropriate range of services to support people with dementia living at home and their carers. Access to flexible and reliable services, ranging from early intervention to specialist home care services, which are responsive to the personal needs and preferences of each individual and take account of their broader family circumstances. Accessible to people living alone or with carers, and people who pay for their care privately, through personal budgets or through local authority-arranged services.

This draft 10.11.09
-
Page 30 of 59
Objective 7: Implementing the Carers’ Strategy
Family carers are the most important resource available for people with dementia. Active work is needed to ensure that the provisions of the Carers’ Strategy are available for carers of people with dementia. Carers have a right to an assessment of their needs and can be supported through an agreed plan to support the important role they play in the care of the person with dementia. This will include good-quality, personalised breaks. Action should also be taken to strengthen support for children who are in caring roles, ensuring that their particular needs as children are protected.
Objective 8: Improved quality of care for people with dementia in
general hospitals
Identifying leadership for dementia in general hospitals, defining the care pathway for dementia there and the commissioning of specialist liaison older people’s mental health teams to work in general hospitals.
Objective 9: Improved intermediate care for people with dementia
Intermediate care which is accessible to people with dementia and which meets their needs.
Objective 10: Considering the potential for housing support, housing-related services and telecare to support people with
dementia and their carers
The needs of people with dementia and their carers should be included in the development of housing options, assistive technology and telecare. As evidence emerges, commissioners should consider the provision of options to prolong independent living and delay reliance on more intensive services.
Objective 11: Living well with dementia in care homes
Improved quality of care for people with dementia in care homes by the development of explicit leadership for dementia within care homes, defining the care pathway there, the commissioning of specialist in-reach services from community mental health teams, and through inspection regimes.
Objective 12: Improved end of life care for people with dementia
People with dementia and their carers to be involved in planning end of life care which recognises the principles outlined in the Department of Health End of Life Care Strategy. Local work on the End of Life Care Strategy to consider dementia.
Objective 13: An informed and effective workforce for people with dementia. Health and social care staff involved in the care of people who may have dementia to have the necessary skills to provide the best quality of care in the roles and settings where they work. To be achieved by effective basic training and continuous professional and vocational development in dementia.

This draft 10.11.09
-
Page 31 of 59
Objective 14: A joint commissioning strategy for dementia
Local commissioning and planning mechanisms to be established to determine the services needed for people with dementia and their carers, and how best to meet these needs. These commissioning plans should be informed by the World Class Commissioning guidance for dementia developed to support this Strategy and set out in Annex 1.
Objective 15: Improved assessment and regulation of health and care services and of how systems are working for people with dementia and their carers
Inspection regimes for care homes and other services that better assure the quality of dementia care provided.
Objective 16: A clear picture of research evidence and needs. Evidence to be available on the existing research base on dementia in the UK and gaps that need to be filled.
Objective 17: Effective national and regional support for
implementation of the Strategy.
Appropriate national and regional support to be available to advise and assist local implementation of the Strategy. Good-quality information to be available on the development of dementia services, including information from evaluations and demonstrator sites.

This draft 10.11.09
-
Page 32 of 59
APPENDIX 3
NATIONAL AND LOCAL NEEDS AND TRENDS
1. NATIONAL NEEDS AND TRENDS
1.1 The National Picture
• There are currently 700,000 people in the UK with dementia;
• Dementia costs the UK economy £17 billion per year;
• Direct costs to the NHS and social care are estimated at £3.3 billion per year- more than cancer, heart disease and stroke combined!;
• In the next 30 years the number of people with dementia will double to 1.4 million, with costs trebling to £50 billion;
• One in 14 people over 65 has a form of dementia;
• This rises to one in every 6 people over the age of 80;
• By the age of 95 one in 3 people are affected;
• One in every 3 people over the age of 65 will develop dementia before they die.
1.2 Dementia is caused by a variety of diseases which affect people in different ways. The term dementia is used to describe a collection of symptoms, including a decline in memory, reasoning and communication skills, and a gradual loss of skills needed to carry out daily living activities. These symptoms are caused by structural and chemical changes in the brain as a result of physical diseases such as Alzheimer’s disease.
1.3 Dementia can affect people of any age but is most common in older people. One in six people over 80 has form of dementia and one in 14 people aged over 65 has a form of dementia. Prevalence roughly doubles every five years over the age of 65.
1.4 Dementia is one of the main causes of disability later in life. Older people are particularly likely to have multiple health conditions but dementia has a disproportionate impact on capacity for independent living.8 Dementia contributes 11.2% of all years lived with a disability among people over 60: more than stroke (9.5%), musculoskeletal disorders (8.9%), cardiovascular disease (5%) and all forms of cancer (2.4%)9.
1.5 Alzheimer’s disease is the most common form of dementia. The proportion of those with different types of dementia can be broken down as per Figure 1 below:
8 See Appendix 2 for stages of disease progression 9 2003 World health Report Global Burden of Disease estimates

This draft 10.11.09
-
Page 33 of 59
1.5 Dementia is life limiting. It is a long term progressive condition which is terminal. Sixty thousand deaths a year are attributable to dementia;
• Two thirds of people with dementia are women:
• Up to half of people with dementia also have depression;
• People with both dementia and depression have higher rates of disability and decline and higher rates of hospitalisation than people with dementia alone.10
• People with dementia are at greater risk of developing delirium, and misdiagnosis is common since both dementia and delirium result in cognitive impairment. Delirium is preventable and treatable.11
• Two thirds of people with dementia live in the community whilst one third live in care homes;
10 Age Concern: Improving services and support for older people with mental health problems 11 Age Concern:Improving services and support for older people with mental health problems: Prevention
Fig 1. Proportion of those people with Different Types of Dementia
Alzheimer's Disease - 62%
Vascular dementia - 17%
Mixed Dementia – 10%
Dementia with Lewy Bodies – 4%
Fronto - Temporal Dementia – 2%
Parkinson's Dementia – 2%
Other Dementia – 3%
Percentages (%)
Reference: National Audit Office

This draft 10.11.09
-
Page 34 of 59
• Dementia is often seen as inevitable in later life and therefore not preventable however there is evidence that the risks for some types of dementias can be reduced;
• It is estimated that nationally there are around 11,000 people from black and minority ethnic groups with dementia and it is worth noting that generally they experience higher rates of young onset dementia and vascular dementia related to heart disease and stroke;
• Dementia in younger people is comparatively rare, nationally approximately 15,000 people under 65, but this number is likely to increase with improved awareness and earlier diagnosis;
• People with Downs Syndrome have an increased genetic risk of developing dementia. They are four times more likely to develop dementia and for it to begin at an earlier stage;
• The emotional impact on people with dementia and their families can be enormous and often includes high levels of depression and stress.
2. LOCAL NEEDS AND TRENDS
2.1 The Local Picture
• Prevalence rates suggest that there are over 4,100 people in Kirklees with dementia;
• GP registers in Kirklees currently identify 1,790 people who have received a diagnosis;
• By 2025 the number of people experiencing dementia in Kirklees is forecast to rise to over 6,200;
• It is estimated that currently there are approximately 100 people with young onset dementia in Kirklees.
NB Data used in this report should be viewed with caution and has been included for indicative purposes. Accurate population estimates and population projections of people with dementia are not a routinely produced national statistic.
2.2 Dementia is most common in older people. Kirklees has an ageing population, in line with the national picture, and so we can expect to see a dramatic growth in the incidence of dementia in the next 15 years, particularly in the 85+ age group, as illustrated at Figure 2a below.

This draft 10.11.09
-
Page 35 of 59
Dementia Population Graph
0
1000
2000
3000
4000
5000
6000
7000
2008 2010 2015 2020 2025
Year
No
. o
f P
eo
ple Aged 85 and over
Aged 80-84
Aged 75-79
Aged 70-74
Aged 65-69
Figure 2a: Dementia Population Projections
2.3 The Alzheimer’s Society report: Dementia UK provided methodology which has allowed us to estimate the numbers of people with mild, moderate and severe dementia and the additional number of cases we are likely to experience in Kirklees in the future.
2.4 In 2008 approximately 55% (2,311) of people with dementia had the mild form of the condition and 32% (1,339) have a moderate form. Around 13% (521) are classed as severe, with 70% (360) of those being over 80 years of age. See Figure 2b below.
Dementia Projections by Severity
0
1000
2000
3000
4000
5000
6000
7000
2008 2010 2015 2020 2025
Year
Nu
mb
er
of
Peo
ple
Severe
Moderate
Mild
Fig 2b: Dementia Population Projections by Severity of the Condition

This draft 10.11.09
-
Page 36 of 59
2.5 The graphs in Figures 2a and 2b illustrate that during the period 2008 to 2015, there are likely to be an additional 53812 new cases, of which:
• approximately 297 will have mild dementia;
• 172 will have moderate dementia; and
• 68 will experience severe symptoms of dementia.
2.6 During the period 2015-2020, there are likely to be a further, additional 619 new cases, of which:
• approximately 343 will have mild dementia;
• 201 will have moderate dementia; and
• 77 will experience severe symptoms of dementia.
2.7 The period 2020-2025 is projected to exhibit the largest growth in numbers, with approximately an additional 918 new cases, of which:
• approximately 509 will have a mild dementia;
• 295 will have moderate dementia; and
• 115 will experience severe dementia.
2.8 Estimates suggest that although only 1790 people have a confirmed diagnosis at present;
• Approximately 1,600+ people with mild-moderate dementia may be living in the community and not accessing any health and social care support.
• Approximately 1,200+ people with moderate dementia will continue to live at home with varying degrees of support from a community care service, e.g. telecare, day care, home care etc.
• Approximately 1,200 people with moderate- severe dementia will be living in a long term residential setting.
2.9 The Alzheimers report: Dementia UK 200713 indicated that 49% of day care users and 36% of home care users were likely to have mid-severe cognitive impairment related to dementias.
12 Please note that population trends may not be exact. We acknowledge that future predictions can fluctuate and may become less definite the further into the future we predict; they are the best current estimates
13 Section 5.2 of the main document
This draft 10.11.09
-
Page 37 of 59
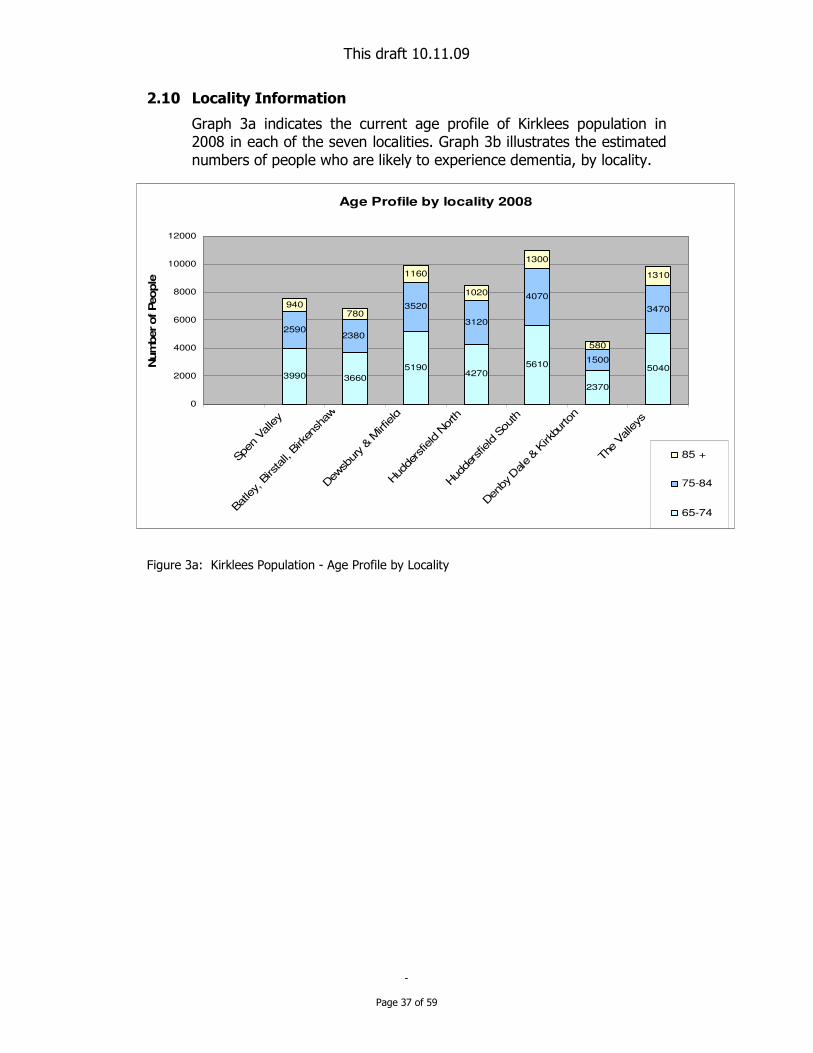
2.10 Locality Information
Graph 3a indicates the current age profile of Kirklees population in 2008 in each of the seven localities. Graph 3b illustrates the estimated numbers of people who are likely to experience dementia, by locality.
Figure 3a: Kirklees Population - Age Profile by Locality
Age Profile by locality 2008
3990 3660
51904270
5610
2370
5040
2590
3520
3120
4070
1500
3470940
780
1160
1020
1300
580
1310
2380
0
2000
4000
6000
8000
10000
12000
Spe
n Valley
Batley, B
irstall, B
irken
shaw
Dew
sbury & M
irfield
Hud
dersfie
ld N
orth
Hud
dersfie
ld S
outh
Den
by D
ale & K
irkbu
rton
The
Valleys
Num
ber of People
85 +
75-84
65-74

This draft 10.11.09
-
Page 38 of 59
Estimated No of People with Dementia by Locality 2008
80 73104 85 112
47100
130
176156
202
75
173
235
195
290
255
325
145
327
119
0
100
200
300
400
500
600
700
Spen V
alley
Batley,
Birs
tall, B
irkens
haw
Dewsb
ury &
Mirf
ield
Hudde
rsfie
ld N
orth
Hudders
field
Sout
h
Denby
Dal
e & K
irkbu
rton
The Valle
ys
No
s o
f p
eo
ple
lik
ely
to
ha
ve
a d
em
en
tia
85+ (1in 4)
75-84(1in 20)
65-74(1in 50)
Figure 3b: Estimated Number of People with Dementia in Kirklees in 2008, by Locality
2.11 These statistics provide information which indicates where there is likely to be highest demand for services/ support and enables us to target support closer to home. The information clearly suggests that the highest numbers of people affected are likely to live in Huddersfield South, The Valleys and Dewsbury and Mirfield
2.12 Early Onset Dementia (a term that includes anyone diagnosed with dementia under the age of 65) will increase. PANSI14 data indicates that for Kirklees, the numbers of people predicted to have early onset dementia (EOD) will increase from 102 currently to 114 by 2025 (Figure 4a below).
14 Pansi.org.uk

This draft 10.11.09
-
Page 39 of 59
Figure 4a: Numbers of people predicted to experience early onset dementia in the Yorkshire and Humber Region, by Local Authority District15
Some 65 people with EOD are in touch with mental health support, alongside 15 people supported by alcohol treatment. Social services support solutions, which are limited, do not appear to meet individual need. At least a further 22 people are unknown. We also know that only 34 are supported by the Alzheimer’s society.
2.13 Alcohol Related Dementia - Korsakoff’s syndrome. The national dementia strategy anticipates that 10% of people with early onset dementia will have it because of alcohol misuse. A detailed study has been conducted of Lifeline’s work and there are currently 15 cases where alcohol related dementia is an issue in Kirklees.
2.14 Black and Minority Communities (BME) It is worth noting that 6.1% of people with dementia among BME groups are likely to be people with young onset dementia, compared with only 2.2% for the UK population. This is a reflection of the younger age profile of BME communities.
Kirklees has a large BME community accounting for 12% of the community. It is therefore predicted that the number of older people with dementia from BME groups will rise quickly and there will be an increased demand for appropriate, culturally sensitive, accessible health and social care.
15 Yorkshire and Humber Improvement Partnership (YHIP) Dementia in Yorkshire and Humber a Demographic Profile (2009)

This draft 10.11.09
-
Page 40 of 59
2.15 Carers Family carers are the most important resource available for people with dementia. Many carers of older people with dementia are themselves older and up to 60% are spouses or partners. Carers of people with dementia generally experience greater stress than other carers. Nearly one half of carers have some kind of mental health problem themselves and one third of carers have depression.
Carers tell us that the most difficult problems are coping with personality changes, lack of every day conversation, excessive demands, criticism, disturbance at night and wandering, incontinence.
2.16 Older Prisoners. The number of prisoners aged 60+ has increased by 300% in the last 10 years and is expected to continue to increase in the future. This population will also require access to professional mental health support.
2.17 Identified Needs The Joint Strategic Needs Assessment (JSNA)16 has given us a good understanding of current levels of diagnosis v predicted prevalence and of forecasted future prevalence of dementia. We have established that currently there is a relatively low level of diagnosis (approximately 40%). We have also mapped current service provision and identified a level of unmet need for:
• People with early onset dementia
• People with alcohol related dementia
• People from BME communities- diagnosis is very low and people are not accessing support services;
• Carer support,- including education, peer support, respite and night time support
• Access to flexible community support services ( including housing support) to support people with dementia to remain safely at home
• Access to mainstream services, including leisure activities and physical activity
• Support to prevent unnecessary or prolonged hospitalisation
• End of life care - advanced care planning, anticipatory drugs prescribing, and preferred place of dying.
2.18 Assuming that treatment, current care pathways and provision of services remained the same in Kirklees17 by 2025 the impact on services would be as follows:
• Registered EMI Nursing and residential care capacity would need to increase from 600 beds to 2,150 beds;
16 http://www.kirklees.gov.uk/community/statistics/jsna/jsna.shtml 17 Based upon predictions of the numbers of people with dementia, current provision and forecasts as per Poppi.org.uk

This draft 10.11.09
-
Page 41 of 59
• Community care services would need to provide an increasing range of services to support an increasing number of people with dementia at home - predicted increase from 1,200 people to 1,900 people;
• The number of people not accessing any statutory involvement will increase from approximately 1,600 people to 2,370 people;
• The numbers of people accessing mental health services such as memory monitoring and Community Mental Health Teams are also forecasted to increase.
• The majority of people with dementia would continue to die in hospital or residential care rather than at home or in a hospice.
It is clear that the current care pathway and model of care will not be financially sustainable and will not deliver our vision to support people with dementia and their carers to live life to the full and delay or prevent the need for more costly service solutions.
2.19 Outcomes
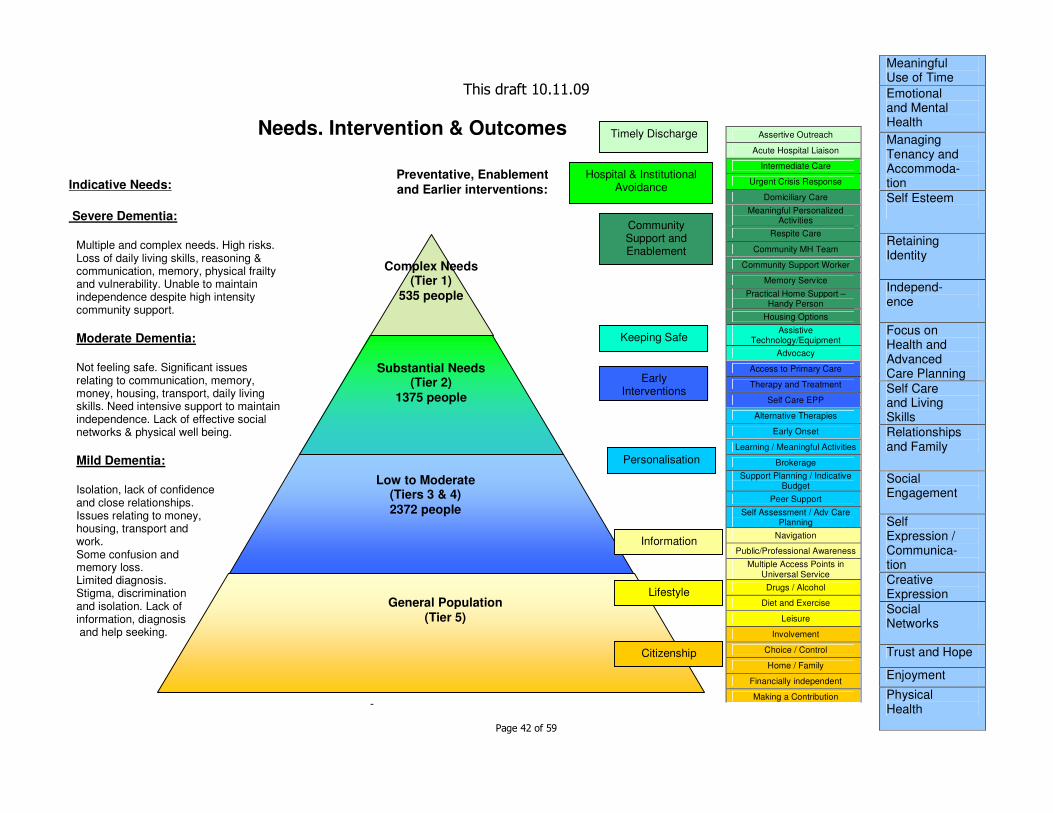
The model below aims to describe the indicative needs of people with mild, moderate and severe dementia, (left of the diagram) the approximate numbers of people at the various stages of the ‘journey’ ( triangle), the potential breadth of preventative, enablement and earlier interventions (yellow-green boxes) that may be provided and the outcomes that they aim to achieve for people ( blue right hand side of diagram.
This draft 10.11.09
-
Page 42 of 59
Assertive Outreach
Acute Hospital Liaison
Intermediate Care
Urgent Crisis Response
Domiciliary Care
Meaningful Personalized Activities
Respite Care
Community MH Team
Community Support Worker
Memory Service
Practical Home Support – Handy Person
Housing Options
Assistive Technology/Equipment
Advocacy
Access to Primary Care
Therapy and Treatment
Self Care EPP
Alternative Therapies
Early Onset
Learning / Meaningful Activities
Brokerage
Support Planning / Indicative Budget
Peer Support
Self Assessment / Adv Care Planning
Navigation
Public/Professional Awareness
Multiple Access Points in Universal Service
Drugs / Alcohol
Diet and Exercise
Leisure
Involvement
Choice / Control
Home / Family
Financially independent
Making a Contribution
Timely Discharge
Hospital & Institutional Avoidance
Community Support and Enablement
Keeping Safe
Early Interventions
Personalisation
Information
Lifestyle
Citizenship
Indicative Needs:
Severe Dementia:
Multiple and complex needs. High risks. Loss of daily living skills, reasoning & communication, memory, physical frailty and vulnerability. Unable to maintain independence despite high intensity community support.
Moderate Dementia:
Not feeling safe. Significant issues relating to communication, memory, money, housing, transport, daily living skills. Need intensive support to maintain independence. Lack of effective social networks & physical well being.
Mild Dementia:
Isolation, lack of confidence and close relationships. Issues relating to money, housing, transport and work. Some confusion and memory loss. Limited diagnosis. Stigma, discrimination and isolation. Lack of information, diagnosis and help seeking.
Preventative, Enablement
and Earlier interventions:
Needs, Intervention & Outcomes
Complex Needs (Tier 1)
535 people
Substantial Needs (Tier 2)
1375 people
Low to Moderate (Tiers 3 & 4)
2372 people
General Population (Tier 5)
Meaningful Use of Time
Emotional and Mental Health
Managing Tenancy and Accommoda-tion
Self Esteem
Retaining Identity
Independ- ence
Focus on Health and Advanced Care Planning
Self Care and Living Skills
Relationships and Family
Social Engagement
Self Expression / Communica- tion
Creative Expression
Social Networks
Trust and Hope
Enjoyment
Physical Health

This draft 10.11.09
-
Page 43 of 59
APPENDIX 4
SUMMARY OF KEY PRIORITIES
1. ADULT SERVICES
Priority Link to NDS Objective No
Lead Officer(s)
Improve Carer Support NDS 2,4,5,7 Gill Neal
Develop a comprehensive community personal support service NDS 6 Sue Richards
Keep an eye on new emerging assistive technology and telecare NDS 10 Frances Barnes
Improve care for people with dementia in care homes NDS 11 Keith Smith
Develop a joint workforce planning and dementia training strategy which clearly identifies core competencies for all staff from all sectors
NDS 13 Peter Kelly
Develop a joint commissioning strategy for dementia NDS 14 Keith Smith/ Julie Orlinski
Strengthen contract management and inspection across all settings NDS 15 Margaret Watt
2. NHS KIRKLEES
Priority
Link to NDS
Objective No
Lead Officer(s)
Improve early diagnosis and intervention – Primary Care and Memory Services etc NDS 2 Vicky Dutchburn
Provide good quality information for those diagnosed with dementia and their carers NDS 3 All Workstreams
Improve carer support NDS 2,4,5,6,7 Naomi Reay
Improve the quality of care within hospitals for people with dementia NDS 8 Sharon Hall
Improve intermediate care for people with dementia NDS 9 Paul Howatson/Naomi Reay
Improve care for people with dementia in care homes NDS 11 Paul Howatson/Vicky Dutchburn
Improve end of life care for people with dementia NDS 12 Loraine Turner
Develop a joint workforce planning and dementia training strategy which clearly identifies core competencies for all staff from all sectors
NDS 13 Laura Campbell
Develop a joint commissioning strategy for dementia NDS 14 Vicky Dutchburn/Paul Howatson

This draft 10.11.09
-
Page 44 of 59
3. PUBLIC HEALTH
Priority
Link to NDS
Objective No
Lead Officer(s)
Improve public awareness and understanding of dementia, provide health promotion message and benefits of timely diagnosis.
NDS 1 Karen Coleman/Mick Gudgeon
4. STRATEGIC HOUSING
Priority
Link to NDS Objectives No
Lead Officer(s)
Develop more supported housing options, extra care provision and practical home maintenance for people with dementia.
NDS 6 & 10 Paul Evans/Emma Hanley

This draft 10.11.09
-
Page 45 of 59
APPENDIX 5
KIRKLEES DEMENTIA STRATEGY – ACTION PLAN
This action plan has been developed to meet both the objectives of the National Dementia Strategy and the key outcomes and priorities set out in the Older People’s Partnership Board’s Living Life to the Full: Dementia Strategy.
OUTCOME 1: IMPROVED HEALTH AND WELLBEING
Objective Action 10/11 11/12 12/13 13/14 Lead
1.1.1 Implement Kirklees wide intermediate care pathway. Commission additional professional mental health support for the pathway
����
1.1.2 Review pathway and identify gaps and redesign opportunities e.g. Hospital at Home, Home form Hospital schemes
����
����
1.1 Develop a Kirklees wide intermediate care pathway which is inclusive of people with dementia, and provides equitable, high quality integrated services which promote faster recovery from illness, reduce the need for hospital admission, support timely discharge and maximise independent living. NDS 9
1.1.3 Implement revised service provision
����
NHS Kirklees/ Adult Services
1.2.1 Develop pathway and service specification �
� �
1.2.2 Commission services �
1.2 Improve urgent care responses to people with dementia, delirium and/or falls, to mobilise intermediate care services, avoid inappropriate attendance at A&E and hospital admissions. NDS 9
1.2.3 Review pathway and implement improvements
NHS Kirklees
1.3 To provide health and social care closer to home. NDS6
1.3.1 Refurbish Community Hospitals- dementia friendly environment, signage, lightening, décor etc
1.3.2 Environment audits to be arranged (SEAT Tool)
�
�
NHS Kirklees/ Adult Services

This draft 10.11.09
-
Page 46 of 59
OUTCOME 2: IMPROVE SUPPORT IN DAILY LIVING
Objective Action 10/11 11/12 12/13 13/14 Lead
2.1.1 Commission outcome focused home care services to meet the needs of people with mental health needs - continuity of care, longer visits and social interaction time, integrated services, e.g. continence care, flexible enough to vary tasks according to need.
� Adult Services/SWYPFT
2.1.2 Implement an enablement approach within home care services which is outcome focused, encourages independence and focuses on ability rather than lost skill
� �
2.1 Support people with dementia to maintain their independence and remain at home for as long as they wish to. NDS 6
2.1.3 Commission specialist home care services for those with highest complex needs and basic training for lower level need.
�
�
Adult Services
2.2.1 Review current range of technology available. �
2.2.2 Identify and pilot personalised telecare packages �
2.2 Use emerging assistive technology and telecare to support people with dementia to remain independent longer and manage risk. NDS 6 & 10
2.2.3 Extend info and access to a wider range of equipment
�
Adult Services/NHS Kirklees

This draft 10.11.09
-
Page 47 of 59
OUTCOME 3: IMPROVED ACCESS TO LEISURE AND SOCIAL ACTIVITIES
Objective Action 10/11 11/12 12/13 13/14 Lead
3.1.1 Commission a range of short breaks and meaningful day opportunities providing personalised social activity which maintain skills and maximise individual abilities/potential.
�
�
3.1.2 Complete the review and restructure of in-house daytime opportunities to meet the specialist requirements of older people with dementia and higher levels of need, to include integrated mental health support, eg memory assessment and therapies.
�
Adult Services
Adult Services/NHS Kirklees/SWYPFT
3.1 Provide access to meaningful personalised activities and support to access to mainstream activities.
Improve access to physical activity.
NDS 6
3.2.1 Commission day time opportunities support to meet the needs of younger people with early onset dementia
� Adult services
OUTCOME 4: A SAFE PLACE TO LIVE
Objective Action 10/11 11/12 12/13 13/14 Lead
4.1 Increase the range of housing options available to older people with mental health needs. NDS 10
4.1.1 Commission extra care units with appropriate dementia friendly design and specific dementia care supports
� � Strategic Housing
4.2 Improve the quality of EMI care within residential and nursing homes. NDS 11 & 13
4.2.1 Commission additional contract management support for the nursing sector
� �
NHS Kirklees/ Adult
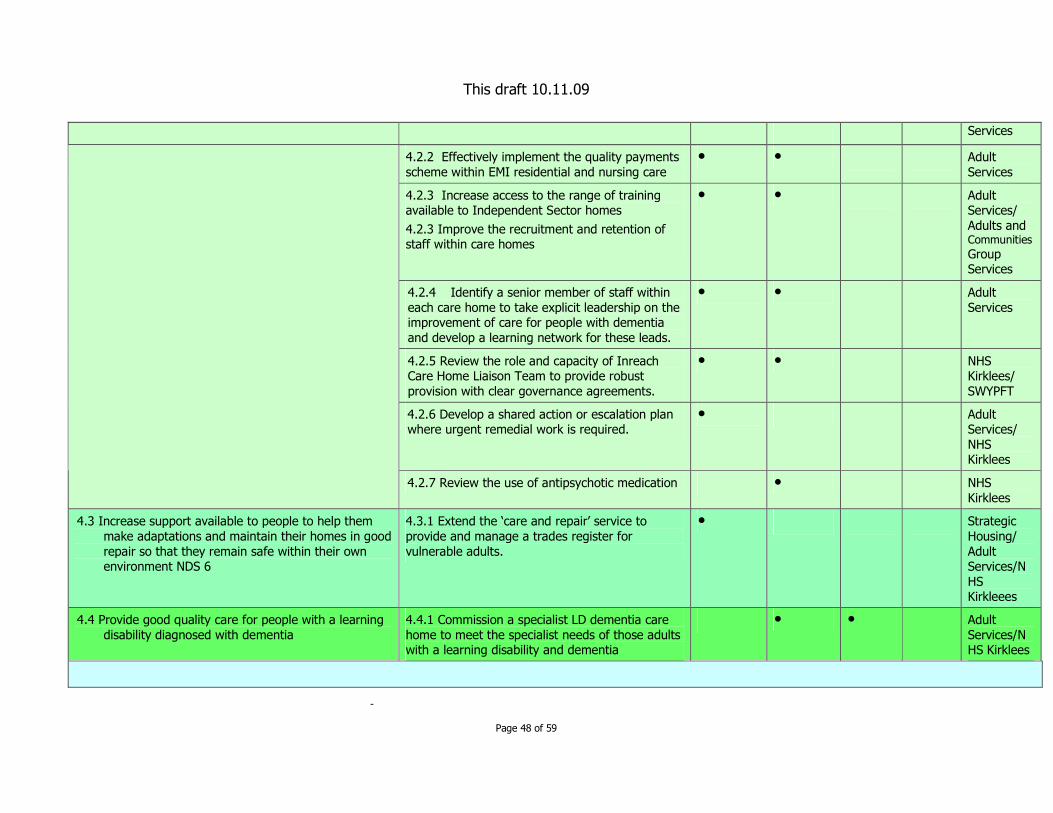
This draft 10.11.09
-
Page 48 of 59
Services
4.2.2 Effectively implement the quality payments scheme within EMI residential and nursing care
� � Adult Services
4.2.3 Increase access to the range of training available to Independent Sector homes
4.2.3 Improve the recruitment and retention of staff within care homes
� � Adult Services/ Adults and Communities
Group Services
4.2.4 Identify a senior member of staff within each care home to take explicit leadership on the improvement of care for people with dementia and develop a learning network for these leads.
� � Adult Services
4.2.5 Review the role and capacity of Inreach Care Home Liaison Team to provide robust provision with clear governance agreements.
� � NHS Kirklees/ SWYPFT
4.2.6 Develop a shared action or escalation plan where urgent remedial work is required.
� Adult Services/ NHS Kirklees
4.2.7 Review the use of antipsychotic medication � NHS Kirklees
4.3 Increase support available to people to help them make adaptations and maintain their homes in good repair so that they remain safe within their own environment NDS 6
4.3.1 Extend the ‘care and repair’ service to provide and manage a trades register for vulnerable adults.
� Strategic Housing/ Adult Services/NHS Kirkleees
4.4 Provide good quality care for people with a learning disability diagnosed with dementia
4.4.1 Commission a specialist LD dementia care home to meet the specialist needs of those adults with a learning disability and dementia
� � Adult Services/NHS Kirklees

This draft 10.11.09
-
Page 49 of 59
OUTCOME 5: IMPROVED INFORMATION AND ACCESS TO SERVICES
Objective Action 10/11 11/12 12/13 13/14 Lead
5.1.1 Develop a local public information campaign. Strong prevention message needed - link to better cerebrovascular health, lifestyle, early diagnosis and challenge the view that there is little that can be done, symptoms of dementia, risk factors and lifestyle.
5.1.2 Include website and local media.
�
�
Public Health/ Adult Services/ Voluntary Sector
5.1.3 Develop a targeted campaign for specific groups, e.g. Gateway to care, assessment staff, frontline service points, older people’s organisations. other Council services. Link to Be Head Strong and Living Life to the Full.
� � Adults and Communities Group Services/ Adult Services/ NHS Kirklees
5.1.4 Develop educational programmes and intergenerational work to encourage lifestyle change and reduce the stigma associated with dementia.
� Children and Young People Service/ Adult Services/NHS Kirklees
5.1 Increase public and professional awareness and understanding of what dementia is and isn’t. NDS 1
5.1.5 Develop universal information in partnership with the voluntary sector - to include:
• self care,
• information prescriptions
• and signposting. NDS 1 & 3
•
�
�
Alzheimer’s Society/ NHS Kirklees/ SWYPFT
5.2 Enable easy access to care, support and advice following diagnosis. NDS 4
5.2.1 Implement the Dementia Advisor model (focus South Asian community).
�
Adult services/ Alzheimer’s

This draft 10.11.09
-
Page 50 of 59
5.2.2 Evaluate the Dementia Advisor role �
5.2.3 Implement recommendations �
Society/NHS Kirklees/SWYPFT
5.3.1 Commission appropriate GP awareness programme.
5.3.2 Develop GP information pack/information
� � NHS Kirklees
5.3.3 Verify and interrogate information sources to establish full picture of demand/need i.e SWYPFT, PCT, LA, Vol sector
5.3.4 Monitor through QOF Register IAP (Improved Access to psychological therapies) service and Memory Monitoring
�
�
�
5.3.5 Review and re-launch pathway/protocol �
5.3.6 Review capacity of and demand on Memory Service.
�
5.3 Increase earlier diagnosis of dementia NDS 2:
5.3.7 Remodel service to meet demand in line with NICE guidance
�
NHS Kirklees/ Adult Services
OUTCOME 6: CITIZENSHIP and INVOLVEMENT
Objective Action 10/11 11/12 12/13 13/14 Lead
6.1 Improve peer support and opportunities to access practical support and advice from other people living with dementia and their carers. NDS 5
6.1.1 Commission an expert patients programme specifically for people with dementia
�
NHS Kirklees/ Adult Services

This draft 10.11.09
-
Page 51 of 59
6.1.2 Commission a Looking After Me (LAM) programme for carers
�
6.1.3 Extend capacity of existing VCS contracts to provide peer support, including culturally specific groups.
�
OUTCOME 7: IMPROVE CHOICE AND CONTROL FOR INDIVIDUALS
Objective Action Year 1 Year 2 Year 3 Lead
7.1 Improve choice and control for people with dementia. . NDS 2
7.1.1 Empower people to report symptoms to GPs earlier- monitor through GP register?
� � � NHS Kirklees
7.2.1 Implement personalised outcome focused support planning
�
�
7.2 Increase numbers of people with dementia accessing direct payments and Individual budgets. NDS 6
7.2.2 Increase support for people with dementia and their carers to access direct payments and individualised budgets as part of the personalisation agenda
�
�
Adult Services
7.3. (Improve choice and control for people with dementia and their carers D
NDS 6
7.3.1 Continue to develop a choice of low level services within the voluntary sector which promote independence, social inclusion, learning and active ageing and awareness and understanding of dementia.
� Adult Services
7.4 Support people with mental health needs to make their wishes understood. NDS 11
7.4.1Commission additional advocacy capacity to meet DOL/safeguarding pressures.
� Adult Services

This draft 10.11.09
-
Page 52 of 59
OUTCOME 8: HAVE ENOUGH MONEY TO LIVE A GOOD LIFE
Objective Action 10/11 11/12 12/13 13/14 Lead
8.1.1 Increase take up of benefits- target people with information regarding benefits advice throughout the care pathway.
� �
�
8.1 Ensure that people have enough money to live a good life. NDS11
8.1.2 Monitor increased take up of benefits for older people
�
�
Adult Services
OUTCOME 9: PERSONAL DIGNITY & RESPECT
Objective Action 10/11 11/12 12/13 13/14 Lead
9.1.1 Embed the Dignity in Care Challenge in the contract specifications for the provision of dementia care within hospitals, care homes, community support services and end of life care.
� �
9.1.2 Extend Dignity in care network and recruit more Dementia Champions, support ‘whistle blowing’, raise awareness through training and publicity across all partners.
�
�
9.1.3 Deprivation of Liberty and safeguarding training and investigation to be compulsory for all providers and explicit within contracts. NDS 6, 11 & 13
�
�
9.1 Improve the quality of care for people and ensure that they are treated with dignity and respect . NDS 8, 11,12,13 & 15
9.1.4 Embed the use of Action Plans and audit tools which raise awareness, guidance, screening and training regarding nutrition and hydration
�
�
Adult Services/ NHS Kirklees
OUTCOME 10: CARERS SUPPORTED TO CARE AND HAVE A LIFE OF THEIR OWN
Objective Action 10/11 11/12 12/13 13/14 Lead
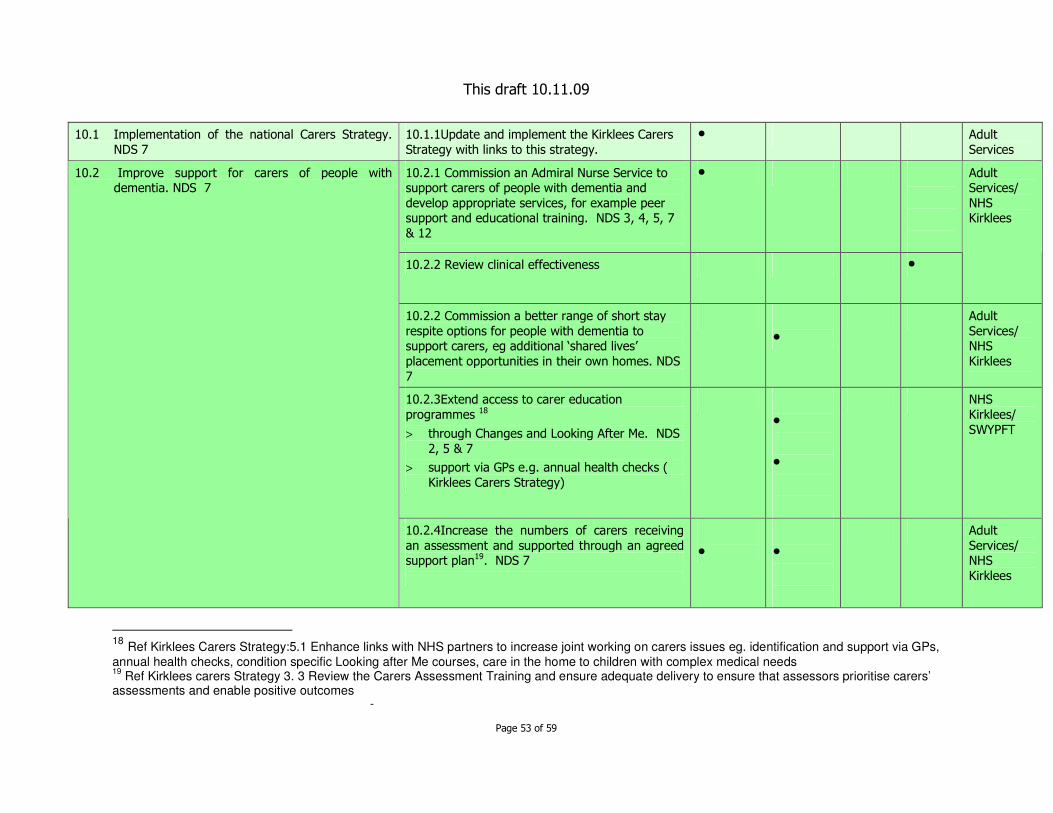
This draft 10.11.09
-
Page 53 of 59
10.1 Implementation of the national Carers Strategy. NDS 7
10.1.1Update and implement the Kirklees Carers Strategy with links to this strategy.
� Adult Services
10.2.1 Commission an Admiral Nurse Service to support carers of people with dementia and develop appropriate services, for example peer support and educational training. NDS 3, 4, 5, 7 & 12
�
10.2.2 Review clinical effectiveness �
Adult Services/ NHS Kirklees
10.2.2 Commission a better range of short stay respite options for people with dementia to support carers, eg additional ‘shared lives’ placement opportunities in their own homes. NDS 7
�
Adult Services/ NHS Kirklees
10.2.3Extend access to carer education programmes 18
> through Changes and Looking After Me. NDS 2, 5 & 7
> support via GPs e.g. annual health checks ( Kirklees Carers Strategy)
�
�
NHS Kirklees/ SWYPFT
10.2 Improve support for carers of people with dementia. NDS 7
10.2.4Increase the numbers of carers receiving an assessment and supported through an agreed support plan19. NDS 7
�
�
Adult Services/ NHS Kirklees
18 Ref Kirklees Carers Strategy:5.1 Enhance links with NHS partners to increase joint working on carers issues eg. identification and support via GPs,
annual health checks, condition specific Looking after Me courses, care in the home to children with complex medical needs 19
Ref Kirklees carers Strategy 3. 3 Review the Carers Assessment Training and ensure adequate delivery to ensure that assessors prioritise carers’ assessments and enable positive outcomes

This draft 10.11.09
-
Page 54 of 59
10.2.5 Commission additional capacity within the advice and information service for carers and people with dementia. NDS3
�
NHS Kirklees/ Adult Services
10.2.6 Commission carer support that meets the needs of carers of younger people with dementia20
�
Adult Services
OUTCOME 11: AN INFORMED AND EFFECTIVE WORKFORCE
Objective Action 10/11 11/12 12/13 13/14 Lead
11.1.1 Develop a joint workforce planning and dementia training strategy
�
�
11.1.2 Implement the strategy �
11.1.3 monitor and review impact �
Adult services and NHS Kirklees
Adults and Communities Group Services /Adult Services
11.1.4 Training and competencies in dementia care to be compulsory for all commissioned and in-house services, homecare providers, day care providers, residential care providers
�
11.1 To have an informed, trained and effective workforce. NDS 13
11.1.5 Effective training and continuous professional development in dementia care to be provided to all health professionals responsible for
� NHS Kirklees
20
Ref Kirklees Carers Strategy 4.4 Enhance support for carers of people with dementia, especially early onset dementia

This draft 10.11.09
-
Page 55 of 59
care of the elderly. NDS 13
11.1.6 Staff working within housing and housing related services to develop skills needed to provide good quality care and floating support for people with dementia. NDS 10 & 13
�
�
Strategic Housing/ Supporting People
11.1.7 Identify the training needs of professionals responsible for the care of people with learning disabilities. NDS 13
�
�
Adult Services
OUTCOME 12: IMPROVE THE QUALITY OF CARE FOR PEOPLE WITH DEMENTIA IN HOSPITAL
Objective Action 10/11 11/12 12/13 13/14 Lead
12.1.1 Identify senior clinicians and build leadership within hospitals. (1/10 consultant per week per hospital)
�
12.1 Improve the quality of care in general hospitals
NDS 8
12.1.2 Identify dignity/dementia champions on all wards
�
NHS Kirklees
12.2.1Define care pathway for people with dementia.
�
12.2.2Improve diagnosis and management of dementia and delirium on wards.
� �
12.2 Reduce the average length of stay in hospital for people with dementia. NDS8
12.2.3Improve the environment for people with a dementia, e.g. signage, access to food and drinks.
� � �

This draft 10.11.09
-
Page 56 of 59
12.3.1Improve nutrition and hydration for people with dementia/delirium in hospital
�
12.3.2Review Acute Liaison Team input. �
12.3 Improve diagnosis of dementia during hospital stays. NDS 8
12.3.3 Implement the Vulnerable In-Patients card �
OUTCOME 13: IMPROVE END OF LIFE CARE FOR PEOPLE WITH DEMENTIA
Objective Action 10/11 11/12 12/13 13/14 Lead
13.1.1 Identify end of life responsibilities within the dementia care pathway.
�
13.1 Increase the numbers of people supported to die in the place of their choice. NDS 12
13.1.2 Commission end of life care support at home
�
NHS Kirklees
13.2.1 Implement the use of end of life tools in all care settings, i.e. GSF, LCP and PPC. (Gold Standards framework, Liverpool care pathway, and Preferred Place of care)
� � 13.2 Improve the quality of care provided for people with dementia at the end of their life. NDS 12
13.2.1 Review the use of advanced prescribing at end of life
�
OUTCOME 14: IMPROVED QUALITY OF SERVICES
Objective Action 10/11 11/12 12/13 13/14 Lead
14.1 Commission nursing expertise to support contract monitoring within care homes. NDS 11 & 15
� � NHS Kirklees
14.2 Strengthen all contract monitoring arrangements. NDS 15
� � Adult Services
14.1 Improve the quality of service provided to people with dementia through commissioning, inspection and contract management.
14.3 Involve LINKS in inspection of care homes � � NHS

This draft 10.11.09
-
Page 57 of 59
and hospitals. NDS 15
Kirklees
OUTCOME 15: EARLY ONSET DEMENTIA
Objective Action 10/11 11/12 12/13 13/14 Lead
15.1.1 Investigate unmet need for younger people with dementia e.g. alcohol related dementia
�
15.1.2 Ensure service user involvement �
15.1.3 Identify service gaps �
15.1.4 Review and/or decommission services �
15.1 Ensure all commissioning activity meets the needs of people experiencing early onset dementia.
15.1.5 Commission new services �
Adult Services/ NHS Kirklees

This draft 10.11.09
-
Page 58 of 59
APPENDIX 6
WHAT IS DEMENTIA?/TYPES OF DEMENTIA
Alzheimer’s disease accounts for 62% of dementias in England. It changes the chemistry and structure of the brain, causing brain cells to die.
Vascular dementia is caused by problems with the supply of oxygen to the brain following a stroke or small blood vessel disease. Vascular dementia along with those mixed vascular with Alzheimer’s dementias, make up around 30% of the total. Conditions that affect the circulation of blood to the brain, such as hypertension, can contribute to vascular dementia.
Dementia with Lewys Bodies is caused by protein deposits that develop inside nerve cells in the brain and interrupt its normal functioning. It shares symptoms with Parkinson’s disease including, slowness of movement. It accounts for 4% of dementias in England.
Fronto-temporal dementia is a rare form of dementia encompassing Pick’s disease, and affecting 2% of people with dementia in England. It often affects the under 65’s with dramatic effects on behaviour and personality rather than memory, in the early stages.
Source: National Audit Office analysis
Korsakoff’s syndrome is a brain disorder usually associated with heavy drinking over a long period. Not strictly a dementia, but people experience loss of short term memory. Korsakoff’s syndrome is caused by a lack o thiamine (vitamin B1) which effects the brain and nervous system. It cannot be diagnosed unless the person has abstained from alcohol for at least four to five weeks. Those affected tend to be men between ages of 46 and 65. Women can also be affected. They tend to develop this at a slightly younger age. It may take around 20 years to develop. The progress of Korsakoff’s can be halted if the person abstains from alcohol and adopts a healthy diet. Improvement usually occurs within a period of 2 years. About a quarter of those affected make good recovery and about half a partial recovery and need support to manage their daily living.

This draft 10.11.09
-
Page 59 of 59
ACKNOWLEDGEMENTS We would like to thank the following for their contributions in bringing together this strategy for improving supports for people with dementia and their carers in Kirklees. Older Peoples Partnership Board : special thanks to representatives of KOP (Kirklees Older Peoples network) Doreen Denton and Sheila Horton South West Yorkshire Mental Health Partnership Foundation Trust Kirklees NHS Kirklees Council Adult Services Mental Health Partnership Board Carers Strategy Group








![Crando Plugins en ImageJ [de http://www.imagingbook.com/fileadmin/goodies/ijtutorial/tutorial171.pdf]](https://img.pdfslide.us/doc/110x75/555585f0b4c905a5178b4630/crando-plugins-en-imagej-de-httpwwwimagingbookcomfileadmingoodiesijtutorialtutorial171pdf.jpg)