Embed Size (px)
Citation preview

HOW TO USE THE SLIDE SET
This slide set was created as a supplement for use in teaching clinical reasoning. Please feel free to use and modify as needed for use at your institution.
There are 3 components of this slide set:
1.
2.
3.

A 60-year-old Woman with Chorea and Weight Loss
Clinical Reasoning Series

A 60-year-old woman was transferred to our institution for further evaluation of chorea and
weight loss

What are your initial thoughts about chorea?

Chorea An uncommon symptom, especially in older
adults Hyperkinetic movement disorder Rapid, semi-purposeful, non-patterned
involuntary movements involving distal or proximal muscle groups
Link to video http://www.youtube.com/watch?v=OveGZdZ_sVs

Most Common Causes of Chorea
1. Huntington’s Disease– Look for family history (usually autosomal
dominant, but can be de novo) – Associated with early cognitive decline
2. Sydenham’s Chorea– Post-rheumatic fever– Usually in children and young adults

The Dual-Process Theory
Two different approaches used to make diagnostic decisions developed by cognitive
psychologists
1. Intuitive
2. Analytical
Most physicians use one or the other, but ideally both should be used because they
complement each other

The Intuitive Approach Usually used by experienced or expert
clinicians Relatively quick Based on pattern recognition Implicit, uses first impressions Requires little cognitive effort

The Intuitive Approach
Example:
“Common disorders associated with chorea are Sydenham’s chorea and Huntington’s chorea”

The Analytical Approach Usually used by novice clinicians or by
experienced clinicians when confronted with difficult cases
Explicit Based on knowledge and logic Less susceptible to bias Slow process Requires considerable cognitive work

The Intuitive Approach
Example:
“Metabolic disorders, nutritional deficiencies, infections, autoimmune disorders, vascular ischemia, toxins and medication side effects are possible etiologies of chorea”

For the past 6 months: Progressive clumsiness and chorea Difficulty speaking and eating due to
involuntary movements of the mouth Intermittent progressive abdominal pain and
nausea Unintentional weight loss (sixty pounds)

What is your differential diagnosis?

Differential Diagnosis Infectious
- CNS, HIV-associated, neurosyphilis Malignancy Toxins/Deficiencies
- Heavy metal toxicity, vitamin B12 deficiency Wilson’s Disease Autoimmune Neuroacanthocytosis Anti-phospholipid syndrome Celiac disease Sarcoidosis Hepatocerebral degeneration

Which type of reasoning are you
currently using?
Intuitive or Analytical?

Past Medical History - Atrial fibrillation
- Hypertension
- Hypothyroidism
- Vitamin B12 deficiency Widowed. No family history of
neurodegenerative disorder or malignancy 30-pack-year history of tobacco use and quit
6 months ago No alcohol or illegal drug use

Home Medications Atorvastatin Digoxin Furosemide Levothyroxine Vitamin B12 Warfarin

Physical Exam
Temp: 98.6 °F, BP: 108/62 mm Hg, HR: 74
General: cachectic, chronically ill appearing, in no distress. Alert and oriented
Cardiovascular: heart rhythm irregularly irregular
Pulmonary, gastrointestinal and integumentary unremarkable

Physical Examination Neurologic: Oral dyskinesias and severe dysarthria Conjugate gaze and symmetric face Choreiform movements in upper extremities Motor 4/5 strength in all four extremities Moderate generalized muscle atrophy consistent
with cachexia and displayed paratonia in both upper extremities (involuntary variable resistance during passive movement)

Physical Examination Neurologic: Reflexes: 1+ in upper extremities, absent in lower
extremities Plantar responses: flexor Proprioception: decreased at the toes Vibratory sensation: decreased below the knees of
bilateral lower extremities Diffuse allodynia, more prominent in the abdomen Coordination testing: finger-to-nose task was
impaired due to her upper extremity chorea Gait: not tested as patient was wheelchair-bound

What tests or studies should be done next?

Complete metabolic panel, blood count, and thyroid function tests: unremarkable
International normalized ratio (INR): 2.3 Electromyographic study: mild distal motor
neuropathy Computed tomographic scans of head, chest,
abdomen and pelvis with and without contrast: unremarkable

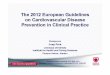
MRI brain Magnetic resonance imaging showed T1
hyperintensities within the basal ganglia with thalamic sparing and no areas of ischemia or hemorrhage

What would you do next?

What type of reasoning are you
currently using?
Intuitive or Analytical?

Blood was tested for the presence of paraneoplastic antibodies and returned positive for anti-CRMP-5 IgG at a level of 1:3,840 (negative < 1:240)

What do you know about paraneoplastic syndromes?

Paraneoplastic Syndromes Manifest as symptoms or findings that are
explained by the presence of a malignancy, but that are not produced by a local effect from tumor cells
Examples: hyponatremia from small cell lung cancer or neurological paraneoplastic syndromes due to immune responses against a tumor expressing a certain antigen that cross-reacts with neuron antigens

Paraneoplastic Syndromes Often precede the diagnosis of cancer The presence of a paraneoplastic antibody in
an individual with a neurological disorder is not necessarily diagnostic of an underlying malignancy
Some antibodies are more likely to be associated with an underlying neoplasm than others

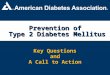
Paraneoplastic Antibody Predominant Associated Neoplasm
Associated Paraneoplastic Syndrome
Anti-Hu Small cell lung carcinoma (93%)
Cerebellar degeneration, neuropathy
Anti-Yo Ovarian (47%), breast (25%), endometrial (13%)
Cerebellar degeneration, dementia, neuropathy
Anti-Ma2 +/- anti-Ma1 Testicular (55%), non-small cell lung carcinoma (21%)
Brainstem encephalitis, parkinsonism
Anti-CRMP-5 Small cell lung carcinoma, (77%), thymoma (8%)
Cerebellar degeneration, chorea, myelopathy, neuropathy
Anti-Amphiphysin Small cell lung carcinoma, (59%), breast (35%)
Cerebellar degeneration, stiff person syndrome, dementia, psychiatric symptoms, myelopathy, neuropathy
Anti-Ri Breast (43%), small-cell lung carcinoma (24%) and non-small cell lung carcinoma (24%)
Cerebellar degeneration, opsoclonus-myoclonus syndrome, brainstem encephalitis, myelopathy, neuropathy

The presence of the CRMP-5 antibody with the patient’s clinical findings supported the diagnosis of “definite” paraneoplastic syndrome
Malignancy has been reported in greater than 90% of cases with this antibody

Repeat CT scans of the chest, abdomen, and pelvis: unrevealing
Mammogram: normal Colonoscopy had been performed six months
prior with negative results
Three months after the initial panel was sent, CRMP-5 antibody titer was repeated and again returned positive

What would you do next?

Referred to Oncology
PET scan: 1.5 cm hypermetabolic lymph node posterior to the trachea with a standardized uptake value of 3.4
(normal < 2.5)

Endoscopic ultrasound-guided fine needle aspiration was positive for malignant cells that stained for synaptophysin, thyroid transcription factor 1 (TTF-1), and CD56
This confirmed the diagnosis of small cell cancer of pulmonary origin

Underwent 4 cycles of chemotherapy, lung radiation therapy and prophylactic whole brain radiation therapy
One year following treatment, she had gained weight, was eating well, and was no longer wheelchair-bound
Most recent CRMP-5 antibody titer was negative

Chorea, from the Latin dance or Greek khoreia, is a specific type of movement disorder that is characterized by rapid, semi-purposeful, non-patterned involuntary movements

Chorea can be caused by: Sydenham’s chorea Genetic disorders: Huntington’s disease, Wilson’s
disease Metabolic disorders: electrolyte disturbances,
vitamin deficiencies, thyroid disorders Space-occupying lesions and paraneoplastic
processes Autoimmune conditions Toxin ingestions

Paraneoplastic syndromes manifest as symptoms or findings that are explained by the presence of a malignancy, but that are not produced by a local effect from tumor cells

Patients found to have paraneoplastic antibodies should be evaluated for an occult malignancy
The CRMP-5 antibody can produce chorea and seems to be associated with malignancy in greater than 90% of cases

References
Bhatnagar D, Morris JL, Rodriguez M, Centor RM, Estrada CA, Willett LL. A middle-age woman with sudden onset dyspnea. J Gen Intern Med. 2011;26:551-4.
Dhaliwal G. Going with Your Gut. J Gen Intern Med 26:107–109. Henderson MC, Dhaliwal G, Jones SR, Culbertson C, Bowen JL. Doing what comes
naturally. J Gen Intern Med. 2010;25:84-7. Croskerry P. A universal model of diagnostic reasoning. Acad Med. 2009; 84:1022–1028. Norman G. Dual processing and diagnostic errors. Adv Health Sci Educ Theory Pract.
2009. Suppl 1:37-49. Eva KW, Hatala RM, LeBlanc VR, Brooks LR. Teaching from the clinical reasoning
literature: combined reasoning strategies help novice diagnosticians overcome misleading information. Med Educa 2007; 41: 1152–1158. 10.1111/j.1365-2923.2007.02923.x
Bowen, JL. Educational Strategies to Promote Clinical Diagnostic Reasoning. N Engl J Med 2006;355:2217-2225.
Gozzard P, Maddison P. Which antibody and which cancer in which paraneoplastic syndromes? Pract Neurol. 2010;10:260-70.
Pellacia T, Tardif J, Triby E, Charlin B. An analysis of clinical reasoning through a recent and comprehensive approach: the dual process theory. Med Educ Online 2011; 16:5890. doi: 10.3402/meo.v16i0.5890.

Chorea – Videos
Clinical assessment of chorea severity (Medscape login required). Available at: http://www.medscape.com/infosite/xenazine/article-1?src=0_nl_sm_0&eguid=MTEyMTM5NzU. Accessed August 29th, 2011.
YouTube. Available at: http://www.youtube.com/watch?v=OveGZdZ_sVs. Accessed August 29th, 2011.