Embed Size (px)
Citation preview

Hospital Israelita Albert EinsteinHospital Israelita Albert Einstein São PauloSão Paulo
SBHCI 2010SBHCI 2010Belo Horizonte, MG; July 23, 2010Belo Horizonte, MG; July 23, 2010
Update on TAVI Studies:Update on TAVI Studies:Edwards SAPIEN® Edwards SAPIEN®
Transcatheter Heart Valve Transcatheter Heart Valve
Adriano Caixeta, MD, PhDAdriano Caixeta, MD, PhD

NoneNone
Disclosure Statement of Financial InterestWithin the past 12 months, I or my spouse
partner have had a financial Interest /arrangement or affiliation with the
organization (s) listed below

Dr. Alain CribierDr. Alain CribierFirst-in-Man PIONEERFirst-in-Man PIONEER
April 16, 2002April 16, 2002
Percutaneous Transcatheter Implantation of an Aortic Valve Prosthesis for Calcific Aortic Stenosis First Human Case Description Alain Cribier, MD; Helene Eltchaninoff, MD; Assaf Bash, PhD; Nicolas Borenstein, MD; Christophe Tron, MD; Fabrice Bauer, MD; Genevieve Derumeaux, MD; Frederic Anselme, MD; François Laborde, MD; Martin B. Leon, MD
AHA; Nov, 2002AHA; Nov, 2002

Lessons Learned… Lessons Learned… Lessons Learned… Lessons Learned…
TAVI in 2010TAVI in 2010
1.1. ……2.2. ……3.3. ……4.4. ……5.5. ……6.6. ……7.7. ……8.8. ……

1.1. The “high risk” severe AS patients are The “high risk” severe AS patients are “under-treated” and are excellent “under-treated” and are excellent candidates for TAVI procedurescandidates for TAVI procedures
Lessons Learned… Lessons Learned… Lessons Learned… Lessons Learned…
TAVI in 2010TAVI in 2010

At Least 30% of Patients with Severe At Least 30% of Patients with Severe Symptomatic AS are “Untreated”!Symptomatic AS are “Untreated”!
5968 70
4052
69
55
4132 30
6048
3145
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Bouma1999
Iung* 2004
Pellikka2005
Charlson2006
Bach Spokane(prelim)
Vannan(Pub.
Pending)
Severe Symptomatic Aortic StenosisPercent of Cardiology Patients Treated
1. Bouma B J et al. To operate or not on elderly patients with aortic stenosis: the decision and its consequences. Heart 1999;82:143-148
2. Iung B et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. European Heart Journal2003;24:1231-1243 (*includes both Aortic Stenosis and Mitral Regurgitation patients)
3. Pellikka, Sarano et al. Outcome of 622 Adults with Asymptomatic, Hemodynamically Significant Aortic Stenosis During Prolonged Follow-Up. Circulation 2005
4. Charlson E et al. Decision-making and outcomes in severe symptomatic aortic stenosis. J Heart Valve Dis2006;15:312-321
AVR
No AVR
Under-treatment especially
prevalent among patients
managed by Primary Care physicians

2.2. The Edwards technology platform has The Edwards technology platform has achieved excellent prosthetic valve achieved excellent prosthetic valve hemodynamic resultshemodynamic results
Both acute and mid-term valve performance Both acute and mid-term valve performance has surpassed expectations; equivalent to has surpassed expectations; equivalent to surgical valve implantssurgical valve implants
Striking improvements in system Striking improvements in system characteristics (and performance) over a short characteristics (and performance) over a short time! time!
Lessons Learned… Lessons Learned… Lessons Learned… Lessons Learned…
TAVI in 2010TAVI in 2010

The Current GenerationThe Current Generation Edwards – SAPIEN THVEdwards – SAPIEN THV
Current Skirt Height
Untreated EquineTissue
[]
Edwards-SAPIEN THV
New Skirt Height
Bovine TissueThermaFix TreatmentPericardial MappingLeaflet DeflectionProprietary Processing
Cribier-Edwards THV

Edwards Sapien XT THVEdwards Sapien XT THV
Cobalt Frame & New Leaflet Geometry Tissue Attachment
.0109 .0217 .0187 .0210 .0196 .0177 .0156 .0189 .0171 .0182 .0121
.0193 .0136 .0189 .0173 .0118 .0189 .0261 .0247 .0212 .0231 .0235 .0205 .0208 .0177 .0166 .0149 .0153 .0170 .0155
.0111 .0138 .0187 .0204 .0144 .0141 .0250 .0244 .0189 .0187 .0214 .0204 .0208 .0187 .0135 .0140 .0150 .0150 .0134
.0113 .0115 .0162 .0218 .0184 .0139 .0256 .0292 .0194 .0164 .0186 .0211 .0217 .0169 .0144 .0115 .0118 .0135 .0117
.0130 .0111 .0133 .0198 .0225 .0167 .0259 .0343 .0268 .0179 .0195 .0181 .0253 .0163 .0144 .0118 .0112 .0115 .0050
.0136 .0104 .0124 .0154 .0243 .0178 .0237 .0372 .0337 .0231 .0180 .0138 .0200 .0145 .0127 .0132 .0116 .0109 .0104
.0119 .0208 .0369 .0330 .0272 .0210 .0108 .0302 .0134 .0115 .0133 .0119 .0135 .0110
.0122 .0100 .0110 .0128 .0113 .0136 .0110
.0113 .0110 .0084 .0117
Leaflet Matching & ThermaFix
Finite ElementAnalysis
Partially Closed Design Sapien XTSapien XT

Sapien XT + NovaFlex Delivery SystemSapien XT + NovaFlex Delivery System
18 Fr profile18 Fr profile


TransfemoralTransfemoral TransapicalTransapical
Transcatheter AVITranscatheter AVITransapical Access RouteTransapical Access Route

PrePre PostPost
Mean Gradient (mm Hg)Mean Gradient (mm Hg) AVA (cm²)AVA (cm²)
p = .0076p = .0076 p = .0076p = .0076
00
1010
2020
3030
4040
5050
6060
7070
8080
00
0,20,2
0,40,4
0,60,6
0,80,8
11
1,21,2
1,41,4
1,61,6
1,81,8
22
PrePre PostPost
8.58.5
4343
0.560.56
1.691.69
Cribier – Early PHV ExperiencesCribier – Early PHV ExperiencesProcedural Results (n=16)Procedural Results (n=16)

3.3. The Edwards technology platform has also The Edwards technology platform has also achieved acceptable early and mid-term achieved acceptable early and mid-term clinical outcomesclinical outcomes
Clinical outcomes are improving, perhaps due Clinical outcomes are improving, perhaps due to better patient selection, device and to better patient selection, device and procedure enhancements, and “learning curve” procedure enhancements, and “learning curve” issues issues
Lessons Learned… Lessons Learned… Lessons Learned… Lessons Learned…
TAVI in 2010TAVI in 2010

Edwards TAVIEdwards TAVIClinical Data SourcesClinical Data Sources
CANADA multi-center (6) (TF=167 pts, TA=172 pts)CANADA multi-center (6) (TF=167 pts, TA=172 pts)
PARIS single center (TF=51 pts, TA=24 pts)PARIS single center
(TF=51 pts, TA=24 pts)
VANCOUVER single center (TF=164 pts, TA=86 pts)
VANCOUVER single center (TF=164 pts, TA=86 pts)
Other StudiesOther Studies
TOTAL = 664 PTSTOTAL = 664 PTSPARTNER FDA
(US/OUS, TF/TA ~1400 pts)PARTNER FDA
(US/OUS, TF/TA ~1400 pts) PIVOTAL RCTPIVOTAL RCT
POSTPOSTCE-APPROVALCE-APPROVAL
PARTNER EU (OUS, TF/TA 130 pts)SOURCE (OUS, TF/TA, 1123 pts)PARTNER EU (OUS, TF/TA 130 pts)SOURCE (OUS, TF/TA, 1123 pts)
FEASIBILITYFEASIBILITY(CE-APPROVAL)(CE-APPROVAL)
REVIVE (OUS, TF, 106 pts) TRAVERCE (OUS, TA, 172 pts) REVIVAL (US, TF/TA, 95 pts)
REVIVE (OUS, TF, 106 pts) TRAVERCE (OUS, TA, 172 pts) REVIVAL (US, TF/TA, 95 pts)
Transseptal Experience (RECAST, I-REVIVE; 36 pts)
Transseptal Experience (RECAST, I-REVIVE; 36 pts) FIRST-in-MANFIRST-in-MAN
EdwardsEdwards
TOTAL = 3062 PTSTOTAL = 3062 PTS
OVERALL TOTAL OVERALL TOTAL 3726 PTS 3726 PTS
0
0.2
0.4
0.6
0.8
1
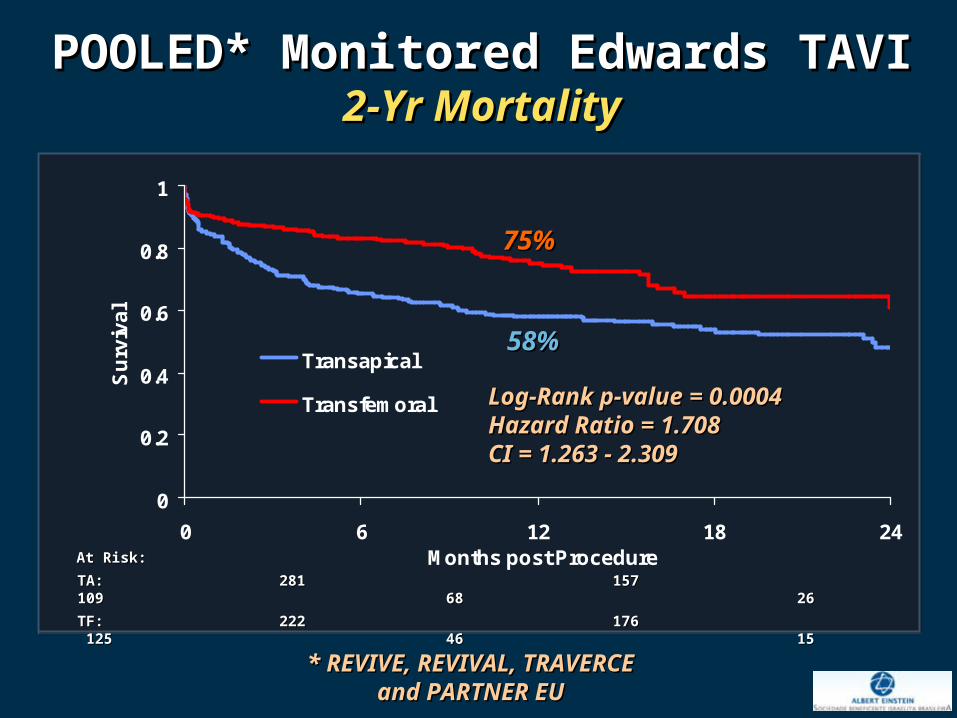
0 6 12 18 24Months post Procedure
Su
rviv
al
Transapical
Transfemoral
At Risk: At Risk:
TA: 281 157 109 68 26TA: 281 157 109 68 26
TF: 222 176 125 46 15TF: 222 176 125 46 15
Log-Rank p-value = 0.0004Log-Rank p-value = 0.0004Hazard Ratio = 1.708Hazard Ratio = 1.708CI = 1.263 - 2.309CI = 1.263 - 2.309
POOLED* Monitored Edwards TAVIPOOLED* Monitored Edwards TAVI2-Yr Mortality2-Yr Mortality
* REVIVE, REVIVAL, TRAVERCE* REVIVE, REVIVAL, TRAVERCEand PARTNER EUand PARTNER EU
75%75%
58%58%

0%10%20%30%
40%50%60%70%
Coronaryartery
disease
MitralDisease
Peripheralvasculardisease
Prior CABG Carotiddisease
PriorPacemaker
TF TAP = <0.0001P = <0.0001 P=0.008P=0.008P=0.008P=0.008
P=0.04P=0.04
P=0.02P=0.02P = nsP = ns
TF (n=61)TF (n=61) TA (n=69)TA (n=69)
Logistic EuroSCORELogistic EuroSCORE 25.7 ± 11.5 (Range: 6-65)25.7 ± 11.5 (Range: 6-65) 33.8 ± 14.7 (Range: 5-72)33.8 ± 14.7 (Range: 5-72)
STS ScoreSTS Score 11.3 ± 6.1 (Range: 4-32)11.3 ± 6.1 (Range: 4-32) 11.8 ± 6.8 (Range: 2-41)11.8 ± 6.8 (Range: 2-41)
V. Schächinger; euroPCR 2009
PARTNER EU TrialPARTNER EU TrialRisk ProfilesRisk Profiles

POOLED* Monitored Edwards TAVIPOOLED* Monitored Edwards TAVI30-Day Mortality (vs. SOURCE)30-Day Mortality (vs. SOURCE)
0.8
0.85
0.9
0.95
1
0 5 10 15 20 25 30
Days post Procedure
Su
rviv
al
SOURCE:SOURCE:Log-Rank p-value = 0.0226Log-Rank p-value = 0.0226Hazard Ratio = 1.666Hazard Ratio = 1.666CI = 1.068 - 2.598CI = 1.068 - 2.598
POOLED:POOLED:Log-Rank p-value = 0.0589Log-Rank p-value = 0.0589Hazard Ratio = 1.608Hazard Ratio = 1.608CI = 0.974 - 2.652CI = 0.974 - 2.652 POOLED TA (n=281)POOLED TA (n=281)
SOURCE TF (n=463)SOURCE TF (n=463)
SOURCE TA (n=575)SOURCE TA (n=575)
POOLED TF (n=222)POOLED TF (n=222)
* REVIVE, REVIVAL, TRAVERCE* REVIVE, REVIVAL, TRAVERCEand PARTNER EUand PARTNER EU
6.3%6.3%
10.3%10.3%
10.4%10.4%
16.4%16.4%

15%
19%18%
27
3436
5%
10%
15%
20%
TRAVERCE PARTNER EU REVIVAL CANADA SOURCE BERLIN
25
30
35
40
45
Clinical Trials
30d
Mor
talit
y (%
)30
d M
orta
lity
(%)
12%
TAVI in EvolutionTAVI in EvolutionTrans-apicalTrans-apical
Improved short-term outcomes!
Courtesy of Dr. Martin LeonCourtesy of Dr. Martin Leon

15%
19%18%
11%10%
6%27
3436
3029
41
5%
10%
15%
20%
TRAVERCE PARTNER EU REVIVAL CANADA SOURCE BERLIN
25
30
35
40
45
12%
Clinical Trials
30d
Mor
talit
y (%
)30
d M
orta
lity
(%)
TAVI in 2010TAVI in 2010Trans-apicalTrans-apical
Improved short-term outcomes!
Courtesy of Dr. Martin LeonCourtesy of Dr. Martin Leon

62%
49%
60%
40%
50%
60%
70%
80%
TRAVERCE PARTNER EU REVIVAL CANADA BERLIN
65%
TAVI in 2010TAVI in 2010Trans-apicalTrans-apical
Clinical Trials
1-ye
ar s
urvi
val (
%)
1-ye
ar s
urvi
val (
%)
Improved one-year outcomes!
Courtesy of Dr. Martin LeonCourtesy of Dr. Martin Leon

62%
49%
60%
78%83%
40%
50%
60%
70%
80%
TRAVERCE PARTNER EU REVIVAL CANADA BERLIN
65%
TAVI in 2010TAVI in 2010Trans-apicalTrans-apical
1-ye
ar s
urvi
val (
%)
1-ye
ar s
urvi
val (
%)
Clinical Trials
Improved one-year outcomes!
Courtesy of Dr. Martin LeonCourtesy of Dr. Martin Leon

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Baseline 30 Days 3 Months 6 Months 1 Year 18 Months
2 Years
NY
HA
IV
III
II
I
NYHA Class
N=492 N=231 N=271 N=235 N=243 N=64 N=48
Visit
POOLED* Monitored Edwards TAVIPOOLED* Monitored Edwards TAVINYHA ClassNYHA Class
* REVIVE, REVIVAL, TRAVERCE* REVIVE, REVIVAL, TRAVERCEand PARTNER EUand PARTNER EU

55%
Vancouver TAVI Vancouver TAVI LearningLearning Experience Experience
Courtesy of John WebbCourtesy of John Webb
Mortality @ 30 days – Trans-arterialMortality @ 30 days – Trans-arterial

56%
Courtesy of John WebbCourtesy of John Webb
Vancouver TAVI Vancouver TAVI LearningLearning Experience Experience
Mortality @ 30 days – Trans-apicalMortality @ 30 days – Trans-apical

4.4. Many TAVI complications have emerged Many TAVI complications have emerged and require further analysis and and require further analysis and clarificationclarification
Paravalvular ARParavalvular AR Conduction disturbancesConduction disturbances Vascular complicationsVascular complications StrokeStroke Coronary obstruction Coronary obstruction
Lessons Learned… Lessons Learned… Lessons Learned… Lessons Learned…
TAVI in 2010TAVI in 2010

Edwards TAVI Complications Edwards TAVI Complications Multiple Data Sources (TA and TF)Multiple Data Sources (TA and TF)
POOLED*POOLED*(503 pts)(503 pts)
SOURCESOURCE(1038 pts)(1038 pts)
VANCOUVERVANCOUVER(250 pts)(250 pts)
PARISPARIS(75 pts)(75 pts)
CA-MultictrCA-Multictr(339 pts)(339 pts)
Vascular (maj)** (%)Vascular (maj)** (%) 18.518.5 10.610.6 10.310.3 11.811.8 13.113.1
AR >2+ (%)AR >2+ (%) 10.910.9 4.74.7 5.05.0 5.35.3 7.77.7
Stroke (%)Stroke (%) 4.04.0 2.52.5 3.03.0 4.04.0 2.32.3
New Pacemaker (%)New Pacemaker (%) 4.44.4 7.07.0 5.55.5 5.35.3 4.94.9
Renal Failure (%)Renal Failure (%) 5.25.2 8.78.7 4.24.2 nana 2.62.6
Coronary Obstr (%)Coronary Obstr (%) 0.40.4 0.60.6 nana 00 00
** REVIVE, REVIVAL, TRAVERCE, PARTNER EUREVIVE, REVIVAL, TRAVERCE, PARTNER EU** TF Only** TF Only

Para-valvular Regurgitation Para-valvular Regurgitation

5.5. Long-term durability evaluations of TAVI Long-term durability evaluations of TAVI bioprosthetic valves are still ongoingbioprosthetic valves are still ongoing
Meticulous follow-up necessary including Meticulous follow-up necessary including echocardiograms (core lab assessments)echocardiograms (core lab assessments)
Ultimate value of TAVI will require proof of Ultimate value of TAVI will require proof of “near surgical” valve durability “near surgical” valve durability
Lessons Learned… Lessons Learned… Lessons Learned… Lessons Learned…
TAVI in 2010TAVI in 2010

6.6. TAVI requires a major milieu adjustment to TAVI requires a major milieu adjustment to develop an optimal programdevelop an optimal program
Hybrid cath lab - ORsHybrid cath lab - ORs Intense clinical care continuum – screening, Intense clinical care continuum – screening,
procedure, pot-procedure care, follow-upprocedure, pot-procedure care, follow-up Surgeons and interventionalists working Surgeons and interventionalists working
closely together (Heart Valve Team)!!!closely together (Heart Valve Team)!!! Strict training requirements Strict training requirements
Lessons Learned… Lessons Learned… Lessons Learned… Lessons Learned…
TAVI in 2010TAVI in 2010

Transcatheter AVRTranscatheter AVRHybrid OR-Cath LabHybrid OR-Cath Lab
Courtesy of Dr. Martin LeonCourtesy of Dr. Martin Leon

7.7. The PARTNER trial should provide The PARTNER trial should provide valuable insights and will provide the valuable insights and will provide the evidence-based medicine justification for evidence-based medicine justification for future expansion of TAVI!future expansion of TAVI!
Lessons Learned… Lessons Learned… Lessons Learned… Lessons Learned…
TAVI in 2010TAVI in 2010

Medical Medical Management Management
ControlControl
PRIMARY ENDPOINTPRIMARY ENDPOINTAll-cause mortality (1 yr)All-cause mortality (1 yr)
Non-inferiorityNon-inferiority
2 Trials2 TrialsIndividually PoweredIndividually Powered
(Cohorts A & B)(Cohorts A & B)
PARTNER Trial DesignPARTNER Trial DesignFully enrolled: continued access to both patient cohorts approved by FDA
Symptomatic Severe Aortic StenosisSymptomatic Severe Aortic Stenosis
AssessmentAssessment High Risk High Risk
AVR CandidateAVR CandidateYesYes NoNo
Cohort ACohort A Cohort BCohort B
AssessmentAssessmentTransfemoral AccessTransfemoral Access
AssessmentAssessmentTransfemoral AccessTransfemoral Access
Not in StudyNot in Study
vsvsTransTrans
FemoralFemoral
Cohort A TFCohort A TF
AVRAVRControlControl vsvs
TransTransApicalApical
AVRAVRControlControl vsvs
TransTransFemoralFemoral
1:1 Randomization1:1 Randomization
PRIMARY ENDPOINTPRIMARY ENDPOINTAll-cause mortality (1 yr)All-cause mortality (1 yr)
SuperioritySuperiority
YesYesYesYes NoNo
Cohort A TACohort A TA
1:1 Randomization1:1 Randomization
NoNo
N=491N=491 N=203N=203
N=694N=694 N=358N=358
Total = 1,052 ptsTotal = 1,052 pts

PARTNER PARTNER Baseline Characteristics*Baseline Characteristics*
Variable %Variable %Cohort A-TFCohort A-TF(test control)(test control)
Cohort A-TACohort A-TA(test control)(test control)
Cohort B-TFCohort B-TF(test control)(test control)
Number of patientsNumber of patients 450450 182182 430430
Age (years)Age (years) 83.6 83.6 ++ 10.4 10.4 82.4 82.4 ++ 10.8 10.8 83.1 83.1 ++ 8.5 8.5
Gender (male)Gender (male) 58.158.1 57.457.4 48.748.7
DiabetesDiabetes 40.240.2 41.741.7 35.435.4
HyperlipidemiaHyperlipidemia 79.579.5 79.379.3 74.074.0
HypertensionHypertension 90.090.0 95.495.4 85.385.3
SmokingSmoking 42.642.6 56.656.6 46.946.9
Prior MIPrior MI 25.325.3 31.431.4 25.225.2
*subset of all randomized patients *subset of all randomized patients in cohort A (TF+TA) and cohort B (incl. CA)in cohort A (TF+TA) and cohort B (incl. CA)
•Preliminary snapshotPreliminary snapshot•Outcomes data blindedOutcomes data blinded

PARTNER PARTNER High Risk Co-Morbidities (1)*High Risk Co-Morbidities (1)*
Variable %Variable %Cohort A-TFCohort A-TF(test control)(test control)
Cohort A-TACohort A-TA(test control)(test control)
Cohort B-TFCohort B-TF(test control)(test control)
Number of patientsNumber of patients 450450 182182 430430
Periph Vasc DiseasePeriph Vasc Disease 32.732.7 56.256.2 26.826.8
Hx CHFHx CHF 97.697.6 96.696.6 97.097.0
NYHA Class III/IVNYHA Class III/IV 94.094.0 91.691.6 93.293.2
Prior CABGPrior CABG 59.559.5 69.869.8 59.559.5
Prior PCIPrior PCI 45.745.7 48.448.4 37.237.2
Prior BAVPrior BAV 15.915.9 15.915.9 25.625.6
Severe COPD (O2 dep)Severe COPD (O2 dep) 7.17.1 9.79.7 23.823.8
*subset of all randomized patients *subset of all randomized patients in cohort A (TF+TA) and cohort B (incl. CA)in cohort A (TF+TA) and cohort B (incl. CA)

PARTNER PARTNER High Risk Co-Morbidities (2)*High Risk Co-Morbidities (2)*
Variable %Variable %Cohort A-TFCohort A-TF(test control)(test control)
Cohort A-TACohort A-TA(test control)(test control)
Cohort B-TFCohort B-TF(test control)(test control)
Number of patientsNumber of patients 450450 182182 430430
CNS DiseaseCNS Disease 23.023.0 32.032.0 26.926.9
Recent Stroke/TIARecent Stroke/TIA 2.52.5 3.63.6 2.42.4
CirrhosisCirrhosis 2.02.0 00 2.22.2
Porcelain aortaPorcelain aorta 0.40.4 1.01.0 15.115.1
Chest radiationChest radiation 0.60.6 1.01.0 7.87.8
Chest wall deformityChest wall deformity 00 00 6.96.9
FrailtyFrailty 18.918.9 17.617.6 27.927.9
*subset of all randomized patients *subset of all randomized patients in cohort A (TF+TA) and cohort B (incl. CA)in cohort A (TF+TA) and cohort B (incl. CA)

Medical Medical Management Management
ControlControl
PRIMARY ENDPOINTPRIMARY ENDPOINTAll-cause mortality (1 yr)All-cause mortality (1 yr)
Non-inferiorityNon-inferiority
2 Trials2 TrialsIndividually PoweredIndividually Powered
(Cohorts A & B)(Cohorts A & B)
PARTNER Trial DesignPARTNER Trial DesignFully enrolled: continued access to both patient cohorts approved by FDA
Symptomatic Severe Aortic StenosisSymptomatic Severe Aortic Stenosis
AssessmentAssessment High Risk High Risk
AVR CandidateAVR CandidateYesYes NoNo
Cohort ACohort A Cohort BCohort B
AssessmentAssessmentTransfemoral AccessTransfemoral Access
AssessmentAssessmentTransfemoral AccessTransfemoral Access
Not in StudyNot in Study
vsvsTransTrans
FemoralFemoral
Cohort A TFCohort A TF
AVRAVRControlControl vsvs
TransTransApicalApical
AVRAVRControlControl vsvs
TransTransFemoralFemoral
1:1 Randomization1:1 Randomization
PRIMARY ENDPOINTPRIMARY ENDPOINTAll-cause mortality (1 yr)All-cause mortality (1 yr)
SuperioritySuperiority
YesYesYesYes NoNo
Cohort A TACohort A TA
1:1 Randomization1:1 Randomization
NoNo
N=491N=491 N=203N=203
N=694N=694 N=358N=358
Total = 1,052 ptsTotal = 1,052 pts
First Presentation of First Presentation of PARTNER Data PARTNER Data
at TCT 2010!at TCT 2010!

8.8. The future is exciting – TAVI procedure The future is exciting – TAVI procedure device enhancements and expanded device enhancements and expanded clinical indications!clinical indications! New valve designs, lower profile systems, New valve designs, lower profile systems,
Lessons Learned… Lessons Learned… Lessons Learned… Lessons Learned…
TAVI in 2010TAVI in 2010

New TAVI TechnologiesNew TAVI Technologies Direct FlowDirect Flow
SadraSadra
AorTx AorTx
Jena ValveJena Valve
HLTHLT
ABPS PercValveABPS PercValve
EndoTechEndoTech
Ventor EmbracerVentor Embracer
SymetisSymetis

Next Clinical TargetsNext Clinical TargetsNext Clinical TargetsNext Clinical Targets
• Valve-in-valve for bio-prosthetic aortic Valve-in-valve for bio-prosthetic aortic and mitral valve failureand mitral valve failure
• Lower risk AS patientsLower risk AS patients• Mixed AS and CAD patientsMixed AS and CAD patients• Asymptomatic severe ASAsymptomatic severe AS• Low flow - low gradient AS – impedance Low flow - low gradient AS – impedance
mismatchmismatch• Aortic regurgitationAortic regurgitation
TAVI in 2010TAVI in 2010

Transcatheter AVITranscatheter AVIEndless Possibilities!Endless Possibilities!
Trans-apicalTrans-apicalAVRAVR
Courtesy of Dr. John WebbCourtesy of Dr. John Webb
Trans-apicalTrans-apicalMVRMVR
(valve-in-valve)(valve-in-valve)
Edwards-SapienEdwards-Sapien

In the next 5-10 years, many (? most) patients with severe AS requiring AVR
will be treated using transcatheter lesser-invasive modalities!
Martin Leon





























