Embed Size (px)
Citation preview
Assisted Admission/Return V2 1
Page 1 of 44
HSE Mental Health Services
Policy Title: Assisted Admission (Removal of the Person to the
Approved Centre Section 13 Mental Health Act 2001)
and Assisted Return (Return of a person to the
Approved Centre Section 27 Mental Health Act 2001).
Quality Framework: Theme’s 1, 2, 3, 4, 6, 7 & 8.
Document
reference number:
PPG-MHATG-
CLN-03
Document
developed by
HSE-Mental Health
Act Implementation
Group
Revision number:
-2-
Document approved by
National Mental Health Division
Management Team
Approval
date:
26th May 2014 Responsibility
for
implementation
Local Mental
Health Services
Revision
date
April 2017 Responsibility
for review and audit
Mental Health Act
Training Group
Assisted Admission/Return V2 2
Page 2 of 44
Table of Contents: Page
1.0 POLICY STATEMENT ..................................................................... 4
2.0 POLICY PURPOSE ......................................................................... 5
3.0 SCOPE OF THE POLICY ................................................................. 6
4.0 Legislation/Other Related Policies ................................................... 6
5.0 GLOSSARY OF TERMS AND DEFINITIONS ........................................ 7
6.0 RESPONSIBILITIES....................................................................... 9
6.1 Organisational: ............................................................................ 9
6.2 Management: .............................................................................. 9
6.3 Clinical Director: .......................................................................... 9
6.4 Staff ......................................................................................... 10
7.0 PROCEDURE .............................................................................. 10
8.0 ASSISTED ADMISSION TEAM ....................................................... 11
9.0 ROLE OF THE CLINICAL DIRECTOR OR CONSULTANT PSYCHIATRIST
ACTING ON HIS/HER BEHALF: ..................................................... 12
10.0 ROLE OF THE ASSISTED ADMISSION COORDINATOR: .................. 13
11.0 ROLE OF THE ASSISTED ADMISSION TEAM LEADER: .................... 14
13.0 ASSISTED ADMISSION INITIATION: ........................................... 16
14.0 WHERE A PERSON IS NO LONGER AT THE STATED LOCATION: ...... 18
18.0 ON ARRIVAL AT THE APPROVED CENTRE: ................................... 21
19.0 REVIEW PROCESS: ................................................................... 21
20.0 GARDA HSE LIAISON GROUP: ................................................... 22
21.0 REVISION AND AUDIT OF POLICY: ............................................. 22
22.0 IMPLEMENTATION OF POLICY: .................................................... 22
23.0 ABBREVIATIONS ....................................................................... 23
Assisted Admission/Return V2 3
Page 3 of 44
24.0 REFERENCES ............................................................................ 23
25.0 ELEARNING AND DOCUMENTATION ............................................. 23
26.0 APPENDIX 1: HEALTH (MISCELLANEOUS PROVISIONS) ACT 2009. . 24
27.0 APPENDIX 2: PRO-FORMA LETTER MOU SECTION 5.5 ................... 27
28.0 APPENDIX 3: EMERGENCY BOX CONTENTS. ................................ 28
29.0 Appendix: 4. Assisted Admission Recording Form (Sample). ........... 29
30.0 Appendix 5:Assisted Admissions Coordinators Check List (Sample). 30
31.0 Appendix: 6. Assisted Admission Team Leader’s Report Form. ........ 31
32.0 Appendix: 7. Assisted Admission Team Leader’s Report Guidelines. . 32
33.0 Appendix: 8. Assisted Admission Risk Screening Form. .................. 33
34.0 Appendix: 9. Assisted Admission Risk Screening Form (Continuation
Sheet). ......................................................................................... 34
35.0 Appendix: 10. Assisted Admission Risk Screening Form (Continuation
Sheet). ......................................................................................... 35
36.0 ASSISTED ADMISSION FLOW CHART: ......................................... 36
37.0 ASSISTED RETURN FLOW CHART: ............................................... 37
38.0 PRODUCTION AND CONSULTATION TRAIL .................................... 38
39.0 REVISION HISTORY: ................................................................ 38
40.0 QUALITY FRAMEWORK STANDARDS ADDRESSED IN THIS POLICY: . 40
41.0 SIGNATURE SHEET: (ALL STAFF TO SIGN THAT THEY HAVE READ AND
UNDERSTAND THIS POLICY) ....................................................... 42
Assisted Admission/Return V2 4
Page 4 of 44
1.0 Policy Statement:
1.1 The HSE is committed to providing a high quality mental health
service accessible to all citizens in line with the requirements of national policy and legislation.
1.2 THE HSE is committed to ensuring that the rights and interests of
service users and their families/carers are protected in the context of the delivery of care and treatment.
1.3 The right to liberty is a fundamental personal and human right under
the Irish Constitution and the European Convention on Human Rights
and Fundamental Freedoms. A person may only be deprived of the right to liberty strictly in accordance with the law.
1.4 Section 13 of the Mental Health Act 2001 (MHA) makes provisions for
the removal of a person to an approved centre. An application must be made to a registered medical practitioner and a recommendation
must then be made by the registered medical practitioner to have an individual involuntarily detained in an approved centre.
1.5 Where a recommendation is made the applicant concerned shall
arrange for the removal of the person to the approved centre. However if the applicant is unable to arrange for the removal of the
person concerned to the approved centre, the clinical director of the approved centre or the consultant acting on his/her behalf shall at
the request of the registered medical practitioner who made the
recommendation arrange for the removal of the person to the approved centre by members of staff of the approved centre or
authorised persons.
1.6 Where an assisted admission is requested it shall be commenced and completed without any undue delay.
1.7 The removal of a person to an approved centre must comply with the
MHA 2001, therefore the application and Recommendation to have a person involuntarily admitted to the approved centre must be strictly
in compliance with the MHA 2001.
1.8 Section 27 of the MHA 2001 makes provisions for the return of a person to an approved centre by staff of the approved centre or
authorised persons.
1.9 The removal of a person or the return of a patient to an approved
centre is a planned intervention informed by the therapeutic skills of mental health professionals.
Assisted Admission/Return V2 5
Page 5 of 44
1.10 A person’s right to information is vital in all aspects of mental health
care and they must, as far as is reasonably practicable, be provided with information in relation to the assisted admission in a manner
and form that they understand. They should also be allowed to make representations in relation to it and due consideration to those
representations must be made under the MHA 2001.
1.11 The transfer of a person to another approved centre or service is not an Assisted Admission.
2.0 Policy Purpose:
2.1 The purpose of this policy is to guide staff of the approved centre and authorised persons in the provision of Assisted Admissions related to
section 13 (removal of a person to an approved centre) and section 27 (Absent without Leave) of the MHA 2001. The policy also acts as a
guide to staff of the community mental health services who may have a peripheral role in the removal or return of a person/patient to
the approved centre.
2.2 This policy aims to ensure that the most appropriate, most sensitive, discreet, safest and least restrictive method of conveying the person
(whom a recommendation applies) to the approved centre is used, ensuring that risk is minimised to the person or to others.
2.3 Human and civil rights are a fundamental tenet of our society. Such
rights are enshrined in the Irish Constitution and in the European
Convention on Human Rights Act 2003. For mental health service users those rights are paramount and ensuring protection of these
rights is a significant responsibility of mental health services and a component of providing excellence in mental health practice. In
making a decision under the Mental Health Act 2001 concerning the care or treatment of a person, including a decision to make an
admission order or an assisted admission to an approved centre “the best interests of the person concerned shall be the principal
consideration with due regard being given to the interests of other persons who may be at risk of serious harm if the decision is not
made” (section 4(1), MHA 2001,). The removal of a person or return of a person to an approved centre is a planned intervention informed
by the therapeutic skills of mental health professionals where “due regard shall be given to the need to respect the right of the person to
dignity, bodily integrity, privacy and autonomy” (section 4(3), MHA
2001,).
Assisted Admission/Return V2 6
Page 6 of 44
3.0 Scope of the Policy:
3.1 This policy relates to all community staff, staff of the approved centre
and authorised persons, in particular staff who are members of the assisted admission team, or persons involved in the arranging and or
co-ordination of assisted admissions.
3.2 This policy should be read in conjunction with the documents in section 4.0.
3.3 This policy may be reviewed as a result of any changes to relevant
legislation or identification of areas for improvement as a result of
the learning accrued from practice, including any incidents or near misses in relation to the removal or return of a person/patient to the
approved centre.
4.0 Legislation/Other Related Policies
4.1 Mental Health Act 2001.
4.2 Statutory Instrument, No. 551 of 2006, Mental Health Act (2001) (Approved Centres) Regulations 2006.
4.3 Data Protection Acts 1988 & 2003.
4.4 Interpretation Act 2005.
4.5 Health (Miscellaneous Provisions) Act 2009
4.6 Freedom of Information Acts 1997 & 2003.
4.7 Code of Practice on Admission, Discharge and Transfer to and from Approved Centres (Mental Health Commission, 2009).
4.8 Code of Practice Guidance for persons working in Mental Health
Services with people with Intellectual Disabilities.
4.9 HSE Authorised Officer Policy PPG-MHATG-CLN-02: Authorised Officer (Consideration of an application for involuntary admission
following assessment by an Authorised Officer as defined within the Mental Health Act 2001).
4.10 HSE Policy on Power to Detain a Person/Patient (Adult & Child) (Formally Holding Powers Policy Adult and Child).
Assisted Admission/Return V2 7
Page 7 of 44
4.11 Memorandum of Understanding between An Garda Síochána and the
HSE on Removal to or Return of a person to an Approved Centre in accordance with Section 13 & Section 27, and the Removal of a
person to an Approved Centre in accordance with Section 12, of the Mental Health Act 2001.
4.12 Local policies/guidelines on records management, confidentiality and
consent.
5.0 Glossary of Terms and Definitions :
5.1 Admission order: An order (signed by a consultant psychiatrist
responsible for the care and treatment of the patient) for the reception, detention and treatment of the person the admission order
relates to MHA 2001, section 14(1)(a).
5.2 Applicant: means a person who under section 9 of the MHA 2001, may make an application to a registered medical practitioner to have
a person involuntarily admitted to an approved centre.
5.2 Application: means an application (to a registered medical practitioner by a person under section 9 of the MHA 2001) for a
recommendation that a person be involuntarily admitted to an approved centre.
5.3 Approved “Centre”: a hospital or other inpatient facility for the care
and treatment of persons suffering from mental illness or mental
disorder (section 62, MHA 2001).
5.4 Assisted Admission: Where a recommendation under section 10 of the MHA 2001 is made and the applicant concerned (other than an
application made under section 12 of the MHA 2001) is unable to arrange for the removal of the person to the approved centre the
clinical director of the approved centre specified in the recommendation or a consultant psychiatrist acting on his or her
behalf shall, at the request of the registered medical practitioner who made the recommendation, arrange for the removal of the person to
the approved centre by members of the staff of the approved centre or authorized persons or where a patient (including a child) is absent
without leave from the approved centre (Section 27, MHA 2001), the clinical director of the approved centre concerned may arrange for
members of the staff of the approved centre or authorised persons to
bring the patient back to the approved centre.
5.5 Assisted Admission Coordinator: A senior nurse manager of the approved centre who coordinates the assisted admission.
Assisted Admission/Return V2 8
Page 8 of 44
5.6 Authorised Officer: An officer of the Health Service Executive who is
of a prescribed rank or grade and who is authorised by the Health Service Executive to make an application under section 9 of the MHA
2001.
“For the purposes of section 9 of the Mental Health Act 2001, the rank and grade of “authorised officer” is hereby prescribed as Local
Health Manager, General Manager, Grade VIII, Psychiatric Nurse, Occupational Therapist, Psychologist or Social Worker”. (Mental
Health Act 2001 (Authorised Officer) Regulations). Subject to section 9(2) of the Mental Health Act 2001).
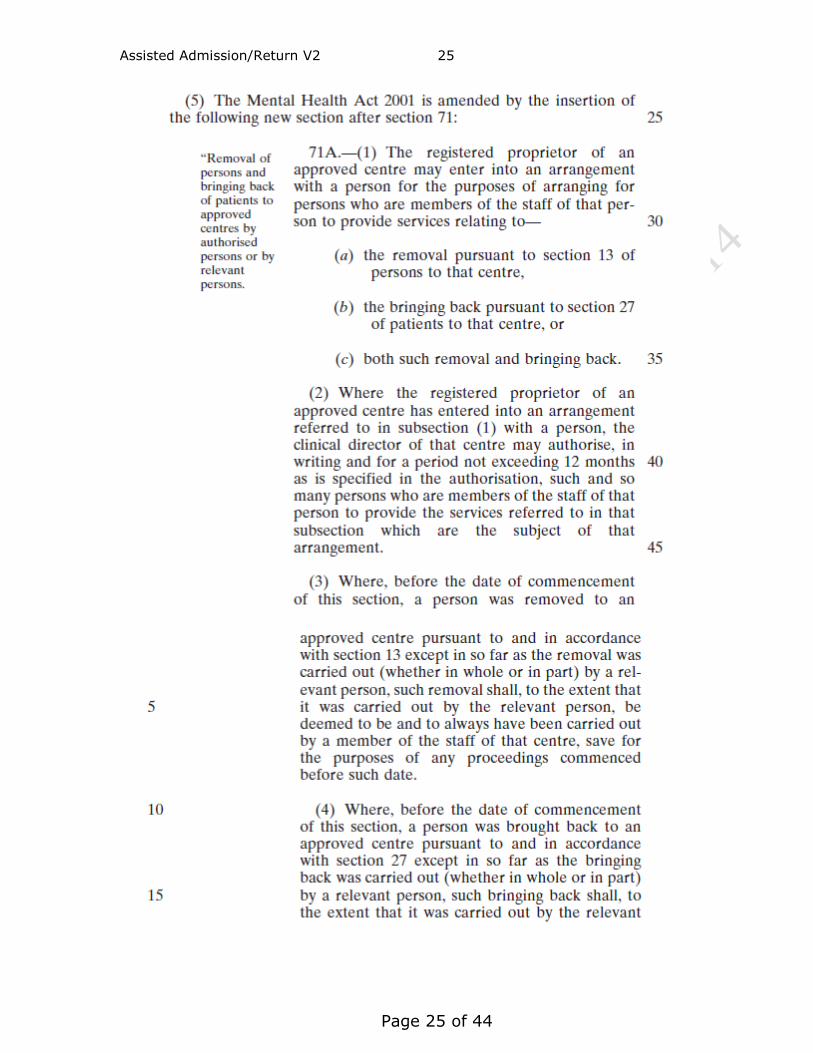
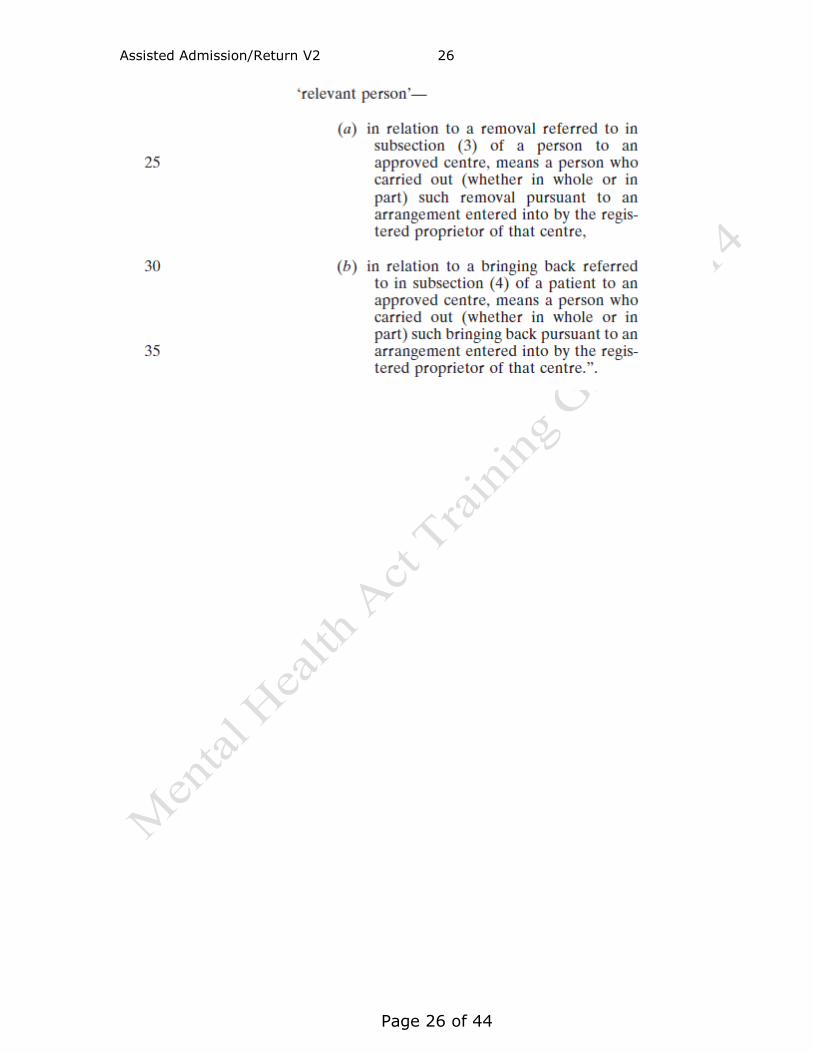
5.7 Authorised Person: in relation to the removal pursuant to section 13 (MHA 2001), or the bringing back pursuant to section 27 (MHA 2001)
of a patient to an approved centre, means a person who is for the time being authorised pursuant to section 63(5) of the Health
(Miscellaneous Provisions) Act 2009 to provide services relating to such removal (Appendix 1).
5.8 Clinical Director: A consultant psychiatrist appointed in writing by the
governing body of an approved centre/s, to be the clinical director of the approved centre/s named in the appointment letter or a
consultant psychiatrist acting on his/her behalf.
5.9 Patient: A person to whom an admission order or renewal order pursuant to the Mental Health Act 2001 relates.
5.10 Registered Proprietor: means the person whose name is entered in the register of approved centres as the person carrying on the centre
(section 62, MHA 2001).
5.11 Relevant Individual: in this policy means a family member, relative, carer, neighbour, advocate or authorised officer.
5.12 Renewal Order: An order extending the period of detention of the
person (section 15(2) and 15(3), MHA 2001).
5.13 Staff of the approved centre: Means suitably qualified persons (nursing, medical, allied health professionals and care staff) who are
or can be deployed to work in the approved centre.
5.14 The Person: means the individual to whom an application and
recommendation relates.
Assisted Admission/Return V2 9
Page 9 of 44
6.0 Responsibilities:
6.1 Organisational:
6.1.1 The HSE is responsible for the provision of adequate resources to
effect assisted admissions for the approved centre concerned.
6.1.2 The HSE is responsible for the provision of training to mental health service personnel involved in assisted admissions.
6.2 Management:
6.2.1 It is the responsibility of the mental health services senior management team to monitor the implementation of this policy.
6.2.2 It is the responsibility of the mental health services senior
management team to ensure this policy is reviewed within the allocated time frame and or as a result/outcome of incidents
accidents/complaints or changes to legislation or policy.
6.2.3 It is the responsibility of the appropriate service line manager to ensure that local members of the Assisted Admission team are
adequately prepared for the role in terms of competence and training.
6.2.4 It is the responsibility of the mental health services senior
management team to ensure that advocacy services are in place to
assist the patient in requesting and where necessary participating in a review of their assisted admission. This process should include
where necessary access to a responsive, fair and formal complaints procedure.
6.3 Clinical Director:
6.3.1 It is the responsibility of the Clinical Director to authorise an Assisted
Admission following a request from the Registered Medical Practitioner (which includes an assessment of risk).
6.3.2 It is the responsibility of the Clinical Director of the approved centre
to request the assistance of the Gardaí where necessary.
6.3.3 It is the responsibility of the Clinical Director of the approved centre
to ensure that “Authorised Persons” are authorised in writing for a period not exceeding 12 months (Appendix 1).
Assisted Admission/Return V2 10
Page 10 of 44
6.4 Staff:
6.4.1 It is the responsibility of all staff to be aware of and adhere to this
policy.
6.4.2 All staff will be required to sign that they have read and understand this policy.
6.4.3 It is the responsibility of all staff to ensure that they are familiar with
the Mental Health Act 2001 and other relevant legislation governing the delivery of mental health services.
7.0 Procedure:
7.1 Under the section 13(1), MHA 2001 the applicant should arrange the removal of the person the subject of the recommendation to the
approved centre specified in the recommendation.
7.2 If the applicant is unable to make such arrangements, the registered medical practitioner who made the recommendation must request
the clinical director of the approved centre or consultant psychiatrist acting on his/her behalf specified in the recommendation to arrange
for members of staff of the approved centre or authorised persons to remove the person to that centre (section 13(2), MHA 2001).
7.3 Before the initiation of the assisted admission, the assistance of the
Gardaí may be requested by the clinical director of the approved
centre or consultant psychiatrist acting on his/her behalf, if the clinical director of the approved centre or consultant psychiatrist
acting on his/her behalf and the registered medical practitioner are of the opinion that there is a serious likelihood of the person
concerned causing immediate and serious harm to himself or herself or others (section 13(3), MHA 2001) (see also 10.6 &.10.7).
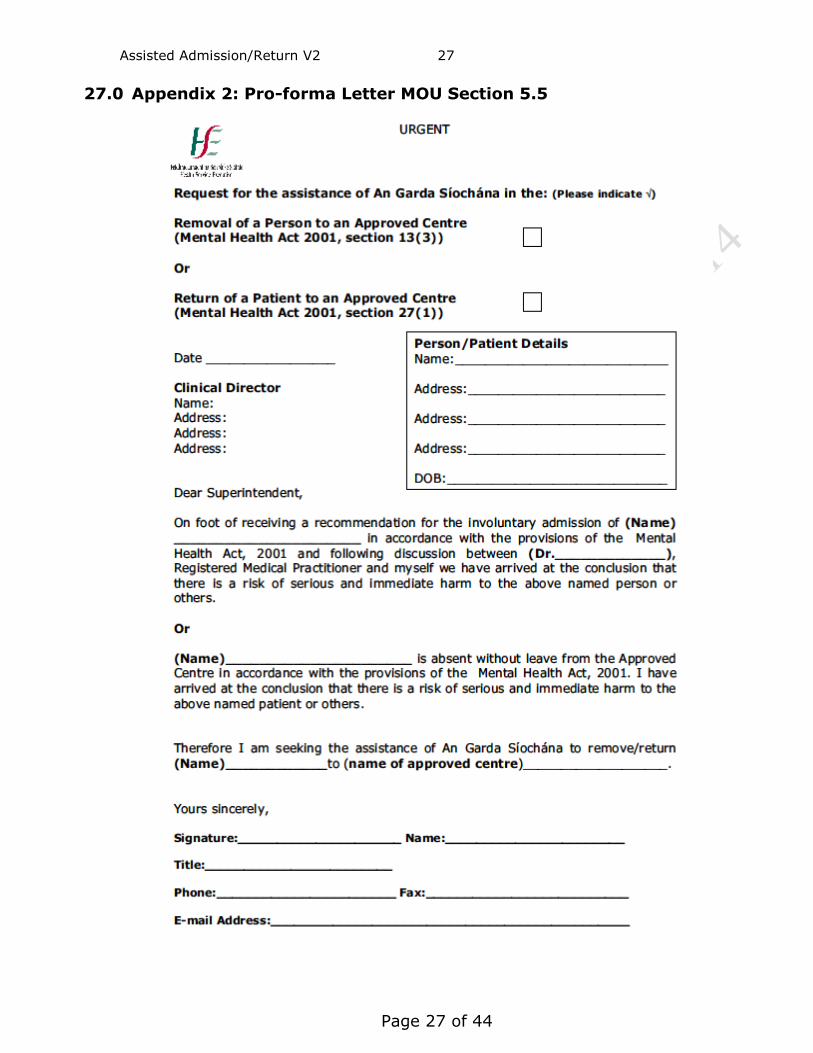
7.4 A verbal request for assistance of the Gardaí must be followed up in
writing as soon as practicable (Appendix 2).
7.5 Members of the Gardaí are empowered to “enter, by force if necessary, any premises where they have reasonable cause to
believe the person concerned may be and may take all reasonable measures necessary for the removal of the person to the approved
centre including the detention or restraint of the person concerned”
(section 13(4), MHA 2001).
7.6 During the assisted admission process all reasonable efforts should be made to protect the privacy and dignity of the person concerned.
Assisted Admission/Return V2 11
Page 11 of 44
7.7 The assisted admission team will make every effort to gain the
cooperation of the person during the assisted admission process.
7.8 The assisted admission team will ensure that adequate information is provided to the person on the procedure for assisted admission, the
review of the assisted admission, the complaints procedure and their right to make a complaint.
7.9 An assisted admissions log should be maintained in each approved
centre to collect information relating to assisted admissions by the assisted admission coordinator.
8.0 Assisted Admission Team:
8.1 The assisted admission team will consist of a minimum of a team leader (who will be a registered psychiatric nurse) and two other
staff, at least one of whom will be a registered psychiatric nurse.
8.2 At least one of the team members will be of the same gender as the person the subject of the assisted admission.
8.3 The team members will have read and be familiar with the policy on
assisted admissions and the Mental Health Act 2001.
8.4 An education/training programme specific to assisted admissions has been developed and is available to staff undertaking the role of
assisted admission team leader, team member or team co-ordinator.
(There is also an eLearning programme available to update knowledge on HseLand).
8.5 The assisted admission’s coordinator will nominate the team leader
who will be given a mobile phone for the period of the assisted admission.
8.6 Where an assisted admission is proposed, the community mental
health services, including the community mental health nurse/community key worker, should be involved at the earliest
stage of the process, where possible.
8.7 Other members of the mental health service may be required to assist at the location of the person.
8.8 On deployment the assisted admission team leader will ensure that the assisted admission team are in possession of emergency
equipment which may be required during the assisted admission (Appendix 3).
Assisted Admission/Return V2 12
Page 12 of 44
9.0 Role of the Clinical Director or Consultant Psychiatrist acting on
His/Her Behalf:
9.1 The registered medical practitioner shall arrange for the application and recommendation forms to be sent to the clinical director (or
consultant psychiatrist acting on his/her behalf) of the approved centre concerned (section 10(4), MHA 2001). (A referral letter,
requesting an assisted admission to the approved centre and detailing the patient’s relevant clinical details, should also be sent to
the approved centre by the registered medical practitioner).
9.2 The registered medical practitioner should ensure that the referral
letter, application and recommendation forms are delivered to the approved centre. Where circumstances require, a faxed copy may
suffice at this initial stage, if the registered medical practitioner has given assurances that the original forms are available for collection
by the assisted admission team prior to the removal of the individual to the approved centre.
9.3 The application and recommendation forms will be reviewed to
ensure they are correctly and fully completed (see 13.2).
9.4 Where the application and recommendation forms are faxed to the approved centre by the registered medical practitioner, the original
forms must be present at the site where the assisted admission is taking place. The original forms are checked by the assisted
admission team leader on site to ensure that the assisted admission
is effected in compliance with the MHA 2001.
9.5 Where the clinical director or consultant psychiatrist acting on his/her behalf and the registered medical practitioner consider there is a
serious likelihood of the person concerned causing immediate and serious harm to himself or herself or to others, the clinical director or
consultant psychiatrist acting on his/her behalf, may request the Gardaí to assist the staff of the approved centre or authorised
persons in the removal of the person to the approved centre (section 13(3), MHA 2001).
9.6 Gardaí will assist the assisted admission team in the removal or
return of a person/patient in accordance with section 13(3) and 27(2), MHA 2001 and the Memorandum of understanding between
An Garda Síochána and the HSE on the Removal to or Return of a
person to an Approved Centre in accordance with Section 13 & Section 27, and the Removal of a person to an Approved Centre in
accordance with Section 12, of the Mental Health Act 2001.
Assisted Admission/Return V2 13
Page 13 of 44
9.7 The clinical director or consultant psychiatrist acting on his/her behalf
will discuss the case with appropriate staff to arrange the assisted admission of the person concerned.
9.8 The clinical director or consultant psychiatrist acting on his/her behalf
or non consultant hospital doctor (under the supervision of a consultant psychiatrist acting on his/her behalf) will complete and
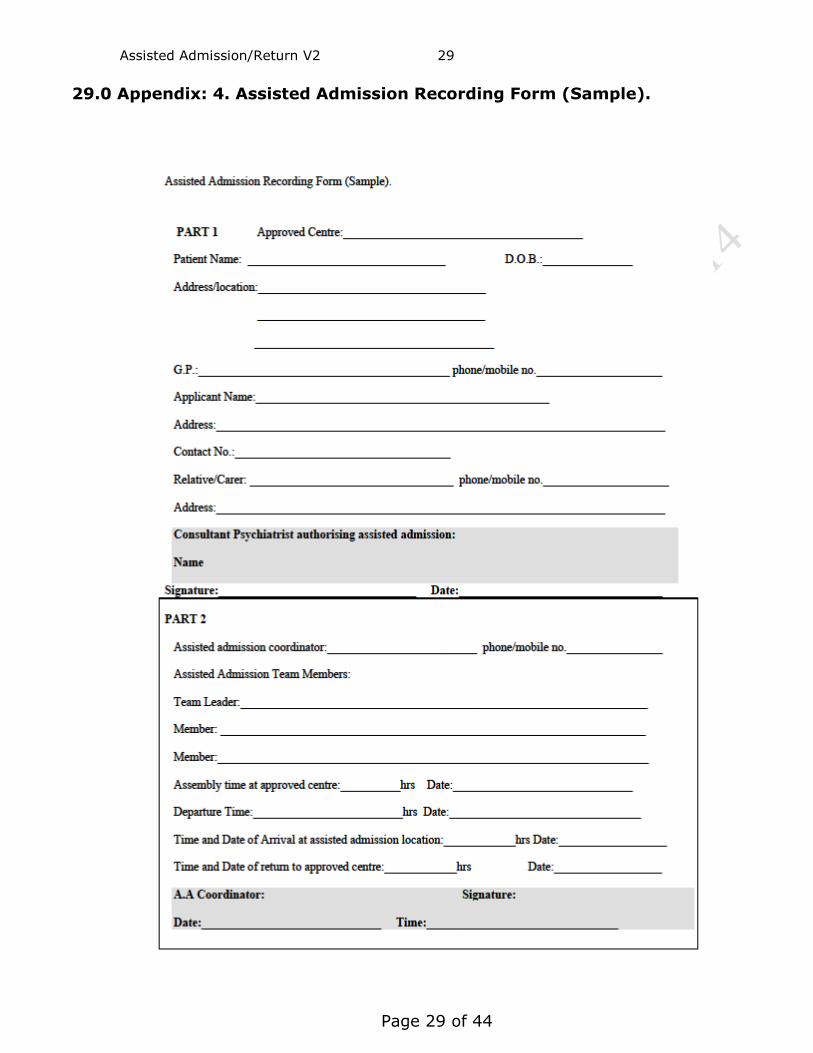
sign part 1 (authorising the assisted admission) of the assisted admission recording form (Appendix 4).
10.0 Role of the Assisted Admission Coordinator:
10.1 The assisted admission coordinator will coordinate the formation of the assisted admission team and the nomination of the team leader.
10.2 The mode of transport is determined by the person’s clinical condition
and following discussion between the assisted admission coordinator, the clinical director or consultant psychiatrist acting on his/her behalf
and ambulance control (see 17.0).
10.3 The assisted admission coordinator will liaise with the assisted admission team leader in relation to transport of the patient and
ensuring that the process of assisted admission is safely managed.
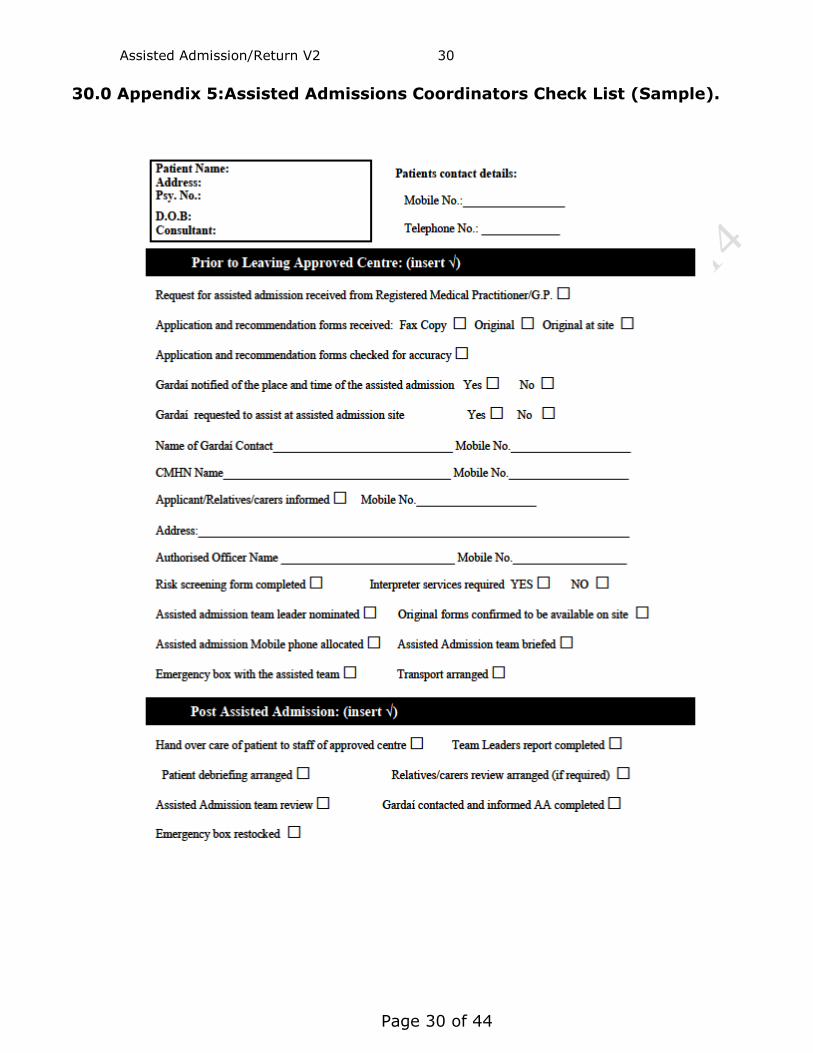
10.4 The assisted admission coordinator will complete the assisted admission check list prior to the assisted admission team deployment
(Appendix 5).
10.5 The assisted admission coordinator will communicate with the team
leader and/or others as appropriate in relation to any difficulties that may arise during the process of assisted admission.
10.6 The assisted admission coordinator will liaise with the Gardaí in the
area of the assisted admission to inform them of the date, time and location of an assisted admission and to inform them that they may
be requested to assist the assisted admission team.
10.7 The assisted admission coordinator will pass on a contact name and number of the Gardaí to the assisted admission team leader.
10.8 The assisted admission coordinator will liaise with the applicant or
Authorised Officer (if they are the applicant) and the registered
medical practitioner who made the recommendation and inform them of the date and time of the assisted admission. The assisted
admission coordinator will also inform them that their assistance may be required at the assisted admission site especially if the registered
Assisted Admission/Return V2 14
Page 14 of 44
medical practitioner has not informed the person that an
application and recommendation has been completed for their involuntary admission to the approved centre.
10.9 If necessary, the assisted admission coordinator will liaise with the
applicant, next of kin or relevant other to check that appropriate steps are taken for the care of children/dependants, the security of
the person’s accommodation, and/or care of animals while the person is admitted to the approved centre.
10.10 Where an assisted admission is conducted by the external provider or
the local assisted admission team, the assisted admission coordinator
will review the assisted admission with the assisted admission team on completion of the assisted admission.
10.11 The assisted admission coordinator will arrange a review session for
the person concerned (and the family) if requested as soon as practicable.
10.12 The assisted admission coordinator will complete and sign part 2 of
the assisted admission recording form (Appendix 4).
11.0 Role of the Assisted Admission Team Leader:
11.1 It is the responsibility of the assisted admission team leader to ensure that the application and recommendation form or a copy of
same are in their possession before the assisted admission team
depart from the approved centre or meeting point.
11.2 The team leader will ensure that documentation pertaining to the assisted admission is in order and available to show Gardaí and other
relevant people during the assisted admission.
11.3 The team leader is responsible for the identification of the person and must satisfy themselves that they can correctly identify the person
whom the application and recommendation applies to. The team leader may request the assistance of the applicant, family, registered
medical practitioner, authorised officer, community mental health nurse, key worker or any other appropriate person for this purpose.
11.4 The team leader is responsible for ensuring that they have received
all available relevant information regarding the assisted admission.
11.5 The team leader is responsible for ensuring that an on site risk
assessment is conducted.
Assisted Admission/Return V2 15
Page 15 of 44
11.6 The team leader will have regard for the safety and welfare of all
involved and will contact the Gardaí for their assistance in situations of immediate and serious risk of harm to himself or herself or
to other persons.
11.7 The team leader will take a lead in decision making to ensure a safe removal/return, such as obtaining information and communicating
with the approved centre and or assisted admission coordinator.
11.8 The team leader will ensure that the assisted admission team are acquainted with the risk screening carried out on the person for
admission and all other relevant clinical information, including
information provided by the Authorised Officer where they are the applicant.
11.9 The team leader will ensure that the assisted admission team
familiarise themselves with the layout of the location of the person (in as much as is reasonably possible) and liaise with relevant
persons such as family members/carers and health professionals who may introduce the team to the person for admission.
11.10 The team leader will maintain contact with relevant individuals to
obtain directions to the location of the person and update them on the arrangements prior to the assisted admission. The team leader
will also inform them when the person has been admitted to the approved centre and will arrange a review session with the family
and the community Mental Health Nurse /key worker following the
assisted admission (if requested).
11.11 The team leader will determine from the assisted admissions coordinator whether checks have been made (where required) that
the relevant steps have been taken for the care of children/dependants, the security of the person’s accommodation,
and care of animals while the person is admitted to the approved centre (see 10.9).
11.12 The team leader will make every effort to elicit the person’s
cooperation with the assisted admission.
11.13 If the person is uncooperative the team leader will decide the approach required to effect the assisted admission and communicate
this to the assisted team members.
11.14 The team leader is responsible for completing a report following the
assisted admission (Appendix 6) a copy of which should be retained in the patient’s clinical file.
Assisted Admission/Return V2 16
Page 16 of 44
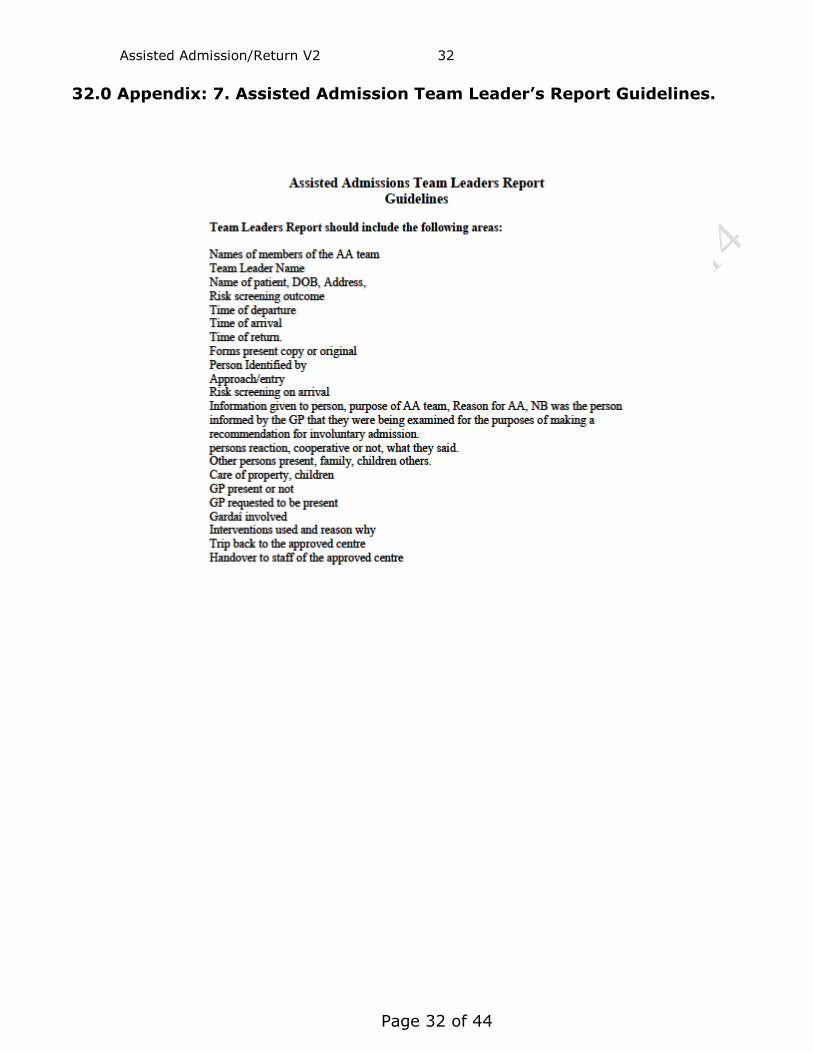
NOTE: The content of the report should be based on the guidelines
in Appendix 7.
12.0 Steps in Risk Assessment:
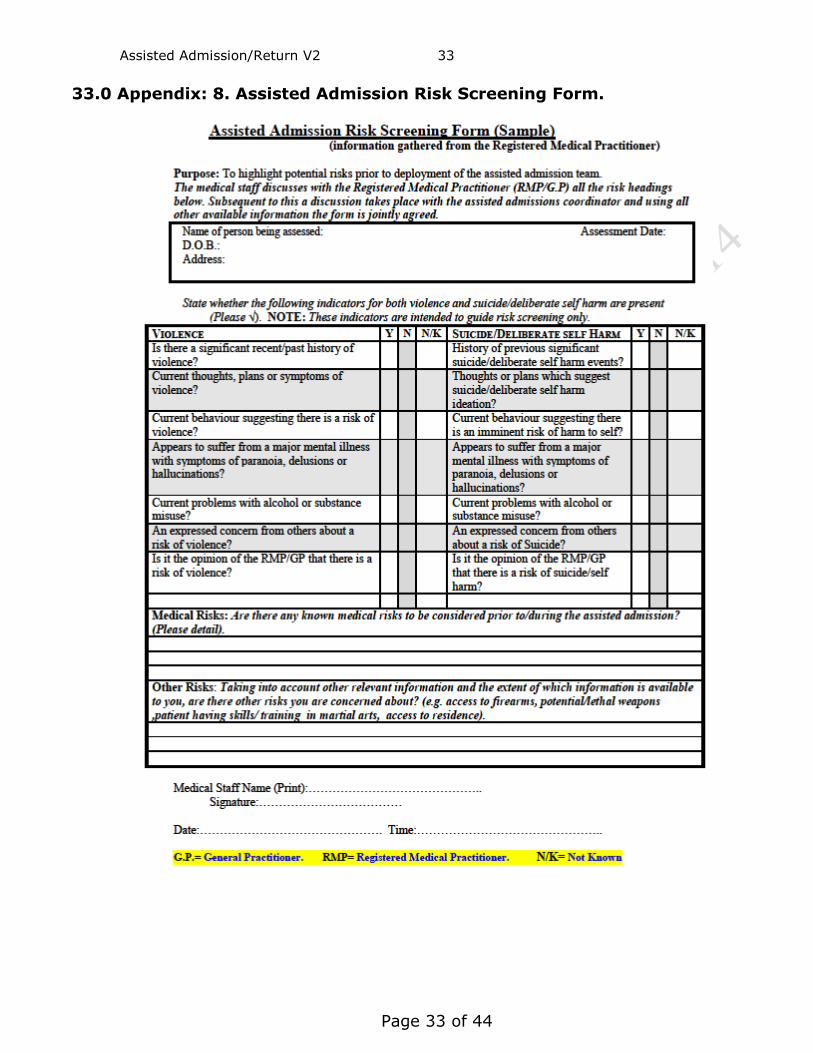
12.1 Step 1: Registered Medical Practitioner making the recommendation performs and documents a risk screening/risk assessment.
12.2 Step 2: Information on the risk screening is taken by the medical
staff of the mental health services (Appendix 8 & 9).
12.3 Step 3: Where the person is known to the mental health services
information on risk is collated and evaluated (e.g. from patient notes).
12.4 Step 4: The assisted admission coordinator will liaise with medical
staff to ensure the collation of all currently available information relating to the assisted admission.
12.5 Step 5: The information is communicated to the assisted admission
team prior to deployment.
12.6 Step 6: The assisted admission team will conduct an appropriate risk assessment at the site of the assisted admission (Appendix 10).
12.7 Where there is a serious likelihood of the person concerned causing
immediate and serious harm to himself or herself or to others, the
Gardaí should be contacted by the clinical director or consultant psychiatrist acting on his/her behalf, to assist the staff of the
approved centre in the removal of the person to the approved centre (section 13(3), MHA 2001).
12.8 Relevant information relating to risk screening/assessment should be
shared with the Gardaí.
13.0 Assisted Admission Initiation:
13.1 Following the receipt of the referral letter, application and recommendation forms from the registered medical practitioner the
clinical director or consultant psychiatrist acting on his/her behalf will request the assisted admission coordinator to arrange and coordinate
assisted admission team.
13.2 Where the clinical director or consultant psychiatrist acting on his/her
behalf is off site the forms will be examined by a non consultant hospital doctor and assisted admission team coordinator and they will
Assisted Admission/Return V2 17
Page 17 of 44
contact the clinical director or consultant psychiatrist acting on
his/her behalf, in relation to the accuracy of the relevant forms and the organisation of an assisted admission.
13.3 Prior to the initiation of the assisted admission the need for the
assistance of the Gardaí should be considered.
13.4 In order to initiate an assisted admission the approved centre must be in possession of the correctly completed application and
recommendation forms or a copy of these.
13.5 Where a copy of the application and recommendation forms are
used, the original forms must be available to the assisted admission team or be present at the site where the assisted admission is taking
place. The original forms are checked by the assisted admission team leader to ensure that the assisted admission is effected in compliance
with the MHA 2001.
13.6 The team leader contacts the relevant individual and Gardaí to inform them of the estimated time of arrival of the assisted admission team.
(The agreement between the Health Service Executive and the Gardaí is such that the mental health service will inform the Gardaí of
the time and location of the assisted admission and that the Gardaí may be requested to assist the assisted admission team).
13.7 On arrival the assisted admission team will be as discreet as possible
and gain entry to the person’s residence with the consent of the
person or relevant individual.
13.8 On gaining entry to the person’s location the team leader assesses the environment for the purposes of ensuring the safety of all
persons concerned.
13.9 The assisted admission team leader will inform the person of their role in an understanding and supportive manner. They should use
their professional judgement, knowledge and skills to assess the situation, allay fear and gain the cooperation of the person to come
to the approved centre for assessment and/or treatment.
13.10 Where the assisted admission team are unable to gain entry to the person’s location, or encounter physical resistance on the part of the
person, or sense a risk of immediate and serious harm they should
initially withdraw from the location, reassess the situation and contact the Gardaí for their assistance. However in an emergency
situation the duty of care to the patient and others is paramount and
Assisted Admission/Return V2 18
Page 18 of 44
actions under common law may be required based on the doctrine of
necessity.
13.11 The Gardaí are empowered to use any reasonable measures, if necessary, to forcibly enter the premises and to detain and or
restrain a person concerned (section 13(4)(a) & (b), MHA 2001).
13.12 Both the team and the Gardaí will use the least restrictive measures to proceed with the Assisted Admission while maintaining the safety
and dignity of all concerned.
13.13 The team/Gardaí should ensure the person is not in possession of
dangerous items/weapons before transportation to the approved centre.
13.14 Where possible the team should ensure that the person’s medications
(for physical and mental health conditions) accompany the patient to the approved centre.
13.15 If necessary, the team leader will liaise with the assisted admission
coordinator to check that the applicant has taken appropriate steps for the care of children/dependants, the security of the person’s
accommodation, and care of animals while the person is admitted to the approved centre.
14.0 Where a person is no longer at the stated location:
14.1 If the person cannot be located the assisted admission team leader
checks with the applicant and or the registered medical practitioner to see if they are aware of the person’s location.
14.2 Where a person is no longer at the stated location on arrival of the
assisted admission team, all reasonable efforts should be made to locate the person.
14.3 The team leader will contact the assisted admission coordinator to
inform them of the situation and obtain further instruction.
14.4 The assisted admission coordinator will inform the clinical director or consultant psychiatrist acting on his/her behalf, the applicant, the
Gardaí and the registered medical practitioner that the assisted admission team were unable to locate the person concerned and the
team returns to the approved centre unless otherwise directed.
Assisted Admission/Return V2 19
Page 19 of 44
15.0 Return of a person who has been granted leave to the Approved
Centre: 15.1 A patient who is the subject of an admission order or renewal order
or in the case of a child an order under section 25 is in force, may be granted permission in writing to be absent with leave from the
approved centre by a consultant psychiatrist responsible for the care and treatment of the patient. The consultant psychiatrist may specify
and attach conditions to the leave (see section 26(1) MHA 2001).
NOTE: The patient should be notified that they may be directed in writing to return to the approved centre before the period of
leave has expired. Issues relating to language and
communication difficulties should be addressed prior to patients being granted leave so as they understand the
conditions that may be attached to leave and any subsequent correspondence relating to the withdrawal of permission for
leave.
15.2 The period of leave must be less than the unexpired period provided for in the relevant admission order, renewal order or section 25 order
(children).
15.3 Where a patient has been granted leave under section 26(1) of the MHA 2001 and the consultant psychiatrist responsible for the care
and treatment of the patient is of the opinion that it is in the best interest of the patient to return to the approved centre before a
period of leave has expired (section 26(2), MHA 2001), the
consultant psychiatrist may withdraw permission for leave and direct the patient in writing to return to the approved centre.
15.4 Arrangements should be made by the community mental health
nurse/key worker or other members of the mental health service team to ensure the letter is delivered to the patient.
15.5 If a patient fails to return to the approved centre as directed, then
they are considered absent without leave and the clinical director of the approved centre or the consultant acting on his/her behalf may
arrange the patient’s return by the staff of the approved centre or authorised persons (section 27(b)& (c), MHA 2001).
16.0 Return of a person (who is absent without permission) to the
Approved Centre:
16.1 A patient (including a child) will be considered to be absent without
permission if he or she:-
Assisted Admission/Return V2 20
Page 20 of 44
a) leaves the approved centre without permission (section
27(a), MHA 2001),
b) was absent from the approved centre with permission and fails to return within the specified time permitted,
c) was absent from the approved centre with permission and
fails to return to the centre in compliance with a written direction from the consultant psychiatrist (responsible for the
care and treatment of the patient) that he or she should so return,
d) fails, in the opinion of the consultant psychiatrist (responsible for the care and treatment of the patient), to comply with any
condition specified in writing to the patient when he or she was granted leave to be absent. (Section 27, MHA 2001)
16.2 The clinical director of the approved centre concerned may arrange
for the return of the patient to the approved centre by staff of the approved centre or authorised persons (section 27(1), MHA 2001).
16.3 If the assisted admission team are unable to return the patient to the
approved centre or if the clinical director of the approved centre or the consultant acting on his/her behalf is of the opinion that there is
a serious likelihood of the person concerned causing immediate and serious harm to himself or herself or others, the clinical director or
the consultant acting on his/her behalf may request via the assisted
admission team coordinator the assistance of the Gardaí in the return of the patient to the approved centre.
17.0 Transport
17.1 Appropriate patient transport provision will be made in accordance
with established local HSE patient transport arrangements.
17.2 Vehicles utilised for the provision of assisted admissions will meet minimum requirements specified for the safe transport of the
individual, the assisted admissions team (minimum 3 persons) and driver with additional capacity to transport other person(s) if required
in accordance with risk assessment for the particular assisted admission (e.g. registered medical practitioner, Gardaí).
17.3 Where the subject of the assisted admission has a known and potentially serious medical condition a standard medical ambulance
will be used.
Assisted Admission/Return V2 21
Page 21 of 44
18.0 On Arrival at the Approved Centre:
18.1 The assisted admission team will transfer the care of the person over
to the staff in the approved centre and ensure that all relevant information is passed on in writing.
18.2 Where the patient has been brought to the approved centre for an
assessment under section 13 of the MHA 2001, staff in the approved centre should establish if the patient is willing to stay voluntarily until
the commencement of the examination by the consultant psychiatrist.
18.3 If the patient is unwilling to stay voluntarily then section 14(2) of the MHA 2001 should be used to detain the patient until the
commencement of the examination by the consultant psychiatrist.
18.4 The team leader will complete a report on the assisted admission, giving details of the assisted admission and any relevant information
relating to it (Appendix 6 & 7).
18.5 A review session will be organised by the assisted admission coordinator, for the assisted admission team and if requested, the
family and the person concerned.
18.6 The person will be informed that an independent advocate will be available to meet with them to provide information on their rights
and assist the patient in requesting and where necessary
participating in a review of their assisted admission with the assisted admission coordinator.
18.7 A copy of the complaints procedure will be provided to the person
and their carers if requested. The contact details of the local advocate may also be given to the person and their carers.
18.8 The team leader will ensure that the emergency box is fully
restocked for the next assisted admission.
19.0 Review Process:
19.1 The review of an assisted admission should focus on identifying: a) What went well?
b) What did not go well? c) The service user’s perception of the process.
d) The family/carer’s perception of the process.
e) What can be learned from and/or improved for the next Assisted Admission/Return.
Assisted Admission/Return V2 22
Page 22 of 44
f) Communicating any changes or issues to other Assisted
Admission Teams?
19.2 Any issues or concerns raised by the patient or family should be addressed using the complaints process. These should also be
brought to the appropriate management team meetings and if necessary then forwarded to the local governance group meetings for
investigation/action and/or recommendations.
19.3 Where issues or concerns relating to the cooperation between the assisted admission team and the Gardaí are raised, these should be
brought to the local Garda/HSE Liaison Group meeting.
20.0 Garda HSE Liaison Group:
20.1 Each mental Health service should have a Liaison group convened to
maximise interagency cooperation in relation to the Removal and Return of a patient/person under the 2001 Act and the operation of
section 12 of the MHA 2001.
20.2 Terms of reference for liaison groups are prescribed in the Memorandum of understanding between An Garda Síochána and the
HSE on the Removal to or Return of a person to an Approved Centre in accordance with Section 13 & Section 27, and the Removal of a
person to an Approved Centre in accordance with Section 12, of the Mental Health Act 2001.
20.3 Issues or concerns from these liaison groups may be escalated to the
national liaison group.
21.0 Revision and Audit of Policy:
21.1 This policy will be revised every 3 years from the date of implementation or sooner as a result of changes in practice, policy or
legislation.
21.2 The Mental Health Act Training Group may select a local service to audit compliance with the policy and give feedback to that service on
the results.
22.0 Implementation of policy:
22.1 Following consultation with relevant stakeholders this policy will be posted to the Mental Health Services Hub and circulated via email to
approved centres.
Assisted Admission/Return V2 23
Page 23 of 44
22.2 Staff should sign that they have read and understood the policy on the
attached signature forms.
23.0 Abbreviations:
23.1 MHA = Mental Health Act 2001. 23.2 HSE = Health Service Executive.
24.0 References:
24.1 Department of Health and Children (2006) Statutory Instrument, No. 551
of 2006, Mental Health Act (2001) (Approved Centres) Regulations. Dublin. Stationary Office.
24.2 Government of Ireland (2005) Interpretation Act 2005. Dublin. Stationary
Office.
24.3 Government of Ireland (2006) Mental Health Act 2001. Dublin. Stationary Office.
24.4 Government of Ireland (2009) Health (Miscellaneous Provisions) Act 2009.
Dublin. Stationary Office.
24.5 Health Service Executive (2010) Memorandum of Understanding between
An Garda Síochána and the HSE on Removal to or Return of a person to an Approved Centre in accordance with Section 13 & Section 27, and the Removal of a person to an Approved Centre in accordance with Section 12,
of the Mental Health Act 2001. Available on line @ http://www.hse.ie/eng/services/Publications/services/Mentalhea
lth/Memo_of_Understanding_between_HSE_and_Garda_.pdf Accessed 12-12-2013.
24.6 Health Service Executive (2014) Power to detain a person/patient under
section 14(2) & 23(1) of the MHA 2001. Available on the MHS Hub.
24.7 Mental Health Commission (2006) Reference Guide to Mental Health Act
2001. Mental Health Commission (2006) Reference Guide to Mental Health
Act 2001. Mental Health Commission.
25.0 elearning and Documentation:
Assisted Admission e-learning module, policy and documents available
(for staff registered on HSELand) on the Mental Health Services HUB @ http://www.hseland.ie/mhsn/en-us/home.aspx
Assisted Admission/Return V2 24
Page 24 of 44
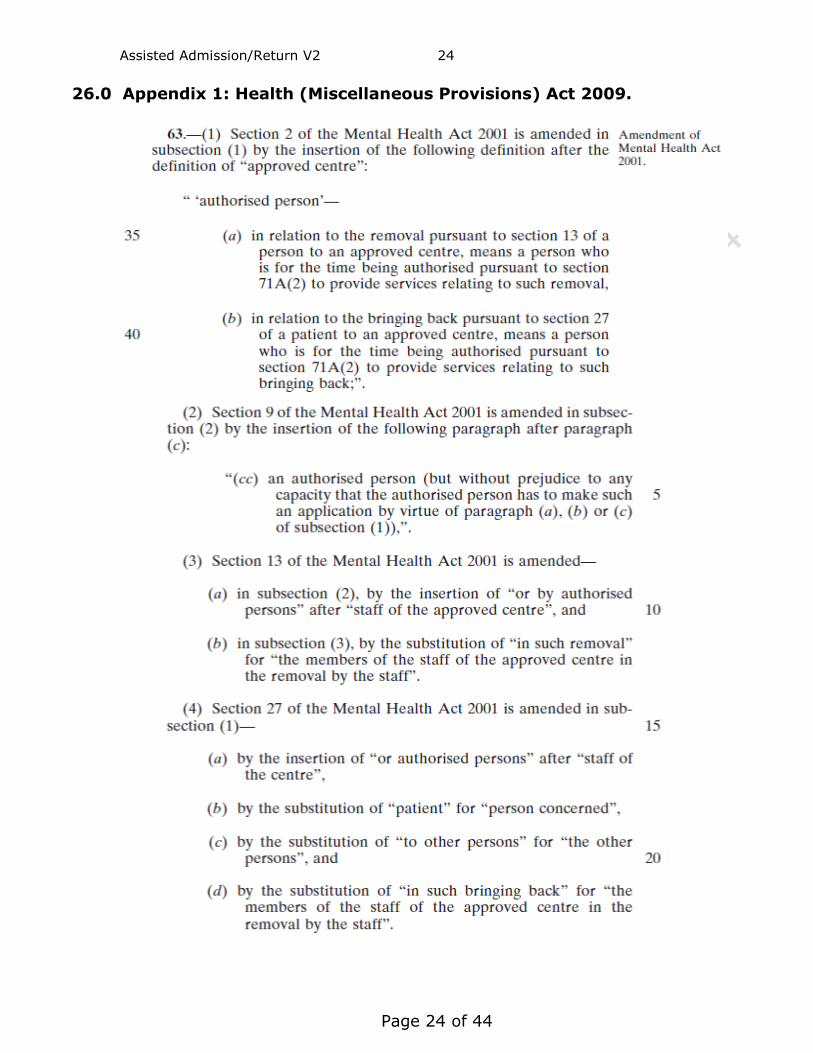
26.0 Appendix 1: Health (Miscellaneous Provisions) Act 2009.
Assisted Admission/Return V2 25
Page 25 of 44
Assisted Admission/Return V2 26
Page 26 of 44
Assisted Admission/Return V2 27
Page 27 of 44
27.0 Appendix 2: Pro-forma Letter MOU Section 5.5

Assisted Admission/Return V2 28
Page 28 of 44
28.0 Appendix 3: Emergency Box Contents.
Disposable gloves Hoffman Knife Selection of plasters Selection of wound pads Bandages Swabs Antiseptic wipes Antiseptic wound cleaning agent Selection Steri-strips Burn creams/sprays Bag valve mask e.g. Ambu bag Laerdal Mask Assorted sizes of Guedal Airways Flash Lights x 3 Spare Batteries (to fit flashlights) Stab proof vests Stab proof gloves
Please Note: This is not a definitive list and may be added to.
Assisted Admission/Return V2 29
Page 29 of 44
29.0 Appendix: 4. Assisted Admission Recording Form (Sample).
Assisted Admission/Return V2 30
Page 30 of 44
30.0 Appendix 5:Assisted Admissions Coordinators Check List (Sample).
Assisted Admission/Return V2 31
Page 31 of 44
31.0 Appendix: 6. Assisted Admission Team Leader’s Report Form.
Assisted Admission/Return V2 32
Page 32 of 44
32.0 Appendix: 7. Assisted Admission Team Leader’s Report Guidelines.
Assisted Admission/Return V2 33
Page 33 of 44
33.0 Appendix: 8. Assisted Admission Risk Screening Form.
Assisted Admission/Return V2 34
Page 34 of 44
34.0 Appendix: 9. Assisted Admission Risk Screening Form (Continuation
Sheet).
Assisted Admission/Return V2 35
Page 35 of 44
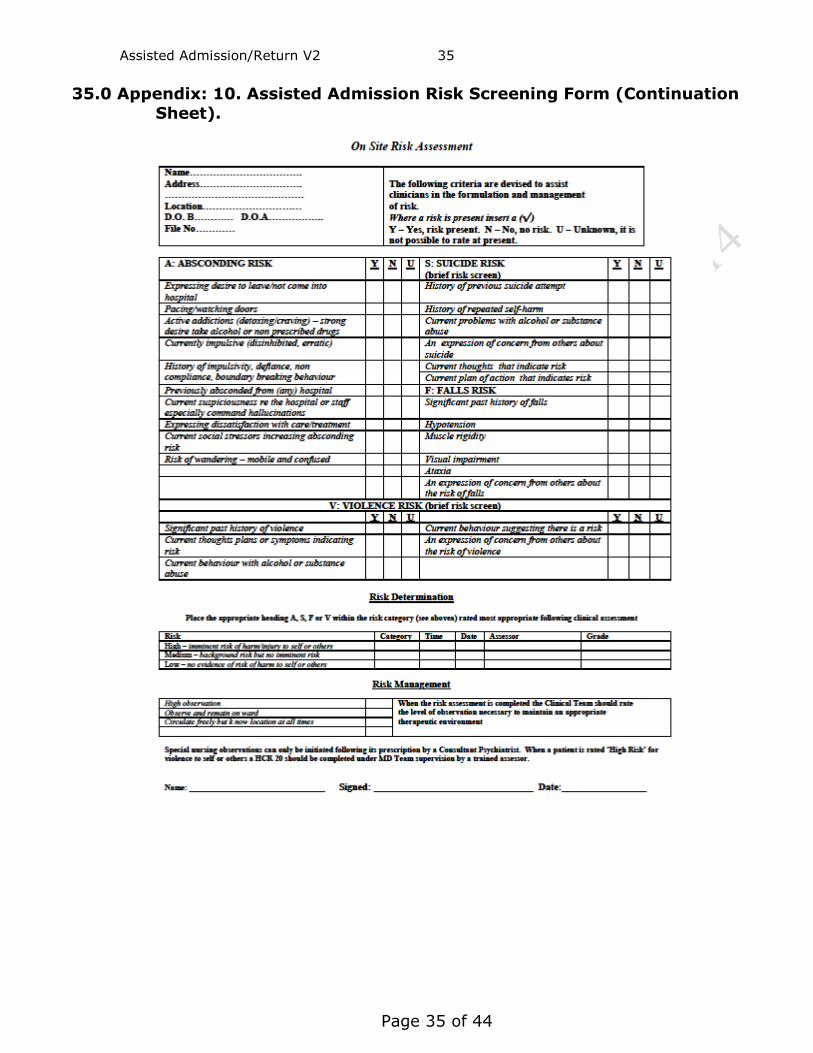
35.0 Appendix: 10. Assisted Admission Risk Screening Form (Continuation
Sheet).
Assisted Admission/Return V2 36
Page 36 of 44
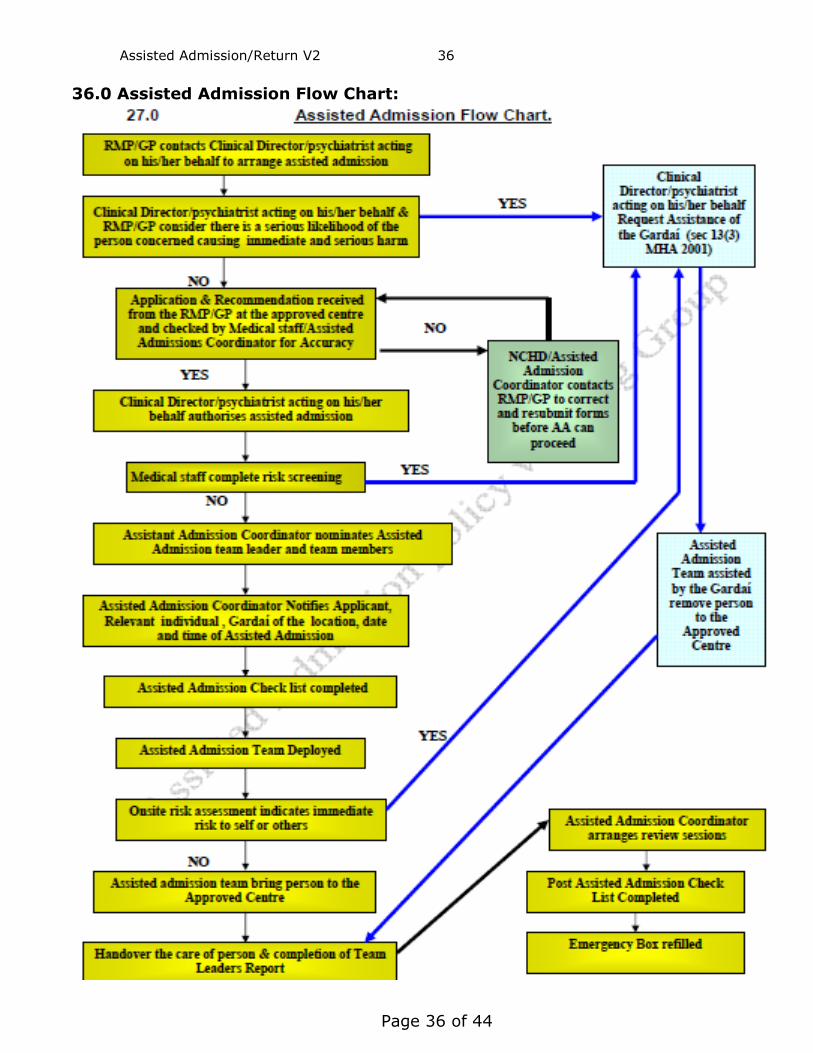
36.0 Assisted Admission Flow Chart:
Assisted Admission/Return V2 37
Page 37 of 44
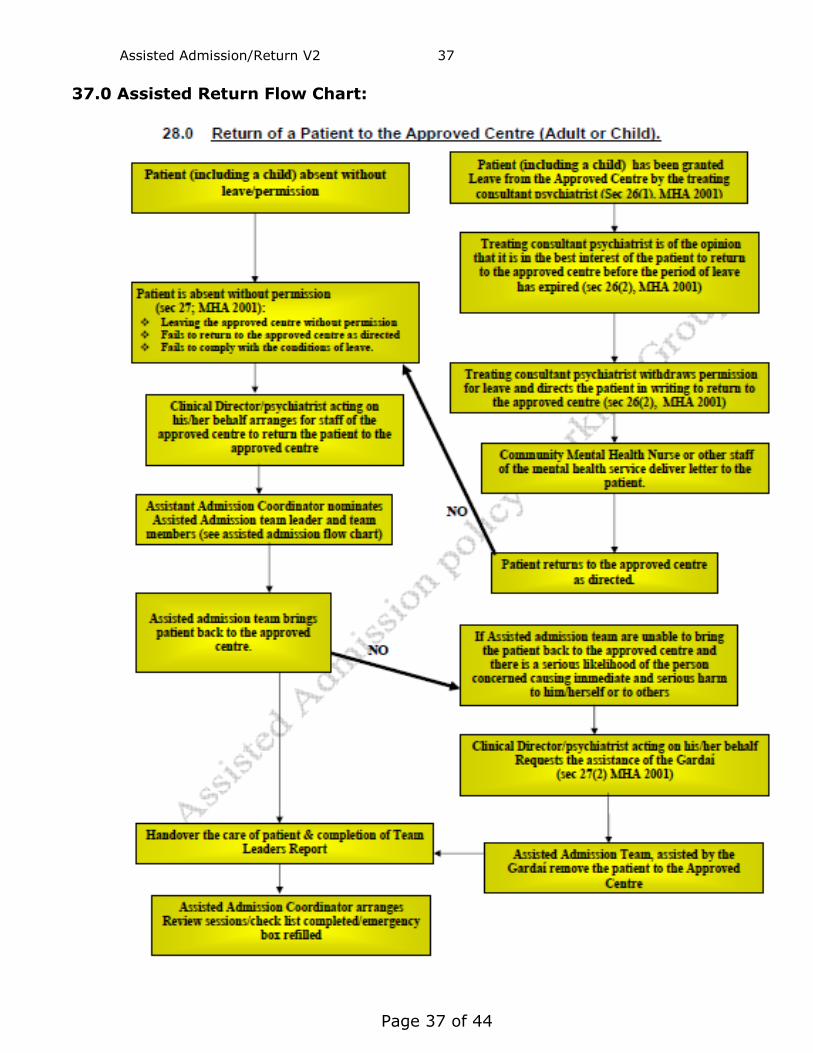
37.0 Assisted Return Flow Chart:
Assisted Admission/Return V2 38
Page 38 of 44
38.0 Production and Consultation Trail:
Version 2 of this document was developed by the authors on January 2014. It was
distributed to the following for comment in February 2014,
ISA Managers Voluntary Organisations (Grow, HAIL, IAN, Bodywhys) MHAIG Mental Health Act Administrators Directors of Nursing ECD’s
The outcome of the consultative process was reviewed and the document was further refined March 2014. Legal opinion was sought from Arthur Cox Ltd Legal Advisor to the HSE in February 2014. The document was sent to the Mental Health Act Implementation Group for final consideration in March 2014. The final document was presented to the National Mental Health Division Management Team on the 26th May 2014 for approval.
39.0 Revision History:
PPG-MHATG-CLN-03 Assisted Admission (Removal of the Person to the Approved Centre
Section 13 Mental Health Act 2001) and Assisted Return (Return of a person to the
Approved Centre Section 27 Mental Health Act 2001).
Section Changes Made
All New National Policy Template
1.1 Added new point “The HSE is committed to providing……”
1.2 Added new point “The HSE is committed to ensuring…..”
2.1 Added “..The policy also acts as a guide to staff of the community mental health
services who may have a peripheral role in the removal or return of a
person/patient to the approved centre.” 2.3 Added “….and ensuring protection of these rights is a significant responsibility of mental
health services and a component of providing”
3.1 Added “…community staff,…”
Assisted Admission/Return V2 39
Page 39 of 44
PPG-MHATG-CLN-03 Assisted Admission (Removal of the Person to the Approved Centre
Section 13 Mental Health Act 2001) and Assisted Return (Return of a person to the
Approved Centre Section 27 Mental Health Act 2001).
Section Changes Made
3.2 Added “This policy should be read in conjunction with the documents in section 4.0.”
3.3 Added new point “ This policy may be reviewed……”
4.0 Legislation/Other related policies content updated.
5.8 Added definition of clinical director.
6.2.2 Added “….or policy.”
6.2.3 Added “….local….”
6.2.4 Added “to assist the patient in requesting and where necessary participating in a review
of their assisted admission. “
Removed “…so that where a patient requests..” and “…that they have access to an
independent advocate to conduct such a review with the patient.”
6.3. New section Added points 6.3.1 to 6.3.3.
7.4 New point added “A verbal request for assistance of the Gardaí must be followed up in
writing as soon as practicable (Appendix 2)”.
7.8 Added new point “ The assisted admission team will ensure…..”
7.9 Added “..maintained…” and “….by the assisted admission coordinator.”
Removed “…used…”
8.1 Added “…(who will be a psychiatric nurse)….”
8.4 Removed “…..is being..” and “..will be…”
Added “…..team leaded..” and “…team co-ordinator. (There is also an eLearning
programme available to update knowledge on HseLand)”.
9.4 Added”…on site….”
9.6 New point added “The Gardaí will assist the assisted admission team in the removal or
return of a person/patient in accordance with section 13(3) and 27(2),………….”
10.10 Removed “…not…” Added “….an….” “…or the local assisted admission team…”
10.11 Added “…as soon as practicable.” 11.8 Added “……including information provided by the Authorised Officer where they are the
applicant.”
11.9 Added “…of…” Removed “…is…” and “…where….”
11.14 Added “) a copy of which should be retained in the patients clinical file.
NOTE: The content of the report should be based on the guidelines in Appendix
7.
13.12 Added “….Both the team and the Gardaí will use the least restrictive measures to
proceed……”
14.3 Added “..obtain..” Removed “..for…”
15.1 Added “…the…”
18.2
Added New Point “Where the patient has been brought to the approved centre for an
assessment………”
18.3 New point added “If the patient is unwilling to stay voluntarily then section 14(2) of
the MHA 2001……..”
18.4 Added “……, giving details of the assisted admission and any relevant information
relating to it (Appendix 6 & 7).”
18.6 Added “..assist the patient in requesting and where necessary participating in a review
of their assisted admission…”
Removed “…if requested by the patient, the independent advocate will review the
assisted admission process…”
18.7 Added “…The contact details of the local advocate may also be given to the person and
their carers.”
19.0 New section (19.1 to 19.3) Review Process
20.0 New Section (20.1 to 20.2) Garda HSE Liaison Group.
Assisted Admission/Return V2 40
Page 40 of 44
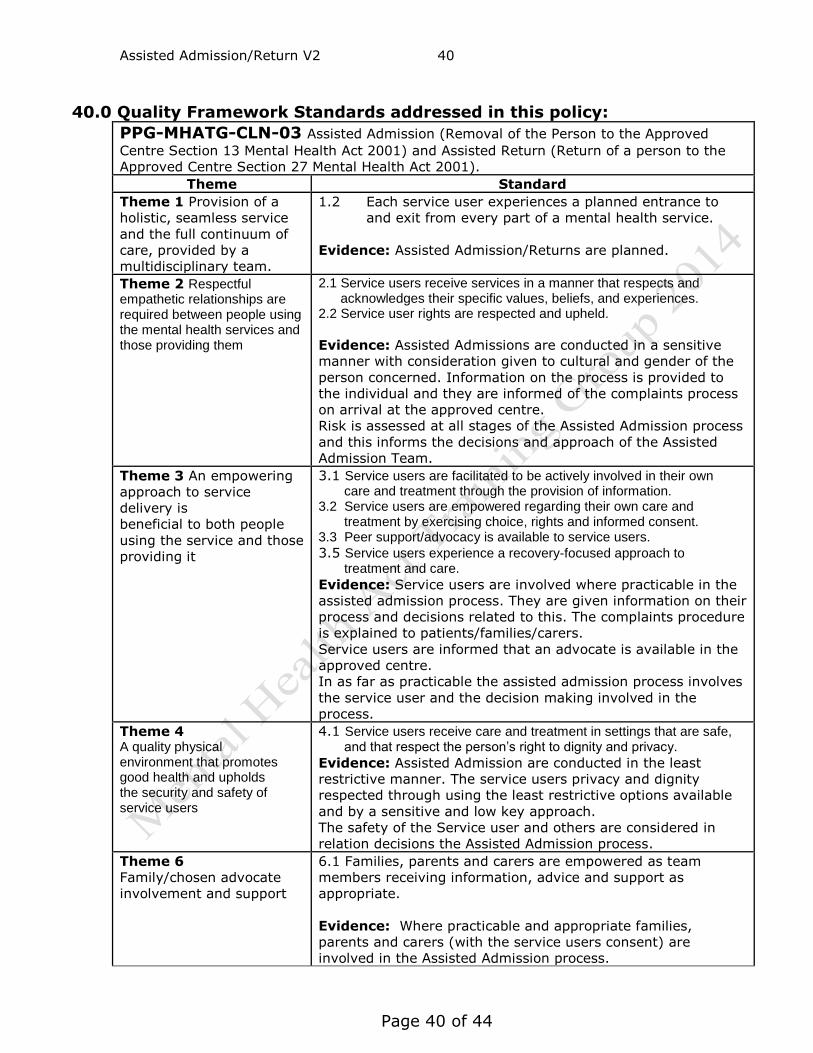
40.0 Quality Framework Standards addressed in this policy:
PPG-MHATG-CLN-03 Assisted Admission (Removal of the Person to the Approved
Centre Section 13 Mental Health Act 2001) and Assisted Return (Return of a person to the
Approved Centre Section 27 Mental Health Act 2001). Theme Standard
Theme 1 Provision of a
holistic, seamless service
and the full continuum of
care, provided by a
multidisciplinary team.
1.2 Each service user experiences a planned entrance to
and exit from every part of a mental health service.
Evidence: Assisted Admission/Returns are planned.
Theme 2 Respectful empathetic relationships are required between people using the mental health services and those providing them
2.1 Service users receive services in a manner that respects and acknowledges their specific values, beliefs, and experiences. 2.2 Service user rights are respected and upheld.
Evidence: Assisted Admissions are conducted in a sensitive
manner with consideration given to cultural and gender of the
person concerned. Information on the process is provided to
the individual and they are informed of the complaints process
on arrival at the approved centre.
Risk is assessed at all stages of the Assisted Admission process
and this informs the decisions and approach of the Assisted
Admission Team.
Theme 3 An empowering
approach to service
delivery is
beneficial to both people
using the service and those
providing it
3.1 Service users are facilitated to be actively involved in their own care and treatment through the provision of information. 3.2 Service users are empowered regarding their own care and treatment by exercising choice, rights and informed consent. 3.3 Peer support/advocacy is available to service users.
3.5 Service users experience a recovery-focused approach to treatment and care.
Evidence: Service users are involved where practicable in the
assisted admission process. They are given information on their
process and decisions related to this. The complaints procedure
is explained to patients/families/carers.
Service users are informed that an advocate is available in the
approved centre.
In as far as practicable the assisted admission process involves
the service user and the decision making involved in the
process.
Theme 4 A quality physical environment that promotes good health and upholds the security and safety of service users
4.1 Service users receive care and treatment in settings that are safe, and that respect the person’s right to dignity and privacy.
Evidence: Assisted Admission are conducted in the least
restrictive manner. The service users privacy and dignity
respected through using the least restrictive options available
and by a sensitive and low key approach.
The safety of the Service user and others are considered in
relation decisions the Assisted Admission process.
Theme 6
Family/chosen advocate
involvement and support
6.1 Families, parents and carers are empowered as team
members receiving information, advice and support as
appropriate.
Evidence: Where practicable and appropriate families,
parents and carers (with the service users consent) are
involved in the Assisted Admission process.
Assisted Admission/Return V2 41
Page 41 of 44
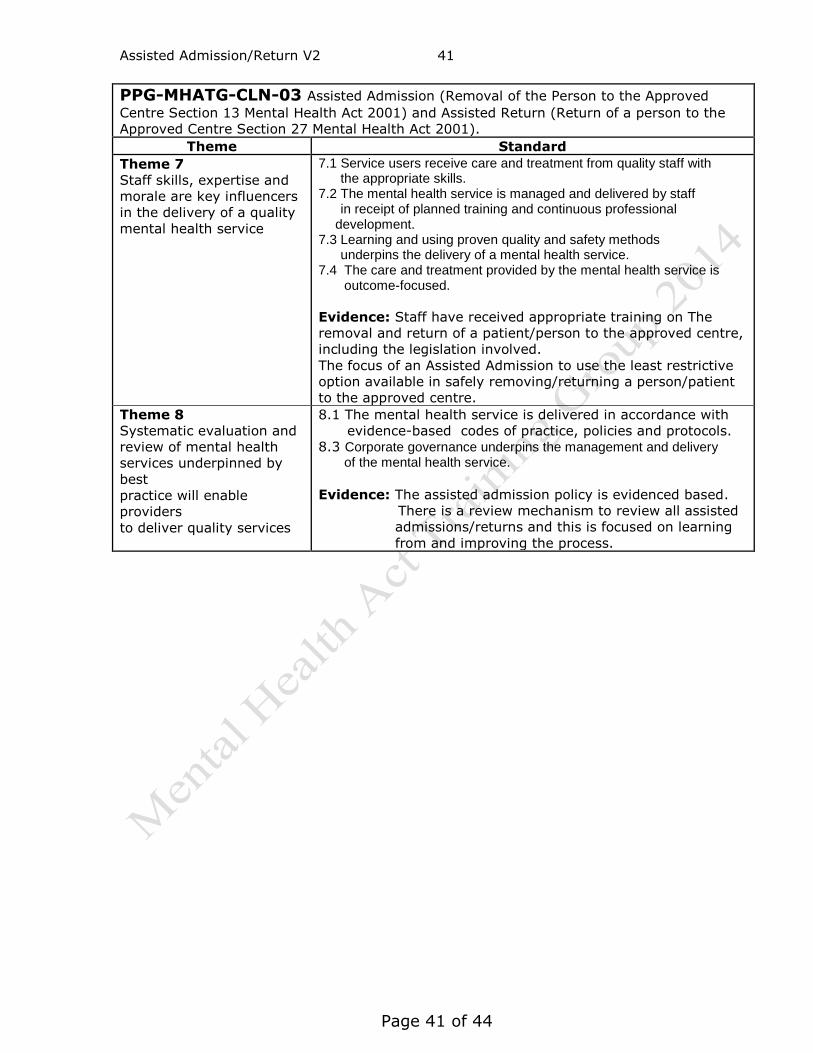
PPG-MHATG-CLN-03 Assisted Admission (Removal of the Person to the Approved
Centre Section 13 Mental Health Act 2001) and Assisted Return (Return of a person to the
Approved Centre Section 27 Mental Health Act 2001). Theme Standard
Theme 7
Staff skills, expertise and
morale are key influencers
in the delivery of a quality
mental health service
7.1 Service users receive care and treatment from quality staff with the appropriate skills. 7.2 The mental health service is managed and delivered by staff in receipt of planned training and continuous professional
development. 7.3 Learning and using proven quality and safety methods underpins the delivery of a mental health service. 7.4 The care and treatment provided by the mental health service is outcome-focused.
Evidence: Staff have received appropriate training on The
removal and return of a patient/person to the approved centre,
including the legislation involved.
The focus of an Assisted Admission to use the least restrictive
option available in safely removing/returning a person/patient
to the approved centre.
Theme 8
Systematic evaluation and
review of mental health
services underpinned by
best
practice will enable
providers
to deliver quality services
8.1 The mental health service is delivered in accordance with
evidence-based codes of practice, policies and protocols. 8.3 Corporate governance underpins the management and delivery of the mental health service.
Evidence: The assisted admission policy is evidenced based.
There is a review mechanism to review all assisted
admissions/returns and this is focused on learning
from and improving the process.
Assisted Admission/Return V2 42
Page 42 of 44
41.0 Signature Sheet: (All staff to Sign that they have read and
understand this Policy)
DATE NAME SIGNATURE
Assisted Admission/Return V2 43
Page 43 of 44
All staff to Sign that they have read and understand this Policy
DATE NAME SIGNATURE
Add additional pages as necessary.
Assisted Admission/Return V2 44
Page 44 of 44
All staff to Sign that they have read and understand this Policy
DATE NAME SIGNATURE
Add additional pages as necessary.





























