Embed Size (px)
Citation preview

How I manage thoracic tumors incorporating the supra aortic trunks
Elie FADEL

Disclosure
Speaker name: Elie FADEL
I do not have any potential conflict of interest

Thoracic tumors that may invade the SAT
requiring surgical resection
From the Lung:
From the mediastinum:
NSCLC: Upper lobes +++
Metastasis to the upper lobes
Thymoma
Primary Mediastinal germ cell tumors
Sarcoma / Pseudoinflammatory tumors

Thoracic tumors that may invade the SAT
requiring surgical resection
From the Lung:
From the mediastinum:
NSCLC: Upper lobes +++
Metastasis to the upper lobes
Sarcoma
Thymoma
Primary Mediastinal germ cell tumors

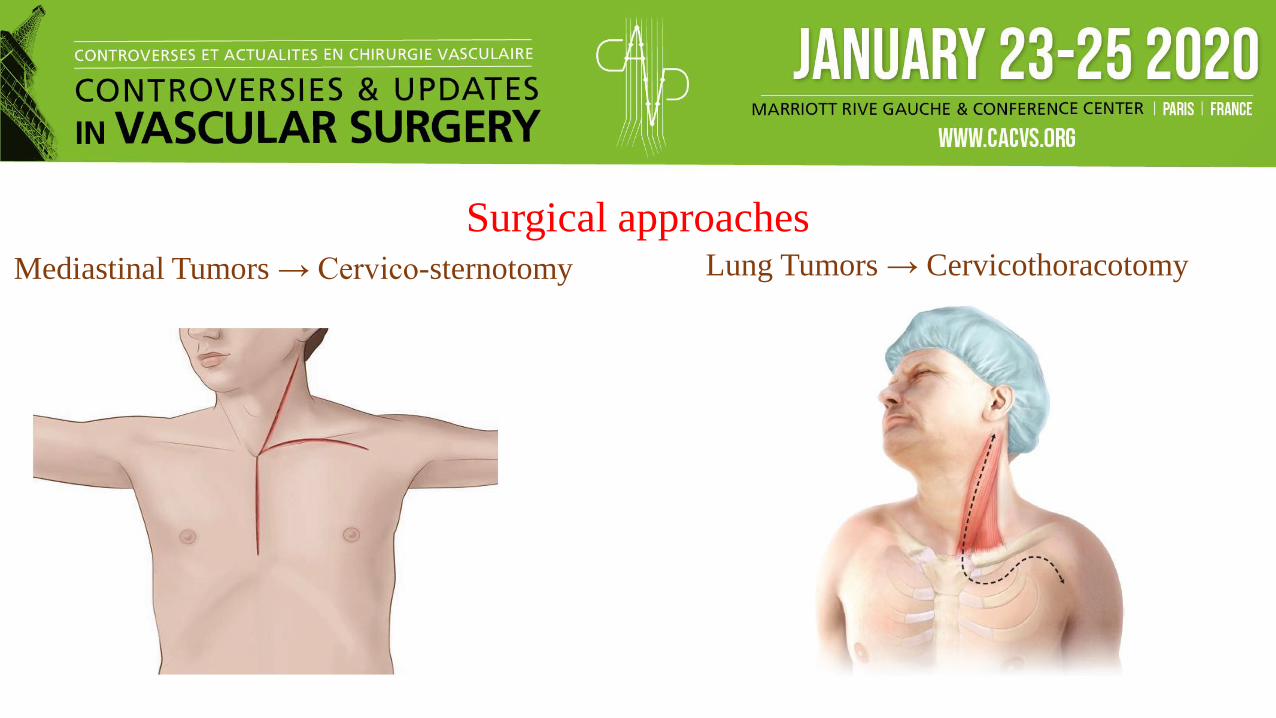
Surgical challenges due to the SAT invasion
Surgical approach:
SAT-cross clamping:
SAT replacement:
• Combined cervicothoracic approach
• Vessels control and replacement
• Enbloc resection of the tumor and the involved vessels
• Always necessary because the collateral network is ligated
• Most of the time end to end anastomosis (rib resection / short vessel length)
• Avoid synthetic graft when potentially contamineted operative field
• Think about postoperative radiation therapy (vein/pericardial patch…)
• Protective pedicled flap
• Should be as short as possible
• As tumor resection time may be long (complexity of the procedure) all the other involved
structures should be resected first and the specimen pedicled around the involved vessel
• If the vessel is a carotid artery, think about shunting

Preoperative workup•Evaluation of the tumor
•Evaluation of the patient’s functional status
•Histological confirmation obtained +++
•Local tumor spread: Neck and chest angio CT, flexible bronchoscopy, EBUS, duplex scanning,
angiography and phlebography, MRI (spine+++)
•Distant tumor spread: PET scan, cerebral MRI or CT
•Standard laboratory and respiratory functional tests
•Ventilation/perfusion scanning
•VO2 max
•Echocardiography
•Coronary angiography
•Right heart catheterization

Contra-indication to surgery
•Predictive inability to achieve complete resection
•Severe co-morbidities jeopardizing survival
cN2,N3 disease
Distant metastasis
Procedures should be performed only with curative intent according
to the well-established principles of oncologic surgery (en-bloc
surgery with microscopically tumor-free margins)

The multimodal treatment of locally extended thoracic tumors
Radiation
therapy
SurgeryNeoadjuvant Adjuvant
Chemotherapy
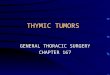
Surgical approachesMediastinal Tumors → Cervico-sternotomy Lung Tumors → Cervicothoracotomy

The Superior Sulcus


The anterior cervicothoracic approach (Dartevelle et al JTCVS1993)

Transclavicular Transmanubrial
Costo clavicular
space



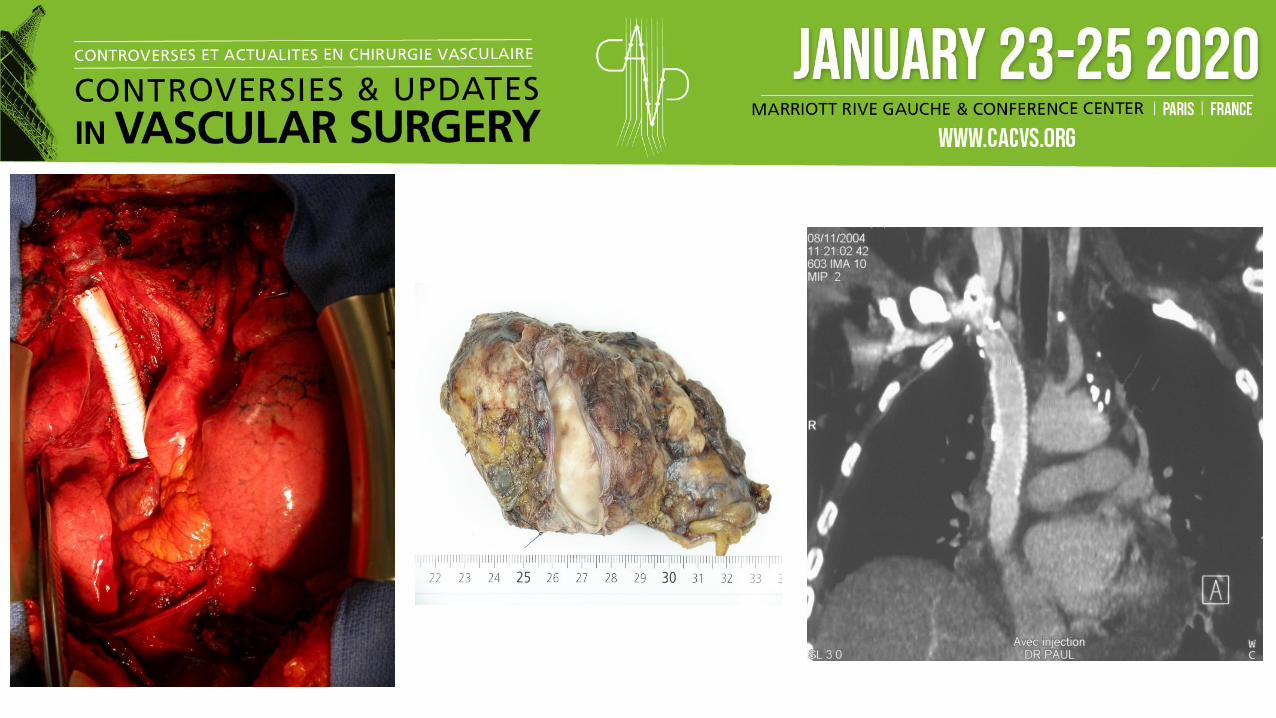
Aortic resection and reconstruction
under CPB

*
**

Mediastinal Tumors
Mostly invade the venous trunks

Mediastinal tumorsContraindications to surgery
• Involvement of both phrenic nerves
• Involvement of both innominate vein
confluences



Germ cell tumor




Use of Cell saver and CPB?

Survival curves of patients with and without
subclavian arterial invasion
(p 0.01)
42%
25%
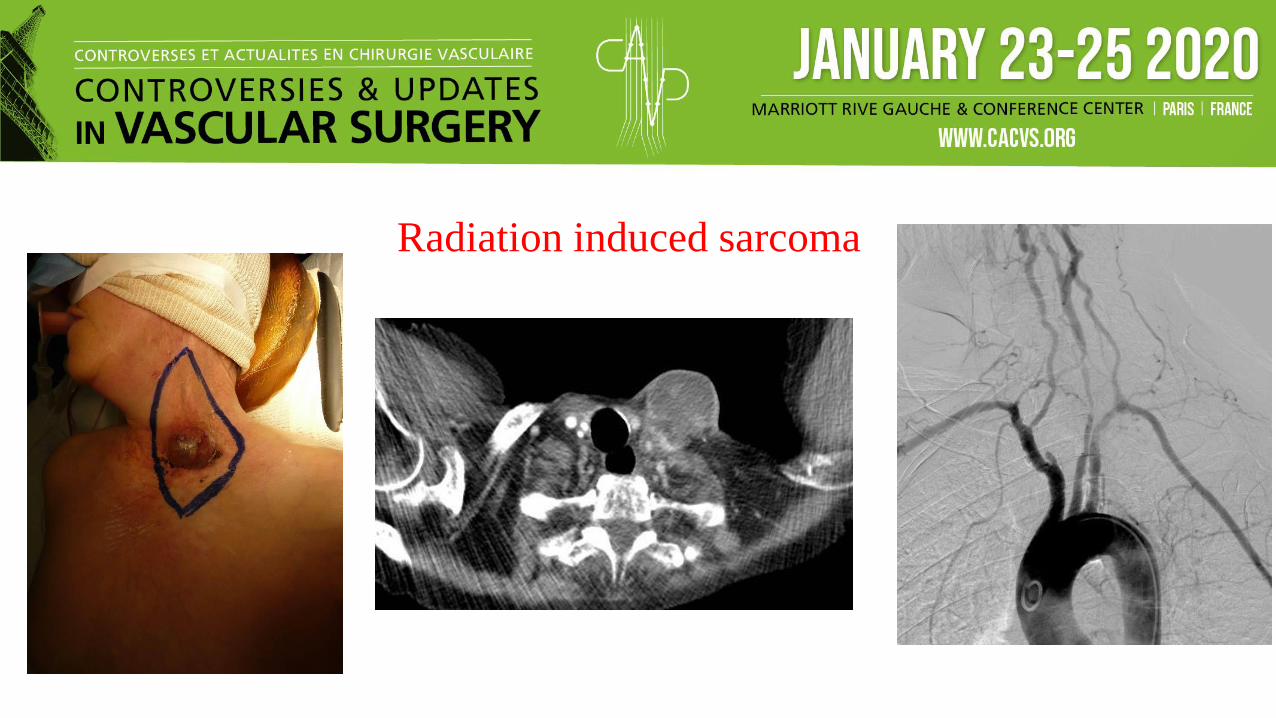
Radiation induced sarcoma

The contribution of reconstructive surgery: tight free flap


Conclusions Surgical resection of locally extended thoracic tumors to the supraortic trunks is
feasible with good longterm outcome provided:
These demanding procedures should be performed by skilled team in thoracic and
vascular surgeries
• Extended preoperative workup ruling out surgical contraindications: distant
metastasis, inabitity to R0 resection, functional compromise (phrenic
nerves…)
• Respect of oncological principles: enbloc resection with R0 margins
• Vascular reconstruction with the shortest clamping time


![Solitary fi brous tumors of the pleura · tumor of the pleura from other lun g tumors, while the contribution of thoracic CT is rather moderate [4]. Although preoperative dia gnosis](https://img.pdfslide.us/doc/110x75/6081a9dfae78a40b630c556a/solitary-i-brous-tumors-of-the-pleura-tumor-of-the-pleura-from-other-lun-g-tumors.jpg)