Embed Size (px)
Citation preview

1
How pen needles influencecompliance and wellbeingof the diabetic patient
Thessaloniki, November 13 2015

2
• Intro – key facts
• Factors influencing compliance and
wellbeing:
o Innovation
o Technology
o Quality

3
Headquarter: Grandate (Como)Turnover 2014: 1.218 Mio €Branches : 24 worldwide, 15 in Europe and4 in emerging countries
Distributors: over 100 worldwideBusiness units: 6 in EuropePoints of Sale : over 400 worldwideEmployees: 6.600
KEY FACTS

4
OUR BRANDS
Baby care Health & beauty

5
Source: IMS sep 15
Thermometers Health CareNebulizers Venipuncture
BPMs WoundcareDiabetes
32%32% 14%14% 20%20%
28%28% 24%24% 77%77% 26%26%
MARKET SHARES - ITALY

6

7

8
• Intro – key facts
• Factors influencing compliance and
wellbeing:
o Innovation
o Technology
o Quality

9
Pen needle technical terminology
1. Primary container
2. Needle shield
3. Cannula
4. Transparent glue
5. Needle hub
6. Medical paper
1
2
3
4
5
6
10
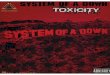
Tip
Bevels
Heel
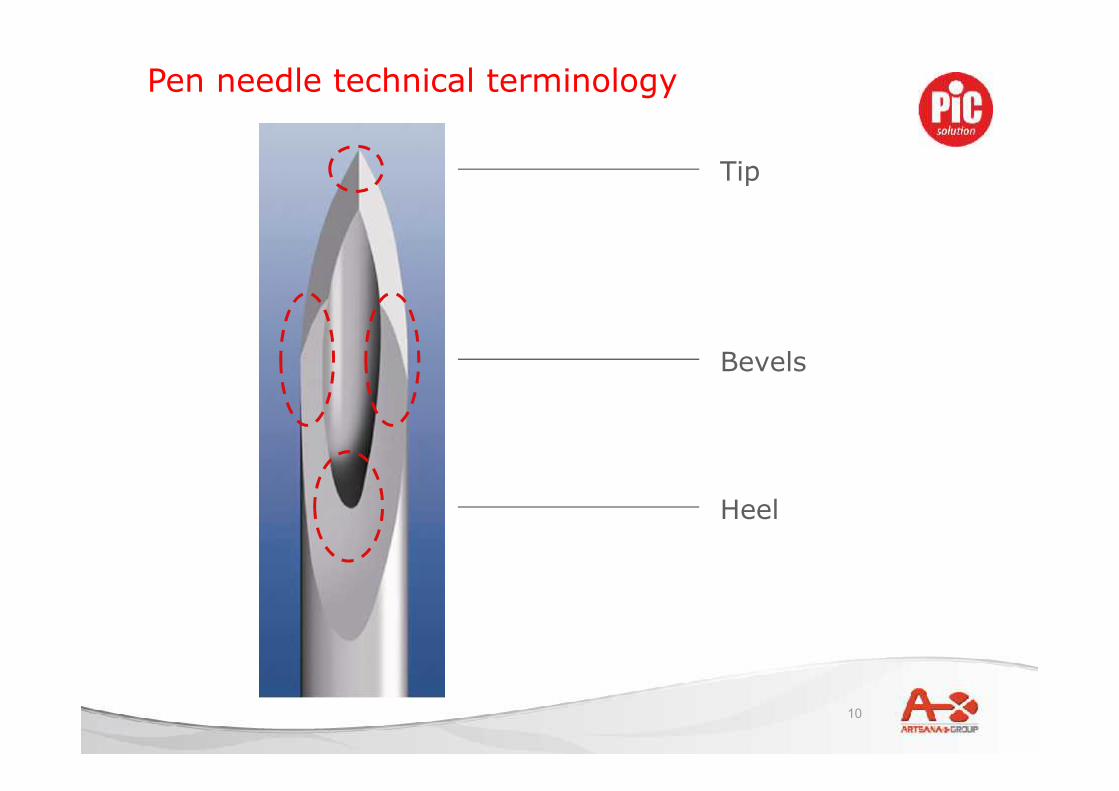
Pen needle technical terminology
11
Patient tip:• enters patient’s skin• entirely covered of silicone to ensure
smooth sliding
Cartridge tip:• enters the cartridge piercing its rubber
lid
Pen needle technical terminology

12
Insupen innovation
1. Extr3me triple sharpening
2. External diameter
3. Internal diameter
4. Length

13
1) Triple sharpening
The top of the cannula (patient tip) undergoes 3grinding treatments:• one central sharpening (A)• two side sharpening (B)
All main Insupen pen needles are sharpenedaccording to the new Extr3me technology,ensuring a more comfortable penetration.
A
BB
Designed for an Extr3me comfort
14
Designed for an Extr3me comfort
1) Triple sharpening – Extr3me
15
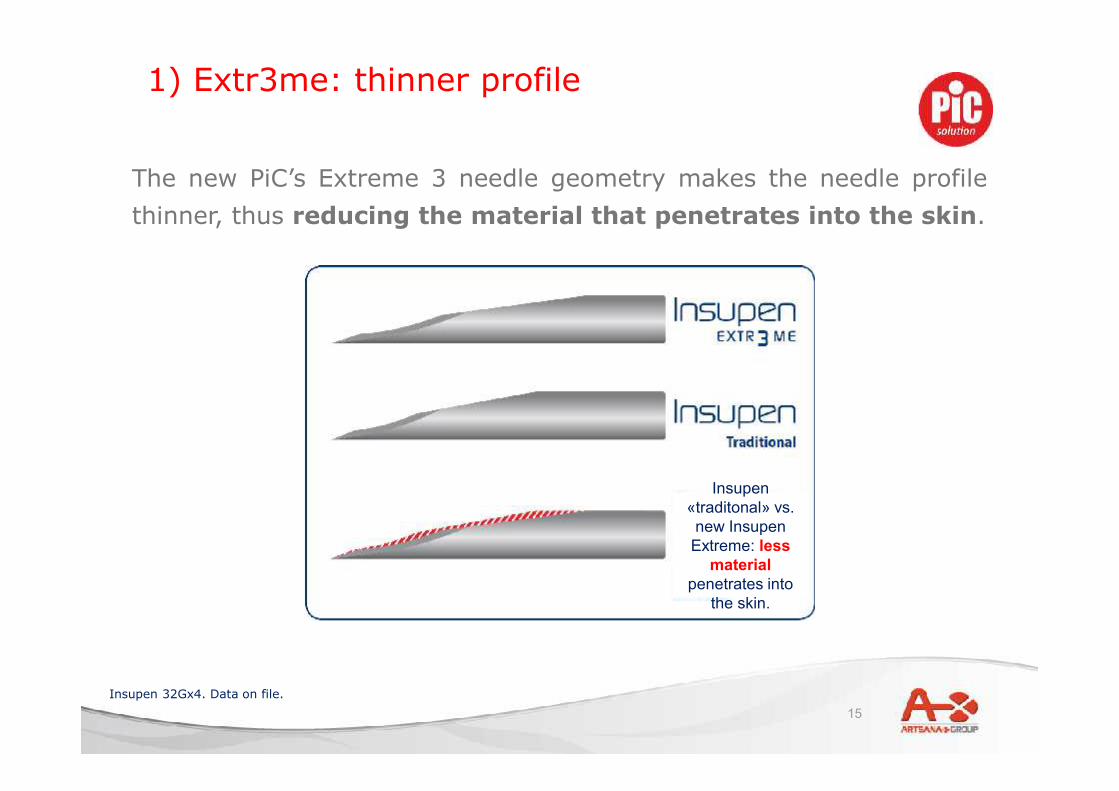
1) Extr3me: thinner profile
The new PiC’s Extreme 3 needle geometry makes the needle profilethinner, thus reducing the material that penetrates into the skin.
Insupen«traditonal» vs.new Insupen
Extreme: lessmaterial
penetrates intothe skin.
Insupen 32Gx4. Data on file.
16
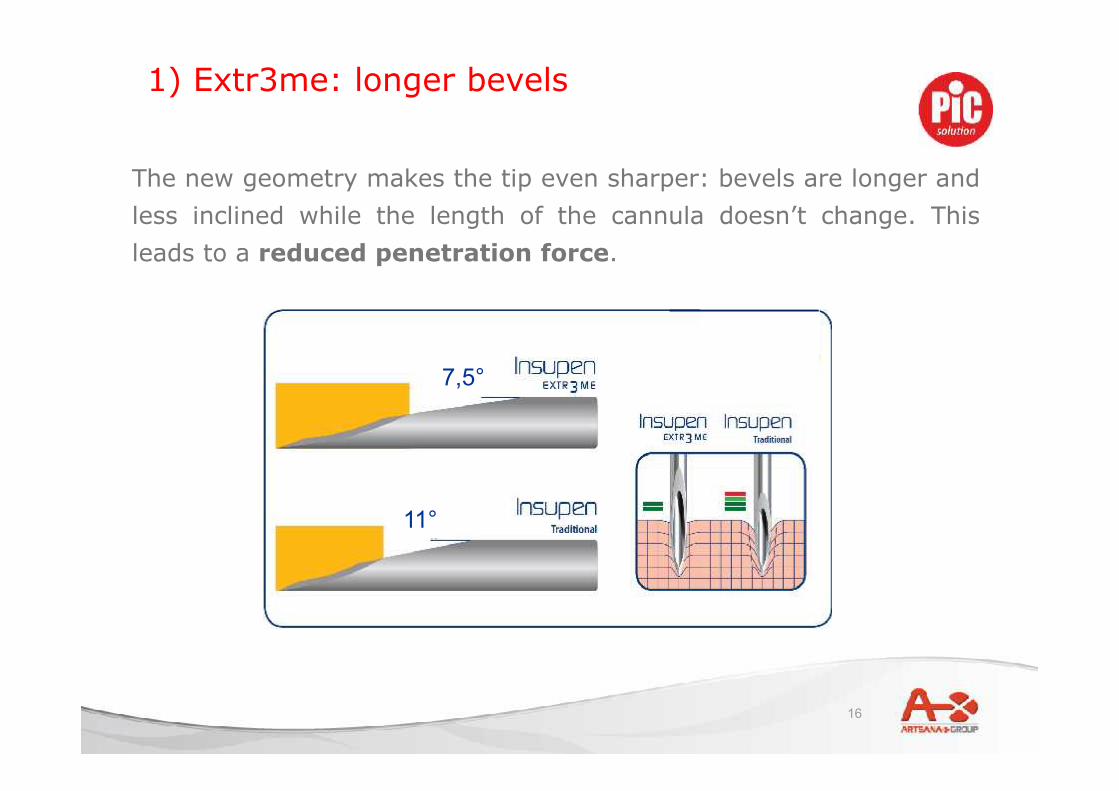
1) Extr3me: longer bevels
The new geometry makes the tip even sharper: bevels are longer andless inclined while the length of the cannula doesn’t change. Thisleads to a reduced penetration force.
7,5°
11°
17
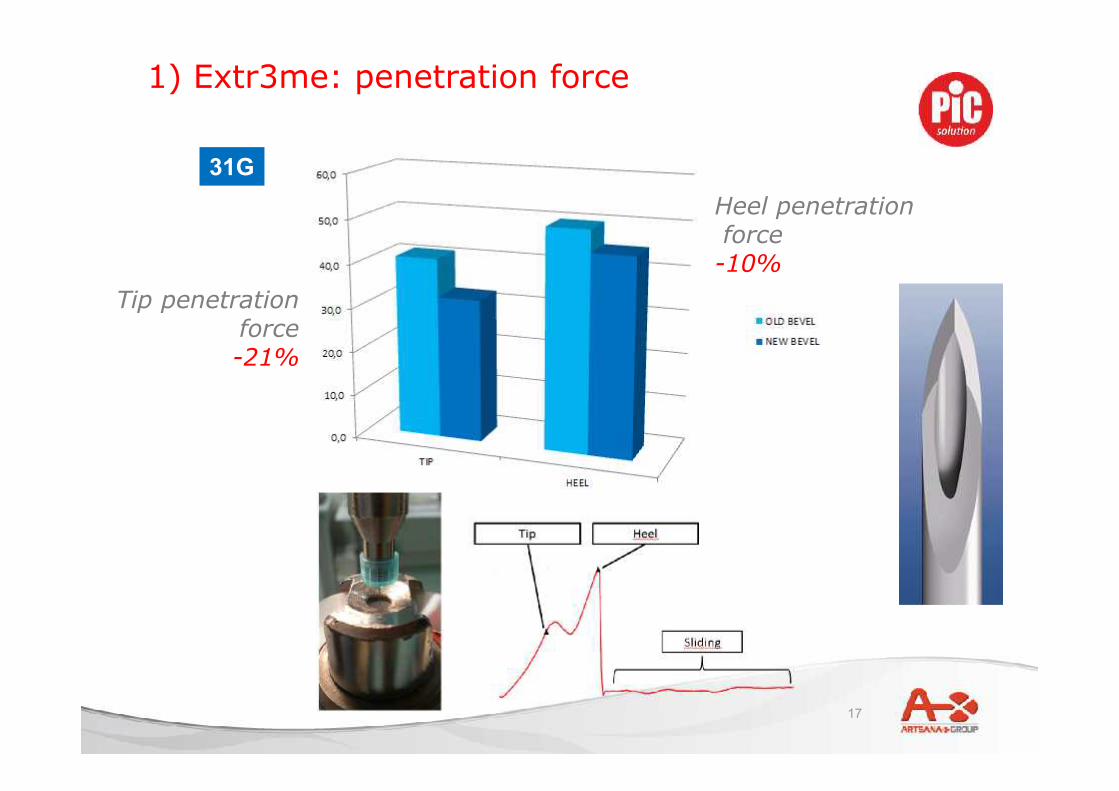
Heel penetrationforce
-10%Tip penetration
force-21%
1) Extr3me: penetration force
31G
18
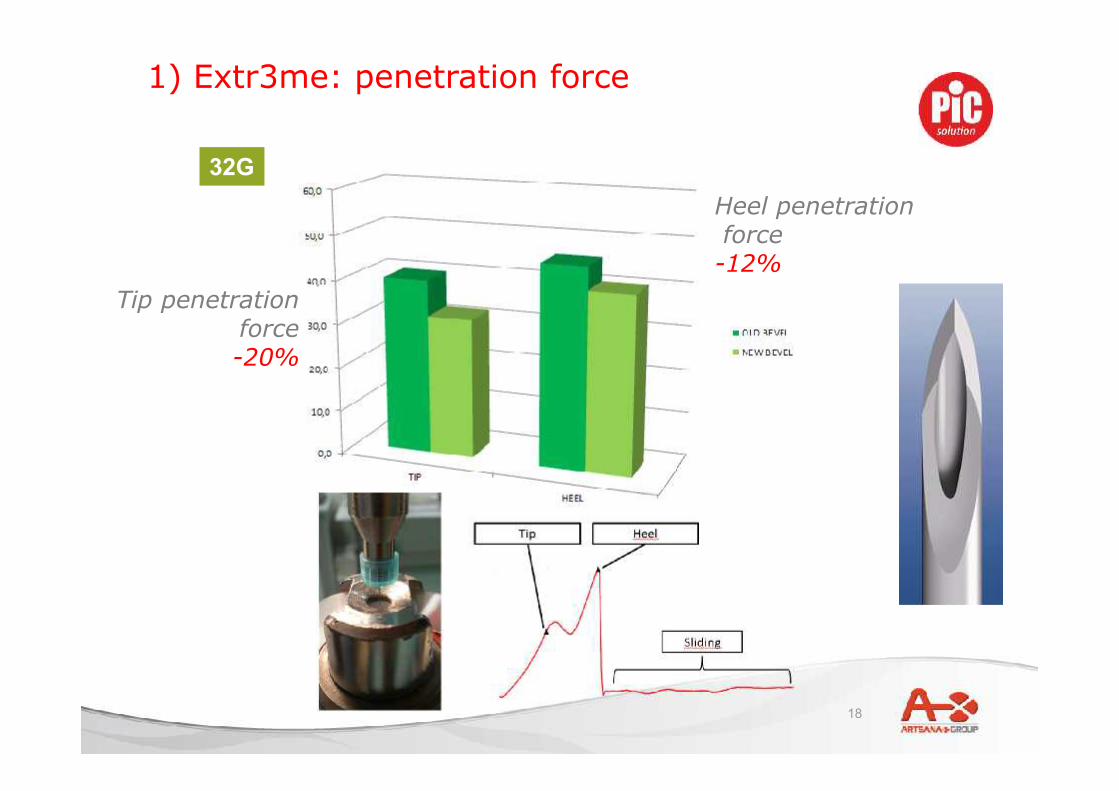
32G
Tip penetrationforce-20%
Heel penetrationforce
-12%
1) Extr3me: penetration force

19
All Insupen 32G and 31G pen needles feature the new Extremesharpening.
1) Triple sharpening – The new Extreme range

20
External diameter(GAUGE)
2) External diameter of the needle
21
Fear and pain of injections:
• 94% of insulin users show symptoms of anxiety, distress or
phobia around blood and injury from injections (1)
• 33% of insulin users are afraid of their injections (2)
• 75% of newly diagnosed children < 9 years old have a fear of
injections (3)
• 47% of people with diabetes say they would be more likely to
follow their prescribed insulin regimen if a product easing pain
and discomfort of injections was available (4)
2) External diameter: patient’s attitude
(1) Berlin I, Bisserbe JC, Eiber R, Balssa, N, Sachon C, Bosquet F, Grimaldi, A: Phobic symptoms, particularly the fear ofblood and injury, are associated with poor glycemic control in type 1 diabetic adults. Diabetes Care 1997;20:176–178
(2) Peyrot M, Rubin RR, Kruger DF, Travis LB: Correlates of insulin injection omission. Diabetes Care 2010;33:240-245(3) Howe CJ, Ratcliffe SJ, Tuttle A, Dougherty S, Lipman TH: Needle anxiety in children with type 1 diabetes and their
mothers. AM J Matern Child Nurs 2010;36:25-31(4) AADE Injection Impact Survey, 2007
22
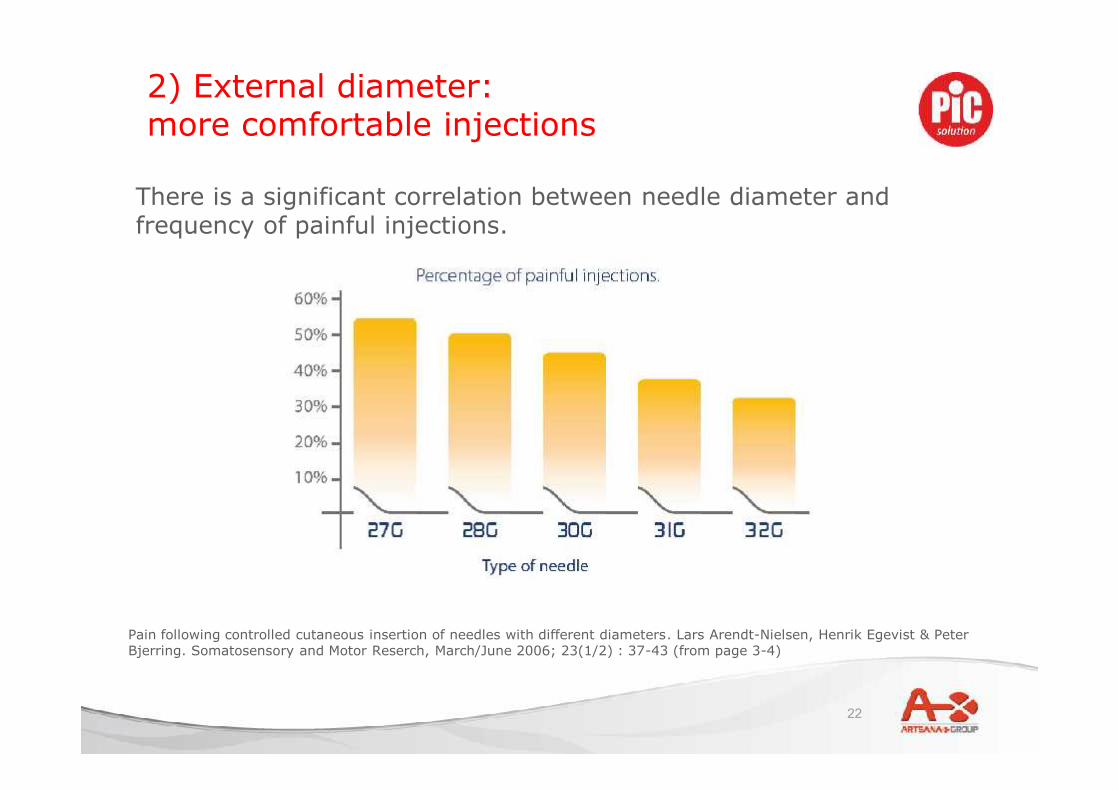
2) External diameter:more comfortable injections
There is a significant correlation between needle diameter andfrequency of painful injections.
Pain following controlled cutaneous insertion of needles with different diameters. Lars Arendt-Nielsen, Henrik Egevist & PeterBjerring. Somatosensory and Motor Reserch, March/June 2006; 23(1/2) : 37-43 (from page 3-4)
23
The first 32G pen needle on the market (2007).
2) External diameter

24
Doc Leader - Evaluation of acceptability of Insupen 32G pen needle
Main results of a customer satisfaction survey* involving 350patients who tried Insupen 32G
Does Insupen 32G make injections morecomfortable and less painful?
Would you recommend Insupen 32Gto another diabetic patient?
2) External diameter: Insupen 32G customersurvey

25
Internal diameter
Cannula wall
3) Internal diameter: the wall of the cannula

26
3) Internal diameter: the wall of the cannula
According to the ISOnorm, the cannula canbe:
NORMAL WALLED
or
THIN WALLED.
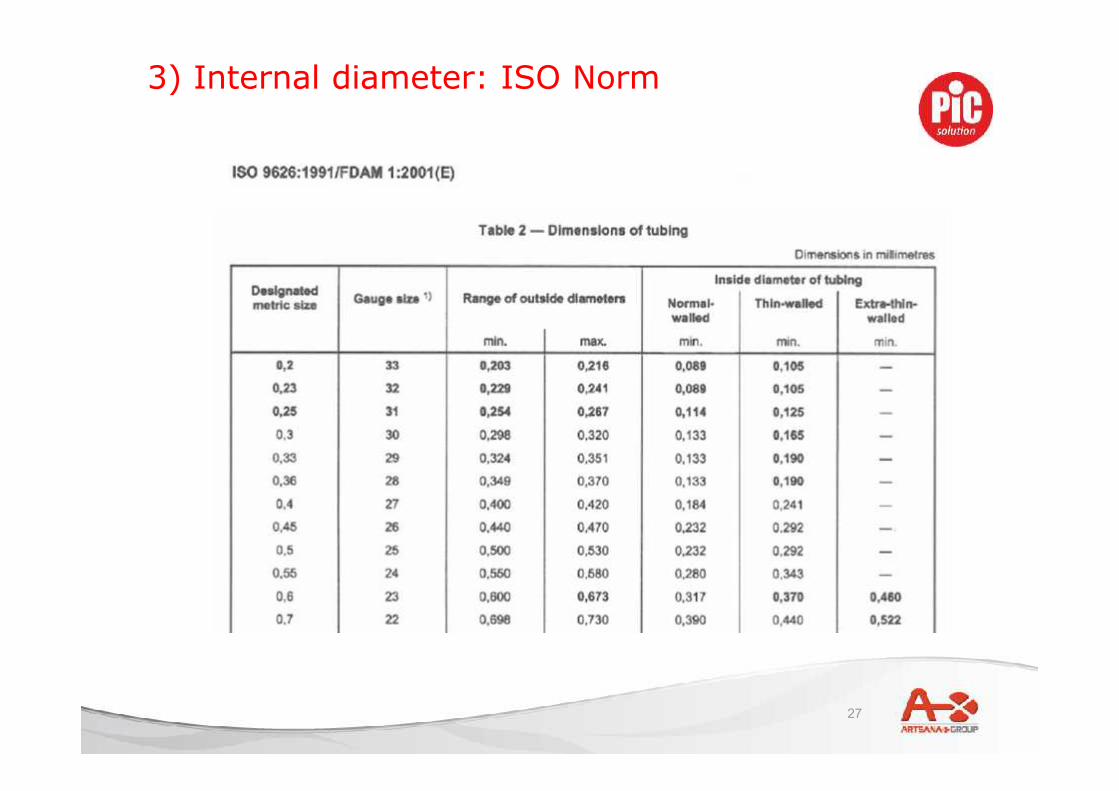
27
3) Internal diameter: ISO Norm
28
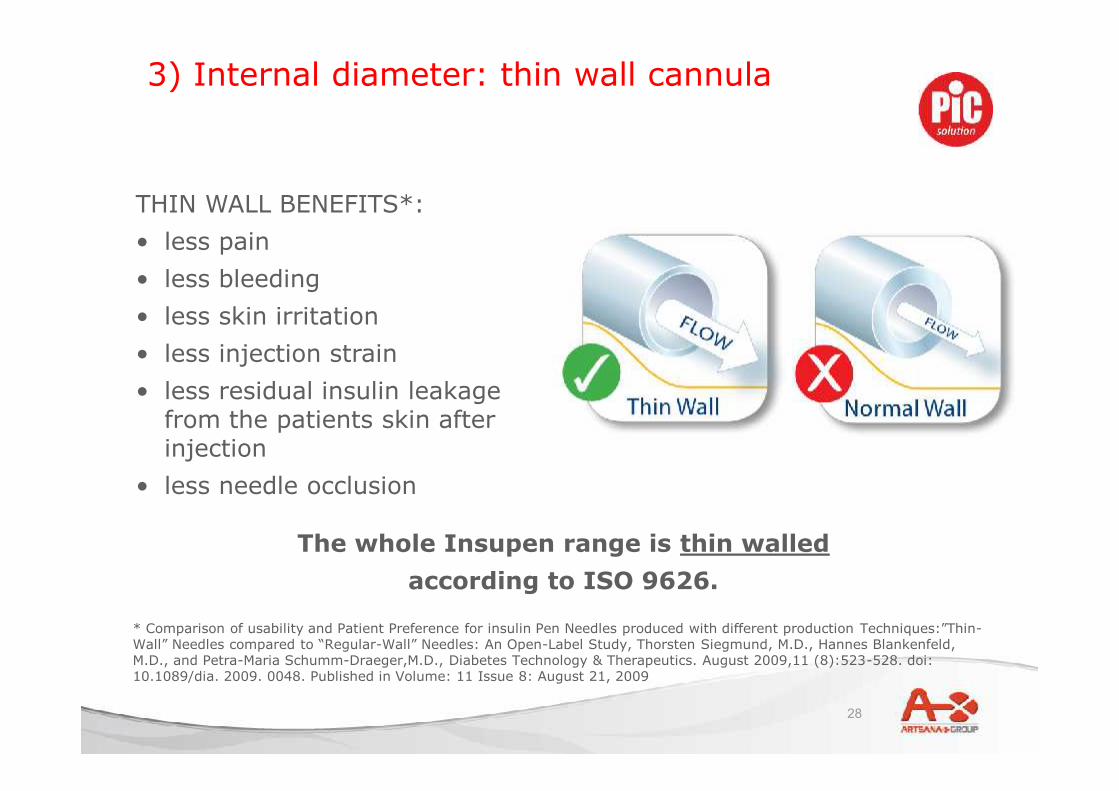
3) Internal diameter: thin wall cannula
* Comparison of usability and Patient Preference for insulin Pen Needles produced with different production Techniques:”Thin-Wall” Needles compared to “Regular-Wall” Needles: An Open-Label Study, Thorsten Siegmund, M.D., Hannes Blankenfeld,M.D., and Petra-Maria Schumm-Draeger,M.D., Diabetes Technology & Therapeutics. August 2009,11 (8):523-528. doi:10.1089/dia. 2009. 0048. Published in Volume: 11 Issue 8: August 21, 2009
THIN WALL BENEFITS*:• less pain• less bleeding• less skin irritation• less injection strain• less residual insulin leakage
from the patients skin afterinjection
• less needle occlusion
The whole Insupen range is thin walledaccording to ISO 9626.

29
1. drug flows easier through the needle, for a faster injection2. more comfortable injection
3) Internal diameter: High Flow Thin Wall
Insupen 32G 4mm goes even beyond:
Super thin wall features a wall thickness of 0,045 mm, still complying with the ISO Normsrequirements (such as cannula stiffness).
HIGH FLOWTHIN WALL
30
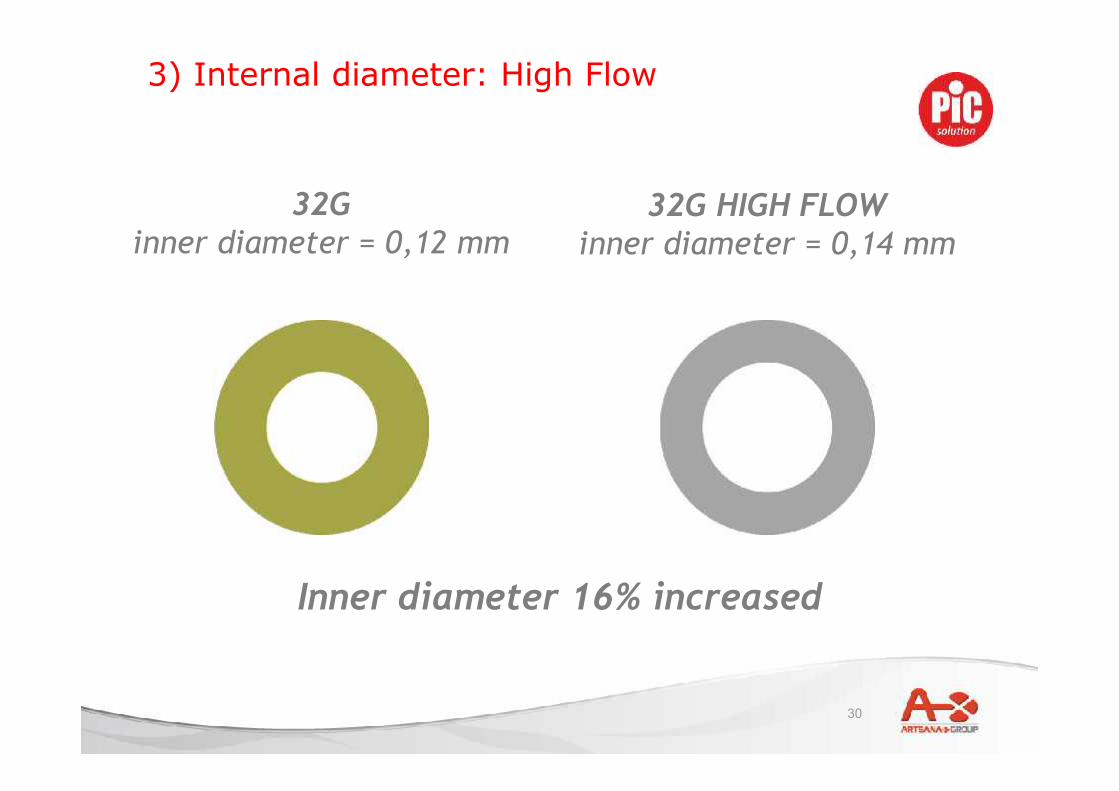
32Ginner diameter = 0,12 mm
32G HIGH FLOWinner diameter = 0,14 mm
Inner diameter 16% increased
3) Internal diameter: High Flow
31
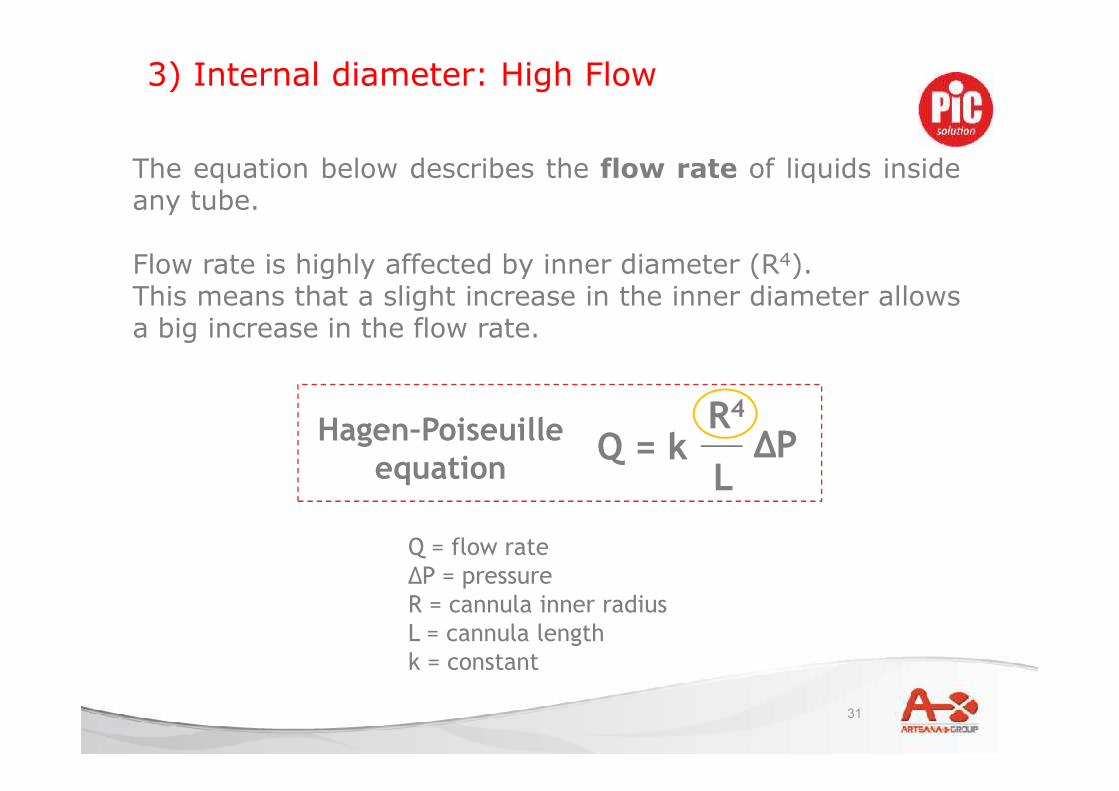
Q = flow rateΔP = pressureR = cannula inner radiusL = cannula lengthk = constant
ΔPL
R4
Q = kHagen–Poiseuilleequation
The equation below describes the flow rate of liquids insideany tube.
Flow rate is highly affected by inner diameter (R4).This means that a slight increase in the inner diameter allowsa big increase in the flow rate.
3) Internal diameter: High Flow
32
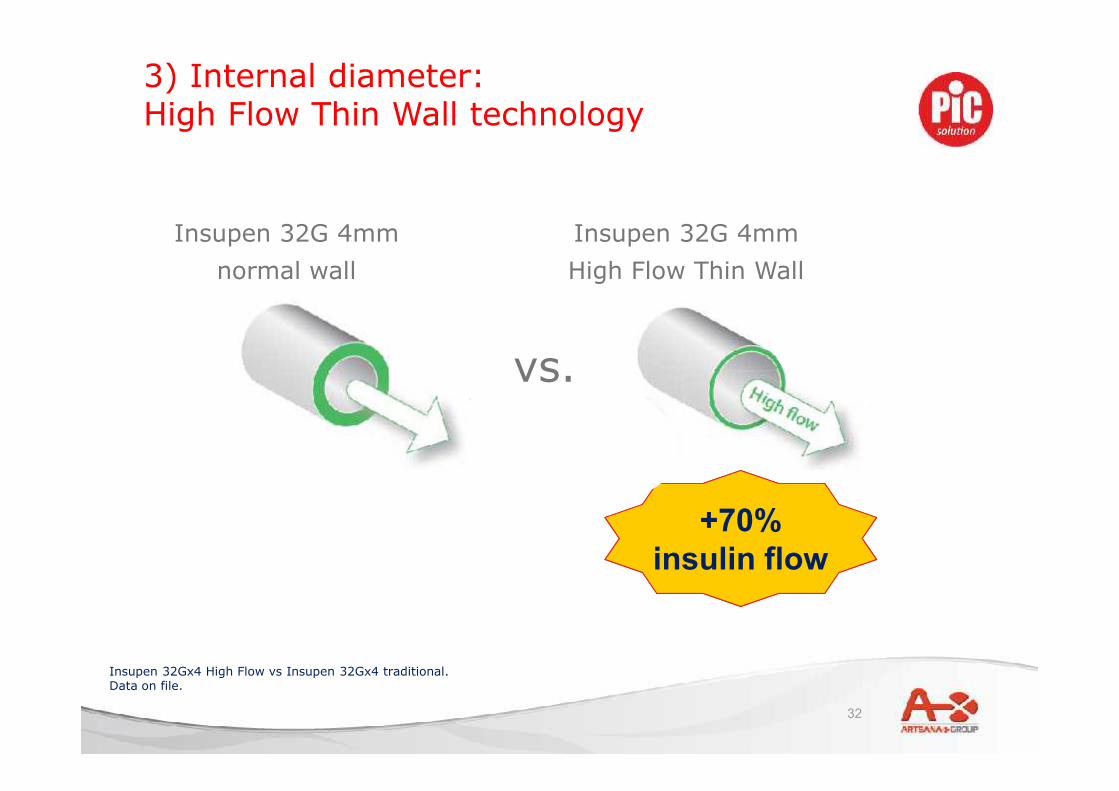
3) Internal diameter:High Flow Thin Wall technology
Insupen 32G 4mmnormal wall
Insupen 32Gx4 High Flow vs Insupen 32Gx4 traditional.Data on file.
+70%insulin flow
+70%insulin flow
vs.
Insupen 32G 4mmHigh Flow Thin Wall
33
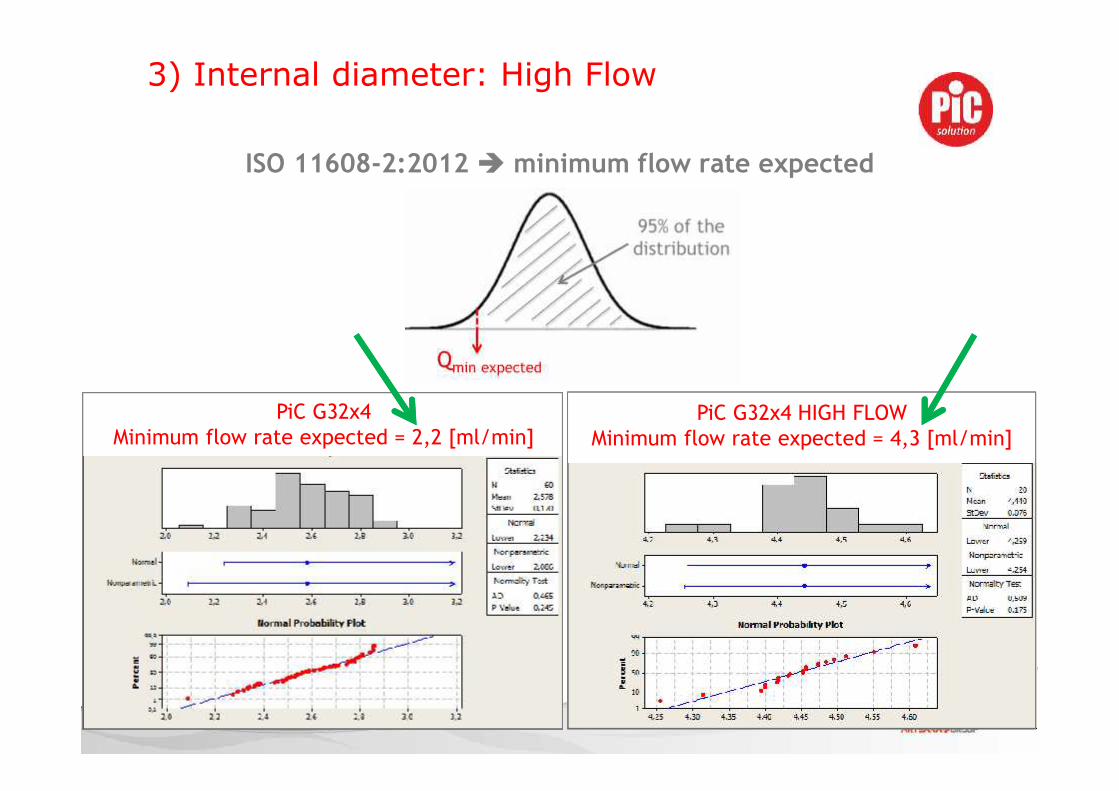
ISO 11608-2:2012 minimum flow rate expected
PiC G32x4Minimum flow rate expected = 2,2 [ml/min]
PiC G32x4 HIGH FLOWMinimum flow rate expected = 4,3 [ml/min]
3) Internal diameter: High Flow
34
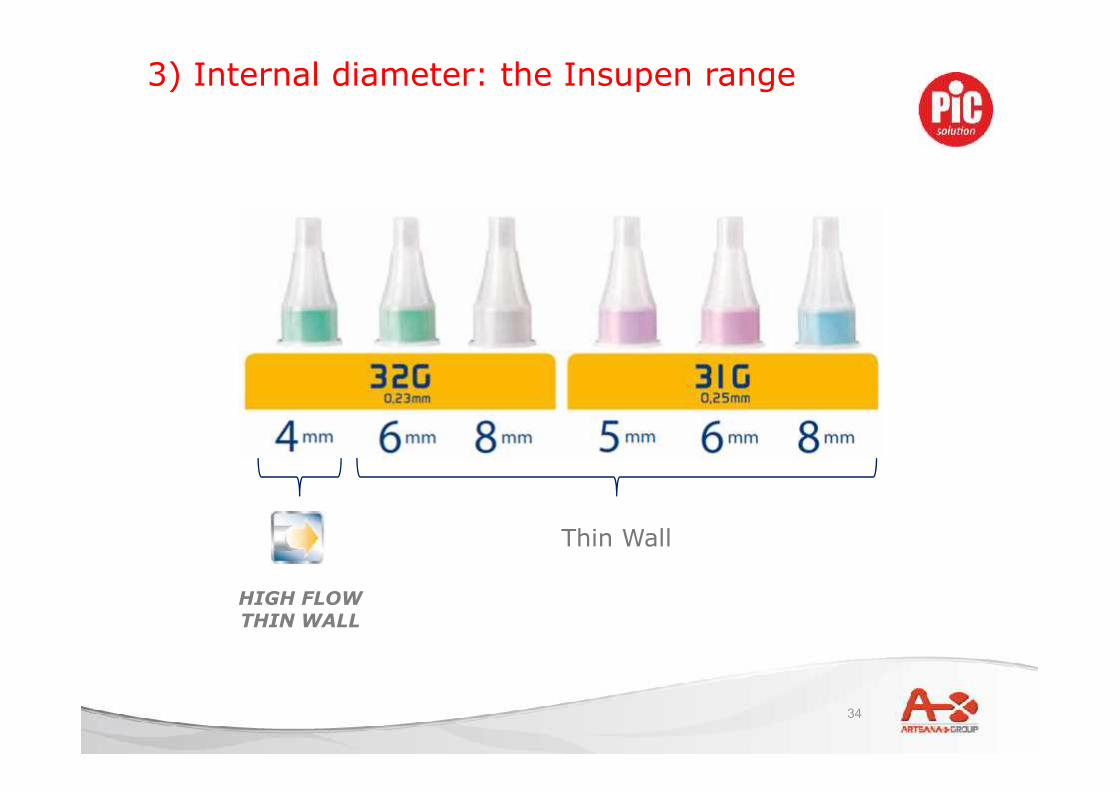
3) Internal diameter: the Insupen range
Thin Wall
HIGH FLOWTHIN WALL
35
• In a 2004 study, blinded assessments of pain showed no significantdifference in pain scores for the 2 needle lengths tested (6mm and12.7mm). This observation would indicate that, at least under theconditions of needle testing in this clinical trial, the discomfort ofpuncturing dermal tissues did not differ materially for the 2 lengths.
• The questions specifically comparing patient perception toward the 2needles showed however a marked preference for the shorter, finerneedle: when specifically asked about needle preference, patientsindicated that they considered the shorter needle (6mm) easier touse.
4) Length: pain and ease of use
A Multicenter, Open-Label, Randomized,Two-Period Crossover Trial Comparing Glycemic Control, Satisfaction, and Preference Achievedwith a 31 Gauge × 6 mm Needle versus a 29 Gauge × 12.7 mm Needle in Obese Patients with Diabetes Mellitus. Sherwyn Schwartz, MD,1 David Hassman, DO, 2 John Shelmet, MD, 3 Richard Sievers, MD, 4 Richard Weinstein, MD, 5 John Liang, PhD, 6 and William Lyness,PhD 6. CLINICAL THERAPEUTICS®/VoL. 26, No. 10, 2004
36
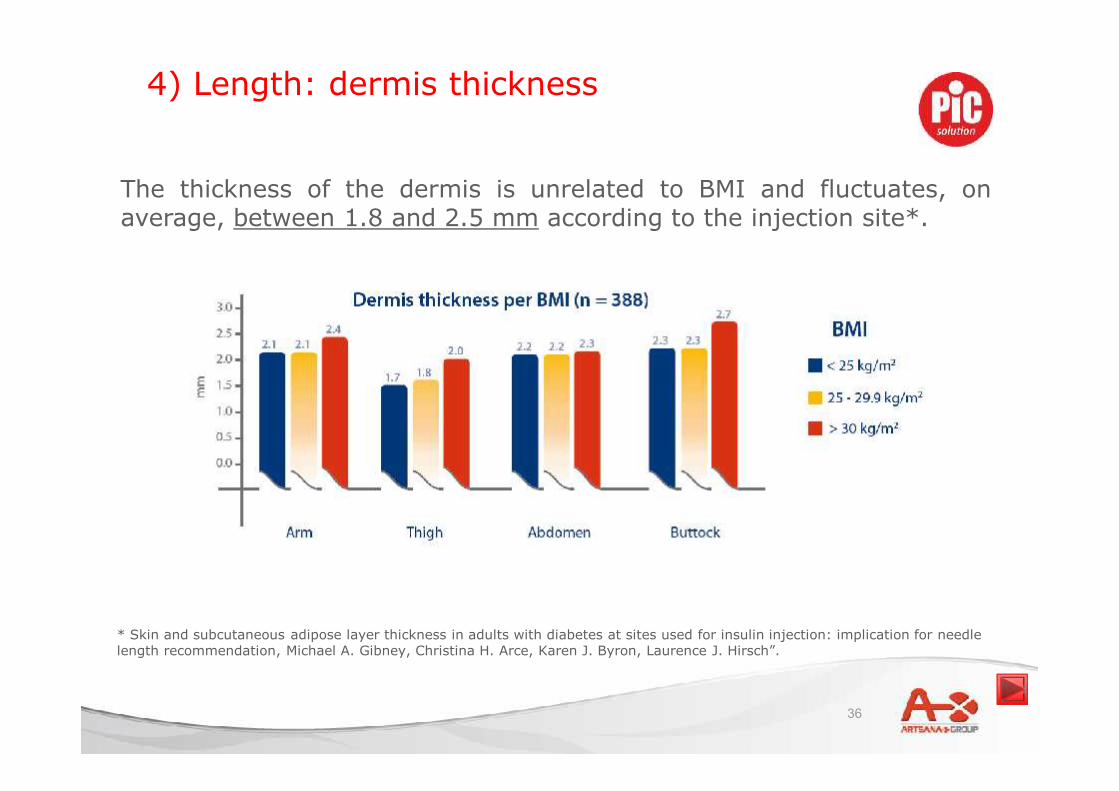
4) Length: dermis thickness
* Skin and subcutaneous adipose layer thickness in adults with diabetes at sites used for insulin injection: implication for needlelength recommendation, Michael A. Gibney, Christina H. Arce, Karen J. Byron, Laurence J. Hirsch”.
The thickness of the dermis is unrelated to BMI and fluctuates, onaverage, between 1.8 and 2.5 mm according to the injection site*.

37
4) Length: suitable needle
* New injection recommendations for patients with diabetes, A Frid, L. Hirsch, R. Gaspar, D. Hicks, G. Kreugel, J. Liersch, C.Letondeur, J.P. Sauvanet, N. Tubiana-Rufi, K. Strauss - Diabetes & Metabolism 36 (2010) S3-S18
The new guidelines for insulin injections recommend to use shortneedles (4 to 6mm) for all patients, including those with a sturdyphysical build, because they can pass through the dermis layer andreach the subcutaneous tissue.

38
We have decided however to have a wide32G range in order to let freedom ofchoice:
• to the patient, who can choose acomfortable pen needle (32G) in avariety of lengths matching his/her ownfavorite injection technique (90°, 45°,with pinch etc)
• to the professional, who –according tohis/her own experience- may prescribea specific pen needle for each patient
4) Length: Insupen’s choice
The above injection techniques are recommended in the Clinical Study “New injection recommended for patients with diabetes”, AndersFrid, Ruth Gaspar, Debbie Hicks, Larry Hirsch, Gillian Kreugel, Jutta Liersch, Corinne Letondeur, Jean-Pierre Sauvanet, Nadia Tubiana-Rufi, Kenneth Strauss - Vol.36 – 2010, Diabetes & Metabolism.”
39
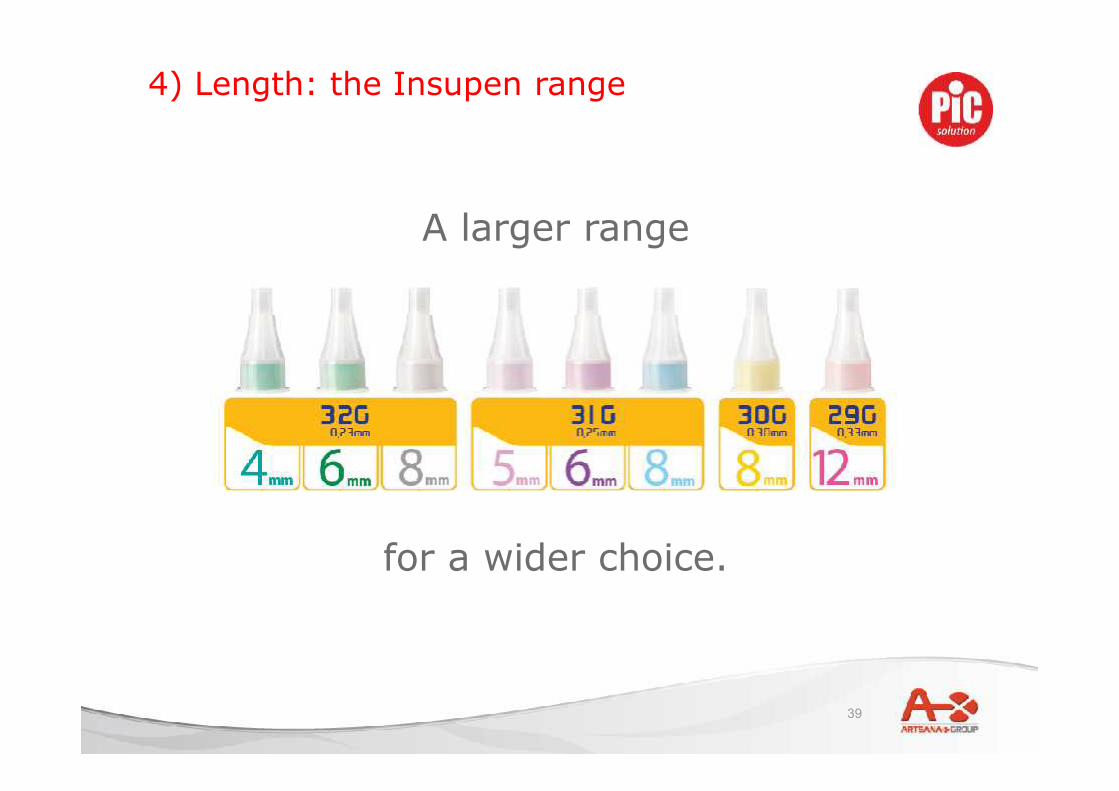
A larger range
4) Length: the Insupen range
for a wider choice.

40
• Intro – key facts
• Factors influencing compliance and
wellbeing:
o Innovation
o Technology
o Quality
41
Insupen technology
1. Anti-coring
2. Electrochemical polishing
3. Silicon
4. Compatibility

42
In order to get the heel surface smooth, tiny glass microspheres are “shot” at the heel to round off its surface andremove all eventual spikes/burrs left after the sharpening.
Closer look
500x magnifying
BEFORE TREATMENT
1) Anti-coring treatment: purpose & process
AFTER TREATMENTHEEL
Comparative scanning microscope examination (Breda Scientific Institute – Milan)
43
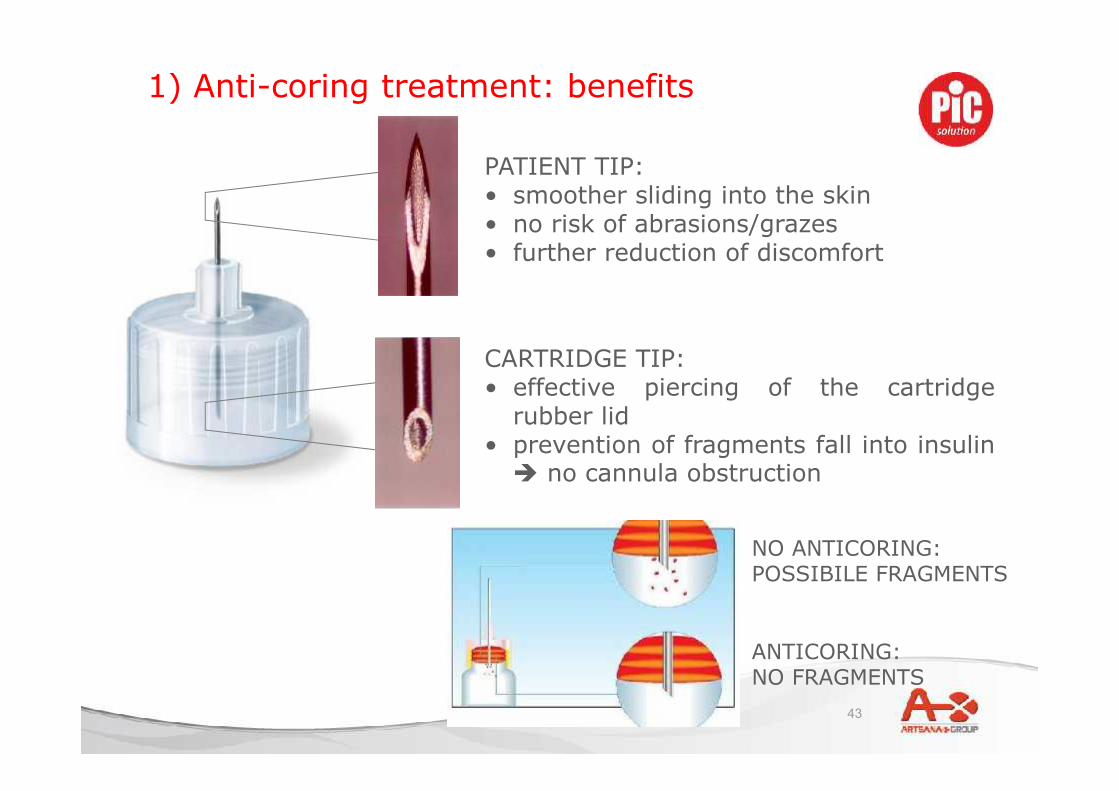
CARTRIDGE TIP:• effective piercing of the cartridge
rubber lid• prevention of fragments fall into insulin no cannula obstruction
1) Anti-coring treatment: benefits
NO ANTICORING:POSSIBILE FRAGMENTS
ANTICORING:NO FRAGMENTS
PATIENT TIP:• smoother sliding into the skin• no risk of abrasions/grazes• further reduction of discomfort

44
2) Electrochemical polishing
Both tip and bevels are treated in an electrochemical acid bath givinga final finishing that:• removes any remaining spikes• gets a surface finish (absence of micro-imperfections on the tip)
Comparative scanning microscope examination (Breda Scientific Institute – Milan)
INSUPEN needle Untreated needle
45
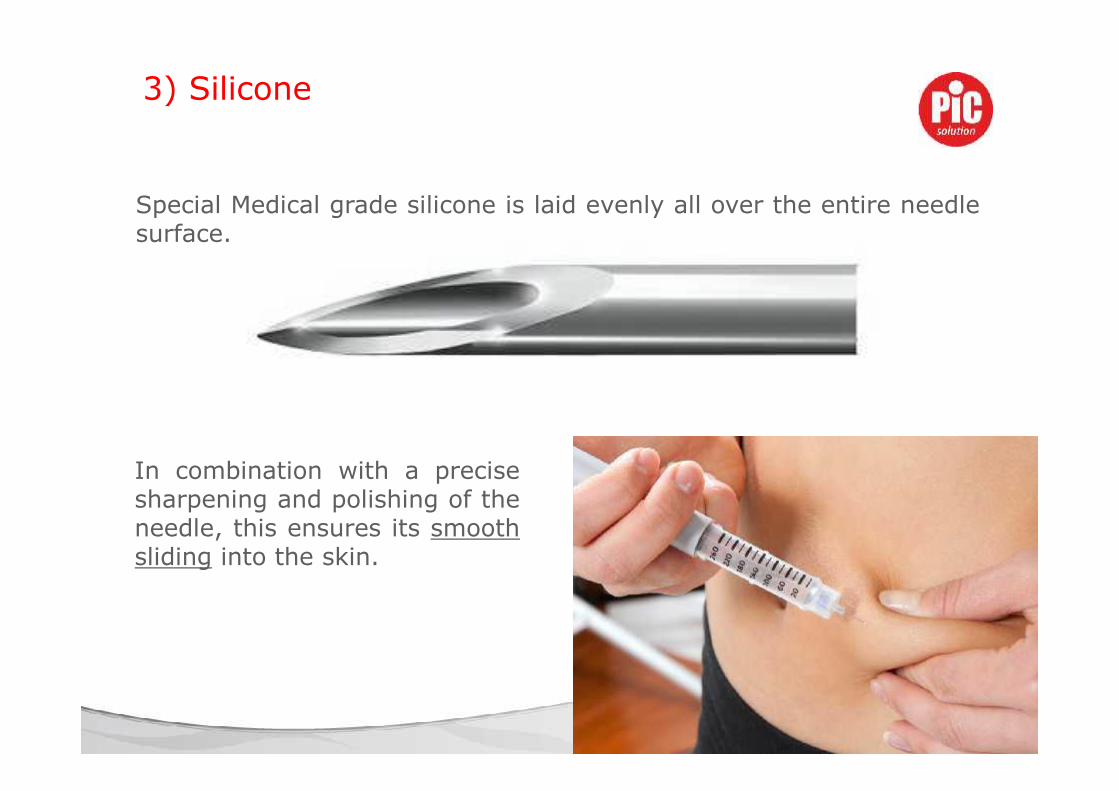
Special Medical grade silicone is laid evenly all over the entire needlesurface.
3) Silicone
In combination with a precisesharpening and polishing of theneedle, this ensures its smoothsliding into the skin.
46
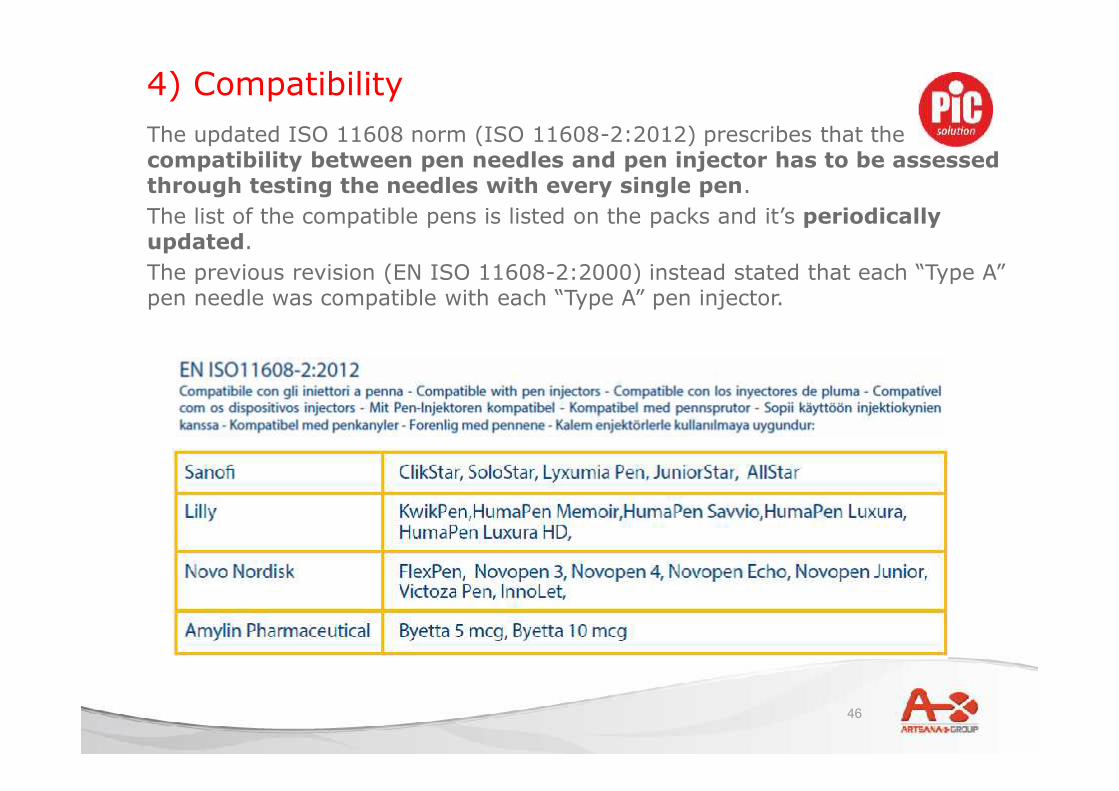
4) CompatibilityThe updated ISO 11608 norm (ISO 11608-2:2012) prescribes that thecompatibility between pen needles and pen injector has to be assessedthrough testing the needles with every single pen.The list of the compatible pens is listed on the packs and it’s periodicallyupdated.The previous revision (EN ISO 11608-2:2000) instead stated that each “Type A”pen needle was compatible with each “Type A” pen injector.
47
Using a needle more than once may cause:
• Inaccurate dosage 1
• Insulin crystallization 2
• Lipodystrophies 3
• Sterilisation 4
• Damage of needle tip 5
• Lubricant removal 6
1. Ginsberg BH, Parkes JL, Sparacino C., The kinetics of insulin administration by insulin pens, Horm Metab Res. 1994Dec;26(12):584-7. - The Importance of Good Insulin Injection Practices in Diabetes Management - Richard Dolinar, MD,2009l
2. Hanas R. (1998), Insulin-Dependent Diabetes in Children, Adolescents and Adults. Uddevalla, Sweden, Piara HB.3. I.V. Misnikova, A.V. Dreval, V.A Gubkina, E.V. Rusanova ; The Risks of Repeated Use of Insulin Pen Needles in Patients with
Diabetes Mellitus; Journal of Diabetology, 2011. - Bahar Vardar, Sevgi Kızılcı; Factors influencing lipohypertrophy; TITAN2009
4. I.V. Misnikova, A.V. Dreval, V.A Gubkina, E.V. Rusanova ; The Risks of Repeated Use of Insulin Pen Needles in Patients withDiabetes Mellitus; Journal of Diabetology, 2011. - Insulin Administration; DIABETES CARE, VOLUME 27, supplement 1, 2004.
5. I.V. Misnikova, A.V. Dreval, V.A Gubkina, E.V. Rusanova ; The Risks of Repeated Use of Insulin Pen Needles in Patients withDiabetes Mellitus; Journal of Diabetology, 2011 . - King L (2003) Subcutaneous insulin injection technique. NursingStandard. 17, 34, 45-52.
6. The Importance of Good Insulin Injection Practices in Diabetes Management - Richard Dolinar, MD, 2009
Single use device

48
These data suggest that if participants reuse pen needles, they have just as muchchance of having lipohypertrophy as not, but if they do not reuse pen needles theyhave a modest (and significant) reduction in the risk of lipohypertrophy, eventhough many of those who do not reuse pen needles still develop lipohypertrophy.
Results and analysis of the 2008–2009 Insulin Injection Technique Questionnaire survey. Carina DE CONINCK, AndersFRID,Ruth GASPAR,Debbie HICKS,Larry HIRSCH,Gillian KREUGEL,Jutta LIERSCH,Corinne LETONDEUR,Jean-PierreSAUVANET,Nadia TUBIANA1and Kenneth STRAUSS. Journal of Diabetes 2 (2010) 168–179
Single use device:reuse and lypohypertrophy

49
• Intro – key facts
• Factors influencing compliance and
wellbeing:
o Innovation
o Technology
o Quality
50
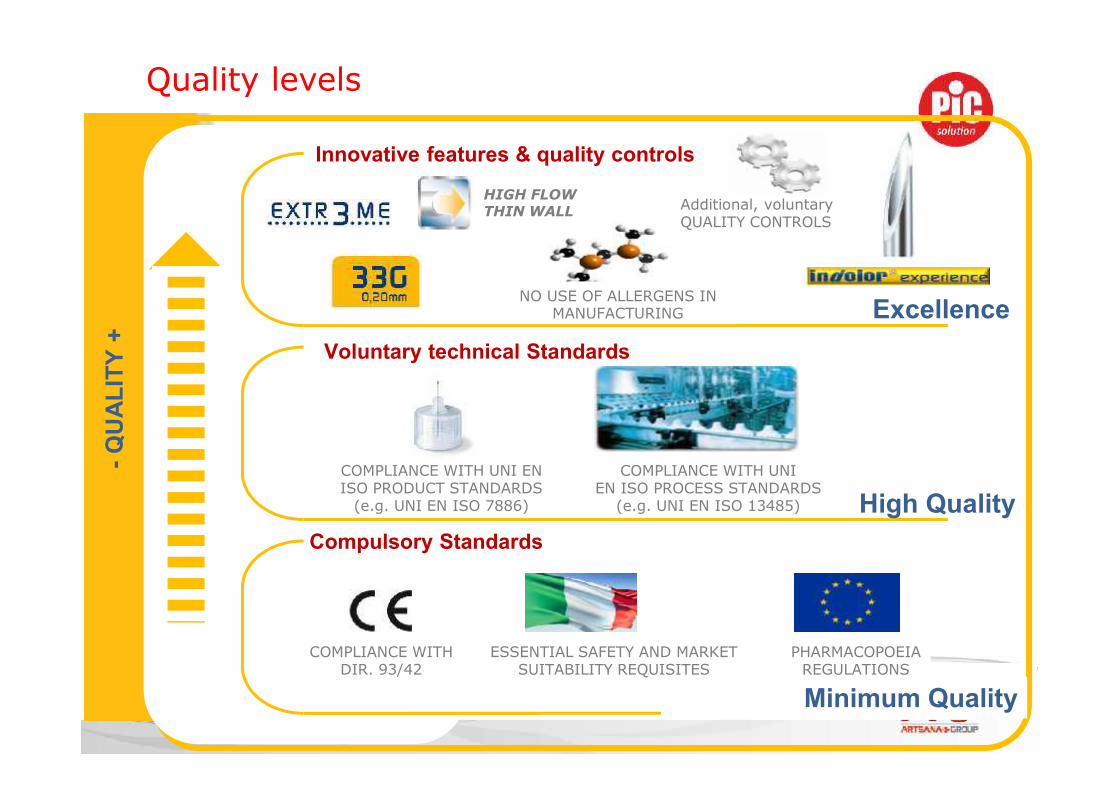
Quality levels-Q
UAL
ITY
+
Excellence
Innovative features & quality controls
Voluntary technical Standards
COMPLIANCE WITH UNI ENISO PRODUCT STANDARDS
(e.g. UNI EN ISO 7886) High QualityCOMPLIANCE WITH UNI
EN ISO PROCESS STANDARDS(e.g. UNI EN ISO 13485)
COMPLIANCE WITHDIR. 93/42
ESSENTIAL SAFETY AND MARKETSUITABILITY REQUISITES
PHARMACOPOEIAREGULATIONS
Compulsory Standards
Minimum Quality
NO USE OF ALLERGENS INMANUFACTURING
Additional, voluntaryQUALITY CONTROLS
HIGH FLOWTHIN WALL

51
The ISO 9626 Stiffness Test is made in order to verify that thenormal bending of the needle stays inside the parameters set by
the ISO.
Quality Control process:stiffness test

52
Quality Control process:cannula pull test
The ISO 7864 pull test,consisting in pulling thecannula with a certainforce, is performed toverify that it does not
detaches from the hub.

53
The ISO 9626 Breakage Test, consisting in bending right andleft several times a cannula, is performed to verify that it does
not break.
Quality Control process:cannula breakage test

54
Quality Control process:dislocation test
This test verifies that thecannula is straightly mounted
onto the hub (ISO 11608)

55
This test, performed accordingto ISO 11608, verifies that thestrength necessary to screw
and unscrew a pen needle on apen stays inside ISO
parameters.
Quality Control process:torque test

56
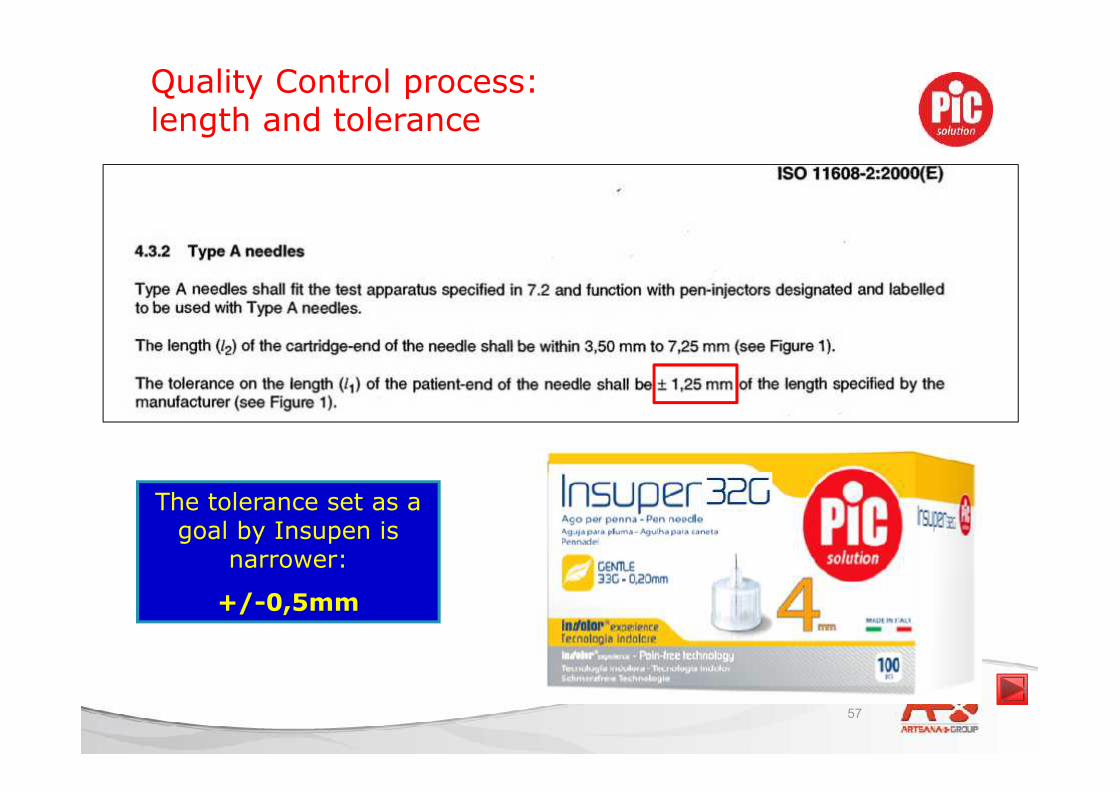
Quality Control process: cannula length
This test, performedaccording to ISO 11608,
verifies that the real lengthof the needle stays inside
ISO tolerances.
57
The tolerance set as agoal by Insupen is
narrower:
+/-0,5mm
Quality Control process:length and tolerance
58
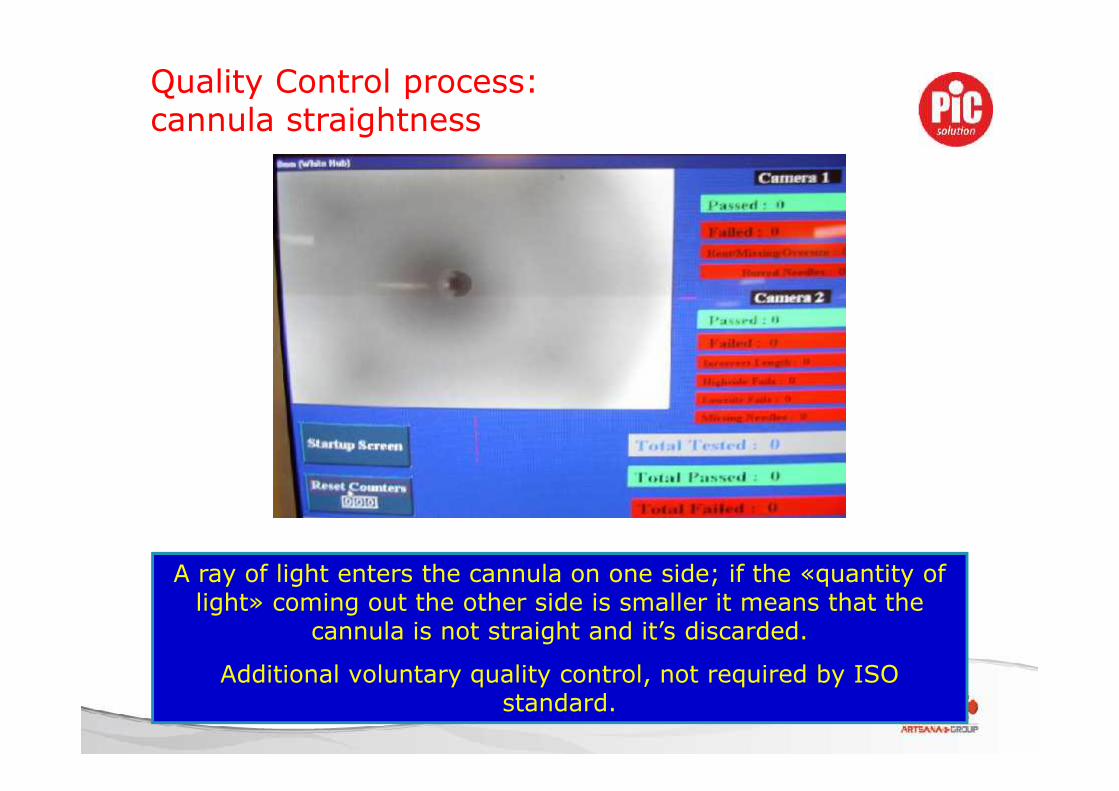
A ray of light enters the cannula on one side; if the «quantity oflight» coming out the other side is smaller it means that the
cannula is not straight and it’s discarded.
Additional voluntary quality control, not required by ISOstandard.
Quality Control process:cannula straightness

59
Additional voluntary qualitycontrol not required by ISO
standard.
Three different checks are performed to ensure that cannulas are notstuck:
1. Automatic control during cannula manufacturing2. Random control at the end of the cannula manufacturing stage3. Automatic control during assembly stage (100% of the production)
Quality Control process:cannula obstruction

60
Polyurethanefilmaccording toISO TC 84SC1 n.252
We check the penetrationforce of Insupen pen needlesusing a special polyurethanefilm that reproduces asclosely as possible thefeatures of the human skin.
The output is then comparedwith our internal database toverify that it stays inside theestablished parameters.
Additional voluntary qualitycontrol not required by ISOstandard.
Quality Control process:needle penetration test

61
Main needle controls
Technical file available on demand
REFERENCE STANDARD AIM OF TEST IMPACT ON QUALITY
SHEAR RESISTANCEUNI EN ISO 7864
(validation control – internal procedure
no. 10.05.01.00 no. 6)
Check cannulas’ shear
resistance under cyclic
stress
Guarantee maximum needle quality
NEEDLE DIMENSIONSISO 7864 (routine control - internal
procedure no. 10.05.01.00 no. 3)
Check cannula and needle
dimensions
(internal/external diameter
- wall/angle/tip thickness
Ensure most painless penetration
possible
FLEXINGISO 9626 (routine control - internal
procedure no. 10.05.01.00 no. 4)
Check needle’s flex
resistance
Ensure utmost needle quality and
safety during use
INTERNAL/EXTERNAL
CANNULA CLEANLINESS
ISO 7864 – ISO 8537 (routine control -
internal procedure no. 10.05.01.00 no.
5)
Exclude contamination by
foreign bodies
Ensure maximum patient health
and safety
62Technical file available on demand
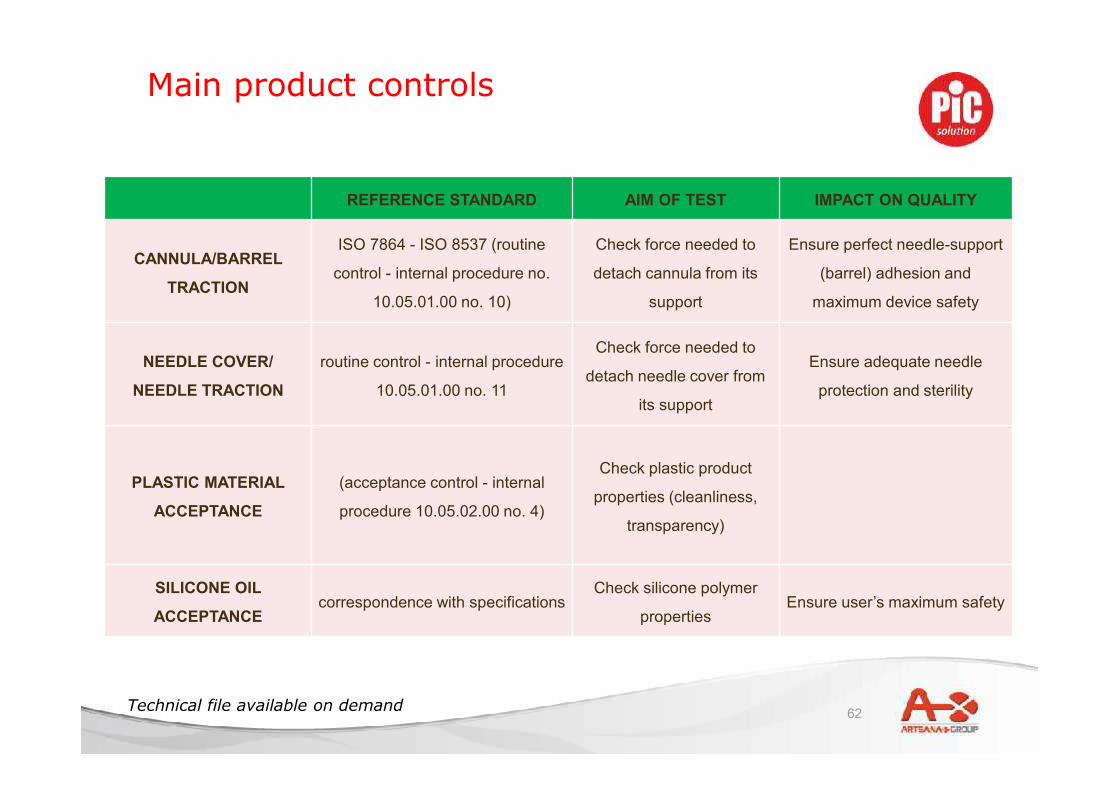
REFERENCE STANDARD AIM OF TEST IMPACT ON QUALITY
CANNULA/BARREL
TRACTION
ISO 7864 - ISO 8537 (routine
control - internal procedure no.
10.05.01.00 no. 10)
Check force needed to
detach cannula from its
support
Ensure perfect needle-support
(barrel) adhesion and
maximum device safety
NEEDLE COVER/
NEEDLE TRACTION
routine control - internal procedure
10.05.01.00 no. 11
Check force needed to
detach needle cover from
its support
Ensure adequate needle
protection and sterility
PLASTIC MATERIAL
ACCEPTANCE
(acceptance control - internal
procedure 10.05.02.00 no. 4)
Check plastic product
properties (cleanliness,
transparency)
SILICONE OIL
ACCEPTANCEcorrespondence with specifications
Check silicone polymer
propertiesEnsure user’s maximum safety
Main product controls
63Technical file available on demand
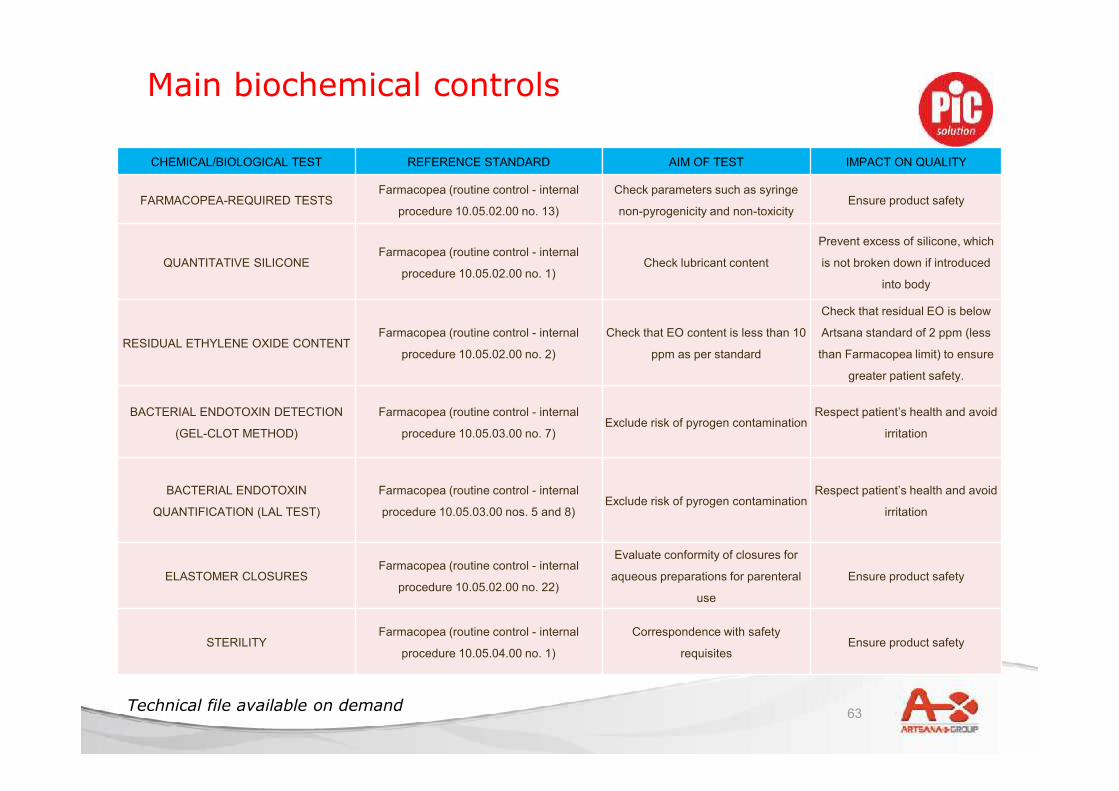
CHEMICAL/BIOLOGICAL TEST REFERENCE STANDARD AIM OF TEST IMPACT ON QUALITY
FARMACOPEA-REQUIRED TESTSFarmacopea (routine control - internal
procedure 10.05.02.00 no. 13)
Check parameters such as syringe
non-pyrogenicity and non-toxicityEnsure product safety
QUANTITATIVE SILICONEFarmacopea (routine control - internal
procedure 10.05.02.00 no. 1)Check lubricant content
Prevent excess of silicone, which
is not broken down if introduced
into body
RESIDUAL ETHYLENE OXIDE CONTENTFarmacopea (routine control - internal
procedure 10.05.02.00 no. 2)
Check that EO content is less than 10
ppm as per standard
Check that residual EO is below
Artsana standard of 2 ppm (less
than Farmacopea limit) to ensure
greater patient safety.
BACTERIAL ENDOTOXIN DETECTION
(GEL-CLOT METHOD)
Farmacopea (routine control - internal
procedure 10.05.03.00 no. 7)Exclude risk of pyrogen contamination
Respect patient’s health and avoid
irritation
BACTERIAL ENDOTOXIN
QUANTIFICATION (LAL TEST)
Farmacopea (routine control - internal
procedure 10.05.03.00 nos. 5 and 8)Exclude risk of pyrogen contamination
Respect patient’s health and avoid
irritation
ELASTOMER CLOSURESFarmacopea (routine control - internal
procedure 10.05.02.00 no. 22)
Evaluate conformity of closures for
aqueous preparations for parenteral
use
Ensure product safety
STERILITYFarmacopea (routine control - internal
procedure 10.05.04.00 no. 1)
Correspondence with safety
requisitesEnsure product safety
Main biochemical controls

64
Automatic, 100% check stations during assembly, impacting ontoproduct quality:
• Vision system checking useful length of the cannula• Vision system checking presence of the glue• Vision system checking patient tip integrity (absence of hooks)• Vision system checking patient tip bending after placing shield• Vision system checking cartridge tip bending• Vision system checking printing of data on the box• Sensor checking non-obstruction of the cannula• Sensor checking integrity of primary container• Sensor checking correct positioning of needle shield• Sensor checking box weight (100 pen needles per box)
The non-complying pieces are automatically discarded.
Assembling process:quality controls
65
KEY FACTS
• More than 50 years of experience in cannula and needles
manufacturing
• More than 5.500 millions pen needles manufactured so far
• Integrated, made in Italy production (ISO and FDA compliant)
• Innovation (32G, Extr3me sharpening, High Flow Thin Wall)
• 32G pen needle in 3 lengths
• Over 60 quality control tests
• Additional quality restrictions and quality level parameters

66
Ευχαριστώ!

67
means:
ExpertiseInnovationTechnology
Quality
68
• These new recommendations come from a 2-steps process:o the results of the second Injection Technique Questionnaire (ITQ)
survey (2008-2009), involving more than 4.300 insulin-injectingpatients with diabetes from 171 centers in 16 countries, making it one ofthe largest multi-center studies of its kind in diabetes. The outcomeswere then presented for review and revision to 127 experts from 27countries at the TITAN workshop in September 2009.
o a systematic literature analysis conducted for all peer-reviewedstudies and publications on injections in diabetes: an international groupof experts met regularly over a two-year period to review this literatureand draft the recommendations. Of 292 articles reviewed, 157 werefound to meet the criteria of relevance to the recommendations.
Injection techniques: the latest guidelines
69
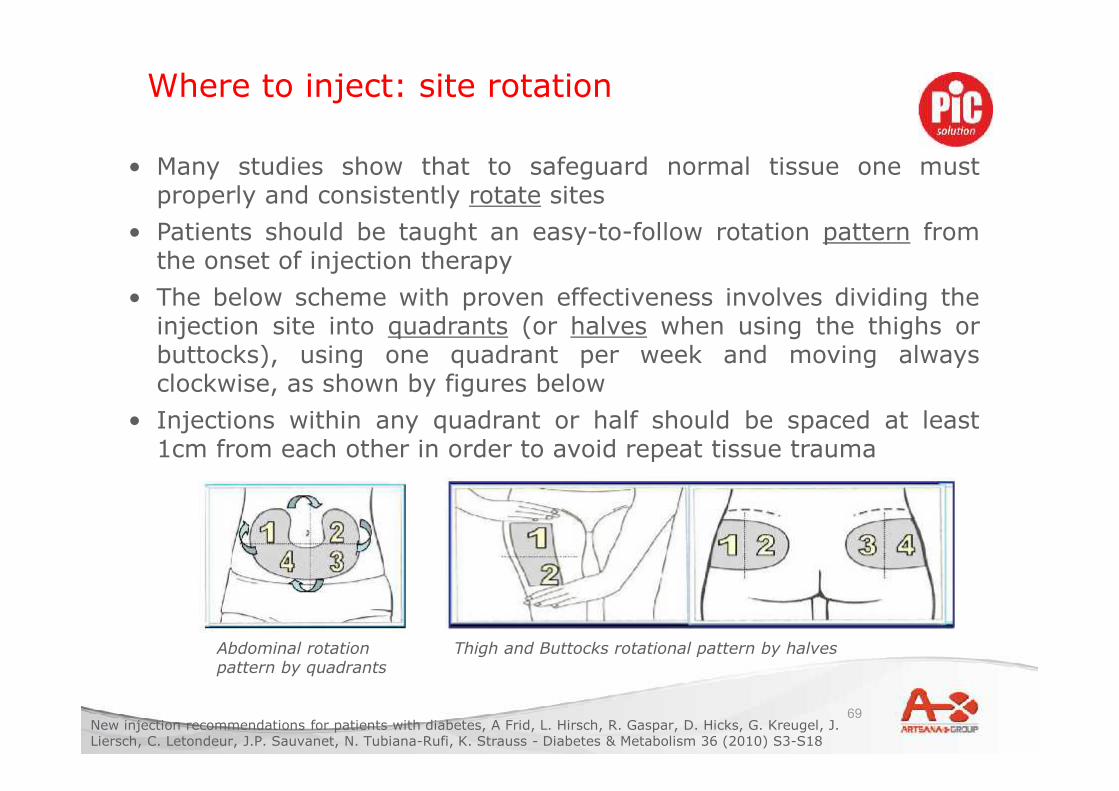
• Many studies show that to safeguard normal tissue one mustproperly and consistently rotate sites
• Patients should be taught an easy-to-follow rotation pattern fromthe onset of injection therapy
• The below scheme with proven effectiveness involves dividing theinjection site into quadrants (or halves when using the thighs orbuttocks), using one quadrant per week and moving alwaysclockwise, as shown by figures below
• Injections within any quadrant or half should be spaced at least1cm from each other in order to avoid repeat tissue trauma
Where to inject: site rotation
New injection recommendations for patients with diabetes, A Frid, L. Hirsch, R. Gaspar, D. Hicks, G. Kreugel, J.Liersch, C. Letondeur, J.P. Sauvanet, N. Tubiana-Rufi, K. Strauss - Diabetes & Metabolism 36 (2010) S3-S18
Abdominal rotationpattern by quadrants
Thigh and Buttocks rotational pattern by halves

70
The choice of the injection site is anessential element for the glycaemiacontrol, since there is (especially withfast insulin) a relevant variability of theabsorption speed (= passage intoblood) for non-analogue insulins.
From fastest to slowest:
abdomen, shoulder, buttock, thigh
Absorption speed depends also on thetype of insulin (human, analogues,rapid- or slow-acting). For example,soluble human insulins may have aslower absorption profile than rapid-acting analogs. The most rapidabsorption of soluble human insulins isin the abdomen, which should be thepreferred site.
Where to inject: absorption speed
Recommended injection sites
New injection recommendations for patients with diabetes, A Frid, L. Hirsch, R. Gaspar, D. Hicks, G. Kreugel, J.Liersch, C. Letondeur, J.P. Sauvanet, N. Tubiana-Rufi, K. Strauss - Diabetes & Metabolism 36 (2010) S3-S18
71
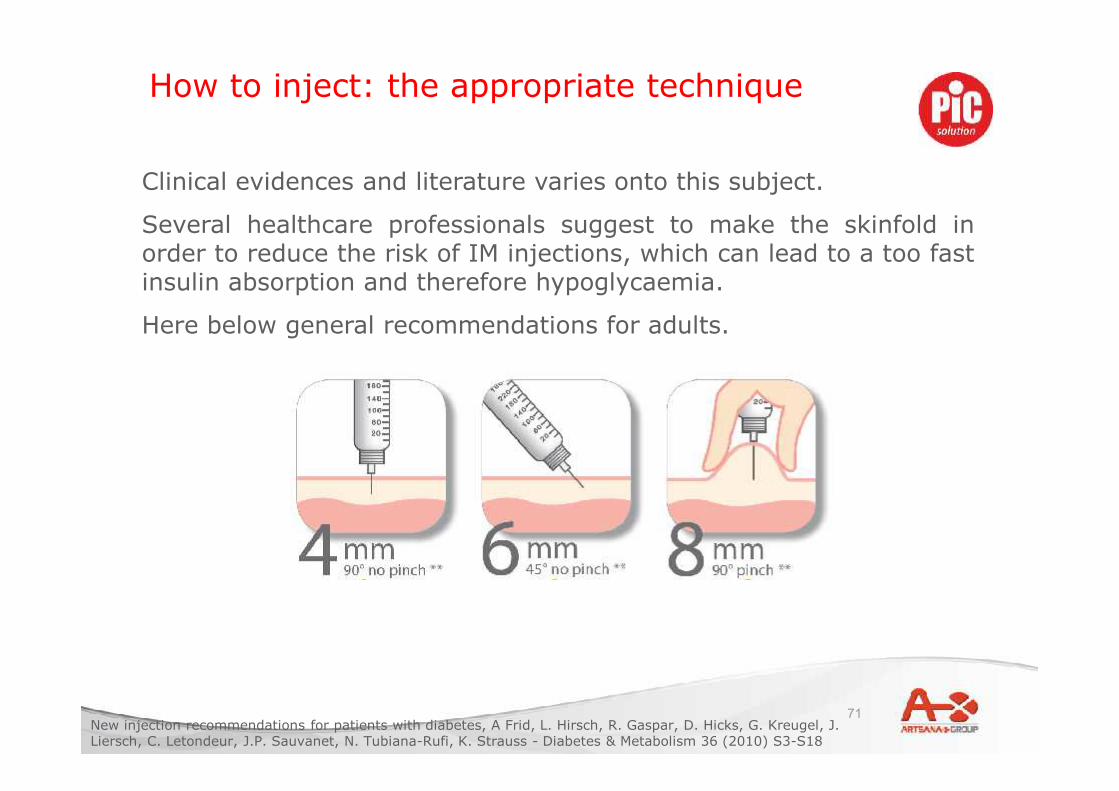
Clinical evidences and literature varies onto this subject.
Several healthcare professionals suggest to make the skinfold inorder to reduce the risk of IM injections, which can lead to a too fastinsulin absorption and therefore hypoglycaemia.
Here below general recommendations for adults.
How to inject: the appropriate technique
New injection recommendations for patients with diabetes, A Frid, L. Hirsch, R. Gaspar, D. Hicks, G. Kreugel, J.Liersch, C. Letondeur, J.P. Sauvanet, N. Tubiana-Rufi, K. Strauss - Diabetes & Metabolism 36 (2010) S3-S18
72
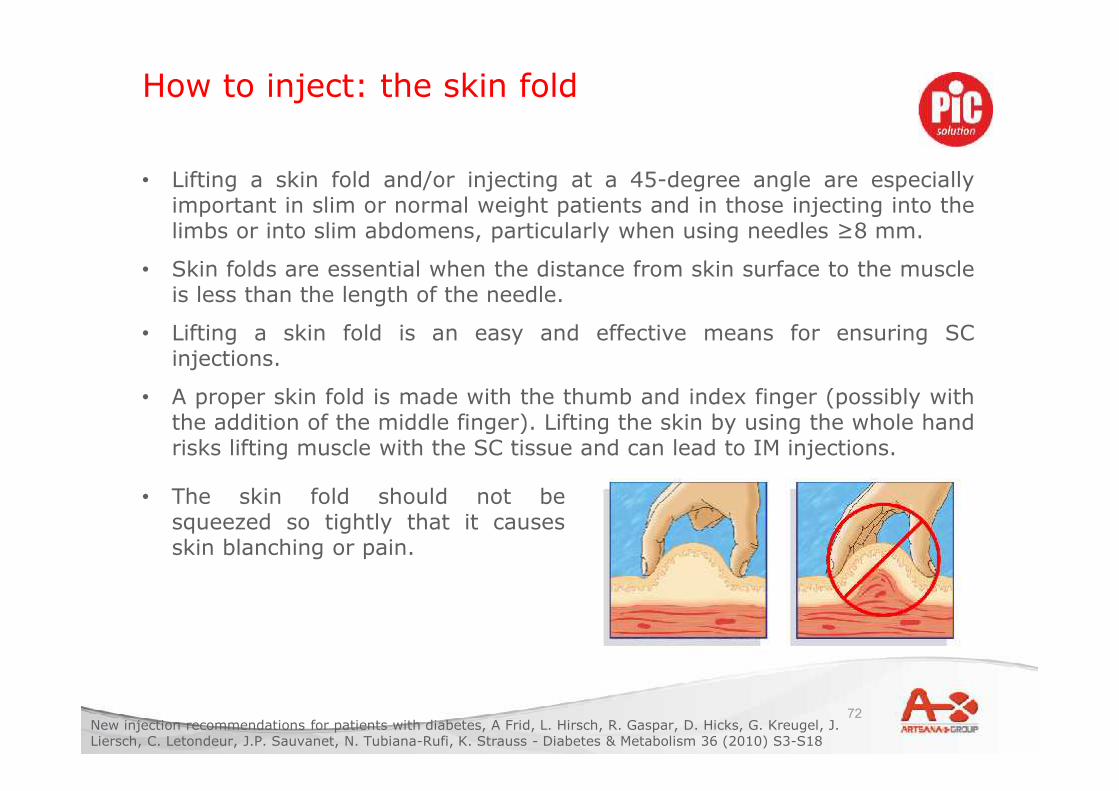
• Lifting a skin fold and/or injecting at a 45-degree angle are especiallyimportant in slim or normal weight patients and in those injecting into thelimbs or into slim abdomens, particularly when using needles ≥8 mm.
• Skin folds are essential when the distance from skin surface to the muscleis less than the length of the needle.
• Lifting a skin fold is an easy and effective means for ensuring SCinjections.
• A proper skin fold is made with the thumb and index finger (possibly withthe addition of the middle finger). Lifting the skin by using the whole handrisks lifting muscle with the SC tissue and can lead to IM injections.
How to inject: the skin fold
• The skin fold should not besqueezed so tightly that it causesskin blanching or pain.
New injection recommendations for patients with diabetes, A Frid, L. Hirsch, R. Gaspar, D. Hicks, G. Kreugel, J.Liersch, C. Letondeur, J.P. Sauvanet, N. Tubiana-Rufi, K. Strauss - Diabetes & Metabolism 36 (2010) S3-S18
73
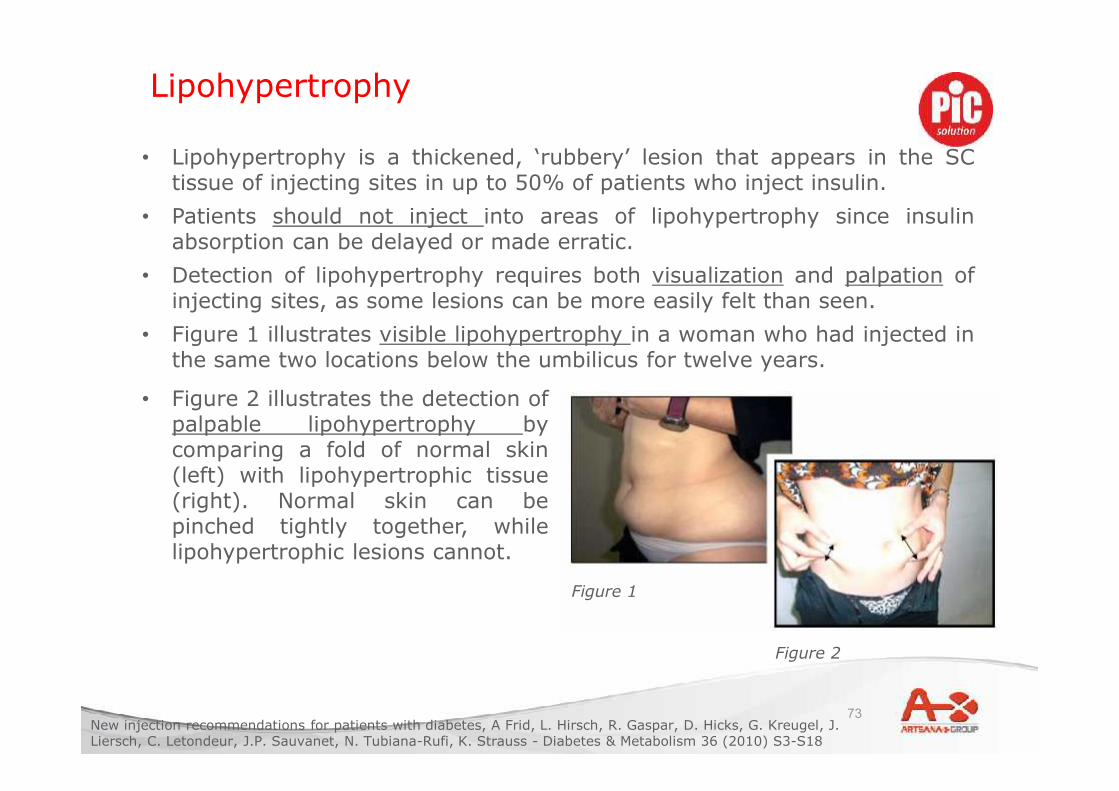
• Lipohypertrophy is a thickened, ‘rubbery’ lesion that appears in the SCtissue of injecting sites in up to 50% of patients who inject insulin.
• Patients should not inject into areas of lipohypertrophy since insulinabsorption can be delayed or made erratic.
• Detection of lipohypertrophy requires both visualization and palpation ofinjecting sites, as some lesions can be more easily felt than seen.
• Figure 1 illustrates visible lipohypertrophy in a woman who had injected inthe same two locations below the umbilicus for twelve years.
Lipohypertrophy
Figure 1
Figure 2
• Figure 2 illustrates the detection ofpalpable lipohypertrophy bycomparing a fold of normal skin(left) with lipohypertrophic tissue(right). Normal skin can bepinched tightly together, whilelipohypertrophic lesions cannot.
New injection recommendations for patients with diabetes, A Frid, L. Hirsch, R. Gaspar, D. Hicks, G. Kreugel, J.Liersch, C. Letondeur, J.P. Sauvanet, N. Tubiana-Rufi, K. Strauss - Diabetes & Metabolism 36 (2010) S3-S18
74
• Inject slowly and ensure that the plunger (syringe) or thumbbutton (pen) has been fully depressed.
• When using a pen, wait another 10 seconds after dose deliverybefore removing the needle in order to avoid leakage/reflux; thisensures full delivery of the injected dose.
• Massaging the site before or after injection may speed upabsorption and is generally not recommended.
• Tips for making injections less painful include:o Keeping insulin in use at room temperature, since cold
insulin can be more painful when injected;o If using alcohol, injecting only when the alcohol has dried
out;o Not injecting at hair roots;o Using a new needle at each injection.
Other recommendations
New injection recommendations for patients with diabetes, A Frid, L. Hirsch, R. Gaspar, D. Hicks, G. Kreugel, J.Liersch, C. Letondeur, J.P. Sauvanet, N. Tubiana-Rufi, K. Strauss - Diabetes & Metabolism 36 (2010) S3-S18
75
Fear and pain of injections:
• 94% of insulin users show symptoms of anxiety, distress or
phobia around blood and injury from injections (1).
• 75% of newly diagnosed children < 9 years old have a fear of
injections (3).
• 47% of people with diabetes say they would be more likely to
follow their prescribed insulin regimen if a product easing pain
and discomfort of injections was available (4).
• 33% of insulin users are afraid of their injections (2).
(1) Berlin I, Bisserbe JC, Eiber R, Balssa, N, Sachon C, Bosquet F, Grimaldi, A: Phobic symptoms, particularly the fear ofblood and injury, are associated with poor glycemic control in type 1 diabetic adults. Diabetes Care 1997;20:176–178
(2) Peyrot M, Rubin RR, Kruger DF, Travis LB: Correlates of insulin injection omission. Diabetes Care 2010;33:240-245(3) Howe CJ, Ratcliffe SJ, Tuttle A, Dougherty S, Lipman TH: Needle anxiety in children with type 1 diabetes and their
mothers. AM J Matern Child Nurs 2010;36:25-31(4) AADE Injection Impact Survey, 2007
Insulin injection and patient’s compliance
76
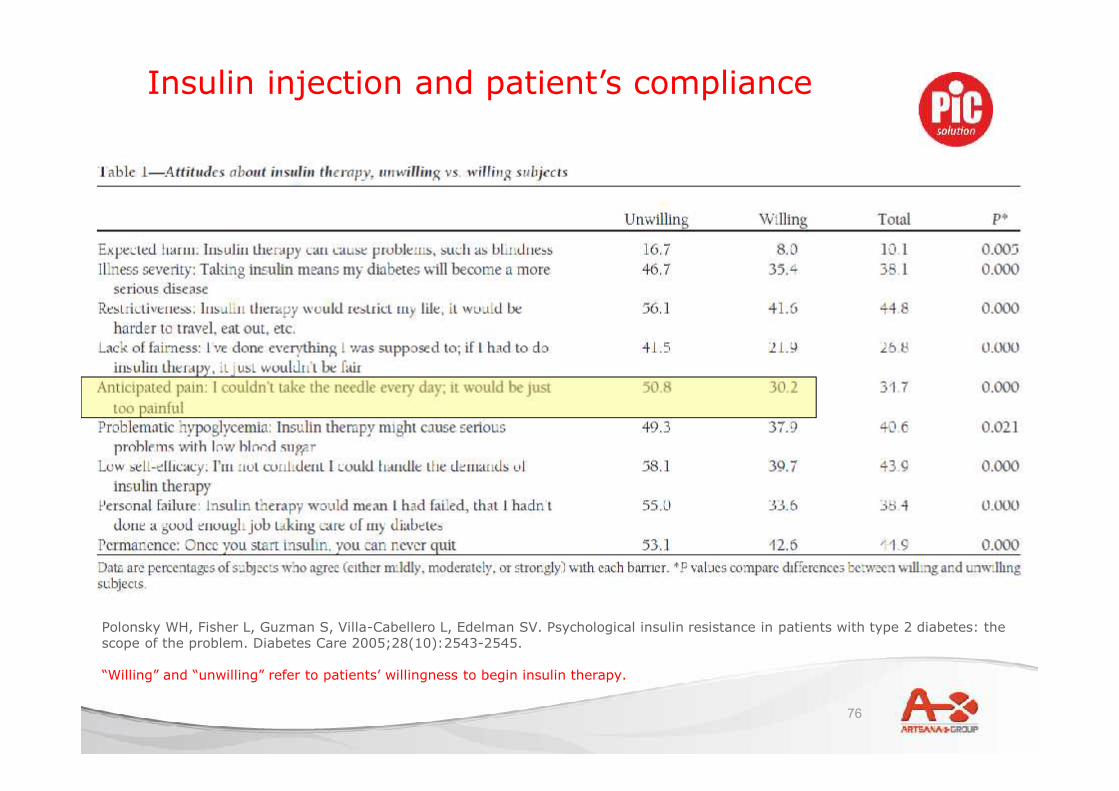
Polonsky WH, Fisher L, Guzman S, Villa-Cabellero L, Edelman SV. Psychological insulin resistance in patients with type 2 diabetes: thescope of the problem. Diabetes Care 2005;28(10):2543-2545.
“Willing” and “unwilling” refer to patients’ willingness to begin insulin therapy.
Insulin injection and patient’s compliance

77
UK data from the 2009 Injection Technique Questionnaire (ITQ)survey of people with diabetes using insulin (*) showed that:• 75% did not follow any site rotation routine.• 60% had not changed their needle size since starting therapy.• 54% reported lipohypertrophy at some time in their life.• 45% experienced bleeding or bruising.• 43% released the skin fold too soon.• 41% failed to re-suspend their cloudy insulin adequately.• 28% admitted injecting into areas of lipohypertrophy.• 17% were using an incorrect technique for lifting a skin fold.• Only 41% reported frequent and adequate inspection of their
injection sites.
The importance of the education:patients’ mistakes
• D. Hicks, The UK & Ireland experience, TITAN 2009 congress
78
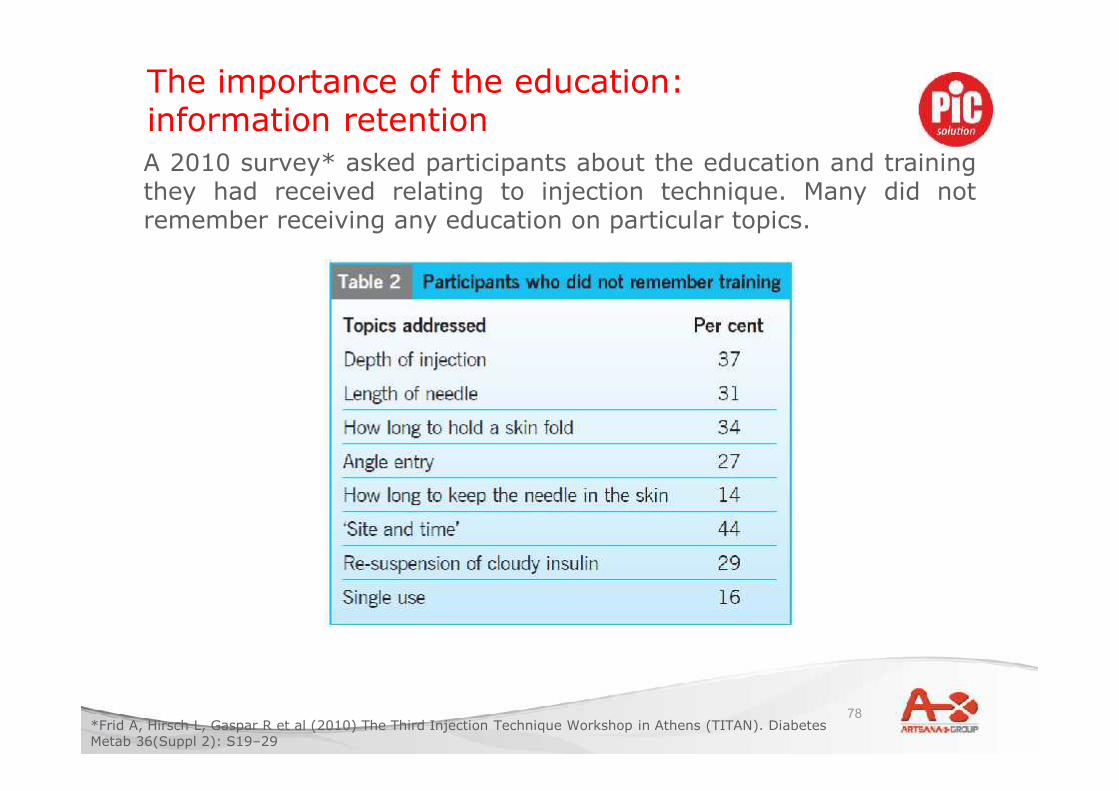
A 2010 survey* asked participants about the education and trainingthey had received relating to injection technique. Many did notremember receiving any education on particular topics.
The importance of the education:information retention
*Frid A, Hirsch L, Gaspar R et al (2010) The Third Injection Technique Workshop in Athens (TITAN). DiabetesMetab 36(Suppl 2): S19–29