Embed Size (px)
Citation preview

MARCH 2018MARCH 2018
Spotlight
For more information on this article, please visit www.aarp.org/ppi.
How Big is the Problem of Low-Value Health Care Service Use?Keith D. LindAARP Public Policy Institute and OptumLabs® Visiting Fellow
In 2014, the use of 16 low-value health care services accounted for roughly 1.5% (about $5.4 billion) of health care spending for enrollees age 50+ in commercial plans and enrollees age 65+ in Medicare Advantage plans. Unfortunately, the solution to reducing low-value care is hardly straightforward because services that are deemed low value in many cases may actually be of high value in some cases, depending on the clinical circumstances.
A number of studies have reported widespread use of low-value health care services that amount to billions of wasted dollars. Use of these services is considered clinically inappropriate in most cases, such as diagnostic imaging for a simple headache or a cold with a runny nose. (For examples of low-value services, see Figure 1 below.)
Two studies conducted among traditional (fee-for-service) Medicare beneficiaries found that in 2008, 8% of the beneficiaries received at least one low-value service (of 20 measured)1 and in 2009, 25% received at least one low-value service (of 26 measured).2 As for whether this issue is limited to Medicare, another study found that use of low-value care appears to be driven by factors unrelated to payer type or anticipated reimbursement.3
Nevertheless, previous studies have not fully clarified the extent of the problem posed by overuse
of low-value services or the magnitude of related costs. In addition, previous studies have not settled questions about how best to curb low-value service use, or avoid potentially negative impacts caused by actions intended to curb them. Specifically, under the right clinical circumstances, these services can in fact be valuable. The AARP Public Policy Institute examined some of these issues by analyzing health insurance claims data.
How pervasive is low-value service use?We studied the use of 16 low-value services (Figure 1), including cancer screening tests, diagnostic imaging, and invasive procedures, from 2009 to 2014 using Medicare Advantage and commercial claims data from the OptumLabs®Data Warehouse (OLDW), a comprehensive, longitudinal, real-world data asset with de-identified lives across claims and clinical information.4

MARCH 2018
2
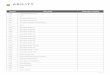
Previous studies have tried to determine how widespread the use of low-value services is but they have not described how this may be changing over time. Our study estimated low-value service use in each of 6 years (2009-2014) allowing us to describe changes over time. Overall, we found that utilization rates in our sample fell over time for all but one
of these low-value services (Figure 1).5 Although declining use rates reflect encouraging trends, we found that total spending on these services by plans and enrollees grew by 3.7% primarily due to the increased cost of expensive invasive procedures.
FIGURE 1Utilization rates of low-value services by age group and insurance type, 2009-2014.
CT indicates computed tomography; COM, commercial insurance; MA, Medicare Advantage; MRI, magneticresonance imaging; PSA, prostate-specific antigen.
Source: Carter EA, Morin PE, Lind KD. Costs and trends in utilization of low-value services among older adults with commercial insurance or Medicare Advantage. Medical Care. 2017 Nov;55(11):931-939.
When we compared our findings with results from other studies of low-value service (Table 1), we found

MARCH 2018
3
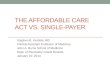
TABLE 1.Comparison of Low-Value Service Rates from OptumLabs Study with Previously Published Studies
Study
Low-Value Service OptumLabs 2009
OptumLabs 2014
Schwartz et al. 2009
Segal et al. 2008
Colla et al.
2006–11
Rosenberg et al.
2011–13
Reid et al. 2013
Charlesworth et al. 2013
Cervical Cancer Screening in Women > 65Commercial 65+ 18.1% 9.9% blank blank blank blank blank blankMedicare Advantage 65+ 10.2% 6.7% blank blank blank blank blank blank
Medicare FFS 65+ blank blank 6.5% blank 9.8% blank blank blankCT/MRI for HeadacheCommercial 18-64 blank blank blank blank blank 14.9-13.4%
(18-50) 1.0% 11.0%
Commercial 65+ 23.9% 22.7% blank blank blank blank blank blankMedicare Advantage 65+ 26.0% 29.6% blank blank blank blank blank blank
Medicare FFS 65+ blank blank 2.4% blank blank blank blank blankCT/MRI for SyncopeCommercial 18-64 blank blank blank blank blank blank 0.1% 9.0%Commercial 65+ 39.1% 37.5% blank blank blank blank blank blankMedicare Advantage 65+ 44.7% 44.3% blank blank blank blank blank blank
Medicare FFS 65+ blank blank 1.0% blank blank blank blank blankCT for Sinusitis Commercial 18-64 blank blank blank blank blank blank 0.3% 3.0%Commercial 65+ 5.2% 4.2% blank blank blank blank blank blankMedicare Advantage 65+ 4.7% 4.0% blank blank blank blank blank blank
Medicare FFS 65+ blank blank 0.3% 1.4% blank blank blank blankCT/MRI for Low Back PainCommercial 18-64 blank blank blank blank blank 53.7%
(18-50) 1.3% 15.7%
Commercial 65+ 6.8% (MRI) 6.7% (MRI) blank blank blank blank blank blankMedicare Advantage 65+ 6.3% (MRI) 5.5% (MRI) blank blank blank blank blank blank
Medicare FFS 65+ blank blank 4.5% 39.5% (MRI) 22.5% blank blank blank
Preoperative Chest X-RayCommercial 18-64 blank blank blank blank blank 91.3–91.5% 0.7% 4.3%Commercial 65+ 13.1% 10.3% blank blank blank blank blank blankMedicare Advantage 65+ 12.8% 11.1% blank blank blank blank blank blank
Medicare FFS 65+ blank blank 1.6% 21.9% blank blank blank blank
Commercial 65+ 0.18% 0.17% blank blank blank blank blank blankMedicare Advantage 65+ 0.15% 0.18% blank blank blank blank blank blank
Medicare FFS 65+ blank blank blank 0.2% blank blank blank blankVertebroplasty or KyphoplastyCommercial 18-64 blank blank blank blank blank blank 0.0004% blankCommercial 65+ 14.3% 13.5% blank blank blank blank blank blankMedicare Advantage 65+ 18.8% 16.2% blank blank blank blank blank blank
Medicare FFS 65+ blank blank 0.3% blank blank blank blank blankHysterectomy for Benign DiseaseCommercial 65+ 0.27% 0.22% blank blank blank blank blank blankMedicare Advantage 65+ 0.16% 0.16% blank blank blank blank blank blank
Medicare FFS 65+ blank blank blank 0.3% blank blank blank blankCT = computed tomography; MRI = magnetic resonance imaging.
Laminectomy

MARCH 2018
4
that some of our findings were comparable. In other cases, however, our low-value service utilization rates diverged dramatically from the published literature. For instance, our rates of diagnostic imaging use for simple headache were more than 10 times greater than those reported by Schwartz and colleagues.6 Conversely, in our sample, diagnostic magnetic resonance images (MRIs) were performed for 6.3% of Medicare Advantage enrollees age 65+ with low back pain in 2009, while Segal and colleagues reported MRIs were performed for 39.5% of traditional Medicare beneficiaries 65+ with low back pain in 2008.7
Such discrepancies may arise from differences in age and case mix of cohorts (e.g., Medicare Advantage enrollees are typically younger and healthier than fee-for-service Medicare beneficiaries while commercial plan enrollees are younger and healthier than most Medicare beneficiaries).
However, the widest variations appear likely to have arisen from differences in service definition and analytic methods. For example, in the measure of diagnostic imaging for headache, the denominator Schwartz and colleagues used included all Medicare fee-for-service beneficiaries in their sample while our denominator included only Medicare Advantage enrollees the first time they presented with a simple headache.
How much money is wasted on low-value services?In our study, we estimated the extent of wasteful spending on low-value services in our data.8 In 2014, we estimated that the use of 16 low-value services amounted to roughly 1.5% of total health care spending for the groups we studied. (See text box.) Nationally, we estimated that this would amount to about $5.4 billion for these groups based on total health care spending.
How did we calculate the cost of low-value services?
To estimate the extent of wasteful spending on low-value services, we started by using cost data from claims in our sample described above. In 2014, utilization of the 16 low-value services we studied cost health plans and enrollees over $418 million ($318 million for commercial age 50+; $101 million for Medicare Advantage age 65+). This amounted to roughly 1.5% of total health care spending for these groups (1.6% for commercial; 1.2% for Medicare Advantage).
To derive a back-of-the-envelope estimate of spending on these services in the US, we applied cost estimates from our study sample to national spending levels for the groups we studied. We assumed that these 16 low-value services were used nationally at the same rates we found for our sample. We estimated that 1.5% of national health care spending for these groups would amount to roughly $5.4 billion based on the market share of health care services represented by our claims data (7% of commercial enrollees age 50+; 12% of Medicare Advantage enrollees age 65+).9 By contrast, total health care spending in the US was over $3 trillion in 2014.10
Other studies have also estimated that annual spending on a limited number of low-value services may amount to billions of dollars ($1.2 billion for 11 services11 and $8.5 billion for 26 services in fee-for-service Medicare12; $32 million for 28 low-value services in a commercially-insured sample of 25 million members).13 These studies have suggested that reducing the use of low-value services could lead to substantial savings.
Differences in spending levels between our estimates and those of previous studies may be due to differences in study population and types of low-value services, as well as differences in the methodology used to compute the estimates.

MARCH 2018
5
Authors of previous studies have noted that the amount of spending on low-value services represents less than 1% of total health care spending for the populations under study. Although no two studies have employed the same set of low-value services, estimates of spending devoted to these services have been consistently under 2% of total health care spending.
Keep in mind that actual spending on low-value services could be much higher than these estimates. Significant indirect costs, as well as serious harm to patients, may arise from unnecessary “downstream” care associated with positive clinical findings from low-value services. For instance, in the case of false positive prostate or cervical cancer screening tests, patients may undergo unnecessary surgery, chemotherapy, and radiation. Therefore, our study and others probably capture only a fraction of the costs incurred by patients and payers for these low-value services. In addition, our estimates do not include the cost of many other services that have been identified as low-value. For instance, the Choosing Wisely Campaign, which encourages patients and physicians to discuss the appropriate use of testing and services to reduce wasteful and unnecessary care, has identified over 500 low-value services.14
What is to be done about the use of low-value services?Advice varies regarding what should be done about low-value service use. Some researchers have suggested that the performance of clinicians, hospitals, and other health care providers should be evaluated, in part, based on their use of low-value services. Some have advocated for measures of low-value care to be linked to insurance coverage and payment for these services. This approach would reduce waste by denying coverage or reducing payment for wasteful services.15
Unfortunately, the solution is hardly that straightforward. Experts have not reached consensus as to what constitutes a low-value service. As noted above, there are substantial differences in the list of services that have been identified for study as low-value, the criteria employed to define each of these services, analytic methods used to cull
low-value services from more appropriate care, and estimates of the cost-burden represented by low-value services.
Of greater concern is that a service characterized as low-value in many cases, may actually be of high value in some cases, depending on the clinical circumstances. For instance, a person with a headache may be having a stroke, which could require an MRI to quickly diagnose.16
For many low-value services, accurate measurement of their appropriate use may not be feasible using currently available claims data, but instead will likely require clinical data. Some researchers have proposed validating claims-based measures of low-value services with clinical data from electronic health records. Indeed, successfully reducing the use of low-value services may require a combination of more innovative and nuanced strategies, such as clinical decision support, shared decision making, physician profiling, and retraining.17
ConclusionThe concerns we have noted are not intended to imply that overuse of low-value care is not a problem. However, more work is needed to effectively reduce the use of these services. The inconsistencies and lack of consensus that we encountered regarding both how to measure and discourage low-value service use suggest that researchers need to address these concerns. For now, it would seem premature for policy makers to link measures of low-value service use to health insurance coverage or payment because this could discourage access to appropriate care. While it may be feasible in the not-too-distant future to discourage low-value care with the deployment of more nuanced strategies, researchers have suggested that the use of low-value services could be difficult to influence by simply adjusting payment rates.18
In the meantime, the Choosing Wisely Campaign’s objective of encouraging patients and their family caregivers to discuss appropriate use of medical services with their clinician seems timely and sensible.19

MARCH 2018
6
1 Segal JB, Bridges JF, Chang HY, et al. Identifying possible indicators of systematic overuse of health care procedures with claims data. Medical Care. 2014;52(2):157-163.
2 Schwartz AL, Landon BE, Elshaug AG, Chernew ME, McWilliams JM. Measuring low-value care in Medicare. JAMA Intern Med. 2014;174(7):1067-1076.
3 Colla, C. H., Morden, N. E., Sequist, T. D., Mainor, A. J., Li, Z. and Rosenthal, M. B. (2017), Payer Type and Low-Value Care: Comparing Choosing Wisely Services across Commercial and Medicare Populations. Health Services Research. doi:10.1111/1475-6773.12665.
4 Wallace, P. J., Shah, N. D., Dennen, T., Bleicher, P. A., Crown, W. H. (2014), OptumLabs: Building a novel node in the learning health care system. Health Affairs (Millwood), 33, 1187–1194.
5 Nasal endoscopy for sinusitis was the only low-value service that increased for all study groups. Carter et al. “Costs and Trends.”
6 Schwartz et al. Measuring low-value care in Medicare.
7 Segal et al. Identifying possible indicators.
8 Carter et al. Costs and Trends in Utilization of Low-Value Services.
9 ($318M/.07) + ($101M/.12) = $5.385B
10 Robert Pear, “Total Health Care Spending in the U.S. Topped $3 Trillion Last Year,” New York Times (December 2, 2015). https://www.nytimes.com/2015/12/03/us/politics/health-spending-in-us-topped-3-trillion-last-year.html.
11 Colla CH, Morden NE, Sequist TD, Schpero WL, Rosenthal MB. (2015), Choosing wisely: prevalence and correlates of low-value health care services in the United States. J General Internal Medicine, 30(2):221-228.
12 Schwartz et al. Measuring low-value care in Medicare.
13 Reid RO, Rabideau B, Sood N. (2016), Low-Value Health Care Services in a Commercially Insured Population. JAMA Internal Medicine.
14 ABIM Foundation. Choosing Wisely Campaign. http://www.choosingwisely.org/.
15 Elshaug AG, McWilliams JM, Landon BE. (2013), The value of low-value lists. JAMA, 309(8):775-776.
16 Mayo Clinic. “Patient Care & Health Information: Stroke.” https://www.mayoclinic.org/diseases-conditions/stroke/symptoms-causes/syc-20350113.
17 Elshaug AG, McWilliams JM, Landon BE. (2013), The value of low-value lists. JAMA, 309(8):775-776.
18 Colla et al., Payer Type and Low-Value Care.
19 ABIM Foundation. Choosing Wisely Campaign. http://www.choosingwisely.org/.Spotlight 31, March 2018
© AARP PUBLIC POLICY INSTITUTE601 E Street, NWWashington DC 20049
Follow us on Twitter @AARPpolicyOn facebook.com/AARPpolicywww.aarp.org/ppi
For more reports from the Public Policy Institute, visit http://www.aarp.org/ppi/.