Embed Size (px)
Citation preview

POSTGRAD MED. J. (1966), 42, 409
HORMONES AND METABOLISM IN PREGNANCY
A. KLOPPER, B.Sc., M.D., F.R.C.O.G. J. M. STOWERS, M.D, F.R.C.P. (Lond. & Ed.)I. MACGILLIVRAY, M.D., F.R.C.O.G. T. HELGASON, Cand. Med. ReykjavikA. C. TURNBULL, M.iD., F.R.C.O.G. K. J. DENNIS, M.B., Ch.B., F.R.C.S.(Ed.),
M.R.C.O.G.A. B. M. ANDERSON, M.D., D.Obst.R.C.O.G.
Department of Obstetrics and Gynaecology and the Maternity Hospital, Aberdeen.
THE marked changes in hormone productionin pregnancy are associated with changes inmetabolism and function. Much of the workwhich has been done and is being continuedin the Clinical Research Unit of this departmentis concerned with the changes in body com-position in normal and abnormal pregnancy andthe puerperium and in the uterine activity inla;bour. The earlier endocrine work had been
principally concerned wi,th the modification ofresearch methods of urinary hormone assayto make them suitable for large scale clinicaluse. The more recent and the projected endo-crine studies are being correlated as far aspossible with the metabolic changes occurringin pregnancy, labour and the puerperium. Thefollowing is an account of some of the hormoneand metabolic studies being carried out.
THE STEROID HORMONES IN PREGNANCYArnold Klopper
Evidence has been accumulating from manycentres which suggests that in late pregnancythe pregnanediol in the mother's urine is ofpurely placenital origin, resulting from the meta-bolic breakdown by the mother of progesteroneproduced in the placenta. On the other hand,oestriol is a combined foetal ,and placentalproduct, possibly formed in part from precur-sors produced in the foetal adrenals. It mightbe expected therefore that, while urinary preg-nanediol was purely a reflection of the functionof the placenta, the level of oestriol in themother's urine might give some indication ofthe state of affairs in the foetus. A series ofinvestigations has therefore been started with aview to examining the change in oestriol andpregnanediol output in such conditions as pre-eclampsia (Klopper, 1961), abortion (Klopperand Macnaughton, 1965), rhesus incompati-bility (Klopper and Stephenson, 1966) and re-tarded intra-uterine foetal growth (Klopper,1966). These studies have confirmed the viewthat oestriol assay is a valuable means of assess-ing the foetal state in a variety of obstetricdiseases and routine assays are now done ona considerable proportion of the patients ad-
mitted to the antenatal ward.It has become evident that the degree to
which oestriol output is affected is very muchdependent on the nature of the obstetric disease.In rhesus incompatibility, even in cases wherethe ibaby is born moribund, the oestriol excre-tion is generally within normal limits. Similarlyin diabetic pregnancy there appears to be nocorrelation betiween the maternal oest*riol excre-tion and the condition of ithe foetus. On theother hand in pre-ecl,ampsia there is a closecorrelation between oestriol excretion and theprogress of the disease so that iby serial assaysit is often possiable to tell when the life of thefoetus is in peril. In the more insidious condi-tions associated with retarded intra-uterinefoetal growth oestriol assay proved to be ofparticular value as there was often a close re-lationship between the oestriol level and theweight of the foetus with a tendency for oestrioloutput to decline to very low levels beforeintra-uterine death took place.These findings raise the interesting questionof what processes in the foetus are responsiblefor oestriol production and why some diseasesshould affect them and others not. Uterine
copyright. on June 16, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.489.409 on 1 July 1966. Dow
nloaded from

410 POSTGRADUATE MEDICAL JOURNAL July, 1966
blood flow may be of some impo;rtance but isunlikely to be the sole factor concerned. It ishoped that a careful categorisation of hormoneexcretion in a variety of conditions may givesome clue as to the relative importance of suchfactors as foetal oxygenation, maternal postureand activity, foetal liver and adrenal functionand the adtivity of the sulphatase and p-glu-curonidase enzyme systems responsible for ste-roid conjugation. Some studies on these lineshave been published (Klopper, 1964), and othersare in progress.One of the most important problems in the
study of the endocrinology of pregnancy todayis the elucidation of the function of the hor-mones. Much work is being done elsewhereon the role of oestrogens at the cellular andmolecular level. A clinical research unit suchas exists in Alberdeen is particularly suited tothe investigation of the physiological role ofthe hormones in such pregnancy phenomenaas the onset of laibour. At present, studies arebeing done comparing the changes in urinaryoestriol and pregnanediol output with altera-tions in myometrial contractility and in cervicalhistology. It may well be that in part the effectof oestrogens on the onset of labou;r is exer-cised by oestrogen-induced changes in the poly-merization of cervical Imucopolysaccharides.The relationship between oestrogen levels andground subs'tance generally has been little stu-died and we intend to devote increasing atten-tion to this aspect.
Urinary steroid assays have proved to be ofvalue in day-to-day clinical management of ob-stetric patients. They are less useful in funda-mental physiological studies because many pro-cesses which might alter the urinary level areinterposed between steroid production in thefoetoplacental unit and its final excretion inthe maternal urine. Urinary levels may not bea true reflection of the endocrine environmentdbtaining at the level of the foetus or themyometrium. It may well 'be that events suchas the onset of 'labour result from endocrinechanges engendered by the foeto-placental unitrather than from the maternal organism. If
this is the case it is essential to study thesechanges at the foeto-placental level. The bio-logical fluids which, one way or another, areavailable for study are: maternal peripheralblood, maternal uterine venous and retropla-cen'tal blood, liquor amnii and cord vein orartery foetal blood. It may well be that muchvaluable information albout the physiology ofpregnancy can be gained by studying the con-centration of the free and conjugated forms ofvarious steroid hormones in these biologicalfluids. The steroids we propose to concentrateon are oestriol, pregnanediol, progesterone anddehydroepiandrosterone, the raw material fromwhich the other steroids are made. Hithertothe methods for estimating the tiny amounts ofsteroids present in such biological fluids havebeen unsatisfactory. The advent of gas liquidchromatography has opened a new dimensionin steroid estimation. It appears very likely thatsatisfactory methods for the estimation of oes-triol and of pregnanediol in blood and liquoramnii will be evolved over the next few months.The applications of such methods ,both to phy-siological and to clinical problems are legion.A further aspect of the role of hormones in
pregnancy is their metabolic effects. In thliscontext studlies on the role of the oestrogens onwater balance have been published (Hyttenand Klopper, 1963). This led to an interest inthe relationship between renal function and hor-mone excretion in pregnancy (Klopper, 1964)and to an investigation, which is still continuing,of the effect of progesterone on sodium excre-tion by blocking the action of aldosterone onthe renal tubulles.The accumulation of fat which occurs in
pregnancy is very probalbly due to progesterone(Galleti and Klopper 1964).The metabolic changes of pregnancy appear
to be rapidly reversed after delivery. A studyof water and electrolyte balance during thepuerperium may therefore be of especial interestand the fact that such a study is being done inthe Department has been ,made .the occasion ofa coincidental analysis of 'hormone excretionduring the puerperium.
WATER AND ELECTROLYTE METABOLISM IN NORMAL AND ABNORMALPREGNANCYIan MacGillivrav
Most of tlhe hormonal changes occurring inpregnancy are concerned with the growth of thebaby and the changes in the maternal organs toaccommodate and provide for the developingfoetus. Because of the inaccessibility it is diffi-cult to measure with any accuracy the rate of
growth of the baby Ibut the response of themother to the 'hormonal changes and metabolicprocesses can often reflect the condition of thefoetus. Thus an assessment of such changes inthe mother ,might be expected to help in reduc-ing perinatal mortality and morbidity.
copyright. on June 16, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.489.409 on 1 July 1966. Dow
nloaded from

July, 1966 MacGILLIVRAY and Others: Hormones in Pregnancy 411
Water forms about half of the weight of non-pregnant females ,and changes in the water con-tent of the pregnant woman might ibe expectedas there is normally an increase in plasmavolume of about 1350 ml. ,(Hytten and Paintin,1963); a volume of liquor amnii of about 1000ml.; and twater forms about 80% of baby 'weight.An excess of water as evidenced by clinicaloedema is one of the signs of pre-eclamptictoxaemia and Hytten and Paintin 1(1963) haveshown that women wit'h a poor increase inplasma volume ,produce smaller 'babies; Hyttenhas suggested that deficient water retention isassociated with retarded foetal growth.
Although the total 'body water can bemeasured with some precision by tracer tech-niques using, for example, deuterium oxide(Hytten, Taggart, Billewicz and Jason, 1962)the compartmental distribution cannot be meas-ured with the same accuracy because the intra-cellular and extracellular fluids are in a constantstate of flux and there is no known substancewhich entirely equilibrates with the extracellularfluid yet does not penetrate into the cells.
In normal pregnancy near term there is aretention of about 6-7 litres of water as meas-ured iby deuterium oxide (Hutchinson, Plentland Taylor, 1954; Haley and Woodbury, 1956;McCartney, Pottinger and 'Harrod, 1959; Mac-Giilivray, 1961a). The "extracellular" space wasfound to be about 55% of the total body waterin 12 normal pregnant women (thiocyanatespace, 53.9%; bromide space, 56.2% sodiumspace 54%) by MacGillivray (1961a). This ishigher than in the non-pregnant female in whomthe range is f'ro!m 41 % thiiocynaite space ito 50.3 %bromide space (Schloerb, Friis-Hansen, Edel-man, Solomon and Moore, 1950; Edelman,Haley, Schloerb, Sheldon, Friis-Hansen, Stooland Moore, 1952; Gilder, Redo, Bar and Child,1954; Ikkos, Ljunggren, Luft asnd Sjogren, 1955).
In pre-eclamptic toxaemia there is a reten'tionof fluid greater than in normal pregnancy. Theresults for 12 normal primigraviidae near term,17 primigravidae with mild and 14 with severe
TABLE 1
TOTAL BODY WA'rER IN NORMAL PREGNANCYAND PRE-ECLAMPTIC TOXAEMIA (P.E.T.)
Normal Pregnancy 38.4 L.Mild P;E.T. with oedem,a 43.5 L.Mild P.E.T. witho,ut oedema 39.4 L.Severe P.E.T. with oedema 43.2 L.Severe P.E.T. without oedema 40.5 L.
pre-eclampsia are shown in Table 1 (fromMacGillivray, 1961b). In normal pregnancythere is an increase in the serum volume bothabsolute and as a proportion of the total fluidvolume. In pre-eclampsia there is a reductionin the serum volume compared with normalpregnancy iboth in absolute amount as well astin terms of total water. (Table 2).The "extracellular" space in pre-eclampsia
is slightly greater than in normal pregnancywhen measured as sodium space but the bromidespace is about the same. The "extracellular"space as a percentage of total body water is lessin pre-eclampsia than in normal pregnancy.(Table 3). The cause of the retention of fluid innormal pregnancy and in pre-eclampsia is stillobscure. The various hormones which have beensuggested are oestrogens, progesterone, adreno-cortical hormones, growth hormone and anti-diuretic hormone. One or several of these hor-mones may be involved in the retention of fluidin normal pregnancy and pre-eclampsia andthey may act by causing a primary water reten-tion or a primary sodium retention. The oedemawhich is common in pregnancy and pre-eclamp-sia may be caused or contributed to by someother factor such as the lowering of colloidosmotic pressure. It is widely accepted thatnutritional oedema occurs when the totalproteins fall Ibelow 5 per cent and the serumalbumin below 2.5 per cent. The total proteinsand serum albumin fall quite markedly innormal pregnancy (MacGillivray and Tovey,1957; Paaby, 1960; de Alvarez, Alfonso andSherrard, 1961) and still further in pre-eclamptictoxaemia.
TABLE 2SERUM VOLUME IN NORMAL PREGNANCY AND PRE-ECLAMPTIC TOXAEMIA (P.E.T.)
No. of Mean Serum Serum Volume Range andCases Volume L. % T.B. Water S.D.
Normal Pregnancy 9 4.1 10.6 (8.2-13.5)1.48
Mild P.E.T. 15 3.5 8.7 (6.4-10.6)1.13
Severe P.E.T. 11 3.4 8.2 (6.1-11.7)1.55
Non Pregnant* -2.4 7.5*Schloerb et al. 1950; Gilder et al. 1954; and Zak and Earle, 1957.
copyright. on June 16, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.489.409 on 1 July 1966. Dow
nloaded from

412 POSTGRADUATE MEDICAL JOURNAL July, 1966
TABLE 3
BROMIDE AND SODIUM SPACES RELATED TO TOTALBODY WATER IN NORMAL PREGNANCY AND
PRE-ECLAMPTIC TOXAEMIA (P.E.T.)
Br. Space Na. Space% T.B.W. % T.;B.W
Normal Pregnancy 56.2 (7) 54.9 (1Q2)Mild P.E.T. 49.4 (10) 52.1 (17)Severe P.E.T. 48.6 ;(7) 52.0 (12)
Number of cases in brackets
The part played by electrolyte changes in thecausation of the oedema of pre-eclampsiaremains controversial. Since Harding and vanWyck (19311), Strauss (1937) and Dieckmann(1950) showed that giving sodium chloride towomen with Ipregnancy toxaemia could causea marked aggravation of hypertension, oedemaand even eclampsia it has become popularamongst clinicians to consider that sodium reten-tion is the cause of the oedema of pre-eclampsiaand that elimination of sodium will improve thecondition. There is no convincing evidence thateither of these beliefs is correct.
Studies of total exchangeable electrolytes haveshown that in normal pregnancy there is anaverage increase of 773mEq. of sodium (Mac-Gillivray and Buchanan, 1958) whidh is similarto the amount calculated by Hytten and Leitch(1964) and the balance study of Hummel,Hunscher, Bates, Bonner and Macey (1937).The increase in exchangeable dhloride was 480mEq. and of potassium 170 mEq. (MacGillivray,
1961a). The amount of sodium and chlorideper litre of body water is about the same innormal pregnancy as in the non-pregnant femalebut in mild and severe pre-eclamptic toxaemiathere is less sodium and chloride 'per litre totalbody water. (Table 4).
MoCartney, Pottinger and Harrod (1959),Plentl and Gray (1959) and Mahran (1961)believe that there is more sodium than waterretained in pre-eclamptic toxaemia but Davey,O'Sullivan and Browne (1961) have confirmedthat the amount of water retained is relativelygreater than the amount of sodium.
It is difficult to reconcile these two opposingviews and it is of obvious importance to do soif the underlying hormonal change is to Ibeindentified. This is also of importance clinicallyin view of the potential dangers of giving sodiumdiuretics. Although they undoubtedly eliminatesodium they have little if any effect on the clini-cal course of the pre-eclamptic toxaemia (Mac-Gillivray, Hytten, Taggart and Buchanan, 1962)and could cause salt deficiency.As the range of values is wide (Table 4) it
may be that there is a fluctuation in the salt:water ratio and in the hormonal blood levels.For example, blood oestrogens which couldhave an effect on sodium retention have beenshown (Roy, Harkness 'and Kerr, 1963) to beeither higher or lower in women with pre-eclamp-tic toxaemia than in normal pregnancy. This israther similar to the situations of water intoxi-cation (Leaf, Bartter, Santos and Wrong, 1953)and hypernatraemic water depletion (Edelman,Leibman, O'Meara and Birkenfeld, 1958) inwhich total body sodium and plasma sodiummove in an opposite direction to the volume ofextracellular fluid. Bartter, Liddle, Duncan,
TABLE 4TOTAL EXCHANGEABLE SODIUM AND CHLORIDE PER LITRE TOTAL BODY WATER INNON-PREGNANT, NORMAL PREGNANT, AND PRE-ECLAMPTIC TOXAEMIA (P.iE.T.)
Na e/L. Range and Cl e/L. Range andT.B.W. S.D. T.B.W. S.D.
Normal Pregnancy 78.1 (70.5-90.8) 57.6 (46.1-68.3)5.74 7.82
Mild P.E.T. 72.8 (61.5-83.1) 50.9 (40.3-59.0)6.53 7.00
Severe P.E.T. 72.7 (61.5-79.0) 51.0 (35.8-65.2)5.95 10.86
Non Pregnant 77.6* __ - 57.0t -
*Edelman et al. (1952)tlkkos et al. (1955) and iMcMurrey et al. (1958)
copyright. on June 16, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.489.409 on 1 July 1966. Dow
nloaded from

July, 1966 MaoGIILLIVRAY and Others: Hormones in Pregnancy 413
Barber and Delea (1956) have shown thaturinary aldosterone is reduced in experimentalwater intoxication and increased in water depri-vation associated with high serum sodium. Theamount of circulating aldosterone is diminishedin pre-eclamptic toxaemia (Louros, Miras andFrangiadakis, 1960; De Bruine, 1960) as is theamount of renin, which through its conversionproduct angiotensin, stimulates the secretion ofaldosterone '(Brown, Davies, Lever and Robert-son, 1965).Brown and his co-workers (1965) however,
have shown that suppression of plasma renin in
patients with primary aldosteronism appears tobe the result of an increase in the 'body sodiumand of the volume of extracellular fluid. Thisadds to the difficulties of interpreting the resultsof studies of patients with pre-eclamptictoxaemia. It will probably ibe necessary to docombined studies of blood hormonal values(e.g. oestrogens and aldosterone) and total waterand electrolyte values in normal and abnormalpregnancies in order to determine whether thereis a primary water or sodium retention in pre-eclamptic toxaemia.
HORMONAL REGULATION OF UTERINE FUNCION IN PREGNANCY AND LABOURA. C. Turnbull and A. B. M. Anderson
The part played by hormones in the regula-tion of uterine function in pregnancy andlalbour is still uncertain.
Intra-amniotic injection of saline causes abor-tion or labour and ,it has been claimed(Bengtsson and Csapo, '1962) that the injectiondamages the placenta to such an extent that itsproduction of hormones is greatly reduced. The"progesterone iblock" is thus removed fromthe myometrium, and labour begins.
Turnbull and Anderson (1965) showed thatuterine activity began to increase 40-80 minutesafter the hypertonic saline injection and theintensity of contractions increased steadily untilabortion, reaching an laverage level of 95 mm.of ,mercury, twice as high as that in full-termlabour. Bengtsson and Csapo (1962) believethat such high ,pressures resulted from the com-plete withdrawal of the "progesterone block".Anderson, Turnbull and Murray (1966) havedemonstrated, however, that relationshipbetween myometrial tension and amniotic fluidpressure during a contraction depends on thesize of the uterus; the smaller the uterus, thehigher the pressure resulting from the samemyometrial tension. They calculated that themyometrial 'tension required to produce 95 mm.amniotic pressure with contractions at 20 weekswould produce contractions of "normal" inten-sity at full term-about 45 to 50 mm. ofmercury.
Furthermore, Klopper, Turnbull and Ander-son (1966) have shown that after the intra-amniotic injection of hypertonic saline, preg-nanedliol excretion is maintained at 85 per centof the mean pre-injection level until after theplacenta and foetus are aborted, indicatingcontinuing progesterone production by theplacenta. Oestriol excretion falls immediatelyafter the injection, due to intra-uterine foetal
death, although this is not essential to thesuccess of the method. Usually, however, theseabortions must occur despite a great excess ofprogesterone relative to oestrogen.
Christie, Anderson, Turnbull and Beck(1966) have shown that placental damage islimited to a thin sulbchorionic layer (amountingat most to 15 per cent of placental thickness)in which there is intervillous thrombosis andnecrosis of villi. In the remaining 85 per centor more of the placenta which was histologicallynormal, new im,munofluorescent techniquesindicated normal concentration of placentalgrowth hormone and of steroids within thesyncytiotrophoblast, in keeping with nortnalfunction.About 40 to 80 minutes after the hypertonic
saline injection a marked antiduresis develops(to a water load of 800 ml./hour). (Turnbulland Anderson, 1966; also unpublished data).The excess salt clearly ,begins to flow out intothe maternal circulation for increases in serumsodium concentration of up to 160 m.'Eq./litrehave been found, despite increases in serumvolume of up to 1400 ml. Serum osmolalityhas also risen as high as 296 mOsmol/Kg.These changes have varied in degree andduration but Turnbull and Anderson (1966)have drawn attention to the risks of thesechanges ,if the technique was to be used inpatients with cardiac or renal disease.
Increased uterine activity following intra-amniotic saline injection may be the result ofdirect effects of electrolytes on the myometriumrather than the result of any effect on placentalsteroid production.
Uterine contractility during 'pregnancy hasbeen recorded by Turnbull and Anderson(unpublished) and differences in activity de-monstrated in patients in whom labour was
copyright. on June 16, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.489.409 on 1 July 1966. Dow
nloaded from

414 POSTGRIADUATE MEDICAL JOURNAL July, 1966
premature, (up to 37 weeks), pre-term, (38-40weeks), and post-term, (41+weeks). Urinaryexcretion and blood levels of placental steroidsand their metabolites are Ibeing measured in thedifferent groups, in conjunction with Dr. A.Klopper.The changes in the connective tissue of the
cervix during pregnancy have been studied byordinary histological methods and by measur-I.,g hydroxyproline and hexosamine concentra-tion in biopsies of cervix with a view to relatingthe "resistance" of the cervix to the progress oflaJbour. The changes are part of a general effectof steroids on connective tissue in pregnancywhich has also been studied in other tissues.The changes in the cervix appear to be verymarked in younger women, (Turnlbull, 1962)but less in those over 30 years of age.
Considerable variation in uterine sensitivity tooxytocin can be demonstrated both by clinicalobservation and experiment in cases in whominduction of labour is required in late preg-nancy. Recognising this, Turnbull and Ander-son have developed an oxytocin "titration"for clinical use, usually for failed amniotomy,with dosage increasing from 1 mU./min. toas high as 128 mU./min. of oxytocin dependingon the activity of the uterus. Careful pre-liminary studies were made with constant in-fusion of oxytocin. The results with thistechnique in almost 500 cases of induction arenow 'being prepared for publication and in-dicate considerable improvement in the successrate over the previous regime for induction aswell as reduction in the inoidence of intra-uterine infection, Caesarean Section and foetalasnhvxia.
THE INTRAVENOUS GLUCOSE TOLERANCE TEST IN PREGNANCYJ. M. Stowers and T. Helgason.
The oral glucose tolerance test in pregnancyis relatively unsatisfactory because nausea andvomiting may be precipitated and there is atendency for delayed absorption causing the2-hour glucose value to be increased well abovethe fasting value, (Hagen, 1961) even in thosein whom there is no reason to suspect dialbetes.The correlation between oral and intravenousglucose tolerance tests is poor (Kaplan, 1961;Welsh, 1960) probably mainly because of thefactor of delayed intestinal albsorption of glu-cose. In pregnancy intravenous glucosetolerance has usually been described as beingno less than in the non-pregnant state (Burt,1954). In the work done (in Aberdeen thisconclusion has been accepted and the samestandards of interpretation have been applied inthe pregnant as in the non-pregnant. Incalculating results the "Increment Index"(Duncan, 1956), based on increments of theblood sugar above the fasting level, has beenused in preference to the absolute or K Index,which is derived from the absolute iblood sugarvalues. The theoretical basis for the IncrementIndex seems to be superior to that of theabsolute index (,Medley, 1965), and the Incre-ment Index, but not the absolute index, isindependent of the amount of glucose injected.Hepain is used to inhiabit venous ihrormbosisand the test is done after the subject has re-mained quietly at rest for at least twentyminutes. The present series is the largestreported of the results of intravenous glucosetesting in pregnancy and the puerperium. 720subjects were tested over a four-year period.
Of the 720, 99 proved to be diabetic, 119probably diabetic and 502 normal (70%). Thereasons for the tests were various, but thecommonest was the finding of glycosuria whichoccurred in 70% of the whole series. Whenglycosuria was the only indication for the testin 233 subjects 27.2% had abnormal glucosetolerance and in 10.6% the result was definitelydiabetic. Those already known to be diabetichave been excluded from consideration.The most significant indication for doing the
intravenous glucose tolerance test was the pre-vious birth of a baby weighing 10 lb. (4.5 Kg.)or more. This was the reason for the test in156 of the 720 suibjects. 35% of those provedto Ibe dialbetic had had such a heavy baby,whereas ,the figure was 19.2% for the probablediabetics and 19.7% of those shown to havenormal i.v. glucose tolerance. Obesity, definedas at least 2st. above the Kemsley (Kemsley,1951-52) standard weight allowing for thestage of pregnancy, was found in 29.7%of the 99 diabetics, 27.5% of the 119 probablediabetics and in only 14.7% of the normals diag-nosed during pregnancy or the puerperium.Multilparity, defined by seven or more preg-nancies carried to at least 28 weeks occurredin 5.1% of the diabetics, 4.2% of ithe Iprobablediabetics and in only 2.4% of 'the normals.Abortions occurred in 26.5% of the diabetics,21.6% of the probable diabetics and 16.7%of the normals. The significance of variousco-existing indications for glucose testing hasbeen analysed in Table 5. It is noteworthy thatonly 50% had a normal intravenous glucose
copyright. on June 16, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.489.409 on 1 July 1966. Dow
nloaded from

July, 1966 MacGiLLIVRAY and Others: Hormones in Pregnancy 415TABLE 5
SIGNIFICANCE OF VARIOUS COMBINATIONS OF INDICATIONS FOR I. V. GLUCOSE TESTINGTotal Diabetic Probable Normal
% Diabetic%
Glycosuria alone 233 10.6 16.6 728Glycosuria + baby of 10lb.(4.5 Kg.) or more 51 21.5 17,8 61Glycosuria + obesity(2 st. or 12.7 Kg. aboveKemsley Standard) 80 22.5 20 57.5Big baby + obesity+/- glycosuria 44 31.8 18.2 50
TABE 6IN PREGNANCY POST-PARTUM
ProbableNo. Diabetics Diabetics Normal
Diabetics 37 9 6 22 (60%)Probable Diabetics 61 15 4 42 (69%)
tolerance when the mother was obese and hadhad a 10 lb. (4.5 Kg.) baby.The intravenous glucose tolerance test results
did not correlate significantly with positivefamily history of diabetes mellitus, a history ofstillbirths, neo-natal deaths or of foetalalbnormality. Hydramnios is difficult to assessobjectively and was seldom an indication forintravenous glucose testing. The diabetic grouphad a mean duration of pregnancy of 38 weeks,the probable diabetics of 39 weeks and thenormals of 40.1 weeks. Allowing for the differ-ences in the gestational period the mean babyweight was 40% or more above the normal
mean (equivalent to 10 lb. or more at 40weeks) in 13.1% of the diabetics, 10.6% ofthe probable diabetics and 3.7% of the normals.Sixty iper cent of the diabetics diagnosed duringpregnancy had a normal i.v. glucose tolerancein the puerperium. In the series of probablediabetics 69% became normal post-partum but25% regressed to the diabetic state. The resultsof a comparison of postpartum intravenous itstswith those performed during pregnancy arepresented in Table 6 which indicates -that intra-venous glucose intolerance demonstrated for thefirst time in pregnancy frequently ,persists andmay indeed progress post-partum.
CHANGES IN THYROID FUNCTION AND IODINE METABOLISM DURINGPREGNANCYA. C. Turnbull
It is generally agreed that abnormal functionof the thyroid gland during pregnancy maypredispose to complications such as abortionbut before such dysfunction can be recognisedthe physiological changes in thyroid functionduring pregnancy have to be understood.
Visible and palpable enlargement of thethyroid gland occurred in 70% of 184 pregnantwomen in Aberdeen and in 37% of 116 non-pregnant controls of similar age and socialstatus from the same area (Aboul-Khair, Crooks,Turnsbull and Hytten, 1964). The distribution ofgoitre in pregnancy was not influenced by mater-
nal age, parity and stage of gestation.Serial studies using the short lived isotope132I were made in 13 women at the 12th, 16th,
24th, 3r2nd and 36th weeks of pregnancy and inthe 2nd, 6th and 12th weeks post-partum.(Aboul-Khair, Crooks, Turnbull and Hytten,1964). Renal clearance of iodine increased earlyin pregnancy to a level twice that normallyfound and this was associated with a lowplasma inorganic iodine (even allowing fordilution by the increased serum volume whichwas also narrowed). Thyroid clearance rateof iodine increased to about three times normal
copyright. on June 16, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.489.409 on 1 July 1966. Dow
nloaded from

416 POSTGRADUATE .MEDICAL JOURNAL July, 1966
but absolute uptake of iodine remained withinthe euthyroid range. These changes were foundbefore the 12th week, ,persisted until term andreturned to normal levels by the 6th weekpost-partum.
Pregnancy therefore results in an iodine de-ficiency state, partly due to a high renalclearance of iodine, and the thyroid gland asa compensating mechanism, apparently, clearsmore plasma of its iodine to produce a normalamount of thyroid hormone and in doing so,increases in size.The same technique has been used to study
iodine metabolism in cases of abortion andhalbitual albortion, premature labour, "placentaldysfunction", pre-eclampsia and "other hyper-tension" in pregnancy. (Aboul-Khair, Crooks,Turnbull and Turnbull, 1966). There is someevidence of reduced thyroid function in habitualabortion and in premature labour, while inpre-eclampsia the renal clearance of iodine isat normal non-pregnant levels while in "otherhypertensives" it is almost normal for preg-nancy. These differences could be explainedby reduction in renal blood flow and GFR inpre-eclampsia. In some cases where small babies
were born at term, thyroid function wasdiminished.
In cases where therapeutic termination ofpregnancy was ,performed ,by 'abdominalhysterotomy, the development of foetal thyroidfunction was studied following 131.1 administra-tion to the mother. These studies also enabledestimations to be made of the radiation doseto the foetal thyroid and gonads of 131I or1321 to the mother. (Alboul-Khair, Buchanan,Crooks and Turnbull, 1965).The foetal thyroid began to trap iodine about
the 13'th week of gestation and this function in-creased with age up to the 23rd week. How-ever, the gland did not trap iodine effectivelyduring this 'period and the estimated biologicalhalf life of 131!I in the foetal thyroid between13 and 19 weeks gestation was approximately16 to 28 hours compared with 1500 hours forthe normal thyroid gland.
Because of this, together with the rapid renalclearance of iodine by the mother, 5,uc, 131I and132I causes less irradiation to the foetal gonadsthan that due to natural radiation for one year.Irradiation to the ifoetal thyroid exceeds thatfor natural sources only after 17 weeks gesta-tionr in the case of 1321[.
METABOLIC CHANGES IN THE PUERPERIUMK. J. Dennis
It is now generally accepted that, both forpurposes of clinical investigation of patients,and for physiological studies of normal andabnormal pregnancy states, the criteria ofnormality applied to the non-pregnant femaleare not necessarily valid. The erythrocytesedimentation rate can be taken as an exampleof this. In late pregnancy, the rate can be ashigh as 100 mm. in the ,first hour (Furuhjelm,1956). This is probably associated with changesin the concentration and molecular shape ofvarious plasma proteins. Failure to make allow-ances for changes in body composition andfunction can lead to errors in the interpretationof clinical signs such as oedema. Such failureis even more likely to lead to the wrong sig-nificance being attached to the results of bio-chemical estimations.Our understanding of the control of the many
pregnancy changes is very limited. Mostworkers assume that changes in the endocrineenvironment are responsible. Although suchhormonal changes have also been extensivelystudied the relation ibetween endocrine functionand, for example, increases in plasma volumeare not yet understood; though the report byHervey and Hervey (1964) suggesting an asso-
ciation between fat storage and progesteronelevels is of great interest.At the delivery of the baby and of the
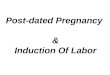
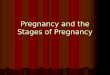
placenta, the now no longer pregnant womanis in a unique situation. All the adaptations topregnancy have fulfilled their functions andare suddenly redundant. Moreover, a potentendocrine unit, the placenta, whose hormonesappear to be to a large extent modified byorgans within the baby ,(Diczfalusy, Cassmer,Alonso and De Miguel, 1961) has ceased pro-duction. A study of the return to the non-pregnant physiological state of certain bodyfunctions during the puerperium was under-taken to ascertain how accurately the pregnancyunwinding process mirrors in !magnitude themore gradual build-up in lpregnancy. The firstparameter stud!ied was body weight. ('Dennisand Bytheway, 1965). Figures 1 and 2 (takenfrom their paper) show that, on average, inprimiparae who 'had not shown any oedemain late pregnancy, and in almost all parouspatients, there is a period of 3 days duringwhich body weight rises by up to as much as3-4 pounds in individual cases. As a rule onthe 4th day weight 'begins to fall. This fall isquite rapid over the next 3 days, and then
copyright. on June 16, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.489.409 on 1 July 1966. Dow
nloaded from

417POSTGRADUATE MEDICAL JOURNAL
107 Priniiparae 1 71 Multiparae
- None
---- - Ankles onlyMO- Generalised
1 2 3 4 a 6 1 2 3 4 5 6Days after delivery Days after delivery
FIG. 1- Body weight changes in the puerperium by oedema groups-178 normal subjects not givenStilboestrol.
52 Primiparae 86 Multiparae
,- .0"
.s~~~~.V
n q "1- 4i
-11--.WOOI- .49 -%~~~44
Oedema in pregnancy
None
Ankles only- - - -.- Generalised
.-
1 2 3 4 5 6 1 2 3 4 5 6Days after delivery Days after delivery
FIG. 2.- Body weigt changes in the puerperium by oedema groups-138 normal subjects givenStilboestrol.
July, 1966
1
laC:0 -1
a0ba
A -30
X -1bDa0bD
9:-3
0
.- mkkr-I%tl
1%
copyright. on June 16, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.489.409 on 1 July 1966. Dow
nloaded from

418 POSTGRADUATE MEDICAL JOURNAL July, 1966
.- tt* * * * * t~~ -,* Constant lvel of dailytotal water intake
1600
~~~~~ml. . **| | ||~~~~~I Water lost in urine8QO00 milk and lochia
400-
122
120lb Body weightlb. \
2 3 4 5 6 7 8 9 10
Day of puerperium
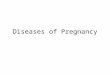
FIG. 3- Weight change and partial water ,balance during the puerperium in a normal primipara.
becomes much more gradual. In approximately40 per cent of the primiparae oedema had beennoted in late pregnancy. In these, on average,the initial weight gain did not occur;indeed, especially in those women, whereoedema in late pregnancy had not been con-fined to feet and legs, weight loss set in assoon as they were delivered. This was also thepattern in a separate group of pre-eclampticwomen.As rapid weight gains and losses from day-to-
day are usually accounted for by changes ining down or mobilisation of stores, anbody water content rather than (by sudden lay-experiment labelled a "partial water balance"was devised to obtain confirmation that wateris held in the body for ithe first 3 days post-partum. Fig. 3 shows the results of one suchexperiment which tends to confirm this hypo-thesis. We are also able to show that theadministration of the synthetic "oestrogen"stilboestrol for the inhibition of lactation tendsto increase the amount of gain in body weightimmediately after delivery, and to reduce the
rate of weight loss thereafter. This constitutesa situation in which an oestrogen has beenshown to cause water retention in the human,a fact commonly assumed, largely on the basisof animal experiment. Experiments are now inprogress to investigate the endocrine back-ground of metabolic changes in the puerperium.Body weight tends to stabilise about 10 weeks
after delivery. At this time there is still apositive balance of about 2.25 Kg. comparedwith the calculated pre-pregnancy weight. Thisbalance is, on average, 0.7 Kg. less in womenwho have continued to breast feed their babiesthan in those who have not lactated, or havelactated for a short period only.The water retention occurring in the early
puerperium, 'however brought about, is alsoassociated with certain changes in the concent-ration of blood constituents. For example, dailyestimations of the haemoglobin concentration ofperipheral venous Iblood in the puerperium showa rise from the late pregnancy level on the firstday, followed by a sharp fall to a minimum levelon the 4th and 5th days. This is followed bya rapid spontaneous rise. The peripheral venous
copyright. on June 16, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.489.409 on 1 July 1966. Dow
nloaded from

July, 1966 MacGILLIVRAY and Others: Hormones in Pregnancy 419
haematocrit behaves in a similar manner. Asthe mean corpuscular haemoglobin concentra-tion remains constant throughout these changes,they were thought to Ibe due principally toalterations in plasma volume. In women whoshow oedema in late pregnancy the mean levelof haemoglobin concentration throughout thesechanges is significantly lower than in the non-oedematous cases.
Actual measurements of plasma volume andtotal body red cell mass confirm that, in non-oedematous primiparae, whereas the total cir-culating red cell volume falls slightly in thefirst three days after delivery, the plasma volumerises slightly at the same time. In the subsequentweek the red cell mass remains static, whereasplasma volume diminishes progressively.
It would seem, therefore, contrary to commonbelief, that water is held in the body for 3 or 4days after delivery, before ibeing disposed of;and that the post-partum diuresis is thusdelayed. There are several possible underlyingmechanisms for this water retention. The effectson body electrolytes described by Landau andLugilbihl (1964) and on connective t,issue shownby Zaohariae (1959) suggest that the sex steroidsare involved in control of total body water andelectrolyte content, and their possible role inthe puerperium is being investigated. Anotherpossibility lis that the dhanges are mediated byaldosterone, or hydrocortisone, either becauseof stress stimulation the result of labour, orbecause the hyperfunction of pregnancy cannotbe immediately reversed.
REFERENCESABOUL-KHAIR, S. A., BUCHANAN, T. J., CROOKS, J.,and TURNBULL, A. C. (1965): The Development ofFunction in the Human Foetal Thyroid Gland,Abstracts of Vth Int. Thyroid Conference, Rome,p. 16.
ABOUL-KHAIR, S. A., CROOKS, J., TURNBULL, A. C.,and HYrrEN, F. E. (1964): The PhysiologicalChanges in Thyroid Function during P,regnafcy,Clin. Sci., 27, 195.
ABOUL-KHAIR, S. A., CROOKS, J.. TURNBULL, A. C.,and TURNBULL, E. (1966): Changes in ThyroidFunction during Pregnancy Complicated by Pre-eclamlpsia. (In preparation).
ABOUL-KHAIR, S. A., CROOKS, J., TURNBULL, A. C.,and TURNBULL, E. (1966): Thyroid Function inCases of Albortion and Premature Delivery. (Inpreparation).
ANDERSON, A. B. M., TURNBULL, A. C., and MURRAY,A. (1966): The Relationship between Amn-ioticFluid Pressure and Uterine Wall Tension in Preg-nancy, Amer. J. Obstet. Gynec. In press.
BARTrER, F. C., LIDDLE, G. W., DUNCAN, L. E.,BARBER, J. K., and DELEA, C. (1956): Regulationof Aldosterone Secretion in Man: Role of FluidVolume, J. clin. Invest., 35, 1'306.
BENGTSSON, L. PH., and CSAPO, A. (1962): OxytocinResponse, Withdrawal, and Reinforcement ofDefense Mechanism of the Human Uterus atMidpregnancy, Amer. J. Obstet. Gynec., 83, 1083.
BROWN, J. J., DAVIES, D. L., LEVER, A. F., andROBERTSON, J. I. S. (1965): Plasma Renin Con-centration in Human Hypertension. 2: Ren-in inRelation to Aetiology, tBrit. med. J., ii, 12115.
BURT, ,R. L. (111954): Peripheral Utilization of Glucosein Pregnancy and the Puerperium, Obst. and Gynec.,4, 58.
CHRISTIE, J., ANDERSON, A. B. M., TURNBULL, A. C.,and BECK, J. S. (1966): The Human Placenta andMeamlbranes: A Histological and Immunofiuores-cent Study of the Effects of Intra-amniotic Injectionof Hypertonic Saline, J. Obstet. Gynaec. Brit.Cwlth. In press.
CROOKS, J., ABOUL-KHAIR, S. A., TURNBULL, A. C.,and IHYT'EN, F. E. (1964): The Incidence of Goitreduring Pregnancy, Lancet, ii, 334.
DAVEY, D. A., O'SULLIVAN, W. J., and BROWNE,J. C. McC. (1961): Total Exchangeable Sodium inNormal iPregnancy and in IPre-eclarnpsia, Lancet, i,519.
DE ALVAREZ, R. R., AFONSO, J. F., and SHERRARD,D. J. (1961): Serum Protein Fractionation inNormal Pregnancy, Amer. J. Obstet. Gynec., 82,1096.
DE BRUINE, T. L. A. (1960): Aldosterone Excretionin Eclaimptogenic Toxicosis, Ned. T. Verlosk., 60,381.
DENNIS, K. J., and BYrHEWAY, W. R. (1965): Changesin Body Weight after Delivery, J. Obstet. Gynaec.Brit. Cwlth., 72, 94.
DICZFALUSY, E., CASSMER, O., ALONSO, C., andDE MIGUEL, M. (1961): Estrogen Metabolism in theHuman Fetus and Newborn, Recent Progr. Hor-mone. Res., 17, 147.
DIECKMANN, W. J. (1950): In "Toxaemias of Preg-nancy", Ciba Foundation Symposium, London:J. & A. Churchill.
DUNCAN, 'L. J. P. (1956): The Intravenous GlucoseTolerance Test, Quart. J. Exp. Physiol., 41, 85.
EDELMAN, I. S., HALEY, H. B., SCHLOERB, P. R.,SHELDON, D. 'B., FRIIS-HANSEN, B. J., STOLL, G.,and MOORE, F. D. (1952): Further Observationson Total Body Water; Normal Values ThroughoutLife Span, Surg. Gynec. Obstet., 95, 1.
EDELMAN, I. S., LEIBMAN, J., O'MEARA, M. P., andBIRKENFIELD, L. W. (11958): Interrelations betweenSerum Sodium Conoentration, Serum Osmolarityan'd Total Exdhangeable Sodium, Total Exchange-alble Potassium and Total Body Water, J. clin.Invest., 37, 1236.
FURUHJELM, U. (1956): Maternal and Cord Blood;Comparative Investigation with Reference to BloodSugar, Serum Proteins, Erythrocyte Sedimentation,Rate and Total Serum Lilpids, Ann. Paediat. Fenn.,2, Suppl., 5, 1.
GALLETrI, F., and KLOPPER, A. (1964): The Effect of{Progesterone on the Quantity and Distribution ofBody Fat in the Female Rat, Acta endocr., (Kbh.),46, 379.
GILDER, H., REDO, S. F., BARR, D., and CHILD, C. G.(1954): Wa.ter Distribution in Normal Subjectsand in Patients with Laennec's Cirrhosis, J. clin.Invest., 33, 555.
HAGEN, A. (1961): Blood Sugar Findings duringPregnanocy in Normals and Possible Predialbetics,Diabetes, 10, 438.
copyright. on June 16, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.489.409 on 1 July 1966. Dow
nloaded from

420 POSTGRADUATE MEDICAL JOURNAL July, 1966
HALEY, H. B., and WOODBURY, J. W. (1956): BodyComposition and Body Water MetaJbolism inNormal Pregnancy, Surg. Gynec. Obstet., 103, 227.
HARDING, V. J., and VAN WYCK, H. B. (1931): Effectsof Hypertonic Saline in Toxaemias of Later Preg-nancy, J. Canad. med. Ass., 24, 635.
HERVEY, G. R., and HERVEY, E. (1964): Effects ofProgesterone on Food Intake and Body Composi-tion in Rats, J. Endocr., 30, vii.
HUMMEL, F. C., HUNSCHER, H. A., BATES, M. F.,BONNER, P., and MACEY, I. G. (1937): Considera-tion of Nutritive State in Metabolism of Womenduring Pregnancy, J. Nutr., 13, 263.
HUTCHINS6N, D. L., PLENTL, A. A., and TAYLOR, H. C.JR. (1954): The Total Body Water and the WaterTurnover in Pregnancy Studied with DeuteriumOxide as Isotopic Tracer, J. clin. Invest., 33, 235.
HYTrEN, F., and KLOPPER, A. (1963): Response to aWater Load in Pregnancy, J. Obstet. Gynaec. Brit.Cwlth., 70, 811.
HYTTEN, F. E., and LEITCH, I. (1964): "The Physiologyof Human Pregnancy", Oxford: Blackwell.
HYTTEN, F. E., and PAINTIN, D. B. (1963): Increasein Plasma Volume during Normal Pregnancy, J.Obstet. Gynec. Brit. Cwlth., 70, 402.
HYTrEN, F. E., TAGGART, N. BILLIEWICZ, W. Z., andJASON, A. C. (1962): The Estimation of SmallConcentrations of Deuterium Oxide in Water bythe Falling Drop Method, Phys. in Med. Biol., 6,415.
IKKOS, D., LJUNGGREN, H., LUFT, R., and SJOGREN, B.(1955): Content and Distribution of Potassium andChloride in Adults, Metabolism, 4, 231.
KAPLAN, N. M. (1961): Tolbutamide Tolerance Testin Carbohydrate Metabolism Evaluation, Arch.intern. Med., 107, 212.
KEMSLEY, W. F. F. (1951-52): Body Weights atDifferent Ages and Heights, Ann. Eugen. (Lond.),16, 3116.
KLOPPER, A. (1961): Oestriol Excretion in Pre-eclampsia, Path. et Microbiol. (Basel), 24, 652.
KLOPPER, A. (1964): Changes in Renal Function inLate Pregnancy, Lancet, ii, 565.
KLOPPER, A. (1966): "Research on Steroids". Ed. A.Klopper. II Pensiero Scienitifico, Rome. In press.
KLOPPER, A., and MACNAUGHTON, M. C. (1965):Hormones in Recurrent Abortion, J. Obstet.Gynaec. Brit. Cwlth., 72, 1022.
KLOPPER, A., and STEPHENSON, R. (1'966): Oestrioland Pregnanediol Excretion in Rhesus Incom-patibillity, J. Obstet. Gynaec. Brit. Cwlth., In press.
KLOPPER, A. I., TURNBULL, A. C., and ANDERSON,A. B. M. (1966): Steroid Hormone Excretionfollowing Intra-amniotic Injection of HypertonicSaline, J. Obstet. Gynaec. Brit. Cwlth. In press.
LANDAU, R. C., and LUGIBIHL, K. (1964): Advancesin Treatment of Menstrual Dysfunction, p. 60.London: Henry Kimpton.
LEAF, A., BARTTER, F. C., SANTOS, R. F., and WRONG,0. (11953): Evidence in Man that Urinary Electro-lyte Loss Induced iby Pitressin is Function of WaterRetention, J. clin. Invest., 32, 868.
LOUROS, N. C., MIRAS, K., and FRANGIADAKIS, L.(1'960): Aldosterone and Pregntanediol Excretion inthe Urine in Normal Pregnancy and in PregnancyToxaemias. (Preliminary Report), Geburtsh u.Fraueheilk, 20, 848.
MOCARTNEY, C. P., POTTINGER, R. E., and HARROD,J. P. (1959): Alterations in Body CompositionDuring Pregnancy, Amer. J. Obstet. Gynec., 77,1038.
MAOGILLIVRAY, I. (1961a): Water and ElectrolyteMetalbolism. Amsterdam: Elsevier.
MACGILLIVRAY, I. (19611b): Salt and Water Balance-in Normal and Toxaemic Pregnancy, Path. etMicrobiol. (Basel), 24, 639.
MACGILLIVRAY, I., and BUCHANAN, T. J. (1958):Total Exchangeable Sodium and Potassium in Non-pregnant Women and in Normal and Pre-eclampticPregnancy, Lancet, ii, 1090.
MACGILLIVRAY, I., HYTTEN, F. E., TAGGART, N., andBUCHANAN, T. J. (1962): The Effect of a SodiumDiuretic on Total Exchangeable Sodium and TotalBody Water in Pre-eclamptic Toxaemia, J. Obstet.Gynaec. Brit. Emp., 69, 458.
MAOGILLIVRAY, I., and TOVEY, J. E. (1957): A Studyof the Serum Protein Changes in Pregnancy andToxaemia, using Paper Strip Electrophoresis, J.Obstet. Gynaec. Brit. Emp., 64, 361.
MCMURREY, J. D., BOLING, E. A., DAVIS, J. M.,PARKER, H. V., MAGNUS, I. C., BALL, M., andMOORE, F. D. (1958): Body Comlposition: Simul-taneous Determination of Several Aspects by theDilution Principle, Metabolism, 7, 651.
MAHRAN, M. (1961): Sodium Metabolism in Gynaeco-logy and Obstetrics, J. Obstet. Gynaec. Brit. Emp.,68, 597.
MEDLEY, D. R. K. (1965): The ,Relations'h,ip betweenDialbetes and Obesity: A Study of Susceptibility toDialbetes in Obese People, Quart. J. Med. N. S., 34Il',l.
PAABY, P. (1960): Changes in Serum Prote:ns duringPregnancy, J. Obstet. Gynaec. Brit. Emp., 67, 43.
PLENTL, A. A., and GRAY, M. J. (1959): Total BodyWater, Sodium Space, and Total ExchangeableSodium in Normal and Toxemic Pregnant Women,Amer. J. Obstet. Gynec., 78, 472.
ROY, E. J., HARKNESS, R. A., and KERR, M. G.(1963): Concentration of Oestrogens in Blood andUrine of Patients Suffering from Pre-eclampsia,J. Obstet. Gynaec. Brit. Emp., 70, 597.
SCHLOERB, P. R., FRIIS-HANSEN, B. J., EDELMAN, I. S.,SOLOMON, A., and MOORE, F. D. (1950): Measure-_ment lof Total Body Water in Human Subjects byDeuterium Oxide Dilution with Consideration ofDynamics of Deuterium Distribution, J. clin. Invest.,29, 12%.
STRAUSS, M. (1937): Observations on Etiology ofToxemias of Pregnancy; Production of Acute Ex-acerbation to Toxemia by Sodium Salts in PregnantWomen with Hypoproteinemia, Amer. J. med. Sci.,194, 772.
TURNBULL, A. C. (-962): Amniotic Pressure, CervicalDilatation and the Cervix in Labour, J. Obstet.Gynaec. Brit. Cwlth., 69, 1047.
TURNBULL, A. C., and ANDERSON, A. B. M. (1965):Changes in Uterine Contractility following Intra-amni.otic 'Injection ,of 'Hypertonic Saline to InduceTherapeutic Abortion, J. Obstet. Gynaec. Brit.Cwlth., 72, 755.
TURNBULL, A. C., and ANDERSON, A. B. M. (1966):Intra-amniotic Hypertonic Saline, Brit. med. J., i, 672.
WELSH, G. W. (1960): Studies of Abnormal GlucoseMetabolism in Pregnancy, Diabetes, 9, 466.
ZACHARIAE, F. (1959): Acd Mucopolysacdharides inthe Female Genital System and their Role in theMechanism of Ovulation, Periodica, p. 13, Copen-hagen. Bogtrgk'keriet, Jorum.
ZAK, G. A., and EARLE, D. P. (1957): Blood Volumeand Body Water in Normal Hospital Subjects, J.lab. Clin. Med., 49, 504.
copyright. on June 16, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.489.409 on 1 July 1966. Dow
nloaded from