Embed Size (px)
Citation preview
Advancing Behavioral Health Care Management: How Intelligent Integration Improves Clinical Case and Health Plan Performance
What is Intelligent Integration?
Best Practices White Paper | Medical Affairs Team, ODH, Inc. | April, 2017
• Learn the five best practice steps of successful population health management
• Uncover strategies to improve health plan performance through optimized behavioral health care delivery
• Explore intelligent integration and its critical role in managing high-risk behavioral health populations
• Find out how population segmentation contributes to improvedhealth outcomes and reduced overall health care costs for high-risk, high-need members
1
TableOfContents:
I. ExecutiveSummary
II. TheImpactOfBehavioralHealthConditionsOnHealthStatus&HealthCareResourceUse
III. TheRoleOfBehavioralHealthOptimizationInPopulationHealthManagement
IV. BehavioralHealthRiskAssessmentForPopulationSegmentation:TheFirstStepInBehavioralHealthOptimizationInPopulationHealthManagement
V. CaseExampleOfBehavioralHealthRiskAssessmentInPopulationSegmentationInitiatives
VI. References

2
I. ExecutiveSummary
Thehealthcaresystemhaslongrecognizedthehumanandfinancialimpactofcomorbidbehavioralhealthandphysicalhealthconditions.Behavioralhealthconditionshaveapronouncedimpactonhealthstatus,healthoutcomes,andresourceutilization.Individualswithphysicalhealthconditionscompoundedbybehavioralhealthissuesaremorelikelytobe“super-utilizers”ofhealthcareresources.1Thosewithundiagnosedand/oruntreateddisordersaremorelikelytobehospitalizedandtousetheemergencydepartment.2Inaddition,lackofintelligentintegrationandcarecoordinationincreasescomplicationsandpoorhealthoutcomes.
Healthplans,providers,policymakers,andadvocateshaveidentifiedandsoughtintegratedbehavioralhealthandphysicalhealthcareasapriorityfordecades.Fortunately,theadventofinnovativemodels,useofdataanalytics,andenablingtechnologyisputtingthisheretoforeelusivegoalwithinreach.
Today,healthplanmanagersareadoptinginnovativestrategiesfocusedonidentifyingandengagingtargetedpopulationsofundiagnosedandhigh-risk/highneedindividuals;expandingaccesstoandsupportingadherencetoappropriatetreatment;coordinatingcareforpopulationswithcomorbidconditions;anddevelopingquality-basedproviderpartnershipstooptimizedeliveryofvalue-basedcare.Examplesofthesestrategiesincludeinnovativeandspecializedintegratedcarecoordinationinitiatives,personalhealthnavigatorprograms,enhancedaccesstotech-enabledservices,psychotropicmedicationreviewinitiatives,specializedemergencydepartmentdiversionprograms,andprovidergainsharingwithincentivesfocusedoninnovativetreatmentmodelsandoutcomes.
Thesestrategiesrequiretheabilitytoidentifyandsegmentpopulations,definepopulationspecifictherapeuticapproachesandvenues,enablecarecoordination,monitortreatmentadherence,andidentifyindividualsforspecifictargetedinterventions.Thispracticeofintelligentintegration–incorporatingpopulationsegmentationbasedonbehavioralhealthriskassessment–isafoundationaltoolinabestpracticesapproachtopopulationhealthmanagement.
Whencombined,clinicalinnovationandtechnologybecomeapowerfultoolforaggregating,analyzingandunderstandinghealthdata,whichmayleadtoimprovedpopulationhealth.
3
$4,121$6,389
$8,780$11,541
$26,286
$0
$5,000
$10,000
$15,000
$20,000
$25,000
$30,000
OneBehavioralHealthDisorder
1Addi`onalCondi`on
2Addi`onalCondi`ons
3Addi`onalCondi`ons
4Addi`onalCondi`ons
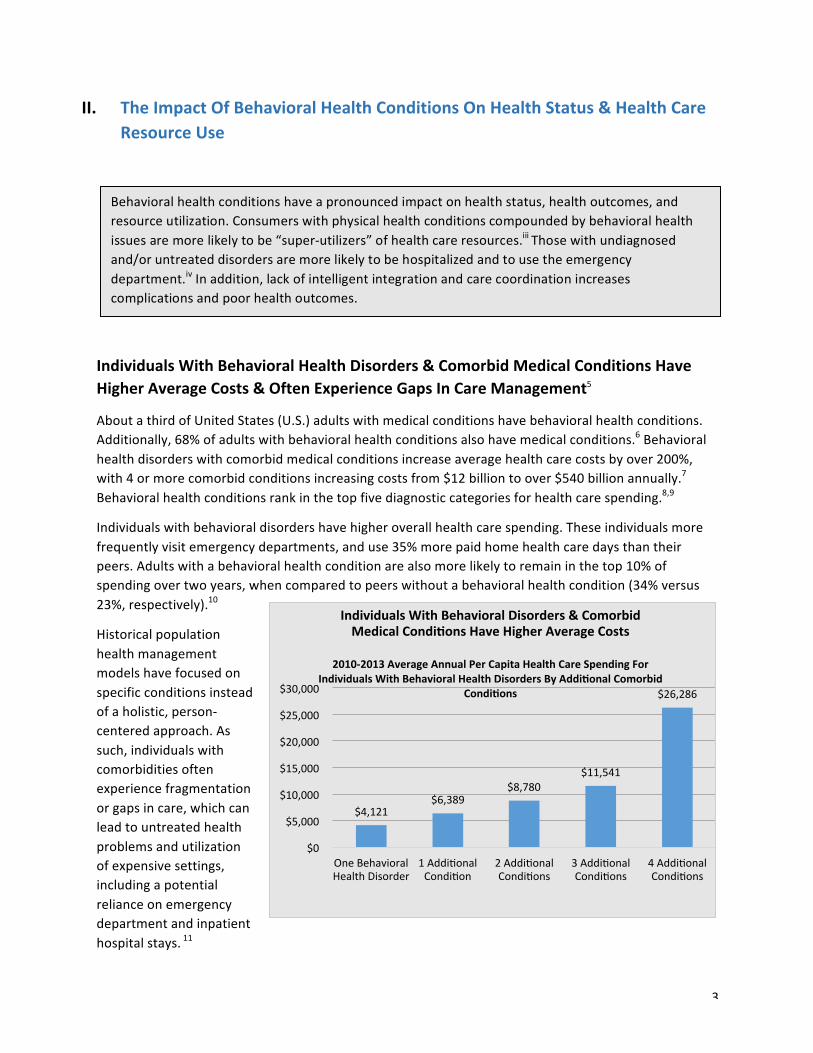
IndividualsWithBehavioralDisorders&ComorbidMedicalCondi?onsHaveHigherAverageCosts
2010-2013AverageAnnualPerCapitaHealthCareSpendingFor
IndividualsWithBehavioralHealthDisordersByAddi?onalComorbidCondi?ons
II. TheImpactOfBehavioralHealthConditionsOnHealthStatus&HealthCareResourceUse3,4
IndividualsWithBehavioralHealthDisorders&ComorbidMedicalConditionsHaveHigherAverageCosts&OftenExperienceGapsInCareManagement5
AboutathirdofUnitedStates(U.S.)adultswithmedicalconditionshavebehavioralhealthconditions.Additionally,68%ofadultswithbehavioralhealthconditionsalsohavemedicalconditions.6Behavioralhealthdisorderswithcomorbidmedicalconditionsincreaseaveragehealthcarecostsbyover200%,with4ormorecomorbidconditionsincreasingcostsfrom$12billiontoover$540billionannually.7Behavioralhealthconditionsrankinthetopfivediagnosticcategoriesforhealthcarespending.8,9
Individualswithbehavioraldisordershavehigheroverallhealthcarespending.Theseindividualsmorefrequentlyvisitemergencydepartments,anduse35%morepaidhomehealthcaredaysthantheirpeers.Adultswithabehavioralhealthconditionarealsomorelikelytoremaininthetop10%ofspendingovertwoyears,whencomparedtopeerswithoutabehavioralhealthcondition(34%versus23%,respectively).10
Historicalpopulationhealthmanagementmodelshavefocusedonspecificconditionsinsteadofaholistic,person-centeredapproach.Assuch,individualswithcomorbiditiesoftenexperiencefragmentationorgapsincare,whichcanleadtountreatedhealthproblemsandutilizationofexpensivesettings,includingapotentialrelianceonemergencydepartmentandinpatienthospitalstays.11
Behavioralhealthconditionshaveapronouncedimpactonhealthstatus,healthoutcomes,andresourceutilization.Consumerswithphysicalhealthconditionscompoundedbybehavioralhealthissuesaremorelikelytobe“super-utilizers”ofhealthcareresources.iiiThosewithundiagnosedand/oruntreateddisordersaremorelikelytobehospitalizedandtousetheemergencydepartment.ivInaddition,lackofintelligentintegrationandcarecoordinationincreasescomplicationsandpoorhealthoutcomes.
4
IndividualsWithBehavioralDisordersOftenHavePoorOutcomesDespiteBeing“Super-Utilizers”OfHealthCareResources12,13
Individualswithabehavioralhealthconditionaremorelikelytobelabeled“super-utilizers”duetotheprevalenceofmultipleillnesses,uncoordinatedandfragmentedcare,andrelatedhighresourceuse.14
Super-utilizersarethe5%ofthepopulationwhoconsumeadisproportionateamountofhealthcareresources.15Thereisauniqueopportunitytousetechnologytoidentifyfactorstopredictwhoislikelytobeclassifiedasasuper-utilizer.Inmanypopulations,the5%grouputilizesasmuchas50%oftheresources,16furtherunderscoringtheimportanceofknowingwhichmembersareinthe5%.Morethan80%ofMedicaidsuper-utilizershaveacomorbidmentalillness.17Inaddition,mentalhealthandsubstanceabusedisordersareamongthetenmostfrequentdiagnosesforsuper-utilizers,regardlessofpayersource.18
Despitehigherutilizationofhealthcareresources,theimpactofuncoordinatedandfragmentedcareultimatelyincreasesthelikelihoodofpoorhealthoutcomesfortheseindividuals.19Foranypopulationhealthprogramtobesuccessful,identificationandmanagementofthissuper-utilizergrouparekey.Riskstratificationandpopulationsegmentationarecriticaltoidentifyingwhotheyare,whatservicestheyuse,andeffectivestrategiesfordiseasemanagementandrecovery.
UntreatedBehavioralHealthConditionsHinderTreatment&LeadToIncreasedUseOfHighCostServices20
Theimpactofbehavioralhealthconditionsonhealthcareuseandspendingislikelyunderestimatedsincebehavioralhealthconditionsoftengoundiagnosedoruntreated.21Individualswithuntreatedbehavioralhealthconditionssufferfromdiminishedhealthstatus,andaremorelikelytousehigh-costservices.22,23
Untreatedbehavioralhealthconditionsresultinrecurrenceofacutecrises,includingadversesocialoutcomessuchaslosthousingandpotentialincarceration,whichrequireimmediateintervention.24Recurringacutecrisesalsoresultinapatternofindividualsseekingcareinhospitalemergencydepartmentsandinpatientunits,twohigh-costlocations.In2013,themostrecentyearforwhichthereisfederaldata,emergencydepartmentshadanestimated640,000visitsforsymptomsofschizophreniaorotherpsychosis.25
Almost60%ofindividualssufferingfromdepression,oneofthemostcommonbehavioralhealthdiagnoses,havenotreceivedtreatmentwithinthelastyear—andtwo-thirdsofdepressioncasesgoundiagnosedinprimarycaresettings.26,27Mooddisorderslikedepressionarethethirdmostcommoncauseofhospitalizationamongnon-elderlyadults.28
Substanceusedisordersalsopresentapopulationhealthmanagementchallenge.Only11%ofthosewithasubstanceusedisorderreceivetreatment.29Individualswithuntreatedsubstanceusedisorderswere46%morelikelytoreportanemergencydepartmentvisitinthepastyear,and81%morelikelytobeadmittedtothehospitalduringanemergencyroomvisit.30,31

5
LackOfIntelligentIntegration&CareCoordinationResultsInPoorerOutcomes&HigherCosts
Traditionally,healthcaresystemshavefocusedonmanagementofspecificdiseasestatesinsteadofusingintelligentintegrationandcarecoordination.Agrowingbodyofknowledgeabouttheeffectsofcomorbidconditionshascreatedgrowinginterestincoordinatedcaremanagement.Therearemultipleopportunitiesforimprovedcarecoordinationforindividualswithcomorbidities.
Thefirstistoaddressthemedical,behavioral,andsocialneedsofbehavioralhealthindividuals.Theabsenceofcoordinated,person-centeredcaremanagementforindividualswithcomorbidbehavioralhealthconditionsleadstomisseddiagnoses,poorfollow-up,andgapsincare.32Forexample,whenschizophreniaisleftuntreated,complications–suchassuicideandalcoholabuse–aresignificantlyincreased.Currently,thesuiciderateforschizophreniaisbetween5%and10%,whichissignificantlyhigherthanthegeneralpopulation.33Estimatesputtherateofexcessiveuseofdrugsoralcoholat50%ofthatpopulation,andnicotineuseatamuchhigherrate(60%to65%)thanthegeneralpopulation(15%).34,35,36Socialproblems,suchaslong-termunemployment,poverty,incarceration,andhomelessness,aremorecommonforindividualswithseriousmentalillness(SMI),whichincludesschizophreniaandmajordepressivedisorder.37Forindividualswithapoorlymanageddiagnosis,allofthesefactorscontributetoanaveragelifeexpectancythatis13to30yearsshorterthanforthosewithoutthediagnosis.38
Appropriatebehavioralhealthdiagnosis,treatment,andcarecoordinationarealsoessentialforthosewithphysicalhealthconditionscompoundedbybehavioralhealthissues.Thisisespeciallycriticalforchronicconditionswheremedicationadherenceandotherbehavioralfactorsdirectlyimpactoutcomes.
Forexample,thereisa200%highermortalityforindividualswithdiabetesanddepressioncomparedtothosewhoonlyhavediabetes.Thispopulationalsohasa2-3foldincreasedriskoffuturecardiaceventsforindividualswithcoronaryarterydisease(CAD)anddepressioncomparedtothosewithout.39Recentstudieshavealsoshownthatindividualswithmajordepressionwhoarerecoveringfromstrokesorheartattackshaveamoredifficulttimemanagingtheirillness,andhaveahigherriskofdeathinthefirstfewmonthsafteraheartattack.40
Onecurrentmeasureofsystemperformanceforcarecoordinationispromptcommunity-basedfollow-upafterdischargefromhospitalizationforabehavioralhealthdiagnosis.CurrentHealthcareEffectivenessDataandInformationSet(HEDIS)scoresshowthatmorethan47%ofcommercially-insuredindividuals,55%ofMedicaidenrollees,and64%ofMedicareenrolleesdidnotreceivefollow-upcarewithin7days.41Thislackoffollow-upcausesagapinthecarecontinuum,andcanpotentiallyleadtorelapse,crisis,orreturningtotheemergencydepartmentandhospitalforcare.42
Summary
Behavioralhealthconditionshaveapronouncedimpactonhealthstatus,healthoutcomes,andresourceutilization.Individualswithphysicalhealthconditionscompoundedbybehavioralhealthissuesaremorelikelytobesuper-utilizersofhealthcareresources.43Thosewithundiagnosedand/oruntreateddisordersaremorelikelytobehospitalizedandtousetheemergencydepartment.44Inaddition,lackofintelligentintegrationandcarecoordinationincreasesthelikelihoodofcomplicationsandpoorhealthoutcomesforindividualswithchronicconditions.Withgrowingevidenceaboutthese
6
effects,payersandhealthplansneedenhancedtoolstooptimizetheirbehavioralhealthdeliverysystem.45
III. TheRoleOfBehavioralHealthOptimizationInPopulationHealthManagement
Withthegrowingunderstandingoftherelationshipbetweenindividualbehavioralhealthconditionsandhealthcareresourceuse,healthplansandpayersareadoptingawiderangeofstrategiestooptimizetheperformanceofthebehavioralhealthsystemtoimproveindividualoutcomes.46Thiswiderangeofstrategiesisfocusedonaccess,engagement,qualityimprovement,andcarecoordination.Toolswhichprovideenhancedanalyticcapabilities,suchasthosewhichallowforaccuratepopulationsegmentation,arecriticaltothesuccessoftacticsfocusedonoptimizingthebehavioralhealthservicesystem.
Healthplansareadoptinginnovativestrategiesfocusedonimprovingtheeffectivenessofbehavioralhealthservices.Includedinthesestrategiesarethosewhichincreaseengagement,improveaccess,andensurequality.Strategiesforimprovingcoordinationofcareforpopulationswithcomorbidconditionshavebeenofaparticularinterest. Moreandmoreresearchisshowingalinkbetweencarecoordinationandvalue.
Effectivestrategiesrequiretheabilitytoidentifyandsegmentpopulations,definepopulation-specifictherapeuticapproachesandvenues,enablecarecoordinationandmonitortreatmentadherence,aswellasidentifyindividualsforspecifictargetedinterventions.Thispracticeofintelligentintegrationincorporatingpopulationsegmentationbasedonbehavioralhealthriskassessmentisafoundationaltoolinthebestpracticesapproachtopopulationhealthmanagement.
7
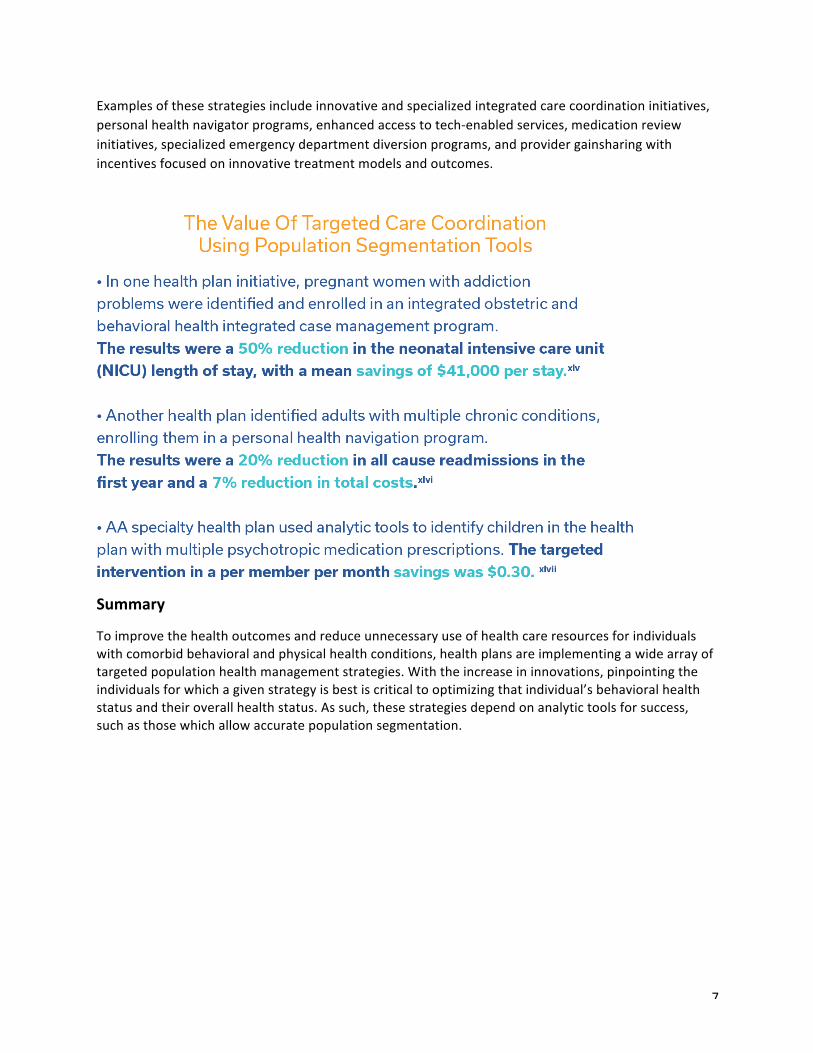
Examplesofthesestrategiesincludeinnovativeandspecializedintegratedcarecoordinationinitiatives,personalhealthnavigatorprograms,enhancedaccesstotech-enabledservices,medicationreviewinitiatives,specializedemergencydepartmentdiversionprograms,andprovidergainsharingwithincentivesfocusedoninnovativetreatmentmodelsandoutcomes.
Summary47
Toimprovethehealthoutcomesandreduceunnecessaryuseofhealthcareresourcesforindividualswithcomorbidbehavioralandphysicalhealthconditions,healthplansareimplementingawidearrayoftargetedpopulationhealthmanagementstrategies.Withtheincreaseininnovations,pinpointingtheindividualsforwhichagivenstrategyisbestiscriticaltooptimizingthatindividual’sbehavioralhealthstatusandtheiroverallhealthstatus.Assuch,thesestrategiesdependonanalytictoolsforsuccess,suchasthosewhichallowaccuratepopulationsegmentation.
8
IV. BehavioralHealthRiskAssessmentForPopulationSegmentation:TheFirstStepInBehavioralHealthOptimizationInPopulationHealthManagement
Proactivelysupportingtheneedsofhigh-riskindividualsiskeytoimprovingpopulationhealthandreducingunnecessaryhealthcarespending.Foramaximumreturnonstrategiestosupporttheseindividuals,accurateandtimelymatchingofspecificindividualstospecificinterventionsisessential.Forsuccessfulpopulationhealthmanagement,findingtheappropriatestrategy-individualmatchisthegoalofpopulationsegmentationusingbehavioralhealthriskassessment.
ThePopulationHealthManagementFramework
Populationhealthsegmentationhappenswithintheoverallcontextofbestpracticepopulationhealthmanagement.Broadly,thepopulationhealthmanagementframeworkincorporates:50,51
• Definingthepopulationandproblemfirst.Forexample,apopulationmaybedefinedasindividualswithchronicmedicalconditionswhohavecomorbidSMI.Theproblemisdisease-based,fragmented,uncoordinatedcareresultinginsub-optimaloutcomesfortheindividualandsubstantiallyhighercosts.
• Leveragingthepowerofclinicalandfinancialdatafrommultiplesystems.Thisdatahelpsidentifywhichspecificindividualsfallintothedefinedpopulation;gaugetheprevalenceofthedefinedproblemamongthispopulation;observeadditionalbarriers,gaps,unmetneeds,andrisksexperiencedbythedefinedpopulation;andinformtheadoptionofcaremanagementstrategiestomeetthegaps,needs,andrisksobserved.
• Transformingdataintoactionableinformation.Informaticsanddataanalytictoolsorganizeaggregateddatasetsintoactionableinformationtodrivepopulationhealthstrategyandempowerthecaremanagementprocess.Informationiseffectivewhenitistransparentandaccessibleacrossthecareteam;timely,allowingaswiftreactiontochangingrisks;andrelevanttospecificquestionsthatinformclinicaldecision-making.Inthisbestpracticeapproach,greaterinformationtransparencycreatesaccountability.
• Makinginformation-drivenclinicaldecisions.Atitsfoundation,populationhealthmanagementrequirestheuseofinformationtopredictfuturerisks,andthenrequiresthedevelopmentofcaremanagementapproachesthatmitigatethoserisks.Information-drivendecision-makingenhancescomprehensivecaremanagement,improvesthequalityofcare,improvesindividualhealthoutcomes,reducesavoidableandpreventableutilization,andhelpspredictfuturecosts.
• Continuouslyseekingimprovement.Populationhealthsegmentationstrategiesarepartofstandardpractice,andshouldbecontinuouslymeasuredforperformanceandsuccess.Thisincludesevaluatingriskassessmentmethodologyandriskidentification;timelinessofinformation;relevance
Toaddresstheneedsofhigh-riskconsumersinhealthplans,particularlythosewithcomorbidbehavioralhealthandphysicalhealthconditions,anumberofinnovativeapproachesareemerging.Formaximumeffectiveness,thesestrategiesdependontheabilitytoidentifytheappropriateindividualsforspecific,targetedinterventions.Thisabilitytodointelligentintegration,incorporatingpopulationsegmentationbasedonbehavioralhealthriskassessment,isafoundationaltoolinpopulationhealthmanagement.
9
ofinformationtospecificcaremanagementdecisions;andeffectivenessofcaremanagementstrategiesatboththeaggregateandindividuallevels.
PopulationSegmentationUsingBehavioralHealthRiskAssessment:TheFirstStepInPopulationHealthManagementStrategy
Populationsegmentationusingbehavioralhealthriskassessmentisanimportantstepinidentifyingpopulationhealthmanagementimprovementopportunities–andmatchingthepopulationtotheappropriateintervention.52Thisprocessusesavailabledatatoidentifyspecifichealthrisksforindividualsthatarelinkedtofuturespending.53
Simplemodelsforpopulationsegmentationinpopulationhealthmanagementprogramshavemostoftenuseddemographicsandself-reportedhealthstatusinformation.Moreadvancedmodelsincorporatediagnosesandmedicalconditions,treatmentandprescriptionutilization,and/orprevioushealthspendingpatterns–oftenfocusedexclusivelyonmedicalcare.54
Themanagementissueisthattheseriskstratificationmodelstypicallyunderestimatecostsofcareforindividualswithbehavioralhealthconditions,whileoverestimatingcostsofcareforindividualswithoutbehavioralhealthconditions.55Thisisasignificantbecausebehavioralhealthissuesarehighlyprevalent,complex,andcostly-andahighproportionofsuper-utilizerindividualshaveoneormorebehavioralhealthconditions.56Theseissuescanbeaddressedbymodifyingtraditionalriskstratificationmodelstoincludemorebehavioralhealthfactorstosupportimprovementsincostpredictions.57
Enhancedanalytictoolswhicharedesignedtoassessbehavioralhealthriskcanbeusedtoaddresstheeffectsofbehavioralhealthconditionsonindividualhealthoutcomesandspending.Intheseadvancedapproaches,additionalcharacteristicsofindividuals–suchasprimaryandsecondarydiagnoses,mentalillnessseverity,medicalconditions,ethnicity/minoritystatus,language,andsocio-economicstatus(loweducation,lowerincome,homelessness,unemployment,etc.)–canbeincorporated.58,59
Summary
Forpopulationhealthmanagementstrategiestobemosteffective,populationsegmentationiscriticaltomatchingindividualstohealthmanagementsupports.Whileahighproportionofsuper-utilizershavebehavioralhealthdisorders,thepopulationhealthmodelsdevelopedformedicalcaredonotsufficientlyexplainthevarianceintotalhealthcarecostsforpopulationswithbehavioralhealthconditionssincemedicalmodelsdonotincorporatesufficientbehavioralhealthdata.Asaresult,traditionalmedicalmodelsunderestimatetotalhealthcarecostsforindividualswithbehavioralhealthconditions,andoverestimatecostsforthosewithoutthem.60Thiscanberesolvedbysupplementingtraditionalapproacheswithbehavioralhealthdatatoaccuratelyestimatetotalhealthcostsandidentifyindividualsmostat-riskforhighresourceutilizationandcosts.
Tomakepopulationhealthmanagementstrategiesforindividualswithbehavioralhealthdisordersmoreeffective,enhancedanalytictoolsfocusedonassessingbehavioralhealthriskmustbeusedtoaddresstheeffectsofbehavioralhealthconditionsonindividualhealthoutcomesandspending.
10
V. CaseExampleOfBehavioralHealthRiskAssessmentInPopulationSegmentationInitiatives61
ThiscasestudydescribestheMissouriCommunityMentalHealthCenter(CMHC)HealthcareHomeModelexperience.
DefinitionofHealthHomes
InMarch2010,Section2703oftheAffordableCareAct(ACA)allowedstatestoamendtheirMedicaidstateplanstoprovideHealthHomesforenrolleeswithchronicconditions,creatingtheopportunityfortheMissouriCMHCmodel.TheHealthHomemodelprovideshealthservices,preventiveandhealthpromotionservices,andmentalhealthandsubstanceabuseservicestoindividualswithchronicconditionsusingawholepersonapproach.Ideally,thehealthhomeachievespopulationmanagementthroughcomprehensivecaremanagement,empowermentoftheindividual,team-basedcare,andpromotionofwellnessandhealthylifestyles.
MissouriHealthcareHomePurpose,PhilosophyandApproach
MissourichosetoestablishCMHCHealthcareHomesafterrecognizingthatindividualswithmentalhealthconditionstendtohavehigherhealthcarecostsduetocomorbidphysicalhealthconditions.Theyconcludedthat,inadditiontobehavioralhealthneeds,otherhealthcareissuesmustbeaddressedinordertoimproveoverallwholepersonhealthwhilereducinghealthcarecosts.Afteridentifyingthatleadingcontributorstopoorhealthoutcomesandhighercostswerepreventablecauses,MissourichosetocreatetheCMHCHealthcareHomestoaddressgeneralhealthissues,wellness,andpreventionalongwithbehavioralhealthissues.Thegoalwastoimprovenotonlyhealthoutcomes,butthequalityofcare.
StateofMissouriHealthHomeInitiatives
In2011,MissouriwasthefirststateinthenationtoreceiveapprovalofaMedicaidStatePlanAmendment(SPA)establishingHealthHomesunderSection2703oftheAffordableCareAct.MissourihastwotypesofHealthcareHomes:PrimaryCareHealthHomesandCMHCHealthcareHomes.EffectiveJanuary2012,Missouriauto-enrolled17,882individualsinto28CMHCHealthcareHomes(thesubjectofthiscasestudy).Thesehealthhomesreceivedan$80.31permemberpermonthreimbursement(PMPM).
TargetPopulations,CharacteristicsAndCostsOfIndividualsEnrolledInMissouriHealthcareHomes
Missouri’sCMHCHealthcareHomestargetedindividualswithmentalillness,substanceusedisorders,andchronichealthconditionsincludingdiabetes,cardiovasculardisease,COPD/asthma,overweight(BMI>25),tobaccouse,anddevelopmentaldisability.Thefollowingshowstargetpopulationbycondition:
TheMissouriteamobservedtheleadingcontributorstopoorhealthoutcomesandhighercostswerepreventablecauses
11
• 89%haveaseriousmentalillnesso 36%withMajorDepressiono 30%withSchizophreniao 28%withBipolarDisordero 16%withPostTraumaticStressDisorder
• ~25%withCOPD/Asthma• >than25%withDiabetes• 35%withHypertension• 81%withaBMI>25• Atleast50%reportsmoking• ~50%ofadultshaveahistoryofsubstanceabuse
TheImportanceOfPopulationHealthManagementInTheCMHCHealthcareHomeSetting
PriortotheACA,Missourihadidentifiedpopulationhealthmanagement,expandedservicesforindividualslivingwithbehavioralconditions,andtheintegrationofbehavioralandphysicalhealthcareasimportanttoimprovinghealthcareoutcomesandcosts.Theyinitiatedkeystepstobettersegmentandservehigh-riskpopulationsthroughtheuseoftechnology,aswellasastructuredapproachtocareintegrationandcoordination,whichbecamethefoundationforwhattheyidentifiedasthenextlogicalstep–theMissouriCMHCHealthcareHome.
SuccessFactors,Technology,Metrics,andReports
Byincorporatingtechnologythatallowedcareteamstotakea360-degreeapproachtomembercareanddecisionmaking,consideringsocialservicesandsupportsinadditiontomedicalandbehavioralhealthneeds,careteamsareabletoidentifythehigh-riskindividuals.Monthlyreportsallowcaremanagersto“flag”individualsandprioritizeappropriateinterventions.Onanindividuallevel,someinterventionsmayberequiredtoaddressimminentlyharmfulneeds.Onanaggregatelevel,selectinterventionsmayimpactthecareofalargerpopulation.TechnologythroughouttheCMHCHealthcareHomesenabledprovidersandcareteamstoaccessaweb-basedMedicaiddatasystemwhichincluded:
• patienthistoriesbasedonMedicaidclaims;• ametabolicscreeningdatabase;• caremanagementreportsbasedonpaidMedicaidclaimsdata;• medicationadherencereports;and,• behavioralhealthpharmacymanagementreports.
Withoutintegration,careteamswouldnothavehadaccesstocompletecarerecords.Thedisparatedatafrommultiplesourceswouldhavepreventedtheteam’sabilitytoaccuratelyidentifytheindividualsandpopulationsconsideredhigh-risk.
ImpactofCMHCHealthHomes
ThecombinationofinnovativeprogramswithenablingtechnologyresultedinatotalMedicaidcostsavingsof$2.4million.Morethanjustcostsavings,theintegratedapproachresultedinbettercare:62

12
• Overallimprovementinhospitalfollow-upafterdischarge(upfrom33%to66%ofallhospitaldischarges)
• Overallimprovementinmedicationreconciliationonhospitaldischarge(upfromapproximately25%to60%ofallhospitaldischarges)
• Reductionof12.8%inhospitaladmissions/1000• Reductionof8.2%inemergencydepartmentvisits/1000• ImprovementinmedicationsbeingfilledbyindividualsintheCMHChealthhomes,when
comparedtothestateoverall(asdeterminedbyamedicationpossessionratioofatleast80%inthequartersbeingevaluated).Between80-84%ofindividualsintheCMHChealthhomesareadherentbasedonthiscriterion.
13
VI. References
1Hayes,S.,McCarthy,D.,&Radley,D.(2016).TheImpactofaBehavioralHealthConditiononHigh-NeedAdults.TheCommonwealthFund.Retrievedfromhttp://www.commonwealthfund.org/publications/blog/2016/nov/behavioral-health-high-need-adults2Klein,S.&Hostetter,M.(2014).InFocus:IntegratingBehavioralHealthandPrimaryCare.QualityMattersArchive.Retrievedfromhttp://www.commonwealthfund.org/publications/newsletters/quality-matters/2014/august-september/in-focus3Hayes,S.,McCarthy,D.,&Radley,D.(2016).TheImpactofaBehavioralHealthConditiononHigh-NeedAdults.TheCommonwealthFund.Retrievedfromhttp://www.commonwealthfund.org/publications/blog/2016/nov/behavioral-health-high-need-adults4Klein,S.&Hostetter,M.(2014).Infocus:Integratingbehavioralhealthandprimarycare.Retrievedfromhttp://www.commonwealthfund.org/publications/newsletters/quality-matters/2014/august-september/in-focus5Druss,B.&Walker,E.(2011).Mentaldisordersandmedicalcomorbidity.RobertWoodJohnsonFoundation.Retrievedfromhttp://www.rwjf.org/content/dam/farm/reports/issue_briefs/2011/rwjf69438/subassets/rwjf69438_16Druss,B.&Walker,E.(2011).Mentaldisordersandmedicalcomorbidity.RobertWoodJohnsonFoundation.Retrievedfromhttp://www.rwjf.org/content/dam/farm/reports/issue_briefs/2011/rwjf69438/subassets/rwjf69438_17Thorpe,K.,Jain,S.,&Joski,P.(2017).PrevalenceAndSpendingAssociatedWithPatientsWhoHaveABehavioralHealthDisorderAndOtherConditions.HealthAffairs,36(1).8CentersforMedicare&MedicaidServices.(2016).Historical.Retrievedfromhttps://www.cms.gov/research-statistics-data-and-systems/statistics-trends-and-reports/nationalhealthexpenddata/nationalhealthaccountshistorical.html9Roehrig,C.(2016)MentalDisordersTopTheListOfTheMostCostlyConditionsInTheUnitedStates:$201Billion.HealthAffairs,35(6).Retrievedfromhttp://content.healthaffairs.org/content/early/2016/05/13/hlthaff.2015.1659.full.pdf+html10Hayes,S.,McCarthy,D.,&Radley,D.(2016).TheImpactofaBehavioralHealthConditiononHigh-NeedAdults.TheCommonwealthFund.Retrievedfromhttp://www.commonwealthfund.org/publications/blog/2016/nov/behavioral-health-high-need-adults11Boyd,C.,etal.(2010).FacesOfMedicaidDataBrief:ClarifyingMultimorbidityPatternstoImproveTargetingandDeliveryofClinicalServicesforMedicaidPopulations.CenterforHealthCareStrategies,Inc.Retrievedfromhttp://www.chcs.org/media/clarifying_multimorbidity_patterns.pdf12Jiang,H.,etal.(2015).CharacteristicsofHospitalStaysforSuper-UtilizersbyPayer,2012.Retrievedfromhttps://www.hcup-us.ahrq.gov/reports/statbriefs/sb190-Hospital-Stays-Super-Utilizers-Payer-2012.pdf13CaliforniaHealthcareFoundation.ReducingCareFragmentation:AToolkitforCoordinatingCare.Retrievedfromhttp://www.improvingchroniccare.org/downloads/reducing_care_fragmentation.pdf14Hayes,S.,McCarthy,D.,&Radley,D.(2016).TheImpactofaBehavioralHealthConditiononHigh-NeedAdults.TheCommonwealthFund.Retrievedfromhttp://www.commonwealthfund.org/publications/blog/2016/nov/behavioral-health-high-need-adults15Jiang,H.,etal.(2015).CharacteristicsofHospitalStaysforSuper-UtilizersbyPayer,2012.Retrievedfromhttps://www.hcup-us.ahrq.gov/reports/statbriefs/sb190-Hospital-Stays-Super-Utilizers-Payer-2012.pdf16Stanton,M.(2005).ThehighconcentrationofU.S.healthcareexpenditures.AgencyforHealthcareResearchandQuality,19.AHRQPub.No.06-0060.Retrievedfromhttps://archive.ahrq.gov/research/findings/factsheets/costs/expriach/expendria.pdf17Thorpe,K.,Jain,S.,&Joski,P.(2017).PrevalenceAndSpendingAssociatedWithPatientsWhoHaveABehavioralHealthDisorderAndOtherConditions.HealthAffairs,36(1).18Jiang,J.,etal.(2015).CharacteristicsofHospitalStaysforSuper-UtilizersbyPayer,2012.Retrievedfromhttps://www.hcup-us.ahrq.gov/reports/statbriefs/sb190-Hospital-Stays-Super-Utilizers-Payer-2012.pdf19CaliforniaHealthcareFoundation.ReducingCareFragmentation:AToolkitforCoordinatingCare.Retrievedfromhttp://www.improvingchroniccare.org/downloads/reducing_care_fragmentation.pdf
14
19WebMD.UntreatedDepression.Retrievedfromhttp://www.webmd.com/depression/guide/untreated-depression-effects#120CaliforniaHealthcareFoundation.ReducingCareFragmentation:AToolkitforCoordinatingCare.Retrievedfromhttp://www.improvingchroniccare.org/downloads/reducing_care_fragmentation.pdf21Hayes,S.,McCarthy,D.,&Radley,D.(2016).TheImpactofaBehavioralHealthConditiononHigh-NeedAdults.TheCommonwealthFund.Retrievedfromhttp://www.commonwealthfund.org/publications/blog/2016/nov/behavioral-health-high-need-adults22CaliforniaHealthcareFoundation.ReducingCareFragmentation:AToolkitforCoordinatingCare.Retrievedfromhttp://www.improvingchroniccare.org/downloads/reducing_care_fragmentation.pdf23WebMD.UntreatedDepression.Retrievedfromhttp://www.webmd.com/depression/guide/untreated-depression-effects#124MayoFoundationforMedicalEducationandResearch.(2017).Complications.Retrievedfromhttp://www.mayoclinic.org/diseases-conditions/mental-illness/basics/complications/con-2003381325Fuller,D.RESEARCHWEEKLY:PrevalenceofTreatedandUntreatedSevereMentalIllnessbyState.Retrievedfromhttp://www.treatmentadvocacycenter.org/fixing-the-system/features-and-news/307626Managingpopulationstoimproveindividualcare.Optum.Pages4-5.Retrievedfrom:https://campaign.optum.com/content/dam/optum/CMOSpark%20Hub%20Resources/White%20Papers/89FD003DE48545C5A46F24F17C886C23.pdf27ThreeKeyElementsforSuccessfulPopulationHealthManagement.ResearchBriefing.TheAdvisoryBoardCompanyRetrievedfrom:https://www.advisory.com/-/media/Advisory-com/Research/HCAB/Research-Study/2013/Three-Elements-for-Successful-Population-Health-Management/Three-Key-Elements-for-Successful-Population-Health-Management.pdf28Managingpopulationstoimproveindividualcare.Optum.Pages4-5.Retrievedfrom:https://campaign.optum.com/content/dam/optum/CMOSpark%20Hub%20Resources/White%20Papers/89FD003DE48545C5A46F24F17C886C23.pdf29JoinTogetherStaff.(2012).NewDataShowMillionsofAmericanswithAlcoholandDrugAddictionCouldBenefitfromHealthCareReform.Retrievedfromhttp://www.drugfree.org/new-data-show-millions-of-americans-with-alcohol-and-drug-addiction-could-benefit-from-health-care-r/30FloridaAlcohol&DrugAbuseAssociation.TheImpactofSubstanceUseDisordersOnHealthCare.Retrievedfromhttp://www.fadaa.org/documents/Legislative%20Booklets/HealthCare.pdf31Rockett,Putnam,Chang,andSmith(2005)AnnalsofEmergencyMedicine32CaliforniaHealthcareFoundation.ReducingCareFragmentation:AToolkitforCoordinatingCare.Retrievedfromhttp://www.improvingchroniccare.org/downloads/reducing_care_fragmentation.pdf33Hor,K.,&Taylor,M.(2010).Suicideandschizophrenia:asystematicreviewofratesandriskfactors.JournalofPsychopharmacology(Oxford,England),24(4_supplement),81–90.http://doi.org/10.1177/135978681038549034Volkow,N.D.(2009).SubstanceUseDisordersinSchizophrenia—ClinicalImplicationsofComorbidity.SchizophreniaBulletin,35(3),469–472.http://doi.org/10.1093/schbul/sbp01635Manzella,F.,Maloney,S.E.,&Taylor,G.T.(2015).Smokinginschizophrenicpatients:Acritiqueoftheself-medicationhypothesis.WorldJournalofPsychiatry,5(1),35–46.http://doi.org/10.5498/wjp.v5.i1.3536CentersforDiseaseControlandPrevention.(2016).CurrentCigaretteSmokingAmongAdultsintheUnitedStates.Retrievedfromhttps://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/37UniversityofMarylandMedicalCenter(UMMC).Schizophrenia.Retrievedfromhttp://umm.edu/health/medical/reports/articles/schizophrenia38Hert,M.,etal.(2011).Physicalillnessinpatientswithseverementaldisorders.I.Prevalence,impactofmedicationsanddisparitiesinhealthcare.WorldPsychiatry;10:52-77.Retrievedfromhttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC3048500/pdf/wpa010052.pdf39ODH,Inc.Mentrics.http://www.odhsolutions.com/mentrics40WebMD.UntreatedDepression.Retrievedfromhttp://www.webmd.com/depression/guide/untreated-depression-effects#1

15
41NationalCommitteeforQualityAssurance.(2015).Follow-uponHospitalizationforMentalIllness.Retrievedfrom:http://www.ncqa.org/report-cards/health-plans/state-of-health-care-quality/2015-table-of-contents/follow-up42CaliforniaHealthcareFoundation.ReducingCareFragmentation:AToolkitforCoordinatingCare.Retrievedfromhttp://www.improvingchroniccare.org/downloads/reducing_care_fragmentation.pdf43Hayes,S.,McCarthy,D.,&Radley,D.(2016).TheImpactofaBehavioralHealthConditiononHigh-NeedAdults.TheCommonwealthFund.Retrievedfromhttp://www.commonwealthfund.org/publications/blog/2016/nov/behavioral-health-high-need-adults44Klein,S.&Hostetter,M.(2014).Infocus:Integratingbehavioralhealthandprimarycare.Retrievedfromhttp://www.commonwealthfund.org/publications/newsletters/quality-matters/2014/august-september/in-focus45R.G.Kathol,S.Melek,andS.Sargent,“MentalHealthandSubstanceUseDisorderServicesandProfessionalsasaCorePartofHealthinClinicallyIntegratedNetworks.”InClinicalIntegration:AccountableCare&PopulationHealth,thirdedition,eds.K.Yale,J.Bohn,C.Konschaketal.(VirginiaBeach,Va.:ConvurgentPublishing,forthcoming).46Hayes,S.,McCarthy,D.,&Radley,D.(2016).TheImpactofaBehavioralHealthConditiononHigh-NeedAdults.TheCommonwealthFund.Retrievedfromhttp://www.commonwealthfund.org/publications/blog/2016/nov/behavioral-health-high-need-adults47NationwideChildrens.(2017).Patientpriceinformationlist.Retrievedfromhttp://www.nationwidechildrens.org/price-information-list50Optum.Managingpopulationstoimproveindividualcare.Retrievedfromhttps://campaign.optum.com/content/dam/optum/CMOSpark%20Hub%20Resources/White%20Papers/89FD003DE48545C5A46F24F17C886C23.pdf51TheAdvisoryCompany.ThreeKeyElementsforSuccessfulPopulationHealthManagement.ResearchBriefing.Retrievedfromhttps://www.advisory.com/-/media/Advisory-com/Research/HCAB/Research-Study/2013/Three-Elements-for-Successful-Population-Health-Management/Three-Key-Elements-for-Successful-Population-Health-Management.pdf52Hayes,S.,McCarthy,D.,&Radley,D.(2016).TheImpactofaBehavioralHealthConditiononHigh-NeedAdults.TheCommonwealthFund.Retrievedfromhttp://www.commonwealthfund.org/publications/blog/2016/nov/behavioral-health-high-need-adults53HermannRCetal.,2007.HarvRevPsychiatry.12(5):52-69;AmericanAcademyofActuaries.2010.IssueBrief:RiskAssessmentandRiskAdjustment.54HermannRCetal.,2007.HarvRevPsychiatry.12(5):52-69;R.WinkelmanandS.Mehmud,AComparativeAnalysisofClaims-BasedToolsForHealthRiskAssessment,SocietyofActuaries,2007;Ettneretal.,Inquiry.1998Summer;35(2):223-39;Barryetal.AmJPsychiatry2012;169:704–709.55HermannRCetal.,2007.HarvRevPsychiatry.12(5):52-6956Druss,B.&Walker,E.(2011).Mentaldisordersandmedicalcomorbidity.RobertWoodJohnsonFoundation.Retrievedfromhttp://www.rwjf.org/content/dam/farm/reports/issue_briefs/2011/rwjf69438/subassets/rwjf69438_157HermannRCetal.,2007.HarvRevPsychiatry.12(5):52-69;R.WinkelmanandS.Mehmud,AComparativeAnalysisofClaims-BasedToolsForHealthRiskAssessment,SocietyofActuaries,2007;Ettneretal.,Inquiry.1998Summer;35(2):223-39;Barryetal.AmJPsychiatry2012;169:704–709.58AssociationforCommunityAffiliatedPlans(ACAP).(2012).ImprovingRiskAdjustmentinHIEstoEnsureFairPayment.59HermannRCetal.,2007.HarvRevPsychiatry.12(5):52-69;HermannRC.Improvingmentalhealthcare:aguidetomeasurement-basedqualityimprovement.Washington,DC:AmericanPsychiatricPress,200560HermannRCetal.,2007.HarvRevPsychiatry.12(5):52-69;R.WinkelmanandS.Mehmud,AComparativeAnalysisofClaims-BasedToolsForHealthRiskAssessment,SocietyofActuaries,2007;Ettneretal.,Inquiry.1998Summer;35(2):223-39;Barryetal.AmJPsychiatry2012;169:704–709.61MissouriDepartmentofMentalHealth.Missouri’sCMHCHealthcareHomes.Retrievedfromhttps://www.mainequalitycounts.org/image_upload/Parks%202nd%20presentation%20HCH%20101%20Team%20Training.pdf
16
62DepartmentofMentalHealthandMOHealthNet.(2013).ProgressReport:MissouriCMHCHealthcareHomes.Retrievedfromhttps://dmh.mo.gov/docs/mentalillness/prnov13.pdf©Copyright2017–ODH,Inc.