Embed Size (px)
Citation preview
How to develop a ‘MindBody’ approach to How to develop a ‘MindBody’ approach to physical disorders in medical practice!physical disorders in medical practice!
Brian Broom Brian Broom MBChB, FRACP, MSc(Imm), MNZAPMBChB, FRACP, MSc(Imm), MNZAPConsultant Physician(Clinical Immunology), Psychotherapist, Consultant Physician(Clinical Immunology), Psychotherapist, Department of ImmunologyDepartment of Immunology, Auckland City Hospital., Auckland City Hospital.
Adjunct Professor Adjunct Professor MINDBODY HEALTHCARE Post-Graduate Programme, MINDBODY HEALTHCARE Post-Graduate Programme, Department of PsychotherapyDepartment of Psychotherapy, , AUT University, Auckland, New ZealandAUT University, Auckland, New Zealand
If we desire to be effective as ‘whole person’ If we desire to be effective as ‘whole person’ clinicians there are only three issues!clinicians there are only three issues!
ParadigmParadigm
Attitudes and SkillsAttitudes and Skills
The Clinical FrameworkThe Clinical Framework

Meaning-full disease: How personal experience and meanings initiate and maintain physical illnessMeaning-full disease: How personal experience and meanings initiate and maintain physical illness . . B C Broom (2007) Karnac Books, LondonB C Broom (2007) Karnac Books, London
Somatic Illness and the patient’s other story. A practicalSomatic Illness and the patient’s other story. A practical integrative approach to disease for doctors and psychotherapistsintegrative approach to disease for doctors and psychotherapists. . B C Broom (1997) Free Association Books, B C Broom (1997) Free Association Books, New York/LondonNew York/London
Symbolic Disorders and MindBody Co-Emergence. Symbolic Disorders and MindBody Co-Emergence. A challenge for psychoneuroimmunology.A challenge for psychoneuroimmunology. Broom, B., Booth, R., and Schubert, C. Broom, B., Booth, R., and Schubert, C. EXPLORE: Journal of Science and Healing (IN PRESS)EXPLORE: Journal of Science and Healing (IN PRESS)
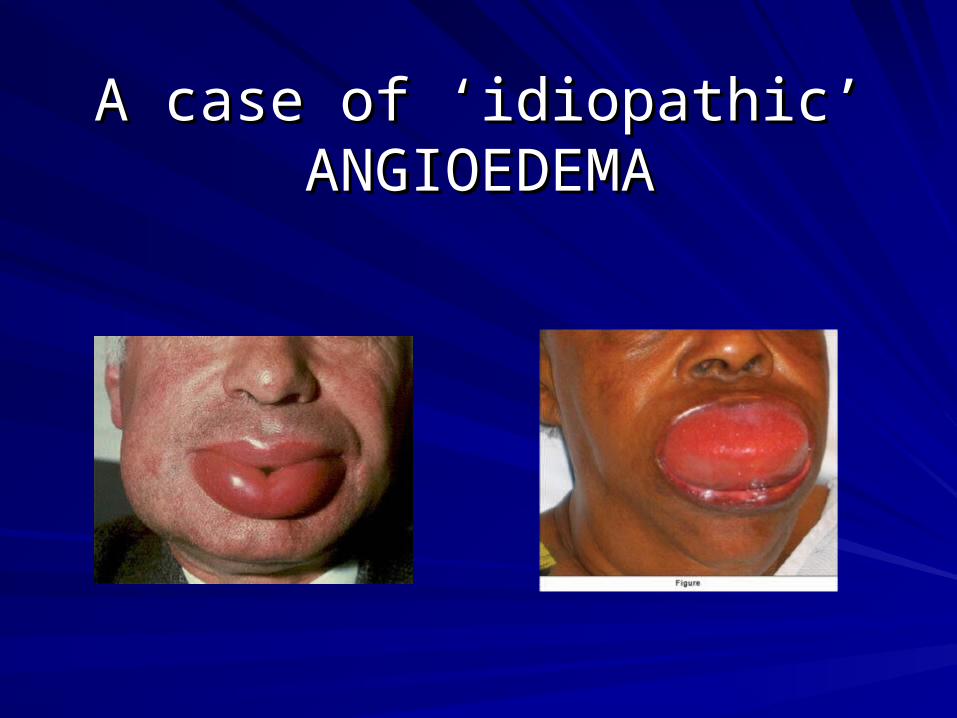
A case of ‘idiopathic’ A case of ‘idiopathic’ ANGIOEDEMAANGIOEDEMA
Clinical ParadigmClinical Paradigm
In my clinical frameworkIn my clinical framework
PersonhoodPersonhood
People are unitivePeople are unitive
Body and mind, physicality and Body and mind, physicality and subjectivity are not dividedsubjectivity are not divided
Body and mind co-emerge SL3Body and mind co-emerge SL3
Personhood core conceptPersonhood core concept
ClinicallyClinically
Avoid Avoid medicalmedical dualism SL1 dualism SL1
Avoid the Avoid the either/oreither/or, body or mind , body or mind defaultdefault position position
Avoid Avoid defaultdefault linearity i.e. body first, linearity i.e. body first, then mindthen mind
Diagnosis is a role-related activity Diagnosis is a role-related activity based on a certain way of seeing SL1based on a certain way of seeing SL1
We can have the diagnosis but not We can have the diagnosis but not have the ‘story’have the ‘story’
Diagnosis takes its place within a Diagnosis takes its place within a wider view of the personwider view of the person
Think person, think Think person, think storystory, think , think diagnosisdiagnosis
Co-emergenceCo-emergence
Assumes unbroken continuity between internal Assumes unbroken continuity between internal body processes and external interpersonal body processes and external interpersonal meanings and influences, meanings and influences, Asserts that disease-related 'internal' bodily Asserts that disease-related 'internal' bodily changes and collateral ‘external’ interpersonal changes and collateral ‘external’ interpersonal and environmental fluxes are mutually and environmental fluxes are mutually contingent and crucial to the development of the contingent and crucial to the development of the disease. disease. Offers an expanded PNI and medical framework Offers an expanded PNI and medical framework
Co-emergence ofCo-emergence of
Physicality and subjectivity Physicality and subjectivity
Body and mindBody and mind
Body and storyBody and story
Illness/disease and symbolIllness/disease and symbol
Illness/disease and meaningIllness/disease and meaning
Illness/disease and ‘story’Illness/disease and ‘story’
Medical dualismMedical dualism
the the widespread assumption in Western widespread assumption in Western healthcare that physical diseases (in healthcare that physical diseases (in particular) can be worked with particular) can be worked with therapeutically without much attention paid therapeutically without much attention paid to mind (subjectivity) factors i.e. that mind to mind (subjectivity) factors i.e. that mind and body are and body are in essencein essence or or functionallyfunctionally separated in some way such that mind separated in some way such that mind factors may be ignored. factors may be ignored.
What is a DIAGNOSIS?What is a DIAGNOSIS?
An observed pattern of dysfunction, recognized by a group An observed pattern of dysfunction, recognized by a group of people who look at patients and dysfunction in the same of people who look at patients and dysfunction in the same way, and in a way that enables them to use agreed upon way, and in a way that enables them to use agreed upon therapies, which are based on that same way of looking. therapies, which are based on that same way of looking.

In practice what does this mean?In practice what does this mean?

Every medical behaviour flows from Every medical behaviour flows from clinician’s paradigm-the first hurdle to a clinician’s paradigm-the first hurdle to a
‘mindbody’ practice‘mindbody’ practice
The first big hurdle is paradigmThe first big hurdle is paradigm
What you say, how you introduce ‘mind’, how you educate, What you say, how you introduce ‘mind’, how you educate, when you educatewhen you educate
We Drs are more the problem than the patientsWe Drs are more the problem than the patients
Patients greatly prefer being treated as persons rather than Patients greatly prefer being treated as persons rather than diagnostic objects (they want diagnosis as well!)diagnostic objects (they want diagnosis as well!)
Residual dualism Residual dualism
All disease is multidimensional and multifactorialAll disease is multidimensional and multifactorial
Disease is a dysfunction in a whole person (system)Disease is a dysfunction in a whole person (system)
The patient’s story is always important—The patient’s story is always important— in some wayin some way
Physicality and subjectivity up front togetherPhysicality and subjectivity up front together
What does this mean in practice?What does this mean in practice?New patients-beginning issuesNew patients-beginning issues
the pre-emptive strikethe pre-emptive strike
declare up front that illness and disease occur in a person, not declare up front that illness and disease occur in a person, not just in a body separated off from the rest of them. just in a body separated off from the rest of them.
I am interested in the whole of them, and I will be asking I am interested in the whole of them, and I will be asking questions about the whole of themquestions about the whole of them
we get unwell for both visible and not so visible reasonswe get unwell for both visible and not so visible reasons
transference or ‘baggage’ from previous encounters: nutter, transference or ‘baggage’ from previous encounters: nutter, hypochondriac, making it up, not realhypochondriac, making it up, not real
hope/investigation/’normal’/pushed awayhope/investigation/’normal’/pushed away
Attitudes and skills Attitudes and skills the ‘fix-it’ mode versus the listening/empathy modethe ‘fix-it’ mode versus the listening/empathy mode
suspending focus, expanding ‘marginal capacity’suspending focus, expanding ‘marginal capacity’
accurate recognition and reflection of storyaccurate recognition and reflection of story
honoring the ‘little’ (you are seeing what ‘is’ already)honoring the ‘little’ (you are seeing what ‘is’ already)
educating about paradigmeducating about paradigm
stories, normalisation, universalisation, self-revelationstories, normalisation, universalisation, self-revelation
the smorgasbord questionthe smorgasbord question
prism metaphorprism metaphor
comfortable with affective intimacycomfortable with affective intimacy
using specialists as contract investigatorsusing specialists as contract investigators
avoiding psychiatrisationavoiding psychiatrisation
The Story in the MacroThe Story in the Micro
(Exploring the Fault-lines)
LISTENING VERY CAREFULLY TOTHE PATIENT’S ACTUAL USE OF LANGUAGE
Believing in the Mind/Body Connections against the Odds.
DerailmentOrganic/functional dichotomies
Self–doubt: haven’t got the skillsFear of medico-legal consequences
Issues of respectHumanistic waiting
When will the patient be ‘ready’?
Discovering the undeniable
The Pursuit of the Particular
Must Go Slowly, and Expect to Find what is Needed in the Little that is Given
Believing in the Mind/Body Connections against the Odds.
Adequate investigation The problem specialist (overinvestigating/or
nothing wrong with you)
Believing in the Mind/Body Connections against the Odds.
Adequate investigation
The problem specialist (overinvestigating/or
nothing wrong with you)
HELPING PATIENTSACCEPT THE M/B
CONNECTIONS
But it is difficult!
“If the therapist has the wit to seeit, the truth is there to be seen inthe first session’(Harry Stack Sullivan--quotedby E. Levenson).
“Nothing certain can be saidabout the nature of truth,except perhaps that it is whatour peers will let us away with”Rorty
“No map includes every detailof the territory that itrepresents, and events thatdon’t make it onto the mapdon’t exist in that map’s worldof meaning.”Freedman and Combs
HELPING PATIENTS ACCEPT THE M/BCONNECTIONS
“bits and pieces”
SupervisionThe power of intuitionAn issue of intimacyThe ‘fix-it’ mentalityThe doctor’s reality
Symbolic DiseasesSymbolic Diseases
Symbolic diseases (SDs) are defined as Symbolic diseases (SDs) are defined as occurring when “occurring when “the organ system involved, the organ system involved, and/or the pathological process, and/or the and/or the pathological process, and/or the clinical phenomenology, appears to be clinical phenomenology, appears to be particularly congruent with, or appropriate to, the particularly congruent with, or appropriate to, the patient’s subjective meanings or “story”, as patient’s subjective meanings or “story”, as ascertained from the patient’s language, life ascertained from the patient’s language, life history, and behaviours” history, and behaviours” [4]. [4].
HELPING PATIENTS ACCEPT HELPING PATIENTS ACCEPT THE MIND/BODY THE MIND/BODY CONNECTIONSCONNECTIONS
HELPING PATIENTS ACCEPT THE M/BCONNECTIONS
Discovering the undeniable in a waywhich is acceptable
I Believe in Education educating the patient -the Prism Metaphor other patient’s stories normalisation/commonality the pre-emptive strike. The clinician’s ‘story’
Auckland University of Technology Auckland University of Technology Dept of PsychotherapyDept of Psychotherapy
Post-Graduate Program in MindBody HealthcarePost-Graduate Program in MindBody Healthcare
Diploma and MastersDiploma and Masters
Part-time, block course-based, multidisciplinary, open to Part-time, block course-based, multidisciplinary, open to clinicians of all kinds clinicians of all kinds
HELPING PATIENTS ACCEPT THE M/BCONNECTIONS
Believing in the Mind/Body Connections againstthe Odds.
The Disarming CharmerThe Slow Learner
The Sceptical Eroder
HELPING PATIENTS ACCEPT THE M/BCONNECTIONS
Believing in the Mind/Body Connections againstthe Odds.
Either/Or ResiduesIn the patient/client
In meIn my colleagues
HELPING PATIENTS ACCEPT THE M/BCONNECTIONS
Believing in the Mind/Body Connections againstthe Odds.
The courage to keep going
Enduring intense scepticismCoping with being undermined
Financial implications/losing patients