Embed Size (px)
Citation preview

1
Hormone replacement therapy and elevated breast cancer risk: An artifact of growth acceleration? 1 2 Jutta Engel, Gabriele Schubert-Fritschle, Dieter Hölzel 3 4 Munich Cancer Registry (MCR), Institute for Medical Information Processing, Biometry and 5 Epidemiology (IBE), Ludwig-Maximilians-University (LMU), D-81377 Munich, Germany 6 7 8 Corresponding author: 9 Prof. Dr. Dieter Hölzel 10 Munich Cancer Registry 11 D-81377 München, Germany 12 [email protected] 13 Tel: ++49-89-8414875 14 15 16 17 Abbreviations: 18 BC breast cancer 19 ER+/- estrogen positive/negative 20 GD Growth duration of BC 21 GF Growth factor 22 HR Hazard Ratio 23 HT hormone replacement therapy 24 HTD hormone replacement therapy duration 25 WHI-S Women health initiative study 26 27 28 Keywords: 29 breast cancer; hormone replacement therapy; tumor growth; risk factor 30 31 32 33 34
. CC-BY-NC-ND 4.0 International licenseIt is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 7, 2020. .https://doi.org/10.1101/2020.04.04.20050708doi: medRxiv preprint

2
Abstract: 35 Background: Available data on accelerated proliferation and increased breast cancer risk due to 36 hormone replacement therapy (HT) are inconsistent. Data on long-term effects of HT are limited. The 37 interaction between several key factors was examined using a model-based approach. 38 39 Methods: Cohorts of 50 year old women, BCs were randomly generated for 30 years based on the 40 age-specific incidence. A control group received a HT that increased the growth of occult BCs. In a 3rd 41 cohort BCs were additionally induced by HT. This model illustrates the interrelationship of important 42 parameters and allows the simulation and comparison of previously published clinical studies. 43 44 Results: Using plausible parameters for BC growth factor (GF) and HT-related effects it was 45 demonstrated that HT caused accelerated growth of occult BCs with an apparent increase in 46 incidence and shortened time to diagnosis. The Women’s Health Initiative (WHI) study was 47 reconstructed assuming a GF of 1.43 induced by HT. The decision of millions of women to 48 discontinue or forego HT based on the published risks of the WHI-study in 2002 could explain the 49 marked jump of 6.7% in incidence within a few months. If additional BCs were induced by HT, then 50 these BCs may become apparent after 10 or more years together with those appearing according to 51 the normal incidence. At this time conclusive data on type, timing, and molecular characteristics of 52 HT induced BCs are not yet available. 53 54 Conclusion: The acceleration in growth of occult BC has been underestimated. Initially HTs can cause 55 an apparent increase in BC incidence thereby explaining the WHI-dependent decrease in 2003. A HT 56 associated BC risk should only be detectable with a delay of ten and more years. 57 58 59 60 61
. CC-BY-NC-ND 4.0 International licenseIt is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 7, 2020. .https://doi.org/10.1101/2020.04.04.20050708doi: medRxiv preprint

3
Introduction 62 Hormone replacement therapy, hereafter referred to as hormone therapy (HT), has been the subject 63 of over 50 years of research and discussions leading to a varying use in clinical practice 1. The reasons 64 for this disparity are reported negative and positive side effects of HTs2 such as a higher risk for 65 invasive breast cancer (BC), endometrial cancer, or stroke. On the other hand positive side effects 66 have also been published such as a reduced risk for fractures, diabetes, colon cancer, or heart 67 disease. Cost-benefit analyses are complex due to the dependency on age, the type and duration of 68 HT application. Guidelines generally emphasize the need and the benefit of HTs, but also vary in 69 their restrictiveness. A recently updated meta-analysis 3,4 continues this HT narrative by which 70 approximately 5% or 1 million BCs have been induced by HT since 1990. This result of the study 71 motivated the analysis herein. The main objective was to assess the association of BC with key 72 factors using models based on studies and populations, compare their results, and discuss the use 73 and suitability of the currently available data. 74 75 Methods 76 The models described below were based on cohorts of 50 years old women. BCs were randomly 77 generated for 30 years according to the age-specific incidence5,6. For a comparison with published 78 clinical trials the respective age distributions and competing mortality according to life expectancy 79 were considered. The second cohort begins with HT application, and expected effects of HTs were 80 modeled according to 4 parameters: duration of BC growth (GD), duration of HT application (HTD), 81 and an accelerated growth (GF) due to HT. In the 3rd cohort a BC risk was also modeled. It was 82 assumed that proliferation and BC risk begins and ends with HT application, as the well-known BC 83 incidence jump in 2003 suggests. 84 The modeling approach based on the association of 15 years of GD, 4 years HTD, a doubled GF, and a 85 BC risk is clarified in figure 1. Herein illustrated are the growth trajectories for BCs, the number of 86 tumor cells (log scale), as well as the age of the occult BCs over time. The logarithm of the tumor cells 87 resulted in a linear trajectory for the assumed exponential BC growth. A second key component was 88 the GF, a linear transformation of the growth induced by HT. The impact of growth acceleration may 89 be subdivided into 6 phases (Figure 1B). Plausible model assumptions were taken from peer-90 reviewed literature, direct comparisons were taken from the Women´s Health Initiative Study (WHI-91 S)7,8, and the updated meta-analysis.3 The model was constructed and all statistical analysis were 92 done in R Version 3.1.3.9 93 94 Results 95 Plausibility of model assumptions 96 97 For the model a GD of 15 years for ER+ BCs was assumed. Regarding chemoprevention, a rise in 98 incidence in the following 15 years after the end of prevention was not found.10-12 This conservative 99 presumption is presented in Figure 2A after a 2-year preventive therapy which successfully 100 eradicated 50% of occult and BCs emerging on HTs. A GD of 15 years resulted in a duration of 166 101 days for the required 33 consecutive BC volume doubling of BCs of 20 mm.13 The GD was also 102 estimated based on screening data.14 The calculated 25%/50%/75% percentile for the time required 103 for a volume doubling in women between 60-69 years old and a tumor diameter of 15 mm was 104 65/143/308 days. Applying this to an increase in diameter from 2.5 mm (pT1a) to 28 mm (pT2) with 105 10.5 volume doublings resulted in 1.9/4.1/8.8 years. Based purely on this calculation and beginning 106 with the first tumor cell, all BCs – not just ER+ – would grow to a diameter of 20 mm after 33 VDs in 107 approximately 5.9/12.9/27.8 years. 108 109 In addition a twofold BC risk was assumed for HT (Figure 2A), which by way of the Gail-Model15 110 estimated a higher prevalence of common risk factors. This model was used in prevention studies to 111 recruit participants and confirmed its results 11. However, the GF in the model varied. In Figure 1 the 112 factor of 2 is easily discernible and plausible following the above described doubling times. This GF 113
. CC-BY-NC-ND 4.0 International licenseIt is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 7, 2020. .https://doi.org/10.1101/2020.04.04.20050708doi: medRxiv preprint

4
was also identified from data on the 2.5-fold accelerated growth of ER- compared to ER+ BCs. In BC 114 20% of MET occur 10 years after the initial diagnosis, and together with the BC GD clarify for a time 115 span of 30 years on the x-axis.16 116 117 Simulation results 118 119 Results based on the parameters GD 15 years, HTD 4 years, and GF 2 are shown in Figure 1A. The 120 trajectories illustrate a growth in diameter starting from BC initiation and the effect of HT. The model 121 was based on the cumulative incidence of a cohort of 100 000 50 years old women (Figure 2A, red 122 curve). Initially 216 BCs (SD 14) were randomly generated per year according to the age-specific SEER 123 incidence, 30 years later the cases numbered 372 (SD 21) (Fig.2B), with an overall total of 10 219 (SD 124 105) BCs without considering competing risks. The slight curvature was a result of the increased 125 incidence due to age, which is why only 40% of BCs occurred within the first 15 years. 126 Chemoprevention applied over two years effective in 50% of cases could have prevented 2 431 or 127 24% BCs. 128 129 The application of HT stimulated the growth of occult BCs (Figure 2A, green curve). This lead to six 130 marked follow-up periods P1-6 (Fig.1B) associated with HTD and GF. Three variations of this 131 stimulated growth can be described, namely with 4 years of HTD with a GF of 2 there is a cumulation 132 of BCs in the first two years, twice as many were diagnosed overall compared to the control group. 133 Period P1 ends after two years (HTD/GF) at a turning point for the cumulative incidence. This point is 134 defined by BCs that became apparent under HT 0 to a maximum of 2 years earlier following a linear 135 course (Figure 1B P1 red with HT). 136 137 The second variation begins after 4 years when all BCs have been exposed throughout the HTD and 138 become symptomatic two years earlier through this induced growth (Figure 1B green, P2-4 with HT). 139 A gap subsequently appears in P4 (Figure 2B). In P4-6 (Figure 1B, brown) BCs were diagnosed also 140 exhibiting accelerated growth that arise according the age-specific incidence for women aged 50 141 years or older under HT. The shift in this third variation spans from 0 to a maximum of two years 142 similar to P1, however in the form of its mirror image. The consequences were as follows: The first 143 BCs are maximally expedited and the duration of diagnosis is expanded thus lowering overall 144 incidence. However, the cohort under HT (Figure 2A green) exhibits the same number, although 145 faster growing, BCs as those without HT. Up until P6 the same number of BCs become evident and 146 thereafter there is no longer a HT effect.. 147 148 The concept that HT may induce de novo BCs was also simulated (Figure 1-2, blue). If HT caused BCs 149 and these would be induced during HT with an accelerated growth rate, then these induced BCs 150 would become apparent in the same phase P4-6 as the age-dependent BCs. A twofold BC-risk would 151 double the number of normally HT induced BCs during an exposure to HT for women 54 years old or 152 younger. A second turning point would be expected starting from P4 when the hazard rate would 153 again increase due to BC risk (Figure 2C). It should be noted that HR at the 2nd turning point is likely 154 to underestimate the true BC risk. If the growth of HT-induced BCs is also accelerated, then initiation 155 occurs in P1-2 and diagnosis in the expanded period P4-6 (Fig.1B). 156 157 This type of non-proportional hazard rate can remain latent in an overall analysis. The hazard ratios 158 (red vs. green) were identical up to the turning point due to the linear GF-transformation, only the 159 confidence interval decreases due to the increasing number of patients. The HR is the quotient of the 160 number of BCs that initially became evident with or without HT, therefore HR at this turning point is 161 equivalent to the GF. After the turning point the HR fell to 1 in P6, meaning that even at the end of 162 the HT the HR already underestimated the proliferative effect (HR 1.55 after 4 years in Figure 2A). If a 163 BC risk is present (blue vs. red comparison) the HR may again increase from P4. Post interventional 164
. CC-BY-NC-ND 4.0 International licenseIt is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 7, 2020. .https://doi.org/10.1101/2020.04.04.20050708doi: medRxiv preprint

5
analysis (Figure 2C) can exhibit time lagged effects that may result in a protective effect in 165 comparison to a cohort without HT.17 166 167 Due to the overlapping influence of BC risk and the proliferative effect small risks hardly become 168 evident in studies with small sample sizes, a follow-up period spanning over 2 decades, and a lack of 169 model assumptions. On the other hand it can be confirmed that the initial increase in incidence can 170 be caused by the accelerated growth of previously existing BCs. Interpreting this as a BC-risk is 171 therefore incorrect, it would be an incidence-increase imitation-bias. 172 173 The women health initiative studies 174 175 In order to model the WHI-S the following data are used: Incidence, age-distribution, competing 176 risks, and a sample cohort of 8 506 receiving HT with estrogen plus progestin for a total of 5.6 years. 177 After 7.2 years the HR reached 1.24 (95%CI: 1.05 – 1.43).8 This HR can be achieved with a GF of 1.43 178 (95%CI: 1.18 – 1.78) with a turning point after 3.9 (5.6/1.43) years. The effect of the WHI-S can be 179 explained with a boost in growth through HT (Figure 3). If after 13 years (HR=1.3, 95%CI 1.01-1.27) 180 the HR continues to decrease, then there is no BC-risk with HT. Currently published is a HR of 1.29 181 (95%CI 1.14-1.47) based on 16.1 years of follow-up 18. This would correspond to a twofold BC risk 182 after 19 years (HR 1.28, 95%CI 1.16-1.40). 183 184 Even if the long-term results of the WHI-S were modeled with proliferation and BC risk, the 185 discrepancy between the incidence curves should be noted. A negative mammography exam as an 186 inclusion criterion could shift the first date of diagnosis of ER+ BCs by months, however a shift of 3 187 years as shown in the WHI-S is not plausible. This delayed opening of curves could not be reproduced 188 in the WHI observational study which corresponds to Fig.3.19 A GF of 1.43 offered an explanation for 189 the study results but did not directly explain the immediate drop in incidence observed in the United 190 States after the publication of the study in July 2002. There was a 6.7% or 11.8% drop of BCs in all 191 women or between the ages of 50-69 between 2002 and 2003 and the decrease was more evident in 192 those with ER+ BCs.5,20 193 194 This simultaneous decline in the incidence of BCs and HT prescriptions can most likely be attributed 195 to the publication of the associated BC risk. Simulations and the study data showed that HTs do lead 196 to an apparent short-term increase in the incidence. This increase was just as brief and reversible as 197 the change in breast density that results from HT discontinuation. Figure 1B illustrates the continued 198 forward shift that resulted from a continued HT application. It should also be considered if no HT was 199 started due to published BC risk, then no proliferative effect was induced accordingly. Taken together 200 these results point to one reason for the observed drop in incidence, namely the decision of many 201 women to abstain from or discontinue HT due to a perceived BC risk. 202 203 The simulation showed 8 506 women and 49/36 BCs in the first year with/without HT, in 100 000 204 women this added up to a total of 701/499 BCs. These results fluctuated because of the random 205 generated data. Transferring these findings to the 203 500 newly diagnosed cases of BC in 2002 in 206 the USA 21, out of which 44% were diagnosed between the age of 50-69, would explain the 11.8% 207 drop in incidence equivalent to 10 570 BCs . A decline of this magnitude can be attributed to a GF of 208 1.43 and an average incidence of 360/10**5 in patients under HT if 6.8 million women discontinued 209 or abstained completely from HT. A simulation of the WHI-S resulted in a difference of approximately 210 200 accelerated BCs out of 10**5 women after HT and 5.3 million women. However, the number of 211 women under HT in total has decreased by 5 million between 2001 to 2003.22 212 213 The meta-analysis 214 215
. CC-BY-NC-ND 4.0 International licenseIt is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 7, 2020. .https://doi.org/10.1101/2020.04.04.20050708doi: medRxiv preprint

6
The updated meta-analysis summarized unique data from 58 clinical studies, included almost 150 216 000 BCs, and follow-up data of up to 20 years.3 Results herein for different HTD and post intervention 217 phases were shown for the HT model with estrogen plus progestin. The remarkably high HRs for 218 current users contradict these modeling results. A nearly implausible GF of 4 would still not be 219 obtainable even after a HTD of 7 years and a resulting HR of nearly 2. 220 221 If the relative risk is determined using case-control studies the inclusion criteria must be observed in 222 order to separate the two effects, growth acceleration and BC induction, according to Fig.2. Up to 223 the turning point of the HT, the relative risk also estimates the GF. With an increasing time since HT 224 in P2-P4, the HRs of past users kept becoming smaller compared to those of current users. If the sum 225 of the HT duration and the time since the end of the HT reaches the mean GD of the BCs in P4-P6 for 226 past users the BC risk can be analyzed. For several of these constellations, an increased BC risk of 227 approximately 1.2 was shown after more than 10 years. An apparent protective effect due to 228 proliferation (Fig. 2C red vs. green) cannot be seen, as in the WHI-S. 229 230 As with the WHI-S attention was also drawn to the increased BC mortality after 20 years for HT user. 231 23 The term proliferation was missing, so that an increased incidence did not differentiate between 232 accelerated growth and BC risk. 233 234 Discussion 235 236 The incidence and the associated BCs in the control group without HT are used as model parameters. 237 The GD of ER+ BC varies greatly but 15 years appears to be a plausible assumption based on the 238 exponential growth and volume doublings estimated from screening. The widening gap between 239 incidence- and survival curves of chemoprevention and adjuvant therapy also highlight this 240 observation. A GF of 1.43 explains the results of the WHI-S.8,19 The proliferation observed in HT 241 exposed BCs characterised by a short-term increase in breast density and cellular activation is known 242 from imaging during screening. This effect is reversible within a few weeks. Switching growth on and 243 off through HT is the only plausible explanation for the sudden drop in BC incidence in 2002/2003.5,24 244 The change appears to be limited to the luminal A-like BC subtype and can be reversed by HT 245 discontinuation.25 Similarly an increased level of Ki67 indicates an increased proliferation in benign 246 breast tissue samples.26 This specific proliferative activity leads to a more frequent diagnosis of ER+ 247 BCs under HT 19 compared to the ER- BCs 2.5 times faster growth rate. 248 249 While the HTs appear to accelerate short-term growth, the cellular pathways and characteristics of 250 the induced BCs have so far not been adequately described. It is biologically plausible that BCs 251 caused by HT are delayed.27 A risk relative to the age-specific incidence for women during HT was 252 modeled. However, the assumption that the BC risk follows a linear increase and can be switched on 253 and off similar to the proliferation activity is not plausible. Many risks do not follow a linear course, 254 and at this time there is no evidence that HTs enable the rapid formation of the necessary driver 255 mutations. This assumption would be in strong contrast to most other tumor types where 256 carcinogenesis processes develop over years or even decades.28,29 By applying sensible assumptions 257 the first BCs induced through HT would manifest at a later time, perhaps even 20 years after the start 258 of HT. 259 260 In addition, data on the difference between BC-associated mutations promoted immediately through 261 HT and those that occur normally as a result of serial mutations according to the known incidence 262 remain to be reported. Are genetic modifiers of HT associated BCs available soon? Are there fewer 263 passenger mutations due to short-term transformations in cancer cells? Do the 4% of occult BCs in 50 264 year old women present with a distinctive signature from the HT promoted growth? Do the BCs have 265 an inherent memory for the exposition to HT? Is the growth boost dependent on tumor size? The 266 molecular processes involved offer a unique research platform to study complex cancer pathways.30 267
. CC-BY-NC-ND 4.0 International licenseIt is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 7, 2020. .https://doi.org/10.1101/2020.04.04.20050708doi: medRxiv preprint

7
268 Even epidemiological data currently do not offer sufficient evidence for HT-induced BC-risk.31 The 269 chemoprevention results clarify that short-term eradication of prevalent BCs decreased the BC rate 270 over more than 15 years.10 Similar results were seen for other risk factors such as alcohol 271 consumption and smoking, which have an effect on cancer incidence after decades. However, up to 272 this point it has not been proven that a withdrawal of HT can stop or even eradicate an already 273 initiated cancerous growth. If the BC risk is efficiently reduced by millions of women who abstain 274 from HT, then this should have a long-term effect on incidence. However, there was only a drop in 275 incidence in 2002/2003 following the initial publication of the WHI-S and so far no further increase in 276 the past 15 years.5 I.e. the status quo ante was already an artifact, the incidence has increased with 277 the increasing use of HT, as the SEER data from 1995-2000 show. After the publication of the study 278 results on the secondary prevention of coronary heart disease by HTs32 the BC incidence and the HT 279 use have both continued to decline since 1999.33,34 280 The time with which BCs occur earlier increases continuously and reaches a maximum of HTD/GF 281 years. The incidence in a population increases accordingly. If BCs grow 15 years, no induced BCs are 282 expected in the first 10 years after the start of HT with a GF <1.5. 283 284 There is no valid evidence and it is not plausible27 that occult BCs shortly before becoming manifest 285 should abandon their autonomous growth, regress, or only become evident at a later time through 286 HT discontinuation.20,35,36 Even a slowly decreasing participation rate for screening examinations 287 cannot explain this effect.34,37 The jump in incidence of about 10 000 BCs is a real effect and was 288 achieved by about 5 million women not beginning or discontinuing an HT. With 360 BCs per 100,000 289 annually, this would achieve a short-term proliferation with a GF 1.59. A BC risk that only slowly 290 increases with the duration of the therapy, as in meta-analysis, would lead to an implausibly high 291 number of women who refrained from HTs or discontinued HTs. Since a GF of a specific HT should be 292 uniform it would be desirable to prepare different HRs for the incidence curves when long-term 293 follow-up is available. 294 295 Even if no evidence is available on a higher risk for recurrent cancer, then the entire process of 296 cancerogenesis should be accelerated under HT. This includes the growth of BCs, tumor cell 297 dissemination, and growth of prevalent metastases. Through this type of proliferation more cases of 298 interval cancers, with a larger tumor size, increased number of node positive lymph nodes, and faster 299 growing metastases occur as shown in the discussed studies.8,23,38 The 15-year survival of BCs with a 300 diameter of 17 vs. 15 mm8 varies by 3%, a change from 11 to 15mm increases this difference to 5%.39 301 For this reason an annual instead of 2-3 yearly screening would have and will reduce proliferation risk 302 in women with HT. A small increase in mortality is therefore plausible even without the additional BC 303 risk. 304 Modeling the effect of a few parameters on the cumulative incidence and the post-interventional risk 305 is a valuable approach. The interactions are complex, but in the sense of Occam’s razor, proliferation 306 is a simple principle that can explain observations and stimulate the generation of hypotheses. For 307 example the effect of a wash-out period of HTs on proliferation would be quite illogical. Rather, the 308 sum of all HT-intervals should be correlated with the incidence. The increase in BC with prior HT use 309 in the WHI-S has now been shown.18 Modeling studies can aid in continually specifying research 310 objectives, prerequisites for future observations, and data analysis approaches. The previously 311 discussed time-dependency and the P1-6 time-shifted effects are obstacles for any type of case-312 control studies. The immense value of prospective studies and real world data with follow-up data 313 over decades becomes clear, since there is no valid data to point to specific factors which are 314 correlated with frequency and timing of additional HT-induced BCs. This constitutes a major 315 limitation: data is missing that allows models to be verified and improved. 316 317 The WHI-S showed that millions of women discontinued or completely abstained from HTs due a fear 318 of cancer. By foregoing HTs many women suffering from postmenopausal symptoms have accepted a 319
. CC-BY-NC-ND 4.0 International licenseIt is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 7, 2020. .https://doi.org/10.1101/2020.04.04.20050708doi: medRxiv preprint

8
lower quality of life2,40,41. That should not be repeated. There are no valid estimates which of the 1 320 million BCs simply occurred earlier or which were induced with what timing. Balanced information 321 also about possible induced and delayed BCs for women are necessary even after 50 years of HT. 322 323 Conclusion 324 325 HTs appear to boost the growth of occult BCs, leading to an apparent rise in the overall incidence. A 326 GF of 1.43 was estimated for the WHI-S which explains the decrease in incidence in 2002/2003. HT 327 induced BCs would manifest simultaneous to the BCs originating under HT according to the age 328 specific incidence. Although sound data on proliferation is available, type, timing, and especially the 329 molecular characteristics of HT-induced rapidly growing BCs are currently not readily available. This 330 work is mainly based on the analysis of cancer registry data and basic metastasis process. Modeling 331 studies may aid in specifying research objectives and also provide direction during the search for 332 effects in large datasets. 333 334 335 Key clinical points 336 Hormone Therapy for Postmenopausal Women 337 338
The reported BC risk of HTs reduced their use after the publication of the WHI study in 2002 339 and caused an immediate 6.3% decrease in the incidence in the SEER data 340
To date there is no reliable data on how large the BC risk is according to the type and 341 duration of the HT 342
Hormone receptor positive BCs grow slowly, on average maybe 15 or more years 343
The increase in incidence with the onset of HTs can only be caused by a faster growth of 344 occult hormone receptor positive BCs. 345
Information is lacking on how quickly HTs induce the necessary driver mutations and 346 whether these de novo BCs differ from normal BCs 347
Induced BCs, even if mutations occur in a flash, are only likely to occur with a time delay of 348 10 or more years with growth factors < 1.5 349
The 6.3% jump in incidence in a single year can only be caused by preventing faster growth 350
The increased incidence in the SEER data up to this jump is correlated with the increasing HT 351 use and caused by the assumed faster growth of occult BCs 352 353
354 355 Appendices: 356
Disclosure The authors have declared no conflicts of interest. 357
358 359 360 Acknowledgment 361 We thank Doris Mayr, Sylvia Heywang-Köbrunner, Christian Thaler, Michael Lauseker for valuable 362 scientific and technical advice, Ingo Bauernfeind for the Project Group Breast Cancer for the 363 opportunity to present and discuss preliminary results. Kathrin Halfter helped us with the manuscript 364 and in particular, we would like to thank the staff of the Munich Cancer Registry for their meticulous 365 and systematic recording and maintenance of the data. 366 367 368
. CC-BY-NC-ND 4.0 International licenseIt is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 7, 2020. .https://doi.org/10.1101/2020.04.04.20050708doi: medRxiv preprint

9
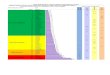
Fig.1: Tumor growth and the effects of hormone replacement therapy (HT) 369 A: The x-axis represents age beginning at 50 years with a second x-axis representing the BC growth 370 time relative to the beginning of the cohort. Double-sided arrows depict the time span of BC growth 371 (black, mean 15 years) and the HT (4 years, red and gray area). On the left y-axis the number of 372 tumor cells is shown (log-scale and example tumor diameters in mm), the right y-axis the age of the 373 occult BCs. Their trajectories follow an exponential growth and are therefore shown as lines. Each 374 trajectory depicts one of three respective growth spurts caused by HT (HTD of 4 years) with dashed 375 lines representing the control group. The blue points at the top and bottom symbolize the origin of 376 additional induced BCs and their shift in time to diagnosis after HT. (Periods: see Fig. 1B and legend). 377 378
Abb.1A
379 B: Diagnosis of BC with and without HT with a GD of 15 years, HTD 4 years, and a GF 2. The 380 proliferation caused by HT initiates a transformation of the BC-free time span leading to 6 separate 381 phases. The resulting concentration of BCs at the beginning leads to an apparently increased 382 incidence. The 6 vertical lines distinguish time periods during follow-up: 1. HT beginning, 2. Turning 383 point (HTD/GR), 3. End of HT, 4. Diagnosis of first BCs initiated or induced after start of HT and 384 accelerated by HT, 5. Mean time of BC growth: Limit for all BCs prevalent at time=0. 6. End of HT 385 effects (GD+HTD). 386 387
Abb.1B
388 389
. CC-BY-NC-ND 4.0 International licenseIt is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 7, 2020. .https://doi.org/10.1101/2020.04.04.20050708doi: medRxiv preprint

10
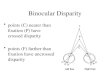
Fig 2: Simulation of the cumulative BC incidence for women starting from 50 years of age using the 390 model parameters GD 15, HTD 4, GF 2, twofold BC risk. 391 A: Cumulative BC incidence according to currently reported incidence (red), with accelerated growth 392 after HT and the same number of BCs (green), and additional BC risk (blue). Were a cohort to receive 393 a 50% effective chemoprevention for two years, the incidence would increase again two years after 394 GD. Overlapping lines were manually shifted for better illustration. 395 396
Fig. 2A
397 398
. CC-BY-NC-ND 4.0 International licenseIt is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 7, 2020. .https://doi.org/10.1101/2020.04.04.20050708doi: medRxiv preprint

11
B: BC cases per year for each of the three cohorts of Fig. 2A without HT (red), with HT (green), and 399
additional BC risk of HT (blue). The effect of GF 2 (green) with the concentration of cases in P1 400
(incidence doubling), the expedition of BCs, and the expansion in P4-5 are clearly evident for the 401
same number of BCs. The HT induced BCs all occur during P4-5 (blue). Yearly fluctuations are caused 402
by random generation. Overlapping lines were manually shifted to improve visualization. 403
404
Fig. 2B
405 406
. CC-BY-NC-ND 4.0 International licenseIt is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 7, 2020. .https://doi.org/10.1101/2020.04.04.20050708doi: medRxiv preprint

12
Fig.2C Cumulative incidence starting 4 years after HT end (post-HT cumulative incidence) 407 408
409
. CC-BY-NC-ND 4.0 International licenseIt is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 7, 2020. .https://doi.org/10.1101/2020.04.04.20050708doi: medRxiv preprint

13
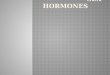
Fig.3 Simulations of the WHI-S using a cohort of n=8 506 according to their respective age-410 distribution (Mean age 63.7) and competing risks. HTD 5.6 years and GF 1.43 result in a HR of 1.26 411 after 7.2 years as reported in the WHI-S. 412 413
Fig.2A
414 415
. CC-BY-NC-ND 4.0 International licenseIt is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 7, 2020. .https://doi.org/10.1101/2020.04.04.20050708doi: medRxiv preprint

14
References 416 417 418 1. Lobo RA. Hormone-replacement therapy: current thinking. Nature reviews Endocrinology 419 2017;13:220-31. 420 2. Marjoribanks J, Farquhar C, Roberts H, Lethaby A, Lee J. Long-term hormone therapy for 421 perimenopausal and postmenopausal women. The Cochrane database of systematic reviews 422 2017;1:Cd004143. 423 3. Collaborative Group on Hormonal Factors in Breast Cancer. Type and timing of menopausal 424 hormone therapy and breast cancer risk: individual participant meta-analysis of the worldwide 425 epidemiological evidence. Lancet 2019;394:1159-68. 426 4. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormone 427 replacement therapy: collaborative reanalysis of data from 51 epidemiological studies of 52,705 428 women with breast cancer and 108,411 women without breast cancer. Collaborative Group on 429 Hormonal Factors in Breast Cancer. Lancet 1997;350:1047-59. 430 5. Noone A, Howlader N, Krapcho M, Miller D, Brest Ae. SEER Cancer Statistics Review, 1975-431 2015 National Cancer Institute. Bethesda, MD,: http://seer.cancer.gov/ (accessed March 20, 2020). 432 6. Munich Cancer Registry. http://www.tumorregister-433 muenchen.de/en/facts/specific_analysis.php (accessed March 20, 2020). 434 7. Writing Group for WHI Investigators. Risks and benefits of estrogen plus progestin in healthy 435 postmenopausal women: principal results From the Women's Health Initiative randomized controlled 436 trial. Jama 2002;288:321-33. 437 8. Chlebowski RT, Hendrix SL, Langer RD, et al. Influence of estrogen plus progestin on breast 438 cancer and mammography in healthy postmenopausal women: the Women's Health Initiative 439 Randomized Trial. Jama 2003;289:3243-53. 440 9. R Core Team. R: A language and environment for statistical computing. R: Foundation for 441 Statistical Computing, Vienna, Austria. URL http://www.R-project.org/. 2015. 442 10. Cuzick J, Sestak I, Forbes JF, et al. Use of anastrozole for breast cancer prevention (IBIS-II): 443 long-term results of a randomised controlled trial. Lancet 2019. 444 11. Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for the prevention of breast cancer: 445 current status of the National Surgical Adjuvant Breast and Bowel Project P-1 study. Journal of the 446 National Cancer Institute 2005;97:1652-62. 447 12. Visvanathan K, Hurley P, Bantug E, et al. Use of pharmacologic interventions for breast cancer 448 risk reduction: American Society of Clinical Oncology clinical practice guideline. Journal of clinical 449 oncology : official journal of the American Society of Clinical Oncology 2013;31:2942-62. 450 13. Santen RJ, Yue W, Heitjan DF. Modeling of the growth kinetics of occult breast tumors: role in 451 interpretation of studies of prevention and menopausal hormone therapy. Cancer epidemiology, 452 biomarkers & prevention : a publication of the American Association for Cancer Research, 453 cosponsored by the American Society of Preventive Oncology 2012;21:1038-48. 454 14. Weedon-Fekjaer H, Lindqvist BH, Vatten LJ, Aalen OO, Tretli S. Breast cancer tumor growth 455 estimated through mammography screening data. Breast cancer research : BCR 2008;10:R41. 456 15. Gail MH, Brinton LA, Byar DP, et al. Projecting individualized probabilities of developing 457 breast cancer for white females who are being examined annually. Journal of the National Cancer 458 Institute 1989;81:1879-86. 459 16. Hölzel D, Eckel R, Bauerfeind I, et al. Improved systemic treatment for early breast cancer 460 improves cure rates, modifies metastatic pattern and shortens post-metastatic survival: 35-year 461 results from the Munich Cancer Registry. Journal of cancer research and clinical oncology 462 2017;143:1701-12. 463 17. Chlebowski RT, Rohan TE, Manson JE, et al. Breast Cancer After Use of Estrogen Plus 464 Progestin and Estrogen Alone: Analyses of Data From 2 Women's Health Initiative Randomized 465 Clinical Trials. JAMA oncology 2015;1:296-305. 466
. CC-BY-NC-ND 4.0 International licenseIt is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 7, 2020. .https://doi.org/10.1101/2020.04.04.20050708doi: medRxiv preprint

15
18. Chlebowski RT, Anderson G, Aragaki A. Long-term influence of estrogen plus progestin and 467 estrogen alone use on breast cancer incidence: The Women's Health Initiative randomized trials 468 SABCS Abstract 2019;GS5-00. 469 19. Chlebowski RT, Manson JE, Anderson GL, et al. Estrogen plus progestin and breast cancer 470 incidence and mortality in the Women's Health Initiative Observational Study. Journal of the National 471 Cancer Institute 2013;105:526-35. 472 20. Ravdin PM, Cronin KA, Howlader N, et al. The decrease in breast-cancer incidence in 2003 in 473 the United States. The New England journal of medicine 2007;356:1670-4. 474 21. Jemal A, Thomas A, Murray T, Thun M. Cancer statistics, 2002. CA: a cancer journal for 475 clinicians 2002;52:23-47. 476 22. Hersh AL, Stefanick ML, Stafford RS. National use of postmenopausal hormone therapy: 477 annual trends and response to recent evidence. Jama 2004;291:47-53. 478 23. Beral V, Peto R, Pirie K, Reeves G. Menopausal hormone therapy and 20-year breast cancer 479 mortality. Lancet 2019;394:1139. 480 24. Dietel M, Lewis MA, Shapiro S. Hormone replacement therapy: pathobiological aspects of 481 hormone-sensitive cancers in women relevant to epidemiological studies on HRT: a mini-review. 482 Hum Reprod 2005;20:2052-60. 483 25. Wunderle M, Pretscher J, Brucker SY, et al. Association between breast cancer risk factors 484 and molecular type in postmenopausal patients with hormone receptor-positive early breast cancer. 485 Breast cancer research and treatment 2019;174:453-61. 486 26. Hofseth LJ, Raafat AM, Osuch JR, Pathak DR, Slomski CA, Haslam SZ. Hormone replacement 487 therapy with estrogen or estrogen plus medroxyprogesterone acetate is associated with increased 488 epithelial proliferation in the normal postmenopausal breast. The Journal of clinical endocrinology 489 and metabolism 1999;84:4559-65. 490 27. Shapiro S, Farmer RD, Seaman H, Stevenson JC, Mueck AO. Does hormone replacement 491 therapy cause breast cancer? An application of causal principles to three studies: Part 1. The 492 Collaborative Reanalysis. The journal of family planning and reproductive health care 2011;37:103-9. 493 28. Gerstung M, Jolly C, Leshchiner I, et al. The evolutionary history of 2,658 cancers. Nature 494 2020;578:122-8. 495 29. Sjoblom T, Jones S, Wood LD, et al. The consensus coding sequences of human breast and 496 colorectal cancers. Science (New York, NY) 2006;314:268-74. 497 30. Rudolph A, Hein R, Lindstrom S, et al. Genetic modifiers of menopausal hormone 498 replacement therapy and breast cancer risk: a genome-wide interaction study. Endocrine-related 499 cancer 2013;20:875-87. 500 31. Shapiro S, Farmer RD, Stevenson JC, Burger HG, Mueck AO, Gompel A. Does hormone 501 replacement therapy (HRT) cause breast cancer? An application of causal principles to three studies. 502 The journal of family planning and reproductive health care 2013;39:80-8. 503 32. Hulley S, Grady D, Bush T, et al. Randomized trial of estrogen plus progestin for secondary 504 prevention of coronary heart disease in postmenopausal women. Heart and Estrogen/progestin 505 Replacement Study (HERS) Research Group. Jama 1998;280:605-13. 506 33. Haas JS, Kaplan CP, Gerstenberger EP, Kerlikowske K. Changes in the use of postmenopausal 507 hormone therapy after the publication of clinical trial results. Annals of internal medicine 508 2004;140:184-8. 509 34. Sprague BL, Trentham-Dietz A, Remington PL. The contribution of postmenopausal hormone 510 use cessation to the declining incidence of breast cancer. Cancer causes & control : CCC 2011;22:125-511 34. 512 35. Chlebowski RT, Kuller LH, Prentice RL, et al. Breast cancer after use of estrogen plus progestin 513 in postmenopausal women. The New England journal of medicine 2009;360:573-87. 514 36. Narod SA. Hormone replacement therapy and the risk of breast cancer. Nature reviews 515 Clinical oncology 2011;8:669-76. 516
. CC-BY-NC-ND 4.0 International licenseIt is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 7, 2020. .https://doi.org/10.1101/2020.04.04.20050708doi: medRxiv preprint

16
37. Kerlikowske K, Miglioretti DL, Buist DS, Walker R, Carney PA. Declines in invasive breast 517 cancer and use of postmenopausal hormone therapy in a screening mammography population. 518 Journal of the National Cancer Institute 2007;99:1335-9. 519 38. Beral V. Breast cancer and hormone-replacement therapy in the Million Women Study. 520 Lancet 2003;362:419-27. 521 39. Engel J, Weichert W, Jung A, Emeny R, Holzel D. Lymph node infiltration, parallel metastasis 522 and treatment success in breast cancer. Breast (Edinburgh, Scotland) 2019;48:1-6. 523 40. Pinkerton JV. Hormone Therapy for Postmenopausal Women. The New England journal of 524 medicine 2020;382:446-55. 525 41. Burger HG, MacLennan AH, Huang KE, Castelo-Branco C. Evidence-based assessment of the 526 impact of the WHI on women's health. Climacteric : the journal of the International Menopause 527 Society 2012;15:281-7. 528
529
. CC-BY-NC-ND 4.0 International licenseIt is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 7, 2020. .https://doi.org/10.1101/2020.04.04.20050708doi: medRxiv preprint