-
[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER
> NOTES AND HANDOUTS]
4/14/20161
How I Do It: Aortic Arch DebranchingExposures, Tunnels and
Techniques
4/14/2016
Warren Gasper MDAssistant Professor of SurgeryUCSF Vascular
Surgery
No disclosures
2 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
Into the arch
� Zone 2
• Occlude the left subclavian artery
� Zone 1
• Occlude the left carotid and left subclavian arteries
� Zone 0
• Occlude the innominate, left carotid and left subclavian
arteries
3 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
J Endovasc Ther 2002;9:suppl 2; II98–105
Zone 2 – preserve the left subclavian
� Left carotid to left subclavian bypass
• Short, prosthetic bypass from common carotid to subclavian
• Need to ligate/occlude the subclavian proximal to the
vertebral
• Preferred if there is LIMA-coronary bypass, no need to
interrupt LIMA flow
� Left subclavian to carotid transposition
• No bypass conduit, proximal subclavian artery is oversewn
• Can be difficult to get proximal to the vertebral and internal
mammary
Assess the origin of the vertebral artery to ensure it is
preserved
Preoperative carotid duplex – treat occlusive disease
concomitantly
4 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
-
[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER
> NOTES AND HANDOUTS]
4/14/20162
Carotid-subclavian bypass
5 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
� Supraclavicular incision
� Divide the platysma
� Divide the clavicular head of the SCM if needed
� Divide the omohyoid
Rutherford Atlas of Vascular Surgery 1993
Carotid-subclavian bypass
6 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
� Supraclavicular incision
� Divide the platysma
� Divide the clavicular head of the SCM if needed
� Divide the omohyoid
� Ligate the external jugular if needed
Valentine Vascular Exposures 2003
� Mobilize the inferior and medial edges of the scalene fat pad
and retract superolateral
� Divide the thoracic duct if needed
� Identify the phrenic nerve running anterior to the anterior
scalene muscle
7 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
Carotid-subclavian bypass
Valentine Vascular Exposures 2003
� Mobilize the inferior and medial edges of the scalene fat pad
and retract superolateral
� Divide the thoracic duct if needed
� Identify the phrenic nerve
� Divide the anterior scalene (bovie, bipolar, scissors)
8 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
Carotid-subclavian bypass
Rutherford Atlas of Vascular Surgery 1993
-
[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER
> NOTES AND HANDOUTS]
4/14/20163
� Proximal and distal control of the subclavian artery
9 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
Carotid-subclavian bypass
Rutherford Atlas of Vascular Surgery 1993
� Divide the SCM or retract it medially
� Expose the lateral edge of the internal jugular and retract
medially
� Expose the left common carotid artery while protecting the
vagus nerve
10 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
Carotid-subclavian bypass
Rutherford Atlas of Vascular Surgery 1993
� Prosthetic graft
• 6 or 8mm PTFE or Dacron
� Sew the graft end-to-side to the subclavian artery first
11 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
Carotid-subclavian bypass
Ouriel Atlas of Vascular Surgery 1998
� Pass above or below the phrenic nerve
� Pass below the internal jugular vein
� Use 5mm aortic punch (optional) and sew end-to-side
� Ligate the subclavianproximal to vertebral or use an
endovascular plug
� Close the platysma and skin over a JP drain
12 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
Carotid-subclavian bypass
Ouriel Atlas of Vascular Surgery 1998
-
[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER
> NOTES AND HANDOUTS]
4/14/20164
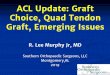
Zone 1: Preserve the left carotid and left subclavian
arteries
Right carotid – left carotid – left subclavian bypass
= 4 anastomoses
Alternative: Right carotid – left subclavian – right carotid
bypass
= 3 anastomoses
13 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
Perspect Vasc Surg Endovas Ther 2012;24(4) 184–192
Carotid-carotid-subclavian bypass tips� Expose right common
carotid with a longitudinal incision and the left common
carotid and subclavian through a supraclavicular incision
� Be aware of the vagus nerves
• In an unlucky situation, injury to both nerves can cause
bilateral vocal cord paralysis and airway compromise
� Bypass technique:
• 6 or 8mm PTFE or Dacron
• Right common carotid – Left subclavian – Left common
carotid
� Tunnel choices
� Ligate/occlude the proximal left subclavian and left common
carotid arteries
14 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
15 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
Tunnels
Retropharyngeal
Anterior
Valentine Vascular Exposures 2003
Rarely used option: subclavian-subclavian bypass
16 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
Ouriel Atlas of Vascular Surgery 1998
-
[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER
> NOTES AND HANDOUTS]
4/14/20165
Rarely used option: subclavian-subclavian bypass
17 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
Ouriel Atlas of Vascular Surgery 1998
Rarely used option #2: axillo-axillary bypass
18 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
Ouriel Atlas of Vascular Surgery 1998
Rarely used option #2: axillo-axillary bypass
19 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16
Ouriel Atlas of Vascular Surgery 1998
Conclusions
� Debranching procedures have high success and long-term patency
rates
�Watch for anatomic variations and carotid artery disease
� Right carotid-left subclavian-left carotid bypass will save an
anastomosis
20 Aortic Arch Debranching | UCSF Vascular Symposium 2016
4/14/16