Embed Size (px)
Citation preview

How Clinicians Use Data For How Clinicians Use Data For Clinical Decision MakingClinical Decision Making
March 5, 2003March 5, 2003Anti-Infective Drug Advisory CommitteeAnti-Infective Drug Advisory Committee
How Clinicians Use Data For How Clinicians Use Data For Clinical Decision MakingClinical Decision Making
March 5, 2003March 5, 2003Anti-Infective Drug Advisory CommitteeAnti-Infective Drug Advisory Committee
John Bradley, MDJohn Bradley, MD
Children’s Hospital San DiegoChildren’s Hospital San Diego

Clinicians’ Use of DataClinicians’ Use of Data
•Clinical informationClinical information– Patient being treatedPatient being treated– Infection being treatedInfection being treated
•Organism information from Organism information from cultures (ID and susceptibility)cultures (ID and susceptibility)
•Antibiotic PK, PD, toxicity Antibiotic PK, PD, toxicity characteristics of the FDA-characteristics of the FDA-approved agents which are active approved agents which are active in vitroin vitro

Clinicians’ Use of DataClinicians’ Use of Data• FDAFDA
– Review of data on safety and Review of data on safety and efficacy, with approval only for the efficacy, with approval only for the particular indications submitted by particular indications submitted by the sponsor (no new indications for the sponsor (no new indications for ampicillin!)ampicillin!)
• The medical literature for The medical literature for preferred antibiotic therapypreferred antibiotic therapy– IDSA guidelines, AAP Redbook IDSA guidelines, AAP Redbook
Committee, Sanford Guide, Committee, Sanford Guide, published clinical trials, etc.published clinical trials, etc.

Clinicians’ Use of DataClinicians’ Use of Data
•Patient informationPatient information– Immune competenceImmune competence
•AgeAge•Co-morbiditiesCo-morbidities•EtcEtc
– Clinical exam, laboratory Clinical exam, laboratory (organ dysfunction (organ dysfunction information) and imaging information) and imaging studiesstudies

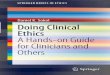
Clinicians’ Use of DataClinicians’ Use of Data
FDAFDA
IDSA, othersIDSA, othersNCCLSNCCLS
CDCCDC
Safety and efficacy Safety and efficacy analysis of submitted analysis of submitted datadata
RecommendationRecommendations for clinicians s for clinicians for treating for treating patients for all patients for all infections, all infections, all abxabx
Organism ID, Organism ID, and and interpretationinterpretations of s of susceptibility, susceptibility, based on in based on in vitro testing, vitro testing, and PD and PD
Epidemiological evaluation of pathogens (particularly resistant ones)Epidemiological evaluation of pathogens (particularly resistant ones)

Clinicians’ Use of DataClinicians’ Use of Data
• Example 1:Example 1:– A 12 year old with leukemia with A 12 year old with leukemia with
neutropenia and pneumonia, grows neutropenia and pneumonia, grows Pseudomonas aeruginosaPseudomonas aeruginosa ceftazidime-resistant, meropenem- ceftazidime-resistant, meropenem- and ciprofloxacin-susceptible from a and ciprofloxacin-susceptible from a bronch washbronch wash
– I will treat with meropenem based on I will treat with meropenem based on safety and efficacy in pediatric safety and efficacy in pediatric meningitis, and published adult and meningitis, and published adult and pediatric data on clinical efficacy of pediatric data on clinical efficacy of carbapenems in pneumoniacarbapenems in pneumonia

Clinicians’ Use of DataClinicians’ Use of Data• Example 2 (pre-Example 2 (pre-HaemophilusHaemophilus vaccine): vaccine):
– 18 month old with periorbital cellulitis 18 month old with periorbital cellulitis and bacteremia (with and bacteremia (with H. influenzaeH. influenzae, type , type b), is being treated with ceftriaxoneb), is being treated with ceftriaxone
– I am asked by a resident why I don’t use I am asked by a resident why I don’t use i.v. TMP-SMZ, as he frequently uses this i.v. TMP-SMZ, as he frequently uses this drug for drug for H. fluH. flu in otitis. in otitis.
– No published series exists on bacteremic No published series exists on bacteremic infections caused by infections caused by H. fluH. flu, treated with , treated with TMP-SMZ. I feel uncomfortable TMP-SMZ. I feel uncomfortable extrapolating from otitis efficacy to extrapolating from otitis efficacy to sepsis and cellulitis efficacysepsis and cellulitis efficacy

When Can You Extrapolate When Can You Extrapolate Efficacy?Efficacy?
• If you can successfully treat a If you can successfully treat a difficult infection, you should difficult infection, you should be able to treat a simple be able to treat a simple infectioninfection

When Can You Extrapolate When Can You Extrapolate Efficacy?Efficacy?
• Some infections are harder to treat Some infections are harder to treat based on penetration of antibiotic to the based on penetration of antibiotic to the site of infectionsite of infection– Poor drug penetration (intra-abdominal Poor drug penetration (intra-abdominal
abscess, meningitis) vs excellent abscess, meningitis) vs excellent penetration (UTI, pneumonia)penetration (UTI, pneumonia)
• Seriousness of infection, spontaneous Seriousness of infection, spontaneous resolution of infectionresolution of infection– Meningitis or pneumonia (Fine Class V) Meningitis or pneumonia (Fine Class V)
vs. AECB or AOMvs. AECB or AOM• Co-morbidities of patientsCo-morbidities of patients
– Healthy young adult vs neutropenia, Healthy young adult vs neutropenia, old age or neonate old age or neonate

When Can You Extrapolate When Can You Extrapolate Safety?Safety?
•Safety of Safety of high dosehigh dose anti- anti-infectives in situations infectives in situations demonstrating borderline drug demonstrating borderline drug exposure to a pathogen in exposure to a pathogen in infected tissuesinfected tissues

When Can You Extrapolate When Can You Extrapolate Efficacy?Efficacy?
• We use published data on safety We use published data on safety and efficacy for infections caused and efficacy for infections caused by a certain pathogen, consider the by a certain pathogen, consider the host and location of the infection, host and location of the infection, antibiotic toxicities and in vitro antibiotic toxicities and in vitro susceptibilities, as well as the risk susceptibilities, as well as the risk of failure, to extrapolate efficacy in of failure, to extrapolate efficacy in using an antibiotic which has not using an antibiotic which has not been previously studied for the been previously studied for the type of infection or the patient type of infection or the patient population we are treatingpopulation we are treating