Embed Size (px)
Citation preview

Hortensia Amaro
Director
Institute on Urban Health Research
Northeastern University9th Annual Summer Public Health Videoconference on Minority Research
Innovations in HIV Prevention with Latina and African American Women at High Risk

OverviewOverview
EpidemiologyLimitations of traditional behavioral
models for HIV preventionGender and cultural factors in HIV
riskMarginalization and HIV RiskIntervention for Women at High RiskConclusion

Epidemiology: HIV/AIDS Among Epidemiology: HIV/AIDS Among Women WorldwideWomen Worldwide

Adults and Children Estimated to Be Adults and Children Estimated to Be Living With HIV/AIDS As of End 2001Living With HIV/AIDS As of End 2001
Western Europe
560 000560 000North Africa & Middle East
440 000440 000Sub-Saharan
Africa
28.1 28.1 millionmillion
Eastern Europe & Central Asia
1 million1 million
South & South-East Asia
6.1 million6.1 million
Australia & New Zealand
15 00015 000
North America
940 000940 000Caribbean
420 000420 000
Latin America
1.4 1.4 millionmillion
Total: 40 million
East Asia & Pacific
1 million1 million
UNAIDS Report, December 2001

14,000 New Infections Per Day 14,000 New Infections Per Day WorldwideWorldwide
In 2001, there were 14,000 new HIV infections per day:
half were women and half were persons ages 15-24.

Regional HIV/AIDS Statistics and Features, Regional HIV/AIDS Statistics and Features, End of 2001End of 2001 Main mode(s) of
transmission
Sub-Saharan Africa
North Africa & Middle EastSouth and South-East Asia
East Asia & PacificLatin America
CaribbeanEastern Europe & Central Asia
Western EuropeNorth America
Australia & New Zealand
TOTAL
Hetero
Hetero, IDU
Hetero, IDU
IDU, Hetero, MSMMSM, IDU, Hetero
Hetero, MSM
IDU
MSM, IDU
MSM, IDU, Hetero
MSM
8.4%
0.2%
0.6%0.1%
0.5%
2.2%
0.5%
0.3%0.6%
0.1%
1.2%
55%
40%
35%20%
30%
50%
20%
25%20%
10%
48%
Adult prevalence
rate *% of HIV-positive who are women
UNAIDS Report, December 2001

Epidemiology: HIV/AIDS Epidemiology: HIV/AIDS Among Women in the USAmong Women in the US

*Adjusted for reporting delay
Estimated* AIDS Incidence in Women and Adolescent Girlsand Percentage of AIDS Cases,
January 1986 –December 2001, United States
Year of Diagnosis1986198719881989199019911992199319941995199619971998199920002001
16,000
12,000
8,000
4,000
0
30
25
20
15
10
5
0
% o
f Case
s
Nu
mb
er
of
Case
s
*Adjusted for reporting delay
and Percentage of AIDS Cases,January 1986 –December 2001, United States
Year of Diagnosis1986198719881989199019911992199319941995199619971998199920002001
16,000
12,000
8,000
4,000
0
30
25
20
15
10
5
0
% o
f Case
s
Nu
mb
er
of
Case
s

*Includes14 women of unknown race/ethnicity
AIDS Cases and Rates among Women and
Number %
7,023 63
2,040 18
1,894 17
42
69
11,082
<1
1
100
Race/EthnicityRate per100,000
White, not Hispanic
47.8Black, not Hispanic
2.4
Hispanic 12.9
American Indian/Alaska Native
Asian/Pacific Islander
Total*
4.9
1.5
*Includes14 women of unknown race/ethnicity
AIDS Cases and Rates among Women andAdolescent Girls, by Race/Ethnicity, Reported in 2001, United States
Number %
7,023 63
2,040 18
1,894 17
42
69
11,082
<1
1
100
Race/EthnicityRate per100,000
White, not Hispanic
47.8Black, not Hispanic
2.4
Hispanic 12.9
American Indian/Alaska Native
Asian/Pacific Islander
Total*
4.9
1.5

** Includes patients whose medical record review is pending; patients who died, were lost to follow-up, or declined interview;and patients with other or undetermined modes of exposure
* Data adjusted for reporting delays and estimated proportional redistribution of cases initially reported without risk.Data reported through June 2002
Includes sex with a bisexual male, a person with hemophilia, a transfusion recipient with HIV infection, or an HIV-infectedperson with an unspecified risk
†
Sex withinjection drug user
16%
Injection drug use32%
Other/not identified**3%
Sex with men ofother or
unspecified risk50%
†
Heterosexualtransmission
66%
United States
** Includes patients whose medical record review is pending; patients who died, were lost to follow-up, or declined interview;and patients with other or undetermined modes of exposure
* Data adjusted for reporting delays and estimated proportional redistribution of cases initially reported without risk.Data reported through June 2002
Includes sex with a bisexual male, a person with hemophilia, a transfusion recipient with HIV infection, or an HIV-infectedperson with an unspecified risk
†
Sex withinjection drug user
16%
Injection drug use32%
Other/not identified**3%
Sex with men ofother or
unspecified risk50%
†
Heterosexualtransmission
66%
Estimated* AIDS Incidence in Women and Adolescent Girls, by Exposure Category, Diagnosed in 2001,
United States

Number of Cases
FemaleMale
AIDS in 13- to 19 -Year-Olds, by Sex and Year of Report, through December 2001, United States
N=4,428
34 35 5377
126136181162 152
578
412392398371
298311
1993 definition change
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999
Year of ReportBefore1985
0
100
200
300
400
500
600
700
340372
2000 2001
Num
ber o
f Cas
es
Number of Cases
FemaleMale
AIDS in 13- to 19 -Year-Olds, by Sex and Year of Report, through December 2001, United States
N=4,428
34 35 5377
126136181162 152
578
412392398371
298311
1993 definition change
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999
Year of ReportBefore1985
0
100
200
300
400
500
600
700
340372
2000 2001
Num
ber o
f Cas
es
FemaleMale
AIDS in 13- to 19 -Year-Olds, by Sex and Year of Report, through December 2001, United States
N=4,428
34 35 5377
126136181162 152
578
412392398371
298311
1993 definition change
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999
Year of ReportBefore1985
0
100
200
300
400
500
600
700
340372
2000 2001
Num
ber o
f Cas
es
Number of Cases
FemaleMale
AIDS in 13- to 19 -Year-Olds, by Sex and Year of Report, through December 2001, United States
N=4,428
34 35 5377
126136181162 152
578
412392398371
298311
1993 definition change
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999
Year of ReportBefore1985
0
100
200
300
400
500
600
700
340372
2000 2001
Num
ber o
f Cas
es
FemaleMale
AIDS in 13- to 19 -Year-Olds, by Sex and Year of Report, through December 2001, United States
N=4,428
34 35 5377
126136181162 152
578
412392398371
298311
1993 definition change
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999
Year of ReportBefore1985
0
100
200
300
400
500
600
700
340372
2000 2001
Num
ber o
f Cas
es
Number of Cases
FemaleMale
AIDS in 13- to 19 -Year-Olds, by Sex and Year of Report, through December 2001, United States
N=4,428
34 35 5377
126136181162 152
578
412392398371
298311
1993 definition change
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999
Year of ReportBefore1985
0
100
200
300
400
500
600
700
340372
2000 2001
Num
ber o
f Cas
es
FemaleMale
AIDS in 13- to 19 -Year-Olds, by Sex and Year of Report, through December 2001, United States
N=4,428
34 35 5377
126136181162 152
578
412392398371
298311
1993 definition change
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999
Year of ReportBefore1985
0
100
200
300
400
500
600
700
340372
2000 2001
Num
ber o
f Cas
es

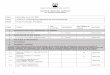
As of December 2001, 4,428 adolescents (persons aged 13-19 years) have been reported with AIDS.
In earlier years, most reported cases were in men; over time, the male-to-female ratio has decreased. In 2001, 372 adolescents were reported with AIDS; of these, 195 (52%) were men and 177 (48%) werewomen.
AIDS in 13- to 19-Year-Olds, by Sex and Year of Report,through December 2001, United States
-
-to-
- - -
As of December 2001, 4,428 adolescents (persons aged 13-19 years) have been reported with AIDS.
In earlier years, most reported cases were in men; over time, the male-to-female ratio has decreased. In 2001, 372 adolescents were reported with AIDS; of these, 195 (52%) were men and 177 (48%) werewomen.
AIDS in 13- to 19-Year-Olds, by Sex and Year of Report,through December 2001, United States
-
-to-
- - -

0
1000
2000
3000
4000
AIDS in 20- to 24 -Year-Olds, by Sex and Year of Report, through December 2001, United States
N=28,665
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1998 1999 2000 20011996 1997
Year of Report1985Before
297 364
642
969
1499 14881673
1502 1503
2653
3862
2424
1843
2169
1482 14931341 1461
1993 definition change
FemaleMale
Num
ber o
f Cas
es

As of December 2001, a total of 28,665 persons aged 20 to 24 years were reported with AIDS; most were men.In 1985, 89% of cases reported in persons 20 to 24 years old were in men. However, as heterosexual contact has accounted for an increasing proportion of HIV infections, particularly in women, the proportion of cases reported in women has increased. In 2001, 41% of the 1,461 cases reported were in women.
AIDS in 20- to 24-Year-Olds, by Sex and Year of Report, through December 2001, United States
As of December 2001, a total of 28,665 persons aged 20 to 24 years were reported with AIDS; most were men.In 1985, 89% of cases reported in persons 20 to 24 years old were in men. However, as heterosexual contact has accounted for an increasing proportion of HIV infections, particularly in women, the proportion of cases reported in women has increased. In 2001, 41% of the 1,461 cases reported were in women.
AIDS in 20- to 24-Year-Olds, by Sex and Year of Report, through December 2001, United States

AIDS in Adolescents and Adults, by Sex and Age atDiagnosis, Reported in 2001 , United States
13-19 years
N=372 N=1,461
20-24 years
Male Female
59%
41%
N=40,271
25 years
75%
25%
52%
48%
AIDS in Adolescents and Adults, by Sex and Age atDiagnosis, Reported in 2001 , United States
13-19 years
N=372 N=1,461
20-24 years
Male Female
59%
41%
N=40,271
25 years
75%
25%
52%
48%

AIDS in Adolescents and Adults, by Sex and Age at Diagnosis, Reported in 2001, United States
AIDS in Adolescents and Adults, by Sex and Age at Diagnosis, Reported in 2001, United States
The ratio of men to women with AIDS varies by age at diagnosis.
Of adolescents aged 13 to19 years at AIDS diagnosis, 48% were women; of persons20-24 years of age, 41% were women.
In 2001, most persons 25 years of age and older reported with AIDS were men (75%).
AIDS in Adolescents and Adults, by Sex and Age at Diagnosis, Reported in 2001, United States
AIDS in Adolescents and Adults, by Sex and Age at Diagnosis, Reported in 2001, United States
The ratio of men to women with AIDS varies by age at diagnosis.
Of adolescents aged 13 to19 years at AIDS diagnosis, 48% were women; of persons20-24 years of age, 41% were women.
In 2001, most persons 25 years of age and older reported with AIDS were men (75%).

13-19 years
Reported HIV* in Adolescents and Adults, by Sex and Age at Diagnosis, Reported in 2001,
United States
Male Female
25 years20-24 years
*From the areas with confidential HIV case surveillance for adults and adolescents in 2001
60%
40%
70%
30%
44%
56%
13-19 years
Reported HIV* in Adolescents and Adults, by Sex and Age at Diagnosis, Reported in 2001,
United States
Male Female
25 years20-24 years
*From the areas with confidential HIV case surveillance for adults and adolescents in 2001
60%
40%
70%
30%
44%
56%

** Includes patients whose medical record review is pending; patfollow-up or declined interview; and patients with other or undetermined modes of exposure
Estimated* AIDS Incidence in Male Adolescents and Young Adults, by Exposure Category,
Diagnosed through December 2001, United States
Men who have sex with menInjection drug useMen who have sex with menand inject drugs
HemophiliaHeterosexual contactTransfusion recipientOther/undetermined**
Total
1,066253
150769186103136
2,663
%4010
629745
100
N20-24 years
N13-19 years
13,4642,867
2,217696
1,409126107
20,887
%6414
113711
100
Exposure category
** Includes patients whose medical record review is pending; patients who died, were lost to*Data adjusted for reporting delays and redistribution of risk for cases initially reported without risk
Young Adults, by Exposure Category, Diagnosed through December 2001, United States
Men who have sex with menInjection drug useMen who have sex with menand inject drugs
HemophiliaHeterosexual contactTransfusion recipientOther/undetermined**
Total
1,066253
150769186103136
2,663
%4010
629745
100
N20-24 years
N13-19 years
13,4642,867
2,217696
1,409126107
20,887
%6414
113711
100
Exposure category
** Includes patients whose medical record review is pending; patfollow-up or declined interview; and patients with other or undetermined modes of exposure
Estimated* AIDS Incidence in Male Adolescents and Young Adults, by Exposure Category,
Diagnosed through December 2001, United States
Men who have sex with menInjection drug useMen who have sex with menand inject drugs
HemophiliaHeterosexual contactTransfusion recipientOther/undetermined**
Total
1,066253
150769186103136
2,663
%4010
629745
100
N20-24 years
N13-19 years
13,4642,867
2,217696
1,409126107
20,887
%6414
113711
100
Exposure category
** Includes patients whose medical record review is pending; patients who died, were lost to*Data adjusted for reporting delays and redistribution of risk for cases initially reported without risk
Young Adults, by Exposure Category, Diagnosed through December 2001, United States
Men who have sex with menInjection drug useMen who have sex with menand inject drugs
HemophiliaHeterosexual contactTransfusion recipientOther/undetermined**
Total
1,066253
150769186103136
2,663
%4010
629745
100
N20-24 years
N13-19 years
13,4642,867
2,217696
1,409126107
20,887
%6414
113711
100
Exposure category

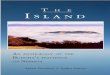
Since the beginning of the epidemic, more than 2,600 adolescent men aged 13 to 19 years and more than 20,000 men aged 20 to 24 years have been reported with AIDS. In adolescent men with AIDS, 29% had hemophilia and acquired their infection before blood products were heat treated to prevent HIV transmission. In contrast, 3% of AIDS cases among young adult men were attributed to receipt of blood products for hemophilia. A majority (64%) of the men in the older age group were reported as having sex with other men and another 11% were men who were reported as having sex with men and injecting drugs. Injection drug use is more common among the 20 to 24 year old men reported with AIDS than among adolescents with AIDS, but less common than among men over 24 years. Approximately 7% of AIDS cases among men aged 13 to 24 years were reported with heterosexual contact as their exposure category.
Estimated AIDS Incidence in Male Adolescents and Young Adults, by Exposure Category, Diagnosed through December 2001, United States
Since the beginning of the epidemic, more than 2,600 adolescent men aged 13 to 19 years and more than 20,000 men aged 20 to 24 years have been reported with AIDS. In adolescent men with AIDS, 29% had hemophilia and acquired their infection before blood products were heat treated to prevent HIV transmission. In contrast, 3% of AIDS cases among young adult men were attributed to receipt of blood products for hemophilia. A majority (64%) of the men in the older age group were reported as having sex with other men and another 11% were men who were reported as having sex with men and injecting drugs. Injection drug use is more common among the 20 to 24 year old men reported with AIDS than among adolescents with AIDS, but less common than among men over 24 years. Approximately 7% of AIDS cases among men aged 13 to 24 years were reported with heterosexual contact as their exposure category.
Estimated AIDS Incidence in Male Adolescents and Young Adults, by Exposure Category, Diagnosed through December 2001, United States

Injection drug useHemophiliaHeterosexual contactTransfusion recipientOther/undetermined**
Total
N13-19 years 20-24 years
Exposure Category
38418
1,321111158
1,992
%
191
6668
100
N
2,55929
5,86415785
8,383
%
29<16721
100
Estimated* AIDS Incidence in Female Adolescents and Young Adults, by Exposure Category,
Diagnosed through December 2001, United States
** Includes patients whose medical record review is pending; patients who died, were lost tofollow-up or declined interview; and patients with other or undetermined modes of exposure
*Data adjusted for reporting delays and redistribution of risk for cases initially reported without risk
Injection drug useHemophiliaHeterosexual contactTransfusion recipientOther/undetermined**
Total
N13-19 years 20-24 years
Exposure Category
38418
1,321111158
1,992
%
191
6668
100
N
2,55929
5,86415785
8,383
%
29<16721
100
Estimated* AIDS Incidence in Female Adolescents and Young Adults, by Exposure Category,
Diagnosed through December 2001, United States
** Includes patients whose medical record review is pending; patients who died, were lost tofollow-up or declined interview; and patients with other or undetermined modes of exposure
*Data adjusted for reporting delays and redistribution of risk for cases initially reported without risk

AIDS Cases 2001N=372
<1%
18%61%
21%
AIDS Cases in 13- to 19-Year-Olds by Race/Ethnicity, United States
White not Hispanic
Black not Hispanic
Hispanic Asian/Pacific Islander and American Indian/Alaska Native
AIDS Cases 1981-2001N=4,428
1%
27%
51%20%
U. S. Population 13-19 N 28 Million
5%
65%
15%15%
AIDS Cases 2001N=372
<1%
18%61%
21%
AIDS Cases in 13- to 19-Year-Olds by Race/Ethnicity, United States
White not Hispanic
Black not Hispanic
Hispanic Asian/Pacific Islander and American Indian/Alaska Native
AIDS Cases 1981-2001N=4,428
1%
27%
51%20%
U. S. Population 13-19 N 28 Million
5%
65%
15%15%

AIDS and HIV Among African AIDS and HIV Among African American and LatinosAmerican and Latinos

Estimated AIDS Incidence in Women, by Exposure Category and Age at Diagnosis,Diagnosed in 2001, United States
Most of the AIDS cases diagnosed in 2001 among females aged greater than 13 years were attributed to heterosexual contact.
Of cases among women aged 30-49 years, 35% were attributed to injection drug use, compared with 16% of cases in females aged 13-19 years, 21% in women aged 20-29 years, and 29% in women over 50.
Of females aged 13-19 years, 19% were exposed to HIV through perinatal transmission, and are included in the “other/not identified” exposure category.
Estimated AIDS Incidence in Women, by Exposure Category and Age at Diagnosis,Diagnosed in 2001, United States
Most of the AIDS cases diagnosed in 2001 among females aged greater than 13 years were attributed to heterosexual contact.
Of cases among women aged 30-49 years, 35% were attributed to injection drug use, compared with 16% of cases in females aged 13-19 years, 21% in women aged 20-29 years, and 29% in women over 50.
Of females aged 13-19 years, 19% were exposed to HIV through perinatal transmission, and are included in the “other/not identified” exposure category.




AIDS Rates in Women, Reported in 2001
Rates of reported cases of AIDS per 100,000 women and adolescent girls are shown for each state, the District of Columbia, Puerto Rico, and the Virgin Islands. The highest rates were found in the District of Columbia, New York, the Virgin Islands, Maryland, Delaware, Puerto Rico, and Florida.
Rates were lowest in states in the Midwest. Nearly every state reported some AIDS cases among females in 2001.
The high rate in the District of Columbia should be interpreted with consideration that D.C. is more similar to a city than a state.
Rates were not calculated for states that reported fewer than 5 AIDS cases in females in 2001.
AIDS Rates in Women, Reported in 2001
Rates of reported cases of AIDS per 100,000 women and adolescent girls are shown for each state, the District of Columbia, Puerto Rico, and the Virgin Islands. The highest rates were found in the District of Columbia, New York, the Virgin Islands, Maryland, Delaware, Puerto Rico, and Florida.
Rates were lowest in states in the Midwest. Nearly every state reported some AIDS cases among females in 2001.
The high rate in the District of Columbia should be interpreted with consideration that D.C. is more similar to a city than a state.
Rates were not calculated for states that reported fewer than 5 AIDS cases in females in 2001.

Limitations of Traditional Limitations of Traditional Behavioral Models in HIV Behavioral Models in HIV PreventionPrevention

Health Belief ModelHealth Belief Model
•Perception of:
•Susceptibility to illness
•Severity of illness
•Effectiveness of prevention measures
•Barriers to action
Cues to Action
Behavior
Change

Theory of Reasoned ActionTheory of Reasoned Action
Attitude toward the behavior
Subjective norm
Intention Behavior

Perceived Self EfficacyPerceived Self Efficacy
•Knowledge
•Perception of risk
•Sense of competency in performing new behavior
•Social support
BehaviorChange

Stages of ChangeStages of Change
Proposes stages in behavior changePrecontemplationContemplationPreparationActionMaintenance

Faulty Assumptions of HIV Risk Faulty Assumptions of HIV Risk Behavior ModelsBehavior Models Individualistic conception of behavior; fail
to consider the cultural and social context of sexuality
Ignore unequal status of women and power differential between women and men
Fail to ignore that “safer sex” involves very different behaviors for women and men
Fail to consider impact of addiction, trauma and mental illness

Gender and Cultural Factors in HIV Gender and Cultural Factors in HIV RiskRisk

Relevant Findings from Previous Relevant Findings from Previous Research: Male Gender RolesResearch: Male Gender Roles Male beliefs about gender roles is strongly
related to attitudes toward sexuality and women (Pleck et al, 1992)– Negative attitudes toward condom use– Less use of condoms– Less belief in male responsibility to prevent
pregnancy– Greater belief that pregnancy validates
masculinity It is important to consider that gender roles vary
across cultures and these roles have been found to impact HIV risk behaviors (Amaro et al, 2001a; 2001b; 2001c).

Relevant Findings from Previous Relevant Findings from Previous Research: Relationship PowerResearch: Relationship Power Women with lower relationship power are
significantly more likely to not use condoms (Purlerwitz et al, 2000; 2002)
Girls with lower relationship power are significantly more likely to experience intimate partner violence (Amaro et al, 2003)
Because relationship power is based on cultural norms, differences are likely to exist by race/ethnicity, class, religion, etc.

Relevant Findings from Previous Relevant Findings from Previous Research: Abuse and HIV RiskResearch: Abuse and HIV RiskWomen who fear violence and/or are in
violent relationships are less likely to use condoms (Amaro & Raj, 2000)
History of childhood and adult physical and/or sexual abuse is associated with increased sexual risk behaviors and non-condom use (Amaro & Raj, 2000)

Gender Informed HIV Prevention Gender Informed HIV Prevention ApproachesApproaches Recognize the role of power differentials between
women and men Seek to give women tools to change the power
imbalance in sexual negotiation Recognize the limitations of individual models of
behavior change Stress the importance of interventions to change
social norms, male risk behaviors and women’s social status
However, many of these approaches have not addressed the specific needs of women with drug dependence, mental illness and history of trauma

Prevalence of Co-Occurring DisordersPrevalence of Co-Occurring Disorders

Current Prevalence Estimates for Current Prevalence Estimates for Substance Abuse Disorders, Mental Substance Abuse Disorders, Mental Illness and ComorbidityIllness and Comorbidity
Substance abuse or dependence: – 6% of adult population = 11.5 million people
Diagnosable mental illness:– 23% of population 18-54 years = 44 million people
Comorbidity:– 3% of adult population =6 million people
National Comorbidity Study, Mental Health: A Report of the Surgeon General, 1999

Percent of Persons with Substance Abuse Percent of Persons with Substance Abuse Disorders & Psychiatric DisordersDisorders & Psychiatric Disorders
0
10
20
30
40
50
60
ECA Study NC Study
Per
cent
Reiger et al, 1990; Kessler et al, 1994

Substance Abuse and Substance Abuse and Dependence and VictimizationDependence and Victimization
Substance abuse disorders are more prevalent in individuals with a history of criminal victimization
– Burnam et al J Consult Clin Pscycho 1988
– Cottler et al Am J Psychiatry 1992
– Elliot et al Multiple Problem Youth 1989
– George et al Sexual Assault 1986
– Helzer et al N Engl J Med 1987
– Kulka et al Trauma and the Vietnam War Generation 1990

VictimizationVictimization
Women were victims of >4.5 million violent crimes in 1993– 29% of perpetrators were intimates,
50% acquaintancesBureau of Justice Statistics National Crime Victimization Survey, 1995
1 in 5 women has been the victim of a completed rape
1 in 4 has been physically battered
American College of Obs. & Gyns 1993

Victimization Reported by Medical PatientsVictimization Reported by Medical Patients Emergency Departments
– Denver 1995: 11.7% “acute” domestic violence among women with current male partner, 50% lifetime history
– Philadelphia 1987, 1989: 1/3 of female trauma patients with injuries from DV
Family Practice– Midwest 1992: Lifetime 39% Previous Year 23%
Internal Medicine and General Medicine– Irvine, CA 1991: Lifetime 34% Previous Year
17%– Rochester, Minn 1990: Childhood Sexual 17%
Childhood Physical 5% Prenatal Care:7% abuse during pregnancy (Amaro et al
AJPH,1990)

Victimization Reported by Psychiatric and Victimization Reported by Psychiatric and Substance Abuse Treatment ClientsSubstance Abuse Treatment Clients
Psychiatric Emergency Services– 25% (Stark et al, Office of Domestic Violence 1981)
Psychiatric Outpatient– 50% (Hilbermann & Muston, Victimology 1977-78)
Psychiatric Inpatient– 64% (Jacobsen & Richardson, AJP 1987)
Substance Abuse Treatment– 60-90% (Amaro et al, HJBS 1999; Helzer et al, NEJM 1987; Brady et
al, AJP 1993; Rohsenow et al, JSA 1998, Walen, NIDA 1992)
– 41% (Liebshutz et al,Arch of Int Med 1997)

Comorbidity in a Boston Sample of Comorbidity in a Boston Sample of Women in Substance Abuse Treatment Women in Substance Abuse Treatment (n=354)(n=354)
Race/Ethnicity Total n(%)
Hispanic 119 (35%)
White 98 (29%)
Black 117 (35%)
Alaskan 1 (0.30%)
Multi race 3 (0.89%)

Trauma HistoryTrauma History
0102030405060708090
100
AnyTrauma
IntimatePartnerViolence
SexualAssault
ChildhoodAbuse

Mental Health SymptomsMental Health Symptoms
0
10
20
30
40
50
60
70
80
90
100
Depression Anxiety Suicide UncontrollableThoughts

Association of Mental Health Association of Mental Health Symptoms with Trauma ExposureSymptoms with Trauma Exposure
(-) Trauma
(+) Trauma
No Mental Health Symptoms
2%
10%
Mental Health Symptoms
5%
83%
p=0.025

Typical Presentations of Women in TxTypical Presentations of Women in Tx
Chronic and severe physical and sexual abuse, in abusive relationship
Major depression, anxiety disorder, or PTSD
Addiction to crack, cocaine, heroin
Multiple treatment attempts
Partner is active drug user
Multiple health problems Past/current criminal justice
history Few educational and job
skills Has 3-5 children, DSS
involved Living in poverty, may be
homeless or in temporary housing
HIV Risk Behaviors

Marginalization and HIV Risk in Marginalization and HIV Risk in WomenWomen

Gender Specific Nature of Risk Gender Specific Nature of Risk in Women in Women Marginalized populationsLower social status and lower power
in relationshipsSexual relationships with older menViolence against women in the home,
rape in war, sexual abuseBiological vulnerability due to age and
transmission effectivenessUnited Nations Report on the Global HIV/AIDS Epidemic, June 2000

Marginalization and HIV RiskMarginalization and HIV Risk
Women most affected:– Black and Latinas– Poor– Abuse history– Addiction disorders– Mental health problems– Incarceration history– Sex workersLogan, TK, Cole, J & Leukefeld, Women, sex and HIV: Social and contextual factors, meta-analysis of published interventions, and implications for practice and research. Psych Bulleting, 2002, 128(6), 851-885.

Pathways of Marginalization to Pathways of Marginalization to HealthHealth1. Economic and social deprivation2. Socially inflicted trauma3. Responses to discrimination4. Targeted marketing of commodities
that harm health5. Inadequate medical care6. Toxic substances and hazardous
conditionsKrieger, N. Does racism harm health? AJPH, 93(2), 2003, 195-199.

Relationship of Marginalization to HIV Relationship of Marginalization to HIV RiskRisk
HIV Risk Behaviors
Drug Addiction
Mental Illness
Abuse/Trauma
Marginalization
•Negative ascriptions, social & economic status-resources, political power, ecological risks
•Stress, coping and resistance, horizontal violence
•Silencing, violence and fear, internalization

Dynamics of the MarginDynamics of the Margin
Silencing Violence & Fear Internalized
Oppression
Amaro & Raj, 2000

Dynamics of Oppression: Dynamics of Oppression: SilencingSilencing
Discourages subordinate’s full and free expression of their experience, characterizes subordinates falsely, and describes this as the normal or natural situation ordered by higher and better powers ranging from God to biology
Amaro & Raj, 2000; Bulhan, 1985; Miller, 1986; Freire, 1970

Violence and Fear: HIV as An Violence and Fear: HIV as An ExampleExample
Relationship of HIV Risk Behaviors to:– History of abuse– Current abusive relationship– Fear of partner reaction to sexual
negotiation

Silencing: HIV as an Example Silencing: HIV as an Example
Individual Level– gender roles – power in relationships

Coping and ResistanceCoping and Resistance Culture of Silence
– internalization, shame of one’s experience, identification with values of the oppressor
Awareness– speaking and discovering one’s reality,
recognizing the institutionalized basis of oppression, connection to others
From Awareness to Practice– organized connections to others in the margin,
learning from those who came before you, translating concepts to practice, taking risks, working with outsiders aligned with your goals
Freire

A Trauma-Informed Intervention A Trauma-Informed Intervention for Women with Co-Occurring for Women with Co-Occurring DisordersDisorders

Women and Co-Occurring Disorders Women and Co-Occurring Disorders StudyStudy
Goal: To test the effectiveness of an integrated and trauma informed system of care for women and their children in 9 sites across the US
Rationale: Women who have substance abuse and mental health problems experience high rates of trauma. Lack of integrated services results in ineffective treatment for women with co-occurring disorders
Funded by: Substance Abuse and Mental Health Services Administration

Study DescriptionStudy Description
Sample: Women in substance abuse treatment with co-occurring mental illness and history of abuse
Design: Quasi-experimental design using intervention vs service as usual sites
Outcomes: length of stay in treatment, trauma and mental illness symptomatology, relapse, re-victimization, other measures of functioning, and HIV risk behaviors

Study DescriptionStudy Description
October 2000-September 2003181 women in SA treatment received the
Enhanced Intervention at 5 participating sites:161 women in SA treatment received Standard
Care at comparable treatment programsMeasures: baseline, 3, 6, 9 & 12 months Study participants: African American, Latina and
non-Hispanic white women

Trauma Recovery and Leadership Trauma Recovery and Leadership Skills Enhanced ServicesSkills Enhanced Services 25-week Trauma Recovery Group
– Focus on breaking the silence, giving voice to one’s experience, awareness of social status and risk of violence, HIV risk, development of resistance and coping skills and safer sex skills
Peer-led intensive leadership training– Focus on giving voice to their experience, connecting
to the shared experience, leadership skills development and practicing leadership skills in policy and community settings
Consumer role & voice in services Psychiatric services for trauma and mental
health treatment

Findings on HIV Risk Behaviors Findings on HIV Risk Behaviors at 6-month Followupat 6-month Followup Intervention is associated with significantly less
high risk sex behavior at 6 months, compared to the treatment-as-usual group.
After controlling for differences in treatment modality, baseline sex behavior, age, ethnicity, living situation (controlled environment or not), lifetime and recent trauma history, trauma symptoms, illegal drug use at follow-up and treatment status at follow-up.– OR=0.29 (95% CI=0.12, 0.67)

Findings on Relationship Power Findings on Relationship Power (N=173)(N=173)
After adjusting for baseline characteristics– 6-month RPS scores are associated
with HIV risk behavior at that time.• Higher scores (more relationship power) are
associated with less HIV risk behavior (Total RPS score OR=0.39 per unit; RPS Control OR=0.46; RPS decision OR=0.51)

HIV Prevention Intervention with HIV Prevention Intervention with LatinasLatinas
Raj, A., Amaro, H., Cranston, K, Martin, B., Cabral, H., Navarro, A., & Conron, K. (2002) Is a women’s health program as effective as an HIV program in reducing HIV risk among Latinas? Public Health Reports, 116, 599-607.

HIV/AIDS and LatinasHIV/AIDS and Latinas
HIV is disproportionately affecting Latinas– Hispanics comprise 9% of the US population,
but 20% of female AIDS cases are among Hispanic women
– In Massachusetts, Hispanics comprise 4.6% of the population, but 27% of AIDS cases are among Hispanic women
No published studies on effective interventions for Latinas

Study PurposeStudy PurposeTo evaluate two gender-specific HIV
prevention program for Latinas– 1. An Intensive HIV Prevention Program– 2. A General Health Program with 4 HIV
sessions

The Intensive HIV Prevention ProgramThe Intensive HIV Prevention Program
12 week intensive HIV intervention conducted in Spanish
Theoretical Framework– Social Cognitive Theory– Empowerment Theory– Self-in-Relation Theory– Theory of Gender and Power
Strategies– Psychoeducational – Participatory

The General Health ProgramThe General Health Program
12 week Women’s Health Program including 4 sessions on HIV and 8 sessions on various social and health topics-conducted in Spanish
Theoretical Framework– Not specified
Strategies– Psycho-educational

Research DesignResearch Design
Compare 3 treatment groups on Outcome Behaviors– Condom Use and Intentions– Safer Sex Communication– HIV Testing
Survey at Pre, Post, 3 & 15 Month Follow-up

Pre-Post Data AnalysesPre-Post Data Analyses
Crude Analyses– Logistic and linear regression analyses
Adjusted Analyses– Logistic and linear regression analyses
controlling for demographicsDose Analyses
– Logistic and linear regression analyses controlling for demographics and dosage

SampleSample
Eligibility Criteria– Age 18-35– In a relationship with a main male partner– Not a consistent condom user
Sample Size=170Dropped From Analyses (n=8)
– reporting consistent condom use– HIV-positive women– heavy substance use/cognitive
impairment

Sample (n=162)Sample (n=162) Age 18-36
– (meanage=28.6)
Employed: 47% Income
– 17% none– 57% $1-800/month– 50% on govt. asst
Education– 29% <H.S.
Main Partner: 98.1%– 27% Married– 38% Live With
Relationship Length– mean= 5.4 years
Kids: 90%

Sample (n=162)Sample (n=162)
68% Non-English speakersBirthplace
– 55% Dominican Republic– 13% Puerto Rico– 13% Central America and Mexico– 8% South American– 11% United States

HIV RiskHIV Risk
63.2% never use condoms with their main partner
51% expressed some worry they might get AIDS
16.1% have had an STD13% had a risky main partner11% had more than one sex
partner in past 3 months

Study Retention RatesStudy Retention Rates
Posttest 3 Month Follow-up
15 Month Follow-up
HIV Intervention 94% 100% 91%
General Health Program
93% 97% 88%
Wait-List Control 73% 75% 77%

Increased Condom Use, Past 3 MonthsIncreased Condom Use, Past 3 Months
T1-T2
OR(95%CI)
T1-T3
OR(95%CI)
T1-T4
OR(95%CI)
HIV Intensive
Gen Health
Control
2.51
(.96-6.55)
2.67
(1.10-6.52)
4.26
(1.45-12.56)
4.88
(1.80-13.19 )
1.19
(0.41-3.43)
1.63
(0.61-4.35)

Increased Condom Use, AlwaysIncreased Condom Use, Always
T1-T2
OR(95%CI)
T1-T3
OR(95%CI)
T1-T4
OR(95%CI)
HIV Intensive
Gen Health
Control
2.93
(.51-17.04)
5.35
(1.09-26.33)
5.00
(.50-50.51)
9.73
(1.16-81.36)
1.57
(0.29-8.42)
2.88
(0.66-12.61)

Intent to Use CondomsIntent to Use Condoms
T1-T2
OR(95%CI)
T1-T3
OR(95%CI)
T1-T4
OR(95%CI)
HIV Intensive
Gen Health
Control
3.92
(1.21-12.69)
6.56
(2.19-19.69)
2.71
(.85-8.68)
5.54
(1.96-15.70)
0.32
(0.08-1.3)
1.95
(0.72-5.28)

Safer Sex CommunicationSafer Sex Communication
T1-T2
OR(95%CI)
T1-T3
OR(95%CI)
T1-T4
OR(95%CI)
HIV Intensive
Gen Health
Control
3.88
(1.53-9.80)
1.17
(.55-2.49)
3.26
(1.34-7.92)
1.83
(.84-3.95)
0.68
(0.24-1.87)
0.58
(0.23-1.46)

HIV Testing, Past 3 MonthsHIV Testing, Past 3 Months
T1-T2
OR(95%CI)
T1-T3
OR(95%CI)
T1-T4
OR(95%CI)
HIV Intensive
Gen Health
Control
1.79
(.66-4.81)
2.50
(1.02-6.12)
.84
(.30-2.37)
1.10
(.44-2.74)
0.95
(0.35-2.59)
0.44
(0.15-1.3)

ConclusionsConclusions
Intensive HIV Intervention and the General Health Program participants reported significantly greater condom use and condom use intent than did Control participants.
Only the HIV Intensive Intervention reported increases in safer sex communication
Only the Comparison Program reported a significant increase in HIV testing.
Majority of program effects were maintained at 3 month follow-up but lost at 15 month follow-up

LimitationsLimitations
Quasi-Experimental DesignReliance on Self ReportNon-generalizable sample

ImplicationsImplications
Latinas can be recruited and retained into 12 week HIV prevention/Health programs
These programs appear to have the potential of promoting HIV risk reduction
Research should be replicated with an RCT design
Further research is needed to determine how program effects can be maintained long-term with use of booster sessions

ConclusionConclusion
HIV epidemic among women in the US affects primarily African American and Latina women– Heterosexual transmission and drug use are
primary modes of transmission Sexual risk among women is embedded in the
cultural and social context of women’s lives – Social and cultural norms that ascribed power
based on gender places women at risk for abuse and lower control over sexual decision making
– There are high rates of history of abuse among women, especially among drug users
– History of abuse is associated with psychological trauma, which negatively affects women’s HIV risk

ConclusionsConclusions
Trauma informed interventions can reduce HIV risk behaviors among women with co-occurring disorders
Trauma informed interventions may also be useful in reducing HIV risk in women with a history of trauma without drug dependence