Embed Size (px)
Citation preview
Lucia Silla, MD, PhD
Cellular Therapy Center
HSCT Program Hospital de Clínicas de Porto Alegre
School of Medicine
Federal University of Rio Grande do Sul
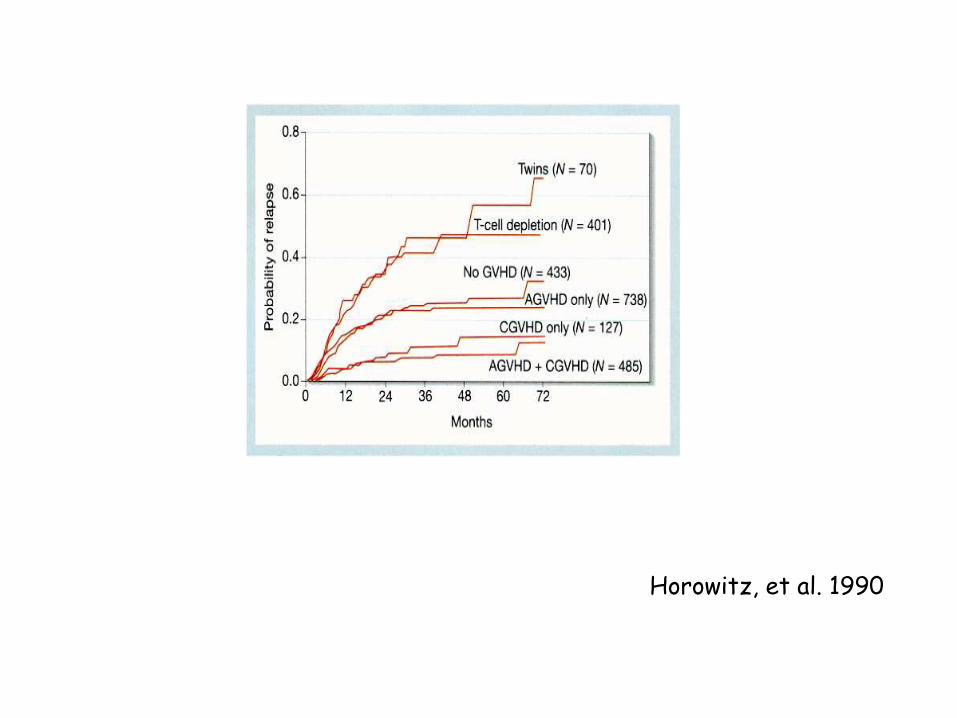
Horowitz, et al. 1990
graft versus leukemia effect
• T cells ?
• NK cells ?
• Malignant stem cell is the target?
• GVL and other hematological
malignancies?
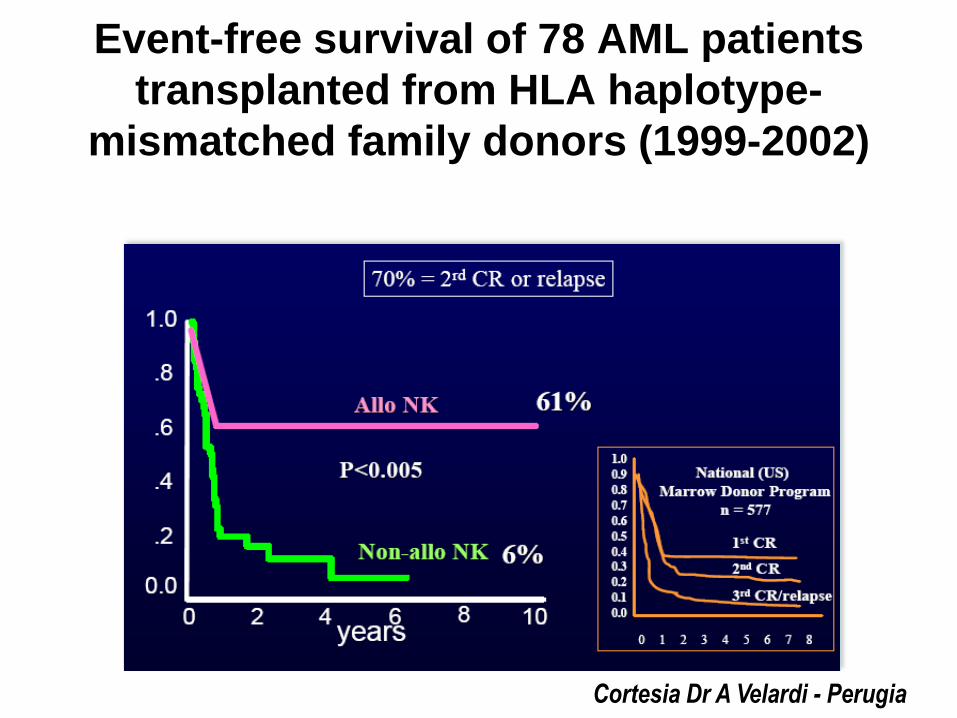
Event-free survival of 78 AML patients
transplanted from HLA haplotype-
mismatched family donors (1999-2002)
Cortesia Dr A Velardi - Perugia
NK
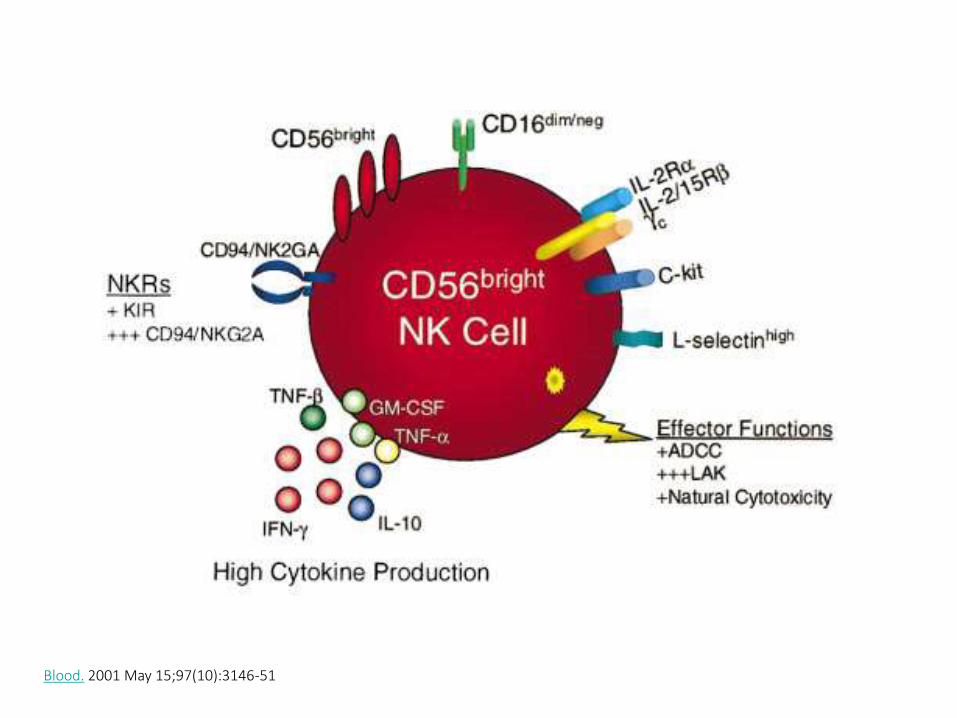
Innate immune system lymphocytes
kills virus infected and malignancy disturbed cells
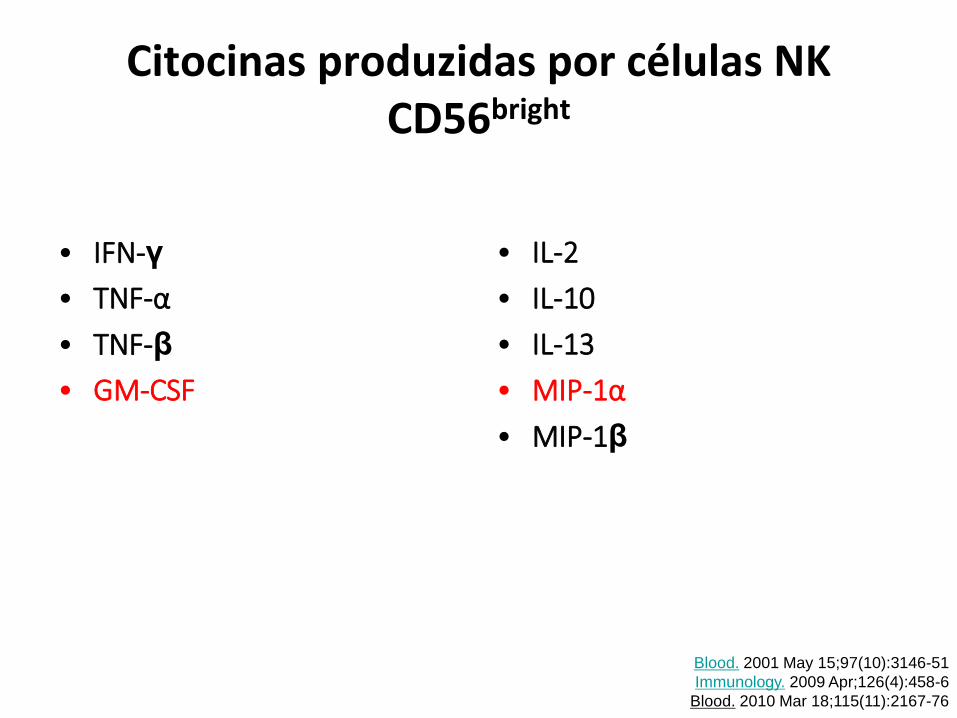
Citocinas produzidas por células NK CD56bright
• IFN-γ
• TNF-α
• TNF-β
• GM-CSF
• IL-2
• IL-10
• IL-13
• MIP-1α
• MIP-1β
Blood. 2001 May 15;97(10):3146-51
Immunology. 2009 Apr;126(4):458-6
Blood. 2010 Mar 18;115(11):2167-76
CD56dim
NK cell

CD56dim
NK cell
KIR(s) e Fc Receptor (CD16)
anti-leukemia potential
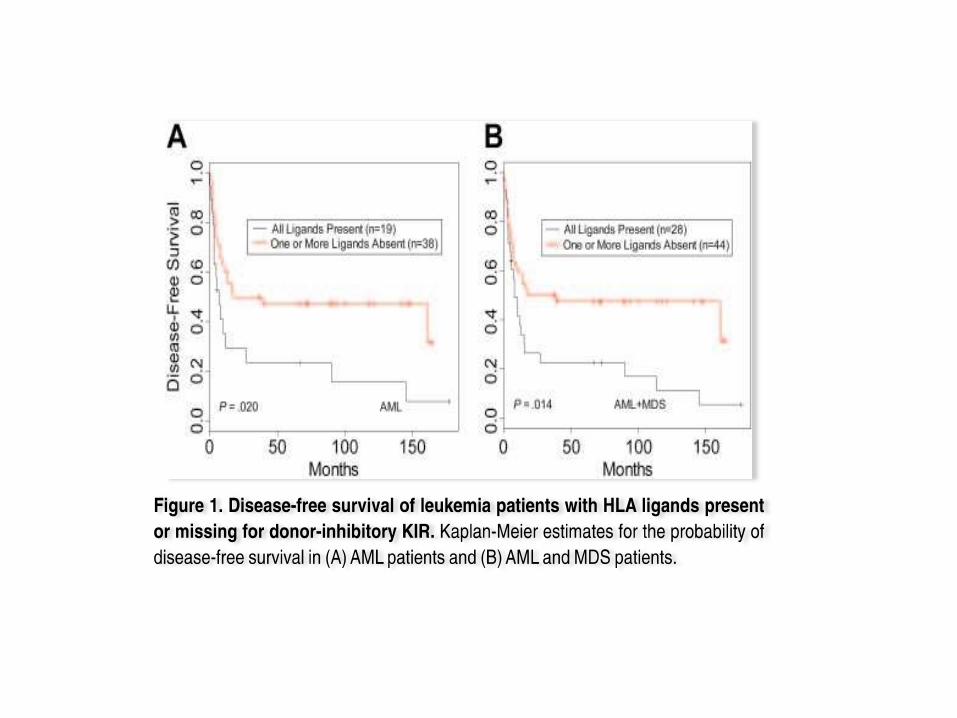
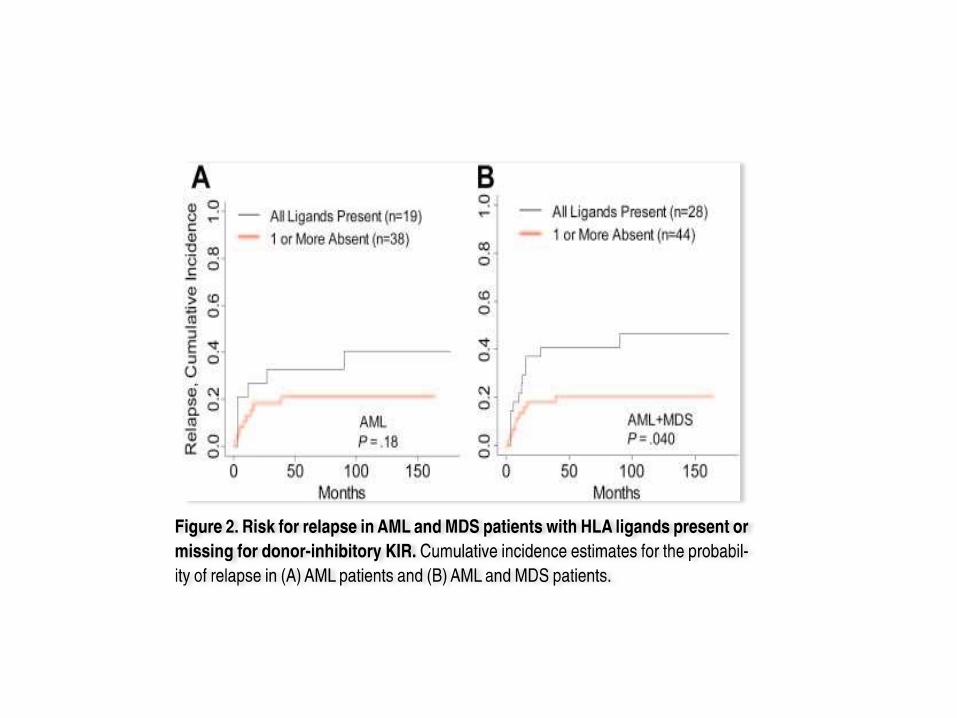
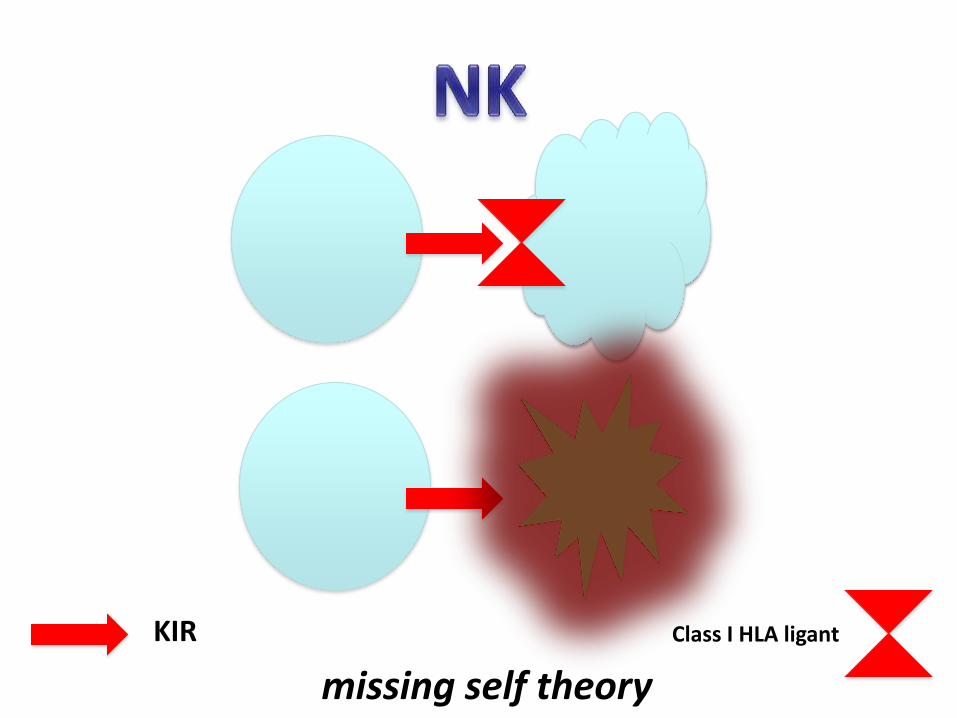
missing self theory
KIR Class I HLA ligant

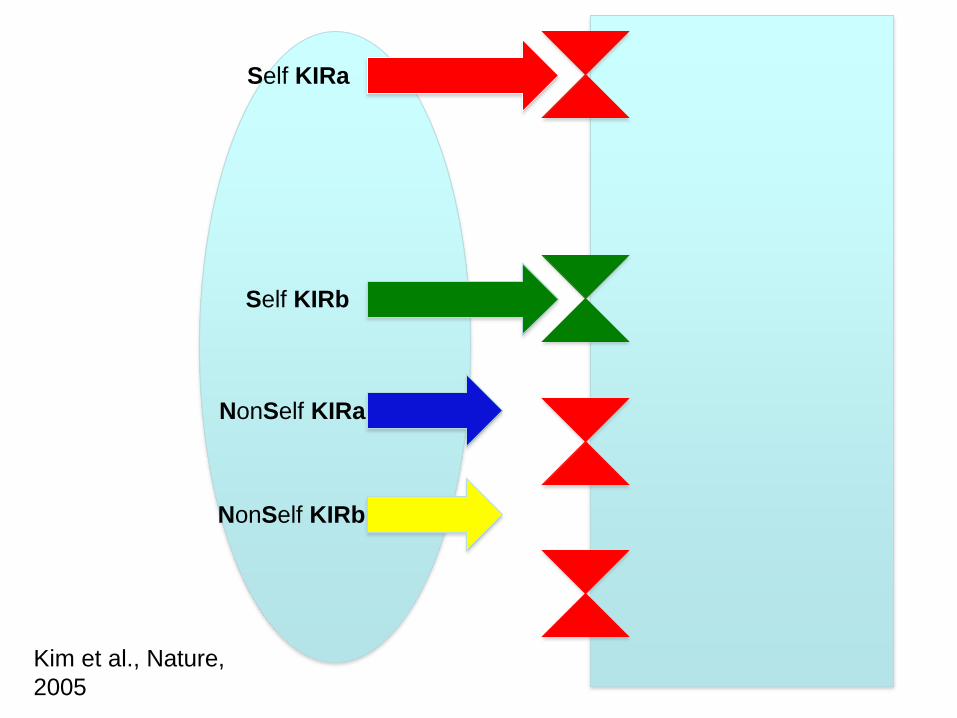
Self KIRa
Self KIRb
NonSelf KIRa
NonSelf KIRb
Kim et al., Nature,
2005
Kim et al. Nature, 2005
“Although recipient HLA class I alleles are clearly important, the absence of the appropriate recipient HLA ligands for the donor killer cell immunoglobulin-like inhibitory receptors (KIR) does not always impart an effective outcome. Licensing indicates that donor HLA class I alleles will influence the functional capacity of transplanted NK cells”.
Kim et al. Nature, 2005
• “Notably, the licensing effect was less prominent in pre-
activated NK cells, suggesting that licensing requirements
could be bypassed under certain circumstances. Perhaps
unlicensed NK cells become activated in response to pro-
inflammatory cytokines, which are known to activate most, if
not all, NK cells during infections. Such effects may aid anti-
pathogen defenses by potentially breaking NK-cell tolerance and
allowing the participation of larger numbers of NK cells at local sites
of inflammation, suggesting a potentially important function of
unlicensed NK cells”.
In vitro expansion can “license” in vivo
unlicensed NK Cells?
myeloid leukemias

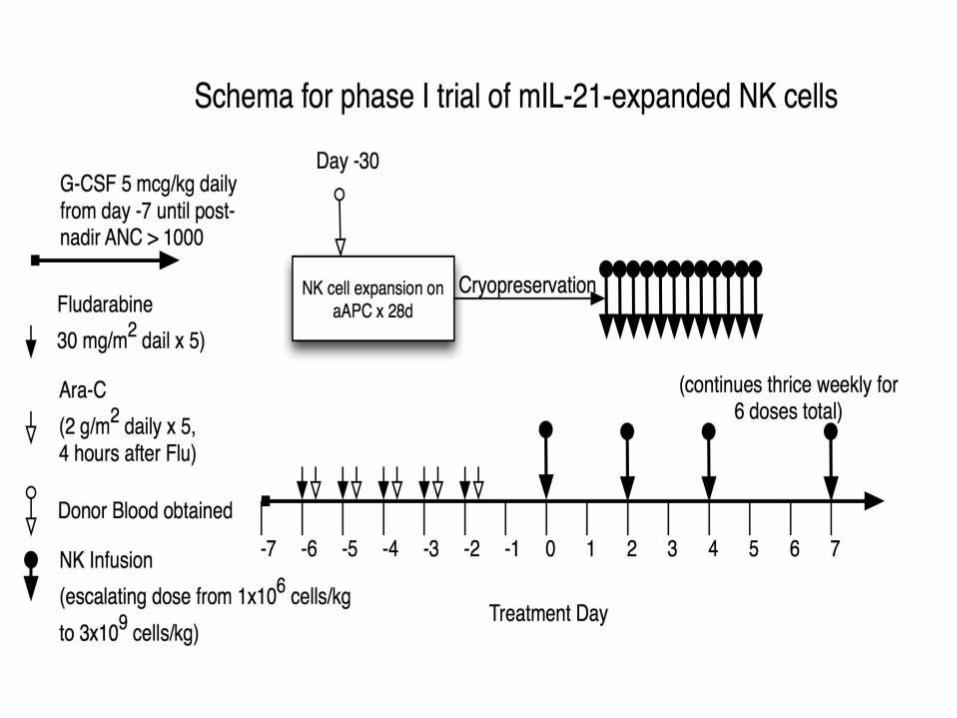
NK Adoptive Immunotherapy
W/WO HSCT
NK cell in vitro expansion
5-15% PBMC
in vitro expansion/activation
platform
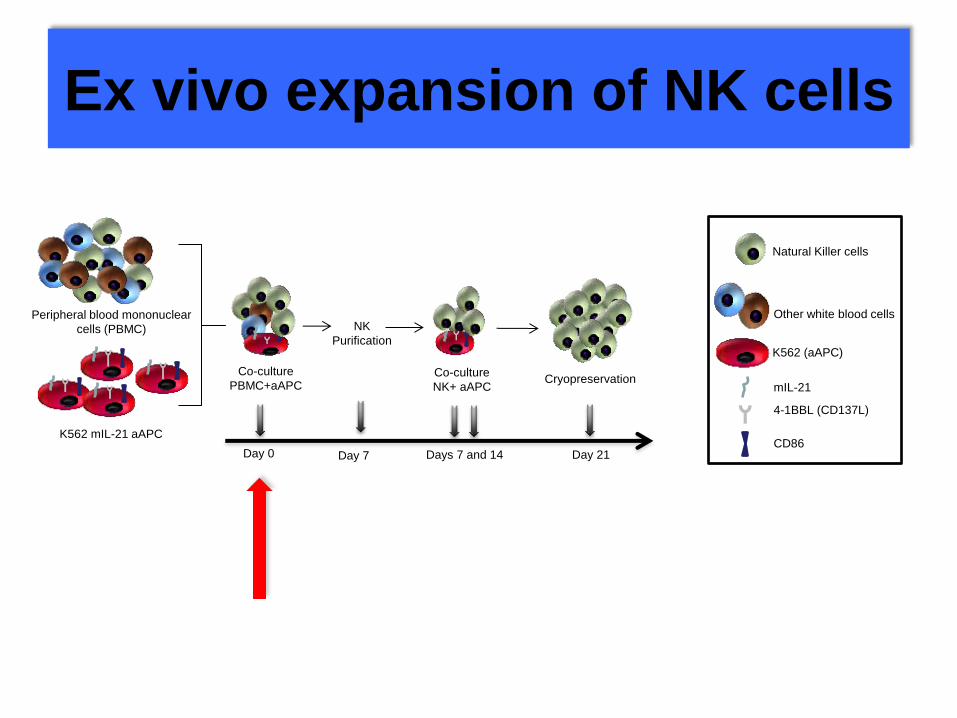
Ex vivo expansion of NK cells
Peripheral blood mononuclear
cells (PBMC)
K562 mIL-21 aAPC
Co-culture
PBMC+aAPC
NK
Purification
Co-culture
NK+ aAPC
Other white blood cells
Natural Killer cells
K562 (aAPC)
mIL-21
4-1BBL (CD137L)
CD86
Cryopreservation
Day 0 Day 7 Days 7 and 14 Day 21
Phase I adoptive immunotherapy
with in vitro expanded NK cell safety and feasibility
GMP facility – HCPA, Porto Alegre, Brazil
GPPG 10.0457
Clinicaltrials.gov in progress
INCLUSÃO Adultos:
LMA refratária
LMA alto risco, sem doador aparentado
LMA recidivada após TCTH
Crianças
LMA refratária
LMA recidiva após TMO
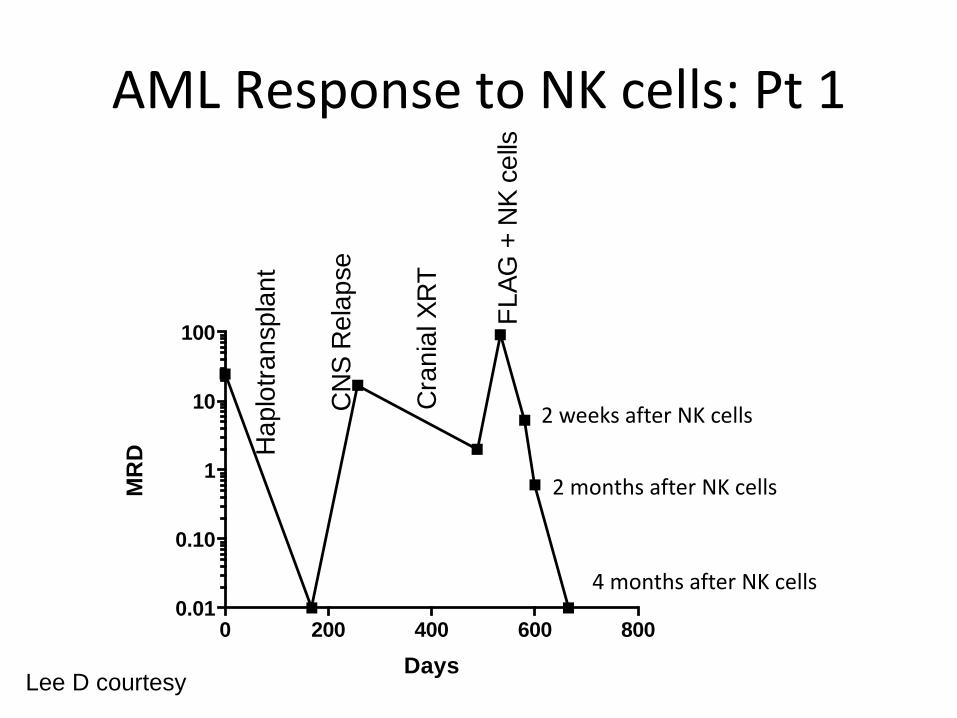
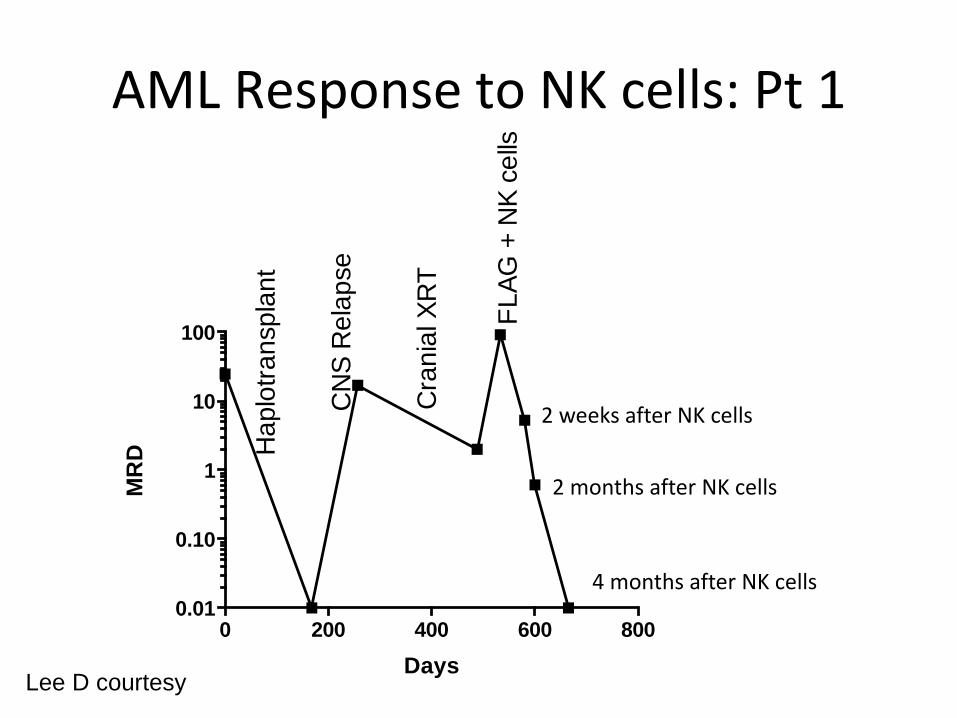
AML Response to NK cells: Pt 1
0 200 400 600 8000.01
0.10
1
10
100
Days
MR
D
CN
S R
ela
pse
Ha
plo
tra
nspla
nt
FL
AG
+ N
K c
ells
Cra
nia
l X
RT
2 weeks after NK cells
2 months after NK cells
4 months after NK cells
Lee D courtesy
CASO 01
Paciente feminina, 48 anos
20/12/2013
LEUCEMIA MIELÓIDE AGUDA MIELO-MONOCÍTICA
(FAB LMA- M4) – RISCO INTERMEDIÁRIO - Hemograma:
Hb 8d/dL, Leucócitos 26 mil (61 % blastos), Plaquetas: 56
mil
46, XX
SNC negativo
FTL3 negativo
CASO 01
31/12/2013
# Protocolo de indução 7+3 = RC (3.8% de blastos na MO)
C1 03/03/2014, C2 17/04/2014, C3 09/06/2014
# Encaminhada para avaliação de TCTH alogênico: não encontrado
doador compatível na família e no REREME, optado por fazer
Transplante Autólogo.
# BMO 13/04/2015 (de controle) : RC
22/04/2015
# Transplante de células tronco hematopoéticas autólogo em - BuCy
Infusão de 2,23 x 10^6 células CD 34/kg
BMO D + 30 25/05/2015: 7 % blastos.
CASO 01
Azacitidina SC C1 12/11/2015 –após 8 ciclos
18/07/2016: BMO 24% de blastos
Protocolo MEC por persistência de doença
Ciclo 1: 30/07/2016 - BMO 01/09/16: 2% de blastos
Ciclo 2: 15/09/17 – BMO 21/11/2016: 6% de blastos.
Persistência de pancitopenia no ambulatório dependente de transfusão de plaquetas
BMO 21/01/2017: medulograma com 21% de blastos
Protocolo Mitoxantrone, Cladribina e Citarabina 18/02/17
BMO 30/03/2017: 3% de blastos – intensa pencitopenia, dependente de transfusão
Diagnóstico de Aspergilose pulmonar e de SNC provável (alterações em Tc de tórax
compatíveis, RNM de crânio com lesão de 2, 2 cm em região frontal e galactmana sérico
e de Lavado Broncoalveolar positivo)
Tratamento com Micafungina e Voriconazol endovenoso com nível sérico de Vorico
adequado a partir do dia 26/05/2017.
Alta hospitalar com Voriconazol 400mg via oral 12/12 horas + CHAD + Plaquetas
CASO 01
02/06/2017
AMO:: 24% blastos
Cariótipo: 46 XY
AP: acentuadamente hipocelular
Protocolo de Pesquisa de terapia celular com infusão de células NK
expandidas para tratamento de Leucemia Mieloide Aguda recidivada/refratária.
Doadora: filha (haploidêntica)
1ª infusão 06/06/17 – Hb: 7,2g/dL, Leucócitos: 520, com 90 segmentados,
Plaquetas: 7.000
2ª infusão 08/06/17
3ª infusão 10/06/17
4ª infusão 12/06/17
5ª infusão 15/06/17
6ª infusão 17/06/17 - Hb: 8,4 g/dL, Leucócitos: 1170, Plaquetas: 10.000
Não apresentou nenhum evento adverso relacionado às infusões.
CASO 01
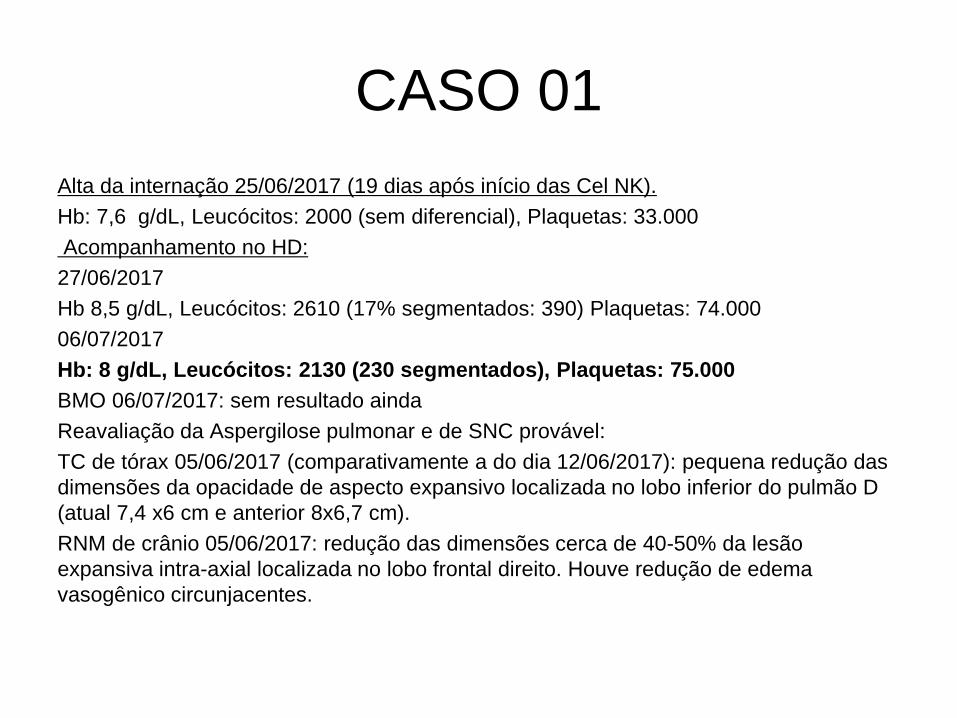
Alta da internação 25/06/2017 (19 dias após início das Cel NK).
Hb: 7,6 g/dL, Leucócitos: 2000 (sem diferencial), Plaquetas: 33.000
Acompanhamento no HD:
27/06/2017
Hb 8,5 g/dL, Leucócitos: 2610 (17% segmentados: 390) Plaquetas: 74.000
06/07/2017
Hb: 8 g/dL, Leucócitos: 2130 (230 segmentados), Plaquetas: 75.000
BMO 06/07/2017: sem resultado ainda
Reavaliação da Aspergilose pulmonar e de SNC provável:
TC de tórax 05/06/2017 (comparativamente a do dia 12/06/2017): pequena redução das
dimensões da opacidade de aspecto expansivo localizada no lobo inferior do pulmão D
(atual 7,4 x6 cm e anterior 8x6,7 cm).
RNM de crânio 05/06/2017: redução das dimensões cerca de 40-50% da lesão
expansiva intra-axial localizada no lobo frontal direito. Houve redução de edema
vasogênico circunjacentes.
CASO 01
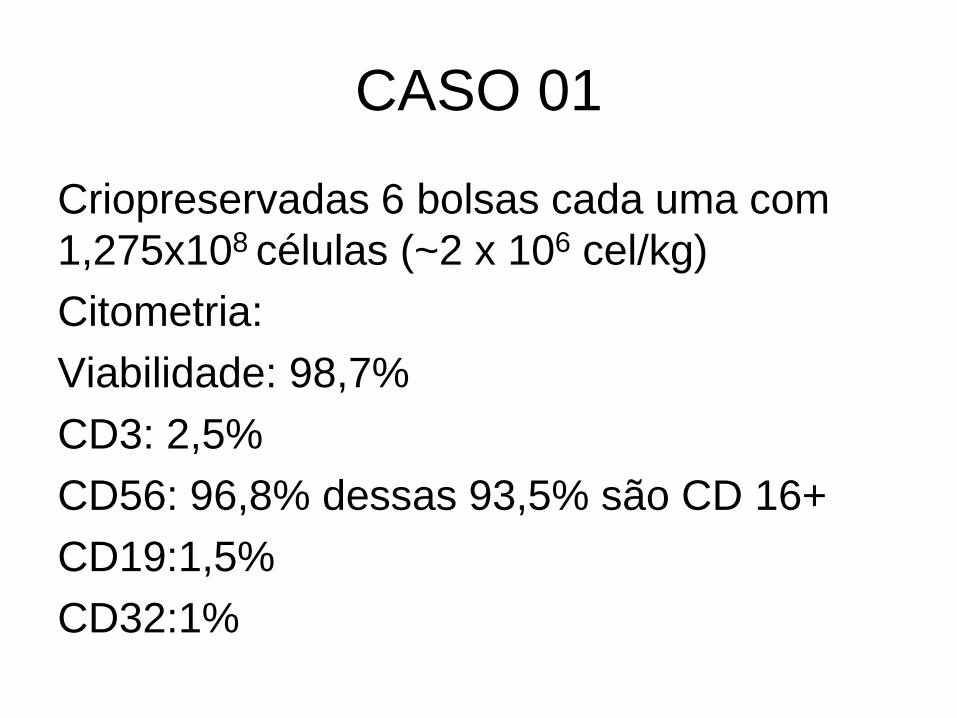
Criopreservadas 6 bolsas cada uma com
1,275x108 células (~2 x 106 cel/kg)
Citometria:
Viabilidade: 98,7%
CD3: 2,5%
CD56: 96,8% dessas 93,5% são CD 16+
CD19:1,5%
CD32:1%
00%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
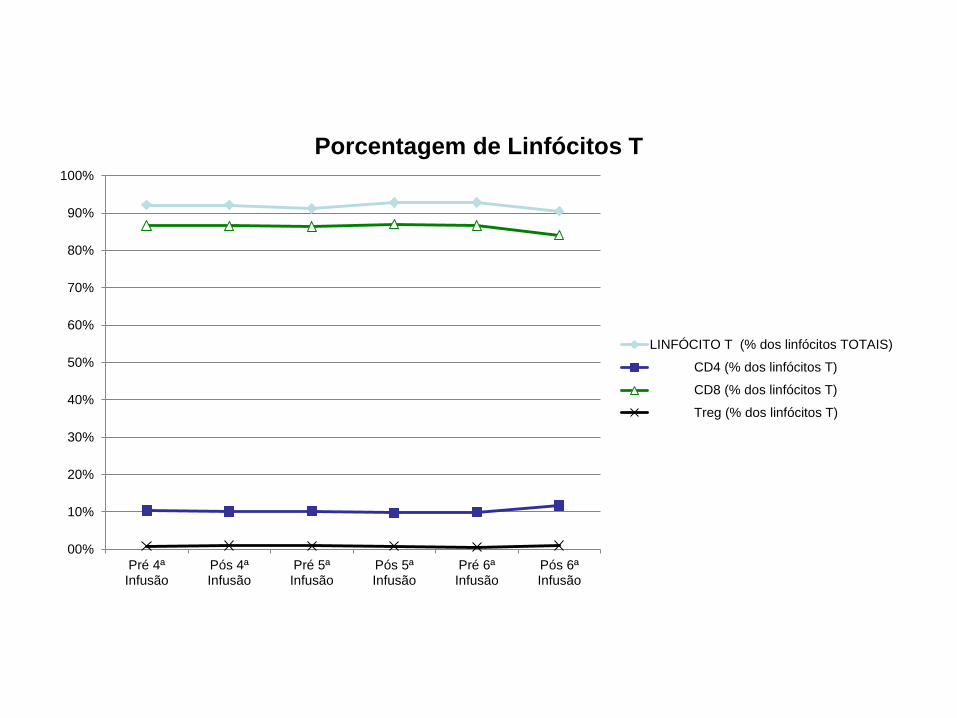
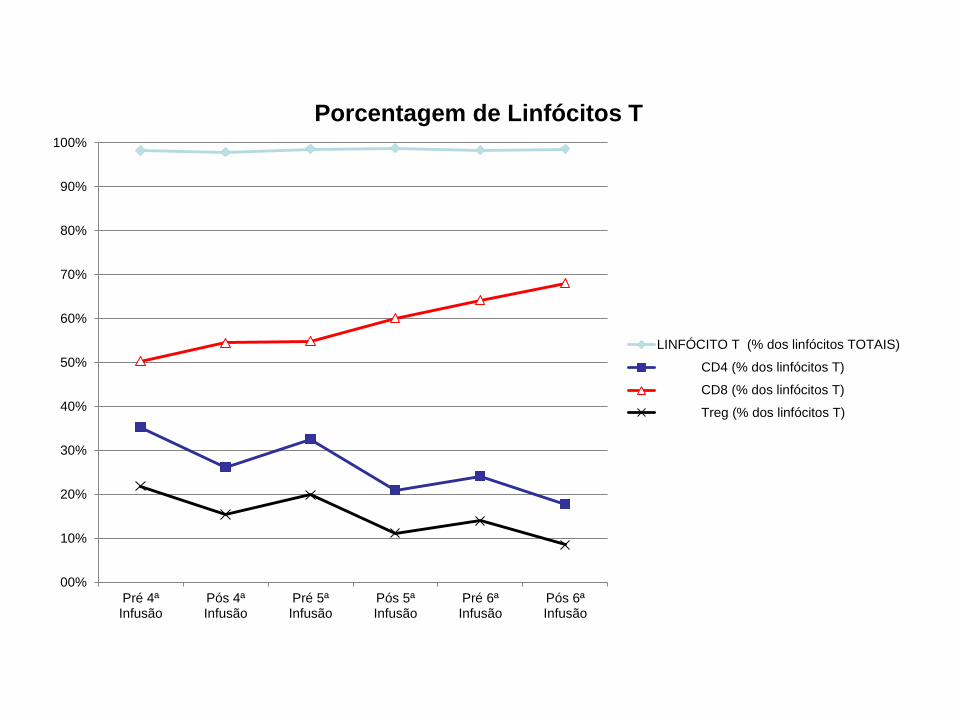
Pré 4ªInfusão
Pós 4ªInfusão
Pré 5ªInfusão
Pós 5ªInfusão
Pré 6ªInfusão
Pós 6ªInfusão
Porcentagem de Linfócitos T
LINFÓCITO T (% dos linfócitos TOTAIS)
CD4 (% dos linfócitos T)
CD8 (% dos linfócitos T)
Treg (% dos linfócitos T)
00%
01%
02%
03%
04%
05%
06%
07%
08%
09%
10%
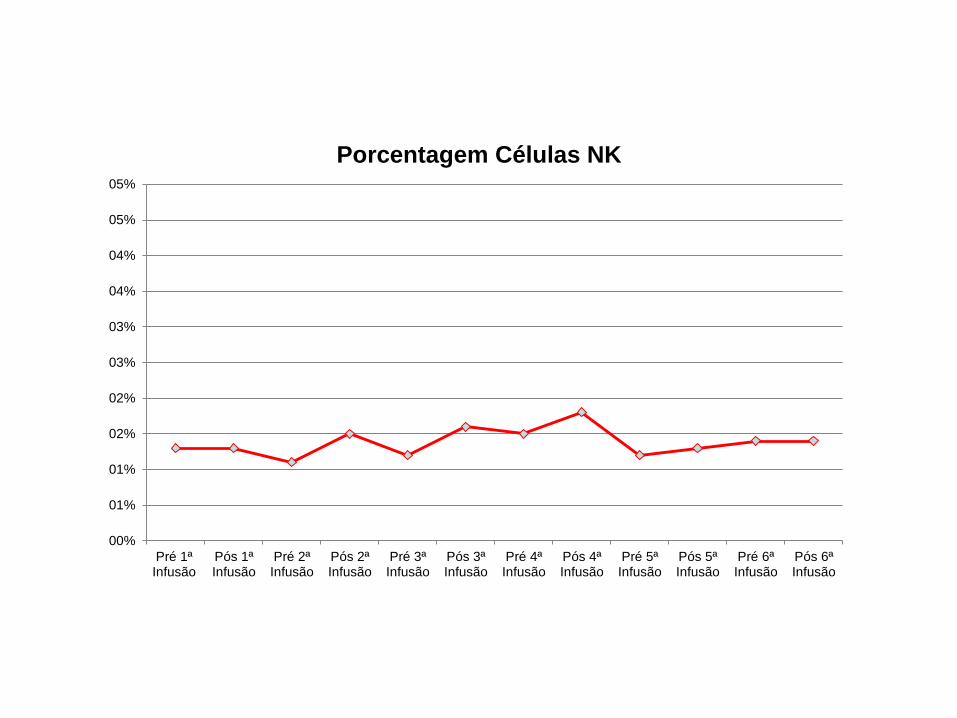
Pós 1ªInfusão
Pós24h
Pré 2ªInfusão
Pós 2ªInfusão
Pré 3ªInfusão
Pós 3ªInfusão
Pré 4ªInfusão
Pós 4ªInfusão
Pré 5ªInfusão
Pós 5ªInfusão
Pré 6ªInfusão
Pós 6ªInfusão
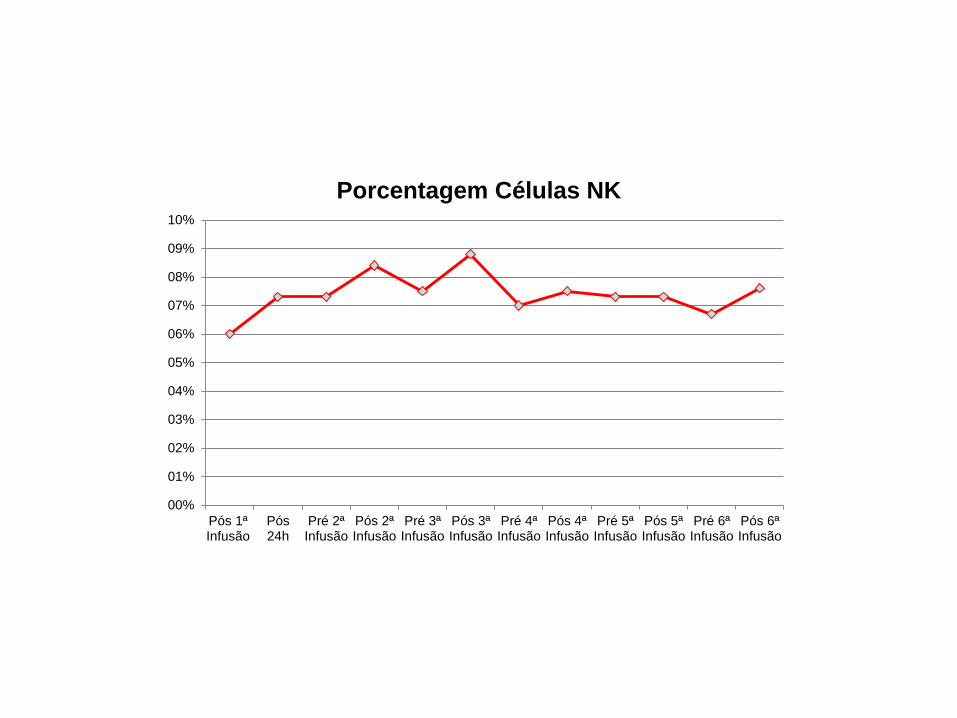
Porcentagem Células NK
00%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
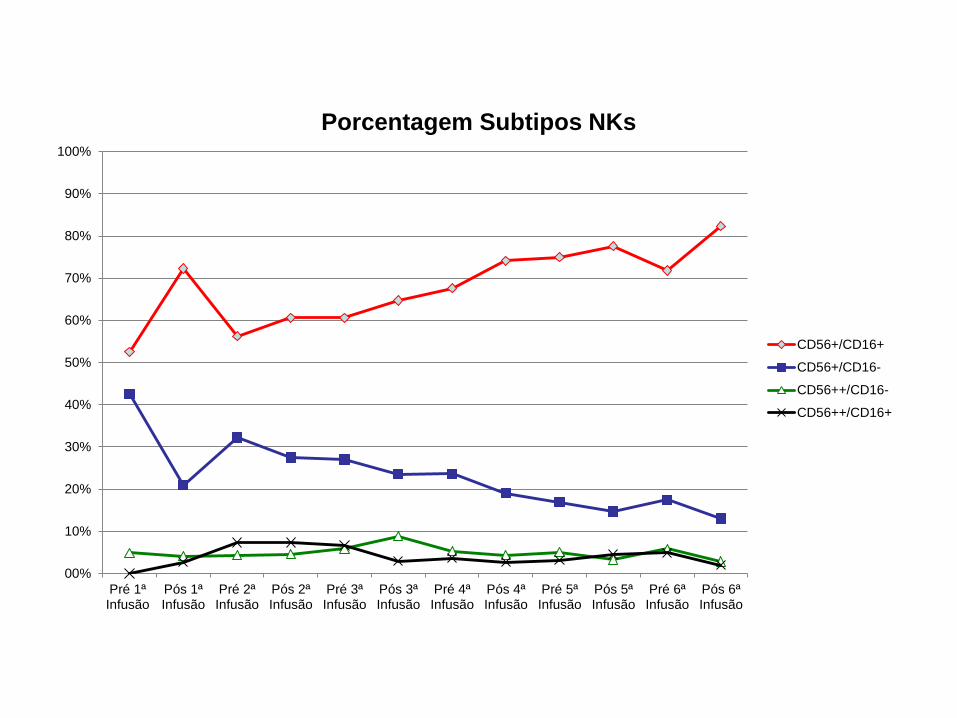
Pós 1ªInfusão
Pós24h
Pré 2ªInfusão
Pós 2ªInfusão
Pré 3ªInfusão
Pós 3ªInfusão
Pré 4ªInfusão
Pós 4ªInfusão
Pré 5ªInfusão
Pós 5ªInfusão
Pré 6ªInfusão
Pós 6ªInfusão
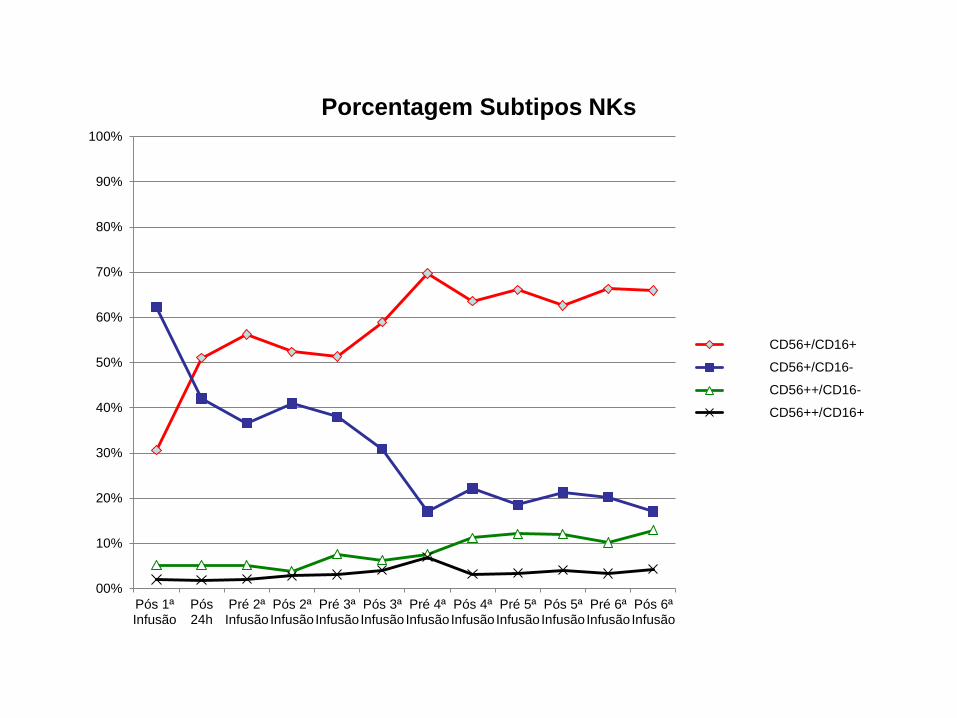
Porcentagem Subtipos NKs
CD56+/CD16+
CD56+/CD16-
CD56++/CD16-
CD56++/CD16+
CASO 02
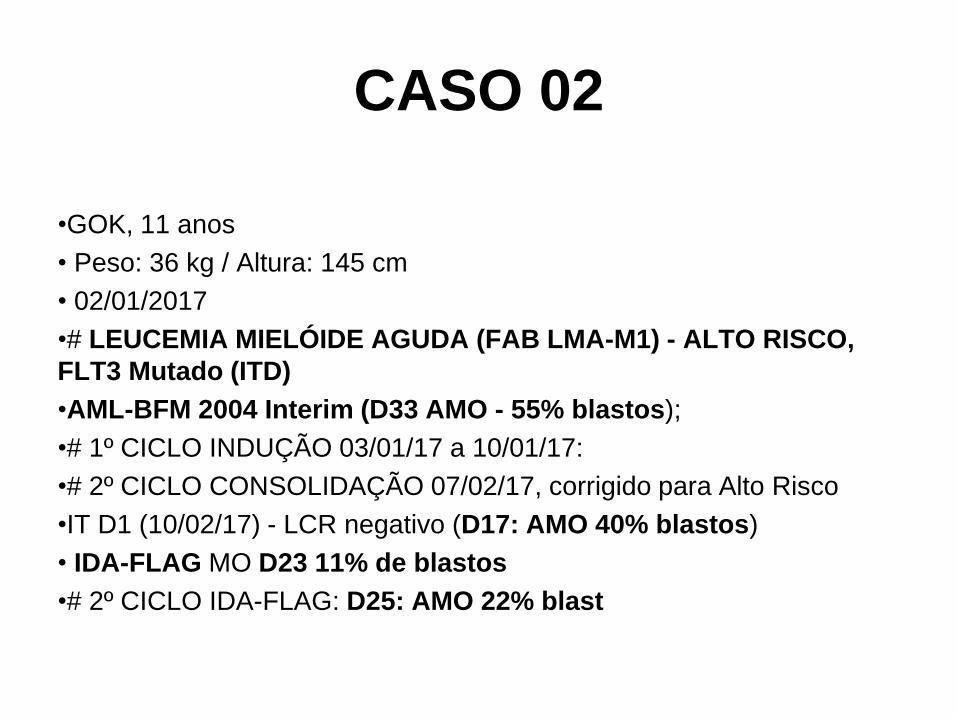
•GOK, 11 anos
• Peso: 36 kg / Altura: 145 cm
• 02/01/2017
•# LEUCEMIA MIELÓIDE AGUDA (FAB LMA-M1) - ALTO RISCO,
FLT3 Mutado (ITD)
•AML-BFM 2004 Interim (D33 AMO - 55% blastos);
•# 1º CICLO INDUÇÃO 03/01/17 a 10/01/17:
•# 2º CICLO CONSOLIDAÇÃO 07/02/17, corrigido para Alto Risco
•IT D1 (10/02/17) - LCR negativo (D17: AMO 40% blastos)
• IDA-FLAG MO D23 11% de blastos
•# 2º CICLO IDA-FLAG: D25: AMO 22% blast
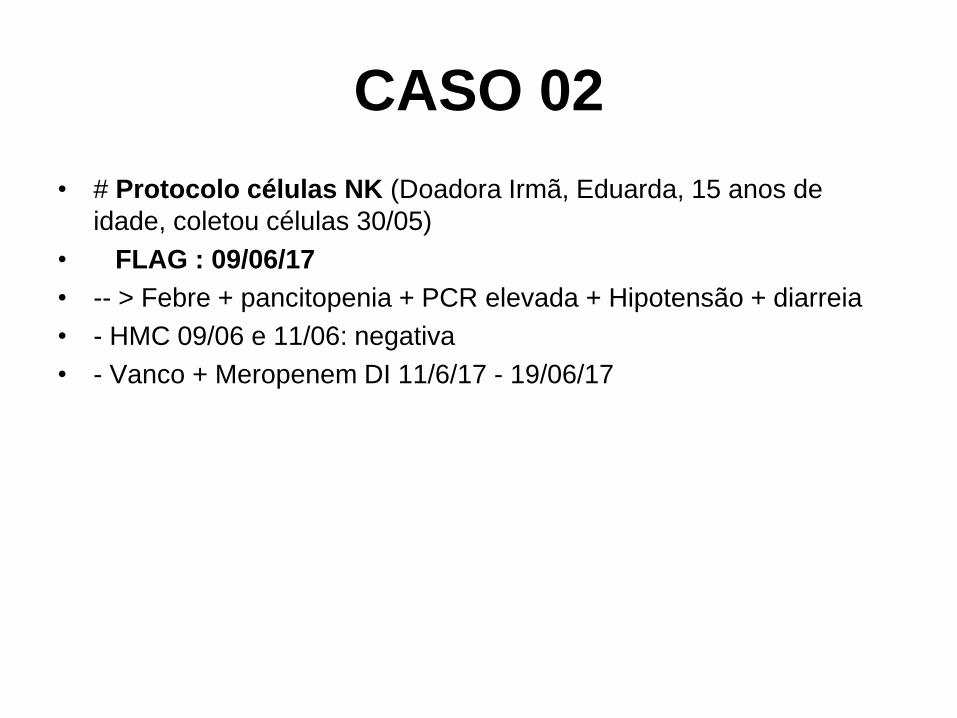
CASO 02
• # Protocolo células NK (Doadora Irmã, Eduarda, 15 anos de
idade, coletou células 30/05)
• FLAG : 09/06/17
• -- > Febre + pancitopenia + PCR elevada + Hipotensão + diarreia
• - HMC 09/06 e 11/06: negativa
• - Vanco + Meropenem DI 11/6/17 - 19/06/17
CASO 02
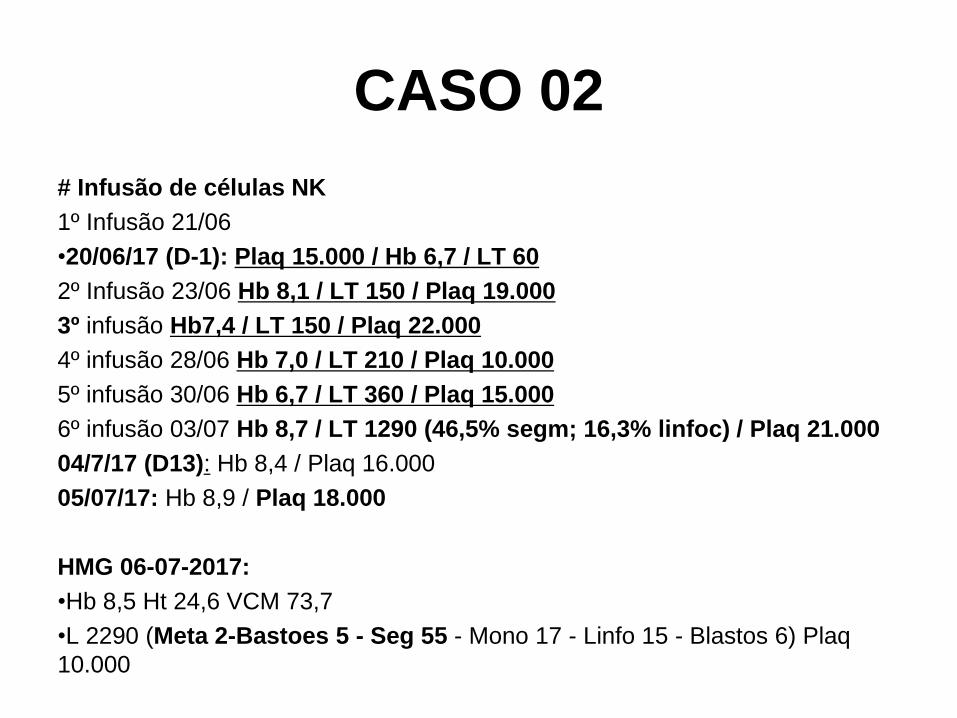
# Infusão de células NK
1º Infusão 21/06
•20/06/17 (D-1): Plaq 15.000 / Hb 6,7 / LT 60
2º Infusão 23/06 Hb 8,1 / LT 150 / Plaq 19.000
3º infusão Hb7,4 / LT 150 / Plaq 22.000
4º infusão 28/06 Hb 7,0 / LT 210 / Plaq 10.000
5º infusão 30/06 Hb 6,7 / LT 360 / Plaq 15.000
6º infusão 03/07 Hb 8,7 / LT 1290 (46,5% segm; 16,3% linfoc) / Plaq 21.000
04/7/17 (D13): Hb 8,4 / Plaq 16.000
05/07/17: Hb 8,9 / Plaq 18.000
HMG 06-07-2017:
•Hb 8,5 Ht 24,6 VCM 73,7
•L 2290 (Meta 2-Bastoes 5 - Seg 55 - Mono 17 - Linfo 15 - Blastos 6) Plaq
10.000
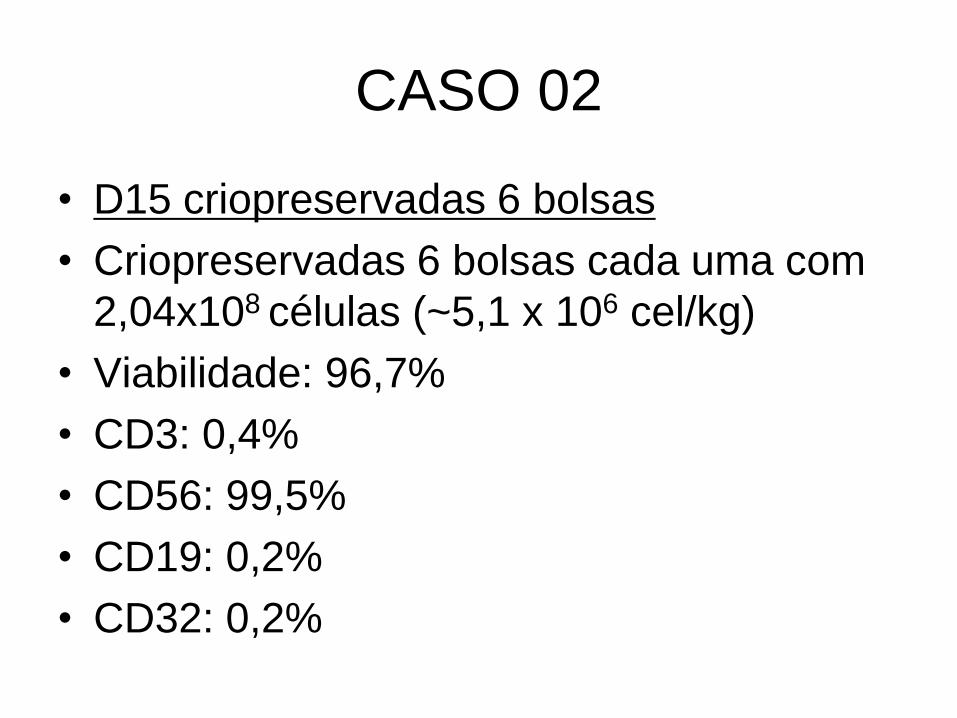
CASO 02
• D15 criopreservadas 6 bolsas
• Criopreservadas 6 bolsas cada uma com
2,04x108 células (~5,1 x 106 cel/kg)
• Viabilidade: 96,7%
• CD3: 0,4%
• CD56: 99,5%
• CD19: 0,2%
• CD32: 0,2%
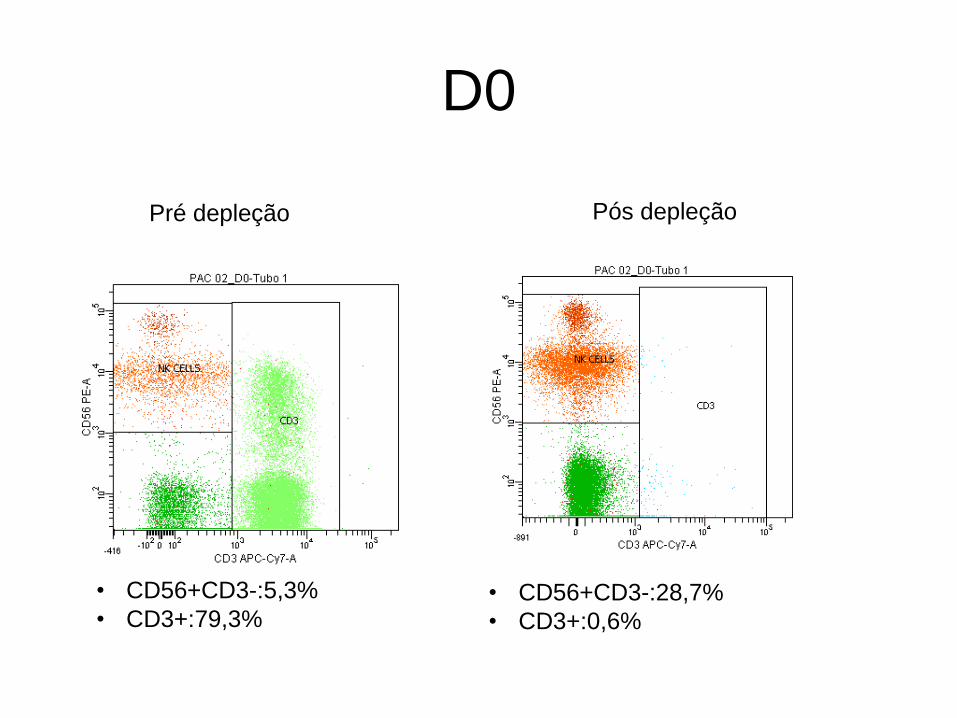
D0
Pré depleção Pós depleção
• CD56+CD3-:5,3%
• CD3+:79,3% • CD56+CD3-:28,7%
• CD3+:0,6%
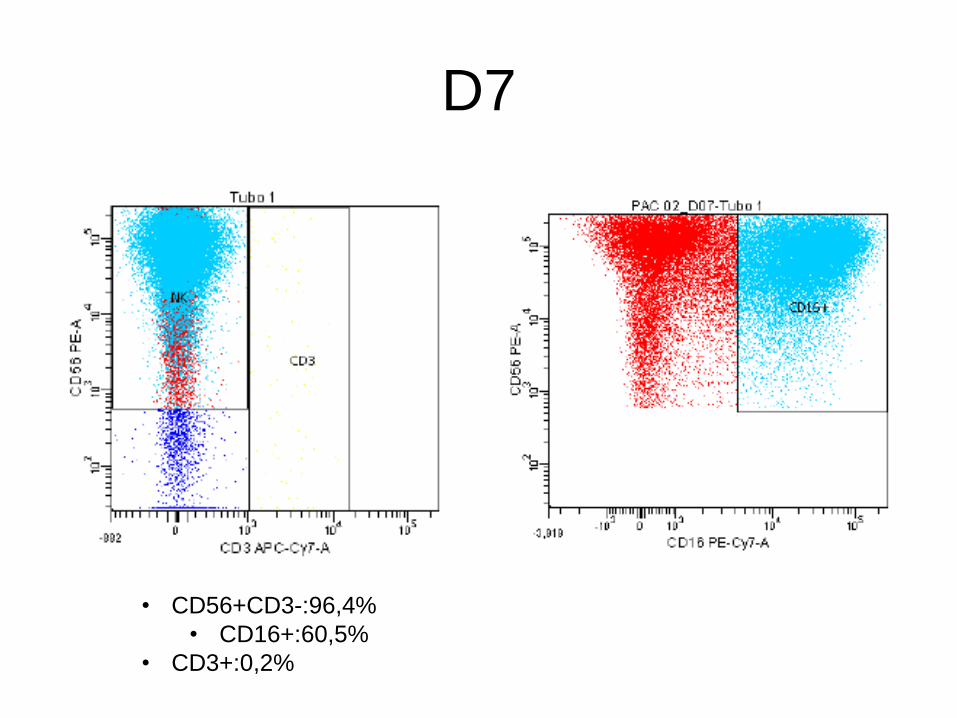
D7
• CD56+CD3-:96,4%
• CD16+:60,5%
• CD3+:0,2%
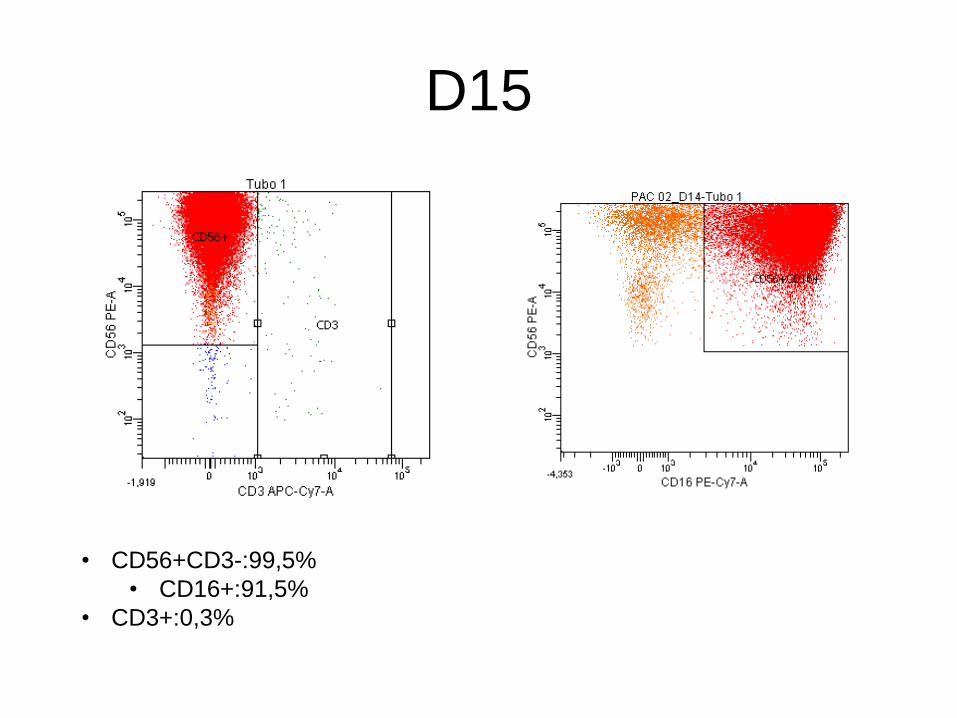
D15
• CD56+CD3-:99,5%
• CD16+:91,5%
• CD3+:0,3%
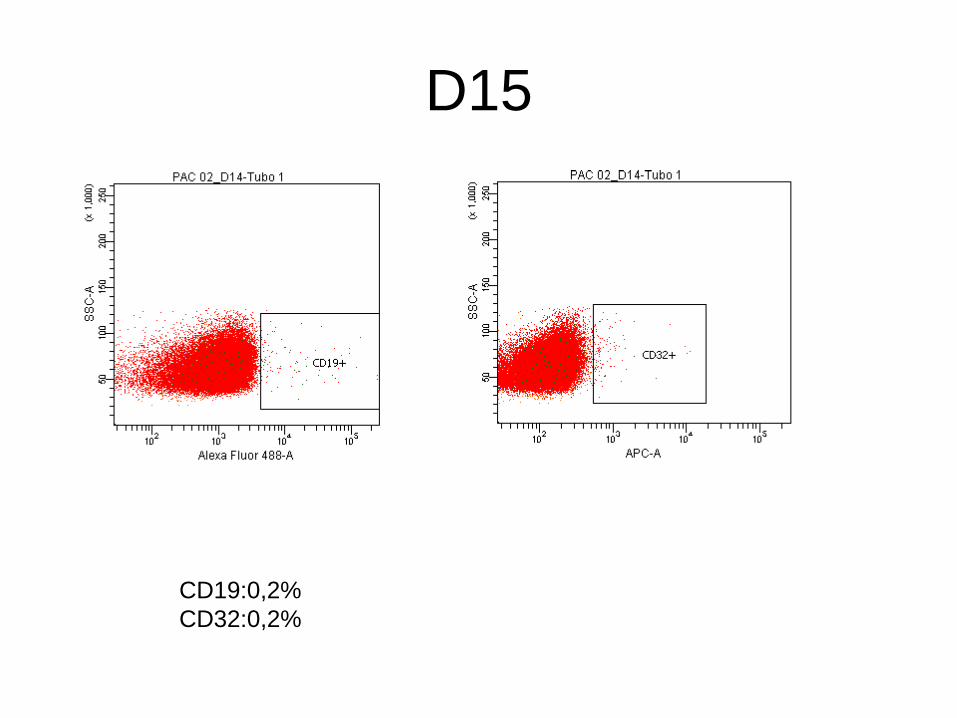
D15
CD19:0,2%
CD32:0,2%
00%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pré 4ªInfusão
Pós 4ªInfusão
Pré 5ªInfusão
Pós 5ªInfusão
Pré 6ªInfusão
Pós 6ªInfusão
Porcentagem de Linfócitos T
LINFÓCITO T (% dos linfócitos TOTAIS)
CD4 (% dos linfócitos T)
CD8 (% dos linfócitos T)
Treg (% dos linfócitos T)
00%
01%
01%
02%
02%
03%
03%
04%
04%
05%
05%
Pré 1ªInfusão
Pós 1ªInfusão
Pré 2ªInfusão
Pós 2ªInfusão
Pré 3ªInfusão
Pós 3ªInfusão
Pré 4ªInfusão
Pós 4ªInfusão
Pré 5ªInfusão
Pós 5ªInfusão
Pré 6ªInfusão
Pós 6ªInfusão
Porcentagem Células NK
00%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pré 1ªInfusão
Pós 1ªInfusão
Pré 2ªInfusão
Pós 2ªInfusão
Pré 3ªInfusão
Pós 3ªInfusão
Pré 4ªInfusão
Pós 4ªInfusão
Pré 5ªInfusão
Pós 5ªInfusão
Pré 6ªInfusão
Pós 6ªInfusão
Porcentagem Subtipos NKs
CD56+/CD16+
CD56+/CD16-
CD56++/CD16-
CD56++/CD16+
00%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
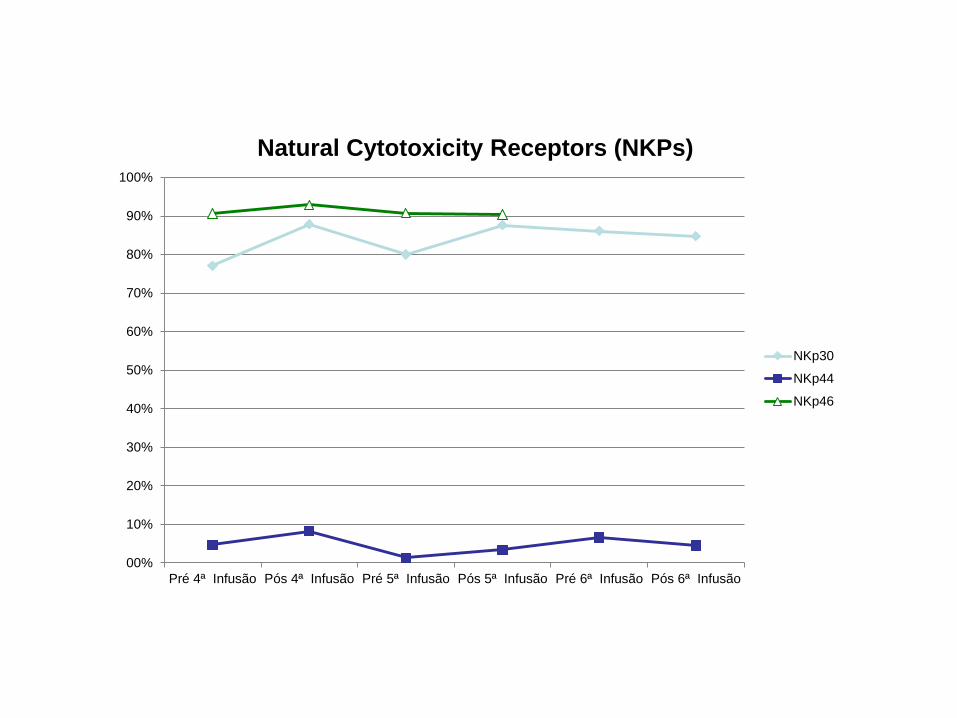
Pré 4ª Infusão Pós 4ª Infusão Pré 5ª Infusão Pós 5ª Infusão Pré 6ª Infusão Pós 6ª Infusão
Natural Cytotoxicity Receptors (NKPs)
NKp30
NKp44
NKp46
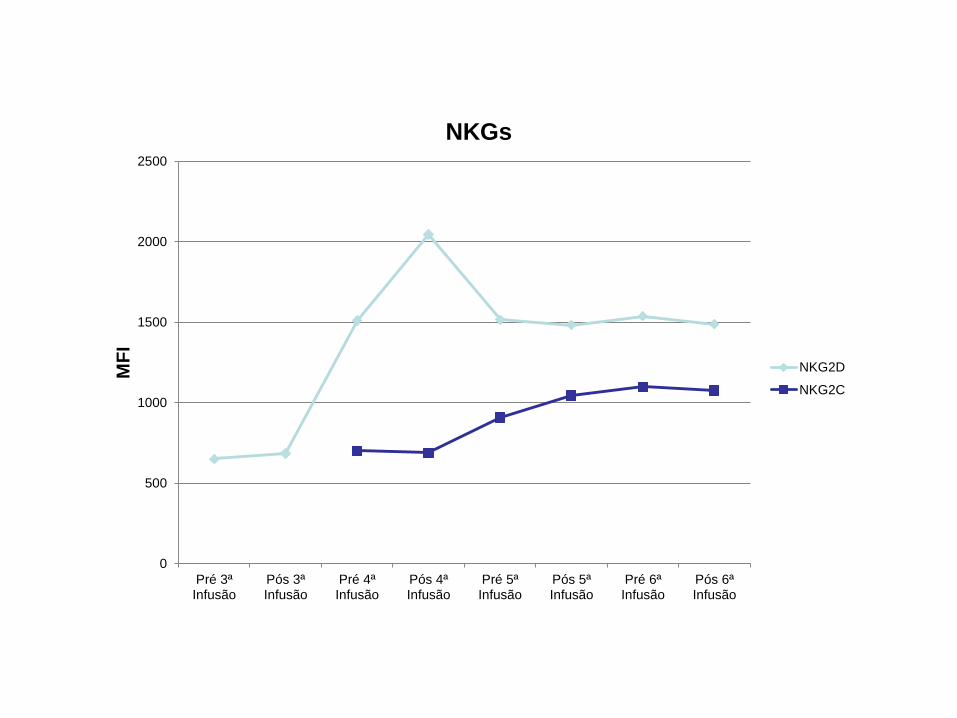
0
500
1000
1500
2000
2500
Pré 3ªInfusão
Pós 3ªInfusão
Pré 4ªInfusão
Pós 4ªInfusão
Pré 5ªInfusão
Pós 5ªInfusão
Pré 6ªInfusão
Pós 6ªInfusão
MF
I NKGs
NKG2D
NKG2C
AML Response to NK cells: Pt 1
0 200 400 600 8000.01
0.10
1
10
100
Days
MR
D
CN
S R
ela
pse
Ha
plo
tra
nspla
nt
FL
AG
+ N
K c
ells
Cra
nia
l X
RT
2 weeks after NK cells
2 months after NK cells
4 months after NK cells
Lee D courtesy


Equipe do TCTH
Best Lab People Ever!