Embed Size (px)
Citation preview

Hospital Mortality in Acute Myocardial Infarction in the Era of Reperfusion Therapy
(the Myocardial Infarction Triage and Intervention Project)
Charles Maynard, PhD, W. Douglas Weaver, MD, Paul E. Litwin, MS, Jenny S. Martin, RN, Peter J. Kudenchuk, MD, Timothy A. Dewhurst, MD, Mickey S. Eisenberg, MD, PhD,
Alfred P. Hallstrom, PhD, and Joseph Chambers, MD, for the MIT1 Project Investigators
This study was conducted in 19 hospitals in the metropolitan Seattle area and included 6,270 UR selected patients who had acute myocardial infarction (AMI) between January 1966 and April 1991. Hospital mortality was determined and re- lated to patient demographic and clinical charao teristics, the use of reperfusion therapies, and to complications after AMI. Thrombolytic therapy or direct coronary angioplasty <6 hours from symp tom onset was used to treat 1,165 (19%) and 524 (9%) patients, respectively. There were 629 (10%) hospital deaths; most occurred during the first 3 days of hospitalization. Factors affecting mortali- ty after admission included: recurrent chest pain, recurrent AMI, development of heart failure, and the occurrence of stroke. After adjustment for age, treatment with thrombolytic therapy or direct angioplasty had no independent effect on reduc- ing the overall mortality rate. Hospital mortality rates for AMI have improved considerably since 1970, although recurrent myocardial ischemic events continue to have an adverse effect on out- come. The current use of reperfusion treatments has had minimal causal impact on overall mortali- ty rates, principally because less than one third of patients, who are relatively “low risk,” are es@- ble and receive these treatments.
(Am J Cardiol1993;72:877-662)
From the Department of Medicine, School of Medicine, and the De- partment of Biostatistics, School of Public Health and Community Medicine, University of Washington, Seattle, Washington. This study was supported by Grant ROl HL38454 from the National Heart, Lung, and Blood Institute, Bethesda, Maryland, and by an unrestricted grant from Genentech, Inc., South San Francisco, California. Manuscript received March 16, 1993; revised manuscript received and accepted June 2, 1993.
Address for reprints: Charles Maynard, PhD, MIT1 Project HL-21, 1910 Fait-view East, #205, Seattle, Washington 98102.
S ince 1970, the number of patients hospitalized for acute myocardial infarction (AMI) in the United States has steadily increased, yet case fatality rates
have steadily declined.’ In previous studies of in-hospi- tal mortality for AMI, age, sex, evidence of prior car- diac illness, type of infarct (Q-wave vs non-Q-wave), and the location and size of the infarct as well as resul- tant left ventricular function, each have been identified as important predictors of hospital mortality.2-4 In the past decade, aspirin and thrombolytic therapy have each been shown to be effective in reducing mortality in patients considered appropriate for treatment with these drugs.5 Other means of coronary reperfusion, including direct coronary angioplasty, rescue angioplasty of failed thrombolytic drug treatment, and coronary artery bypass surgery have also been evaluated.6,7 Since these re- perfusion therapies may prevent damage to jeopardized myocardium, it is important that serious silent and symp- tomatic (recurrent angina) myocardial ischemia be de- tected during the course of hospitahzation.4,8 This study examines, in the era of reperfusion therapy, factors affecting hospital mortality, when death occurred, and the event immediately preceding death.
METHODS Patient population: From January 1988 through
April 1991, 6,270 patients with AMI were admitted to 19 hospitals in King County, Washington, which in- cludes the city of Seattle. The hospital records for each consecutive patient were reviewed, and relevant infor- mation was recorded on study data forms and entered in the Myocardial Infarction Triage and Intervention (MITI) database. The details of this project as well as the scope of the database have been described.9
This population-based study contains all patients who had contirmation of AMI at discharge or death as indicated by coronary care unit logs and review of dis- charge diagnoses from medical records. The small num- bers of patients with AMI complicated by cardiac arrest and resuscitation before hospital admission were exclud- ed as were patients who developed AMI after admission for treatment of another medical problem (e.g., subse- quent to noncardiac surgery). During this 3-year study, 94% of patients had 1 hospital admission for AMI, 5% had 2 admissions, and 1% had 23 admissions for AMI.
Study variables: Demographic and diagnostic vari- ables were collected and included age, sex, race, mode
ACUTE MYOCARDIAL INFARCTION MORTALITY 877

1 r TABLE I MIT1 Classification of Terminal Events in Patients with Acute Myocardial Infarction
Sudden death Abrupt and unanticipated cardiac arrest with loss of blood pressure and/or pulse in patients with previous apparently stable blood pressure
Cardiogenic Rapid deterioration ( < 1 hour) of blood pressure and/or shock pulse, usually characterized by progressive hypoten-
sion requiring vasopressors or pulmonary edema rap- idly leading to death. Also defined as immediate and unanticipated cardiac arrest with loss of blood pres- sure and/or pulse but preceded by unstable blood pressure or worsening congestive heart failure
Myocardial failure
Gradual deterioration (> 1 hour) of blood pressure and/or pulse, characterized by progressive hypoten- sion requiring vasopressors and is distinguished from cardiogenic shock by duration of symptoms and signs
Other deaths Includes neurologic sequelae, procedure-related, and noncardiac causes such as sepsis, cancer or respira- tory failure
MIT1 = Myocarcial Infarction Triage and Intervention project.
of hospital transport, and initial and discharge diagnos- tic categories. Vital status and date of discharge or death were determined. Clinical variables, as indicated in the medical record, included history of angina before admis- sion, prior myocardial infarction, known congestive heart failure or pulmonary edema systemic hypertension, hyper- lipidemia, coronary artery surgery, coronary angioplasty, and prior treatment with thrombolytic therapy. Informa- tion about clinical status at the time of admission, treat- ments and procedures administered, cardiac complica- tions (new heart failure, recurrent chest pain, reinfarc- tion), and the occurrence of hospital events was also recorded.
For patients who died before discharge, the number of hours until death and mode were recorded. All rec- ords pertaining to the deaths were reviewed by investi- gators (JC, JSM) in order to characterize the circum- stances of death. Complete data were present in 525 patients (83% of deaths); information for the remaining patients who died was not available. The terminal event preceding death was classitied as 1 of 4 categories (Ta- ble I). Also, the lirst cardiac rhythm associated with death was classilied in all patients who were monitored at the time of collapse. Cardiac rhythms were grouped as follows: (1) ventricular tachycardia/ventricular fibril- lation, (2) asystolekxadycardia, or (3) “other,” which included electromechanical dissociation.
Statistical methods The cl-&square statistic and the t test were used to test for differences in character- istics between survivors and those who died during hospitalization. Age adjusted p values were computed with the Mantel-Haenszel test. Multiple stepwise logis- tic regression was used to identify the predictors of hos- pital mortality. These analyses included baseline charac- teristics as well as signiticant events occurring during the course of hospitalization.
RESULTS Univariate results: The overall hospital mortality
was 10% for the 6,270 patients. Hospital mortality rates
TABLE II Hospital Mortality and Patient Characteristics at the Time of Hospital Admission
Mortality P Age-Adjusted Characteristic Number Rate L%) Value p Value
Age (years) <0.0001 25-50 782 1.4 50-64 1,838 4.5 65-74 1,737 11.1 75-79 752 14.1 80-84 623 20.1 85+ 466 24.0
Gender 10.0001 0.01 Men 4,059 8.3 Women 2,140 13.7
Weight (kg) <0.0001 0.0008 160 831 14.8
60-74.9 1,669 10.1 75-89.9 1,795 6.8 90-99.9 684 5.6 100+ 553 3.1
Race 0.17 0.77 White 5,332 10.7 Black 233 6.9 Other race 253 9.9
Prior angina 0.08 0.20 Yes 2,409 11.1 No 3,467 9.3
Prior systemic 0.52 0.68 hypertension*
Yes 2,886 10.3 No 3,229 9.9
Prior myocardial 10.0001 0.006 infarction
Yes 1,715 12.5 No 4,356 9.0
Prior congestive < 0.0001 <0.0001 heart failure
Yes 806 19.7 No 5,343 8.5
Known hyperlipi- <0.0001 < 0.0001 demia*
Yes 1,247 4.6 No 4,846 11.5
Prior coronary 0.024 0.20 angioplasty
Yes 332 5.7 No 5,853 10.3
Prior coronary 0.66 0.34 bypass surgery
Yes 615 11.1 No 5,576 10.0
Mode of hospital <0.0001 <0.0001 arrival
Paramedic 2,920 12.4 Ambulance 802 13.0 Self-transport 2,043 6.1 Other 51 11.8
Hospital arrival 0.008 0.02 < 6 hours from
symptom onset Yes 3,982 9.0 No 1,051 11.7
Chest pain present at <0.0001 0.62 time of admission
Yes 5,722 9.4 No 464 18.3
Cardiogenic shock < 0.0001 <0.0001 on admission
Yes 123 45.5 No 6,068 9.4
*As indicated in the medical record.
878 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 72 OCTOBER 15, 1993

increased with age, were higher for women, and de- creased with increasing body weight (Table II). Patients with known hyperlipidemia had significantly lower hos- pital mortality, whereas those with prior myocardial in- farction and prior congestive heart failure had higher mortality. The mortality rate for patients who were ad- mitted with cardiogenic shock was 36% in 50 patients who were initially treated with thrombolytic therapy, coronary angioplasty, or coronary artery bypass surgery, and was 52% in 73 patients who did not receive these initial treatments (p = 0.08).
The apparent beneficial effects of thrombolytic ther- apy, direct angioplasty, and early cardiac catheterization on mortality were no longer evident after age adjustment (Table III). Reperfusion therapies (thrombolytic therapy or direct coronary angioplasty <6 hours from onset of chest pain) were used in 1,627 patients (26%). Patients receiving these therapies were younger (64% aged ~65 years vs 35% in those not receiving these treatments), less often had a history of previous myocardiaf infarc- tion (21 vs 30%), and had less co-morbidity, including diabetes and renal failure (6 vs 13%).
Within age strata, patients receiving reperftision ther- apies had in-hospital mortality rates 0 to 17% lower than those not receiving these therapies; the greatest differ- ence was in older patients (Figure 1). The occurrence of recurrent chest pain and reinfarction was similar in both groups, although evidence of new congestive heart fail- ure was more common in those not receiving reperfu- sion therapies (Figure 2).
In-hospital mortality was significantly higher in pa- tients who developed evidence of reinfarction, new-onset congestive heart failure, or stroke in the days after ad- mission (Table III). Strokes from all causes occurred in 2.1%, with hemorrhagic strokes (both parenchymal hem- orrhage and hemorrhagic conversion of infarct) resulting in 0.6% of all patients, 0.4% of patients not receiving thrombolytic therapy, and in 1.3% (95% confidence in- terval, l.O%, 1.6%) of those treated with thrombolytic drugs. Over 40% of the 37 hemorrhagic strokes occurred in 21% of patients receiving thrombolytic therapy.
flGURE 1. Inhospital mortalRy by age for patients treated with direct angioplasty or thrombolytic therapy (ll), or both, <6 hours from onset of symptoms versus those not so treated. Pet = percent; PTCA q direct percutaneous transluminal coronary at@- Nasty.
Multivariate results Multiple stepwise logistic re- gression using factors listed in Tables II and Ill (stroke was not included) was used to identify variables associ- ated with hospital mortality in 5,112 patients for whom complete information was available. In order of entry the following variables were independently associated
TABLE Ill Mortality, Treatments and Complications After Hospital Admission
Mortality p Age-Adjusted Characteristic Number Rate f%) Value p Value
Thrombolytic therapy < 0.0001 0.58 ~6 hours
Yes 1,185 6.7 No 5,014 11.0
Direct coronary 0.01 0.89 angioplasty < 6 hours
Yes 524 6.9 No 5,617 10.4
Cardiac catheterization 0.003 0.75 < 6 hours (no angio-
plasty) Yes 383 5.7 No 4,983 10.5
Bypass surgery ~48 0.22 0.99 hours from admission
Yes 187 7.5 No 6,012 10.2
Recurrent chest pain <0.0001 <0.0001 Yes 1,553 12.7 No 4,394 8.9
Recurrent myocardial <0.0001 <0.0001 infarction
Yes 256 36.3 No 5,691 8.7
New-onset congestive < 0.0001 <0.0001 heart failure
Yes 1,421 18.1 No 4,565 7.5
Any stroke <0.0001 <0.0001 Yes 123 35.8 No 5,821 9.4
Intracranial hemorrhage < 0.0001 <0.0001 Yes 37 54.1 No 5,903 9.6
25 r
20
P C t 15
D e 10 a d
Pm.95 Pm.62 Pm.53
50-64 65-74
Age
Pm.41
No TT or PTCA D TT and/or PTCA
N.4672 N-1626
ACUTE MYOCARDIAL INFARCTION MORTALITY 879

with higher hospital mortality: advanced age (for each lo-year increase), reinfarction during hospitalization, new onset of congestive heart failure, history of conges- tive heart failure, cardiogenic shock on hospital arrival, and recurrent chest pain. Greater body weight (for each 10 kg increase) and presence of known hyperlipidemia were predictive of lower mortality (Figure 3). After ad- justment for these predictors, neither direct angioplasty (p = 0.84) nor thrombolytic therapy (p = 0.43) reduced overall hospital mortality rates.
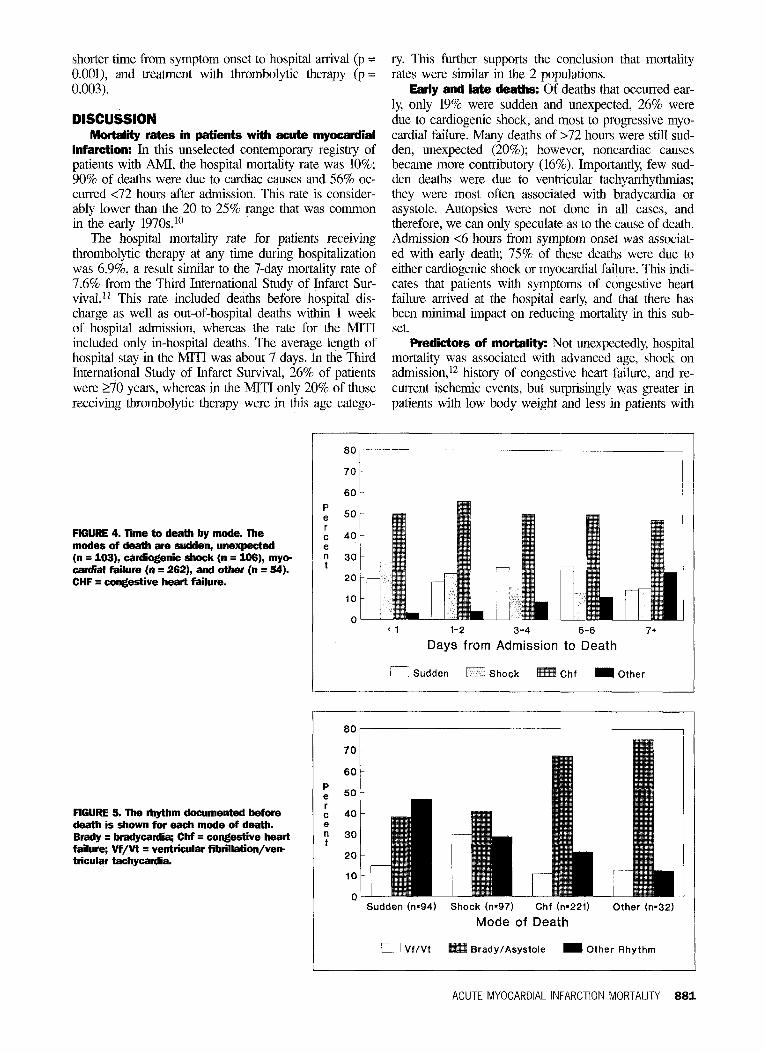
Time and made of death: The mode of death was classified as sudden and unexpected in 20%, cardiogenic shock in 20%, progressive myocardial failure leading to death after several days in 50%, and noncardiac cause in 10%. During day 1, 36% of deaths occurred, and by day 3,63% had occurred (Figure 4). Myocardial or con- gestive heart failure and sudden death had similar daily frequencies of death. The course of death was most rap- id for patients who died of cardiogenic shock and was least rapid for those who died of noncardiac causes.
There was a statistically significant association be- tween the mode of death and the cardiac rhythm imme- diately before death (p <O.OOOl) (Figure 5). The great- est proportion of deaths (50%) was due to bradycardia or asystole; only 14% of deaths were due to ventricular tachycardia or ventricular fibrillation. Sudden and un- expected deaths were far more often due to bradycardia or asystole than ventricular tachycardia or ventricular fi- brillation (38 vs 15%). Logistic regression indicated that sudden, unexpected death after admission for AM1 was associated with the following factors: history of prior myocardial infarction, (p = 0.007), history of congestive heart failure (p = O.OOl), new congestive heart failure during hospitalization (p = 0.006), and cardiac catheter- ization <6 hours from hospital admission (p = 0.02).
Characteristics of patients who died 124 hours from hospital admission (36%) were compared with those who died >24 hours from hospital admission (64%). Death on day 1 was associated only with absence of known history of systemic hypertension (p = O.OOS),
30 t
Pm.26 Pm.47 P-.84 P=.OOOi
Mortality Rcrnt Chest Pain MI Extension
Outcome New CHF
No TT or PTCA 0 TT and/or PTCA
N.4572 N.1626
Age (10 yr)
MI Extension
New CHF
Prior CHF
Shock on Arrival
Weight (10 kg)
Recurrent Chest Pain
Known Hyperlipidemia
Factors associated with better outcome
Factors associated with worse outcome
1
Odds of Death
FlGURE 2. ltiospital mortality by complicb tion for patients treated with angioplasty or thrombolytic therapy (ll), or both, <6 hours from symptom onset versus those not so treated. CHF q congestive heart failure; Ml q myocardial infarction; Rcrnt = recurrent; other abbreviations as in Figure 1.
FlGURE 3. The odds of death with 96% confiince intervals for predicks of hospital mortality in acute myocardial infarction (Ml). The scale for the odds of death is logarithmic. CHF q congestive heart failure.
880 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 72 OCTOBER 15, 1993
shorter time horn symptom onset to hospital arrival (p = O.OOl), and treatment with thrombolytic therapy (p = 0.003).
DlSCU&lON Mortality rates in patients with acute myocardial
infarction: In this unselected contemporary registry of patients with AMI, the hospital mortality rate was 10%; 90% of deaths were due to cardiac causes and 56% oc- curred ~72 hours after admission. This rate is consider- ably lower than the 20 to 25% range that was common in the early 197Os.‘O
The hospital mortality rate for patients receiving thrombolytic therapy at any time during hospitalization was 6.9%, a result similar to the 7-day mortality rate of 7.6% from the Third International Study of Infarct Sur- vival.” This rate included deaths before hospital dis- charge as well as out-of-hospital deaths within 1 week of hospital admission, whereas the rate for the MITI included only in-hospital deaths. The average length of hospital stay in the MITI was about 7 days. In the Third International Study of Infarct Survival, 26% of patients were 270 years, whereas in the MIT1 only 20% of those receiving thrombolytic therapy were in this age catego-
ry. This further supports the conclusion that mortality rates were similar in the 2 populations.
Early and late deaths: Of deaths that occurred ear- ly, only 19% were sudden and unexpected, 26% were due to cardiogenic shock, and most to progressive myo- cardial failure. Many deaths of ~72 hours were still sud- den, unexpected (20%); however, noncardiac causes became more contributory (16%). Importantly, few sud- den deaths were due to ventricular tachyarrhythmias; they were most often associated with bradycardia or asystole. Autopsies were not done in all cases, and therefore, we can only speculate as to the cause of death. Admission ~6 hours from symptom onset was associat- ed with early death, 75% of these deaths were due to either cardiogenic shock or myocardial failure. This indi- cates that patients with symptoms of congestive heart failure arrived at the hospital early, and that there has been minimal impact on reducing mortality in this sub- set.
Predictors of mortality: Not unexpectedly, hospital mortality was associated with advanced age, shock on admission,12 history of congestive heart failure, and re- current ischemic events, but surprisingly was greater in patients with low body weight and less in patients with
FlGURE 4. Time to death by mode. The modes of death are sudden, unexpected (n q 103), cardiogenic shock (n q 105), my* cardial faihre (n = 262), and other (n q 54). CHF = congestive heart failure.
FlGURE 5. The rhythm documented before death is shown for each mode of death. Brady q bradycardia; CM = congestive heart failure; Vf/Vt = ventricular fibrillation/verr tlicular tachycardia.
80
70
80
P e 50 r C 40 e n 30 t
20
IO
0 ( 1 l-2 3-4 5-6
Days from Admission to Death 7+
0 Sudden 0 Shock Chf m Other
60
P e 50 r C 40 e n 30 t
20
Sudden (n.94) Shock (n-97) Chf (n=221) Other b32)
Mode of Death
BradyIAsystole m Other Rhythm
80r
ACUTE MYOCARDIAL INFARCTION MORTALITY 881

known hyperlipidemia. A possible explanation for the latter tinding is that a history of hyperlipidemia is indic- ative of care-seeking behavior and thus may be related to general health status. There was no association be- tween cause of death and body weight; death rates from all causes were greater as body weight decreased.
Thrombolytic drug treatment or direct coronary an- gioplasty were used to treat 26% of all patients. Al- though by univariate analysis, both treatments were highly associated with improved survival, this salutary effect on overall mortality rates from AMI was no long- er evident after adjustment for age. Although the bene- fits of thrombolytic therapy in reducing mortality after AMI are well established, the failure to observe the ef- fect of this treatment on overall community mortality indicates that this treatment is restricted to the 20 to 30% of patients who are eligible, and that this subset is younger with less co-morbidity than patients who are older and less likely to be eligible to receive these thera- pies. l3 Thus, the magnitude of this treatment effect on reducing overall mortality rates is small.
In estimating the effect of treatment, power calcula- tions suggest that the thrombolysis effect in reducing overall mortality will not be detectable until the popula- tion with AMI includes 220,000 patients. Alternatively, to enhance the effect, treatment must be used in more appropriate high-risk patients if community mortality rates are to be further reduced.14J5 These high-risk pa- tients include subjects 275 years as well as those with coexisting conditions that potentially increase the risk of serious bleeding if treated with thrombolytic drugs. The need for research to identity high-risk candidates who could benefit from thrombolytic therapy with an accept- able risk is considerable if we are to treat as many pa- tients as possible.16
at the hospital sooner, and thus were possibly treated earlier than in other large cities.
Third, important variables such as history of cigarette smoking, initial blood pressure, electrocardiographic characteristics (e.g., heart rate, type and location of infarct), and in-hospital medical therapy were only avail- able in subsets of patients. In 1,847 patients who had information about current smoking status, there was no association between smoking and mortality. Finally, the relatively small numbers of patients treated with throm- bolytic therapy or direct angioplasty limited the likeli- hood of detecting a sign&ant reduction in hospital mor- tality.
1. Gillum RF. Acute myocardial infarction in the United States, 197&1983. Am Heart J 1987;113:804-811. 2. Karmel WB, Sorlie P, McNamam PM. Prognosis after initial myocanlial infarc- tion: the Framingham study. Am J Cardiol 1979;&53-59. 3. Greenland P, Reicher-Reiss H, Goldbomt U, Behar S, and the Israeli SPRINT Investigators. In-hospital and l-year mortality in 1,524 women after myocaxlial infarction. Circulation 1991;83:484-49 1. 4. Moss AJ. Benborin J. F’rormosis and manaaement after a first myocardial infarc- tion. N Engl J Med 1990;322:743-753. u 5. Gmppo Italian0 per lo Studio della Streptocbinasi Miocardio (GISSI). Effec- tiveness of intravenous tbmmbolvtic treatment in AMI. Lancei 1986;1:397-402. 6. O’Neill WO. Timmis GC. B&lillo~~ PD. Lai P. Ganghadarhan V, Walton J, Ramos R, La& N, Gordon s, Schork MA, Pitt B. A pmspective randomized clin- ical trial of intracoronary streptokinase vs. coronary angioplasty for AMI. N Engl J Med 1986;314:812-818. 7. The TIMI Study Group. Comparison of invasive and conservative strategies after treatment with intravenous tissue plasminogen activator in AMI: results of the Tbrombolysis in Myocardial Infarction (Tan) Phase Kl trial. N En& J Med 1989; 32R618-527.
Patients who had recurrent ischemia or stroke had much worse outcomes. The adverse effect of reinfarc- tion is consistent with the result of worse hospital out- come in patients who developed reocclusion after suc- cessful reperfusion. l7 This demonstrates the need for and potential value of treatments that will prevent rein- farction after initial treatment for AMI. The overall stroke rate in the MIT1 is higher than those reported in large clinical trials of patients treated with thrombolytic therapy. l8 Patients in the MIT1 Registry were unselect- ed, although the use of heparin and aspirin is standard practice in the community.
6. Tzivoni D, Gavish A, Zin D, Gottlieb S, Moriel M, Keren A, Banai S, Stem S. Prognostic simcance of ischemic episodes in patients with previous myocaniial infarction. Am .I Cardiol 198&62:6616&l. 9. Weaver WD, Eisenberg MS, Martin JS, Lihvin PE, Shaeffer SM, Ho MT, Kudenchuk P, Hallstrom AP, Cerequeira MD, Copass MK, Kennedy JW, Cobb LA, Ritchie JL. Myocardial infarction triage and intervention project-phase I: patient characteristics and feasibility of prehospital initiation of tbrombolytic therapy. J Am Cdl Cardiol 1990; 15:925-931. 10. Feinleib M. Changes in canliovascular epidemiology since 1950. Bull NY Acad Med 1984;60:44%464. 11. ISIS-3 Collaborative Group. ISIS-3 study: a randomized comparison of strep- tokinase vs tissue plasminogen activator YS anistreplase and of aspirin plus heparin vs aspirin alone among 41,299 cases of suspected acute myocardial infarction. Lmcet 1992:339:753-770. 12. Goldberg RI, Gore JM, Alpert JS, Osganian V, D&root J, Bade J, Chen Z, Frid D, Dalen JE. Cardioxenic shock after acute mvocaxlial infarction. N Engl J Med 1991;325:1117-1122.
Study limitations: There are limitations to extrapo- lation or comparison of this study with other communi- ties. First, deaths due to AMI before hospital admission were not included. Consequently, this mortality rate is conservative with respect to the overall effect of AMI on vital status. Second, in Seattle, the presence of a highly efficient emergency medical system might have served to improve survival as patients may have arrived
13. Weaver WD, Lihvin PE, Mm JS, Kudenchuk PJ, Maynard C, Eisenberg MS, Ho MT, Cobb LA, Kennedy JW, Wirkus M. Effect of age on use of tbmm- bolytic therapy and mortality in AMI. I Am Co[l Cardiol 1991;17:14861491. 14. Kmmholz HM, Paster& RC, Weinstein MC, Friesinger GC, Ridker PM, Tosteson ANA. Cost effectiveness of thrombolytic therapy with streptokinase in elderly patients with suspected AMI. N Engl J Med 1992;327:7-13. 15. Top01 EJ, Califf RM. Tbrombolytic therapy for elderly patients. N Engl J Med 1992;327:45-47. 16. Gum&, Co1 NF, Avom J. The exclusion of the elderly and women from clin- ical trials in acute myoca~dial infarction. JAMA 1992;268:1417-1422. 17. Top01 EJ, Calii RM, George BS, Kereiakes DJ, Abbotsmitb CW, Candela RJ, Lee KL, Pitt B, Stack RS, O’Neill WW. A randomized trial of immediate vs. de- layed elective angioplasty after intravenous tissue plasminogen activator in AMI. N Engl J Med 1987;317:581-588. 16. ISIS-2 Collaborative Grow. Random&d trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 wes of suspected AMI: ISIS-2. Lmcet 1988;2:525-530.
882 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 72 OCTOBER 15.1993



























