Embed Size (px)
Citation preview

8/31/14
1
Developing Treatment Strategies Hypertension Management: What’s High and What’s not
Amelie Hollier, DNP, FNP-‐BC, FAANP Advanced PracAce EducaAon Associates
JNC 8 Guidelines
• JNC 7: 2003 • JNC 8: 2013
Stone NJ, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce AtheroscleroFc Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart AssociaFon Task Force on PracFce Guidelines. CirculaFon 2013.
JNC 8 Guidelines
• Controversial! • ACC/AHA released a statement: AnAcipate new guideline in 2015
Stone NJ, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce AtheroscleroFc Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart AssociaFon Task Force on PracFce Guidelines. CirculaFon 2013.

8/31/14
2
JNC 8 Guidelines • Evidence Based (different from JNC 7)
• Lead author, Dr. Paul James, “we wanted to make the message very simple”
• 14 pages (vs. 51 pages for the lipids) Stone NJ, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol
to Reduce AtheroscleroFc Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart AssociaFon Task Force on PracFce Guidelines. CirculaFon 2013.
“Consensus” Lifestyle Changes (evidence based) • Healthy EaAng Habits (Mediterranean diet?)
• Limit Na intake to 2400 mg daily • Stop smoking • Achieve healthy weight • Regular physical acAvity
JNC 8: BP by Age
140/90 150/90 < 60 years old > 60 years
DM CKD
Stone NJ, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce AtheroscleroFc Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart AssociaFon Task Force on PracFce Guidelines. CirculaFon 2013.
Start Pharmacotherapy* if BP exceeds:
*ConAnue lifestyle changes

8/31/14
3
JNC 8: PaAents with Diabetes • < 140/90 mmHg • Evidence Level A (high quality RCTs) • Unproven clinical benefit to lower BPs more than 140/90
Curb JD, Pressel SL, Cutler JA, et al. Effect of diureFc-‐based anFhypertensive treatment on cardiovascular disease risk in older diabeFc paFents with isolated systolic hypertension. Systolic Hypertension in the Elderly Program CooperaFve Research Group. JAMA 1996;276:1886-‐92. Tuomilehto J, Rastenyte D, Birkenhager WH, et al. Effects of calcium-‐channel blockade in older paFents with diabetes and systolic hypertension. Systolic Hypertension in Europe Trial InvesFgators. N Engl J Med 1999;340:677-‐84. UK ProspecFve Diabetes Study Group. Tight blood pressure control and risk of macrovascular and microvascular complicaFons in type 2 diabetes: UKPDS 38. BMJ 1998;317:703-‐13. ACCORD Study Group, Cushman WC, Evans GW, et al. Effects of intensive blood pressure control in type 2 diabetes mellitus. N Engl J Med 2010;362:1575-‐85.
American Diabetes AssociaAon • BP Goal < 140/80 mmHg • ACCORD: Intensive BP lowering did not result in reduced risk of fatal or non-‐fatal CV events in adults with Type 2 DM who were at high risk of these events (and they had more side effects related to intensive treatment)
ACCORD Study Group, Cushman WC, Evans GW, et al. Effects of intensive blood pressure control in type 2 diabetes mellitus. N Engl J Med 2010;362:1575-‐85.
JNC 8: PaAents > Age 60 years
• BP target < 150/90 mmHg • Evidence Level B (low quality RCTs) • If toleraAng lower BP, then OK
JATOS Study Group. Principal results of the Japanese trial to assess opFmal systolic blood pressure in elderly hypertensive paFents (JATOS). Hypertens Res 2008;31:2115-‐27. Oglihara T, Saruta T, Rakugi H, et al. Target blood pressure for treatment of isolated systolic hypertension in the elderly: valsartan in elderly Isolated systolic hypertension study. Hypertension 2010;56:196-‐202.

8/31/14
4
What Med?
JNC 8: IniAal Choice African American With or without DM
Non-‐Black With or without DM
Thiazide diureAc Thiazide diureAc
Calcium channel blocker
Calcium channel blocker
ACE
ARB
Which one? Thiazide or CCB???
8/31/14
5
Thiazide Diuretics
• HCTZ
• Chlorthalidone
• Indapamide
Hydrochlorothiazide • Most commonly prescribed diuretic for HTN in the world!
• Starts working in about 2 hours
• Half life 6-12 hours
• Sulfa allergy precaution!!!
Chlorthalidone • Most evidence for improved CV outcomes
• Twice as potent as HCTZ
• Appears to work in the ascending limb of Henle’s loop (2.6 h initial diuresis occurs)
• Longer half-life (up to 72 hours vs. 6-12 with HCTZ)
• Longer control of BP!!!

8/31/14
6
Indapamide • Half life is about 14 hours
• Indications: HTN, salt and fluid retention associated with HF
• Disadvantage: Not found in combo with other BP meds
• Cheap! ($4 drug)
Thiazide Diuretics HCTZ, indapamide, chlorthalidone
• Systolic reduction: 5-16.4 mmHg • Diastolic reduction: 2-9.3 mmHg • Minimal decreases in potassium (check
potassium levels after 2 weeks of therapy).
• Keep K+ at least 4 mm/L • Reduces LVH (equivalent to ACEs?)
Take Home Point!
• Consider chlorthalidone or indapamide
• More evidence for improving cardiovascular outcomes than HCTZ
Need a thiazide?
Weber MA, Schiffrin EL, White WB, et al. Clinical pracFce guidelines for the management of hypertension in the community: a statement by the American Society of Hypertension and the InternaFonal Society of Hypertension. J Clin Hypertens (Greenwich) 2013 Dec 17. doi: 10.1111/jch.12237.
8/31/14
7
JNC 8 Take Home Point
• Thiazides no longer “only” first line agent to treat HTN unless “compelling indicaAons”
52 y/o AA male with long standing, poorly controlled HTN, proteinuria. Average BP= 170/100. Takes no meds.
JNC 8 Target BP < 140/90
• HTN is a MAJOR issue in AA • Earlier onset than in other ethnic groups • Usually of greater severity • HTN is associated with CV and renal complicaAons
JNC 8
Average BP: 170/100
• Goal < 140/90
• > 20/10 points over goal,
• Patient likely needs 2 meds today
2014 evidence-‐based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint NaFonal Commibee (JNC 8). JAMA. 2014;311(5):507.
J Hypertens. 2013;31(7):1281.

8/31/14
8
JNC 8, ESH, ESC
In African Americans…
• Calcium channel blocker
• Diuretic
European SocieFes of Hypertension and Cardiology
2014 evidence-‐based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint NaFonal Commibee (JNC 8). JAMA. 2014;311(5):507.
J Hypertens. 2013;31(7):1281.
A Drug Combo You’ll NEVER find in a pharmacy
CCB plus a thiazide diuretic
Why don’t we do that?
Add thiazide diuretics to ACEs, ARBs, BBs, direct renin inhibitors, etc.

8/31/14
9
Combining 2 Synergistic Drugs
Decreases BP about 5x more than doubling the dose of a single drug! BMJ. 2009;338:b1665.
When you treat HTN…
Seek Synergism!!!!
Take Home Point
Take Home Point! CCBs provide beoer
stroke prevenAon than ACE or ARB in AA.
Stone NJ, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce AtheroscleroFc Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart AssociaFon Task Force on PracFce Guidelines. CirculaFon 2013.

8/31/14
10
Which CCB?
DHPs
Non-DHPs
52 y/o AA male with long standing, poorly controlled HTN, proteinuria. Average BP= 170/100. Takes no meds.
Both will decrease BP. Only one decreases proteinuria.
True or False
Amlodipine is a better choice to treat this patient’s HTN/proteinuria than diltiazem.
Calcium Channel Blockers
Anti-Proteinuric Effect • Diltiazem and verapamil (non-DHPs) • Decrease proteinuria by 30% • DHPs increased proteinuria by 2% • Similar effects if used in combo with
ACE or ARB
Kidney Int. 2004;65(6):1991

8/31/14
11
Calcium Channel Blockers 2 Groups of Agents
DHPs Decrease BP, not HR amlodipine (Norvasc®) felodipine (Plendil®) nicardipine (Cardene®) nifedipine (Procardia®) nisoldipine (Sular®)
Non-DHPs Decrease HR at low doses DILTIAZEM: (Cardizem®, Dilacor®,
Tiazac®) VERAPAMIL: (Isoptin®, Calan®,
Covera® HS, Verelan®)
Non-DHP BP Lowering Effects
• Must use doses >180 mg per day • 240 mg, 300 mg, 360 mg, 420 mg, 520 mg
What medication would be a good synergist with
diltiazem?
If no contraindicaAons, start paAent on 180 mg dilAazem daily
1. Beta blocker 2. ACE 3. ARB 4. DiureAc

8/31/14
12
Rate Lowering CCB + BB
• Doesn’t seem like a good idea!
• Studies indicate usually well tolerated
• But don’t risk it!!!
hbp://dailymed.nlm.nih.gov/dailymed/lookup.cfm?seFd=af12246f-‐890c-‐4c31-‐bb77-‐136f47dda222. Accessed March 20, 2014.
CCB + ACE or ARB • 10 years worth of good outcomes data
• AA, Asians, Caucasians, Hispanics
Hypertension. 2010;56(5):780. Management of high blood pressure in Blacks: an update of the InternaFonal Society on Hypertension in Blacks consensus statement.
When you treat HTN…
Don’t forget about the non DHPs!
Take Home Point
8/31/14
13
JNC 8: IniAal Choice African American With or without DM
Non-‐Black With or without DM
Thiazide diureAc Thiazide diureAc
Calcium channel blocker
Calcium channel blocker
ACE
ARB
JNC 8 Take Home Point
• DiabeAcs no longer treated as different from general populaAon (at least iniAally)
• No deference to ACEs or ARBs
No ACEs or ARBs for DMs iniFally
• PaAents with DM are at increased risk of CV events and nephropathy-‐-‐-‐ACEs and ARBs are beneficial
• ASH: “makes sense to use these first line in paAents with diabetes”

8/31/14
14
Take Home Point! When giving an ACE or ARB
to an AA, add thiazide diureAc!
(or ACE or ARB plus CCB) Erase cultural differences!
Weber MA, Schiffrin EL, White WB, et al. Clinical pracFce guidelines for the management of hypertension in the community: a statement by the American Society of Hypertension and the InternaFonal Society of Hypertension. J Clin Hypertens (Greenwich) 2013 Dec 17. doi: 10.1111/jch.12237.
What about “Non Black” hypertensive
paAents (without DM)?
JNC 8: IniAal Choice African American With or without DM
Non-‐Black With or without DM
Thiazide diureAc Thiazide diureAc
Calcium channel blocker
Calcium channel blocker
ACE
ARB

8/31/14
15
What drug classes are missing from iniFal treatment?
JNC 8: IniAal Choice African American With or without DM
Non-‐Black With or without DM
Thiazide diureAc Thiazide diureAc
Calcium channel blocker
Calcium channel blocker
ACE
ARB
Alpha and Beta Blockers
Associated with worse cardiovascular outcomes data (HTN treatment)
Stone NJ, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce AtheroscleroFc Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart AssociaFon Task Force on PracFce Guidelines. CirculaFon 2013.

8/31/14
16
JNC 8: Chronic Kidney Disease
African American Non-‐Black
ACE ACE
ARB ARB
ACE or ARB even in African American
3 or more Agents??? • Thiazide diuretic • ACE or ARB • CCB • Alpha blocker (have another
reason to give it-BPH) • Beta Blocker (have another
reason to give it-anxiety, angina, rate control, MVP, HF)
3 or more Agents??? FYI • ACE or ARB is always less
effective when given in combo with a Beta blocker
• BB reduce renin secretion and therefore, AT2 formation
8/31/14
17
3 or more Agents??? • Consider referral to HTN specialist
if intensive treatment for 6 months doesn’t bring about normotensive state
• Always suspect secondary hypertension
JNC 8 “FYI” Do not add an ACE plus ARB to a medicaAon regimen; either one or the other—NOT BOTH.
ACE + ARB??? • ONTARGET trial: ramipril plus
telmisartan in 25,000 patients at high risk for CV events (DM or vascular disease)
• Predictable outcomes: hypotension, syncope, hyperkalemia, renal dysfunction

8/31/14
18
ACE + ARB??? Does not improve CV outcomes in: • Patients with DM • Patients with vascular disease • Patients with HTN • Patients Post-MI
• J Hypertens. 2011;29(4):623. Syncope and renal impairment likely
42 y/o male with HTN, dyslipidemia, Pre-‐DM, obese but trying to lose weight
10 mg amlodipine 40 mg lisinopril 25 mg HCTZ
JNC 8 Goal: Reach target BP < 140/90
AM BP Readings PM BP Readings
142/92 146/98
148/94 152/94
150/96 146/90
140/88 148/98
1. Increase HCTZ? 2. Change a medicaAon? 3. Add another medicaAon?
Try Chlorthalidone! DiureAc Average Systolic Drop
25 mg HCTZ -‐4.5 mm Hg (+ 2.1 mm Hg) 12.5 mg
Chlorthalidone -‐15.7 mm Hg (+2.2 mm Hg)
Ernst ME, Carter BL, Goerdt CJ, Steffensmeier JJ, Phillips BB, Zimmerman MB, Bergus GR ComparaFve anFhypertensive effects of hydrochlorothiazide and chlorthalidone on ambulatory and office blood pressure. Hypertension. 2006;47(3):352.
OpAon 2: Change a medicaAon

8/31/14
19
42 y/o male with HTN, dyslipidemia, Pre-‐DM, obese but trying to lose weight.
10 mg amlodipine 40 mg lisinopril 12.5 mg Chlorthalidone
Primary Goal: Reach target BP < 140/90
Day 1-‐7 Ave BP
Day 8-‐14 Ave BP
142/92 140/90 144/94 138/88 140/90 128/82 140/88 130/80 144/90 132/82 138/88 128/78 136/90 130/80
Day 6
Chlorthalidone • Most evidence for improved CV outcomes
• 1.5 -2 times as potent as HCTZ
• Appears to work in the ascending limb of Henle’s loop (2.6 h initial diuresis occurs)
• Longer half-life (up to 72 hours vs. 6-12 hours with HCTZ)
• Longer control of BP!!!
Chlorthalidone
• 7-8% will require therapy for hypokalemia
• Hypokalemia most likely in first 2 weeks, so if K is normal at 3 weeks, unlikely to have hypokalemia
Hypertension. 2011;57(4):689.

8/31/14
20
Chlorthalidone • No 12.5 mg tabs, 25 mg tabs must be split
• Sometimes hard to find
• NO fixed dose combos except 2
• 15 mg chlorthalidone (Thalitone®)
Chlorthalidone • Sensitivity reactions may occur in patients with a history of allergy or asthma
• Possibility of exacerbation of lupus (SLE) with thiazide diuretics—none reported with chlorthalidone
• Category B
Try Chlorthalidone!
DiureAc (mg) Average Systolic Drop HCTZ 25 mg -‐4.5 mm Hg (+ 2.1 mm Hg)
Chlorthalidone 12.5 mg
-‐15.7 mm Hg (+2.2 mm Hg)
Ernst ME, Carter BL, Goerdt CJ, Steffensmeier JJ, Phillips BB, Zimmerman MB, Bergus GR ComparaFve anFhypertensive effects of hydrochlorothiazide and chlorthalidone on ambulatory and office blood pressure. Hypertension. 2006;47(3):352.
Take Home Point

8/31/14
21
If you want to Control Blood Pressure long term:
Protect the Kidneys
Triple Whammy= risk of acute kidney injury
ACE or ARB plus diuretic plus NSAID or Aspirin
Triple Whammy • ACE/ARB: reduce glomerular filtration
pressure via vasodilation of the efferent arteriole
• NSAID/ASA: inhibits renal prostaglandin synthesis (inhibits dilation of renal arteries and decreases blood flow to the glomerulus)
• Diuretics decrease intravascular volume and reduce blood flow to the glomerulus
The combo leads to reduction in renal blood flow and renal dysfunction
8/31/14
22
Triple Whammy
• Especially deleterious in elderly patients, diabetics, renal insufficiency, ascites, or HF (“double whammy” can cause acute injury)
Protection from the Triple Whammy
• Keep well hydrated • NSAID use: 6-12 hour (not
24 hours) • Avoid NSAID, use
tramadol, acetaminophen instead, other modality
Hypertension Management

8/31/14
23
Chronopharmacology WHEN we take meds can make a difference in pharmacokineAcs and pharmacotherapeuAcs
BP management, and overall 24 hour BP control
Chronopharmacology Strategy for Aming of medicaAons: Deliver the drug in high concentraAons when it’s needed most!
Which Meds at Nighume? • Calcium channel blockers • ACEs • ARBs

8/31/14
24
24 Hour Blood Pressure
BP is about 15% lower during the evening and nighume vs dayAme
Nocturnal BP • BP is about 15% lower at nighume vs dayAme values (“Physiologic Dipping”)
• Non-‐Dippers= BP falls < 10% while sleeping
Nocturnal BP The problem occurswhen you “SKIP the DIP”… • Predictor of CV events • Greater incidence of LVH, HF, target organ damage
• Associated with microalbuminuria, faster progression of nephropathy
J Hypertens. 2010;28(10):2036.
8/31/14
25
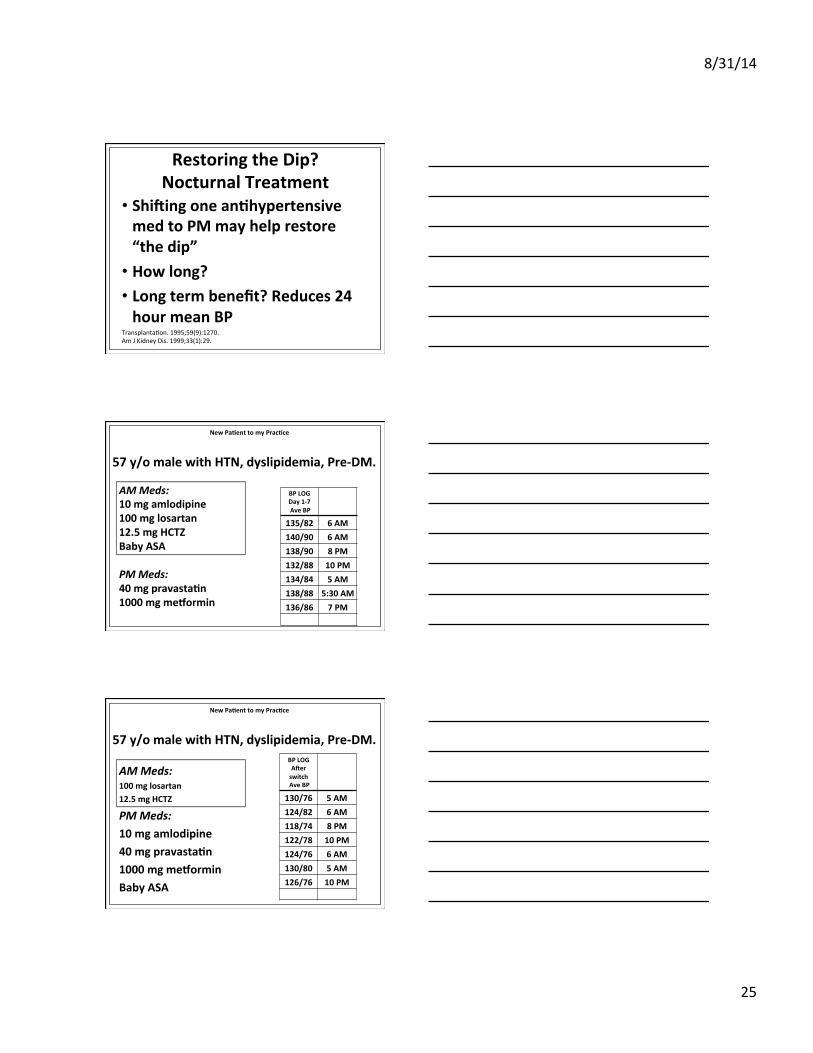
Restoring the Dip? Nocturnal Treatment
• Shiwing one anAhypertensive med to PM may help restore “the dip”
• How long? • Long term benefit? Reduces 24 hour mean BP
TransplantaFon. 1995;59(9):1270. Am J Kidney Dis. 1999;33(1):29.
57 y/o male with HTN, dyslipidemia, Pre-‐DM.
AM Meds: 10 mg amlodipine 100 mg losartan 12.5 mg HCTZ Baby ASA PM Meds: 40 mg pravastaAn 1000 mg mexormin
New PaAent to my PracAce
BP LOG Day 1-‐7 Ave BP
135/82 6 AM 140/90 6 AM 138/90 8 PM 132/88 10 PM 134/84 5 AM 138/88 5:30 AM 136/86 7 PM
57 y/o male with HTN, dyslipidemia, Pre-‐DM.
AM Meds: 100 mg losartan 12.5 mg HCTZ PM Meds: 10 mg amlodipine 40 mg pravastaAn 1000 mg mexormin Baby ASA
New PaAent to my PracAce
BP LOG Awer switch Ave BP
130/76 5 AM 124/82 6 AM 118/74 8 PM 122/78 10 PM 124/76 6 AM 130/80 5 AM 126/76 10 PM

8/31/14
26
Consider d/c’ing the HCTZ? AM Meds: 100 mg losartan 12.5 mg HCTZ PM Meds: 10 mg amlodipine 40 mg pravastaAn 1000 mg mexormin Baby ASA
New PaAent to my PracAce
BP LOG Awer switch Ave BP
130/76 5 AM 124/82 6 AM 118/74 8 PM 122/78 10 PM 124/76 6 AM 130/80 5 AM 126/76 10 PM
“Timing is Everything”
Take Home Point
43 y/o male with HTN, dyslipidemia, Pre-‐DM
AM Meds: 100 mg losartan 12.5 mg HCTZ PM Meds: 10 mg amlodipine 40 mg pravastaAn 1000 mg mexormin
“Mr. Boudreaux”

8/31/14
27
Awer 3 months of monitoring and meds, BP is
BeauAful! AM Meds: 100 mg losartan 12.5 mg HCTZ PM Meds: 10 mg amlodipine 40 mg pravastaAn 1000 mg mexormin
BP LOG Ave BP
130/76 5 AM 124/82 6 AM 118/74 8 PM 122/78 10 PM 124/76 6 AM 130/80 5 AM 126/76 10 PM
What about lower extremity edema?
• Occurs in up to 1 in 3 patients
• DHPs more likely than non-DHPs
• Dose dependent
• Occurs bilaterally
• NOT caused by fluid overload!!!!!
Why lower extremity Edema?
• Secondary to arteriolar dilation, then increased capillary pressure, and fluid shift

8/31/14
28
Summary and
Take Home
It Goes without Saying….
Make therapeuAc lifestyle changes
JNC 6, JNC 7, JNC 8
Take advantage of good medicaAon combinaAons
And avoid deleterious ones!

8/31/14
29
Timing is Everything!
Thank you!
To Reach me: Amelie Hollier, DNP, FNP-‐BC, FAANP
Advanced PracAce EducaAon Associates Lafayeoe, LA





























