Embed Size (px)
Citation preview

How Networks Can Help
Dr Lynda BrookMacmillan Consultant in Paediatric Palliative Care,
Liverpool
Chair Northwest Region
Children and Young People’s Palliative Care Network

How networks can help Shared aims and objectives from
Aiming High for Disabled Children
Better Care: Better Lives
What are managed clinical networks?
Specific projects and initiatives Information
Involvement of the child and family
Joint interagency working
Response to changing needs
Next steps…
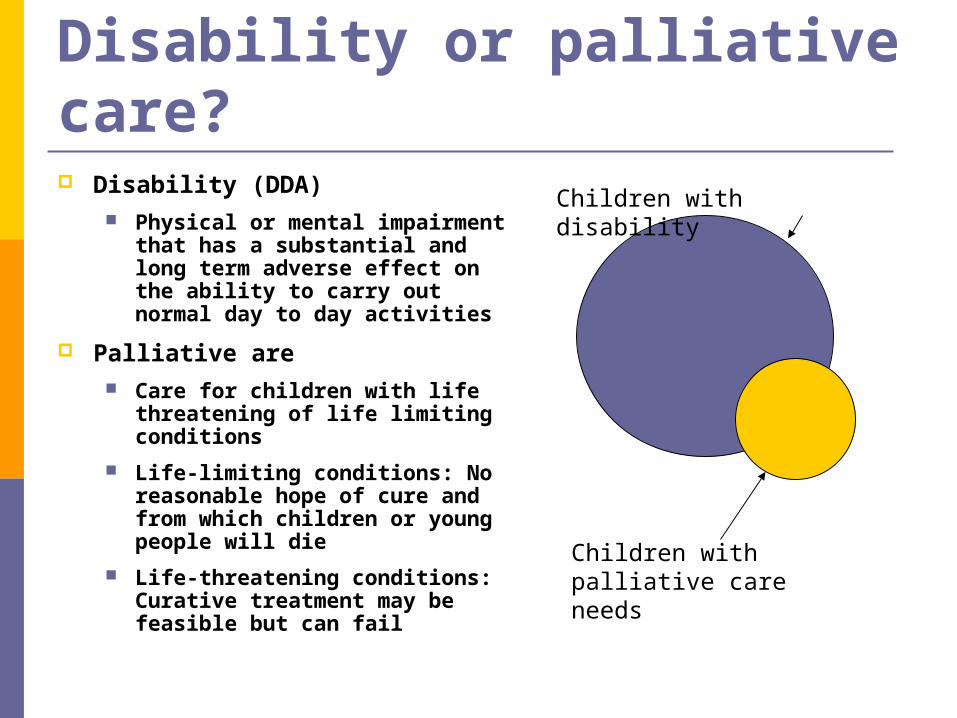
Disability or palliative care? Disability (DDA)
Physical or mental impairment that has a substantial and long term adverse effect on the ability to carry out normal day to day activities
Palliative are Care for children with life
threatening of life limiting conditions
Life-limiting conditions: No reasonable hope of cure and from which children or young people will die
Life-threatening conditions: Curative treatment may be feasible but can fail
Children with disability
Children with palliative care needs
Aiming High for Disabled ChildrenBetter Care Better Lives Shared aims and objectives
Information
Involvement of the child and family
Joint interagency working
Response to changing needs

Shared aims and objectives Information
Prevalence of children with disability and palliative care needs
Information on universal and targeted services For children, families and professionals Health, voluntary [independent sector] and local
authority: children’s services, housing, leisure, transport
How and when to access services How services are commissioned, delivered and
allocated
Demand for services and patterns of service use Short break care
Involvement of the child and family Input into shaping & planning
services: feedback & user views
Choice in place of care/care in setting of choice
Needs assessment: fair, understandable eligibility criteria
Care planned and delivered in full consultation with child, family & service providers
Joint interagency working Health, education, local authority children’s
services, voluntary sector
Primary, secondary & tertiary healthcare settings
Universal, targeted and specialist services
Commissioning and delivery of services
Pooled or aligned budgets or resources: value for money
Joint workforce strategy
Response to changing needs Joint [interagency] assessment of need
Key-worker
Range of services designed to meet identified needs of service users End of life care/ advanced care planning Short break support as preventative not crisis service Menu of short break options
Daytime, overnight Home, away from home Appropriate provision for special needs including moving
and handling, behavioural problems, palliative care
Transition to adult services
Sustainable care and support
What are managed clinical networks?
Interdisciplinary network Representing providers and users of services for a
particular client group
Over a defined geographical area
Recognized by the Department of Health [1] as an exemplary model for informing both commissioning and delivery of palliative care services for children and young people
[1] Better Care: Better Lives DH Feb 2008

Managed clinical networks in children’s palliative care
Bring together representatives of Children, young people with palliative care needs and their
families, Commissioners and providers of children’s palliative care
NHS, Voluntary sectors, Social Services and Education, across Primary, secondary and tertiary care Universal, targeted and specialist services
With the aim of improving co-ordination availability and delivery of palliative care.
Also available to provide advice and expert opinion on a wide range of service issues including
Service configuration, Interdisciplinary team working and Guidelines for best practice.
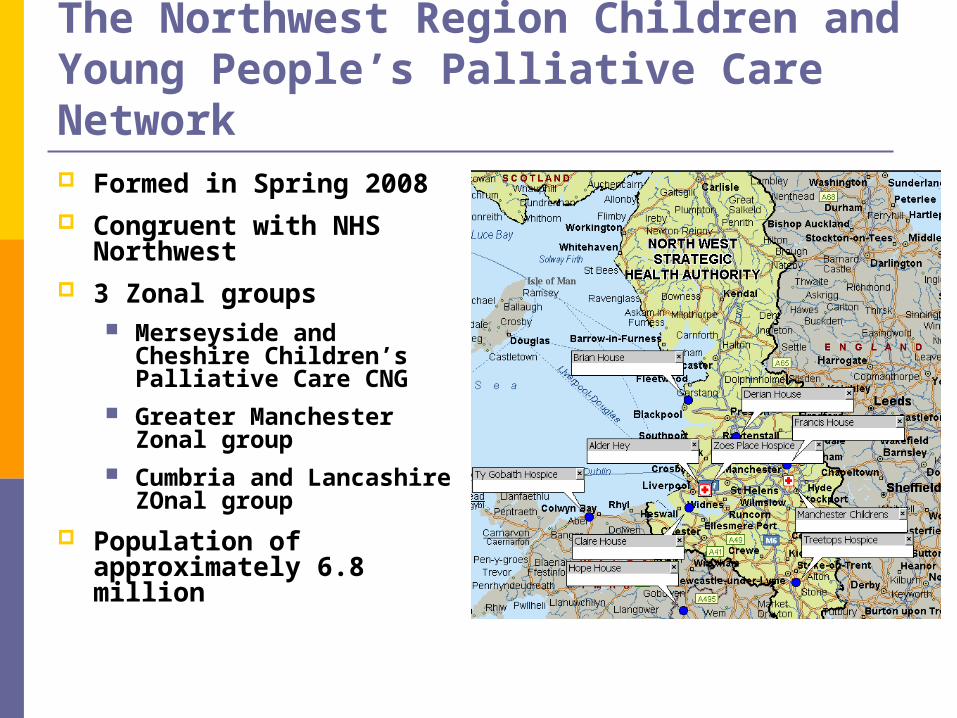
The Northwest Region Children and Young People’s Palliative Care Network Formed in Spring 2008 Congruent with NHS
Northwest 3 Zonal groups
Merseyside and Cheshire Children’s Palliative Care CNG
Greater Manchester Zonal group
Cumbria and Lancashire ZOnal group
Population of approximately 6.8 million
How networks can help Information
Children’s palliative care minimum dataset [MDS]
Children’s palliative care services mapping
Children’s palliative care services directory
Involvement of the child and family Patient and parent representation; links into
patient and parent groups
Evaluation of services
Planning of services
How networks can help Joint interagency working
Planning & commissioning of services
Delivery of services
Effective communication and partnership working
Response to changing needs Education and training
Ensuring services are fit for purpose
End of life care
Standards for key-working and interagency working
Information Children’s palliative care minimum dataset
(MDS) to identify Children with life threatening and life limiting
conditions Patterns of referral to children’s palliative care
services
20-item minimum dataset collected When a child is referred to a service When a child dies
Implementation Initial pilot and ongoing rollout in Merseyside and
Cheshire Funding for national roll-out
Children’s Palliative Care MDS First year pilot 2005 – 6 121 referrals for 103 children in Wirral and West
Cheshire CNS anomaly (34%),
Muscle disease (15%)
Cancer (12%)
100 notifications were received for 87 deaths 63% children were under 5 years at death
Children with cardiac conditions were younger, not known to palliative care services and most likely to die in hospital
Overall 190 children were identified
An estimated 23 children were in their last 6 months of life at any one time
Information Children’s palliative care services
mapping To provide a directory of services for
professionals and families
To facilitate effective, networked, co-ordinated, child and family-centred, provision of care
To facilitate needs based assessment and inform strategic planning of children’s palliative care services
Involvement of the child and family Short break care audit
Joint project between Liverpool health, local authority children’s services and education
Questionnaire to families of children with complex healthcare needs who would be eligible for short break care
Families identified through Children’s community nursing team
Specialist palliative care team
Children with disabilities social work team
Children’s hospices
Short break care audit 97 eligible children identified: 44% replied
9% children identified only through school
Although 53% families reported having an assessment of short breaks only 15% families reported awareness of a menu of short break care options
Most families were aware of hospice but only half of these accessed this service
24% families accessed care at home but 55% were not aware of this option and 18% had been offered care at home but declined.
68% were aware of direct payments but only 17% families reported using them

Joint interagency working
Locally based multidisciplinary teams Named lead paediatrician
for palliative care identified for majority of acute and community services
Regular clinical meetings Alder Hey SPC team
CCN teams
Where possible: named paediatricians for palliative care
Response to changing needs Equity of access to children’s community
nursing (CCN) Central to development of multidisciplinary
community teams, key-working and end of life care at home
Current configuration of many teams too small to allow sustainable 24 hour 7 day a week cover
Differences in management and funding structure prevent effective partnership working
Work to develop core standards against which services can be benchmarked

Response to changing needs Transition to adult services
Lack of appropriate services in the adult sector, particularly for young people with complex healthcare needs and severe learning difficulties
Active engagement of adult services Primary, secondary and tertiary healthcare
Multiple specialties: neurology, respiratory, adult learning difficulties
Aim to develop a multispecialty multidisciplinary team
Links with voluntary sector and social care
Response to changing needs Liverpool care pathway for the dying
child (LCP) Integrated care pathway
Practical advice and support for professionals caring for dying children
Versions for home, hospital or hospice
Developing and sharing best practice across the Network

Response to changing needs To develop a Network-wide
coordinated multidisciplinary education program for paediatric palliative care
Specific palliative care education based around core competencies for CCNs and DNs
Carers and support workers

Next steps … Sustainable support and commitment
More active involvement of commissioners
Closer working between health and social care Transferrable skills?
Shared education and training?
Working together Common aims
Sharing and learning
Next steps… Strategy and workplan
Identify and overcome barriers to meeting needs of children and families
Learning from experience and example
SMART objectives
Standards and benchmarking
Different footprints Local team or service
PCT/Local authority
Collective commissioning and delivery across partner PCTs and Local Authorities
Northwest Region
Summary Children with significant disability and children with
palliative care needs are a small but important group with significant overlapping health and social needs
The numbers and needs of these children mean that collective arrangements for commissioning and delivery of services across a wider footprint than PCT or local authority is required
Networks have a pivotal role in joining commissioners and providers of services across health, social care, education, statutory and voluntary sectors in order to meet these needs





























