Embed Size (px)
Citation preview

Hormone Independent
Metastatic Breast Cancer
Anne Moore, MD
Attending Physician, New York Presbyterian Hospital
Professor of Clinical Medicine
Weill Cornell Medical College
New York

Hormone Independent MBC Definition
• Metastatic breast cancer
– Triple negative from diagnosis
– Biomarkers changed at time of metastatic disease
– ER+ or Her 2+ that is refractory to targeted therapy

Stage IV disease
• Screening for metastases with markers or annual scans not recommended by ASCO guidelines
• Metastatic disease usually found by patient in between doctor visits-lump, pain, other routine exams (eg, pre-op chest xray)
• 3- 5% of newly diagnosed breast cancer patients present with metastatic disease

Stage IV breast cancer Initial work up when metastatic disease is suspected
• History and physical examination
• Routine labs (markers may help)
• Imaging: Bone scan + CT of c-a-p or FDG PET/CT
• Biopsy first recurrence if possible – To establish cancer vs. benign
– To establish metastasis from breast cancer
– To determine ER/PR/HER2
NCCN guidelines 3.2014

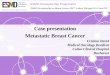
Changes in estrogen receptor (ER), progesterone receptor (PgR), and HER2 between the
original pathology report of the primary tumor and the metastasis.
Amir E et al. JCO 2012;30:587-592
©2012 by American Society of Clinical Oncology

Metastatic breast cancer is an incurable disease
Goals of treatment
ASCO guidelines
• To prolong survival
• To palliate symptoms
• To optimize quality of life
Are these in the same order for every patient?
For every treating physician?
ASCO guidelines 2014

Metastatic breast cancer
• What is the average survival after a diagnosis of stage 4 breast cancer?

ECOG adjuvant chemotherapy trials Survival after recurrence
• Almost 14, 000 women enrolled in adjuvant chemotherapy trials: 1978 to 1999
• 24.4 % developed metastatic disease
• Median survival after recurrence was 20 months
Tevaarwerik 2013 Cancer 119:1140

ECOG adjuvant chemotherapy trials Survival after recurrence
• Survival for the general population of metastatic patients has not improved over time
• Inferior survival associated with: – Shorter disease free interval (< 3 years)
– ER and PR negative disease
– Number of positive nodes at diagnosis
– Black race
Tevaarwerik 2013 Cancer 119:1140

ECOG adjuvant chemotherapy trials Longer disease free interval from primary dx is better
Tevaarwerik 2013 Cancer 119:1140

ECOG adjuvant chemotherapy trials ER negative has worse survival
Tevaarwerik 2013 Cancer 119:1140

ECOG adjuvant chemotherapy trials Longer disease free interval is better
ER/PR negative
Tevaarwerik 2013 Cancer 119:1140
Disease free interval less than 3 years- no improvement whether diagnosed in ‘78 or ‘04
Disease free interval more than 3 years- more recent cases doing better
Possible Trastuzumab effect?

Treatment for triple negative metastatic breast cancer
• Surgery
– Oligometastasis-
• Is there a oligometastatic phenotype? Are these the “extraordinary responders?”
• Should we screen for metastasis?
– Mastectomy with stage IV disease?
• Tata Memorial Hospital study-No effect on survival

Treatment for triple negative metastatic breast cancer
• Surgery
– Oligometastasis-
• Is there a oligometastatic phenotype? Are these the “extraordinary responders?”
• Should we screen for metastasis?
– Mastectomy with stage IV disease?
• Tata Memorial Hospital study-No effect on survival
• Radiation therapy
– Palliation

Treatment for triple negative metastatic breast cancer
• Surgery – Oligometastasis-
• Is there a oligometastatic phenotype? Are these the “extraordinary responders?”
• Should we screen for metastasis?
– Mastectomy with stage IV disease? • Tata Memorial Hospital study-No effect on survival
• Radiation therapy – Palliation
• Supportive care – Treatment of bone metastasis: Pain relief and decrease fractures
• Bisphosphonates • RANK ligand inhibitor-denosumab

What is the best way to treat the disease?

High dose chemotherapy and bone marrow or stem cell transplant does not cure metastatic breast cancer

ASCO Guidelines

ASCO guidelines: For hormone independent metastatic breast cancer
• Sequential single agent chemotherapy is recommended
• Combination chemotherapy may be used for patients who present with rapidly advancing disease where time may allow only one potential chance for treatment

Best evidence: E1193 Trial • Large published randomized trial comparing
single agent to combination therapy in 1st line metastatic patients – Used our most active drugs: doxorubicin and
paclitaxel – alone or in combination
– Cross-over mandated at time of progression
– Phase III, cooperative setting
Sledge, G. et al. JCO 21:588-592 (2003)

Results E1193
Response (CR + PR)
Median TTF (Months)
Median Survival
(Months)
DOX 36 6 18.9
Paclitaxel 34 6 22.2
Dox/Pac 47 8 22
Sledge, G. et al. JCO 21:588-592 (2003)

There are some doublet chemotherapies that have shown
superior survival

Combination taxane chemotherapy
options
Line of
Rx
ORR
(%)
TTP
(mo)
OS
(mo)
X vs. XD (511) 1st – 3rd
Capecitabine (X) 30% 4.2 11.5
Cape/docetaxel (XD) 42%* 6.1* 14.5 *
T vs. GT (529) 1st
Paclitaxel (T) 26.9% 4.0 15.8
Gemcitabine/Paclitaxel
(GT) 43.1%* 6.1* 18.6*
O’Shaughnessy J JCO 2002;20:2812
Albain K JCO 2008;26:3950
Doublet chemotherapies that have shown superiority

ASCO guidelines: Metastatic breast cancer
No single agent is superior –several active agents appropriate for first line chemotherapy

Single vs Combination regimens No compelling evidence that combination regimens
are superior to sequential single-agent regimens
SINGLE AGENT • Anthracyclines Doxorubicin Pegylated liposomal doxorubicin • Taxanes Paclitaxel Albumin bound paclitaxel Docetaxel • Antimetabolites Capecitabine
Gemcitabine • Non-taxane microtubule agents Vinorelbine Ixibepilone Eribulin

News from WebMD: March 2011

Phase III EMBRACE Trial of Eribulin Versus Treatment of
Physician’s Choice for Heavily Pretreated MBC
Twelves et al. J Clin Oncol 2010; 28(suppl):958s (abstract CRA1004).
Eligibility criteria:
•Locally recurrent or
metastatic breast cancer
•2-5 prior chemotherapies:
– ≥ 2 for advanced disease
– Prior anthracycline and
taxane
•Progression ≤ 6 months
since last chemotherapy
•Neuropathy grade ≤ 2
Treatment of Physician’s Choice (TPC) Any monotherapy approved for treatment of cancer or supportive care only
Eribulin mesylate 1.4 mg/m2, days 1, 8
q 3 weeks
R
A
N
D
O
M
I
Z
E
Primary endpoint: OS
Secondary endpoints: PFS, ORR, safety
2 : 1)

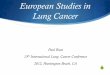
Phase III EMBRACE Trial: Overall
Survival
Cortes J Lancet 2011;377:914
OS: 13.1 vs 10.7 mos
PFS: 3.7 vs 2.2 mos

• In this day of “personalized medicine” with next-generation sequencing etc, can we match the chemotherapy to the individual tumor?

ASCO guidelines: Metastatic breast cancer
• “Chemotherapy regimens should not be tailored to specific subtypes such as triple negative or lobular”
• BUT we should look for signals to pursue…
• We are looking for true synergistic interaction that may have the potential to increase survival

ERIBULIN 301 STUDY Eribulin vs Capecitabine for patients previously treated with
anthracyclines and taxanes
Kaufman et al, SABCS 2012 Abstr S6-6

ERIBULIN 301 STUDY Eribulin vs Capecitabine for patients previously treated with
anthracyclines and taxanes
Kaufman et al, SABCS 2012 Abstr S6-6

Is this a signal to listen to?

How long to continue chemotherapy in the responding/stable patient?

ASCO guidelines: Metastatic breast cancer
Chemotherapy should be continued until progression of disease as tolerated because it modestly improves overall survival and substantially improves progression free survival…. Balance against toxicity and quality of life

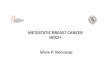
Optimal Duration of First Line Chemotherapy for MBC
Progression Free Survival
Gennari A et al. JCO 2011;29:2144-2149
11 trials
2,269 pts

ASCO Guidelines
• With regard to targeted agents, the role of bevacizumab is controversial and this therapy should only be considered with single-agent chemotherapy when there is life-threatening disease..

Treatment for triple negative metastatic breast cancer
Targeted therapy
Bevacizumab - Approved in 2008 for first line therapy with paclitaxel in metastatic Her2 negative breast cancer

Treatment for triple negative metastatic breast cancer
On June 29, 2011 the FDA’s Oncologic Drugs Advisory Committee removed the approval based on follow up studies showing a small effect on tumor growth with no benefit to overall survival or QOL

Are we rethinking VEGF inhibition for metastatic breast cancer?
ESMO 2014
2 studies for metastatic disease, her 2 negative, ER/PR negative or positive (most had been treated with hormonal therapy) TANIA (494 pts): After initial response to bevacizumab + first line chemotherapy, pts showed benefit to continuing bevacizumab with second-line chemotherapy as compared to second-line chemotherapy alone
IMELDA (284 pts): After response or stable disease on bevacizumab and docetaxel, there was improved PFS and OS in those pts who received maintenance with bevacizumab and capecitabine as compared to maintenance bevacizumab alone.
Lancet Oncology 15: October 2014

Are we rethinking VEGF inhibition for metastatic breast cancer?
ESMO 2014
2 studies for metastatic disease, her 2 negative, ER/PR negative or positive (most had been treated with hormonal therapy) TANIA (494 pts): After initial response to bevacizumab + first line chemotherapy, pts showed benefit to continuing bevacizumab with second-line chemotherapy as compared to second-line chemotherapy alone
IMELDA (284 pts): After response or stable disease on bevacizumab and docetaxel, there was improved PFS and OS in those pts who received maintenance with bevacizumab and capecitabine as compared to maintenance bevacizumab alone.
These papers were discussed by Dr Hope Rugo who “concluded that at present the role of bevacizumab is unclear in breast cancer.”
Lancet Oncology 15: October 2014

What to do with the “stage 4 ned” patient?
• 52 yo woman has a chest wall recurrence 3 years after mastectomy for stage 2A triple negative breast cancer treated with adjuvant chemorx
• The mass is excised (triple negative) and RT is given
• “Stage 4 ned”—What to recommend

Aebi,S SABCS 2012

Benefit of chemotherapy limited to ER/PR negative

Future Therapies
• Clinical trials.gov: 400 studies currently recruiting and open for MBC
– TN specifically: 41 studies
– Many targeting specific pathways related to molecular profiling and the biology of the disease
PARP inhibitors GPNMB (CDX-011) PIK3CA
HSP 90 Angiogenesis Aurora Kinase
MET FGFR mTOR
ADC (folate) EGFR HER3
ɣ-Secretase estradiol JAK2
LIV-1 AKT Src

[TITLE]

THANK YOU!