-
How accurate is model planning A. Sharifi, R. Jones, A. Ayoub,K.
Moos, F. Walker, B. Khambay,
er-impacted anteriorly than predicted by
supine or anaesthetized patient would appear to be the principal
reasons for errors.Keywords: model surgery; orthognathic sur-gery;
articulator; osteotomy.
Current methods of orthognathic surgical
ware.6,13
Model surgery depends on the accuracy
tion of the occlusal plane to the Frankfort
they found a mean difference of 58, which
One of the commonest errors in orthog-
accompanied by inherent errors in the
lator.4,11
Int. J. Oral Maxillofac. Surg. 2008; 37: 10891093://deformity
and malocclusion. Analysis ofModel surgery planning on dental
castsis used for the final correction of facial
horizontal on the Hanau articulator andcompared this with
lateral cephalograms;
adjustment of the instrument to thepatients face and transfer to
the articu-planning involve clinical evaluation,photographs,
freehand surgical simula-tion based on cephalometric tracingand
then transferred to study model sur-gery, and computerized
prediction soft-
of the recording of the dental occlusion inthe retruded position
and the face bowtransfer to the articulator. These record-ings both
have inherent inaccuracies.BAILY and NOWLIN1 measured the
angula-
nathic model surgery occurs in mountingthe models on the
articulator. The accu-racy of the face bow transfer may differfrom
one type of face bow to another. Thekinematic face bow transfer
record isInaccuracies are associated with the transfer of
prediction planning to model surgeryplanning and prediction, which
should be eliminated to improve the accuracy andpredictability of
orthognathic surgery.model surgery. The amount of mandibular
setback was more than that predicted bymodel surgery. None of the
differences between prediction planning and actualsurgical changes
was statistically significant at p < 0.05. Inaccuracy with the
facebow recording, the intermediate wafer, and auto-rotation of the
mandible in thefrom model surgery prediction and a statmaxilla was
more under-advanced and ovthe model surgery allows the transfer
ofplanned three-dimensional movements forthe surgical correction of
complex dento-facial deformities.8
0901-5027/1201089+ 05 $30.00/0 # 2008 Interncorresponded to a
70% error. The three-dimensional accuracy of the position ofthe
upper first molar was highly variableusing four different Hanau
facebows.16
ational Association of Oral and Maxillofacial SurgeoAccepted for
publication 13 June 2008Available online 28 August 2008for
orthognathic surgery?A. Sharifi, R. Jones, A. Ayoub, K. Moos, F.
Walker, B. Khambay, S. McHugh: Howaccurate is model planning for
orthognathic surgery?. Int. J. Oral Maxillofac. Surg.2008; 37:
10891093. # 2008 International Association of Oral and
MaxillofacialSurgeons. Published by Elsevier Ltd. All rights
reserved.
Abstract. The purpose of this study was to evaluate the accuracy
of model surgeryprediction after orthognathic surgery and to
identify possible errors associated withthe prediction process. The
study included 46 patients who had undergoneorthognathic surgical
procedures; 22 in Group Awho had had a Le Fort I osteotomy;and 24
in Group B who had had a Le Fort I osteotomy and mandibular
setbacksurgery. The immediate postoperative and preoperative
lateral cephalograms wereanalysed to calculate surgical changes;
these were compared with those obtained
istical analysis was undertaken. TheS. McHughGlasgow Dental
Hospital & School, GlasgowUniversity, 378 Sauchiehall Street,
Glasgow,G2 3JZ, UKdoi:10.1016/j.ijom.2008.06.011, available online
at http www.sciencedirect.comClinical PaperOrthognathic
SurgeryAssessing the accuracy of orthognathicsurgery by comparing
surgical changeswith model surgery is prudent. It is impor-tant to
recognize why the pre-planned
ns. Published by Elsevier Ltd. All rights reserved.
-
and those predicted. SPSS version 11.5
ior point of the posterior plate. The pro-
model. In 36% (n = 8) the maxilla wasunder-advanced and in 14%
(n = 3) itwas over-advanced in comparison withprediction planning
(Fig. 1). Table 1 shows
There was no statistically significantdifference between the two
groups regard-ing the magnitude of disparities of actual
1090 Sharifi et al.
th.
Table 1. Differences between the actual changes and those
predicted for movements in Group Aalong the X co-ordinate; a
negative sign means less advancement surgically than that
predictedby model surgery
Mean SD Median IQ (25%:75%)
ANS 1.16 1.98 0.80 2.97:0.24PNS 0.20 2.06 0.47 1.04:1.44A 0.20
2.21 0.10 2.36:1.40UIE 0.14 2.34 0.25 2.72:1.08UME 0.32 2.36 0.21
2.33:1.40P point 0.86 2.33 1.03 2.85:0.66M & M 0.34 2.15 0.21
2.49:0.86Abbreviations: A: Maxillary A Point; ANS: Anterior Nasal
Spine; IQ: Interquartile; M&M:Mean of all the maxillary
landmarks; P: The maximum concavity of palate; PNS: PosteriorNasal
Spine; SD: Standard Deviation; UIE: Upper Incisor Edge; UME: Upper
Molar Edge.(Statistical Package for Social Science)was used to
analyse the data.model surgery is not always reflected inthe final
outcome.
Materials and methods
The most common group of patients trea-ted in the authors unit
are those withmaxillary hypoplasia and those with ClassIII skeletal
deformity due to maxillarydeficiency and mandibular
prognathism.This investigation was carried out on 46
patients: 22 in Group A who had had a LeFort I maxillary
advancement and impac-tion; and 24 in Group B who had
hadbimaxillary osteotomies, maxillaryadvancement and impaction with
a man-dibular setback. None of the cases hadsegmental surgery or
facial asymmetry.In all cases the maxillary position wastransferred
to the articulator using an aver-age value condylar face bow
(Dentatusface bow). The upper and lower casts weremounted on a
Dentatus semi-adjustablearticulator.The availability of
preoperative and
immediate postoperative lateral cephalo-grams and casts was
mandatory for thisinvestigation. The following landmarkswere
digitized on all the pre- and post-operative radiographs: ANS
(anteriornasal spine), PNS (posterior nasal spine),A point, UIE
(upper incisor edge), UME(upper molar edge), P (the most
concavepoint of the palate), B point, LIE (lowerincisor edge), LME
(lower molar edge),Pg (pogonion), Me (menton), Ge (genion:the most
posterior point on the lingualcortical aspect of the symphysis
abovethe genial tubercle and usually 12 mmbelow the level of the
lower incisor apex).The pre- and postoperative lateral
cephalograms were superimposed on thebest fit of the anterior
cranial base8 usingAdobe Photoshop 7.0 (Adobe incorpo-rated 2004
USA).The Frankfort horizontal (FHP) was
chosen as the reference line for this study(X axis). A
perpendicular line to the FHPwas drawn from the centre of the sella
(Yaxis). All pre- and postoperative land-marks were measured to
extract X andY coordinates. The actual changes follow-ing surgery
were measured at A and Ppoints for the Le Fort I osteotomy and at
Band Ge points for mandibular setbacksurgery. These changes were
comparedwith the changes predicted by the modelsurgery. Students
t-test was used to iden-tify the skeletal significance of the
differ-ence between the actual surgical changescedure was repeated
after 1 month. TheDahlberg formula was applied to assessthe
magnitude of errors.5,10
Results
The errors in the landmark locationstraced from the cephalogram
were only0.2 mm across the X axis and 0.3 mmacross the Y axis.In
Group A, in 50% of the cases, the
actual forward movement of the maxillawas accurate to within 1
standard deviationof the mean, with that of the predictionError of
methods
The reproducibility of the superimpositionof the lateral
cephalographs was assessed.The pre- and postoperative radiographs
of5 randomly selected cases were superim-posed on the cranial base
of the skull, andthe following 4 landmarks were placed:upper
incisor edge, lower incisor edge,lower antero-inferior point of
anteriorfixation plate, and the most postero-infer-
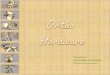
Fig. 1. Difference in advancement between(maximal concavity of
the palate) in Group Athe tendency toward under-advancement ofthe
maxilla.Fig. 2 shows the accuracy of the pre-
diction planning in Group A at point P.Similar to the horizontal
changes, about50% (n = 11) of the cases had anteriormaxillary
impaction similar to the predic-tion values (within 1 standard
deviation ofthe mean). In about 33% (n = 7) the max-illa was
over-impacted, and it was under-impacted in the remainder (n =
4)(Table 2). Posterior maxillary impactionat PNS was similar to
model surgery pre-diction in 64% (n = 14) (Table 2).In Group B (n =
24), a similar pattern of
differences between the actual surgicalchanges and the
prediction movementwas also identified (Tables 3 and 4). Accu-rate
maxillary advancement as predictedwas achieved in 46% of cases (n =
11),with 37% (n = 9) showing under-advance-ment and 17% (n = 4)
over-advancement(Fig. 3). Anterior over-impaction wasnoted in 33%
(n = 8) and posteriorunder-impaction in 25% (n = 6) of cases(Figs.
4 and 5, Table 4).
e actual changes and prediction at point P
-
How accurate is model planning for orthognathic surgery?
1091
tun
tuTable 2. The differences in mm between the acin Group A along
the Y axis; a negative sig
Fig. 2. Difference in impaction between the acconcavity of the
palate) in Group A.maxillary surgical movement and the pre-dicted
values from orthognathic models.In Group B, 46% (n = 11) had an
accuratemandibular setback as predicted in thestudy models.
Over-correction wasdetected in 37% (n = 9) and under-correc-tion in
17% (n = 4) (Fig. 6). The meanvalues showed a tendency towards
settingthe mandible more posteriorly than pre-dicted.None of the
differences detected in
Groups A and B between the actual sur-gical movements and the
predictions from
predicted by model surgery
Mean SD
ANS 0.29 2.38A 0.37 2.97UIE 0.50 2.13P point 0.94 2.01
Table 3. The differences between the actualadvancement in Group
B along the X axis; a nethan that predicted by model surgery
Mean SD
ANS 0.37 2.20PNS 0.73 2.10A 0.50 2.68UIE 0.20 1.98UME 0.39 2.77P
point 0.63 2.92M & M 0.06 2.1
Table 4. The differences between the actualimpaction in Group B
along the Y axis; a nega
Mean SD
ANS 0.42 1.85A 0.25 2.30UIE 0.06 2.45P point 0.65 2.09al changes
and those predicted for movementsmeans more impaction surgically
than that
al changes and prediction at point P (maximalstudy models was
statistically significant(p < 0.05). The difference at ANS
wasclose to statistical significance atp = 0.051.
Discussion
In this study, the maxilla showed a ten-dency to
under-advancement comparedwith the predicted movement in about33%
of the cases in both groups. Thiscould be a result of the
inaccuracy oftransferring the maxillary plane angle
Median IQ (25%:75%)
0.28 1.96:1.350.83 1.69:1.871.13 2.42:1.101.16 2.5:0.22
changes and those predicted for maxillarygative sign means less
surgical advancement
Median IQ (25%:75%)
0.05 1.94:1.190.21 2.41:-0.210.22 1.79:2.630.47 1.13:1.440.62
1.87:2.381.17 2.68:1.160.06 1.67:1.07
changes and those predicted for maxillarytive value means over
impaction
Median IQ (25%:75%)
0.10 1.90:0.810.31 1.94:0.970.14 1.64:0.490.78 2.58:0.57and the
inaccuracy of recording the man-dibular position.The
semi-adjustable articulator used for
model surgery in this study was originallycreated for prosthetic
dentistry. Its facebow was designed to transfer the relation-ship
of the maxilla to the terminal hingeaxis of the mandible. To
accomplish this,the posterior end of the face bow is alignedto the
terminal hinge axis (middle of con-dyle), and the anterior end is
aligned to theorbitale. These points define a plane calledthe
axis-orbital plane,7,9 which is relatedto the upper cross arm of
the articulator tomount the maxillary occlusal model.The upper
cross member of the articu-
lator represents the Frankfort horizontalplane, which may not be
horizontal(Fig. 6), as assumed in designing the exist-ing
semi-adjustable articulator. This couldcause errors in model
planning becausemost vertical measurements made duringmodel surgery
are parallel to a referenceline, usually the upper arm of the
articu-lator. When the maxilla is impacted in ahorizontal plane
superiorly on the articu-lator, the magnitude of the upward
move-ment is related to a horizontal referenceline. The extent of
the impaction is dif-ferent when the cast has been mountedwith an
angle between the occlusal planeand the upper member of the
articulator,which is different from the real anglebetween the
occlusal plane and the Frank-fort horizontal in that patient, for
which adifferent amount of impaction would berequired.7 A more
anterior maxillaryimpaction would be needed surgicallythan that
predicted by model surgery tocompensate for the steepness of the
max-illary plane angle on the articulator; thiswas true in 33% of
the cases in this study.When using a conventional articulator
for orthognathic surgery, it is essential thatthe angle between
the occlusal plane andthe Frankfort horizontal for the patient
isthe same as the angle between the occlusalplane and the upper
member of the articu-lator on the maxillary model. If this
isincorrect, the result of the model surgeryis erroneous.The
authors suggest that every indivi-
dual lateral cephalogram should bechecked for the accuracy of
the mountingof the maxillary cast on the articulator.Further
research is needed to prove andconfirm the accuracy of this
hypothesis.GATENO et al.9 showed that if there were
a 128 difference between the Frankforthorizontal plane and the
axis-orbital plane,with bimaxillary model surgery, the max-illa
would move 15% less than desired formaxillary advancement. In the
presentstudy, in about 33% of cases, the maxilla
-
1092 Sharifi et al.
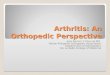
Fig. 5. Difference in impaction between the actual changes and
predictions at PNS in Group B.
Fig. 4. Difference in impaction between the actual changes and
predictions at point P (maximalconcavity of the palate) in Group
B.
Fig. 3. Difference in advancement between the actual changes and
predictions at point P(maximal concavity of the palate) in Group
B.showed under-advancement from that pre-dicted for both groups.The
other source of error is the differ-
ence in the patients mandibular positionwhen supine and upright;
the mandibletends to be positioned more posteriorlywhen the patient
is lying down and themouth has been actively closed into therelaxed
position of centric occlusion.12
BOUCHER and JACOBY3 reported that themandible was positioned up
to 2 mmmoreposteriorly in the anaesthetized patient. Aslight
posterior displacement, with a ver-tical drop of the condyle (mean
2.4 mm)under general anaesthesia was reported.15
BAMBER et al2 recommended recording thecentric relationship in
the supine con-scious position when planning
bimaxillaryosteotomies. All the cases in the presentstudy had the
wax bite and face bow takenin the upright position and in
centricocclusion. This would have registeredthe mandible in a more
anterior positionthan its location when the patient waslying flat
under general anaesthesia. Oncethe maxilla was down-fractured at a
LeFort I level, the mandible would be theonly reference point to
adjust the maxil-lary position in an antero-posterior direc-tion
using the occlusal wafer. Therefore,less maxillary advancement
would beachieved than predicted on the articulatorowing to the more
posterior mandibularposition. The mandible has been over-corrected
(more setback) to compensatefor maxillary under-advancement.The
other possible source of errors in
planning orthognathic surgery is inherentin the nature of
mandibular hinge axis andthe consequences of its application
inprediction planning. The true hinge axisof mandibular rotation is
the axis exactlylocated as a result of the combined rotationand
translation of the condyles. It has beenshown that an insignificant
gliding of thecondyles of 0.5 mm significantly displacesthe located
hinge axis. The inaccuracy inregistering and transferring the true
hingeaxis of the condyle to the articulator wouldcause errors in
predicting mandibular rota-tion secondary to maxillary surgery.
Usingthe current instrumentation, discrepanciesbetween the true
hinge axis and the trans-ferred axis for the mounted casts on
semi-adjustable articulators are inevitable.14
Intermediate wafers are another majorsource of inaccuracy. After
a Le Fort Iosteotomy and mobilization of the max-illa, the wafer
places the maxilla in thepre-planned position relating it to
themandible for fixation. Under generalanaesthesia, the muscles of
masticationare relaxed and the mandible wouldnot serve as a fixed
reference plane for
-
5. DahlbergG. Statistical method for med-ical and biological
students. Interscience
How accurate is model planning for orthognathic surgery?
1093
na 1maxillary surgery. In addition, the wafercannot be placed
exactly in the pre-planned position because there are noanatomical
references points outside theosteotomy cuts against which a check
canbe made. An instrument that would placethe intermediate wafer in
its correct rela-tion to the Frankfort horizontal or visualaxis
plane should be designed. Thisinstrument should be able to transfer
reli-able anatomical references (e.g. externalauditory meatus and
nasion) from patientto articulator. If there were clear anato-mical
references, which act as externalframes of reference, these could
guide thewafer into the planned position moreaccurately.There were
no statistically significant
differences between the predicted andactual changes, mainly due
to the smallsample size, however, this study has iden-tified clear
differences in some casesbetween what was planned and
achieved.These discrepancies may produce an unac-ceptable
occlusion, therefore every effortshould be made to address the
disparity
Fig. 6. Frankfort plane. (After DOWNS WB. Abetween model
planning and surgicalplanning.This article did not investigate the
clin-
ical significance of the mismatch betweenmodel prediction and
actual surgicalchange, but it did prove its existenceand highlight
ways of improving orthog-nathic model surgery. The use of a
spe-cially designed orthognathic articulatorthat takes into
consideration anatomicalvariations, accurately locating the
mand-ible in three dimensions and reproducingits autorotation,
should improve orthog-nathic model surgery.New York 1940.6.
Donatsky O, Hillerup S, Jorgensen
JB, Jacobsen PU. Computerised cepha-lometric orthognathic
surgical simula-tion, prediction and postoperativeAcknowledgements.
The authors wouldlike to thank Mrs A Maguire and Ms AMcCormack for
their help in compilingthis manuscript.
References
1. Bailey JO, Nowlin TP. Accuracy ofFrankfort plane transfer of
the Hanauarticulator. J Dent Res 1981: 60: 531.
2. Bamber MA, Firouzai R, Harris M,Linney AD. A comparative
study oftwo arbitrary face bow transfer systemsfor orthognathic
surgery planning. Int JOral Maxillofac Surg 1996: 25: 339343.
3. Boucher L, Jacoby J. Posterior bordermovement of the human
mandible move-ments. J Pros Dent 1961: 11: 836.
4. Bowley JF,MichaelsGC, Lai TW, LinPP. Reliability of face bow
transfer pro-cedure. J Pros Dent 1992: 67: 491498.
lysis of the dentofacial profile. Angle Orthodevaluation of
precision. Int J Oral Max-illofac Surg 1992: 21: 199203.
7. Ellis E, Tharanon W, Gambrell K.Accuracy of face bow
transfer: Effects onsurgical prediction and post surgicalresult. J
Oral Maxillofac Surg 1992: 50:562567.
8. FONSECA RJ. Oral Maxillofac Surg. Saun-ders: Philadelphia,
2nd Vol. 2000, Chap-ter 5, p. 98.
9. Gateno J, Forrest KK, Camp B. Acomparison of three methods of
facebow transfer recording: Implication fororthognathic surgery. J
Oral MaxillofacSurg 2001: 59: 635640.10. Ghafari J, Engel FE,
Laster LL.Cephalometric superimposition on thecranial base: A
review and a comparisonof four methods. Am J Orthod
DentofacOrthopod 1987: 91: 403413.
11. Gold BR, Setchell DJ. An investiga-tion of the
reproducibility of face bowtransfer. J Oral Rehab 1983: 10:
495503.
12. Helkimo M, Ingervall B, CarlssonGE. Variation of retruded
and muscularposition of mandible under recordingconditions. Acta
Odonto Scand 1971:29: 423427.
13. Loh S, Yow M. Computer prediction ofhard tissue profile in
orthognathic sur-gery. Int J Adult Ortho Orthognat Surg2002: 17:
342347.
14. Lotzmann U. Considerations of preci-sion and consistence of
mandibular trans-verse hinge axis Zentrum fur Zahn-Mund-und
Kieferheilkunde, 99. derGeorg-August-Universitat Gottingen1990: p.
372379.
15. McMillan LB. Border movements ofhuman mandible. J Pros Dent
1972: 27:524.
16. OMalley MA, Milosevic A. Compar-ison of three face bow/semi
adjustable
956: 26: 192212.)articulator systems for planning orthog-nathic
surgery. Br J Oral Maxillofac Surg2000: 38: 185190.
Address:Ashraf F. AyoubGlasgow Dental Hospital &
SchoolProfessor of Oral & Maxillofacial Surgery378 Sauchiehall
StreetGlasgowG2 3JZUnited KingdomTel: +44 141 211 9604Fax: +44 141
211 9601E-mail: [email protected]
How accurate is model planning for orthognathic
surgery?Materials and methodsError of
methodsResultsDiscussionAcknowledgementsReferences