-
How Can Genetic Information Impact Management?
Dec 3, 2012
Samuel F Berkovic MD FRS
Epilepsy Research Centre
University of Melbourne
American Epilepsy Society | Annual Meeting
-
Disclosure
Name of Commercial Interest
UCB Sanofi-Aventis
SciGen Bionomics Inc
(holds SCN1A patent)
American Epilepsy Society | Annual Meeting 2012
Type of Financial Relationship
Research Support, Speaker
Research Support, Speaker
Research Support
Research Support
-
Learning Objectives
• To appreciate the expanding understanding of genetics in the
causation of epilepsies. • To understand how genetic knowledge can
be applied in everyday clinical practice
American Epilepsy Society | Annual Meeting 2012
-
Outline
• How important is genetics in Epilepsy Causation? Genetic
Epidemiology
“Hidden” Genetics of Epilepsy
• Role in daily Practice Closure to causation; avoid unnecessary
investigation
What tests and when?
Genetic Knowledge that alters treatment
Genetic Knowledge that alters genetic counseling
American Epilepsy Society | Annual Meeting 2012
-
Doctor...….
What is wrong with my child?
Can you cure it?
What caused it?
➤ Clinically, cause is very important
➤ Much of the causation of epilepsy is genetic
The Transfiguration
Raphael
-
Traditional View of Epilepsy Causation
Rochester Study Hauser et al 1975
-
Genetic Epidemiology
1. FAMILIAL AGGREGATION STUDIES Recurrence risk ratio Compare
frequency in particular relatives to controls Epilepsy overall 2.5
in first degree relatives
Generalized epilepsy 4 - 9 Partial epilepsy 2 - 3 Febrile
seizures 3 - 5
-
Constance Absence
Onset 6 yr
Kathryn Absence
Onset 6 yr
Twins of William Lennox, 1949
2003: Seizure free since teenage 8
Slide Unavailable
-
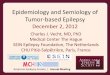
Genetic Epidemiology
2. TWIN STUDIES
Generalised (n = 99) 0.73 0.33 p = 0.0001
Focal (n = 103) 0.34 0.04 p = 0.002
Febrile (n = 180) 0.60 0.14 p = 0.0001
Unclassified (n = 36) 0.43 0.13 p = 0.1
Case-wise concordance
Syndrome Monozygous Dizygous
Berkovic et al Ann Neurol 1998 Vadlamudi and Berkovic 2012 (in
preparation)
-
Genetic Generalized Epilepsy (Helbig et al 2008)
10
Slide Unavailable
-
MULTIPLEX FAMILY STUDIES Select for families with two or more
affecteds - bias Source of most gene discoveries to date
• AD Nocturnal Frontal Lobe Epilepsy
• First epilepsy gene
• Nicotinic receptor (1995)
• Epilepsy channelopathies
-
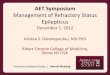
single
gene
epilepsies
epilepsies with
polygenic
inheritance
epilepsies with a major
acquired cause trauma,
infections, vascular etc.
Structural/Metabolic Genetic
The Neurobiological Spectrum of the
Epilepsies
12 Modified from Helbig et al 2008
-
Genes for Epilepsies: Big picture 2012
Ion channel subunits
Voltage-gated (Sodium, Potassium)
Ligand-gated (Nicotinic, GABA)
Non-ion channel genes (LGI1, GLUT1, PRRT2 etc)
Genetic heterogeneity for rare monogenic disorders
Pleiotropic expression of individual genes
Complex Epilepsies (majority of cases)
Common variants (GWAS) – few identified
Rare variants – some identified (CNVs, ion channels, others)
Monogenic Epilepsies (largely dominant, rare)
-
Genes for Epilepsies: Big picture 2012
• Under-ascertainment of family history
• Obvious family history not expected in a complex disorder
Not expected – Importance of de novo mutagenesis Severe
childhood encephalopathies
Dravet syndrome (sodium channel SCN1A)
Other single gene disorders
Copy Number Variants (CNVs)
Milder epilepsies
GLUT-1 deficiency in early onset absence
CNV 15q13.3 in GGE
Hidden Genetics of ‘Sporadic’ Epilepsy
-
Febrile Seizures Dravet syndrome
*SCN1A mutation
Monozygosity confirmed
Dravet syndrome – Discordant MZ twins
15
-
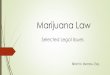
What is the Mechanism for Discordance?
• Study DNA from multiple tissues
– Blood lymphocytes
– Hair
– Buccal cells
– Skin fibroblasts
– Neural cells
Posterior septum and
superior turbinate
Olfactory (nasal) epithelium - source of neural tissue
Contains neuronal precursor cells 16
-
Heterozygous mutation in all tissues
No mutation in any tissue of co-twin
17
-
Vadlamudi et al NEJM 2010 18
-
Post-zygotic Mutations and Mosaicism
Hemimegalencephaly Post-zygotic mutations in 30% in the PIK3CA,
AKT3 or mTOR genes Lee at al Nat Genet 2012; Poduri et al Neuron
2012
Genetically mosaic disease caused by gain of function in
phosphatidylinositol 3-kinase (PI3K)-AKT3-mTOR signaling
Linear nevus sebaceous Post-zygotic KRAS HRAS mutations Groesser
et al. Nat Genet 2012
Can cause severe and lateralized epilepsies
-
Post-zygotic Mutations and Mosaicism
Can cause mild epilepsies
Somatic mutations in SCN1A Mild GEFS+ phenotype
Discovered in parents of Dravet children
Important because of recurrence risk in children
Is this a common phenomenon? Usual in cancer where tumor is
examined
Why not in epilepsies?
Challenging, but not impossible hypothesis to test!
-
Doctor - What caused it?
The Transfiguration
Raphael
Unknown
Idiopathic
Congenital
Trauma Stroke
Others
Mostly Genetic!!
-
Role in Daily Practice
‘Closure’ of diagnosis is very important Patients/Families stop
searching
Allows families to focus on the problem
Empowers families to advocate (eg Dravet foundation)
Avoids unnecessary testing
multiple MRIs
inappropriate pre-surgical work-up
intracranial electrodes
-
Role in Daily Practice What tests and when?
Before thinking tests..
Proper family history!
Precise clinical syndromic diagnosis if possible
Testing
Landscape is rapidly changing
Individual gene testing often costly and low yield but still
appropriate in some cases
Multiple new genes being discovered
Low cost technology for screening multiple genes evolving
Interpretation of tests is an issue
Genetic literacy of Neurologists!
-
High Yield Tests in Appropriate Settings
Copy Number Variation (Array CGH; SNP arrays)
“Epilepsy +“ (see Dr Mefford’s talk)
+ Intellectual Disability
or Autistic Spectrum Disorder
or Congenital Anomalies
or Brain Malformations
Epileptic Encephalopathies
Consider in pediatric and adult clinics
-
High Yield Tests in Appropriate Settings
SLC2A1 sequencing (GLUT1 deficiency)
Classic GLUT1 encephalopathy (De Vivo)
Early-onset Absence Epilepsy (10% cases)
Myoclonic-atonic Epilepsy (5% cases)
Epilepsy and Paroxysmal Exercise induced Dyskinesia
Presentation can be in adolescents and adults!
Treatment implication – ketogenic diet if refractory
-
High Yield Tests in Appropriate Settings
SCN1A Testing Suspected Dravet syndrome
Diagnostic evolution in children well known
Normal infant
Onset 6 months hemi-clonic seizures
Intellectual slowing/regression in 2nd year
Multiple seizure types
Harder to recognize in adults
Gait is a big clue (Rodda et al Arch Neurol 2012)
Treatment implication – avoid sodium channel blockers
-
High Yield Tests in Appropriate Settings
PCDH19 testing – Girls only epilepsy
Familial or sporadic
Onset usually < 3 years
Clusters of febrile seizures every 1-3 months
Focal or generalized convulsive seizures
Many seizures / day for few days
Intellectual disability in 2/3; Regress or never normal
Prominent psychiatric features
ASD, aggression, depression, psychosis
Outcome quite variable
-
High Yield Tests in Appropriate Settings
PCDH19 which girls to test
Female only family history
Sporadic cases in girls
SCN1A negative Dravet
Typical pattern: onset < 3, clusters, psychiatric
features
Management implication – counseling a special challenge
Males are unaffected but transmit gene to daughters
-
Impact on Clinical Care and Practice Role of genetics in
epilepsy under-estimated
- Mendelian epilepsies uncommon - Familial aggregation modest –
complex inheritance - De novo mutagenesis emerging as very
important - Genetics may explain much of the 75% of ‘unknown’
causes
Genetics in daily Practice - Closure to causation; avoid
unnecessary investigation - Directly alter treatment: GLUT1, SCN1A
mutations - Diagnosis essential for counseling Recurrence risk of
de novo mutations Unusual inheritance patterns - Female-limited
epilepsy Prenatal diagnosis