Embed Size (px)
Citation preview

ARTICLE IN PRESS
0277-9536/$ - se
doi:10.1016/j.so
�Correspondfax: +618 6304
E-mail addr
Y.Hauck@exch
J.Fenwick@em
Social Science & Medicine 63 (2006) 64–75
www.elsevier.com/locate/socscimed
How social context impacts on women’s fears of childbirth:A Western Australian example
Colleen Fishera,�, Yvonne Hauckb, Jenny Fenwickb
aEdith Cowan University, Joondalup, WA AustraliabCurtin University of Technology
Available online 14 February 2006
Abstract
This paper addresses the limited sociological understanding of the phenomena of childbirth fear using data from a
qualitative research project conducted in Western Australia. This qualitative study used an exploratory descriptive design,
with 22 women identified as being fearful of birth participating in an in-depth interview. Data analysis using the method of
constant comparison revealed that social context, explored within the framework of the medicalisation of childbirth, and
the intervening circumstances in which the women gave birth, impacted on how and why they experienced fear. As such,
this paper argues that fear of childbirth has social as well as personal dimensions and is both a prospective and
retrospective phenomena.
The analysis identified prospective fear as both social and personal. The social dimensions were labelled as ‘fear of the
unknown’, ‘horror stories’ and ‘general fear for the well-being of the baby’. Personal dimensions included the ‘fear of pain’,
‘losing control and disempowerment’ and ‘uniqueness of each birth’. Retrospective fear was exclusively personal and was
clustered around the themes of ‘previous horror birth’ and ‘speed of birth’. The analysis also revealed two central factors
that mediated against childbirth fear: positive relationships formed with midwives, and the support women received from
their informal network. Understanding and unpacking the dimensions of women’s childbirth fear, and understanding the
nature of relationships that mediate women’s fear, provides health care professionals with information on which to base
potential intervention strategies and support women in ways that lessen rather than heighten their fear.
r 2005 Elsevier Ltd. All rights reserved.
Keywords: Australia; Childbirth; Women’s fear; Medicalisation
Introduction
Pregnancy and childbirth are normal physiologi-cal processes and significant social and emotionalevents in the life of any woman and her family. In
e front matter r 2005 Elsevier Ltd. All rights reserved
cscimed.2005.11.065
ing author. Tel.: +61 8 6304 5639;
5449.
esses: [email protected] (C. Fisher),
ange.curtin.edu.au (Y. Hauck),
ail.curtin.edu.au (J. Fenwick).
today’s developed world the experience of child-birth, even though inherently unpredictable (Bewley& Cockburn, 2002), should be a positive life-affirming event associated with minimal risk of anadverse outcome (Geissbuehler & Eberhard, 2002;Searle, 1996). Research demonstrates, however, thatthere is a high prevalence of fear associated withchildbirth (Zar, Wijma, & Wijma, 2001). Althoughup to 80% of women identify common concerns(Saisto & Halmesmaki, 2003), just over 20%
.

ARTICLE IN PRESSC. Fisher et al. / Social Science & Medicine 63 (2006) 64–75 65
(Hofberg & Ward, 2003; Zar et al., 2001) reportmore specific or intense worries with between6–10% of women experiencing severe fear of labourand birth that is dysfunctional or disabling (Wijma,2003).
In Western societies birth ‘fear’ has been asso-ciated with pregnancy complications, increasingchildbirth interventions, emergency and electiveCaesarean Section (CS), postnatal depression(PND), Post Traumatic Stress Disorder (PTSD)and impaired maternal–infant connection (Bewley& Cockburn, 2002; Johnson & Slade, 2002; Ryding,Persson, Onell, & Kvist, 2003). These outcomeshave consequences for a woman’s physical andemotional well-being, for her role as a mother aswell as for her interpersonal parental relationships(Ogrodniczuk, 2004). The importance of nurturingand supporting women’s mental health throughpregnancy is becoming increasingly apparent(Hofberg & Ward, 2003). The most recent Con-fidential Enquiries into Maternal Deaths in theUnited Kingdom (2001) identified suicide as theleading cause of maternal death leaving no doubtthat psychological morbidity in childbearing womenis a significant and pressing issue in the developedworld.
The object of women’s fears
Universally the focus of most childbirth concernsis the well-being of the baby (Searle, 1996). Womencommonly worry about the health of the unbornchild and congenital abnormalities (Szeverenyi,Poka, Hetey, & Torok, 1998). Potential complica-tions that may affect women’s own health and well-being are also rated as concerns (Fava, Grandi, &Michelacchi, 1990). It is also common for women toworry about the biological process of giving birthsuch as the process of labour, the pain of contrac-tions and possible medical interventions (Melender,2002b; Ryding, Wijma, & Wijma, 1997; Sjogren,1998).
When summarising women’s childbirth fears,Wijma, Alehagenm, and Wijma (2002) note thatpersonal and external conditions play a major rolein generating fears. Personal conditions are areflection of women’s anxieties about maintaininga sense of personal control. In a study of 100Scandinavian women identified as suffering intensechildbirth fear, over 65% were worried about theirperformance in labour and their own body’s abilityto birth (Saisto & Halmesmaki, 2003). These
findings are confirmed by Soet, Brack, and Dilorio(2003) who reported that women commonly werefearful of not having the strength to cope withlabour and birth, not being able to breathe and/orpush during the actual birth process and feelingpowerless.
External conditions that generate childbirth fearsoften relate to the context or environment in whichwomen birth and the interactions and actionsshared with health care professionals. Saisto andHalmesmaki (2003), for example, found the mostcommon reason for fear was lack of trust in theobstetric staff (73%). Other studies have identifiedsimilar results. Melender (2002a) for example, in anexploration of 329 antenatal women’s fears revealedthat many Finnish women were worried aboutunfriendly staff, being left alone, appearing silly andnot being involved in decisions. These studies werequantitative and used structured questionnaires. Assuch the voices of women are not heard.
Australian context
In Australia there has been relatively little workspecifically addressing childbirth fear. Searle (1996)conducted a cross-sectional study of 376 postnatalwomen in a major teaching hospital in Melbourne.This study explored women’s beliefs and fears aboutpregnancy and birthing outcomes, through theirperceptions and use of routine antenatal screening.Fifty-five per cent of women were found to havecommon anxieties, and as suggested by the interna-tional literature, these related to the health and well-being of the baby. In this study unlike others(Farrant, 1985; Lupton, 1995) Searle found thatwomen seek normality but worry about having anabnormality detected. In her discussion Searlepurported that women’s concern over detection isconsistent with the medical model of pregnancy. Shewent on to say that the medical model plays adominant role in influencing the perceptions ofrecipients of antenatal care. Searle also concludedthat women’s perceptions of their own risk ofhaving a baby with an abnormality was out ofproportion to actual risk, and to their perception towhat the actual risk was.
More recently Australian researchers such asGamble, Creedy, and Moyle (2004) have investi-gated the relatively new area of PTSD in thechildbearing population. There appears to be ahigh percentage of childbearing women at riskof developing psychological trauma symptoms

ARTICLE IN PRESSC. Fisher et al. / Social Science & Medicine 63 (2006) 64–7566
(Gamble et al., 2004) in addition to the increasingprevalence of PND in the Australian birthingpopulation (Austin, 2004). These are importantconcepts given one of the most common causes ofchildbirth fear is that generated by a previousnegative or traumatic birth experience.
Providing an explanatory framework—
medicalisation—the social context of childbirth
What is largely absent from the research aroundchildbirth fear, however, is a contextualisation ofchildbirth, i.e., the social context and interveningcircumstances in which women give birth. Thispaper argues that social context influences not onlyhow women construct and understand childbirth asan abstract ‘event’ in the lives of all women, but thisconstruction and understanding positions them in adynamic relationship vis-a-vis childbirth in terms ofhow they experience it on an individual level.
As childbirth in Western countries, such asAustralia, becomes more medicalised, the ‘author-itative knowledge’ of women regarding childbirthhas declined and abetted their deskilling andisolation from what was once ‘women’s business’.In many societies this has also led to the margin-alisation of midwifery, which traditionally sup-ported and guided women through childbirth(Stein & Inhorn, 2002). According to Wagner(2000) medicalisation of childbirth has dehumanisedits potential as a deeply significant life event forwomen. Biomedical specialists are exerting a greaterdegree of social control, as well as ever-increasingbiomedical instrumentation, over what was onceviewed in most societies as a woman-centred, non-medical event (Stein & Inhorn, 2002). The con-sequences of medicalised childbirth extend beyondthe individual experiences of individual women tothe broader issue of social relations. That is, theynot only affect an individual woman’s image ofherself, but importantly, tend to generate feelings ofincompetence in all women (De Koninck, 1998).
The construction of childbirth as ‘uncontrollable’,‘unknown’, or ‘threatening’ (Wijma, Wijma, & Zar,1998) provides an intervention point for medicalprofessionals and medical technology that suppo-sedly transforms the uncontrollable natural processof birth into a relatively predictable and control-lable technological phenomenon. This constructalso reinforces Western society’s fundamental be-liefs about the superiority of technology over nature(Davis-Floyd, 1992). Medical management of birth,
however, decreases the control experienced by thebirthing woman, creates a power imbalance betweenthe woman and the attending health care profes-sionals and may alienate the woman from apotentially empowering experience (Fox & Worts,1999). Authors such as Wijma et al. (2002) andSmith and Ellsworth (1985) argue that thesedimensions create the condition under which fearis generated and becomes an emotional response.
Gaining a better understanding of childbirth fear,within the Australian context, is an importantstrategy for health care professionals if we are toimprove the quality of care afforded women andtheir families during the normal, but significant lifeevent of childbirth as the dominant model ofmaternity care provision is centred on obstetriccare (Lane, 2001).
Aim
This paper presents the results of phase three of astudy designed to describe the childbirth expecta-tions of a cohort of Western Australian women.Specifically, phase three explored in detail thechildbirth experiences of women identified as fearfulof birth. The primary research questions for thisphase of the research were
�
What are the knowledge and attitudes of womenidentified as fearing childbirth either during orafter pregnancy? � What are the factors that shape the experiencesand expectations of women identified as fearfulof childbirth either during or after pregnancy?
Method
This study used an explorative descriptive design.As there were gaps in knowledge in the phenomen-on of childbirth expectations particularly within anAustralian context, it was essential to gain a clearerpicture of this issue utilising qualitative researchmethods.
In phase one, the childbirth expectations of acohort of Western Australian women (n ¼ 202)were explored and described (Fenwick, Hauck,Downie, & Butt, 2005). Phase two built on thiswork and aimed to explore and describe theinfluence of met and unmet childbirth expectationsupon women’s perception of their birthing experi-ence and expectations for subsequent births (Hauck,Fenwick, Downie, & Butt, 2005). The purpose of

ARTICLE IN PRESSC. Fisher et al. / Social Science & Medicine 63 (2006) 64–75 67
phase three, reported in this paper, was to explorethe phenomenon of fear within the childbirthexperience.
Recruitment procedure, selection of participants and
data collection
For the first phase of the study women wererecruited using newspaper advertisements outliningthe purpose of the study. Women who werecurrently pregnant and/or who had birthed withinthe past 12 months were invited to participate in atelephone interview. Two hundred and two women(39 from rural areas of Western Australia and 163from metropolitan Perth) responded to the adver-tisements. Recruitment through newspaper adver-tisements aimed to access a diverse sample ofwomen, and although the metropolitan–rural splitreflected the percentages of metropolitan and ruralbirths in Western Australia annually, (Gee & Green,2004), the sample was skewed to those women witha university qualification (49%) and above averageincome. At the completion of their phase onetelephone interview metropolitan participants wereasked if they would be willing to be involved inindividual in-depth interviews in the future. Allmetropolitan participants (n ¼ 163) provided theirfirst name and telephone number confirming theirwillingness to be contacted again.
For phase three the original telephone transcriptswere scanned for words such as ‘‘afraid, scared,frightening, terrified and petrified’’ to select thosewomen who had specifically mentioned this conceptin their discussion of their childbirth expectations.Twenty-eight potential participants were identified;however, only 22 could be contacted for a furtherinterview. All women contacted agreed to partici-pate in a second telephone interview, which wasconducted at a time convenient to them. Thewomen’s ages ranged from 24 to 36 years with amean of 31 years. Half of the women report a familyincome over AUD60,000 which is above thenational average of AUD39,000 (Australian Bureauof Statistics, 2004) and 13 (59%) had a universityeducation. These demographics are a reflection ofthe original sample of 202 women. Eight womenwere primiparas and 14 were multiparas andbetween them they had experienced a total of 35births. Three women were pregnant at the time ofthe interview.
At the commencement of the interview the secondauthor reminded women what they had said in their
original telephone interview between 8 and 10months earlier, using actual quotes. Participantswere then asked if they could elaborate on what fearor being scared/afraid meant to them, how this fearoriginated and what contributed to the fear. Activelistening skills were used to encourage the women toexplain and expand on the concept of fear inchildbirth. The interviews were audio-taped andranged from 30 to 45min.
Data analysis
The interviews were transcribed verbatim andimported into QSR N6 computer-based qualitativedata analysis programme. Data analysis was facili-tated through the use of the method of constantcomparison described by Glaser and Strauss (1967)and Glaser (1978), and operationally refined byLincoln and Guba (1985). As such, each transcriptwas read line by line, and units of meaning identifiedand coded. As data analysis proceeded these units ofmeaning were coded onto major categories ofmeaning. All the categories were then re-examinedand refined. The aim, in refining these categories,was to maximise both internal homogeneity, andexternal heterogeneity. Rigor for the data analysiswas ensured using the criteria recommended bySandelowski (1993).
Ethical approval
Ethical approval for the study was provided bytwo Western Australian universities’ Human Re-search and Ethics Committees. The purpose andbenefits of the interviews were clarified and allparticipants gave verbal consent. Contact details ofthe research team were offered to each participant.Confidentiality of information was ensured and alldata in the study aggregated to ensure participantswere not easily identified.
Findings and discussion
Results from this study suggest that the experi-ence of fear in childbirth for women is multi-layeredand complex. Childbirth takes place within asociocultural and sociopolitical context and thiscontext, we argue, inevitably impacts on the ways inwhich women approach childbirth initially and re-approach it subsequently. Context also impacts howand why women experience fear. As such, fear inchildbirth has social as well as personal dimensions.

ARTICLE IN PRESSC. Fisher et al. / Social Science & Medicine 63 (2006) 64–7568
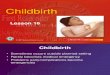
Despite the complex and often overlappingnature of how women experience fear in childbirth,for the sake of clarity and despite its artificiality, thefindings of this research are reported in terms of twooverarching themes—‘prospective fear’ and ‘retro-spective fear’ and the dimensions that constitutethese themes (Fig. 1). ‘Mediating factors’ thatimpact positively on women’s experiences are alsodiscussed. Quotations from the findings to illustratekey points will be presented with the code numberallocated to the 22 participants interviewed(P1–P22).
Prospective fear
Prospective fear has both social and personaldimensions. Social dimensions are reported as ‘fearof the unknown’ ‘horror stories’, and ‘general fearfor the well-being of the baby’. Personal dimensionsof prospective fear are reported as ‘fear of pain’‘losing control and disempowerment’ and ‘unique-ness of each birth’. Despite what might beconsidered ‘common sense’ understandings, pro-spective fear related not only to women who are togive birth for the first time but also to women whoare giving birth for a second, third or more time—manifest through women’s understanding of the‘uniqueness of each birth’. Hence, markers and anypositive experiences from previous births are oftenrendered mute.
Social dimensions of prospective fear
The social dimension of prospective fear is a tri-dimensional construct. Firstly, it incorporates ‘fearof the unknown’, which refers to women’s disen-franchisement from the birthing experience. Sec-ondly, ‘horror stories’ refers to women hearing
Phenomenon of Childbirth Fear Dimensions oSocial Dimen
• Fear o• Horro• Gener
Prospective fear
Personal Dim• Fear o• Losing• Uniqu
Retrospective fear Personal Dim• Previo• Speed
Fig. 1
stories of horrific birthing experiences. The currencythat these stories hold concerned women, especiallyfirst time mothers. The last social dimensionincorporates many mothers’ concerns for the wellbeing of their unborn baby.
Fear of the unknown. ‘Fear of the unknown’ was acommon theme running throughout the data. Aschildbirth constitutes a major event in the lives ofwomen (and their partners), then this is notsurprising—particularly in the event of a first timemother. ‘‘Well I was certainly afraid before my firstbaby because I didn’t know what to expect. I thinkmost women would be really’’. (P11).‘Fear of the unknown’, however, has more far-
reaching implications for women. The eventssurrounding childbirth in Western countries, in-cluding Australia today have, notwithstanding theactive involvement of women in securing theavailability of medical interventions during child-birth (De Koninck, 1998; Morgan, 1998), becomehighly medicalised. The consequences of medica-lised childbirth extend beyond the individual ex-periences of individual women. As can be seen fromParticipant (P5), below, many women have becomedisenfranchised from an understanding of child-birth. Even when they are approaching childbirththemselves, they do not have the ‘cultural store’ ofknowledge that allows them to know which ques-tions they should be asking, often resulting infeelings of incompetence.
you can’t possibly know what it’s [childbirth]going to be like. ‘‘How can I be ready when Idon’t know what it is I’ve got to be ready for?’’When you go to ante-natal classes and people
f Childbirth Fearsion f unknown r birth stories al fear for wellbeing of the baby ension
f pain control and disempowerment
eness of each birth
ension us horror birth of birth
.

ARTICLE IN PRESSC. Fisher et al. / Social Science & Medicine 63 (2006) 64–75 69
say, ‘‘have you got any questions’’? y if I onlyknew what I wanted to ask. (P5)
Not only does medicalisation of childbirth, withits removal from the home and re-location tomedical institutions, mystify childbirth, it renderswhat would, under other circumstances be consid-ered a reputable source of information, problematic.For example, one participant, on seeing childbirthon a video at antenatal classes, was abhorred at itsreality:
I can remember being absolutely horrified by thevideo [at antenatal classes] and just walking outgoing, ‘‘That is just disgusting, I’m not doingthat.’’ It was actually seeing the video I think[that made me fearful]. It was pretty awful. (P19)
In an attempt to mediate their fears aboutchildbirth, many women attempted to give child-birth a concrete meaning in their lives. That is,women often tried to reconcile the unknown(childbirth) with something known and familiar.For example one woman stated: ‘‘I’m scared offlying too but I just try and keep it out of my mindbecause you know that you’ve got to do it’’. (P15)
Despite being disenfranchised from childbirth,many women still acutely felt that they weresubjected to social expectations that women‘should’ be able to give birth with their bodiesdesigned for just such a purpose. The expectationsthat ‘women have been doing this for generations’could act as a positive reinforcement for women andgive them encouragement to ‘labour on’ as was thecase for this woman: ‘‘It’s [giving birth] quite anachievementyand I thought, ‘‘women have beendoing this for thousands of years without thosethings [medical interventions]; if they could do it socould I’’. (P2)
Alternatively, expectations about women’s abilityto give birth placed the ‘bar too high’ for somewomen and they felt inadequate resulting inheightened fear: ‘‘Women do it [give birth] all thetime. Why couldn’t I? To react in that way, tototally lose it, it’s not the norm is it’’? (P22)
Lowe’s (2000) work on self-efficacy and child-birth fear supports these findings. In an analysis of280 predominately white, well educated middle classpregnant women’s responses to fear, Lowe foundthat women who reported high levels of fear lookedto others to make decisions about their health(external health locus of control) and had signifi-cantly lower levels of self-esteem. Lowe concluded
that women evaluate their capabilities to cope withdifferent realities and make decisions accordingly.In terms of childbirth this means that if a womanperceives that birth is too hard and unachievablethen she is likely to behave in a manner thatreinforces this reality.
Horror stories. Horror stories held great currencyamong the women in this study with many first timemothers, in particular, having been exposed to suchstories. ‘‘Well I think the biggest thing is being a firsttime mum, a lot of people choose to be brutallyhonest about childbirth and they tell you all thehorror stories, the ones you don’t want to hear’’.(P8)
Disenfranchisement from childbirth, we argueallows these stories to flourish. This perhapsexplains Hoerger and Howard’s (1995) assertionthat many women become passive recipients ofchildbirth information. Within a context of limited‘culturally stored knowledge’ of childbirth womendo not seek alternatives or investigate issues, whichcan affect their decision-making. This is aided bythe construction of childbirth as ‘hazardous’ and‘uncontrollable’ and so, ripe for medical interven-tion. If a woman is anxious and fearful she is muchmore likely to respond to negative messages, behyper-vigilant and appraise something as dangerous(Saisto & Halmesmaki, 2003).
General fear for the well-being of the baby. Thechildbirth fears of many women extended beyondtheir own health and well-being to that of theirunborn baby. ‘‘Well the major fear for me wasytheactual fear of baby dying’’. (P21) Another womanexpressed her concerns as: ‘‘You’ve got this littleperson in your body inside you and you’re thinking,‘‘Their whole survival depends on your innerstrength and your ability to get them out as quicklyas possible’’. (P8)
The health and well-being of a baby is an intrinsic‘good’ and as such, the concern for this cannotreasonably be called into question. What could beargued, however, is that as more and more domainsof life become medicalised, they become increas-ingly camouflaged as apolitical (De Koninck, 1998).As a result, the construction of the medicalisation ofchildbirth as a benevolent process spreads. Theassociated personal disciplinary practices (Foucault,1973, 1979) that expectant mothers undertakeand importantly, believe they have to undertake(from adhering to diet and exercise guidelines to

ARTICLE IN PRESSC. Fisher et al. / Social Science & Medicine 63 (2006) 64–7570
monitoring their body’s performance during child-birth with respect to delivering a healthy baby)disempowers them and invokes fear concerns for thewell-being of their unborn baby. This phenomenon isneither new nor specifically Western. Internationally,rules exist either through beliefs, food taboos, or thelike. The difference in Western countries includingAustralia lies in the nature of the expertise (medical),its scope and how it is exercised (most notablythrough technology) (De Koninck & Parizeau, 1991).
Personal dimension of prospective fear
The personal dimension of prospective feardescribes how women feel they, as individuals, arelikely to react to the birthing experience. Itincorporates fear of pain, fear of losing control ofboth their physical bodies and their emotions and,women’s feelings of disempowerment during birth.The final personal dimension of prospective fear iswomen’s own knowledge and understanding of theuniqueness of each birth.
Fear of pain. Data from this study suggest that ifwomen are fearful of childbirth, then ‘fear of pain’ isalmost universal. ‘‘To me it was frightening, ‘‘Can Ihandle this? yCan I cope with the pains?’’ (P8)
Rather than being a continuum of experience,fear of pain in childbirth appears to be fragmentedinto two distinct parts in the women’s narratives.Some, like the participant referred to in the aboveparagraph, feared pain during contractions whilstothers feared the experience of pain whilst pushingthe baby out:
you hear people talking about the sensation ofhow awful the whole pushing bit is and how it’sthe most painful thing you can ever experienceand you think, yhow am I going to go withthat? (P13)
Fear of pain evident among women in this study isechoed in the literature. It could be argued that,because pain is such a common experience duringchildbirth, it should represent a common bondamong women (Robertson, 2004). Rather, bolsteredby the perception that pain is a symptom of diseaseand illness, pain in childbirth is often seen as anaffliction women must bear as the price for bearingchildren and, consequently, of no value: an evil to becured by modern treatments and technology. In themidwifery literature such beliefs and assumptionsabout pain are said to give rise to the ‘pain reliefparadigm’, which is in direct contrast to an approach,
referred to as ‘working with pain’. The latterparadigm acknowledges the important role of painin the physiology of normal labour and the woman’sexperience of birth (Leap & Anderson, 2004, p. 34).
Interestingly, Hofberg and Ward (2003) note thataccess to analgesia during labour does not necessa-rily improve a woman’s perception of the experienceof pain. Similarly, Wagner (2000) argues that thecare a woman receives when she goes to a hospitalto give birth markedly affects the pain she willreportedly experience. Wagner argues that labourpain significantly increases when labouring in anunfamiliar place, being surrounded by unfamiliarpeople, having unfamiliar procedures done, beingleft unattended during labour, being put in ahorizontal position, not being allowed to walkabout freely, having the membranes rupturedartificially and by having labour induced oraugmented with drugs: all hallmarks of medicalisedchildbirth in Western countries such as Australia.
Losing control and disempowerment. Loss of controland disempowerment came through strongly as afear for many of the women in the study. Womenwere fearful of losing control of their physicalbodies: ‘‘me tearing, that I think was a very scarythought’’. (P17) Another woman expressed similarconcerns: ‘‘You lose total control. There’s nothingelse that happens in your life that you have nocontrol as such over’’. (P22)
Loss of control extended to emotions as ex-pressed by the following woman. ‘‘I was reallyworried that I was going to be really nasty tosomeone and really demanding and shouting andcarrying on’’. (P1)
Moreover, many women were fearful of beingdisempowered during the birth. This disempower-ment was bi-dimensional. Firstly, women werefearful of being disempowered through use ofmedical interventions, as was the case for thiswoman: ‘‘[I was fearful of] interventions real-lyythat was a big worry. I think every womanthinks the same thing, ‘‘Please don’t let this,happen’’. (P14)
Secondly, women were also fearful that theirbeliefs and values may not coincide with those of themedical staff present at the birth and so, their wishesregarding interventions deemed necessary by med-ical staff, may not be respected.
Will they [the medical staff] be supportive andunderstand if I’m fearful?yYou’re in a situation

ARTICLE IN PRESSC. Fisher et al. / Social Science & Medicine 63 (2006) 64–75 71
where you do have to really relinquish contro-lyto other people. You just have to hope that onthe day they’re the ones you would have chosenanyway. (P7)
Beyond the implications of medical interventionat birth, women were also fearful of their ongoingramifications, physical and emotional. The follow-ing two quotes highlight examples of concerns forthe future. ‘‘My stitches weren’t very good and thathas become more apparent over certain situationswhen you’re having intercourse and stuff like that’’.(P12)
I [was] afraid of the implications of it [medicalintervention] and what could happen, the lack ofcontrol, being unable to move afterwards, anypotential injury from the anaestheticythat’s mymain thing [fear]. (P16)
Uniqueness of each birth. Despite many womenhaving a ‘textbook’ or generally positive experiencewith a previous delivery, some women approachingtheir next birth still held prospective fear. We arguethis is due, in part, to the medicalisation ofchildbirth, which constructs childbirth as ‘unpre-dictable’, ‘uncontrollable’ ‘hazardous’ and a ‘med-ical event’. It is also due to the belief of the womenthat every delivery is unique: ‘‘I had a great birthexperience but then there are thousands of womenwho have horrific birth experiences. My next onemight be totally different’’. (P9) Another motherequated this concern to luck being a limitedresource: ‘‘I had had a pretty good experience lasttime [I gave birth] and can you win lotto twice orwill this time be really horrendous with interventionand stuff like that? That’s my fear this time’’. (P3)
Retrospective fear
Unlike ‘Prospective Fear’, which had both socialand personal dimensions, ‘Retrospective Fear’ isexclusively personal. In this study, retrospective fearwas clustered around the themes of ‘previous horrorbirth’ (either natural or CS) and ‘speed of birth’being either too fast or too slow.
Previous horror birth
Women’s previous experiences of birth, if theywere negative or harrowing, inevitably induced fearin the women for future births.
I’d had a traumatic birth with my son and I wasfrightened that that was going to be repeated andas it was coming closer to my daughter [secondchild] being born, the fear increased and in-creased and I was petrified. I really thought thatthe same sort of things (sic) were going tohappen. (P10)
Reflecting on a very difficult vaginal delivery, fearof future vaginal deliveries is evident in thefollowing quote. ‘‘If the doctors had said to me,‘‘No I think let’s have a try of natural,’’ I would bevery scared’’. (P21)
In cases where women had experienced a previousnegative birth, they continued to experience fearwith subsequent births. This finding supports thecurrent clinical literature (Saisto, Ylikorkala, &Halmesmaki, 1999; Weaver, 2004; Wijma et al.,1998). In essence, women cast their fears from theirprevious delivery onto their upcoming birth. Hof-berg and Ward (2003) argue that this has thepotential to fulfil the ‘vicious cycle’ principle. Feargenerates childbirth intervention, which in turngenerates more fear and increases the likelihood ofa negative birth experience. Although, as discussedabove, women who had experienced a previousgood birth were conscious of the uniqueness of eachbirth, women who experienced a previous horrorbirth did not attach the same uniqueness ofexperience to the event and, so expected futurebirths to be equally as traumatic. This, once againpoints to the dominance of discourses constructingchildbirth as ‘hazardous’ and ‘unpredictable’ andtheir internalisation by women.
Speed of birth
In a similar manner, women whose previouslabours were either very short or very long andarduous, re-cast these fears to future deliveries.Where women experienced a previous long labour,they held fears about enduring a similar experiencewith future births: ‘‘I actually went into labour andhad her forty-four hours later. I was so tired by theend, and that was very scaryyI’m scared again nowfor the next one’’. (P21)
Women who experienced a very quick previousdelivery, on the other hand, were fearful thatensuing deliveries would be even quicker and, hence,were fearful of going into labour in places that theyconsidered ‘inappropriate’.
I certainly was [fearful] with my third because mysecond one had arrived in an hour and a half. My

ARTICLE IN PRESSC. Fisher et al. / Social Science & Medicine 63 (2006) 64–7572
obstetrician kept saying, ‘‘Be very careful thistime, it could be even faster.’’ I kept thinking,‘‘What will I do?’’ (P11)
We would argue that, with childbirth becomingincreasingly medicalised, the ‘appropriate’ and ‘safe’place to deliver a baby is defined as a hospital(Davis-Floyd, 1992; Morgan, 1998; Reibel, 2004). Itis not surprising then that women experience fearwhen faced with the possibility of delivering theirbaby outside this medically constructed safe space.As such, women are confronted with a double set ofsanctions: being constructed as irresponsiblethrough possibly delivering their baby in a poten-tially ‘unsafe’ environment and, secondly, exposingwhat is constructed as a medical event to the outsideworld.
Mediating factors
Results of our research indicate that there are twocentral factors that mediate against fear in child-birth for women: the support provided throughrelationships developed between the women andtheir attending midwives and secondly, supportreceived from within their informal network includ-ing from their partner, family members and closefriends.
Midwives
Findings from this study suggest that supportive,caring, empowering midwives are important inmediating women’s experiences of fear duringchildbirth.
[Childbirth] was a life changing experiencebecause I had some really wonderful people thatlooked after me because I was really scaredyjusthaving these women [midwives] tell me that itwas all going to be okay and they were reallypositivey. Whatever I needed, I goty. If Iwanted music, I got music. (P9)
Moreover, it was not the mere physical presenceof midwives at the birth that was important inmediating women’s fear but it extended to themanner in which they undertook their role andrelayed information, the extent to which theyexuded confidence and the respect they displayedfor the woman. Women’s fear was exacerbated ifmidwives failed to display these qualities. ‘‘One ofthem was just a little bit, not in control. She seemedindecisive and talking aloud of all the things that
needed to be done and not seemingly doinganything’’. (P13) These findings support the workof Hodnett (2002a) who argues that the mostpowerful influence on women’s perception of theirbirthing experience is the attitude and behaviour ofcaregivers.
This study suggests, however, that continuity ofcare from individual midwives throughout thepregnancy and birth provided the most valuablesupport to women and best mediated their experi-ences of fear in childbirth. ‘‘I went through a BirthCentre [which] meant my care was with my midwiferather than a doctor. I wasn’t at all scared because Iwasn’t coming in and seeing these people for thefirst time’’. (P18)
Continuity of midwifery care provided womenwith an opportunity to establish trust and rapport.This not only facilitated joint understanding aboutthe woman’s childbirth expectations but provided a‘safe space’ for the woman to talk about childbirthin general. As a result of this extended sharing ofknowledge and understanding, women regainedsome of the ‘cultural store of knowledge’ aboutchildbirth that they had lost. This in turn mediatedtheir childbirth fears.
Informal networks
In addition to midwives, the presence of othertrusted support people was of paramount impor-tance to the women in terms of mediating theirexperiences of fear as evidenced by the followingquotes: ‘‘My midwife and my husband werefabulous and I was saying, ‘‘Oh I don’t know aboutthis drug free thing, I think I need something.’’ Andmy husband’s saying, ‘‘No, no, you’re fine’’. (P2) Asexpressed by another woman:
My first one [birth]ywas extremely painful andwhilst it [the next birth] was still very painful, Ifelt controlled through the whole thing. Myhusband was very good and [I] felt completelyand utterly in control. What I wantedy-
happened whether it be positions and pain reliefand people actually listening. (P3)
For the women in this study then, their malepartner’s presence in labour was important inmediating their fears. Certainly there is evidence tosuggest that sharing the birth process provides somewomen and men with a heightened level ofconnection as they move from the status of coupleto family (O’Shea, 1998). While the presence of menat birth continues to be debated (Hall & Taylor,

ARTICLE IN PRESSC. Fisher et al. / Social Science & Medicine 63 (2006) 64–75 73
2004) the most important issue is that the womanfeels those sharing her labour and birth will enhancethe experience. The midwifery literature clearlydemonstrates how the presence of unwanted peopleand those with different perceptions of risk and fearcan cause conflict and interfere with the birthprocess (Gaskin, 2002; Hall & Taylor, 2004;Klassen, 2001).
Results of this study are important because thereis very little examination in the social scienceliterature on childbirth about the types of supportgiven to labouring women by midwives, women’sinformal networks and the nature and quality ofthese supports. Rothman (1982) was, perhaps, oneof the earliest authors to suggest a relationshipbetween social support and positive experiences ofchildbirth. She suggested that a woman’s successfultransition to motherhood depended on the receipt ofadequate social support during and after childbirth.Fox and Worts (1999) report similar results in termsof the impact of social support on women’s decisionsto accept medical intervention in childbirth. Theseresearchers suggest that the amount of support awoman receives, and can count on receiving after thebirth of her child, influences decisions she makesduring the course of her labour and delivery, andthus her experience of childbirth. Similarly Campbelland Porter (1997) found that social support before,during and after the birth represented an alternativeto pharmaceuticals to assist women deal with bothfear and pain. Interestingly, in countries wheremidwives are not seen as major care providersduring childbirth, doulas, or women who guide andassist new mothers during childbirth and in thepostnatal period, are providing this support role,particularly in the USA and the United Kingdom. Areview of 15 research trials which involved a total ofalmost 13,000 women found that ongoing care froma female support person such as a doula radicallyreduces a woman’s chance of medical interventionduring childbirth (Hodnett, Gates, Hofmeyr, &Sakala, 2003).
The midwifery literature, however, has beendebating the benefits of continuous support inlabour and continuity of midwifery care over thelast two decades (Halldorsdottir & Karlsdottir,1996; Hodnett, 2002b). In Western countries womenhave stated they want individualised, respectfulconsistent care from maternity caregivers they cantrust. Many, writers, including the well-knownFrench obstetrician Michel Odent (1999), haveargued strongly that the midwife is the best placed
person to share the woman’s childbirth journey.Traditionally seen as a mother figure and aprotector, the midwife is entrusted with helpingthe woman be open and accepting of the uncertaintyof birth. This is best facilitated through theestablishment of a meaningful relationship.
Hall and Taylor (2004) discuss the midwife–mother relationship in terms of a ‘professionalintimacy’ that provides an opportunity for ‘con-necting’ (p. 51). During labour this translates toproviding a ‘secure’ space in which women can feelfreed from the intellectual restraints of the modernworld to give over to the primal birth process.However, as the findings of this study indicate, themidwife must be ‘present’ within the relationship,i.e., the one-to-one relationship is of little benefit tothe woman if the midwife is disengaged from her(Sandell, 1997). ‘Continuity’ then, is not a ‘product’that can be integrated into a service without theconsideration of the individuals providing it (Green,Renfrew, & Curtis, 2000). Downe and McCourt(2004) and Reibel (2004) argue that it is increasinglydifficult for midwives to establish beneficial andsupportive relationships with women within themedicalised context of westernised birthing.
Conclusion
Fear is a normal human reaction that fostersprotection and safety. In relation to childbirth it isprobably sensible to have some level of concern oranxiety as this helps women prepare for childbirth.However if fear becomes all encompassing it can bephysically and emotionally disabling. Although theevidence surrounding fear of labour and birth islimited, what there is suggests that fear may preventand/or interfere with labour, increase perceptions ofpain and contribute to the rising intervention rates.Post-birth, this has implications for how womenreflect on their birth experience and is associated withpoor psychological outcomes and family functioning.
The issue of fear in childbirth, notwithstandingthe research undertaken in Scandinavian countries,is a relatively under-researched area. Whereas muchresearch to date has focused on the personalattributes of individual women in an attempt tolocate the causes and impact of fear in childbirth,our research has examined childbirth within itssocial context.
The research presented in this paper adds tothe existing literature on fear in childbirth intwo important ways. Firstly, it provides deeper

ARTICLE IN PRESSC. Fisher et al. / Social Science & Medicine 63 (2006) 64–7574
understanding of the dimensions of women’s fear.Findings explicate the social and personal dimen-sions of women’s fear and suggest that fear isboth a prospective and retrospective phenomenon.Whereas ‘prospective fear’ is both social andpersonal, ‘retrospective fear’ is almost exclusivelypersonal. Secondly, it highlights the importantnature of relationships between midwives and thewomen, the women and their social networksand the potential both have to mediate, and mitigateagainst, women’s experiences of fear in childbirth.Understanding and unpacking the dimensions ofwomen’s childbirth fear, and understanding thenature of relationships as mediating women’s fearprovides health care professionals with informationon which to base potential intervention strategiesand give direction on how to support women inways that lessen rather than heighten their fear.
It is increasingly apparent that nurturing andsupporting women’s mental health during preg-nancy and childbirth is important in ensuring longterm psychological and social well-being of women,their babies and families. Midwives, other healthcare professionals and policy makers need tounderstand the role medicalisation of birth playsin creating and reinforcing fear of childbirth. Assuch, future research needs to investigate ways inwhich women can regain cultural knowledge ofchildbirth. Clinical practice needs to translate thisinto increasing women’s access to models of carethat provide opportunities to build meaningfulrelationships with midwives within their own localcommunities. Birth is illogical not dangerous. It is asocial phenomena not a medical one.
Acknowledgements
The authors acknowledge the women who parti-cipated in this research. Funding was provided bythe Western Australian Nurses Memorial Charita-ble Trust.
References
Austin, M. P. (2004). Antenatal screening and early intervention
for ‘‘perinatal’’ distress, depression and anxiety: Where to
from here? Archives of Women’s Mental Health, 7(1), 1–6.
Australian Bureau of Statistics (2004). 6302.0. Average weekly
earning, Australia. http://www.abs.gov.au (accessed 23 June
2004).
Bewley, S., & Cockburn, J. (2002). Responding to fear in
childbirth. The Lancet, 359, 2128–2129.
Campbell, R., & Porter, S. (1997). Feminist theory and the
sociology of childbirth: A response to Ellen Annandale and
Judith Clark. Sociology of Health & Illness, 19(3), 348–358.
Confidential Enquiries into Maternal Deaths in the United
Kingdom. (2001). Why mothers die. Fifth report 1997– 1999.
London: RCOG Press.
Davis-Floyd, R. E. (1992). Birth as an American rite of passage.
Berkeley, CA: University of California Press.
De Koninck, M. D. (1998). Reflections on the transfer of
‘‘progress’’: The case of reproduction. In S. Sherwin (Ed.),
The politics of women’s health: Exploring agency and autonomy
(pp. 150–177). Philadelphia: Temple University Press.
De Koninck, M. D., & Parizeau, M. H. (1991). Reflections on
medical sciences and the instrumentalisation of human
reproduction. Health Services, 40(1), 12–30.
Downe, S., & McCourt, C. (2004). From being to becoming:
Reconstructing childbirth knowledges. In S. Downe (Ed.),
Normal childbirth evidence and debate (pp. 3–24). Sydney:
Churchill Livingston.
Farrant, W. (1985). Who’s for amniocentisis? The politics or
prenatal screening. In H. Homans (Ed.), The sexual politics of
reproduction (pp. 96–122). Gower: Hants.
Fava, G. A., Grandi, S. L., & Michelacchi, L. (1990).
Hypochondrial fears and beliefs in pregnancy. Acta Psychia-
try Scandinavia, 82, 70–72.
Fenwick, J., Hauck, Y., Downie, J., & Butt, J. (2005). The
childbirth expectations of a self selected cohort of Western
Australian women. Unpublished manuscript, Curtin Univer-
sity of Technology, Perth.
Fox, B., & Worts, D. (1999). Revisiting the critique of
medicalized childbirth: A contribution top the sociology of
birth. Gender & Society, 13(3), 326–346.
Foucault, M. (1973). The birth of the clinic. New York, NY:
Vintage.
Foucault, M. (1979). Discipline and punish. New York, NY:
Vintage.
Gamble, J., Creedy, D., & Moyle, W. (2004). Counselling
processes to address psychological distress following child-
birth: Perceptions of midwives. Australian Midwifery, 17(3),
16–19.
Gaskin, I. M. (2002). Spiritual midwifery. Cambridge, UK:
Summertown.
Gee, V., & Green, T. (2004). Perinatal statistics in Western
Australia 2003. 21st annual report of the Western Australian
Midwives Notification System. Perth: Department of Health
Western Australia.
Geissbuehler, V., & Eberhard, J. (2002). Fear of childbirth during
pregnancy: A study of more than 8000 pregnant women.
Journal of Psychosomatic and Obsteric Gynecology, 23,
229–235.
Glaser, B. (1978). Theoretical sensitivity. Mill Valley, CA:
Sociology Press.
Glaser, B. G., & Strauss, A. L. (1967). The discovery of grounded
theory: Strategies for qualitative research. Chicago: Aldine.
Green, J. M., Renfrew, M. J., & Curtis, P. A. (2000). Continuity
of carer: What matters to women? A review of the evidence.
Midwifery, 16, 186–196.
Hall, J., & Taylor, M. (2004). Birth and spirituality. In S. Downe
(Ed.), Normal childbirth evidence and debate (pp. 41–56).
Sydney: Churchill Livingston.
Halldorsdottir, S., & Karlsdottir, S. I. (1996). Empowerment or
discouragement: women’s experiences of caring and uncaring

ARTICLE IN PRESSC. Fisher et al. / Social Science & Medicine 63 (2006) 64–75 75
encounters during childbirth. Health Care Women Interna-
tional, 17, 361–379.
Hauck, Y., Fenwick, J., Downie, J., & Butt, J. (2005). The
influence of childbirth expectations upon women’s experi-
ences of their birth experience. Unpublished manuscript,
Curtin University of Technology, Perth.
Hodnett, E. D. (2002a). Pain and women’s satisfaction
with the experience of childbirth: A systematic review.
American Journal of Obstetrics and Gynecology, 186(5),
S160–S172.
Hodnett, E. D. (2002b). Caregiver support for women during
childbirth (Cochrane review). The Cochrane Library Issue 4.
Oxford, Update Software.
Hodnett, E. D., Gates, S., Hofmeyr, G., & Sakala, C. (2003).
Continuous support for women during childbirth (Cochrane
review). The Cochrane Library Issue 4. New York: Wiley.
Hoerger, T. J., & Howard, L. Z. (1995). Search behavior and
choice of physician in the market for pre-natal care. Medical
Care, 33, 332–349.
Hofberg, K., & Ward, M. (2003). Fear of pregnancy and
childbirth. Postgraduate Medical Journal, 79, 505–510.
Johnson, R., & Slade, P. (2002). Does fear of childbirth during
pregnancy predict emergency caesarean section? BJOG: An
International Journal of Obstetrics and Gynaecology, 109,
1213–1221.
Klassen, P. E. (2001). Blessed events: Religion and home birth in
America. Princeton, NJ: Princeton University Press.
Lane, K. (2001). Fear of litigation: The tail that wags the dog.
Paper presented at The Australian Sociological Association
conference, University of Sydney, Sydney Australia, 13–15
December.
Leap, N., & Anderson, T. (2004). The role of pain in normal birth
and the empowerment of women. In S. Downe (Ed.), Normal
childbirth evidence and debate (pp. 25–40). Sydney: Churchill
Livingston.
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry.
Newbury Park: Sage Publications.
Lowe, N. (2000). Self-efficacy for labor and childbirth fears in
nulliparous pregnant women. Journal of Psychosomatic and
Obstetrics and Gynecology, 21, 219–224.
Lupton, D. (1995). Perspectives on power, communication and
the medical encounter: Implications for nursing theory and
practice. Nursing Inquiry, 2(3), 157–163.
Melender, H. (2002a). Experiences of fears associated with
pregnancy and childbirth: A study of 329 pregnant women.
Birth, 29(2), 101–111.
Melender, H. (2002b). Fears and coping strategies associated
with pregnancy and childbirth in Finland. Journal of
Midwifery & Women’s Health, 47(4), 256–263.
Morgan, K. P. (1998). Contested bodies, contested knowledges:
Women, health, and the politics of medicalization. In
S. Sherwin (Ed.), The politics of women’s health: Exploring
agency and autonomy (pp. 83–121). Philadelphia, PA: Temple
University Press.
Odent, M. (1999). The scientification of love. London: Free
Association Books.
Ogrodniczuk, J. S. (2004). Increasing a partner’s understanding
of motherhood significantly reduces postnatal distress and
depression in first time mothers with low self-esteem. Evidence
Based Mental Health, 7(4), 116.
O’Shea, M. (1998). An exploratory study of women’s experience of
childbirth specifically identifying the spiritual dimensions. BSc
Midwifery Studies, King’s College London, The Nightingale
Institute.
Reibel, T. (2004). Normal birth: A thing of the past or the new
future for primary health care? Primary Health Care Research
and Development, 5, 329–337.
Robertson, A. (2004). Counteracting the fear of birth. Retrieved
March 30 2005, from http://www.acegraphics.com.au/arti-
cles/andrea03.html
Rothman, B. K. (1982). Giving birth: Alternatives in childbirth.
Harmondsworth, UK: Penguin.
Ryding, E., Persson, A., Onell, C., & Kvist, L. (2003). An
evaluation of midwives counselling of pregnant women in fear
of childbirth. Acta Obstetricia et Gynecologica Scandinavica,
82, 10–17.
Ryding, E., Wijma, B., & Wijma, K. (1997). Post traumatic stress
disorder after emergency caesarean section. Acta Obstetricia
et Gynecological Scandinavica, 76, 856–861.
Saisto, T., & Halmesmaki, E. (2003). Fear of childbirth: A
neglected dilemma. Acta Obstericia et Gynecological Scandi-
navica, 82, 201–208.
Saisto, T., Ylikorkala, O., & Halmesmaki, E. (1999). Factors
associated with fear of delivery in second pregnancies.
Obstetrics and Gynecology, 94(5), 679–682.
Sandell, J. (1997). Midwives’ burnout and continuity of care.
British Journal of Midwifery, 5, 106–111.
Sandelowski, M. (1993). Rigor or rigor mortis: The problem of
rigor in qualitative research revisited. Advanced Nursing
Science, 16(2), 1–8.
Searle, J. (1996). Fearing the worst: Why do pregnant women feel
‘at risk’? Australian and New Zealand Journal of Obstetrics
and Gynaecology, 36(3), 279–286.
Sjogren, B. (1998). Fear of childbirth and psychosomatic support:
A follow up of 72 women. Acta Obstericia et Gynecological
Scandinavica, 77, 819–825.
Smith, C., & Ellsworth, P. (1985). Patterns of cognitive appraisal in
emotion. Journal of Personal and Social Psychology, 4, 813–838.
Soet, J., Brack, G., & Dilorio, C. (2003). Prevalence and
predictors of women experience of psychological trauma
during childbirth. Birth, 30(1), 36–46.
Stein, E. A., & Inhorn, M. C. (2002). Technologies of pregnancy
and birth. Feminist Studies, 28(3), 611–703.
Szeverenyi, P., Poka, R., Hetey, M., & Torok, Z. (1998).
Contents of childbirth-related fear among couples wishing
the partners presence at delivery. Journal of Psychosomatic
Obstetrics and Gynecology, 19, 38–43.
Wagner, M. (2000). Fish can’t see water: The need to humanise
birth in Australia. Retrieved March 30, 2005, from http://
www.acegraphics.com.au/articles/wagner03.html
Weaver, J. (2004). Caesarean section and maternal choices. Fetal
and Maternal Medicine Review, 15(1), 1–25.
Wijma, K. (2003). Why focus on ‘fear of childbirth’. Journal of
Psychosomatic Obstetrics and Gynecology, 24(3), 141–143.
Wijma, K., Alehagenm, S., & Wijma, B. (2002). Development of
the delivery fear scale. Journal of Psychosomatic Obstetrics
and Gynecology, 23, 97–107.
Wijma, K., Wijma, B., & Zar, M. (1998). Psychometric aspects of
the W-DEQ; a new questionnaire for the measurement of fear
of childbirth. Journal of Psychosomatic Obstetrics and
Gynecology, 19, 84–97.
Zar, M., Wijma, K., & Wijma, B. (2001). Pre and Postpartum
fear of childbirth in nulliparous and parous women.
Scandinavian Journal of Behaviour Therapy, 30(2), 75–81.