-
,
Dr. Pllnkaj Juneja
Dr. Prabhuraj B. Kambalya l
Abstract
Key Words
AN OVERVIEW OF THE ROLE OF DRUGS AND SYSTEMIC FACTORS ON
ORTHODONTIC TOOTH MOVEMENT Authors: Dr. Pankaj Juneja B.D.S.
(M.D.S.) Postgraduate student, Department of Orthodontics and
Dentofacial Orthopedics, Co llege of Dental Sciences, Davangere,
Karnataka. Email : drpankaL1 [email protected] Phone: +91-
9964143808
Dr. G. Shivaprakash B.D.S., M.D.S. Professor and Head,
Department of Orthodonti cs and Dentofacial O rthopedics, College
of Dental Sciences, Davangere, Karnataka. Email :
[email protected] Phone: +91- 9844041 620
Dr. Prabhuraj B. Kambalyal B.D.S., M.D.S. Assoc iate Professor,
Department of Orthodontics and Dentofacia l Orthopedics, College of
Dental Sc iences, Davangere, Karnataka. Email : prabhurajkambalya
[email protected] Phone: +91- 944811 0394
The specialty of Orthodontics is based on the fact that it is
poSSible, by applying appropriate forces, to move the teeth through
the alveolar bone of the jaws. Orthodontic tooth movement and the
concomitant bone remodeling process are dependent on various local
and systemic factors like age, nutrition, consumption of drugs etc.
Orthodontic patients may be affected by systemic diseases that
might need treatment with drugs that could possibly affect bone
metabolism. Patients undergOing orthodontic treatment can
experience significant levels of pain. Analgesics are commonly
recommended for the control of such orthodontic pain.
This article reviews all the existing published biomedical
literature on the effects of some commonly used drugs by the
patients for the relief of orthodontic pain and treatment of
systemic conditions known to affect the bone tissue and thereby
influencing the rate of orthodontic tooth movement. An attempt has
been made to propose a complete picture and orient the reader for
the better understanding of some commonly used pharmaceutical
products.
This is considered essential in order for the orthodontist to
take into account all factors related to the therapy and to select
the best therapeutic strategy in every individual patient keeping
the mechanics as simple as possible.
orthodontics, force, drugs, systemic, tooth movement.
36
-
INTRODUCTION: The aim of orthodontic trea tment in the movement
of teeth through bone is to obtain a more perfect dental occlusion.
Orthodontic tooth movement has been defined by Proffit ' as the
result of a biologi ca l response to interference in the
physiologica l equilibrium in the dentofacial complex by an
externally applied force.
Nowadays, attention is mainly focused on the relation of
orthodontic tooth movement to the applied force. The contro l of
pain during orthodontic treatment is of interest to both clinician
and patients. Prescription and over th e co unter analges ics are
common ly recommended for orthodonti c pain. Interestingly, despi
te cli nica l evidence that patients experi ence pain after
orthodontic procedures, there have been few controlled studies that
address the use of analgesics to contro l post appointment
orthodontic pain.
The objective of this review is to discuss current data concern
ing the mechanism of action and effects of some common ly used
pharmaceutica l products and systemic factors known to affect bone
ti ssue and thereby influenc ing the rat e o f tooth movement. This
is considered essentia l in order for the orthodontist to take into
account all factors related to the therapy and to
,. _=!n~
select the best therapeutic strategy in every individual patient
keeping the mechanics as simple as possible.
An Overview of biological basis of orthodontic tooth movement :
In a recent review on the current concepts in the biology of
orthodontic tooth movement Richard and Malcolm' said that five
micro-environments are altered by O rthodonti c for ce - ex trace
llul ar matri x, ce ll membrane, cytoskeleton, nuclear protein
matri x and genome. Cel l membrane receptor li gand docking is an
important initi ator of signal transdu cti on and a discovery
target for new bone enhancing drugs. Despite progress is identifi
cation of regulatory molecules, the genetic mechanism of
"orchestrated synthesis" between different cell s, tissues and
systems remain largely unknown.
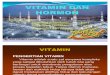
Ei cosa noids/A utoco id s are bi o logical l y ac tive
derivatives of 20 ca rbon atom Polyunsaturated fatty acids (PUFA)
that are released from cell membrane phospholipids. There are two
major lipid derived autocoids :
1) Prostaglandins (PG's), and 2) Leucotrienes (L T's)
Membrane phospholipid
~ Cyclo-oxygenase
Isomerase
PGE,
PGD,
PGF, ..
~ PGG,
PGH, I . ~
Thromboxane synthase
TXA, TXB,
Chemical or mechanical st imuli 1 Phospholipase A ~
Arachidonic Acid -------,~
~ Prostacycl i n
synthase
PGL
6 KetoPGF, ..
..
12 HPETE t
12 HPETE
Biosynthesis of PG 's and L T's'
37
Lipo-oxygenase I
5 HPETE-5 HETE
..
L TB,
~ L TA,
I
LTC,
LTD, LTE, LTF,
-
Cyclooxygenase is known to exist in two isoforms Cox-I and Cox-2
. While both isoforms catalyses the same reactions, cox-1 is
constitu tive enzyme in most cells. O n the other hand cox-2 is
normall y present in insignifi cant amounts but is inducible by
cytokines, grow th fa ctor s and o ther sti mul i during the
inilammatory response. It is believed that eicosanoids produced by
cox- 1, participate in physiological (house keeping) function such
as secretion of mucous for protection of gastric mucosa etc. while
those produced by cox-2 lead to inflammatory and other pathological
changes.
Tooth movement during orthodontic treatment requires remodeling
of periodontal ligament tissues, especia ll y
Table I
in the alveolar bone. Force application disrupts the equilibrium
that ex ists between bone formation on the pressure side and more
bone formation than resorption on tension side. Resorption of bone
by osteoclasts is coupl ed with subsequ ent bone formation by
osteoblasts. Loca l and systemic factors' (Table I ) including
cytokines, hormones, growth factors and mechanica l st imulation
activate osteoblasts to produce the receptor activator of NF-a~
ligand (RANKL) which is vital for osteoclasts differentiation and
activit y. RANKL is expressed on the surface of osteoblastic cell s
and bone marrow stromal cell s and binds to the RANK receptor on
the surface of osteoclastic precursors, thereby stimulating the
differentiation and activation of osteoclasts.
Faclors affecling bone remodeling process Hormones and systemic
faclors
-
-
-
-
-
-
-
-
Growth factors -
-
-
-
Cytokines -
-
-
-
-
Colony stimulating factors -
-
-
Others -
-
-
Intracellular secondary messengers play an important role in the
differentiation of osteoclasts from monocytes in bone resorption
during force app li catio n. Davidovitch et ai' measured cGMP and
cAMP levels in the alveolar bone of cats under orthodontic
treatment and reported that Ca" , cGMP and cAMP acts as a key
mediators or secondary messengers in the function of many drugs and
hormones.
38
PTH Ca lcitosin Insulin Growth hormone Vitamin 0 Glucocorti
coids Sex steroids Thyroid hormones
Insulin like GF I and II TGF~ Fibroblast growth factor Platelet
derived growth factor
IL-1,4,6, 11, 13, 18 TNF Osteoclast differentiating factor
Interferon y Osteoprotegrin
M-CSF G-CSF GM-CSF
Prostaglandins Leukotri enes Nitric ox ide
It is now clear that OTM is influenced both by drug and the
systemic factors. An attempt has been made to review the past and
present literature published in various articles in different
journals on the factors that tend to influence the OTM, and same wi
ll be discussed as presented in Tab le II and Table III.
-
Table II Effects of drugs on tooth movement
Drug Effects on bone tissue Effects on tooth Mechanism of
movement action
1) NSAIDS - Decreased bone - Decreased rate of - Inhibition of -
Aspirin resorption tooth movement cyclooxygenase -
Aceta minophen enzyme. - Ibuprofen - Rofecox ib - Valdecoxib -
Celecoxib
2) Ecosanoids I Autocoids - Increased bone - Increased rate of -
Increases cAMP and - Prostaglandins resorption tooth movement cGMP
levels.
- Leukotrienes - Activates osteoclasts.
3) Bishosphonates - Decreased bone - Decreased rate of - Inhibit
bone resorption tooth movement turnover.
- Decreases root - Increases bone resorption mineral density
4) Fluorides - Increased bone mass - Decreased rate of -
Increases bone and mineral denSity tooth movement. mass/density
- Decreased bone resorption
5) Corticosteroids - I ncreased bone - Increased rate of -
Inhibit osteoblastic resorption tooth movement function.
- Decreased bone - Greater potentia l for - Decreases bone
formation relapse as movement Formation.
is less stable.
6) Epidermal growth factor - Increased bone - Increased rate of
- Enhances osteoclats (EGF) resorption tooth movement.
recruitment.
7) Osteoprotegrin gene - Decreased bone - Decreased rate of -
Inhibits RANKL transfer resorption tooth movement mediated
osteoclastogenesis.
8) Echistatin (RGD peptide) - Decresed bone - Decreased rate of
- Inhibits Integrin resorption tooth movement receptors.
9) Tezosentan - Increased bone - Increased rate of - Enhances
bone resorption tooth movement resorption via ETA
receptors.
Table III Effects of systemic factors on tooth movement
Hormone Effects on bone tissue Effects on tooth movement
Mechanism of action 1) Estrogen - Decreased bone resorption -
Decreased rate of tooth movement - Inhibits cy tokine involved
in
bone resorpti on. 2) Androgen - Decreased bone resorption -
Decreased rate of tooth movement. - Enhances DNA transcription. 3)
Vitamin D - Increased bone resorption - Increased rate of tooth
movement. - Activa tes DNA and RNA
- Enhances reestablishment of w ithin target cell s. supporting
tissues
4) Thyroid - Increased rate of bone - Increased rate of tooth
movement - Activates a spec ific DNA remodeling
- Decreases root resorption sequence ca lled Thyroid hormone
response element.
5) Parathyroid - Increased rate of bone - Increased rate of
tooth movement. - Increases cAMP formation and resorption
intracellular Ca in ta rget cells
39
-
1. EFFECT OF DRUGS ON TOOTH MOVEMENT; NSAID'S: All drugs grouped
in this class have analgesic , antipyreti c and anti -i nflammatory
actions in different measures. They are also ca lled non narcoti c,
non opioid, or aspiri n like analgesics . They act primarily on
peripheral pain mechanisms but also in CNS to raise pain threshold,
by inhibition of cyclo-oxygenase, which modulates the transforma
tion of PG's from arachidonic acid in the cellular plasma
membrane.
They are the most common group of medicati ons used in
orthodontics for relief of pain.b" . Numerous studi es eva luated
the pain reducing effects of va rious NSAIO's. Then drugs have
become the focus of recent research in orthodontics.
Amongst the earliest studies ca rried out Chumbley et ai" eva
luated the effect of indomethacin (an aspirin like drug) and
recommended that aspirin like drugs not to be admi nistered to
patients undergoing orthodontic treatmen t as it may extend the
treatment time. W alker et al '" eva luated the impairment of
O.T.M. ca used by NSAIO's and results showed that they can impair
O,T.M and until long term human data are obtain ed, acetaminophen
remains an appropriate alternative to NSAIO's. Similar results were
found by Arias et al" who compared aspirin, acetaminophen and
ibuprofen and found that acetaminophen did not affect OTM, Even
Roche et al" concluded that acetaminophen has no effect on rate of
OTM, Kehoe et al" also suggested acetaminophen as the analgesic of
cho ice for minor discomiort associated w ith orthodontic
treatment. But in a recen t contrasting study Brad ley et al"
compared Ibuprofen and paracetamol for the control of pain and
iOlll1d that pre-operative and post-operative Ibuprofen to be more
effective than paracetamol. In another study by Polat et al1 ' ,
Naproxem sodium was found to have lower levels of pa in than
patients taking ibuprofen, Moreover the use of over the counter
drugs have also shown aberrant remodeling of th e periodontal
vasculature affecting the tooth movement, Kyrkanides et al '"
investigated the effects of indomethac in on co ll agenase acti
vity and proco ll agen synthesis. Cyclooxygenase inhibit ion
resulted in exacerbation of IL-l beta mediated collagenase B
(MMP-9l production and acti vity, as well as alterati on oftype IV
procollagen synthesis levels by endothelial cells in vi tro. The
studies mentioned above showed that NSAIO's effecti vely reduce the
pain and discomfort caused by orthodontic tooth movement but these
drugs may also aiiect the sequence of tooth movement by inhibiting
or at least by reducing the associated inflammatory and
40
bone resorption process. O ne approach to dea l with this is the
use of selective cox-2 inh ibitors, also cal led as cox ibs, which
are replacing conventiona l NSAIO's, In comparison to NSAIO's,
Cox-2 inhibitors have longer dose interva ls, different side effect
profile, similar onset of action and similar analgesic effect.
Sari et al" showed that the inhibition effect of aspirin on PGE,
was more than that of Rofecoxib, In another study Young et al "
concluded that va ldecoxib may be a better approach to prevent
discomfort of initial archwire placement. In a previous study by
Carlos et al " found no substantial advantage in using a selective
cox-2 inhibitor compared wi th non specific cox inhibitors. But in
a recent study Carlos et al' evaluated orthodontic tooth movement
after different coxib therapies and concluded that celecoxib and
parecox ib, but not rofecoxib, seem appropriate for discomfort and
pain relief while avo iding interference during tooth movement.
Gameiro et al" eva lauted the effects of short and long term
celecoxib on orthodontic tooth movement and concluded that although
celecox ib administration did not affect the number of osteoclasts,
the osteoclasts activity might be reduced, which could explain the
inhibition of tooth movement observed,
However the effect of these drugs on orthodontic root resorption
is not well understood. Gameiro et al" did histologica l analysis
of orthodontic root resorption treated with celecoxib and found
that short and long term celecox ib did not suppress the root
resorption,
Therefore, it is recommended that patients undergoing
orthodontic treatment should be advised not to take these over the
counter drugs w ithout the dentist' s prior knowledge,
EICOSANOIDS / AUTOCOIDS : Prostaglandins: Arachidonic acid is
metaboli zed by cyclooxygenase resulting in prostaglandin
production ." Experiments have shown that PG's are an important
mediators of mechanica l stress during OTM, Ngan et al" observed
that PG 's cause hyperalgesia by facilitating pain stimulus and
increasing the effects of hi stamine and bradykinin , Chao et al"
observed that PGE, injection increased the number of osteoclasts in
pdl membrane. Oavidovitch et ai' demonstrated in vitro direct
effect of PG's on bone resorption along with increase in cAMP and
cGMP levels. Sandy et al" fou nd that inhibition of PG synthes is
by flurbiprofen, a PG inh ibitor, showed inhibition of osteoclast
activity and bone resorption. In another study by Gurton et al"
found that PGI, and TXA, analogs increase the number
-
of multinuclear osteoclasts, osteoclastic bone resorption and
rate of OTM. Si milar results were also shown by Yamasaki et al.
"
Studi es were also conducted in order to eva luate the effect of
PG's on root resorption. Leiker et al" found that the amount of
root resorption did increase w ith the use of PG injec tion s,
specifi ca ll y PGE, . In a contrasting study by Boekenoogen et al
'" conc luded that PGE, appeared to have no effect on the number or
depth of resorption lacunae. In a simi lar study Brudvick et al "
found no significant difference in root resorption but trend
towards more root resorption was seen on teeth where PGE, injecti
on had been performed. In a recent study Seifi et al" showed the
importance of Ca" ions worki ng in association wi th PGE, in
stabili zing root resorption while significantly increased OTM.
Leucotr ienes : They are also metabolites of arachido ni c ac id
, produced by lipo-oxygenase enzymes" They are also important
mediators of OTM. Their role in OTM is clearly demonstrated when
inhibitors of leucotrienes are used in different experiments.
It is a well known observation that inhibition of one pathway of
arachidonic ac id will shunt the effect into an increase in the
conversion via the other pathway. Mohammed et al]) investigated
role of a L T inhibitor AA861 in OTM and found that it caused
signifi cant LTB, inhibition and simultaneous increase in PGE,
production, suggesting L T role in mediating OTM. However inspite
of - PG levels, a selective inhibition of L T synthes is caused a
Significant reduction in tooth movement.
Consequ entl y leucot ri ene inhibitors ca n delay orthodont ic
trea tment, whereas leuco tri enes and prostaglandins can have
future appli ca tions that could result in enhanced tooth movement.
11
BISPHOSPHONA TES: The pharmaco logic agent bisphosphonates are
analogues of pyrophosphate. Recentl y" they have received mu ch att
enti o n in denta l l iterature. Bisphosphonates in oral or IV
forms are used to that va ri ous diseases such as certain ca ncer,
bone and cal c ium related disorders, osteoporosis etc.
Bisphosphonate inhibit bone turnover and result in increased bone
mineral densi ty. The most serious side effect of Bisphosphonate
treatment is osteonecrosis of the mandib le or the maxilla
represented by exposed non hea li ng bone. O ther related
complications include dec reased bone hea ling and an inhibition of
orthodontic tooth movement.
41
Sato Y et al 15 did a study to clarify the effects of Bi
sphosphonate administration on struc ture and function of
osteoclasts in alveolar bone resorption during experimental tooth
movement and found that BP Significant ly impair the osteoclast
structure and reduces express ion of both vacuolar type H(+) ATPase
and cathepsin K in osteoclasts during tooth movement. Liu et al'6
also suggested the inhibitory effect of clodronate on tooth
movement and osteoclasts may be due to inhibition of cox-2
dependent PGE, production and RANKL expression in pdl cells.
Root resorption associated with tooth movement in an un so lved
probl em in orthodontics. If such root resorption could be
prevented, it would be an important co ntribution towa rd s reduci
ng risk factors in orthodontic treatment. The use of BP to reduce
the amount of inflammatory root resorption has been investigated
and were found to be effecti ve in thi s regard.
Liu et al37 found that local clodronate inhibited root
resorption incident to tooth movement and suggested it to be a
usefu l therapeutic adjunct in orthodontic treatment. Igarashi et
al " eva lu ated topi ca l administration of residronate on root
resorption and found that it did not appear to inhibit the repair
process of root resorption .
The clinical utility of Bisphosphonates resides in their ability
to inhibit bone resorpti on. In Orthodontics, undes irable movement
of anchor teeth during tooth movement and relapse of moved teeth
after treatment are the main cause of unsuccessful results. If
these tooth movements could be prevented with pharmacologica l
agents, a less complex orthodontic force system and less extensive
retention wou ld be required.
Igarash i et al" eva luated the anchorage and retentive effects
of a BP (AHBuBP) on tooth movement in rats and concluded that it
could be useful in enhancing anchorage or retaining teeth . Kim et
al'" eva luated the effect of Bisphosphonate administration on
osteoclastic bone resorpti on during relapse and found that it
decrease the extent of initial relapse via mechanism involving
impai rment of the structure and resorption functions of
osteoclasts.
In another study by Adachi et al", found that the top ica l
admini stration of residronate may be helpful in anchoring and
retai ning teeth under orthodontic treatment.
Therefore it is imperative that Bisphosphonate medica l
screening, pat ient counseling, informed con cent, and changes in
treatment planning shou ld be considered for every patient by the
orthodontist."
-
FLOURIDE: The effect of fluoride on bone metabolism has been
well reported in the medica l field, because it has been used as a
drug by itself or as an adjunct in the treatment of osteoporosis.
Fluoride treatment results in an increase in bone mass beca use of
the stimulati on of bone formation .
Hellsing et al" eva luated the effect of fluoride on OTM and
found that the veloc ity of TM is influenced by hormones as well as
trace elements. In another study use of F' as a variable was found
to increase the mean osteocalcin concentration" (a bone protein
that has been used to mark bone turnover). Foom et al" eva luated
the effect of systemic F' in take on root resorpt ion and fo und
that F' reduces the size of resorption craters, but the effect is
va riable.
The clin ical util ity of F' agents includes caries preventive
treatment protocols such as fo llowing oral prophylax is, proxima l
strippi ng/sli c ing etc . may increase the orthodont ic treatment
time due to its anabolic effects on bone, as fl uoride increase
both bone mass and density.
CORTICOSTEROIDS: Orthodontic pat ients may be affected by
systemic diseases that might need treatment w ith drugs that could
po ss ibly affec t bo ne metabo li sm. Sy nth et i c
corticosteroids have been used in therapeutic regimens for the
treatment of a w ide variety of ailments ranging from arthri tis to
renal, collagen, allergic and neoplastic diseases. Supra-phys
iologic doses of these drugs when administered induce the same
osteoporosis found in naturall y occurr ing status of hypercorti so
li sm." Corti costero ids inh ib it osteobl as ti c fun cti on by
mediating its effects on osteoblast and its precursors resulting in
decreased bone formation. The latter may be due to elevated PTH
leve ls caused by direct inhibition of Cal< absorption by the
steroids. End result being increase in bone resorption. Aschroft et
al" found th at rabbi ts subjected to cor ti costero ids induced os
teoporosis underwent more rapid O .T.M and subsequent relapse.
Mavragani et al" found that low dose doxycyl ine may have an
inhibitory effect on orthodont ica lly induced resorptive
activity.
In a recent study Verna et al" investigated the effect of ac ute
and chron ic corti costero id trea tment on orthodont ica ll y
induced root resorption and found more root resorption in acute
group. When compared to chronic group and suggested that it may be
due to lack of ba lance between blastic and clastic activiti es
during initia l phase of drug administration.
42
Because acute corticosteroid ingestion reduces bone turnover, in
these patients orthodontic treatment might best be postponed until
a time the patient is free of the drug.50Chronic stero id ingestion
leads to an increased bio log ica l reac ti on to mechani ca l
perturbat ion indicating that the Orthodontic force level should be
reduced and controlled more frequently in patients on chronic
steroid treatment. 50 Moreover specific attention must be paid to
the retention protocol as the tooth movement is less stable. As a
consequence, carefu l monitor ing of pati ents undergoi ng cort
icostero id treatment is suggested.
MISCELLANEOUS: 1) Epidermal growth factor : Recently the use of
epidermal growth factor (EGF) to develop a suitable environment and
stimulate selective d ifferentiation and proli feration has been
proposed. It has also been suggested that it may be involved in
responses of osteoblasti c cell li ves to mechanica l stimuli.
Saddi et al" found that loca l administration of EGF located w ith
in liposomes had an additive effect on the rate of osteoclasts
recruitment, producing faster bone resorption and tooth
movement.
2) Biological agents - Relaxin: Using biologica l agents to
modify the rate of tooth movement have been shown to be effective
in animals. Relaxin main action is to increase the turnover of
fibrous connecti ve ti ssue. Madan et al" eva luated effect of
human relax in on OTM and found that it does not acce lerate OTM,
it ca n reduce the leve l of Pdl organization and mechanica l
strength and increase tooth mobility at ea rly t ime periods.
3) Osteoprotegrin gene transfer: It has been reported that
osteocl astogenesis is primarily acti vated by the receptor
activator of nuclear factor Ka ppa b li ga nd (RAN KL) and inhi bi
ted by osteoprotegrin (OPG). Pdl cell s which ex ists between teeth
and alveo lar bone, induce osteoclastogenes is in vitro th rough
the up regulati on of RANKL expression via PGE, synthesis w hen
subjected to mechan ical compress ive force.
Kanzaki et al" found significantly d imin ished tooth movement
on loca l O PG gene transfer to pd l ti ssue as it inhibited RANKL
mediated osteoclastogensis and inhibited experimental tooth
movement.
4) Echistatin and RGD peptide : Recently a study done on effect
of echistatin, an Arginine-glycine-aspartic acid peptide by Dolce C
et al" showed that ELVAX loaded w ith RGD peptide which was surgica
ll y implanted next to max illary
-
molars inhibited OTM. The RGD peptide also reduced molar drifts,
therefore it shows the feas ibility of using them to deliver
integrin inhibitors adjacent to teeth to limit loca l tooth
movement in response to orthodontic force.
In another recent study Talic et al" evaluated the effect of
echistatin on orthodontica lly induced root resorption and
concluded that targeting av~3 integrin receptor expressed by
odontocl asts can be effecti ve in reducing root resorption during
tooth movement.
5) Endothelin Antagonist: Tezosentan Endothelin is a cytokine
peptide present in the pdl in physio logica l condit ions. Its
concentration in the pdl doubles after 3 hors of ax ial loading of
a tooth .
In a recent study by Sprogar et al", eva luated the effects of
TBC 32 14, a se lecti ve endothelin ETA receptor antagonist on OTM
in rats and found that H , is involved in OTM probably by enhanci
ng bone resorption via ETA receptors . In another study Drevensek M
et al57 found that Tezosentan, an endothelin antagoni st, enhanced
orthodontic tooth movement in rats.
EFFECT OF SYSTEMIC FACTORS ON ORTHODONTIC TOOTH MOVEMENT:
THYROID AND PARATHYROID HORMONE: The movement of teeth during
orthodontic trea tment requires bo ne rem odelin g. Th e ro le o f
bo ne metabolism, however, in contro lling tooth movement have been
considered secondary to the force applied. This is largely a result
of the difficulty in altering bone metabolism systemica ll y, in
addition to the fac t that the force is the most easil y manipul
ated fac tor . Consequently, several papers have focused on the
changes in bone remodeling in relation to the applied force. In
addition to applied force, tooth movement seems to depend on ca
lcium metaboli sm is alveolar bone. A study by Midgetts" et al
indicated that animals w ith hyperparathyroidism had signifi cantl
y decreased bone density, as well as increased bone remodeling
changes. Engstrom et al" demonstrated that although the level of
PTH in serum plays an important rol e in the regulation of the
resorptive activ ity in bone, a change in serum ca lci um level is
determining fac tor for root resorption . This indicates that
force- induced root resorption is dependent on more than one
endocrine system. In addition to parathyroid hormone, bone resorpti
ve activity is also regulated by L thyroxine. Patient w ith untrea
ted hyperth yro id ism show increased bone resorpti on.'" The
administrati on of high dose o f
43
thyroxine in rats has been shown to increase bone resorption, in
contrast to low dose administrati on, which was found to reduce
peri ostea l resorption."
Po umpros et a l " al so found th at th yrox ine administration
seems to lower the frequency of root resorption in rats. Shi raz i
et alb' eva luated the effect of th yrOid hormone on OTM in rats
and found that administration o f 20/mym/kg i.p. I day L-thyrox ine
Significantl y increased the amount of OTM and the ex tent of root
resorption decreased w ith th yroxine administration.
PTH is secreted by parathyrOid glands, regulated by plasma Ca"
concentration; there is no trophic hormone for it. The PTH receptor
is a G protein coupled receptor which on acti vation increases cAMP
formation and intracellular Ca" in target cells. In bone the target
cells appears to be the osteoblasts because PTH receptors are not
expressed on the surface of osteoclasts. It has been proposed that
PTH-osteoblast complex some how inc reases the acti vity of
osteoclasts as well as the birth rate of bone remodeling units in w
hich osteoclasts precursors are recruited.
Experiments have shown that PTH can induce bone resorption that
would increase the rate of OTM. Soma et al""" eva luated the effect
of loca l and chronic appl ication of PTH on tooth movement and
found that loca l injection of PTH in a slow release formulation is
appli cable to orthodontic therapy.
It is suggested that thyroid and parathyro id function is an
important clini ca l factor in patients undergoing orthodontic trea
tment. Orthodonti st should take a thorough history of the patients
to determine whether they are on any hormonal supplementati on
drugs as it might adversely affect the treatment. Administration of
th y rox ine ca n be considered in some pati ents, especiall y in
those who show beginning root resorption, or those who have low
thyroid function.
VITAMIN D: Vitamin D is the co llecti ve name given to anti
rachitic substances synthes ized in the body and found in foods
activa ted by UV radiation. The ro le of Vit. D in the maintenance
of Ca homeostasis in human bei ngs has been well documented. It is
a steroid hormone Ihat has spec ific receptors in many target
organs and ti ssues. It exerts its actions by activating DNA and
RNA w ithin the target cell to produce proteins and enzymes that
can be used in bone resorption process. In particular, the acti ve
form of Vi t. O, 1,25 dihydroxy choleca lciferol is the most potent
stimulus of osteoclasti c acti vi ty known. It is also involved in
the formati on of osteoclasts from precursor monocytes .
-
Calcitriol enhances resorption of calcium and phosphate from
bone by promoting recru itment and differentiation of osteoclast
precursors in bone remodeling un its. but mature osteoclasts lack
Vit.D receptor. Though osteoblastic cells express ViI. 0 receptor
and respond to it. calcitriol appears to help bone mineral ization
indirect ly by maintai ning normal plasma calc ium and phosphate
concentra tion. Its action is independent of but fac ilitated by
PTH.
Collins et al"" found on histologic levels an increase in the
number of mononuclear osteoclasts recruitment and activation result
ing in bone resorption on pressure side upon injection of Vit.D
metaboli te 1.2 50 into Pd!. Yamamoto et al' found that injections
of 1,25fOH),D, did not change serum Ca, PO, and ALPase activity and
there were no apparent clinica l or microscopic side-effects.
Nevertheless Vit. 0 (1 ,2S(OH),D,l enhances the re-establ ishment
of supporting tissues, especially alveolar bone of teeth, after
orthodontic treatmenl.'"
ESTORGEN : It has become increasingly evident hat estrogen is
the most important hormone to affect bone metabolism in women. The
various cytokines invo lved in bone reso rpt ion are inhibited by
est rogen. Since mechanically induced bone modeling and remodel ing
are essential for orthodont ic tooth movement. the response to
orthodontic force may vary depending upon the phase of menstrual
cycle. ZhaoQ et al" explored the iniluence ofOTM on estrous cycle
and estrogen and found that estrous was the appropria te time for
orthodont ic force. In another study j in Z et al '" suggested that
estrogen promoted the alveolar bone forming and inhibited bone
resorption. Haruyaman et al " also concluded that cycl ic changes
in the estrad iol level may be associated with the estrous cycle
dependent va ri ation in tooth movement through its effect on bone
resorption. Osteoporosis is commonly seen in the postmenopausal
women due to the defi ciency of estrogen. In order to evalua te the
two most commonly used drugs for osteoporosis Wagle et al "
determined the effects of FOSAMAX and EVISTA on OTM. Fosamax
(alendronate) and Evista (ralaxifenel showed evidence of preventing
bone resorption. Alendronate inh ib its orthodontic activity but
not osteoclast recrui tment. whi le ralox ifene regulates
osteoclastic act ivity by binding and modulating estrogen receptors
to affect osteoclast number and acti vity. The author concluded
that orthodontic treatment may be contraindica ted when taking
these drugs. Estrogens are co mmonl y recommended for
contraception. Moreover in orthodontic clinics. there
44
are more fema le patients than male patients. Also there is an
increase in the number of adult female patients seeking orthodontic
treatment worldwide. Orthodontist shou ld pay specia l attenti on
and should take this factor into cons ideration as then drugs have
shown to reduce the velocity of O.T.M by inh ibiting bone
resorption.
ANDROGENS: Androgens are the sub stan ces which cause
development of secondary sex characters in the castrated men.
Anabol ic steroids are used by the athletes during the period of
training w hich are supposed to have higher anabolic and lower
androgenic activi ty. As then drugs also inhibit bone resorption,
it may affect the duration of the orthodontic treatment. Therefore
a thorough history regard ing the use of such drugs should be taken
from the adult males.
CONCLUSION: Since orthodontist plays a pivotal role in cl inical
pharmacology in the dental practice, they should have an
understanding of the fundamentals of drug therapy. Orthodontist
should be able to converse with patients about medica tions prescr
ibed for them, includ ing rev iewing potentia l adverse effects,
drug interact ions. and how to take the medication. A thorough
medica l history should be reviewed with the patient, including any
prescript ion, and over the counter products. as many patients use
drugs on daily basis wh ich have therapeutic as well as adverse
effects.
Drugs like NSAID 's, Bi sphosphona tes, vitam in 0 metabolites,
fluor ides can decrease the velocity of tooth movement. On the
contrary drugs and systemic factors l ike eicosano ids, cor ti
costeroids. th yroid and parathyroid hormones can increase the
veloci ty of tooth movemenl. Orthodontist should be aware of such
medications so that treatment plan best suited for the individual
patient could be made and keeping the mechan ics as simple as
possible.
REFERENCES: I I Proff it W .R. , Field s H .W. , Sarver D.M
..
Contemporary orthodont ics. IV edition. 2) Richard S. Masella,
Malcolm Meister : Current
concepts in the b iology of orthodontic tooth movement. Am J
Orthod Dento fa c Orthop 2006; 129:458-68.
3) Tripathi KD. Essentials of medical pharmacology, V
edition.
41 Krishnan V, Davidovitch Z. Cellular, molecular and tissue
level reactions to orthodontic force. Am J Orthod
2006;129:46ge.I-460e.32.
-
51 Davidovitch Z, Steigman S. Electric currents. bone remodeling
and orthodontic tooth movement. Am J Orthod 1980;77:33 -47.
6) Krishnan V. Davidvitch Z. The effects of drugs on orthodontic
tooth movement. Orthod Craniofac Res. 2006 Nov.;9(4):163-71.
71 Gameiro GH. Pereira-Neto JS, Magnani MB, Nouer OF. The
inileunce of drugs and systemic factors on orthodontic tooth
movement. J Clin Orthod 2007 Feb;41 (21:73-8.
8) Krishnan V. Orthodontic pain : from causes to mana gement - a
review. Eur I Orthod 2007;29: 170-179.
9) Chumbley A B, Orhan e. Tuneay. The effect of indomethacin (an
aspirin like drug) on the rate oi orthosontic tooth movement. Am J
Orthod 1986:89:312-314.
10) I .B. Walker, SM Buring. NSAID impairment of orthodontic
tooth movement. The Annals of pharmacotherapy, 200 ' ;35(1):
113-115.
11 1 Arias OR, Marquez -Orozco Me. Asp irin , acetaminophen, and
ibuprofen: their effects on o rthodo nti c tooth movement. Am I
Orthod Dentofacial Orthop 2006 sep;130(3):364-3 70.
12) Roche Jj , Cisneros GL Acs G. The effect of acetaminophen on
tooth movement in rats. Angle Orthod 1997;67131:231 -6.
13) Kehoe MJ, Cohen SM, Zarrinnia K. Cowan A. The effect of
acetamino ph en, ibuprofen and misoprostol on PGE , synthesis and
the degree and rate of orthodontic tooth movement. Angle Orthod
1996;66(5):339-49.
14) Bradley Rl. Ellis PE , Thomas p, Bellis H, Ireland AI. Sandy
JR. A randomi zed cl i ni cal tr i al compa rin g the efficacy of
ibuprofen and paracetamol in the control oi orthodont ic pain. Am J
Orthod Dentofacial Orthop 2007 Oct;132(4;:511-7.
15) Polat 0 , Karaman Al , Durmus E. Effects of preoperative
Ibuprofen and Naproxen sodium on orthodontic pain. Angle Orthod
75(S):79 1-796.
16) Kyrkan ides 5, O ' Banion MK, subtenly 10. Non steroidal
anti-inflammatory drugs in orthodontic tooth movement :
metalloproteinase activity and collagen synthesis by endothelial
cells. Am I Orthod Dentofac Orthop 2000 Aug: 118(2): 203-9.
17) Sari E, Olmez H, Gurton AV. Comparison of some effects of
acetylsalicylic acid and rofecoxib during
45
,-_tnt::
orthodontic toot h movement. Am I Orthod Dentofac Orthop
2004Mar; 125(3):31 0-5.
18) Young AN, Taylor RW. Taylor SE, linnebur SA, Buschan g PH .
Evaluati o n of p reemptive valdecoxib therapy on initia l archwire
placemenl di scomfort i n adu l ts . Angle orthod. 200 6
Mar;76(2):251-9.
19) De Carlos F, Cobo J, Diag-Esnal B, Arquelles J. Vijande M ,
Costabs M . Orthodon tic tooth movement after inhibition of
cyclo-oxygenase-2 . Am I Orthod D entofac Orthop 2006.
Mar;1290):402-6.
201 De Carlos F, Cobo J. Peri lion C, Garcia MA, Arquelles J,
Vijande M , Costales M. Orthodontic tooth movement after different
coxib therapies. Rur I Orthod 2007 Dec;29(6):S96-9.
21 ) Gameiro GH, Nouer OF, Neto ISP, Siqueira vc. Andrade ED,
Novaes PO, Veiga MCF. Effects of short and long term celecoxibon
orthodontic tooth movement. Angle Orthod 78(S):860-86S.
221 Gameiro GH, Nouer OF, Pereisa- 'eto IS . deAraujo Magnani
MB. deAndrade ED, Novaes PO, de Arruda Veiga Me. Histologica l
analysis of orthodontic root resorption in rats trea ted w ith the
cyc looxygenase 2(cox-2 ) inhibitor celecoxib . Orthod Craniofac
Res 2008 Aug; II (3):1 56-61.
23) Sandy JR, Farndale RW. M eikle Me. Recent advances in
understanding mechanically induced bone remodeling thei r relevance
to orthodontic theory and practice. Am I Orthod 1993; 1
03:2t2-222.
24) Ngan P, Ken B, Wilson S. Perception of discomiort by
patients undergOing orthodonti c treatment. Am I Orthod 1989:96:4
7-53.
25) Chao CF, Sh ih C. Effects of prostaglandin E, on alveolar
bone resorption during orthodontic tooth movement. Acta Anat
1988:132:304-9.
261 Sandy IR, Harris M. Prostaglandins and tooth movement. Eur J
Orthod 1984;6(1 ): 175- 182.
27) Gurton AV, Akin E. Sagdic 0 , Olmez H . Effects of PGI , and
TXA, analogs and inhibitors and orthodontic tooth movement. Angle
Orthod 2004 Aug;74(4):526-32.
28) Yamasaki K, Shibata Y, iukuhara T. The eifect of
prostaglandin on experimental tooth movement in monkeys. I Dent Res
1982:61 : t444-6.
29) Leikar BI. Nanda RS, Currier GF, Howes RI, Sinha PK. The
effects of exogenous prostaglandins 011 orthodontic tooth movements
in rats. Am I Orthod 1995;108:380-8.
-
30) Boekenoogen DI, Sinha PK, Nanda RS, Ghosh ), Currier GF,
Howes RI. The effects of exogenous prostaglandin E, on root
resorption in rats. Am) Orthod Dentofac Orthop 1996Mar;
109(3):277-86.
31) Brudvik P, Rygh P. Root resorption after local injection of
prostaglandin E, during experimental tooth movement. Eur ) Orthod
1991 Aug; 13(4):255-63.
32 ) Se ifi M, Eslani B, Saffar AS. The effect of prostaglandin
E, and calcium gluconate on Orthodoti c tooth movement and root
resorption in rats. Eur) Orthod 2003;25(2):199-204.
33) Mohammad AH, Tataki s DN, Dziak R. Leukotrienes in O
rthotontic tooth movement. Am ) Orthod Dentofacial Orthop. 1989
Mar;95(3):231-7.
34) Rin chu se DL Rinchu se DL Sosavicka MF, Robinsons )M,
Pendleton R. Orthodotnic treatment of patients using
bisphosphonates : a report of 2 cases. Am ) O rthod Dentofac Orthop
200 7 Mar; 131 (3):32 1-6.
35) Sato Y, Sakai H, Kobayashi Y, Shibasaki Y, Sasaki T.
Bisphosphonate administration alt ers subcellular loca li zation of
vacuolar type H (+) ATPase and cathepsi n K in osteoclasts during
experimental movement of rat molars . Anat Rec 2000 Sept
1;260(1):72-80.
36) Liu L, Igarashi K, Karzakin, Chiba m, Shinota H, Mi tani H.
Clodronate inhibits PGE (2) production in compressed periodontal
ligament cells. ) Dent Res 2006 Aug;85 (8) :757-60.
37) Liu L, Igarashi K, haruyama N, Saeki S. Shinoda H, Nitani H
. Effects of loca l administration of clodronate on orthodontic
tooth movement and root resorpt ion in rats. Eur ) Orthod 2004
Oct;26(5):469-73.
38) Igarashi K, Adachi H, Mitani H, Shinoda H. Inhibitory effect
of the topica l adminsitration of a bisphosphonate (residronate) on
root resorption incident to orthodontic tooth movement in rats. )
Den t Res 75:1644-1649.
39) Igarashi K, Mitani H, Adochi H, Shinoda H. Anc horage and
retentive effec ts of a bisphosphonate (AHBuBP) on totoh movement
in rats. Am) Orthod Dentofac Orthop 1994;106:279-89.
40) Kim TW, Yoshida Y, Yokoya K, Sasaki T. An ultrastructural
study of the effects of bisphoshonate administration on
osteoclastic bone resorption during relapse of experimentally moved
rat molars. Am ) O rthod Dentofac Orthop 1999 Jan; 11
5(6):645-53.
46
41 ) Adachi H, Igarashi K, Mitani H, Shinoda H. Effects of
topical administration of a bisphosphonate (residronate) on
orthodontic tooth movement in rats. ) Dent Res 73:1478-1486.
42) Zahrowski JJ . Bisphosphonate treatment : on orthodonti c
concern ca ll ing for a proactive approach. Am) Orthod Dentofacial
Orthop. 2007 Mar; 131(3):311-20.
43) Hellsi ng E, Hammarstrom L. The effects o f pregnancy and
fluoride on orthodontic tooth movement in rats . Eur ) O rth od 199
1 )an;13(3):223-30.
44) Kebsch M, Wilkinson M, Petoez P, Darendelibr MA. The effect
of fluoride administration on rat serum osteocalcin expression
during orthodontic movement. Am) Orthod Dentofacial Orthop 2007
Apr; 131 (4):5 15-24.
45) Foom, Jones A, Darendel iver MA. Physica l properti es of
root cementum: Part 9. Effect of systemic fluoride intake on root
resorption in rats. Am) Orthod Dentofac Orthop 2007 )an;131(1):
34-43.
46) )owsey L Rigg 's BL. Bone formation in hypercortisonism.
Acta EndocrinoI 1970;63 :21-8.
47) Ashcroft MB, Southard KA, Tolley EA. The effect of co rti
costeroid indudced osteoparon's on orthodontic tooth movement. Am )
O rthod 1992;102:310-9.
48) M avraga ni M , Brudvik P, Se lvi g KA . Orthodontically
induced root and alveolar bone resorpti on: inhibitory effec t of
systemic doxycycl ine administration in rats. Eur) O rthod 2005
)an;27(3):2 15-25.
49) Verna C, Harti g LE, Kalia S, Melsen B. Influence of steroid
drugs on orthodotni ca ll y induced root resorption. Orthod
Craniofac Res 2006 feb;9( 1 ):57-62.
50) Kalia S, Melsen B, Verna C. Ti ssue reactions to orthodonti
c tooth movement in acute and chroni c corti costeroid treatment.
Cathod Cranifac Res 2004;7:26-34.
51) Saddi KRGC, Alves GD, Paulino TP, Cincaglin i p, Alves )B,
Epidermal growth factor in liposomes may enhances orthoclast
recruitment during tooth movement in rats. Angle Orthod
78(4):604-609.
52) Madan MS, Liu ZL Gu GM, King G). Effects of human relaxin on
orthodontic tooth movement and periodontal ligaments in rats. Am )
Orthod Dentofacial Orthop 2007; 131(8):el-8, e1 O.
-
53) Kanzaki H, Chiba M, Takahashi I, Haruyama N, Nishinura M,
Mitani H. Loca l OPG gene transfer to periodotnal tissue inhibits O
rthodontic tooth movement. J Dent Res 2004;83(12):920-925.
54) Dolce C, Vakani A, Ancher L, Norri s Wiman JA, Holl iday LS.
Effects of echistatin and an RGD peptide on orthodontic tooth
movement. J Dent Res 2003 Sep;82(9):682-6.
55) Tali c NF, Eva ns C, Za ki AM . Inhib iti on o f O rthodotn
ica ll y induced root resorpti on w ith echistatin, an RGD contain
ing peptide. Am J Orthod Dentofac O rthop 2006; 129:252-60.
56) Sprogar S, Volk l, Drevanek M , Drevenek G, The effects of
TBC 32 14, a selecti ve ETA receptor antagonist, on orthodontic
tooth movement in rats. Eur J Orthod 2007 Dec;29(6):605-8.
57) Drevensek M, Sprogars, Baras I, Devensek G. Effects of
endothelin antagonist tezosentan on orthodont ic tooth movement in
rats. Am J Orthod Detnofacial Orthop 2006;129:555-8.
58) M idgett RJ . The effect of altered bone metabol ism on
orthodontic tooth movement. Am J Orthod Dentofac O rthop 1981
;80:256-262.
59) Engstrom C. Root resorpti on during Orthodontic tooth
movement and bone remodeling dynamics during hypocalcemi a and trea
tm en t w ith bisphosphonate. The Biologic mechanism of tooth
erupti on and roo t resorpt io n. Edited by Davidovitch 1988.,
391-97.
60) Adams PH, Jowsey J, Kell y Pl, Riggs BL, Kinney VR, Jones JJ
. Effects of hyperthyroidism on bone and mineral metabolism in man.
Quaterly Journal of Medica l New seri es 1967;35: 141 :1-1 5.
61) Adams P, Jowsey J. Bone and mineral metabolism in hyperth
yro idi sm. An Exper imental study. Endocrino logy 1967;81
:735-40.
62) Poumpros E, Loberg E, Engst rome. Thy ro id function and
root resorpti on. Angle O rth od 1994;No.5:389-394.
47
63) Shirazi M, Dehpour AR, Jafari F. The effect of thyroid
hormone on Orthodontic tooth movement in rats. J Clin Pediatr Dent
1999 Spri ng; 23(3): 259-64.
64) Soma S, Iwanoto M, Higuchi Y, Kurko K. Effects of continuous
infusion of PTH on experimenta l too th movement in ra ts. J Bone
Minu r Res 1992; 14:546-554.
65) Soma S, Matsumoto S, Hi guchi Y, Takano-Yamamoto T,
Yamashita K, Kuri su K, Iwamoto M . Loca l and chronic applicati on
of PTH accelerates tooth movement in rats. J Dent Res 2000;79:
1717-1 724.
66) Collins MK, Sinclir PM. The loca l use of vitamin D to
increase the rats of orth odonti c too th movement. Am J O rth od
Dentofac O rth op 1988;94:278-84.
67) Yamamoto T, Kawakami M, Yamashi ru T. Effect o f age on th e
rats of too th movemetn in combinati on w ith local use of 1
,25(OH), D1 and mechanica l force in the rat. J Dent Res. 1992 Aug;
71(8): 1487-92.
68) Kawakami , Takano-Yamamoto T. Loca l injecti on of
1,25-dihydroxy vitamin D J enhanced bone formation for tooth
stabili zation after experimental tooth movement in rats. J Bone M
iner Metab 2004;22(6):541 -6.
69) Zhao Q, Tan Z, Guo l, Chen YX. Influence of orthodontic
tooth movement on estrous cycle and estrogen in ra ts. Zhonghua
Kore Q iang Yi Xue Za Zhi 2006 Feb;41 (2):90-1 .
70) Jin Z, Ding Y, Li x. Effec ts of es trogen on experimenta l
tooth movement in osteoparosis rats. Zho nghua Kou Qia ng Y Xue Za
Zhi 2000 Jan;35(1 ):55-7.
71) Haruyama N, Igarashi K, Sarki S, Isoya M. Shinoda H, Mi
tavih . Estrous cycle dependent va riation in orth odonti c too th
moveme nt. J Dent Res 2002;81 (6) :406-1 O.
72) ladx. Confex Com / idadn / 2005 Ba ltltechprog/ abstract -
58651 (1289 Effects of Fosamax and Evista on Orthodontic tooth
movement).
-
REVIEWS (Compiled by Dr. Sridevi Padmanabhan)
Near-end of Treatment Panoromic Radiogrph in the Assessment of
Mesiodistal Root Angulation Ann Marie Owens; Ama Johal, Angle
Orthodontist, Vol. 78, No.3, 2008.
This study aimed to test the hypothes is that there is no
difference between the mesiodistal root angulation and the
mesiodistal root angulation as measured on the panoramic
radiograph. Thi s was eva luated using a typodont dentition set
into Class I occlusion.
Wire strust were placed on the bucca l surface of each tooth to
represent their long axes and the each the denti tion was fixed
into a natural skull for imaging. The radiographic and true
mesio-distal angulati on of each tooth to the horizontal reference
plane was measured. The measurements were repeated after alteri ng
the mes iodistal root pos itions to a more mesia l and more distal
position.
O nly 26.7% of the root angulations were w ithin the clinica lly
acceptable angular vari ation range of 2.5. The greatest va ri ati
on in the upper arch was in the canine premolar region where the
roots were projected as being more divergent. The greatest vari
ation in the lower arch occurred in the lateral incisor-canine
region w here these roo ts appea red more convergent. Radiographic
distortion was statistica ll y more in the lower than in the upper
arch.
Concl usion: There is a cl inica lly signifi cant vari ation
between the radiographic and the true root angulations recorded and
caution is advi sed w hen interpreting mes io-d istal root angulati
on using O PG.
Torque expression of self-ligating brackets Hisham M. Badawi,
Roger W. Toogood, Jason P.R.Carey, Giseon Heo and Paul W. Major. Th
is study measured the difference in third-order mo ments th at ca n
be del ivered by engag ing 0.019xO.025 - in stainless steel
archwires to 2 active self- l igating brackets (In-ovati on and
Speed) and two passive self- ligating brackets (Damon 2 and Smart
Clip) using a novel torque measurement device.
There was a signi ficant di fference in the engagement angle
between the two types of brackets. For the active self- ligat ing
brackets, torque started to be expressed at
48
7.5 of torsion and at 15 for the passive self- ligating
brackets. The torque expression was higher for the active self-li
gating brackets at cl inica lly usable torsion angles (0-35). The
pass ive self-ligating brackets started producing moments at high
torsion that cannot be used clini ca lly.
Thus the cl inica lly applicable range of torque activation and
torque control was greater for the active self- ligating
brackets.
Botulinum toxin type A (Botox) for the neuromuscular correction
of excessive gingival display on smiling (gummy smile)
Introduction: Prev iously, botulinum tox in type A (BTX-A) (Botox;
Allergan, Irvine, Ca li f) was shown to be effecti ve in reducing
excess ive gingiva l display in 5 pati ents with gummy smiles. This
study was conducted to determin e w hether the doses and the
primary injection si tes used in the pilot study for the correcti
on o f gummy smiles prov ide consistent, stati sti ca ll y
significant, and esthetica lly pleasing results.
Methods: Thirty patients received BTX-A injections to reduce
excessive gingiva l display. Gingiva l display was defined as the
difference between the lower margin of the upper lip and the
superior margin of the right incisor. Patients were fo llowed at
2,4,8,12,16,20, and 24 weeks pos t i nj ec ti on, w ith changes doc
um ented by photographs and videos. At week 2, the patients rated
the effects of BTX-A. A group of specia lity cl inicians also
evaluated the effects of BTX-A.
Results: Prei nj ecti on gingival di spl ay averaged 5.2 1 .4mm
in the 30 patients. At 2 weeks post injection, mea n gingiva l di
spl ay had dec lined to 0.09mm (1.06mm) in 30 pati ents (1=26.01 ,
P