Embed Size (px)
Citation preview
This article was downloaded by: [The Aga Khan University]On: 10 October 2014, At: 16:16Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Counselling Psychology QuarterlyPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/ccpq20
How counselling psychologists areperceived by NHS clinical psychologistsSarah Lewis & Robert BorPublished online: 27 Sep 2007.
To cite this article: Sarah Lewis & Robert Bor (1998) How counselling psychologists areperceived by NHS clinical psychologists, Counselling Psychology Quarterly, 11:4, 427-437, DOI:10.1080/09515079808254073
To link to this article: http://dx.doi.org/10.1080/09515079808254073
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Counselling Psychology Quarter&, Vol. 11, No. 4, 1998, pp. 427-437 427
RESEARCH REPORTS
How counselling psychologists are perceived by NHS clinical psychologists
SARAH LEWIS & ROBERT BOR
ABSTRACT The aim of the study was to obtain data reJlecting NHS clinical psychologists’ perceptions of counselling psychologists. A 19-item questionnaire was devised and sent by post to 303 clinical psychology departments throughout the United Kingdom in July 1995. 161 replies were received from areas including mental health, community care, general hospital, neurological rehabili- tation, learning disabilities and combinations of these. Results showed considerable confusion among clinical psychologists around the identity and competencies of counselling psychologists. Much of this confusion seems to be attributable to a lack of information regarding the content of training and a lack of awareness that counselling psychologists are now chartered under the auspices of the British Psychological Society. The survey suggests that counselling psychologists should work to clarify their identity and increase communication with professional colleagues before their contribution to the provision of psychological care can be recognised.
Introduction
1. The development of counselling psychology in the United Kingdom
Counselling was formally acknowledged in the UK when the Standing Council for the Advancement of Counselling (SCAC) was formed in 1971 and became the British Association for Counselling (BAC) in 1976 (McLeod, 1993). It was not until the 1980s that the British Psychological Society (BPS) recognized the strength of the counselling movement and its relevance to psychology by the formation of a Special Group in Counselling Psychology, which voted to become a Division in its own right in 1994 (Collins & Murray, 1995). Despite counselling becoming more structured, there is still a confusing range of counselling training schemes and subsequent inconsistencies in the qualifications held by counsellors (Collins & Murray, 1995). The provision of recognized training courses for counselling psychologists has begun to define the requisite knowledge base. The recognition of counselling by the BPS in the creation of a Division of Counselling Psychology and the conferring of
Correspondence to: Professor Robert Bor, Psychology Department, City University, Northampton Square, London EClV OHB, UK.
0951-5070/98/040427-11 Q 1998 Carfax Publishing Ltd
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
16:
16 1
0 O
ctob
er 2
014
428 Sarah Lewis & Robert Bor
chartered status provides a way in which the quality of counselling services can be assured (Collins 8z Murray, 1995).
Counselling psychology has its foundations in the humanistic model (Watkins, 1987). This is not to say that counselling psychologists only apply a humanistic model to therapy, but that their underlying belief is in the positive potential of the individual and that the reality of an individual’s experience is something which should command respect from the therapist. Woolfe (1990) suggests that coun- selling psychology has as its mission:
not to declare its independence from other areas of psychological activity, but rather to celebrate its product and seek to explore ways in which this can be spread more widely among psychologists and in this why offered more widely to potential customers.
This attitude clearly sees counselling psychology as complementary to, rather than in competition with, other applied psychological disciplines.
2. Defining counselling psychology
The problems inherent in defining counselling psychology illustrate the confusion which currently surrounds its professional identity. Counselling is essentially a psychological process. Its theories focus on the thoughts, feelings and behaviours of the individual and its concepts are derived from a variety of psychological ap- proaches (Woolfe, 1990). One of the hndamental differences between counselling and counselling psychology is that the latter places a central emphasis on psychology as the knowledge base of the discipline (Barkham, 1990). The status of BPS Chartered Counselling Psychologist places a strong emphasis on the role of a psychologist as a scientist, so the qualification of counselling psychologist includes not only a wide understanding of psychological concepts but also a thorough grounding in the principles of research and evaluation. The BPS (1 995) regulations for the Diploma in Counselling Psychology stipulate that research:
is an integral part of the training and practice of Counselling Psychology.
Counselling psychology places a major emphasis on psychotherapeutic training, stressing the process of therapy as well as the content. Therefore, counselling psychol- ogists are encouraged to pay great attention to defining the therapeutic relationship, and attending to it throughout the course of therapy. This acknowledges the belief that the nature of the therapeutic relationship is fundamental to the progress and outcome of therapy and that the person of the therapist plays an intrinsic part in that relationship. This is further stressed by the requirement during training and practice for personal reflection, psychological counselling and ongoing supervision to facilitate deeper understanding of this influence. Woolfe (1 990) suggests that this presents a critical distinguishing characteristic differentiating counselling psychology from other areas of applied psychology. Woolfe (1990) states that:
the more that the self of the therapist is conceived as an active ingredient
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
16:
16 1
0 O
ctob
er 2
014
Clinical psychologists ’ perception of counselling psychologists 429
in the counselling process, the more incumbent it becomes on counsellors to develop the level of understanding of their own psychological processes.
Thus, the essential difference between counselling psychology and other applied areas of psychology may be seen as one of ethos rather than necessarily of content (McLeod, 1993). The principles of a humanistic approach are applied and the importance of the psychotherapeutic relationship to all human problems is stressed.
3. A role for counselling psychology in the NHS
The role of counselling psychology in the UK is currently unclear. Despite the fact that its training requirements are now clearly regulated by the BPS, there is a lack of general information available in NHS clinical psychology departments regarding the content of this training. It may help the definition of a clear role for counselling psychologists within the NHS if more information was made available about the training, therapy and assessment undertaken. Collins & Murray (1 995) surveyed eight clinical psychologists and two counselling psychologists within the Southmead NHS Trust to establish their view of the role of the two recently employed counsellors (who were considered to be ‘counselling psychologists’, while the au- thors acknowledge that they may not fulfil BPS criteria for this). They found a discrepancy between what the clinical psychologists felt the counsellors were com- petent to do, and the competencies identified by the counsellors themselves. The clinical psychologists’ views of the areas of competence of each group were generally in accordance with those of the BPS (1994). However, the counsellors felt their training equipped them to fill a much broader role, including those clients with more complex, intractable and severe difficulties.
The perceived breadth of role that is possible in counselling psychology has been considered both a weakness and a strength. However, this does not appear to take into account that it is the client rather than the therapeutic approach which varies. Until there is a body of outcome research which unequivocally supports one school of therapy over another for specific problems, the supposed weakness can carry little weight. Indeed, there are several studies which identify the therapeutic relationship as a key element in achieving a positive outcome (Stiles et al., 1986). Both counselling and clinical psychologists undertake assessment and plan their intervention although they may use different formulations. Barkham (1 990) applies the concept of the ‘equivalence paradox’ not only to the differences in therapeutic approach adopted by the two but also to the relevance of any fundamental difference between their philosophy. The equivalence paradox describes the effect seen in outcome studies in which there is no significant difference in result seen despite considerable difference between the contrasting approaches used (Stiles, et al., 1986). Barkham (1990) continues, to suggest that:
while the philosophies, rationales and implementations of each discipline may differ, the effects in terms of skills, impact and service delivery are broadly equivalent.
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
16:
16 1
0 O
ctob
er 2
014
430 Sarah Lewis &Robert Bor
The professional identity of counselling psychologists is influenced by several factors: how counselling psychologists perceive themselves in terms of philosophy; how counselling psychology is viewed and understood by others; and in terms of what it is that counselling psychologists actually do in their work (Owen, 1992). This refers to the content of their training and practice (Galassi & Brooks, 1992). At present it is unclear how other professional colleagues view the training and competencies of counselling psychologists.
4. Aims of this study
This research aimed to provide data relating to the perceptions of senior NHS clinical psychologists towards counselling psychologists in terms of their training and practice, the intention being to stimulate discussion about the identity of counselling psychology and its role within the health care system.
Methods
1. Design
A 19-item questionnaire was devised to survey clinical psychologists within NHS departments about their knowledge of counselling psychology. As the questionnaire used was not a validated instrument, the information obtained was analysed using frequency distributions and percentage response rates. The addresses of relevant psychology departments were obtained from a database which supplied a list of all community and mental health care sites in the NHS (Beechwood House, 1995).
2. Materials
The study was conducted in 1995 using a two-part questionnaire taking approxi- mately ten minutes to complete. Items were generated by the first author and gained face validity through discussion with colleagues.
Part 1 asked for information about the nature of the department. It comprised of nine questions establishing the location of the department both within the area health service and geographically; the role of the respondent; the size of the department, assessed in terms of the numbers of clinical and counselling psycholo- gists employed and the number of trainees from both specialities present; the type of problems normally seen within the department; and the average length of the waiting list.
Part 2 asked ten questions all relating to counselling psychology. The purpose of this section was to ascertain whether the respondent had any experience of employing or working with counselling psychologists or of their potential role within a clinical psychology department. The questions addressed the training of coun- selling psychologists, the type of therapeutic approach they would be most likely to use, the range of problems they see in practice, the client groups appropriate to their background and training, and four questions relating to the status of counselling
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
16:
16 1
0 O
ctob
er 2
014
Clinical psychologists ’ perception of counselling psychologists 43 1
psychologists within clinical psychology departments. Question nine asked whether the respondent felt adequately informed about counselling psychology. All the above questions were answered by ‘yes’, ‘no’ or ‘don’t know’. The final question was an open question inviting comments. (A copy of the questionnaire is available from the authors).
3. Subjects
The questionnaires were distributed to the heads or chairpersons of 303 NHS clinical psychology departments identified by the Database of NHS Management. Participation in the study was entirely voluntary and anonymity was guaranteed.
4. Procedure
The questionnaires were posted in July 1995, using address labels supplied with the database. All questionnaires were accompanied by a covering letter and a stamped addressed return envelope in an attempt to maximise the response rate. The covering letter explained the nature of the survey and the time limitations applying to the study. A brief explanation of the relevance of the study to the development of counselling psychology was given. Most responses were received within the first ten days and only those received within the three week deadline were included in the final analysis.
Results
One hundred and sixty-one questionnaires were returned during the survey period in June-July 1995, representing a response rate of 53%.
1: Questionnaire Part 1: Demographic details
The sample was taken from clinical psychology departments across a variety of health care settings. Responses were received from across the whole of the UK, with the greatest number of replies from the southeast of England (30%).
Most commonly the departments employed between 1 and 5 clinical psy- chologists (35%) and had between 1 and 5 clinical psychology trainees (76%). Only 34 (21%) employed 1-5 counselling psychologists and 12 (So/,> had counselling psychology trainees.
37% (59) of the departments offered therapy across the complete range of problems identified by the questionnaire. The most common referrals were for anxiety, phobias, obsessive-compulsive disorders, depression, somatic problems and eating disorders which were all seen in over 90% of departments. HIV/AIDS was the least common problem, seen in only 44% of departments. The average waiting list was more than 6 weeks in 64% (103) of the departments which responded. Only 7% (1 1) had no waiting time for treatment.
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
16:
16 1
0 O
ctob
er 2
014
432 Sarah Lewis & Robert Bor
2: Questionnaire Part 2
Respondents were asked to state whether or not they were familiar with the training requirements for the BPS Diploma in Counselling Psychology. Only 35 ( 2 2 % ) correctly identified the main requirements for the Diploma and a higher proportion indicated that they were unsure about them. Less than half (46%) of all respondents were aware that training in research methods and evaluation of counselling psy- chology was a requirement of the Diploma. A similar number (45%) did not know that personal psychological counselling was also a component of training. A high proportion (70%) correctly stated that counselling psychology training included, among others, a broad coverage of the main psychological theories of counselling and psychotherapy; assessment of client problems and planning of intervention; and course assessments on the form of an examination. Several respondents said that they were unclear about the difference in training between a Counsellor and a Counselling Psychologist.
When asked: ‘What method of therapy would a counselling psychologist be most likely to employ?’, 91 respondents (57%) stated that a humanistic approach would be chosen while 25% (40) did not know what type of therapeutic approach a counselling psychologist might use. Only 8% felt that they may use any or all from the range offered (which included psychodynamic, cognitive behavioural and systemic among others).
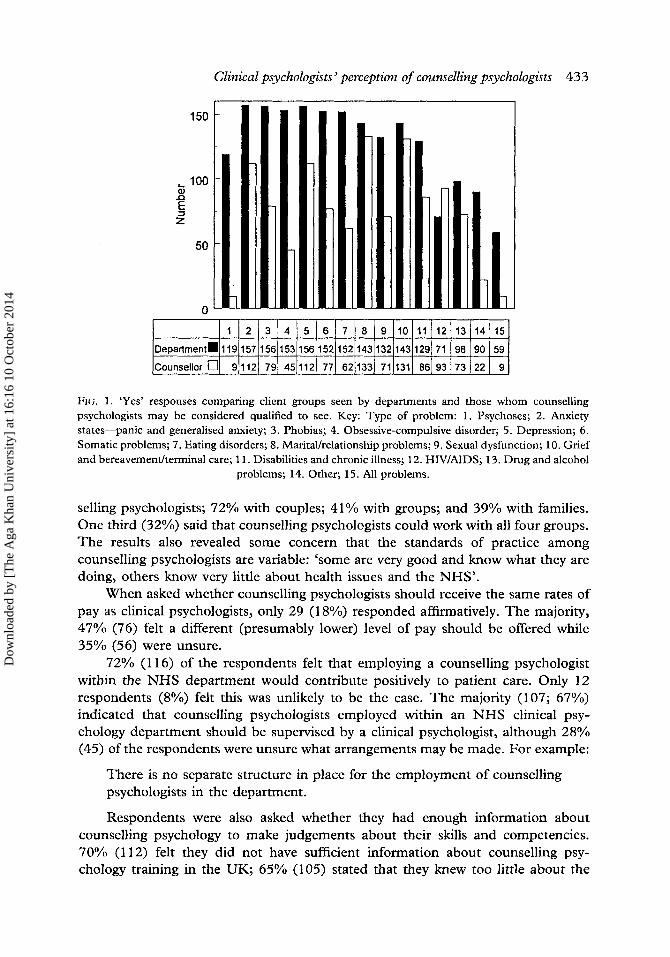
After being asked to list the range of clinical problems which are usually seen in an NHS clinical psychology department, respondents were then asked to select those considered appropriate for treatment by a counselling psychologist. 6% (9) felt that a counselling psychologist would be able to see all of those listed categories suggested. 16% (25) did not know which problems a counselling psychologist could be expected to see. More than half the respondents felt that counselling psycholo- gists should only be involved in the treatment of certain problems. For example, 60% (97) felt that the referral of psychotic individuals would not be appropriate, while 83% (133) felt that counselling psychologists would be expected to see people with marital problems and a similar percentage (82%) stated it would be appropriate to refer those needing help with adjustment to loss and bereavement. A comparison has been made in Fig. 1 between the client groups seen by the departments and those whom clinical psychologists believe counselling psychologists may be qualified to see.
21% (34) of the clinical psychologists surveyed felt that counselling psycholo- gists had expertise in certain areas of practice beyond that provided by clinical psychologists. These areas included a more extensive knowledge of and training in the psychotherapies, treatment of ‘life-adjustment problems’, and bereavement and relationship difficulties. 30% (49) felt that counselling psychologists did not offer anything additional to clinical psychologists, while the majority (48%; 78/16 1) were uncertain.
Respondents were asked whether they felt that counselling psychologists were suitably qualified to work therapeutically with individuals, couples, families and groups. 83% (134) identified individuals as the appropriate client group for coun-
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
16:
16 1
0 O
ctob
er 2
014
Clinical psychologists ’ perception of counselling psychologists 433
9
z i:[ 50 0
FIG. 1 . ‘Yes’ responses comparing client groups seen by departments and those whom counselling psychologists may be considered qualified to see. Key: Type of problem: 1. Psychoses; 2. Anxiety states-panic and generalised anxiety; 3. Phobias; 4. Obsessive-compulsive disorder; 5. Depression; 6 . Somatic problems; 7. Eating disorders; 8. Marital/relationship problcms; 9. Sexual dysfunction; 10. Grief and bereavement/terminal care; 1 1. Disabilities and chronic illness; 12. I-IIV/AIDS; 13. Drug and alcohol
problems; 14. Other; 15. All problems.
selling psychologists; 72% with couples; 41% with groups; and 39% with families. One third (32%) said that counselling psychologists could work with all four groups. The results also revealed some concern that the standards of practice among counselling psychologists are variable: ‘some are very good and know what they are doing, others know very little about health issues and the NHS’.
When asked whether counselling psychologists should receive the same rates of pay as clinical psychologists, only 29 (1 8%) responded affirmatively. The majority, 47% (76) felt a different (presumably lower) level of pay should be offered while 35% (56) were unsure.
72% (1 16) of the respondents felt that employing a counselling psychologist within the NHS department would contribute positively to patient care. Only 12 respondents (8%) felt this was unlikely to be the case. The majority (107; 67%) indicated that counselling psychologists employed within an NHS clinical psy- chology department should be supervised by a clinical psychologist, although 28% (45) of the respondents were unsure what arrangements may be made. For example:
There is no separate structure in place for the employment of counselling psychologists in the department.
Respondents were also asked whether they had enough information about counselling psychology to make judgements about their skills and competencies. 70% (1 12) felt they did not have sufficient information about counselling psy- chology training in the UK; 65% (105) stated that they knew too little about the
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
16:
16 1
0 O
ctob
er 2
014
434 Sarah Lewis & Robert Bor
competence of qualified counselling psychologists; and 59% (95) felt they knew too little about their suitability for employment in the NHS. One respondent stated that he/she thought clinical psychologists had three years more post-graduate training than counselling psychologists.
A number of general comments were made by respondents at the end of the questionnaire regarding counselling psychologists. One person stated that ‘the provision of health care should involve clinical, counselling and health psychologists working together’, while another added that ‘there is a huge demand and unmet need for psychology in all its forms’. The lack of guidelines around employing counselling psychologists was also noticed: ‘counselling psychologists are a cheaper, more limited alternative to clinical psychologists that can make a positive contribu- tion to mental health work’, but ‘we need pay scales and formal guidance on employment. The Leicester office [of the BPS] has not been helpful’.
Discussion
The aim of this study was to survey senior managerial NHS clinical psychologists about their knowledge of and views about the training, methods and expertise of counselling psychologists and their possible role within such departments. The results suggest that the majority of clinical psychologists are unclear about the skills and training undertaken by counselling psychologists but generally assume that they are best equipped to treat clients with ‘life-crisis’ problems and not those classified as having more serious psychological problems. Also, there is a reluctance to accept counselling psychologists as having equivalent, although different, areas of expertise to clinical psychologists. These findings lend support to the suggestion that an improved awareness of the rigours of counselling psychology training may be needed within the field of psychology as a whole and particularly aimed at those with whom counselling psychologists may have a close working relationship.
The results of the survey also confirm the need for clarification of the content of training and help to create a professional identity for counselling psychologists. The results suggest that clinical psychologists do not yet perceive counselling psychologists as meriting professional equivalence. Most respondents were unaware that counselling psychologists undergo training in research methods and evaluation, or that personal therapy is a requirement. These are crucial aspects of the training of a counselling psychologist, the former in defining the psychologist and the latter in defining the uniqueness of counselling. Their presence helps distinguish coun- selling psychology from other areas of applied psychology. The lack of knowledge about counselling psychology is likely to reduce its attractiveness as a complemen- tary, yet equivalent, therapeutic resource.
It may be difficult to integrate counselling psychology with other psychology services if there is thought to be a fundamental difference in psychotherapeutic practice. The results reveal that over half the respondents felt counselling psycholo- gists would be most likely to employ a humanistic method of therapy while over 65% of the respondents indicated at least one other method of therapy may be practised by counselling psychologists. The perceived preference for a humanistic approach to
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
16:
16 1
0 O
ctob
er 2
014

Clinical psychologists’ perception of counselling psychologists 435
therapy needs to be balanced with the practicalities of working within the NHS, where the therapies of choice tend to be time limited and usually cognitive and behavioural (McLeod, 1993). T o the best of our knowledge, no survey of practising counselling psychologists has been conducted and it is therefore not possible to confirm whether a humanistic approach has been adopted by the majority. Pre- sumably much will depend on their training. However, a humanistic approach need not be at variance with the demand for brief solution-focused therapies in the NHS. The extent to which different approaches to assessment and treatment are offered within the psychology departments may become clearer in time.
The results of the study reveal some deficit between what NHS psychology departments need and what the respondents consider counselling psychologists could provide. Less than 6% of the respondents felt that a counselling psychologist would be competent to see a wide range of psychological problems. The general perception among clinical psychologists is that counselling psychologists are best suited to see those suffering from adjustment problems. There is little understanding of the broader application of counselling psychology and it seems that many clinical psychologists see the role of counselling psychologists as much more limited than the counselling psychologists may themselves. This mirrors the findings of Collins & Murray (1995) in their small scale study of one psychology department. It would be interesting to compare these views with the experience of counselling psychologists to discover whether they have confined their practice to adjustment reactions or whether their client base is broader. Such a survey would also reveal whether the perception of respondents to this survey is correct and that counselling psychologists mainly confine their skills to working with individuals, as opposed to couples, families and groups.
The results of this study implied a reluctance by clinical psychologists to accept counselling psychologists as professional equals, even though the standards applied to becoming a chartered psychologist in the UK are viewed as equivalent. A distinction needs to be made between being equivalent, in terms of standard of training and breadth of expertise, and being the same. There is no pretence that counselling psychologists should qualify with exactly the same range of skills and abilities as clinical psychologists. This leads to a contentious issue. What are the similarities and differences between clinical and counselling psychologists? It is reasonable to suggest that training in clinical psychology is closely linked to the needs of the NHS and the career structure of clinical psychologists within the NHS. Most clinical psychology training takes place in mental health services although there is an increasing trend for some training to be undertaken with other popula- tions. Acquiring skills in psychometric assessment and psychological treatments for adults and children is central to their training.
Counselling psychologists, on the other hand, have more explicit experience of the ‘normal’ population and a stronger emphasis on life cycle and developmental approaches to psychotherapy. Assessment and intervention are based less on the use of structured assessment tools and more on individual identification of the problem in the client’s terms. Supervised counselling practice during training often takes place in agencies outside the NHS. It has already been suggested that the strengths
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
16:
16 1
0 O
ctob
er 2
014
436 Sarah Lewis & Robert Bor
of counselling psychology are in the development of the psychotherapeutic relation- ship, personal awareness, research and the application of a different philosophy.
Both clinical and counselling psychologists are trained in the scientist- practitioner approach and are required to attain a level of proficiency in conducting research. Although there are some clear differences in the emphasis of the two trainings, it may be that more meaningful distinctions will emerge from the concep- tual frameworks adopted by the individual chartered psychologists rather than from their generic training. The distinctions are important as they help to identify the respects in which counselling psychology is unique. This should help clarify the role of counselling psychologists within NHS departments who may then be able to use their unique qualities to present for clients options and alternatives which are otherwise unavailable.
The results of the study reveal that there is some confusion about the compe- tencies of counselling psychologists within NHS clinical psychology departments. This has several implications. It appears necessary to provide clearer information regarding the course content and the competencies achieved during training more widely among psychologists. The results of the study showed that clinical psycholo- gists were unaware of the differences between counsellors and counselling psycholo- gists. There appears to be a significant need for the BPS, and particularly the Division of Counselling Psychology, to disseminate the necessary information across its membership. It has been suggested that a clear ‘corporate identity’ will help promote trust in the competence and function of counselling psychology in the community (Guernina, 1995).
Counselling psychology is an evolving speciality. Owen (1 992) suggested three factors which combine to produce a coherent identity: how counselling psychologists perceive themselves; how they are perceived by others; and what they actually do. This study considers only one of these factors. This leaves scope for further research investigating the others. Although this study has revealed some insights into how clinical psychologists currently perceive counselling psychologists, it is interesting to note that there has to date been no national survey of counselling psychologists. Therefore it is not possible to compare these perceptions with what counselling psychologists actually do.
There are various sources of selection bias inherent in the design of the study. The first is sampling bias as although the questionnaires returned reflect a widely distributed sample from across the whole of the UK, it still represents only 53% of the questionnaires sent. Thus, the sample who completed the questionnaire may be significantly different from non-respondents. Each questionnaire was addressed to the Head of Department on the assumption that they would be most likely to reflect the knowledge and attitude of the department as a whole. This may have introduced further bias as the attitudes and knowledge of more recently trained, junior psychologists may be significantly different. Finally, the questionnaire itself, while having face validity, is an unproven instrument from which no statistically significant conclusions can be drawn. Thus, it is not possible to conduct more advanced analysis of the data that would yield greater insights into the issues raised.
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
16:
16 1
0 O
ctob
er 2
014

Clinical psychologists ’ perception of counselling psychologists 437
Conclusion
This study, the first to review the relationship between clinical and counselling psychology in the UK, raises major issues both within counselling psychology itself, and for our closest professional colleagues. The results show that many clinical psychologists do not have a clear understanding of the training and competencies of a counselling psychologist nor how they differ from other counsellors or psycholo- gists. It seems that the issue of identity is a fundamental problem for counselling psychologists. At this stage counselling psychology in the UK is still in its infancy and a clearer professional identity will emerge over time as more counselling psychologists complete their training and begin practice. Their professional identity will also be shaped by the developments in allied specialities and fields such as clinical psychology, counselling and psychotherapy. The problem of professional identity is likely to change and be resolved in three ways: by the Division of Counselling Psychology surveying and publicizing the work of its members; by the Division taking a more proactive approach regarding publicity about what coun- selling psychologists actually do; and by the passage of time.
References
BARKHAM, M. (1990) Counselling psychology: in search of an identity. The Psychologist: Bulletin of the
BEECHWOOD HOUSE PUULISWING LIMITED (1994) The database of NHS management. Essex. TnE BRITISH PSYCHOLOGICAL SOCIETY (1994) The direct0 y of chartered psychologists. Leicester. THE BRITISH PSYCHOLOGICAL SOCIETY (1995) Regulations and syllabus for the diploma in counselling
COLLINS, S. & MURRAY, A. (1995) A pilot project employing counselling psychologists within an adult
GALASSI, J.P. & BROOKS, L. (1 992) Integrating scicntist and practitioner training in counselling psy-
GUERNINA, Z. (1995) The cohesive corporate identity in counselling psychology: public relations in
MCLEOD, J. (1 993) A n introduction to counselling. Buckingham: Open University Press. O\VI!N, I. (1992) The tower of Babel: searching for core clinical, theoretical and ethical issues in
STILES, W.B., SHAI~IRO, D.A. & ELLIOT, R. (1986) ‘Arc all psychotherapies equivalent?’ American
WATKINS, C.E. (1987) On myopia, rhetoric, and reality in counselling psychology. The Counselling
WOOLIT, R. (1990) Counselling psychology in Britain: an idea whose time has come. The Psychologist,
British Psychological Society, 12, 536-539.
psychology. Leicester.
mental health clinical psychology service. Clinical Psychology Forum, 78, 8-1 2.
chology: practicum is the key. Counselling Psychology Quarterly, 5(1), 57-65.
action. Counselling Psychology Review, 10(2), 4-5.
psychothcrapy. Counselling Psychology Quarterly, 5( l), 67-78.
Psychologist, 41, 165-180.
PSycholO&, 15(2), 3 3 2-3 36.
12, 531-553.
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
16:
16 1
0 O
ctob
er 2
014