Embed Size (px)
Citation preview

AUGUST 1977
The American Journal of Medicine
VOLUME 63
NUMBER 2
EDITORIAL
Homogeneous (Monoclonal) lmmunoglobulins in Cancer
ALAN SOLOMON, MD
Knoxville, Tennessee
From the University of Tennessee Memorial Re- search Center and the East Tennessee Cancer Research Center, University of Tennessee Center for the Health Sciences, Knoxville, Tennessee. This work was supported in part by U.S. Public Health Grants CA 10056-l 1 and CA 13237-04 from the National Cancer Institute. Requests for reprints should be addressed to Dr. Alan Solomon, University of Tennessee Memorial Research Center, 1924 Alcoa Highway, Knoxville, Tennes- see 37920. Manuscript accepted September 29, 1976.
Bence Jones proteins, myeloma proteins, Waldenstrom macroglob-
ulins and their subunits are homogeneous (monoclonal) immuno-
globulins produced by single clones of neoplastic immunoglobulin-
synthesizing cells that are present in the bone marrow or lymphoid
tissue of patients with plasma cell or lymphoc,ytic neoplasms.
Monoclonal immunoglobulins (M components), although characteristic
of lymphoproliferative diseases, have also been found in serum or
urine specimens obtained both from patients with nonreticular neo-
plasms or inflammatory diseases and from apparently normal persons,
particularly those over the age of 76 [ l-l 21.
M Components and Cancer. The association of monoclonal immu- noglobulins and plasmacytosis with nonreticular as well as reticular
malignancies has been based on clinical, serologic and histopathologic
observations. For example, the coexistence of carcinoma has been
noted frequently in postmortem examinations of patients with multiple myeloma [ 131. On the other hand, monoclonal immunoglobulins have
often been detected in serum specimens obtained from patients with
carcinoma (especially colorectal cancers) who have no documented
evidence of coexisting multiple myeloma [2,6-l 1 I. lsobe and Os-
serman [ 81, in a review of the clinical and histopathologic data on 806
patients with serum M components seen from 1959 to 197 1 at Pres- byterian and Francis Delafield Hospitals in New York, noted such
proteins in 128 patients with nonreticular neoplasms. These M com-
ponents were found most often in patients with carcinoma of the
rectosigmoid, prostate and breast. When the frequency of occurrence
of M components in patients having six selected neoplasms was
compared with the frequency of these same neoplasms in a general
hospital population, the data revealed that the percentage of patients
with adenocarcinoma of the rectosigmoid, prostate, lung and gall- bladder was twice that found in a random series of patients who lacked
M components.
169

HOMOGENEOUS (MONOCLONAL) IMMUNOGLOBULINS IN CANCER-SOLOMON
Case No.
NHS
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
M component Diagnosis
-
I@ 0)
IgA(U
Is~(X)
I&(A)
I@(K)
IgG(K, A>
W(A)
W(K)
IgG (1)
I@(K)
IgG(K, K)
I@ k)
I@(K)
IgGk)
I@(K)
I@(X)
I@(K)
IgG (K)
- . . . . .
Ca liver . . . . .
Ca lung . . . . . .
Ca lung . . . . . .
Ca prostate . . . .
Ca prostate . . . .
Ca uterus . . . . .
Lymphoma . . . . .
Hodgkins' . . . . .
Acute myel. leuk. .
Thymoma . . . . . .
Ca colon . . . . .
Ca pancreas . . . .
Ca lung . . . . . .
Ca liver + M.M. . .
Ca colon + M.M. . .
Ca colon + M.M. . ,
Lymphoma . . . . .
Lymphoma . . . . .
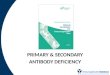
Figure 7. Cellulose acetate electrophoresis of serum specimens containing monoclonal immunoglobulins obtained from patients with nonreticular, reticular or both types of malignancies. Ca = carcinoma; M. M. = multiple myeloma; NHS = normal human serum. The M components are indicated by the arrows; the heavy chain class (IgG, IgA, IgM) and light chain type (K, X) of these M components were established immunochemically.
The detection of hyperproteinemia through routine
examination of serum specimens by multiphasic chemical analyses and the widespread use of protein
electrophoresis has led to increased recognition of
monoclonal immunoglobulins present in patients with
many different histologic types of neoplastic diseases,
such as carcinoma of the colon, prostate, breast and
lung (Figure 1). Mackler et al. [14], using cellulose
acetate electrophoresis, found that 95 of 11,275 serum
specimens obtained from patients at a Veterans Ad- ministration Hospital contained an M component-an incidence of -1 per cent. Surprisingly, their review of
60 such patients revealed that M components were
more frequently found in patients with nonreticular as opposed to reticular neoplasms (18 and 13 patients, respectively). The frequency of occurrence of M com- ponents in patients with nonreticular forms of cancer
is presently‘unknown, primarily because of the limited
resolving capacity of cellulose acetate electrophoresis;
the presence of an M component, particularly when
present in low concentration (CO.5 g/100 ml), is fre-
quently obscured by normal serum globulin compo-
nents. A more sensitive means of detecting M compo-
nents can be provided by the application of other ana-
lytic technics which permit increased electrophoretic
separation and resolution of serum proteins, e.g.,
agarose gel electrophoresis (Figure 2).
In several large series of patients with monoclonal immunoglobulins who showed no evidence of multiple
myeloma or other reticular malignancies, 15 to 30 per cent were reported to have carcinoma [6-l 11. In
comparisons of the frequency of distribution of the heavy chain classes or light chain types of the homo- geneous immunoglobulins in patients with reticular
170 August 1977 The American Journal of Medicine Volume 63

HOMOGENEOUS (MONOCLONAL) IMMUNOGLOBULINS IN CANCER-SOLOMON
Case No. NHS
1
2
3
4
5
6
7
Cancer
NR
R
R
R
NR
NR
R
CELLULOSE ACETATE
_. figure 2.
_ . . Gomparison of cellulose acetate and agarose gel electropnoresrs of serum speomens from
patients with reticular and nonreticular forms of cancer. N/-/S = normal human serum; R, NR = reticular and nonreticular forms of cancer, respectively. The M components on the agarose gel are indicated by the arrows.
AGAROSE GEL
0
f Ire 3. A, cellulose acetate electropherogram ot serum from a patlent w/m squamous cell carcinoma or me lung (the monoclonal protein is indicated by the arrow). The histologic findings of metastatic carcinoma and plasmac:ytosis within a su- praclavicular lymph node obtained from this patient are shown in B (magnification X 400) and C (magnification X 1,000); many of the plasma cells contained intracytoplasmic inclusion bodies as shown in 0 (magnification X 1,000) Similar histologic
findings were evident in a specimen of pericardial tissue. Photomicrographs courtesy of Dr. Anthony A. K&tine.
August 1977 The American Journal of Medicine Volume 63 171

HOMOGENEOUS (MONOCLONAL) IMMUNOGLOBULINS IN CANCER-SOLOMON
TABLE I Antigens Reactive with Human M Components*
Antigen
Albumin Alpha2 macroglobulin Antihemophiliac globulins
(factors VIII, IX) Blood group antigens Brucella Cardiolipids Fibrin monomer Heparin Immune complexes lmmunoglobulin G Klebsiella Lipoproteins Nitrophenyl derivatives Phosphorylcholine Riboflavin Rubella Staphylolysin Streptolysin 0 Transferrin
l Modified from [24].
lmmunoglobulin Class
lgM tgG
IgG, lgM lgM, lgA
tgG lgM tgG tgG lgM
IgM, IgG, lgA IgM lgG
tgM> IgG. lgA
‘gM lgG tgG tgG tgG ‘gG
versus nonreticular malignancies, a predominance of
immunoglobulin G (IgG) proteins has been found in the
latter group [ 2,151. In most cases the concentration of
normal immunoglobulin components was reduced in both groups-a factor which in itself may predispose
to the development of malignancy [ 15,161.
The relationship between M-component concen-
tration and the extent and course of disease, including
therapeutic response and relapse, has been evident in
patients with multiple myeloma; however, this rela-
tionship has not been apparent in patients with M
components and nonreticular malignancies [6]. Fur-
thermore, as has been shown experimentally, a
monoclonal or polyclonal humoral antibody response
is under genetic influence [ 171 as is the occurrence of
multiple. myeloma in certain species [ 18,191. The
Hellstroms [20] have shown that antibody or complexes
of antigen and antibody can block the antitumor effect
of cytotoxic lymphocytes, thus facilitating the growth
of certain clinical and experimental forms of cancer.
These investigators have shown also that serum ob-
tained from animals or patients in remission from
cancer contain “unblocking” antibodies which can
counteract “blocking” antibodies. The M components
found in the serum of patients with carcinoma may
represent either one or the other of these types of an-
tibodies. Whether or not the M components found in the
serum of patients with nonreticular neoplasms repre-
sent a humoral response to tumor-related antigens re-
mains to be established.
Nonreticular neoplasms, especially those of epithelial
origin (as shown in Figure 3), may be associated with
a pronounced mononuclear cell infiltration within or
surrounding the mass of neoplastic cells [5-71. Plasma
cells are often found in this type of “reactive” response,
and their presence perhaps signifies the reaction of an
immunologically-competent host to tumor-associated
or tumor-specific antigens of nonreticular neoplastic
cells. Such “reactive” plasma cells contain monoclonal
immunoglobulin identical to the serum M component,
as has been shown by immunofluorescence studies
[6,21]. Certain human (and murine) M components bind
specific ligands and have demonstrable antibody activity
as evidenced, in some cases, by the localization of this
binding activity to the antibody-combining (Fab) portion
of these molecules (Table I) [22-251. In this regard, a
Figure 4. lmmunochemical demonstration of the idiotypic antigenic determinant. Ouchterlony immunodiffusion analyses of the precipitin reactions of six different IgG myeloma proteins with an antiserum prepared against protein 1. The center well in the pattern on the left contained the unabsorbed antiserum and on the right the same antiserum after absorption with protein 2. The specificity of the unabsorbed antiserum for antigenic determinant(s) unique to protein 1 was evident from the precipitin reactions of partial identity with the other proteins and by the fact that only protein 1 reacted with the absorbed antiserum.
172 August 1977 The American Journal of Medicine Volume 63

HOMOGENEOUS (MONOCLONAL) IMMUNOGLOBULINS IN CANCER-SOLOMON
serum specimen obtained from a patient with colon cancer was found to have a capacity 10 times that of normal serum to agglutinate sheep erythrocytes which had been coated with an antigen extracted from the colon of germ-free rats; this agglutinating (antibody) activity was attributed to a monoclonal IgG protein present in the patient’s serum [26]. lmmunoglobulin Idiotype. The antibody-combining site has been characterized by immunochemical, structural and physicochemical analyses of homogeneous im- munoglobulins. Through studies of human myeloma proteins and rabbit immunoglobulins, Kunkel and co- workers [27-291 and Oudin [30], respectively, dem- onstrated that each immunoglobulin has unique anti-
genie determinants which are specific for that protein. These determinants were termed individually specific or idiotvpic antigenic determinants (Figure 4). The im- portance of this finding was made evident by the sub- sequent demonstration that immunoglobulins with similar antibody specificity share idiotypic determinants [ 29-351. The idiotypic antigenic determinant has been localized immunochemically and structurally to include the antibody-combining site [33,36-4 11; thus, the id- iotype serves as a unique immunochemical marker to identify immunoglobulin molecules of common speci- ficity.
lmmunochemical studies employing idiotype-specific antiserums to M components have provided data for
-- I . _ I I
t------v--+
NH2-
NH2-
Figure 5. Schematic diagram of the basic domain structure of the light and heavy polypeptide chains of r’mmunoglobulins. The domains in the amino-terminal ( NH2) portion of each chain, the variant regions, are designated V, and V, for the light chain and heavy chain, respectively; the hypervariable regions, within the V, and V, are shown as discrete dark stippled areas. The domains in the carboxyl-terminal (COOH) portion of each chain, the constant regions, are designated CL and CH for the light chain and heavy chain, respectively; and the three CH domains are designated C” 1, CH2 and CH3 (the CH of immunoglobulins M and E contain an additional domain designated CH4). An additional polypeptide chain, the J chain, is disulfide-linked to the carboxyl-terminal portions of the CH3 or CH4 domains of polymeric immunoglobulins A and M, respectively. The carbohydrate moiety, usually located exclusively on the heavy chain, is designated CHO. The polypeptide region between the CH 1 and CH2 domains is termed the hinge region (indicated by the lightly stippled area); this region is particularly susceptible to proteolytic cleavage. Papain cleaves the heavy chain on the amino-terminal side of the inter-heavy chain disulfide bonds resulting in the production of fragment Fc and the two monovalent antibody-combining fragments Fab; pepsin cleaves the heavy chain on the carboxyl-terminal side of the inter-heavy chain disulfide bonds resulting in the production of the divalent antibody-combining fragment, F(abh; and under special conditions of peptic cleavage the variant region ( V, and V,) can be cleaved from the intact immunoglobulin molecule yielding the Fv fragment. Reprinted from Solomon A: N Engl J Med 294: 17, 1976 (by permis- sion).
August 1977 The American Journal of Medicine Volume 63 173

HOMOGENEOUS (MONOCLONAL) lMMUNOQLO6ULMS lN CANCER-SOLOMON
TABLE Ii Biologic Activities and Effector Functions of Immunoglobufins
Cytophilic and homocytotropic propertles Neutrophils Macrophages and monocytes Basophils and mast cells Platelets Lymphocytes
Biochemical properties Allotype lsotype Carbohydrate
Physiologic properties Placental passage Catabolism Passive cutaneous anaphylaxis (PCA)
Binding properties Acid proteoglycans Albumin Alkaline phosphatase Alpha, antitrypsin Amylase Choline Coagulation factors Complement Cystic fibrosis factor Lactate dehydrogenase Rheumatoid factor Staphylococcal A protein Transferrin
phorylchoiine by spleen ceils [50]. At present, how- ever, it remains to be determined whether or not anti- iodiotype antiserums can be utilized therapeutically. Functions of immunogiobuiins. lmmunoglobulins serve as humoral and cellular receptors of the immune response because of their capacity to bind antigen and to interact with other biologic substances. These functions are mediated structurally in two separate regions of the immunoglobulin molecule: (1) antigen- binding (antibody function) is localized to the Fab por- tion or, more specifically, to the Fv portion or variant (V) domains of the heavy and light polypeptide chains, and (2) interaction with other biologic substances (ef- fector function) is localized primarily to the Fc portion, although interaction may occur with any of the car- boxyl-terminal, constant (C) domains as well as with the “hinge” region between the first (&I) and second (CH2) domains of the heavy chain (Figure 5).
associating these monocional immunogiobuiins with nonreticular neopiasms. For immunofiuorescence studies of individual tumor specimens, Williams et al. [6] prepared such antiserums to M components which had been isolated from the serum speCiftIens of five patients with different histologic types of carcinoma. In each case, plasma ceils containing specific irnmu- noglobulin, i.e., the M component, were identified clustered about or interspersed among nonreactive (nonstaining) tumor cells. Anti-M-component idiotype antiserums have been utilized for immUnofiuorescence studies of surface immunoglobuiin found on homologous peripheral lymphocytes. In one such study 1421, it was found that the membrane-bound immunogiobulin was idiotypically identical to the patient’s serum M compo- nent.
These two functions may be interrelated: the binding of antigen in the V domain results in steric changes in the C domains [ 5 1 ] One example of this phenomenon is the exposure of complement-binding sites in the CH2 domain as a consequence of antigen-antibody reaction [52]. Some of the effector functions of immunoglobu- lins listed in Table Ii are dependent on specific cellular receptors for the Fc portion of the immunoglobulin molecule whereas others rely on intrinsic properties of the Fc region which not only regulate immunoglobulin catabolism and placental passage but also bind physi- ologic substances [ 531.
Certain myeloma proteins and Waldenstriim mac- roglobulins interact on a “nonimmunologic” basis with several types of biological substances including staphylococcal protein A [ 54-561, choline [ 571, lactate dehydrogenase [ 581, acid proteoglycans [59], alpha, antitrypsin [60], albumin [ 6 1,621 and coagulation factors [63,64]. Although the binding of these sub- stances by homogeneous immunoglobulins is not characteristic of an antigen-antibody reaction and does not involve the Fv region, a structural basis for these reactions is, nevertheless, implied by the evident specificity of the Fc region from certain immunoglobulin molecules to interact with these substances [ 55,561.
The possibility that the idiotypic antigenic determinant Heparin is one substance of special interest which may regulate tumor growth is evidenced by the fact that can interact with immunoglobulins and other serum growth of transplanted murine plasma cell tumors can proteins including lipoproteins [65-681. Homogeneous be markedly suppressed in recipient mice pretreated heparin-binding immunoglobulins have been identified with antiserums containing antibodies to the idiotypic among myeloma proteins and WaldenstrZjm macro- determinants of the myeioma protein synthesized by the globulins [25,69-731 and have also been found in a transplanted tumor [ 43-451. This effect is attributed to patient with breast cancer [74]. The specificity and the presence of membrane-bound specific immuno- mechanism by which immunoglobulin molecules bind globulin (myeloma protein) on the surface of the plasma heparin are still to be determined. Heparin-binding im- cell and, in this capacity, the myeloma protein may munoglobulins may have functional significance serve as a tumor-specific transplantation antigen especially in relation to the regulation of coagulation and [ 43-491. Furthermore, an anti-idiotype antiserum has other heparin-mediated biologic reactions such as the been used to suppress the immune response to phos- regulation of neoplastic growth [75-771.
174 August 1977 The Amerkan Journal oI ffledklne Volume 63

8.
9.
10.
11.
12.
13.
14.
15.
16
17
18.
19.
20.
21.
22.
23.
24.
HOMOGENEOUS (MONOCLONAL) IMMUNOGLOBULINS IN CANCER-SOLOMON
REFERENCES
Osserman EF: Plasma-cell myeloma. il. Clinical aspects. N Engl J Med 261: 1006, 1959.
Osserman EF, Takatsuki K: Plasma cell myeloma: gamma globulin synthesis and structure. A review of biochemical and clinical data with the description of a newly-recognized and related syndrome, “Hy-2-chain (Franklin’s disease).” Medicine (Baltimore) 42: 357, 1963.
Hosley HF: M-proteins, plasmacytosis and cancer. Cancer 20: 295, 1967.
Dammacco F. Waldenstrom J: Bence Jones proteinuria in benign monoclonal gammapathies. Incidence and char- acteristics. Acta Med Stand 184: 403, 1968.
Azar HA: Diffuse (nonmyelomatous) plasmacytosis with dysproteinemia. Am J Clin Pathol 50: 302, 1968.
Williams RC Jr, Bailly RC, Howe RB: Studies of “benign” serum M-components. Am J Med Sci 257: 275, 1969.
Penny R: Paraprotein patterns in Australia. Australas Ann Med 18: 251. 1969.
lsobe T, Osserman EF: Pathologic conditions associated with plasma cell dyscrasias: a study of 806 cases. Ann NY Acad Sci 190: 507, 1971.
Zawadzki ZA, Edwards GA: Nonmyelomatous monoclonal immunoglobulinemia. Progress in Clinical Immunology (Schwartz RS, ed), New York, Grune & Stratton, Inc., 1972.
Coils BM. Lorier MA: Immunocytoma, cancer and other as- sociations of monoclonal gammopathy: a review of 224 cases. NZ Med J 82: 221, 1975.
Ritzmann SE, Loukas D, Sakai H, et al.: Idiopathic (asymp- tomatic) monoclonal gammopathies. Arch Intern Med 135: 95, 1975.
Radl J, Sepers JM, Skvaril F, et al.: lmmunoglobulin patterns in humans over 95 years of age. Clin Exp lmmuno122: 84, 1975.
Weitzel RA: Carcinoma coexistent with malignant disorders of plasma cells; an autopsy survey. Cancer 11: 546, 1958.
Mackler MT, Uyeda C. Perkash A: Letter. Monoclonal gam- mopathies and neoplasia. Am J Clin Pathol 64: 705, 1975.
Fine JM, Lambin P: Distribution of heavy chain classes and light chain types in 757 cases of monoclonal gam- mapathies. Biomedicine 23; 323, 1975.
Rodey GE, Good RA: Immunologic deficiency syndromes, chap 6. Multiple Myeloma and Related Disorders (Azar HA, Potter M, eds). Hagerstown, Harper 8 Row, 1973.
Eichmann K, Braun DG, Krause RM: Influence of genetic factors on the magnitude and the heterogeneity of the im- mune response in the rabbit. J Exp Med 134: 48, 1971.
Potter M: Experimental plasma cell tumors and other immu- noglobulin-producing lymphoreticular neoplasms in mice, chap 3. Multiple Myeloma and Related Disorders (Azar HA, Potter M. eds), Hagerstown, Harper & Row, 1973.
Bazin H, Deckers C, Beckers A, et al.: Transplantable im- munoglobulin-secreting tumors in rats. I. General features of LOU/Wsl strain rat immunocytomas and their monoclonal proteins. Int J Cancer 10: 568, 1972.
Hellstrom KE, Hellstrom I: Lymphocyte-mediated cytotoxicity and blocking serum activity to tumor antigens. Adv lmmunol 18: 209. 1974.
Gorny MK. Zeromski J: Local monoclonal immunoglobulin productlon in cancer patient. Experientia 31: 238, 1975.
Metzger H. Potter M. Terry W: Summary of workshop on ho- mogeneous immunoglobulins with binding activity. Immu- nochemistry 6: 631, 1969.
Seligmann M. Brouet JC: Antibody activity of human myeloma globulins. Semin Hematol 10: 163, 1973.
Nisonoff A, Hopper JE. Spring SB: The Antibody Molecule. New York, Academic Press, 1975.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44
45.
46.
47.
Freedman M, Merrett R, Pruzanski W: Human monoclonal immunoglobulins with antibody-like activity. Immuno- chemistry 13: 193, 1976.
Wang AC, Fudenberg HH: Chemical studies on a monoclonal immunoglobulin from a patient with carcinoma of the colon. lmmunol Commun 4: 483, 1975.
Slater RJ, Ward SM. Kunkel HG: Immunologic relationships among the myeloma proteins. J Exp Med 101: 85. 1955.
Kunkel HG, Mannik M, Williams RC Jr: Individual antigenic specificity of isolated antibodies. Science 140: 1218, 1963.
Kunkel HG: Individual antigenic specificity, cross specificity and diversity of human antibodies. Fed Proc 29: 55, 1970.
Oudin J: The genetic control of immunoglobulin synthesis. Proc R Sot Lond [Biol] 166: 207, 1966.
Williams RC Jr, Kunkel HG, Capra JD: Antigenic specificities related to the cold agglutinin activity of gamma M globulins. Science 161: 379, 1968.
Franklin EC, Frangione B: Common structural and antigenic properties of human yM anti-7 globulins. J lmmunol 107: 1527, 1971.
Kunkel HG. Agnello V, Joslin FG, et al.: Cross-idiotypic specificity among monoclonal IgM proteins with anti-y- globulin activity. J Exp Med 137: 331. 1973.
Potter M, Lieberman R: Common individual antigenic deter- minants in five of eight BALB-c IgA myeloma proteins that bind phosphoryl choline. J Exp Med 132: 737, 1970.
Braun DG, Krause RM: The individual antigenic specificity of antibodies to streptococcal carbohydrates. J Exp Med 128: 969, 1968.
Grey HM, Mannik M, Kunkel HG: Individual antigenic specificity of myeloma proteins. Characteristics and localization to subunits. J Exp Med 121: 561, 1965.
Brient BW. Nisonoff A: Quantitative investigations of idiotypic antibodies. IV. Inhibition by specific haptens of the reaction of anti-hapten antibody with its anti-idiotypic antibody. J Exp Med 132: 951. 1970.
Wells JV, Fudenberg HH, Givol D: Localization of idiotypic antigenic determinants in the Fv region of murine myeloma protein MOPC-315. Proc Nat1 Acad Sci USA 70: 1585. 1973.
Capra JD, Kunkel HG: Amino acid sequence similarities in two human anti-gamma globulin antibodies. Proc Nat1 Acad Sci USA 67: 87, 1970.
Capra JD, Kehoe JM, Winchester RJ. et al.: Structure-function relationships among anti-gamma globulin antibodies. Ann NY Acad Sci 190: 371, 1971.
Kunkel HG. Winchester RJ, Joslin FG, et (al.: Similarities in the light chains of anti-y-globulin showing cross-idiotypic specificities. J Exp Med 139: 128, 1974.
Fu SM. Winchester RJ. Feizi T. et al.: ldiotypic specificity of surface immunoglobulin and the maiuration of leukemic bone-marrow-derived lymphocytes. Proc Natl Acad Sci USA 71: 4487, 1974.
Lynch RG. Graff RJ, Sirisinha S, et al.: Myeloma proteins as tumor-specific transplantation antigens Proc Nat1 Acad Sci USA 69: 1540. 1972.
Hannestad K, Kao M-S, Eisen HN: Cell-bound myeloma pro- teins on the surface of myeloma cells: potential targets for the immune system. Proc Nat1 Acad Sci USA 69. 2295, 1972.
Chen Y, Yakulis V, Heller P: Passive immunity to murine plasmacytoma by rabbit antiidiotypic iantibody to myeloma protein. Proc Sot Exp Biol Med 151: 121. 1976.
Takahashi T. Old LJ, Boyse EA: Surface alloantigens of plasma cells, J Exp Med 131: 1325, 1970.
Takahashi T, Old LJ. Mclntire KR. et al.: lmmunoglobulin and other surface antigens of cells of the irnmune system. J Exp
August 1977 The American Journal of Medicine Volume 63 175

HOMOGENEOUS (MONOCLONAL) IMMUNOGLOBULINS IN CANCER-SOLOMON
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
Med 134: 815, 1971. 63. Harris NS, Jagarlamoody SM, McKhann CF, et al.: The effect
of antiplasma cell sera on the primary immune response. J lmmunol 108: 958, 1972. 64.
Harris NS: Plasma cell surface antigen on human blood lym- phocytes. Nature (Lond) 250: 507, 1974.
Kdhler H: Cited in Claflin HL, Davie JM: Clonal nature of the immune response to phosphorylcholine. IV. ldiotypic uni- formity of binding site-associated antigenic determinants among mouse antiphosphorylcholine antibodies. J Exp Med 140: 673, 1974.
65.
66.
Metzger H: Effect of antigen binding on the properties of antibody. Adv lmmunol 18: 169, 1974.
Schlessinger J, Steinberg IZ, Givol D, et al.: Antigen-induced conformational changes in antibodies and their Fab frag- ments studied by circular polarization of fluorescence. Proc Nab Acad Sci USA 72: 2775, 1975.
Spiegelberg HL: Biological activities of immunoglobulins of different classes and subclasses. Adv lmmunol 19: 259, 1974.
67.
68.
69.
Sjoquist J, Forsgren A, Gustafson GT, et al.: Biological im- portance of the Fc-region of gamma globulins. Cold Spring Harbor Symp Quant Biol 32: 577, 1967.
Kronvall G, Williams RC Jr: Differences in anti-protein A activity among IgG subgroups. J lmmunol 103: 828, 1969.
70.
71. Harboe M, Foiling I: Recognition of two distinct groups, of
human IgM and IgA based on different binding to staphy- lococci. Stand J lmmunol3: 471, 1974.
Mullinax F, Himrod B, Berry ER: Myeloma protein with specific binding of choline. Clin Res 18: 83, 1970.
Biewenga J, Feltkamp TEW: Lactate dehydrogenase (LDH)- IgGs immunoglobulin complexes in human serum. Clin Chim Acta 64: 101, 1975.
72.
73.
Hannestad K, Sletten K: Multiple M-components in a single individual. Ill. Heterogeneity of M-components in two ma- croglobulinemia sera with anti-polysaccharide activity. J Biol Chem 246: 6982, 1971.
74.
Laurel1 C-B, Thulin E: Complexes in plasma between light chain i( immunoglobulins and tu,-antitrypsin respectively prealbumin. Immunochemistry 11: 703, 1974.
Mannik M: Binding of albumin to yA-myeloma proteins and Waldenstrom macroglobulins by disulfide bonds. J lmmunol 99: 899, 1967.
75.
76.
77. Harboe M, Foiling I: Complex formation between monoclonal
IgM and albumin. Stand J lmmunol 1: 412, 1972.
Lackner H, Hunt V, Zucker MB, et al.: Abnormal fibrin ultra- structure, polymerization, and clot retraction in multiple myeloma. Br J Haematol 18: 625, 1970.
Coleman M, Vigliano EM, Weksler ME, et al.: Inhibition of fibrin monomer polymerization by lambda myeloma globulins. Blood 39: 210, 1972.
Holger-Madsen T: Reduction of heparin activity by plasma globulins in patients with increased heparin resistance. Acta Haematol 27: 157, 1962.
Keler-Bagoka M: A specific property of the plasmacytoma serum paraprotein lipids with respect to lipid precipitation by heparin. Clin Chim Acta 16: 365, 1967.
Glueck CJ, Kaplan AP, Levy RI, et al.: A new mechanism of exogenous hyperglyceridemia. Ann Intern Med 7 1: 195 1, 1969.
Becker KE, Gott VL, Allen JC: Purification of some human serum proteins responsible for heparin binding. Am J Physiol 218: 1500, 1970.
Miller D: Heparin precipitability of the macroglobulin in a pa- tient with Waldenstrom’s macroglobulinemia. Blood 16: 1313, 1960.
Favre-Gilly J, Creyssel R. Thouverez JP, et al.: Antithrombine du type de I’heparine dans un gamma-myelome. Consid- erations sur les anticoagulants spontanes dans la maladie de Kahler. Hemostase 3: 325, 1963.
Glueck HI, MacKenzie MR, Glueck CJ: Crystalline IgG protein in multiple myeloma: identification effects on coagulation and on lipoprotein metabolism. J Lab Clin Med 79: 731. 1972.
Beaumont J-L, Lemort N: Les immunoglobulines anti-heparine. Un facteur de thromboses, d’hyperlipidemies et d’ath- erosclerose. Pathol Biol (Paris) 22: 67, 1974.
Wilson DE, Flowers CM, Hershgold EJ, et al.: Multiple mye- loma, cryoglobulinemia and xanthomatosis. Am J Med 59: 721, 1975.
Pogliani E, Cofrancesco E, Praga C: Anti-heparin activity of a macroglobulin from a patient with breast adenocarcino- ma. Acta Haematol 53: 249, 1975.
Hagmar B, Boeryd B: Disseminating effect of heparin on ex- perimental tumour metastases. Pathol Eur 4: 274, 1969.
Suemasu K, lshikawa S: Inhibitive effect of heparin and dextran sulfate on experimental pulmonary metastases. Gann 61: 125, 1970.
Elias EG, Shukla SK, Mink IB: Heparin and chemotherapy in the management of inoperable lung carcinoma. Cancer 36: 129.1975.
176 August 1977 The American Journal of Medicine Volume 63







![Pictorial review of Multiple Myeloma on whole body MRI and PET … · monoclonal immunoglobulins [1]. It is a common malignancy in patients above 40 (70% of cases are diagnosed between](https://img.pdfslide.us/doc/110x75/5fbdcc815cd23e0e940530f7/pictorial-review-of-multiple-myeloma-on-whole-body-mri-and-pet-monoclonal-immunoglobulins.jpg)