PowerPoint Presentation
Hospital EMRs: Getting it Right the First Time
Thomas G. Zimmerman, DO, FACOFP, CPHIMS
South Nassau Communities Hospital
Oceanside, NY
1
Hospital Demographics
440-bed community hospital in suburb of NYC
1023 Medical Staff
850 Physicians (of which 75 are hospital-employed)
3000 Employees
720 RNs
Dually-Accredited Family Medicine Residency (18)
Visiting Residents (OB, Surgery, Peds total 18)
Thomas Zimmerman, DO, FACOFP, CPHIMS
2
Do your homework!!
Thoroughly evaluate the projects feasibility
Preliminary architecture and design specifications
Informed consent of all stakeholders
Consider the financial impact of the project (as well as
work-hours involved)
Complete EHR, or phased approach
Phase 1 Orders and Results
Phase 2 Clinical Documentation
Thomas Zimmerman, DO, FACOFP, CPHIMS
3
Planning
Clarify Project Objectives and Scope
Proposed Timeline
Cost and Quality objectives
Scope of Project
Deliverables
Verify that all stakeholders agree to these guidelines to avoid
confusion, wasted effort or duplication, and/or project
failure.
Thomas Zimmerman, DO, FACOFP, CPHIMS
4
Planning
Identify a single leader of the project
A large steering committee by itself does not allow for personal
responsibility and action.
CMIO / CIO / VP EMR/HIM should take the lead in monitoring
progress and addressing obstacles
Steering committee can serve as a resource to the project leader
to discuss issues and find solutions
Thomas Zimmerman, DO, FACOFP, CPHIMS
5
Planning
Full-Time Project Manager
Day to day management, execution, and delivery of the
implementation
Reports to Project Sponsor / Steering Committee
Should have experience with IT implementations
Thomas Zimmerman, DO, FACOFP, CPHIMS
6
Planning
Interdisciplinary Implementation Teams
Executive Sponsors
Department or section leaders
Experienced Subject Matter Experts (SMEs)
Physicians, IT techs, EMR consultants
End-users with AND without IT experience
Department of Medical Education
Residents, students (of all types)
Thomas Zimmerman, DO, FACOFP, CPHIMS
7
Planning
Strong Administrative Sponsorship and Involvement
Ensures that each implementation team (not just the Steering
Committee) has the authority to make decisions that will stick
Expresses the strong commitment of the hospital for this
implementation (to the end-users)
Ensures better communication and awareness
Thomas Zimmerman, DO, FACOFP, CPHIMS
8
Thomas Zimmerman, DO, FACOFP, CPHIMS
9
Planning
Core Analyst Team
Hire flexible thinkers who have a sense of perspective and a
sense of humor you will need both.
Consultants Caveat Emptor!!
Enlist their services judiciously, respect and acknowledge their
expertise, but make sure that hospital staff retain ownership of
the project
Interfaces
Lab / Rad / Dietary / Admitting
Make sure the time and costs for the
development/testing/verification for all of these are appropriately
accounted for in negotiations, contract, and scope
Thomas Zimmerman, DO, FACOFP, CPHIMS
10
Identify Risks
Technical interface issues, equipment compatibility issues,
delays in upgrades
End User Acceptance resistance to change (computerized physician
order entry, medication reconciliation, etc.)
Recognize, monitor, and address these risks in a timely manner,
and ensure communication between stakeholders (no surprises!)
Thomas Zimmerman, DO, FACOFP, CPHIMS
11
Question the Vendor
Dont accept its hard coded or its working as intended
Clinicians need to drive the train for patient safety
Thomas Zimmerman, DO, FACOFP, CPHIMS
12
Staffing Concerns
Clarify time commitments for staff members involved with the
implementation
Identify times where their hours will need to be back-filled
with other staff to meet daily operational needs
If activities will occur after work hours, consider what type of
compensation will be provided
Thomas Zimmerman, DO, FACOFP, CPHIMS
13
Review Policies
Practice and policies will need to reflect the new world
order
Dont feel that you need to own the practice of the entire
hospital
Users will ask you to make the doctors and nurses do. Avoid the
temptation!
Thomas Zimmerman, DO, FACOFP, CPHIMS
14
Remember
Everyone still needs to talk
Avoid the illusion of communication that follows implementation
of an EMR
Thomas Zimmerman, DO, FACOFP, CPHIMS
15
Scope
Define the scope of the project, and really think it through
In-patient only?
Out-patient areas?
Ambulatory areas vs. Procedural areas?
Consider areas that serve a combination of in-patients and
out-patients
Thomas Zimmerman, DO, FACOFP, CPHIMS
16
Scope (cont)
Will you use niche products in areas such as:
Cath Lab
Labor & Delivery Suite
OR
General EMRs are a mile wide, and an inch deep while niche
products are an inch wide and a mile deep
Thomas Zimmerman, DO, FACOFP, CPHIMS
17
Create a detailed project plan
Gantt Chart or Excel spreadsheet
Document all major outcomes/deliverables
Target dates
Responsible Sponsor / Resources
Approximate work effort
Update these tasks as they are completed or delayed/modified
Thomas Zimmerman, DO, FACOFP, CPHIMS
18
Scope Creep
The expansion of the project to include additional
products/functionalities not originally accounted for in the
project plan and/or contract
Extra Time / work effort
Extra Costs
Increased complexity, confusion
Thomas Zimmerman, DO, FACOFP, CPHIMS
19
Change Control
Changes to the original software are inevitable; the product
must be tailored to suit the individual needs of your
organization
Be prudent in making modifications to the core software
Document all changes in detail:
Date of change
Reason modification was needed
Exact description of the change (in case it needs to be restored
after an upgrade)
Thomas Zimmerman, DO, FACOFP, CPHIMS
20
Current State & Future State Design
All stakeholders involved better design, more user
acceptance/skills
Identify every workflow in every department of the hospital:
clinical, administrative, financial.
Critically evaluate current policies and procedures, and watch
for opportunities for improvement that the EMR may provide
Identify key issues / problems created by the EMR
Document the future state of operations clearly
Thomas Zimmerman, DO, FACOFP, CPHIMS
21
Sample Workflow Diagram
Thomas Zimmerman, DO, FACOFP, CPHIMS
22
Key Theme DescriptionClinical Excellence Quality and Outcomes
FocusWhat will the approach be for identifying outcomes as part of
the EMR implementation? Which outcomes are of the highest priority?
Care StandardizationDetermines the extent to which care and
clinical applications will be standardized. CPOE Strategy This
defines the degree to which CPOE will be rolled out as standard
practice or policy. Medical executive committee establishes
expectations regarding compliance and consequences for physician
non-compliance. Clinical Documentation Describes the approach to
clinical documentation: what types data will be entered, who will
enter it, and how.Clinical Decision SupportDescribes the approach
to the tools that guide real-time clinical decision-making.
Future State Design Guiding Principles
Thomas Zimmerman, DO, FACOFP, CPHIMS
23
24
Key Theme DescriptionTrainingIdentifies the approach and level
of investment for how the hospital addresses staff training for
clinical quality improvements to include use of advanced clinical
systems.Access Strategy Remote and InternalThis defines the
strategy for the placement of devices to enhance adoption and also
determines the extent the physician portal and remote access will
be utilized. Content StrategyThis will define the content strategy
(order sets, clinical documentation, and clinical decision support)
to ensure system utilization and improve quality and
efficiency.Workflow OptimizationRedesigning current workflows with
EHR as an enabler will allow hospital to maximize the integration
of system utilization and clinical workflows.Communication
StrategyAn institutional communication strategy that outlines the
audience, methods, tools and frequency of communication must be
developed to improve institutional ownership.
Future State Design Guiding Principles
Thomas Zimmerman, DO, FACOFP, CPHIMS
Timeline
Nov. 2009 Presentations by 2 Vendors
Jan-March. 2010 Site visits to nearby Hospital using each
system
July 2010 Contract signed with Vendor
January May 2011 Current / Future State Design Sessions
August 2011 Present Physicians Advisory Group Meetings
June 2012: Go-Live!
Thomas Zimmerman, DO, FACOFP, CPHIMS
25
Site Visits
Two hospitals with similar demographics
Community hospital with residency programs
Bed size, service lines, patient population
Evaluation Team
HIM (VP HIM, EMR Manager, Coding Director)
IT (CIO, Network specialist)
Financial (VP Finance and staff)
Medical Staff (President of Med. Staff, Physician champion)
Thomas Zimmerman, DO, FACOFP, CPHIMS
26
Site Visit Itinerary
Presentation by Hospitals CMIO
Divide and Conquer:
Medical Team: Floors, ICU, ED, Ambulatory Clinic
IT Team: IT dept., floors
Finance: Administration, Billing/Coding
Coding: HIM department, Billing/coding
Thomas Zimmerman, DO, FACOFP, CPHIMS
27
Core Build
Extensive work effort to establish the pharmacy formulary
Order sets Diagnosis Based
Core measures (VTE assessment, time to treatment, etc.)
Meaningful use measures
Convenience
Congruent to Paper forms (for downtime episodes)
Communication / Workflows for ancillary processes
Respiratory therapy, Floor-obtained samples, Codes
Discharge Process
Thomas Zimmerman, DO, FACOFP, CPHIMS
28
28
Pharmacy Build
Have a pharmacy build that reflects:
Front-end needs, i.e.
Physician needs for ease of item selection and understanding of
order guidance. Will you build brand name synonyms?
Nursing needs for clarity on the orders tab and eMAR
Back-end needs
Pharmacy needs consistency of build and a full view of the
medications ordered and access to the patients clinical picture
TEST each item from order entry, to dispensing and delivering,
to display on the orders tab and eMAR, to medication
administration
Thomas Zimmerman, DO, FACOFP, CPHIMS
29
Downtime Plans
Have firm downtime plans and tools well before Go-Live
Devise a method of running reports in the background that can be
printed on demand in advance for a planned downtime, and just in
time for an unplanned downtime
Patient list by location
Orders report with all active, on hold, suspended orders
MAR with a list of all medications administered within the prior
48 hours, with a list of all tasks for the next 24 hours
Thomas Zimmerman, DO, FACOFP, CPHIMS
30
Downtime Plans
Create a Meaningful Use Checklist
Ensure all MU measures during downtime are correctly entered
during recovery period (backfill)
Strongly consider building a redundant database on a local
server to be viewable during downtimes/no internet access
Thomas Zimmerman, DO, FACOFP, CPHIMS
31
Training
No amount of training is too much!!
Combination of delivery methods to account for differences in
end-user preferences and schedules
Live, classroom-based sessions (at hospital or office)
Web-Based Training Modules (auto-tutorial)
Remote webinar sessions
One-on-one
Thomas Zimmerman, DO, FACOFP, CPHIMS
32
Superusers
Essential to have key team members receive extra training and
practice with the system
Creates a cadre of first-line support at the unit level during
Go-Live and thereafter
Improves end-user acceptance, they serve as ambassadors of the
EMR team
Helps identify issues in the system earlier in the process
(these people know what works and what wont work!)
Thomas Zimmerman, DO, FACOFP, CPHIMS
33
Preparing for Go-Live
Big-Bang vs. Phased Approach
Entire House or Unit by Unit
Central Command Center
Embed IT and EMR support personnel throughout the building
Superusers, hospital IT/EMR staff, vendor support
Deploy more staff in busier or more critical units
Two weeks minimum, 24/7
Thomas Zimmerman, DO, FACOFP, CPHIMS
34
Activation
Telephone Support Center
Have the Informatics team (Level 2 Help Desk) and the IT team
(Level 1 Help Desk) share a Telephone Support Center where they
handle calls from the users during Go-Live. It will pay off later
with increased knowledge and compassion on both sides later
Keep detailed logs of all issues (as well as their
solutions)
Thomas Zimmerman, DO, FACOFP, CPHIMS
35
Allow for Decreased Productivity
Overstaff units (especially ED, ICU, OR, other critical areas of
the hospital
Consider Go-Live on a weekend, to avoid elective surgeries and
imaging procedures (although ED may be busier)
If a weekday, reschedule as many elective procedures as
possible
Thomas Zimmerman, DO, FACOFP, CPHIMS
36
Questions?
Thomas Zimmerman, DO, FACOFP, CPHIMS
37
Inpatient Documentation of Home Meds List
E
i
t
h
e
r
C
l
i
n
i
c
i
a
n
P
r
o
v
i
d
e
r
N
u
r
s
e
Provider sees
patient
before RN
assessment
Have home meds
been documented
in Rx Writer?
Validate list
with patient
Perform Copy
from Rx Writer
function
Add last dose date
& time info for
home meds
Nurse interviews
patient before
provider
assessment
Add home
meds to
patient profile
in Rx Writer
End
Continue with
Admission
Reconciliation
process
No
Yes
MD option
The height of the text box and its associated line increases or
decreases as you add text. To change the width of the comment, drag
the side handle.
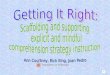
Inpatient Documentation of Home Meds List
Nurse
Provider
Either Clinician
Provider sees patient before RN assessment
Have home meds been documented in Rx Writer?
Validate list with patient
Perform Copy from Rx Writer function
Add last dose date & time info for home meds
Nurse interviews patient before provider assessment
Add home meds to patient profile in Rx Writer
End
Continue with Admission Reconciliation process
No
Yes
MD option