Embed Size (px)
Citation preview

How to manage comorbidities in
relation to antiretroviral therapy in
(aging) HIV-infected individuals
TAIWAN SYMPOSIUM ON HIV COMORBIDITIES 2016Kaohsiung, 1 October 2016
Esteban Martinez

Comorbidities in HIV+ patients
• General overview
• Kidney
• Bone
• Cardiovascular

Comorbidities in HIV+ patients
• General overview
• Kidney
• Bone
• Cardiovascular

http://www.eacsociety.org/files/2015_eacsguidelines_8_0-english_rev-20160124.pdf

In addition to data collection regarding: medical history, HIVdisease and co-infections
EACS guidelines:
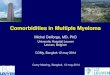
Screening for comorbidities
http://www.eacsociety.org/files/2015_eacsguidelines_8_0-english_rev-20160124.pdf

Kidney Bone CV Cancer CNS
Screening
Blood and
urine
chemistries
DEXA
+/- FRAX
score
Framingham
(or similar)
score
No
(cytology
cervical
cancer)
No
(psychometric
tests?)
Prediction
of clinical
problem
Highly
accurate
Less
accurate
More
innaccurate
More
innacurate
or lacking
Lacking
Not all comorbidities are equally assessed

Avoid antiretrovirals with potential toxicities
impacting on specific comorbidities
http://www.eacsociety.org/files/2015_eacsguidelines_8_0-english_rev-20160124.pdf

High Moderate Low/No
ATV/rit NVP NRTIs (all)
DRV/rit EFV RPV
ATV/cobi ETV MVC
DRV/cobi RAL
EVG/cobi DTG
http://www.eacsociety.org/files/2015_eacsguidelines_8_0-english_rev-20160124.pdf
Avoid antiretrovirals with risk for drug-drug
interactions with comorbidities therapies

Avoid tobacco
http://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/effects_cig_smoking/

Comorbidities in HIV+ patients
• General overview
• Kidney
• Bone
• Cardiovascular

How to assess kidney function in patients with HIV infection?
To measure the capacity
of renal clearance(Nº of functioning nephons)
To assess the degree of
structural damage
(Kidney disease progression)
Glomerular filtration rate Proteinuria

Creatinine is not enough as a measure of
renal clearance
Johnson R, et al. Comprehensive Clinical Nephrology. 2000. Mosby. St. Louis. 4.15.1–4.15.15.
Inulin Clearance (mL/min/1.73 m2)
Se
rum
Cre
ati
nin
e(m
g/d
L)
9.0
8.0
7.0
6.0
5.0
4.0
3.0
2.0
1.0
0.0
0 20 40 60 80 100 120 140 160 180
Creatinine is a poor
reflector of GFR
GFR versus Serum Creatinine

• Cockcroft-Gault (CG) Equation: CLcr (ml/min) =
[140 –Age (yrs] x Wt (kg) x (0.85 if female)
72 x Serum creatinine (mg/dL)
Overestimates GFR at decreased function
Has been used to develop drug dosing algorithms
• Modification of Diet in Renal Disease (MDRD) Equation
GFR (mL/min/1.73m2) = 186 x (Scr)-1.154 x (Age) -0.203 (x0.742 if female)
(x1.21 if black)
In normal ranges, tends to underestimate GFR
Has not been used to develop drug dosing algorithms
• Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) Equation
GFR (mL/min/1.73m2) = 141 x min(Scr /κ,1)α x max(Scr/κ, 1)-1.209 x
0.993Age x 1.018 [if female] x 1.159 [if black]
More specific methods to estimate renal
clearance

National Kidney Foundation. K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease. Am J Kidney Dis 2002
Wetzels JF et al. Kidney Int. 2007;72:632–637., Glassock R. Nephrology Times 2009
0
20
40
60
80
100
120
140
160
180
200
0 20 40 60 80 100
Estim
ate
d G
FR
(m
L/m
in/1
.73m
2)
Age (years)
Inulin (Davies and Shock, 1950)
NHANES III Estimated GFR (median, 95th percentiles)
eGFR decreases with age

Normal eGFR decrease: 0.5-1 mL/min/1.73m2 per year
The slope of eGFR decline increases with age
Abnormal eGFR decrease: > 3-5 mL/min/1.73m2 per year
Lindeman RD et al. J Am Geriatr Soc 1985

For similar creatinine and age, women have
worse eGFR than men
http://mdrd.com/

Ginsberg JM et. al. N Engl J Med 1983
Random urine:
Protein mg/dl
Creatinine mg/dl
24-hour urine - Gold Standard
Simple assessment of proteinuria using
protein/creatinine ratio

Number of
patients
eGFR with TDF vs. Other
(95% CI)
P value
Meta-analysis 1 517 -3.9 mL/min (-2.3 to -5.7) <0.05
10-year cohort 2
Year 1 483 -3.1 mL/min (-5.6 to -0.5) 0.02
Year 2 358 -4.1 mL/min (-6.0 to -2.1) <0.001
Year 3 241 -2.4 mL/min (-4.6 to -0.3) 0.02
Year 4 149 -3.1 mL/min (-7.0 to +0.8) NS
1. Cooper RD et al. Clin Infect Dis 2010
2. Laprise C et al. Clin Infect Dis 2013
TDF significatively lowers eGFR but short-
term effect is limited

Study (Third Agent)TDF
Subjects, nD/C due to Renal
AE, %Follow-up,
weeks
TDF alone GS-102, 103 (TDF for HBV) 426 <1.5 240
Unboosted
Regimens
STARTMRK (RAL or EFV) 563 NR 48
QDMRK (RAL) 770 NR 48
GS-903 (EFV) 299 0 144
GS-934 (EFV) 257 0 144
ECHO/THRIVE (RPV or EFV) 1096 0 96
GS-236 102, 104 (EFV) 396 0 48
ASSERT (EFV) 193 0 48
Boosted
Regimens
ABT-730 (LPV/r) 664 0 96
ARTEMIS (DRV + RTV or LPV/r) 689 0 96
GEMINI (SQV + RTV or LPV/r) 337 0 48
GS-263 103 (ATV+RTV) 355 0.3% 48
GS-263 102, 103, 104 (STRIBILD) 749 0.8% 48
CASTLE (ATV+RTV or LPV/r) 878 <1% 96
HEAT (LPV/r) 345 <1% 96
ARTEN (ATV+RTV or NVP) 569 <1% 48
ABT-418 (LPV/r) 190 <1% 96
ACTG 5202 (ATV+RTV or EFV) 925 1% 96
BATON (ATV+RTV) 100 1% 48
GS-216 105, 114 (ATV+RTV or ATV+COBI) 771 1.6% 48
ALERT (FPV+RTV or ATV+RTV) 106 2.8% 48
Total 10,657 0 - 2.8% 48-144
NR: not reported
Discontinuation due to renal impairment in
TDF-treated pts

Log-rank test
<59kg vs >67kg p=0.002
59-67kg vs >67kg p=0.073
n=160
n=168
n=167
Nishijima T et al. AIDS 2014
Time to 25% eGFR reduction according to baseline weight categories
Low weight is a risk factor for TDF-related
kidney toxicity

Kearney B et al. J Acquir Immune Defic Syndr 2006
0 6 12 18 2410
100
1000
TDF alone
TDF + LPV/r
mean± 95%CI Time (hr)
Tenofo
vir
Concen
tration (
ng/m
L)
TDF AUC
34%
-60
-40
-20
0
20
40
60
80
100
Cmax
AUC
Cmin
ATV 400 mg TDF 300 mg
-25%-20%
-40%
24%
14%22%
% c
han
ge f
rom
wh
en
do
sed
alo
ne
Kaul S et al. ICAAC 2003
Similar plasma TDF increases with DRV/r and EVG/c
Hill A et al. J Int AIDS Soc 2014
Plasma TDF may increase with PI’s and EVG/c

MRP4
OAT3
Blood
(Basolateral)Urine
(Apical)
OAT1N
NN
N
NH2
OPO
O--O
Tenofovir
Active Tubular Secretion
Cation Transport Pathway
Blood
(Basolateral)Urine
(Apical)
OCT2H+MATE1
N
N
NH2O
Creatinine
Active Tubular Secretion
Anion Transport Pathway
NH
HN
ONH
N
O O
O
N
SS N
N
O
Cobicistat
MRP2
Ritonavir
Stray KM et al. Antimicrob Agents Chemother 2013
Intra-tubular TDF may increase with RTV (but
not with COBI)

Pathogenesis of tenofovir-related kidney
dysfunction
Yombi JC et al. AIDS 2014
Baxi SM et al. AIDS 2014
TENOFOVIR
CREATININE
Ritonavir Ritonavir
Rilpivirine
Dolutegravir
Ritonavir
Cobicistat
Creatinine
Tenofovir Tenofovir
Kidney injury: tubular markers in urine
↓eGFR (progressive)
eGFR (estable)
OAT1
OAT3
OCT2
MRP2
MRP4
MATE1
Blood
Tubular Cell
Urine
age
↓BMI
Ritonavir
Cobicistat

CKD Risk by Yrs of ARV Exposure, IRR (95% CI)
Drug 1 Yr 2 Yrs 5 Yrs
TDF1.12
(1.06-1.18)1.25
(1.12-1.39)1.74
(1.33-2.27)
ATV/RTV1.27
(1.18-1.36)1.61
(1.40-1.84)3.27
(2.32-4.61)
LPV/RTV1.16
(1.10-1.22)1.35
(1.21-1.50)2.11
(1.62-2.75)
Relationship Between Increasing Exposure to ARVS and CKD
1.80
1.60
1.40
1.20
1.00
0.00ATV/RTV LPV/RTV TDF
IRR
(9
5%
CI)
Univariate
Multivariate
On treatment
TDF censored
Mocroft A et al. CROI 2015: abstract 142
ARVs and risk of kidney disease:
Is PI-effect a pure one or is it post-TDF-related?
EuroSIDA

TDF and TAF bioavailability
Lee WA et al. Antimicrob Agents Chemother 2005

n (%)E/C/F/TAF
n=866
E/C/F/TDF
n=867
Events
Renal adverse events leading to discontinuation 0 4 (0.5)
Tubulopathy/Fanconi syndrome 0 0
-6.6p <0.001
-11.2
E/C/F/TAF
E/C/F/TDF
TAF vs. TDF: Renal safety
Sax P et al. 22nd CROI 2015: abstract 143LB

Virologically suppressed adults with stable eGFRCG (30–69 mL/min) switched
from TDF- or non-TDF–containing regimens to open-label E/C/F/TAF
(n=80)
(n=162)
Safety of TAF in renal impairment
Pozniak A et al. 22nd CROI 2015: abstract 795

Comorbidities in HIV+ patients
• General overview
• Kidney
• Bone
• Cardiovascular

0 10 20 30 40 50 60
Bone m
ass
Age (years)
Men
Women
Menopause
Fracture threshold
Average annual decrease: 1% BMD per year
BMD decreases with age
Compston. Clin Endocrinol 1990

Dual-X absorptiometry (DXA) measures BMD

-6
-5
-4
-3
-2
-1
0
0 24 48 96 144
Adapted from several references: Rivas et al. HIV Medicine 2008; Hansen et al, IAS 2009; Daar et al. CROI 2010
Semanas
Ch
ang
e in
BM
D fro
m b
ase
line
(%
)
Change in BMD from baseline (%)(irrespective of the antiretroviral drugs used)
Initiation of ART causes BMD decrease

Van Vonderen MG et al. CROI 2011
BMD decrease with ART initiation is due to a
high bone turnover

Overton ET et al. CROI 2014; Ofotokun I et al. CROI 2016
Vitamin D Zolendronate
BMD decrease with ART initiation can be
reduced or avoided

McComsey GA et al. J Infect Dis 2011
ACTG 5202
Greater BMD with TDF (vs. ABC) and with
ATV/r (vs. EFV)

Brown T et al. CROI 2014: abstract 779LB
Greater BMD with ATV/r or DRV/r (vs. RAL)

Low vitamin D is a common cause of low
BMD measurement (DXA)
Dao CN et al. Clin Infect Dis 2011

0
0,5
1
1,5
2
2,5
3
3,5
4
4,5
5
40-45 45-50 50-55 55-60 60-65 65-70 70-75 75-80
HIV infected
HIV uninfected
Ag
e-s
pecif
ic f
rac
ture
in
cid
en
ce
-ra
tes
(/1
000 p
ers
on
-yea
rs)
in H
IV i
nfe
cte
d V
S u
nin
fecte
d p
ati
en
ts
Low absolute risk of fractures: Excess risk in
HIV+ >65 years
Guerri-Fernandez R et al. J Bone Mineral Res 2013

1994 WHO classification according to BMD
measurement (DXA)
Assessment of fracture risk and its application to screening for postmenopausal osteoporosis.
Report of a WHO Study Group. Geneva, World Health Organization, 1994

FRAX score (SPAIN)
https://www.shef.ac.uk/FRAX/tool.aspx?country=4
Treatment
decision making:
Major osteporotic >10%
Hip fracture >3%

FRAX score (TAIWAN)
https://www.shef.ac.uk/FRAX/tool.aspx?country=26
Treatment
decision making:
Major osteporotic >10%
Hip fracture >3%

• Normal:
– No intervention
– DXA in ≥5 years
• Osteopenia:
– Exercise, quitting smoking, calcium intake (diet preferred)
– Measure serum vit D: if low, prescribe supplements
– DXA in 2-5 years (inversely proportional to osteopenia intensity)
• Osteoporosis:
– Exercise, quitting smoking, calcium intake (diet preferred)
– Withdraw TDF
– Measure serum vit D: if low, prescribe supplements
– Estimate FRAX:
• If major osteoporotic ≥10% or hip ≥3% fracture risk, send patient to
Rheumatology Unit to consider biphosphonate therapy
• If major osteoporotic <10% and hip <3% fracture risk, DXA in 1-2 years
Clinical care DXA protocol for HIV+ patients in Hospital Clínic Barcelona
Patient 50y or younger with menopause or
hypogonadism should have bone DXA done

From TDF
To TDF
Bloch M. et al. HIV Med 2014.
Negredo E. et al. J Antimicrob Chemother 2014
Rasmussen TA et al. PLoS One 2012
Cotter AG et al. J Clin Endocrinol Metab 2013
SWAP Study -1.8% (-2.6, -1.1)% BMD loss at hip
PREPARE Study -1.73 (2.76)% BMD loss at hip
TROP Study +2.5 (1.6, 3.3)% BMD gain at hip
OsteoTDF Study +2.1 (-0.6, 4.7)% BMD gain at hip
+
-
BM
DIn treated HIV patients, discontinuation of TDF
has a positive effect on BMD

Pozniak A et al. 22nd CROI 2015: abstract 795
Switch from TDF to TAF in treated HIV pts led
to BMD

HIV adults,
TDF>6mo,
HIV RNA
<50c/mL>3mo,
eGFR>60mL/m,
T-score -1
Zoledronic acid
5 mg iv yearly
Switch TDF
BMD
BMD
Randomization
Hypothesis
Zoledronic acid therapy will increase BMD more effectively over 2 years than
switching from TDF to another antiretroviral drug in the HIV treatment regimen
Bisphosphonate Therapy with Zoledronic acid or Tenofovir Switching
to Improve Low Bone Mineral Density in HIV-Infected Adults
24 months
ZEsT : An Strategic Randomized Clinical Trial

Comorbidities in HIV+ patients
• General overview
• Kidney
• Bone
• Cardiovascular

Law MG, et al. 11th CROI. 2004. Abstract 737.
Duration of HAART (years)
MI
pe
r 1
000
PY
FU
0
1
2
3
4
5
6
7
8
< 1 1-2 2-3 3-4 4+0
Observed
Predicted
Risk of myocardial infarction in HIV+ patients
can be estimated with Framingham score
D:A:D Study
Law MG et al. HIV Med 2006
Framingham score: gender, smoking, age, systolic BP, total and HDL cholesterol

If non-smoking you need to be almost
15y older to have the same CV risk
Man, 50y, smoker = risk >10% Woman, any age, even smoker = risk <10%
http://cvdrisk.nhlbi.nih.gov/
Some practical hints regarding Framingham
risk estimation
However, Framingham does not
include HIV-specific factors
Immune status
Increased inflammatory markers
Insulin resistance
Time on HAART

26510
49091309
302 (1%)
174 (3%)
104 (7%)
0
5000
10000
15000
20000
25000
30000
<10 10-to-20 >20
MI
No MI
If a patient has a low risk, the likelihood of not having a MI is high
D:A:D Study 2009
Framingham score has a low sensitivity, but a
high negative predictive value
Framingham risk score
Num
be
r of patients
Framingham >20
S=18%
E=96%
VPP=7%
VPN=99%
Framingham 10
S=48%
E=81%
VPP=4%
VPN=99%

2013 ACC/AHA score may estimate CV events
better than Framingham score
Triant V et al. 22nd CROI 2015: abstract 751
FRS
0
5
10
15
20
25
5 Y
ear
Eve
nt R
ate
(%
)
<2.5%
2.5-4.9%
5.0-7.4%
7.5-9.9%
5 Year Predicted Risk
Predicted Observed
ACC/AHA
0
5
10
15
20
25
5 Y
ear
Eve
nt R
ate
(%
)
<2.5%
2.5-4.9%
5.0-7.4%
7.5-9.9%
5 Year Predicted Risk
Predicted Observed
Partners HealthCare System HIV longitudinal cohort (n=2270), comprised of patients
seen at Brigham & Women’s Hospital or Massachusetts General Hospital in Boston, MA

Nr of patients 108
Age, years (IQR) 46 (40-52)
Current smoking (%) 50
Total cholesterol (mg/dL) 175
LDL cholesterol (mg/dL) 98
HDL cholesterol (mg/dL) 49
10-year Framingham score, % (IQR) 3 (1-5)
10-year ASCVD score, % (IQR) 3.3 (1.6-6.6)
CD4 cells/mm3 528
Viral load (copies/mL) <50
Patients with any coronary plaque (%) 45
Patients with high-risk plaques (%) 36
Statins recommeded 2004 ATP III (%) 8
Statins recommended 2013 ACC/AHA (%) 21
Zanni MV et al. AIDS 2014
Risk of subclinical CV disease is higher than
predicted

http:// www.europeanaidsclinicalsociety.org/images/stories/EACS-Pdf/EACSGuidelines-v6.1-English-Nov2012.pdf
Prior to 2015

http://www.eacsociety.org/files/2015_eacsguidelines_8_0-english_rev-20160124.pdf
2015

Major steps to intervention on smoking
cessation
U.S. Public Health Service. Agency for Healthcare Research and Quality.
http://www.ahrq.gov/clinic/tobacco/5steps.htm

Smoking cessation studies in HIV patients
Calvo-Sanchez M, Martinez E. HIV Med 2015

• Analysis of MI risk with ABC pre and post 3/08 in D:A:D cohort
• There were trends to less ABC use in high risk individuals post 3/08
• RR with ABC 1.98 (1.72-2.29), Pre 3/08 1.97, Post 3/08 1.97
Overall Pre-March 2008
Post-March 20085
4
3
2
1
0.7
Rela
tive R
isk
ABC and MI risk persists in D:A:D despite
change in ABC use
Sabin C et al. 21st CROI 2014: abstract 747LB

0
0.00 1.00 2.00 3.00 8.00
Full study population
Restricted study population
4.00 5.00 6.00 7.00
Adjusted hazard ratio for MI
Age <40 (vs 50-59) years
Age 40-49 (vs 50-59) years
Age ≥60 (vs 50-59) years
Smoking
Hypertension
Diabetes
eGFR 30-59 (vs ≥60) mL/min/1.73 m2
eGFR <30 (vs ≥60) mL/min/1.73 m2
High (≥240 vs <240 mg/dL) total chol
High (≥300 vs <300 mg/dL) triglycerides
Statin use
Recent ABC use
Adjusted Hazard Ratios of CVD Risk Factors Significantly Associated With MI
Palella F et al. 21st CROI 2015: abstract 747LB
Recent ABC and MI risk:
Controversy in NA-ACCORDMany significant differences in clinically relevant characteristics between
ABC and non-ABC users

Desai M et al. Clin Infect Dis 2015
Current ARV drugs and MI risk:
New data from US Veterans
Marginal Structural Models
(to minimise confounding)

ABC and MI risk: New data from Swiss Cohort
Young J et al. J Acquir Immune Defic Syndr 2015

de Pablo C et al. AIDS 2010; de Pablo C et al. Antivir Ther 2012; de Pablo C et al. J Infect Dis 2013
Satchell CS et al. J Infect Dis 2011; Baum PD et al. AIDS 2011; Chini M et al. Int J Immunopathol Pharmacol 2012;
Falcinelli E et al. Thromb Haemost 2013
• induces Mac-1 on leukocytes, which interacts with ICAM-1 on endothelial cells
• increases platelet activity through inhibition of soluble guanylyl cyclase
• facilitates collagen-induced platelet aggregation
ABC (in vitro or non-controlled in vivo studies):
ICAM-1Platelets
Endothelial cells
LeukocytesMac-1
Abacavir and myocardial infarction:
Pathogenesis

Approximately 1/3 of the PI-related excess risk
for MI in D:A:D is due to DM, HT, or lipids
Adjusted Model 1 Adjusted Model 2
Relative Rate
(95% CI)P Value
Relative Rate
(95% CI)P Value
Exposure to PIs (per year) 1.16 (1.10-1.23) <0.001 1.10 (1.04-1.18) 0.002
Age (per 5 yr) 1.39 (1.31-1.46) <0.001 1.32 (1.23-1.41) <0.001
Male sex 1.91 (1.28-2.86) 0.002 2.13 (1.29-3.52) 0.003
BMI >30 kg/m2 1.70 (1.08-2.69) 0.02 1.34 (0.77-2.34) 0.31
Family history of CHD 1.56 (1.10-2.23) 0.01 1.40 (0.96-2.05) 0.08
Smoking status
Current 2.83 (2.04-3.93) <0.001 2.92 (2.04-4.18) <0.001
Former 1.65 (1.12-2.42) 0.01 1.63 (1.07-2.48) 0.02
Previous cardiovascular event 4.30 (3.06-6.03) <0.001 4.64 (3.22-6.69) <0.001
Diabetes mellitus - - 1.86 (1.31-2.65) <0.001
Hypertension - - 1.30 (0.99-1.72) 0.06
Total cholesterol (per mmol/L increase) - - 1.26 (1.19-1.35) <0.001
HDL cholesterol (per mmol/L increase) - - 0.72 (0.52-0.99) 0.05
D:A:D Study Group. Clin Infect Dis 2008

Martinez E et al. AIDS 2010
RAL arm in SPIRAL led to total-to-HDL cholesterol
ratio

Fisher M et al. 11th International Congress on Drug Therapy in HIV Infection, Glasgow, 2012
RPV arm in SPIRIT also led to total-to-HDL
cholesterol ratio

Median difference of percent change RAL minus PI/r (95% CI)
Martinez E et al. AIDS 2012
• Generally modest or no significant correlation between changes in biomarkers
and changes in lipids
SPIRAL Biomarkers Sub-study
Switching from PI/r to RAL also decreased CV
biomarkers

Lee F et al. HIV Med 2016
Larger decrease in cholesterol fractions with
statin than with PI/r switch

Lo J et al. Lancet HIV 2015
1- year change in non-calcified plaque volume
in HIV+ randomized to atorvastatin vs placebo

Declining relative risk for myocardial
infarction among HIV+ vs. HIV- persons
Klein DB et al. Clin Infect Dis 2015




![27 Puoti.ppt [Compatibiliteitsmodus]regist2.virology-education.com/2011/9eu/docs/27_Puoti.pdf · 2011. 3. 31. · He opted for ADV+TBD vs. TDF based ART NO No activity in several](https://img.pdfslide.us/doc/110x75/61066e8e2c9a08106d7fa996/27-puotippt-compatibiliteitsmodus-2011-3-31-he-opted-for-advtbd-vs-tdf.jpg)