Embed Size (px)
Citation preview
Hospitals and Community Health &
Development
Dr. Anil CherianDirector, Community Health &
DevelopmentEmmanuel Hospital Association
India

Outline of the Presentation
• Community health & development in EHA
• Role of the hospital
• Changes in the context. Redefining the relationship between hospitals and community based programmes.
• Principles of primary care that should be incorporated in to hospital services and care.

Emmanuel Hospital Association
• Federation of 20 Christian mission hospitals.– Started in 1971 – 37 years old– 15 hospitals are rural– 5 hospitals semi-urban
• 29 community health & development projects.– 20 locations – 18 are linked to hospitals and 2
are stand alone.– The projects cover 3 million people

DevelopmeDevelopment Status nt Status MapMap
EHA Units in EHA Units in IndiaIndia
Development of Community Health in EHA
• 70’s – Hygiene education / Community Outreach.• 80’s – Primary Health Care. 1984 EHA’s first PHC
project started (SHARE project started by Dr.Ted Lankaster.
• 90’s – Expansion of the Community Health involvement.
• 2000 – Repositioning of Community Health Projects in the context of over all development.

EHA Vision for communitiesEHA Vision for communities
Empowered communities that are healthy, learning, prospering, caring, stewards of their natural resources, living in harmonious relationship, living in a clean and safe environment, worshiping the true and living God and reaching out to others in need.
Kacchwa, 2001Kacchwa, 2001

Determinants of healthDeterminants of health


EHA Organizational ObjectivesEHA Organizational Objectives
A. The major disease burden of the communities served by our institutions and projects are reduced equitably, through their participation and at a cost that they can afford.
B. Communities prosper economically, demonstrating good stewardship of their available resources, living in a safe and clean environment, constantly learning, demonstrating mutual trust, cooperation and caring attitudes towards other communities.
C. Individuals, families and communities become disciples of Jesus Christ
EHA Strategic Review December 2007

Profile of our Current Community Work
Disease Disease SpecificSpecific
HIV
Tuberculosis
Malaria
Advocacy Advocacy & & Community Community MobilizatioMobilizationn
Water, Sanitation & Hygiene
Literacy & Education – Formal, Non-formal, Vocational
Basic Health Care for common illness
Nutrition / Food security
Thrift/Savings
Micro-finance
Income generation / Livelihood

Micro birthMicro birth planplan
Community Community Analysis Analysis
using using 4 delays4 delays
CapacityCapacity buildingbuilding
SHG role/supportSHG role/support activitiesactivities
CommunityCommunity level level
sensitizationsensitization
Service Service deliverydelivery
Community Community BasedBased
Monitoring Monitoring
AdvocacyAdvocacy
Village health Village health planplan
Maternal Maternal ChildChild
HealthHealth

Reproductive & Child Health

Reproductive & Child Health
Immunisation

Women’s literacy

Women’s literacy

Participatory Learning Exercise

Women Action Group

Women’s groupsWomen’s groups

Walk for malaria

CBOs initiative for Health facilities

Monthly Volunteer’s Meeting

Challenges & choicesChallenges & choices• Shift from a hospital / disease focus to Shift from a hospital / disease focus to
a community health focus.a community health focus.
Social Determinants of health
Health Promotion
Preventive
MedicinePrimary Care
Secondary Level Care Rehabilitation
Integrated Programmes
Continuum of careContinuum of care

Role of the hospitalRole of the hospital
• Initiate the Community Project. – Hospital reputation is important for entry in to the community.
• Administrative support • Technical resource persons
– Health care– Training
• Facilities shared reducing overhead expenses.
Role of the hospitalRole of the hospital
• Important to support communities initiatives with critical / emergency care.
• Financing
• Accountability
• Provide a faith community and family support to community health programme staff.
• Provide linkages with partners

Disadvantages
• Ownership
• Suspicion or mistrust
• Conflict of interests– sharing of resources
• Attitudes of hospital staff
• Pre-conceived notions
• Different time frameworks
• Ghetto or “mission compound” mentality

A different drumbeat
Changes in the context

Non communicable Diseases
• The new killers – CVD, Diabetes, Mental Illness including substance abuse, Injuries which include Accidents, RTA and Suicide, Asthma and COPD
• Dual burden of disease.• Risk-reduction / behaviour change• Need for integrated “continuum of
care” programmes
Health Care Financing -India
• 82.4% of health care expenditure occurs in the private sector of which 77.5% is from out-of pocket payments.
• Of the 5% of GDP spent on health care the government contribution is only 17.8% which amounts to 0.9% of GDP.
• Health care in India is the most privatized in the world

Medical expenses and impoverishment
• Survey conducted in 3 districts in Gujarat and Andhra Pradesh - 85% of the households in Gujarat and 74% of those in AP health expenses was the main reason for their economic decline.
• World Bank estimates that OOP pushes 2.2 % health users in poverty and 1in 4 among those hospitalised.

Catastrophic Health Expenditure
• A adverse health condition that necessitates more than 10% of the household income in medical expenses (Pradhan 2002)
• Illness leads to loss of income and significant extra expenditure. The combination pushes people in to poverty.
• 9% of households in India experience catastrophic health expenditure
• Catastrophic health expenditure is more common in the low income group, but it can also effect the middle income group.
Access to Essential / Life Saving drugs
• WHO lists 270 drugs as essential – take care of 95% of the health problems.
• 60,000 to 80,000 brands of various drugs in India• 10 of the top 25 drugs sold in the Indian market
are non essential, irrational or hazardous.• 56% of the people in India still do not have access
to essential drugs (WHO 2004)• Deregulation of drug price control has led to
spiralling of costs with profit margins being increased to 75-100%

Price variations in drugs
Medicine Brand CompanyPrice in
INR Difference
Ofloxacillin 200 mg
ZO FDC 3.2
Tarivid Aventis 31 969%
Levofloxacillin 500 mg
Levoflox Cipla 6.82
Travanic Aventis 95 1392%
Amlodepine 5 mg
Amolodac Zidus 1.51
Amlogard Pfizer 6 397%
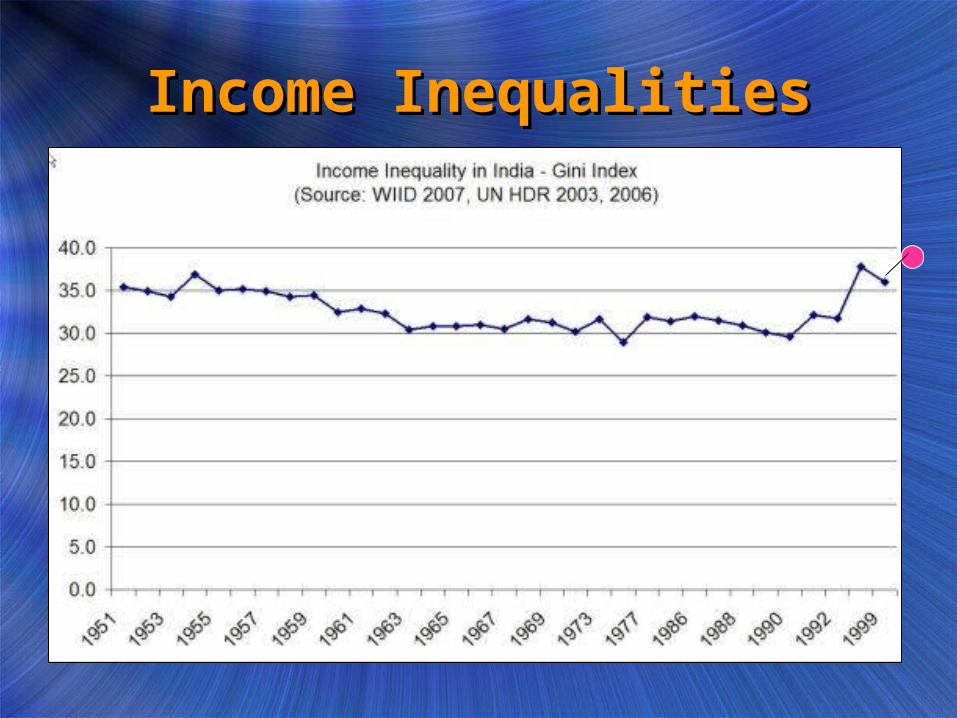
Income InequalitiesIncome Inequalities
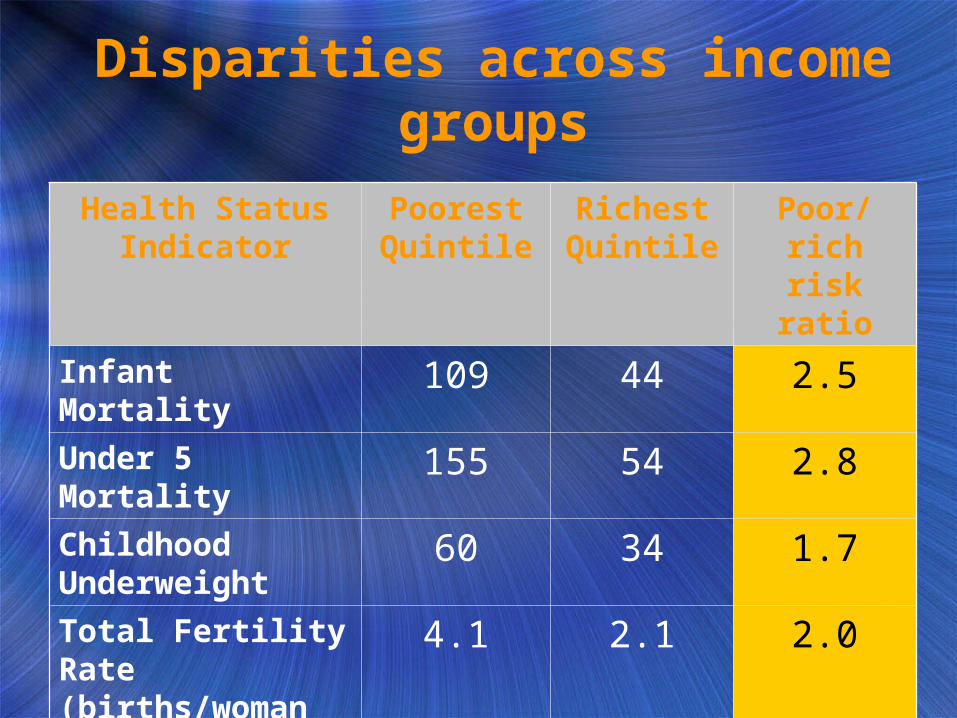
Disparities across income groups
Health Status Indicator
Poorest Quintile
Richest Quintile
Poor/ rich risk ratio
Infant Mortality 109 44 2.5
Under 5 Mortality 155 54 2.8
Childhood Underweight
60 34 1.7
Total Fertility Rate (births/woman age:15-49)
4.1 2.1 2.0
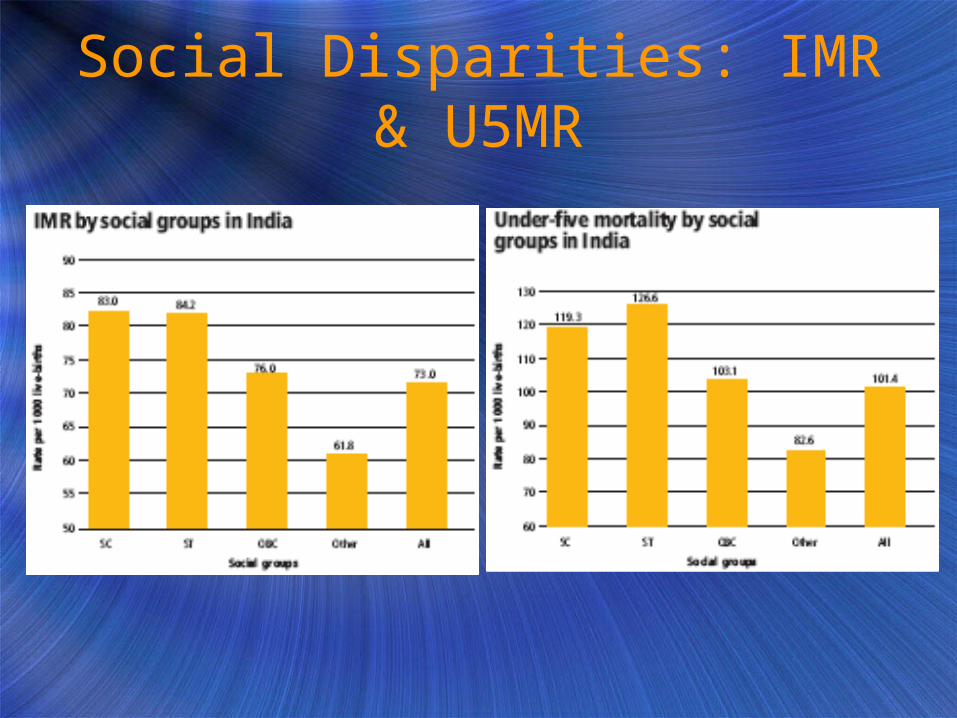
Social Disparities: IMR & U5MR

Impact of Climate ChangeImpact of Climate Change
• Migration of families in search of livelihood.
• Increase in natural disasters

Impact on the programsImpact on the programs
• Health disparities: Averages cannot the only way to summaries data and it is important to look at the data in different groups.
• Hospitals need to synchronize with community based initiatives. Joint planning
• Good quality health care is an important adjuvant to community programmes
• Engage with Government programmes• Establish linkages with Government programme
and to access available resources – private-public partnerships.
Can the principles of Primary Health Care be incorporated in to hospitals to synchronize them with community based programmes?
Applying the Principles of “Primary Health care” to hospitals
• Demystifying medicine – strengthen patient education. Using patients to educate others in the community.
• Participation of the family and the larger community (volunteers) in caring for the patients.
• Using the community as gatekeepers for directing services.
• Community advisory committee in hospitals• Making healthcare affordable.• Vertical equity – differential pricing / cross
subsidization

Applying the Principles of “Primary Health care” to hospitals
• Rational drug therapy
• Use of only appropriate/ cost-effective technology.
Conclusions
• Hospitals can be a good launch pad for community based health programmes
• There are potential synergies in having community health programmes

Thank you for listening