Embed Size (px)
Citation preview

How to Address Tobacco
Disparity and Reduce
Dependence in Substance
Abuse Treatment Facilities
Jill M Williams, MD Director, Division of Addiction Psychiatry
Robert Wood Johnson Medical School

Disclosure
The faculty, Jill Williams, MD, has received grant funding from Pfizer, Inc. in the past
two years. Pfizer, Inc manufactures chantix. Dr. Williams will be discussing chantix
in her presentation.
The following people have no relevant financial, professional or personal
relationships to disclose:
CME/CNE Program Planner(s):
Robert Cohen, MD (CME Programs)
Marsha Marecki, EdD, WHNP-BC (CNE Programs)
Melanie Steilen, RN, BSN, ACRN (CNE Programs)
CME/CNE Program Reviewer(s):
Robert Cohen, MD (CME Programs)
Melanie Steilen, RN, BSN, ACRN (CNE Programs)
There are no commercial supporters of this activity. Accreditation status does not
imply endorsement by NJSNA, CAI, or ANCC of any commercial products or
services.

Housekeeping & Logistics
• Polls
• Live questions
• Typed questions/chat
• Raise hand
• Tech Difficulties
– 1-888-259-8414

IMPORTANT NOTICE
This GotoWebinar/GotoMeeting service
includes a feature that allows audio and any
documents and other materials exchanged or
viewed during the session to be recorded.
By joining this session, you automatically
consent to such recordings.
Please note that any such recordings may be
subject to discovery in the event of litigation.

Introduction/Presenter
Jill M. Williams, MD
Professor of Psychiatry
Director, Division of
Addiction Psychiatry
Rutgers- Robert Wood
Johnson Medical
School
New Brunswick,

Learning Objectives
• Review the high prevalence and consequences of tobacco use in
persons with other addictions.
• Discuss barriers that have prevented substance abuse staff from
addressing tobacco dependence in their clients
• Explain key concepts in brief assessments of tobacco dependence
including level of dependence and motivation to quit.
• Describe how treatment for tobacco dependence is an effective
method for increasing the success of quit attempts and the role a non-
prescriber can have in promoting treatment.
• Review evidence based treatments for tobacco dependence treatment
and how to integrate tobacco dependence treatment into recovery
plans.


Tobacco Use Rates in NJ
Addictions Treatment Settings
NJ ADADS 2001-2002
0
10
20
30
40
50
60
70
80
90
Tobacco Use Rates
US
NJ
Addictions
Residential
Methadone
Outpatient

Smoking Prevalence in
Addiction Treatment
• Review of 40 papers (over 20 years)
• Inpatient, outpatient, methadone programs
• Alcohol and drug treatment
• Median prevalence for a single year 76% (range 65% to 76%)
• Odds of smoking 2.25 times higher in methadone treatment as compared to other outpatient programs (Guydish, Passalacqua, Tajima, Chan, Chun & Bostrom, 2011)

Rationale Not to Treat Tobacco
Dependence in SUD Patients
• Not a real drug
• Fewer consequences / Not as disruptive to patients’ life
• Disruptive to SUD treatment
• Patients don’t want tobacco treatment
• Patients can’t quit smoking successfully
• Jeopardizes recovery from other substances

Not a Real Drug

0
100
200
300
400
500
600
700
800
900
1000
1100
0 1 2 3 4 5 hr
Time After Amphetamine
% o
f B
as
al R
ele
as
e
DA DOPAC HVA
Accumbens AMPHETAMINE
0
100
200
300
400
0 1 2 3 4 5 hr Time After Cocaine
% o
f B
as
al R
ele
as
e
DA DOPAC HVA
Accumbens COCAINE
0
100
150
200
250
0 1 2 3 hr
Time After Nicotine
% o
f B
as
al R
ele
as
e
Accumbens Caudate
NICOTINE
Source: Di Chiara and Imperato
Effects of Drugs on Dopamine Levels

Fewer Consequences; Not Immediate
• More alcoholics die from smoking
related diseases than from alcohol
related diseases
• Synergistic effects of alcohol and tobacco
↑ risk of developing pancreatitis and oral
cancers
• Smoking reduces recovery from cognitive
deficits during alcohol abstinence
Hurt et al, 1996; USDHHS 1982 Durazzo et al, 2007

Disruptive to SUD Treatment
• No increase in irregular discharges when
residential SUD settings went TF(NJ)
• ↑ Clients enrolled in treatment when facility
went TF (Kotz et al, 1993)
• Longer LOS when patients enrolled in smoking
cessation program (Burling et al., 1991).
• No increase in early discharges (Joseph, 1993).
Williams et al, 2005

2001 NJ Integration of Tobacco
Dependence Treatment into
Residential Substance Abuse
Treatment • In 1999, NJ established NJAC 8:42A
• Required residential addictions programs
– To provide tobacco assessment and treatment
– Prohibited tobacco products on the grounds of
facilities.
• Full implementation by Nov 2001.
• The state provided free nicotine patches and
gum to clients in these settings
• UMDNJ training and consultation

Staff shall not use
alcohol, tobacco or illegal
drugs during working
hours or when
representing the
treatment facility.
8:42A-3.5 (b) 1

Advantages of Addressing Tobacco
During Early Substance Recovery
• Structured environment focused on recovery
• Staff and peer support readily available
• Patients may be more motivated, believing this is the best time to quit
• Smoking quit rates in early substance recovery are the same as when treatment is delayed 6 mos (Joseph et al.,2003).
• Financial advantages if clients lack insurance
Joseph et al., 1990; Irving et al., 1994; Sees and Clark, 1993; Saxon et al.,
1997; Seidner et al., 1996; Foulds & Doverty, 2003: Joseph et al., 2002

Did the NJ 2001 implementation of the
Tobacco Provisions of the Licensure Standards result in an increase in premature client
discharges?
• NO
• There was no increase in irregular discharges.
• Rates were not statistically significant from discharge rates in previous years.
• The rates of irregular discharge were also not statistically significant between smokers and non-smokers.
Williams et al, 2005

Figure 1: Percent of New Jersey residential addictions treatment agencies reporting
tobacco-related activities before (1999) and after (2002) statewide Tobacco Licensure
Standards (n=30)
37
50
27
17
50
40
9097
87
67
87
73
0
20
40
60
80
100
Tob
acco
Ass
essm
ent
Tob
acco
Cou
nselin
g
NRT A
vaila
ble
Tob
. in D
isch
arge
Pla
n
Staff T
rain
ed o
n Tob
acco
Wri
tten
Sta
ff T
ob. P
olic
y
%
rep
orti
ng
acti
vit
y
1999
2002
Foulds et al., 2006
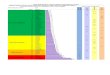
NJ Policy Resulted in Increased
Tobacco Treatment

03,5007,000
10,50014,00017,50021,00024,50028,00031,50035,000A
ug
No
v
Fe
b
Ma
y
Au
g
No
v
Fe
b
Ma
y
Au
g
No
v
Time Period
# A
dm
iss
ion
s
Total For All Major Program Types
August 2007 to December 2009
No Reduction in Program Admissions
Total For All Major Program Types OASAS NY
Tobacco-Free Implementation - July 2008
www.oasas.ny.gov

Patients Resistant to Tobacco
Treatment
• Two-thirds of smokers wanted to stop (41%) or cut down on tobacco use (24%) at time of admission to residential addictions treatment Williams et al, 2005
• Patients highly interested in treatment and believe inpt treatment is best time Orleans & Hutchinson, 1993; Shoptaw et al., 2002; Richter et al, 2001;
Nahvi, et al, 2006; Sees & Clark, 1993; Clemmey et al, 1997; Frosch et al, 1998; Clarke et al 2001; Joseph et al., 1990; Saxon et al., 1997; Joseph et al., 2002

Patients with SUD Can’t Quit Smoking
• H/o ETOH Just as likely to
succeed in quitting smoking as
other smokers
• Usual treatments effective
• Smokers learned skills in
recovering from alcohol that
helped them quit smoking
Hughes & Kalman, 2006

Lifetime Quitting
• Smokers with current alcohol
problems, were less likely to
have quit in their lifetime than
smokers with no problems
• ? Fewer quit attempts
Hughes & Kalman, 2006

Jeopardizes Recovery from other
Substances
• Several studies show no adverse effects on abstinence
Bobo et al. 1996, 1998; Hurt et al., 1994; Cornelius et al. 1997, 1999; Prochaska et al. 2004; Lemon et al, 2003; McCarthy et al, 2002; Shoptaw et al., 2002
• Quitting smoking may help with long-term abstinence from alcohol and other drugs

Smoking Cessation Treatment Does Not
Jeopardize Recovery from other Substances
META ANALYSIS OF 19 RANDOMIZED CONTROL
TRIALS WITH INDIVIDUALS IN CURRENT
ADDICTION TREATMENT OR RECOVERY
• SMOKING CESSATION INTERVENTIONS PROVIDED
DURING ADDICTIONS TREATMENT WERE
ASSOCIATED WITH A 25% INCREASED LIKELIHOOD
OF LONG-TERM ABSTINENCE FROM ALCOHOL AND
ILLICIT DRUGS
• SMOKING CESSATION WORKED WELL INITIALLY BUT
WAS DIFFICULT TO SUSTAIN IN THE GROUPS
• IN THE LATER STUDIES WHICH USED NRT’S,
SUCCESS WAS INCREASED
PROCHASKA ET AL JCCP 2004

Smoking cessation in
outpatient SA treatment • Part of CTN, included methadone sites
• N=225 smokers
SC adjunct or treatment-as-usual (TAU)
9 weeks group counseling plus NP
• No difference in SC vs TAU –on rates of retention in SA tx
–abstinence from primary substance
–craving for primary substance.
Reid et al., 2008

Tobacco Treatment Availability
• National survey of 550 OSAT units (2004–2005) – 88% response rate
• 41% offer smoking cessation counseling or pharmacotherapy
• 38% offer individual/group counseling
• 17% provide quit-smoking medication
• More likely : medically oriented, more comprehensive services, recognize the health burden of smoking
Friedmann et al., JSAT 2008

Twelve Steps to Addressing Tobacco within
Addiction Treatment Programs
1. Acknowledge the Challenge to Address the Barriers and Integrate the Solutions
2. Establish a Leadership Group and Make a Commitment to Change
3. Create a Change Plan and Realistic Implementation Timeline
4. Start with easy program and system changes, including tobacco policies
5. Conduct Staff Training
6. Assess and Document in charts nicotine use, dependence, and prior treatments
7. Incorporate Tobacco Issues into all client education curriculum
8. Provide Medications for Nicotine Dependence Treatment
9. Provide treatment and recovery assistance for interested nicotine dependent staff
10. Integrate Motivation-Based Treatments throughout the program
11. Establish ongoing communication with 12-Step Recovery Groups, Professional Colleagues, and Referral Sources about system changes
12. Consider additional Addressing Tobacco Policies, including Smoke-Free Grounds

Assessment
• Level of Nicotine Dependence
• Motivation to Quit • First age smoked
• Years smoked
• Current amount
• Tobacco types (pipes, cigars, smokeless)
• Smokers in household
• Consequences of use- health or other

Tobacco Use Disorder
– withdrawal
– tolerance
– desire or efforts to cut down/ control use
– great time spent in obtaining/using
– reduced occupational, recreational
activities
– use despite problems
– larger amounts consumed than intended
– Craving; strong urges to use
Most tobacco users are addicted (2 or more)
DSM-5

Nicotine
Pharmacology
Pharmacology depends on delivery route
Reaches brain in 10 sec
Arterial levels 6-10x higher than venous
Half-life 2 hours
Metabolized to cotinine in liver

Russell et al., BMJ, 1983

Tobacco Withdrawal
Depressed mood
Insomnia
Irritability, frustration or anger
Anxiety
Difficulty concentrating
Restlessness
Increased appetite or weight gain

Heaviness of Smoking
Index= Measure of Dependence
Number of cigarettes per day (cpd)
AM Time to first cigarette (TTFC)
≤ 30 minutes = moderate
≤ 5 minutes = severe
Heatherton 1991

Smokers in Addiction Treatment are
Moderately to Severely Addicted to
Nicotine
0
5
10
15
20
25
30
35
40
45
50
0-5 min 6-30 min >31
0-5 min
6-30 min
>31
N=1882 smokers in NJ addictions treatment, 2001-2002;
Williams et al., 2005

MORE Nicotine Dependence
and Withdrawal in SUD
• Current, past or lifetime alcohol problems were associated with ↑nicotine dependence
• Smokers with SUD are more likely to report withdrawal symptoms
• Smokers with SUD have ↑likelihood of withdrawal-related discomfort and smoking relapse
Hughes & Kalman, 2006; Weinberger 2010

READINESS to QUIT in SPECIAL POPULATIONS
48%
41%
55%
43%
40%
22%
24%
24%
28%
20%
0% 20% 40% 60% 80% 100%
Methadone Clients
Psych. Inpatients
Depressed Outpatients
General Psych Outpts
General Population
Intend to quit in next 6 mo Intend to quit in next 30 days
* No relationship between psychiatric symptom severity and readiness to quit
Smokers with
mental illness or
addictive
disorders are
just as ready to
quit smoking as
the general
population of
smokers.
Slide Courtesy J Prochaska; Acton 2001; Prochaska 2004; Prochaska
2006; Nahvi 2006

Hard to Quit
Without
Treatment
70% of smokers report wanting to quit someday
Few people quit successfully without treatment
Only 1/3 of quitters (without treatment) remain
abstinent for 2 days
< 5% ultimately successful
on a given quit attempt

Pharmacological Treatment
Rationale
Reduce or eliminate withdrawal
Block reinforcing effects of nicotine
Manage negative mood states
Unlearn smoking behaviors
Cost-effective treatment
Lessen/delay weight gain

First-line Treatments
(FDA Approved)
• Nicotine Replacement
• Bupropion
Zyban/ Wellbutrin
• Varenicline
Chantix

Nicotine Medications
• Not a carcinogen
• Use high enough dose
• Scheduled better than PRN
• Use long enough time period
• Can be combined with bupropion
• Can be combined with each other
• Have almost no contraindications
• Have no drug-drug interactions

Nicotine Replacement • Smokers misinformed about safety/efficacy
• Risk-benefit ratio nicotine > tobacco

NRT for Smokers with Addictions
No reason not to use
Not introducing a “new drug”
Safer nicotine delivery vs. smoking
More patient education
Off-label ?? Longer time
?? Use when continuing to smoke small
amounts

Pharmacological Treatment
Nicotine Replacement Patch
Gum
Lozenge
Inhaler
Nasal Spray
Bupropion
Varenicline

Combination Therapies
Improves abstinence rates
Decreased withdrawal
Well tolerated
Kornitzer 1995

A randomized placebo-controlled clinical trial
of five smoking
cessation pharmacotherapies
• 1504 smokers
• 5 treatments and 5 placebo groups – nicotine lozenge
– nicotine patch
– bupropion SR
– nicotine patch + nicotine lozenge
– bupropion + nicotine lozenge
Piper et al., 2009

Odds Ratio for 6 months after Quit
Date
0
0.5
1
1.5
2
2.5
Loz
NP
Bup
Bup + Loz
NP + Loz
NP + Loz greatest time to relapse
all monotherapies > placebo

Smoking with NRT
• Relatively safe
• Harm Reduction
• Less reinforcing effects
• Withdrawal of treatment=punishment
for relapsing

Cut Down To Quit (CDTQ)
• NRT previously licensed in the UK for
quitting have recently been granted a new
licensed indication called ‘cut down to quit’
(CDTQ).
• Aims at smokers unwilling or unable to
stop smoking in the short term
• Gradually to cut down smoking over an
extended period while taking NRT
• Gum and inhaler
Wang et al., 2008

NRT Assisted Reduction
• 7 Smoking Reduction trials (four Nicotine gum, two inhaler, and one free choice NRT)
• 2767 smokers
• NRT for 6-18 months
• 6.75% of smokers receiving NRT had sustained abstinence for six months, 2X more those receiving placebo
• No statistically significant differences in adverse events and discontinuation because of adverse events
except nausea →more with NRT
• Whether smokers are motivated to reduce then quit or simply motivated to reduce may make little difference to the efficacy of NRT for smoking cessation Moore et al., BMJ, 2009

First-line Treatments
(FDA Approved)
• Nicotine Replacement
• Bupropion
Zyban/ Wellbutrin
• Varenicline
Chantix

Bupropion SR
• Start 150mg/day to dose of 150mg bid
• Nonsedating, activating antidepressant with effects on NE and DA systems
• Start 10-14 days prior to quit date
• Side effects- headache, insomnia
• Contraindicated in h/o seizures or bulemia
• Noncompetitive nicotinic receptor antagonist
Slemmer 2000

Varenicline Summary
• Selective a4B2 nicotinic
receptor partial agonist
• No drug-drug interactions
• Precaution in ESRD
• Dosed with food to reduce
nausea

Varenicline: a selective a4B2
nicotinic receptor partial agonist
Mesolimbic
system
Nucleus
accumbens
Ventral tegmental
area
Dopamine

Varenicline
Partial Agonist
• Partially stimulates receptor
• Some DA release at NAcc
• Prevents withdrawal
“Antagonist”
• Blocks nicotine binding a4B2
**Don’t use as combination


Varenicline vs Nicotine Patch
• Open label (N=776)
• 12 Week varenicline vs 10 week NP
• Nausea: varenicline (37%) > NP (10%)
Aubin et al., 2008 Continuous Abstinence, Week 9-12 Week 52

Varenicline and Alcohol
• No DB-PC studies
• Open-label, > 6 months sober
– 31% quit at 12 weeks (7dPP)
– No serious adverse events
• Short-term lab studies of heavy drinkers
– Smoked less on varenicline vs. placebo
– Had less alcohol craving and fewer heavy
drinking days on varenicline vs. placebo
• Varenicline reduces alcohol intake in rats
Hays 2011; McKee 2009; Fucito
2011

Varenicline Labeling Updates
Warning (Reported with Chantix)
Observe patients for serious
neuropsychiatric symptoms including
changes in behavior, agitation, depressed
mood, suicidal thoughts or behavior
Worsening of preexisting psychiatric
illness
Causal relationship not established
Clinical trials (N>5000; SI rate = placebo)
Sleep disturbance/ vivid dream www.PfizerPRO.com/chantix

Varenicline and Suicide 80,660 smokers prescribed NRT (~63k), varenicline (~11k), and
bupropion (~6k); UK, primary care
Compared with NRT, the hazard ratio for self harm among people prescribed varenicline was 1.12 (95% CI 0.67 to 1.88), and it was 1.17 (0.59 to 2.32) for people prescribed bupropion.
No clear evidence that varenicline was associated with an increased risk of fatal (n=2) or non-fatal (n=166) self harm
No evidence that varenicline was associated with an increased risk of depression or suicidal thoughts
Gunnell et al., 2009; BMJ

Case Report Data
• Review of FDA's Adverse Event
Reporting System (AERS)
• Case reports for varenicline, bupropion
and NRT
• Suicidal/self-injurious behavior or
depression highest in varenicline group
• Not controlled, randomized studies
• Re-report of same case report data
Moore et al., 2011

Bupropion Adverse Effects French dataset: 700,000 patients
1682 cases of adverse reactions were reported
~ 1/3 of these involved SAR
Allergic reactions (31.2%), including angioedema and serum sickness-like reactions.
Serious neurological reactions were frequent (22.5%), mostly comprising seizures; almost half of these patients had history seizures or other risk factors.
Serious neuropsychiatric adverse events reported (17.3%), suicide attempts/suicides were a cause for concern, although risk factors (history of depression, suicide attempts, etc.) were described for 66% of patients experiencing these events.
Beyens et al., 2008

Medication Interactions with
Tobacco Smoke
• Smoking ↑ P450 enzyme system
• Polynuclear aromatic
hydrocarbons (tar)
• ↑ 1A2 isoenzyme activity
• Smoking ↑ metabolism of meds
– ↓ serum levels
• Smokers on higher medication
doses

Drugs Reduced by Smoking
Antipsychotics
Olanzapine Clozapine
Fluphenazine, Haloperidol, Chlorpromazine
Antidepressants Amitriptyline, doxepin, clomipramine, desipramine,
imipramine, fluvoxemine
Others Caffeine, theophylline, warfarin, propranolol,
acetominophen
Desai et al., 2001; Zevin & Benowitz 1999

Quitting Smoking
• Risk for medication
toxicity
• May ↑ levels acutely
• Consider dose
adjustment
• Clozapine toxicity
– Seizures
• Reduce caffeine
intake
• Nicotine (or
NRT) Does Not
Change
Medication Levels
• Nicotine
metabolized by
CYP2A6

Conclusions
• Medications should be used for all smokers
• No contraindication to NRT for outpatient smokers with other addictions
• Bupropion advantage in depressed smokers- two indications
• Varenicline more effective than other medication treatments
• Combinations more effective

Questions?