Embed Size (px)
Citation preview

Homocysteine status in former top-level male athletes: possible effectof physical activity and physical fitness
E. Unt1,2, K. Zilmer1, A. Magi3, T. Kullisaar1, C. Kairane1, M. Zilmer1
1Department of Biochemistry, University of Tartu, Tartu, Estonia, 2Institute of Exercise Biology and Physiotherapy, University ofTartu, Tartu, Estonia, 3Sports Medicine and Rehabilitation Clinic, Tartu University Hospital, Tartu, EstoniaCorresponding author: Eve Unt, MD, PhD, Institute of Exercise Biology and Physiotherapy, University of Tartu, Jakobi 5,Tartu 51013, Estonia. Tel: 1372 7 375 369, Fax: 1372 7 375 366, E-mail: [email protected]
Accepted for publication 17 February 2007
The importance of elevated homocysteine (Hcy) as a riskmarker for cardiovascular disease is continously underdebate. Lifestyle factors may increase the total Hcy(tHcy) level of the plasma, but there are no consistentfindings relating to Hcy, physical activity, and cardiore-spiratory fitness. Cross-sectional measurement from anongoing follow-up study was performed on 77 former maleathletes and 33 sedentary controls (age range 35–62 years).Lifestyle parameters (current physical activity patterns,smoking, etc.), anthropometric and blood pressure data,and data about tHcy, reduced, and oxidized glutathione(GSH, GSSG, respectively) in blood, lipoproteins, and
maximal oxygen consumption (VO2max) were collected.Our study results showed that the subgroup of physicallyactive ex-athletes (n5 52) had a significantly lower tHcylevel and glutathione redox ratio (GSSG:GSH) in compar-ison with the subgroup of sedentary ex-athletes (n5 25).tHcy level was inversely related to cardiorespiratory fitness(VO2max/kg). Dietary and smoking habits were not signifi-cantly associated with the tHcy level in our study group. Inconclusion, the research findings indicate that both currentphysical activity and cardiorespiratory fitness are signifi-cantly inversely associated with an elevated homocysteinelevel in middle-aged former athletes.
The importance of elevated homocysteine (Hcy) as apossible risk marker for cardiovascular disease(CVD) is continously under debate (Wald et al.,2002; Fruchart et al., 2004; Kaul et al., 2006). Severallifestyle factors (smoking, dietary habits, etc.), ele-vated blood pressure (BP), renal dysfunction, andeven some medicine intake may increase the totalHcy (tHcy) level of the plasma (Homocysteine Stu-dies Collaboration, 2002; Bolander-Gouaille & Bot-tiglieri, 2003; Kaul et al., 2006). However, there areno consistent findings relating to Hcy, physicalactivity, and cardiorespiratory fitness.Homocysteine is a thiol-containing aminoacid that
is produced by intracellular demethylation ofmethionine. Intracellular Hcy levels are normallymaintained within a narrow range by the activityof transsulphuration and remethylation pathways(Andreotti et al., 2000; Bolander-Gouaille & Botti-glieri, 2003). The mechanisms by which Hcy canrelate to vascular risk include endothelial dysfunc-tion, inflammatory response, oxidation of low-den-sity lipoprotein-cholesterol (LDL), and plateletactivation (Poddar et al., 2001; Splaver et al.,2004). Moreover, Hcy metabolism is closely relatedto the glutathione system (characterized by glu-tathione redox ratio), which is important in the
protection of cells against oxygen-derived free radi-cals (Bolander-Gouaille & Bottiglieri, 2003).Regular physical activity and exercise are recom-
mended for the maintenance of optimal health andprevention or management of chronic disease (Boothet al., 2000). Long-term exercise favorably modifiesseveral CVD risk factors including blood lipids,obesity, BP, and glucose tolerance. The presentunderstanding suggests that regular exercise is alsoassociated with better antioxidant capacity (Sen,1995). There is evidence that physical activity mayalso alter Hcy metabolism by increasing protein and/or methyl group turnover (Gibala, 2001). However,there are contradictory data available concerning theassociations between Hcy and exercise (Joubert &Manore, 2006). On the one hand, the Hcy level canbe influenced by the duration, intensity, and mode ofexercise; on the other, the Hcy level may be depen-dent on the individual fitness level of participants(Joubert & Manore, 2006).Former athletes represent a subgroup who have
been at the upper level of sports activity for severalyears, and their post-competitive lifestyle has beenshown to be more healthier than that of the generalpopulation (Fogelholm et al., 1994; Pihl et al., 1998).Thus, the relatively high level of sports activity and
Scand J Med Sci Sports 2008: 18: 360–366 Copyright & 2007 The Authors
Journal compilation & 2007 Blackwell MunksgaardPrinted in Singapore .All rights reservedDOI: 10.1111/j.1600-0838.2007.00674.x
360

aerobic fitness may increase the statistical power indetecting associations between tHcy and physicalactivity.The purpose of this cross-sectional study was to
investigate the level of Hcy and glutathione redoxratio in relation to physical activity and cardiore-spiratory fitness in former top-level athletes andcontrols.
Materials and methodsStudy subjects
Initially, we studied 118 middle-aged male subjects (35–62years old) who were recruited from the ongoing follow-upstudy with the baseline measurements in 1993–1994 (Pihl et al.,1998). The study subjects comprised 82 former athletes and 36age-matched controls. Inclusion criteria for ex-athletes in-cluded previous participation in endurance sports events andsports games at the international or national level at least 15years ago and being without the history of anabolic steroiduse. The control group consisted of males age-matched to ex-athletes who were currently physically inactive and had nocompetitive sports history. They were mostly fellow workersof former athletes.
The former athletes were subdivided into those who werestill physically active, that is, exercising regularly three ormore times per week [physically active ex-atheletes – (PAEA),n5 53] and those with less activity, who were classified assedentary [sedentary ex-athletes – (SEA), n5 29]. A total ofeight subjects (five ex-athletes and three controls) were ex-cluded due to treatment for hypertension. Thus, we ended upwith 52 subjects in the PAEA group, 25 subjects in the SEAgroup, and 33 in the control group.
All the subjects were Caucasian and belonged to themiddle-to-high socioeconomic class. The Medical Ethics Com-mittee of the University of Tartu approved the protocol, andall the participants signed an informed consent document. Allsubjects passed a routine medical examination that included acomplete history, physical examination, and electrocardiogra-phy. None of the participants had any signs and symptoms foracute or chronic diseases. All the study subjects were prohib-ited from participating in vigorous exercise and smoking atleast 24 h before the examination.
Measures
Lifestyle variables
The general health status and lifestyle parameters (smoking,alcohol consumption, dietary habits, etc.) of the study subjectswere evaluated by the modified questionnaire of Fogelholmet al. (1994). Smoking was classified as never, quit smoking,smokes cigars or a close family member smokes, smokes fewerthan 15 cigarettes per day, or smokes more than 15 cigarettesdaily. In addition, the subjects were asked to specify thenumber of cigarettes smoked per day.
Additionally, the subjects recorded their competitive ath-letic history and the current sports activity during the past 12months in detail (mode, weekly frequency, mean duration,intensity). On the basis of detailed physical activity informa-tion, we calculated the score of leisure-time physical activity asMET-hours per week (MET is the ratio of the work metabolicrate to the resting metabolic rate). MET was calculated as aproduct of intensity � duration � frequency. The scoring ofMETs was based on the data of Ainsworth et al. (1993) where
four METs corresponded to walking, seven METs to jogging,and 12 METs to running.
Maximal oxygen consumption
Subjects underwent a maximal exercise test to determinemaximal O2 consumption and maximal workload capacity(Wmax). They performed the modified Balke test on treadmill –the treadmill was kept at a constant speed 6.0 km/h with gradestarting 0.0% and increasing by 2.5% at 3min intervals.VO2max was measured using ‘‘breath by breath’’ gas monitor-ing (Oxygen Record, Erich Jaeger, Friedburg, Germany).Subjects were required to meet two of the three standardcriteria for having achieved VO2max (heart rate �age-pre-dicted maximum heart rate, respiratory exchange ratio�1.10, rating of perceived exertion �19). The exercise testswere carried out two to four hour after breakfast.
Anthropometric measurements
Subjects’ height and weight were determined by the Martinmetal anthropometer (�0.1 cm) and clinical scales (�0.05kg),respectively. The body mass index (BMI) was calculated (kg/m2).Body fat percentage was assessed by the dual-energy x-rayabsorptiometry method (Lunar, DPX-IQ, Madison, WI, USA).
BP measurements
Sitting BP was measured using a mercury sphygmomanometerafter a 5-minute rest. Systolic (Korotkoff phase 1) anddiastolic (Korotkoff phase 5) BP (SBP, DBP) were measuredtwice on the left upper arm, and the average was used for theanalysis. Elevated BP was established on the basis of SBP�135mmHg and DBP �85mmHg (NCEP ATP III, 2001).
Laboratory procedures
Blood samples were obtained in the morning after a 12 h fast.During 4 weeks before the study, the subjects were advised toavoid the use of vitamin supplements. Venous blood sampleswere collected into EDTA vacutainers, placed on ice, andcentrifuged within one to two hour. Plasma for tHcy andsamples of reduced and oxidized glutathione (GSH, GSSG,respectively) in blood were stored at �70 1C until the analysis.tHcy was measured using an Axis
s
Homo-cysteine EnzymeImmunoassay (Dundee, UK). The assessment of GSH andGSSG has been described previously by Kullisaar et al. (2002).The glutathione system redox potency was expressed as theGSSG:GSH. Serum total cholesterol (CHOL), high-densitylipoprotein-cholesterol (HDL-C), low-density lipoprotein-cholesterol (LDL-C), and triglycerides (TG) were measuredenzymatically by standard enzymatic methods at the Labora-tory Department of the Tartu University Clinic.
Statistical analysis
The results are presented as a mean � standard deviation. ThePearson’s product–moment or Spearman correlations wereused to determine the relationships between the variables.Partial correlation analysis was used to eliminate the effects ofage, smoking, and body weight. One-way analysis (ANOVA),followed by Tukey’s post hoc comparison was used for multi-ple comparisons between the groups. The w2-test was used todetermine the between-group differences in categorial vari-ables. Calculations were performed with the SPSS, version11.0 (SSPS Inc., Chicago, Illionois, USA) statistical package.Statistical significance was defined as Po0.05.
Homocysteine and exercise in former athletes
361
ResultsBP, anthropometric, and fitness data
Table 1 provides descriptive information on meanage, anthropometric data, BP, and physical workingcapacity (VO2max, VO2max/kg, W/kg) of the subjects.Our data showed statistically significantly lowermean BMI, and fat percentage in PAEA as comparedwith SEA and the controls. There were no significantdifferences in mean SBP, and DBP between thegroups, although the highest values were shownin SEA.
Biochemical data
Desciriptive data showed that PAEA had signifi-cantly lower CHOL in comparison with SEA andthe controls (Table 1). PAEA also had a significantlylower TG level as compared with SEA. No signifi-cant differences were found in LDL-C and HDL-Cbetween the groups.Table 1 presents the mean tHcy and glutathione
data of the groups. Statistically significantly lowertHcy and GSSG:GSH was found in PAEA in com-parison with SEA. No significant differences in thesebiochemical data were found between PAEA and thecontrols.
Almost half (n5 53) of the total study populationhad a tHcy level higher than 10 mmol/L; no between-group differences were found (there were 19, 17, 17subjects with a tHcy level over 10 mmol/L amongPAEA, SEA, and the controls, respectively). Amongthe SEA group, four men had a tHcy level higherthan 15 mmol/L, which was significantly different(according to a w2-test) from PAEA and the controlgroup, who had no subjects with tHcy over 15mmol/L.In this subgroup (tHcy over 15 mmol/L), the meanBMI was 29.5, SBP 138.3mmHg, DBP 92.0mmHg,CHOL 6.1mmol/L, HDL-C 1.3mmol/L, LDL-C3.0mmol/L, and TG 2.4mmol/L.
Lifestyle variables
There were no significant differences between thegroups with regard to current smokers, vegetable,fruit, coffee, and alcohol consumption (Table 2). Thevitamin intake (asked as regular, non-regular con-sumption, or non-consumption) of the groups wassimilar, showing no differences between the groups.There were eight, four, and four subjects, in PAEA,SEA, and the controls, respectively, who regularlytook vitamins. Thus, the study participants werecharacterized mostly by non- or non-regular con-sumption of vitamins.
Table 1. Mean anthropometric, blood pressure, physical working capacity data, lipoprotein, tHcy, GSH, GSSG and glutathione redox ratio (GSSG:GSH) of
the groups
Parameter PAEA (n 5 52) SEA (n 5 25) Controls (n 5 33)
Age( years) 44.7 � 6.7# 49.4 � 6.0 48.4 � 7.8Height (cm) 182.3 � 7.0 179.3 � 6.9 181.6 � 5.6Weight (kg) 84.4 � 11.6# 92.2 � 12.9 90.9 � 13.6BMI (kg/m) 25.3 � 2.4**### 28.7 � 3.1 27.5 � 3.4Body fat (%) 15.9 � 4.7***### 24.5 � 4.7 22.2 � 5.9SBP (mmHg) 130.6 � 12.4 136.6 � 14.7 135.0 � 14.9DBP (mmHg) 85.2 � 10.8 90.1 � 9.9 87.8 � 8.7VO2max (L/min) 4.0 � 0.5***### 3.42 � 0.56 3.44 � 0.53VO2max/kg mL/kg/min 48.0 � 6.5***### 37.0 � 6.5 37.9 � 7.1Wmax/kg W/kg 4.4 � 0.7***### 3.5 � 0.7 3.6 � 0.9METs 53.9 � 31.0***### 8.9 � 6.9 14.0 � 12.4CHOL (mmol/L) 5.08 � 1.07*## 5.96 � 1.14 5.77 � 1.13HDL-C (mmol/L) 1.46 � 0.32 1.33 � 0.30 1.39 � 0.31LDL-C (mmol/L) 3.51 � 0.85 3.51 � 1.07 3.68 � 1.20TG (mmol/L) 1.03 � 0.60### 1.73 � 1.17 1.43 � 0.62tHcy (mmol/L) 9.43 � 2.12### 12.32 � 4.49 10.55 � 2.50GSH (mmol/L) 1127.5 � 402.7 1044.3 � 587.3 1260.8 � 416.2GSSG (mmol/L) 63.7 � 22.5 63.4 � 25.9 53.3 � 26.7GSSG:GSH 0.06 � 0.02# 0.13 � 0.22 0.05 � 0.03
*Po0.05.**Po0.01.***Po0.001, values statistically significantly different from controls.#Po0.05.##Po0.01.###Po0.001, values statistically significantly different from SEA.
SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; CHOL, serum total cholesterol; HDL-C, high-density lipoprotein-
cholesterol; LDL-C, low-density lipoprotein-cholesterol; tHcy, total homocysteine; TG, triglycerides; PAEA, physically active ex-athletes; SEA, sedentary
ex-athletes; METs, score of leisure-time physical activity (MET-hours per week).
Unt et al.
362
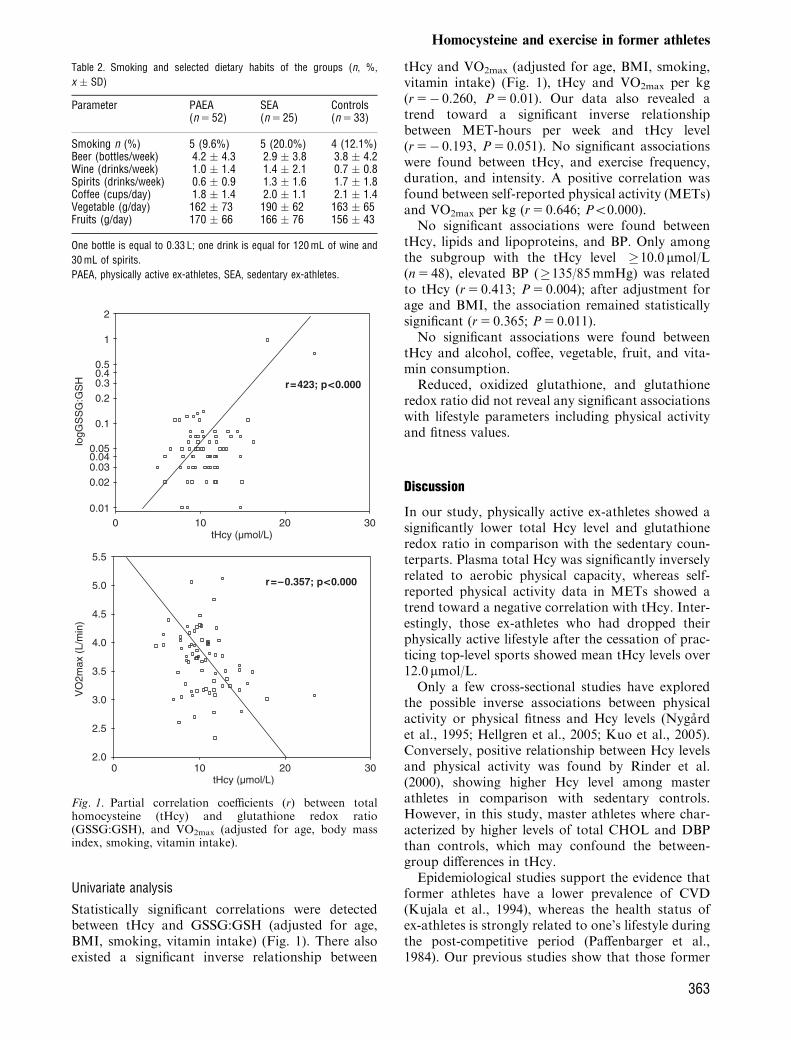
Univariate analysis
Statistically significant correlations were detectedbetween tHcy and GSSG:GSH (adjusted for age,BMI, smoking, vitamin intake) (Fig. 1). There alsoexisted a significant inverse relationship between
tHcy and VO2max (adjusted for age, BMI, smoking,vitamin intake) (Fig. 1), tHcy and VO2max per kg(r5� 0.260, P5 0.01). Our data also revealed atrend toward a significant inverse relationshipbetween MET-hours per week and tHcy level(r5� 0.193, P5 0.051). No significant associationswere found between tHcy, and exercise frequency,duration, and intensity. A positive correlation wasfound between self-reported physical activity (METs)and VO2max per kg (r5 0.646; Po0.000).No significant associations were found between
tHcy, lipids and lipoproteins, and BP. Only amongthe subgroup with the tHcy level �10.0 mmol/L(n5 48), elevated BP (�135/85mmHg) was relatedto tHcy (r5 0.413; P5 0.004); after adjustment forage and BMI, the association remained statisticallysignificant (r5 0.365; P5 0.011).No significant associations were found between
tHcy and alcohol, coffee, vegetable, fruit, and vita-min consumption.Reduced, oxidized glutathione, and glutathione
redox ratio did not reveal any significant associationswith lifestyle parameters including physical activityand fitness values.
Discussion
In our study, physically active ex-athletes showed asignificantly lower total Hcy level and glutathioneredox ratio in comparison with the sedentary coun-terparts. Plasma total Hcy was significantly inverselyrelated to aerobic physical capacity, whereas self-reported physical activity data in METs showed atrend toward a negative correlation with tHcy. Inter-estingly, those ex-athletes who had dropped theirphysically active lifestyle after the cessation of prac-ticing top-level sports showed mean tHcy levels over12.0 mmol/L.Only a few cross-sectional studies have explored
the possible inverse associations between physicalactivity or physical fitness and Hcy levels (Nygardet al., 1995; Hellgren et al., 2005; Kuo et al., 2005).Conversely, positive relationship between Hcy levelsand physical activity was found by Rinder et al.(2000), showing higher Hcy level among masterathletes in comparison with sedentary controls.However, in this study, master athletes where char-acterized by higher levels of total CHOL and DBPthan controls, which may confound the between-group differences in tHcy.Epidemiological studies support the evidence that
former athletes have a lower prevalence of CVD(Kujala et al., 1994), whereas the health status ofex-athletes is strongly related to one’s lifestyle duringthe post-competitive period (Paffenbarger et al.,1984). Our previous studies show that those former
Table 2. Smoking and selected dietary habits of the groups (n, %,
x � SD)
Parameter PAEA(n 5 52)
SEA(n 5 25)
Controls(n 5 33)
Smoking n (%) 5 (9.6%) 5 (20.0%) 4 (12.1%)Beer (bottles/week) 4.2 � 4.3 2.9 � 3.8 3.8 � 4.2Wine (drinks/week) 1.0 � 1.4 1.4 � 2.1 0.7 � 0.8Spirits (drinks/week) 0.6 � 0.9 1.3 � 1.6 1.7 � 1.8Coffee (cups/day) 1.8 � 1.4 2.0 � 1.1 2.1 � 1.4Vegetable (g/day) 162 � 73 190 � 62 163 � 65Fruits (g/day) 170 � 66 166 � 76 156 � 43
One bottle is equal to 0.33 L; one drink is equal for 120 mL of wine and
30 mL of spirits.
PAEA, physically active ex-athletes, SEA, sedentary ex-athletes.
tHcy (µmol/L)3020100
logG
SS
G:G
SH
2
1
0.50.40.3
0.2
0.1
0.050.040.03
0.02
0.01
tHcy (µmol/L)3020100
VO
2max
(L/
min
)
5.5
5.0
4.5
4.0
3.5
3.0
2.5
2.0
r=423; p<0.000
r=–0.357; p<0.000
Fig. 1. Partial correlation coefficients (r) between totalhomocysteine (tHcy) and glutathione redox ratio(GSSG:GSH), and VO2max (adjusted for age, body massindex, smoking, vitamin intake).
Homocysteine and exercise in former athletes
363

athletes who continued a physically active lifestyleafter the cessation of practising top-level sports havea significantly better cardiovascular risk and oxida-tive stress (Pihl et al., 1998; Pihl et al., 2003). There isan ongoing discussion on whether physical fitness is abetter and more sensitive marker of physical activitythan self-reported physical activity or not. In ourstudy, cardiorespiratory fitness had stronger associa-tions with the tHcy level than self-reported physicalactivity. Some data confirm that former athletes tendto maintain their physical fitness advantage overnon-athletes well into the middle age (Saltin &Grimby, 1968; Paffenbarger et al., 1984). Interest-ingly, our data show that there were no significantdifferences in cardiorespiratory parameters betweenthe sedentary ex-athletes and the controls. However,the cross-sectional data do not represent the time-dependent changes in maximal oxygen consumption,but there is a strong likelihood that ex-athletes hadsignificantly higher aerobic capacities during theirtop-level career.Although our cross-sectional study does not show
causal relationships between tHcy, physical fitness,and physical activity, we want to emphasize thatthose ex-athletes who remained sedentary duringtheir post-competitive period showed a significantlyhigher Hcy level (over 12.0 mmol/L) than their phy-sically active counterparts.Our data also revealed that elevated BP (�135/
85mmHg) was significantly associated with the tHcylevel only in those subjects whose tHcy level was�10.0 mmol/L. These data are in good agreementwith other studies showing relationships betweenHcy and hypertension (Nygard et al., 1997; El-Khairy et al., 1999; Muda et al., 2003). In addition,a recent consensus paper suggests that a Hcy levelhigher than 10 mmol/L may require treatment inpatients at increased risk (D.A.CH.-Liga Homocys-teine, 2003). Furthermore, another study refers toHcy levels of 12.1 mmol/L, which are significantlyassociated with higher cardiovascular risk (Leonget al., 2005). Thus, our findings support the sugges-tions that the non-problematic Hcy reference valuemight be lower �10.0 mmol/L. It is only natural thatwell-controlled randomized trials are needed forfurther re-evaluation for a safe and risk-free Hcythreshold value.The lower tHcy level in physically active indivi-
duals may be accounted for by better vitamin con-sumption. Folic acid and vitamins B6 and B12 areimportant cofactors for the enzyme metabolism ofHcy (Konig et al., 2003). Supplementation of thesecofactors reduces elevated Hcy concentrations; how-ever, there is no evidence that vitamin B supplemen-tation reduces cardiovascular risk (Kaul et al., 2006).In our study, the semiquantitative dietary analysisdid not reveal any significant differences in the
vitamin consumption and dietary habits of thegroups. Smoking is another lifestyle factor thatmay increase plasma Hcy level (Nygard et al., 1995;Mansoor et al., 1997; O’Callaghan et al., 2002). Inour study, the prevalence of smokers was relativelylow, and this may be one explanation for the non-confounding effect of smoking on the tHcy level.
Conclusions
According to between-group differences and correla-tion analysis, our study results confirm the evidencethat both current physical activity and cardiorespira-tory fitness are significantly associated with the tHcylevel in middle-aged former male athletes. Surpris-ingly, our data revealed a relatively high tHcy level inthose ex-athletes who had dropped their physicallyactive lifestyle after the cessation of practicing top-level sports.
Perspectives
In our study, the mean tHcy value was under10.0 mmol/L only in physically active ex-athletes,which may indicate that regularly physically activeex-athletes have a lower risk level for CVDs. Further-more, significant negative associations were detectedbetween cardiorespiratory fitness data and the tHcylevel in all subjects. The level of self-reported physicalactivity also showed a significant trend in relation totHcy. Thus, our findings support the previous datawhere physical activity and the tHcy level are in-versely related (Nygard et al., 1995; Hellgren et al.,2005; Kuo et al., 2005).The advantage of the present study is that both
self-reported physical activity as well as maximaloxygen consumption of the subjects were measured.In addition, fluctuation of lifestyle habits (e.g. reg-ular physical activity) of the subgroup of ex-athleteswas minimal.Although the present study focused primarily on
the association between physical activity/physicalfitness in relation to tHcy, a positive associationbetween elevated BP and the tHcy level was found(only in the subgroup with Hcy �10.0 mmol/L). Onehas to admit that our cross-sectional design does notshow any adverse health effects due to the elevatedlevel of tHcy; however, our descriptive between-group and correlation analysis demonstrates thatthe tHcy level is higher in those people who aresedentary and who had a lower level of cardiovas-cular fitness. In summary, the understanding of theoptimal tHcy level and interaction of several cardi-ovascular risk factors (including a sedentary lifestyle)is still unclear. We have designed this study as afollow-up, and the main health outcomes will beevaluated every 5–6 years.
Unt et al.
364

Thus, further studies are needed to evaluate cardi-ovascular risk, regular physical activity, and Hcy level.
Key words: exercise, homocysteine, glutathione, max-imal oxygen consumption, ex-athletes.
Acknowledgements
This study was partly funded by the target-financed themesno. 1833 and 1787 from the Ministry of Education andResearch of Estonia, and Grants no. 5496, and no. 6588 ofthe Estonian Science Foundation.
References
Ainsworth BE, Haskell WL, Leon AS,Jacobs Jr. DR, Montoye HJ, Sallis JF,Paffenbarger Jr. RS Compendium ofphysical activities: classification ofenergy costs of human physicalactivities. Med Sci Sports Exerc 1993:25: 71–80.
Andreotti F, Burzotta F, Manzoli A,Robinson K. Homocysteine and risk ofcardiovascular disease. J ThrombThrombolysis 2000: 9: 13–21.
Bolander-Gouaille C, Bottiglieri T.Homocysteine related vitamins andneuropsychiatric disorders. France:Springer-Verlag, 2003.
Booth FW, Gordon SE, Carlson CJ,Hamilton MT. Waging war onmodern chronic disease: primaryprevention through exercisebiology. J Appl Physiol 2000: 88: 774–787.
D.A.CH.-Liga Homocysteine. ConsensusPaper on the Rational Clinical Useof Homocysteine, Folic Acid, andB-Vitamins in Cardiovascular andThrombotic Diseases–Guidelines andRecommendations–German, Austrian,and Swiss Homocysteine Society, May2003.
El-Khairy L, Uueland PM, Nygard O,Refsum H, Vollset SE. Lifestyle andcardiovascular disease risk factors asdeterminants of total cysteine inplasma: the Hordaland HomocysteineStudy. Am J Clin Nutr 1999: 70: 1016–1024.
Expert Panel on Detection, Evaluation,and Treatment of High BloodCholesterol in Adults. ExecutiveSummary of the Third Report of theNational Cholesterol EducationProgram (NCEP) Expert Panel onDetection, Evaluation, and Treatmentof High Blood Cholesterol in Adults(Adult Treatment Panel III). JAMA2001: 285: 2486–2497.
FogelholmM, Kaprio J, Sarna S. Healthylifestyles of former Finnish world classathletes. Med Sci Sports Exerc 1994:26: 224–229.
Fruchart J-C, Nierman MC, Stroes ESG,Kastelein JJP, Duriez P. New riskfactors for atherosclerosis and patientrisk assessment. Circulation 2004:109(1): III15–III19.
Gibala MJ. Regulation of skeletal muscleamino acid metabolism during exercise.Int J Sport Nutr Exerc Metab 2001: 11:87–108.
Hellgren M, Melander A, Ostgren CJ,Rastam L, Lindblad U. Inverseassociation between plasmahomocysteine, sulphonylurea exposureand physical activity: a community-based sample of type 2 diabetespatients in the Skaraborg hypertensionand diabetes project. Diabetes ObesMetab 2005: 7: 421–429.
Homocysteine Studies Collaboration.Homocysteine and risk of ischemicheart disease and stroke: a meta-analysis. JAMA 2002: 288: 2015–2022.
Joubert LM, Manore MM. Exercise,nutrition, and homocysteine.Int J Sport Nutr Exerc Metab 2006:16: 341–361.
Kaul S, Zadeh AA, Shah PK.Homocysteine hypothesis foratherothrombotic cardiovasculardisease. Not validated. J Am CollCardiol 2006: 48: 914–923.
Kujala UM, Kaprio J, Taimela S, SarnaS. Prevalence of diabetes, hypertension,and ishemic disease in former eliteathletes. Metab Clin Experim 1994: 43:1255–1260.
Kullisaar T, Zilmer M, Mikelsaar M,Vihalemm T, Annuk H, Kairane C,Kilk A. Two antioxidative lactobacillistrains as promising probiotics. Int JFood Microbiol 2002: 72: 215–224.
Konig D, Bisse E, Deibert P, MullerH-M, Wieland H, Berg A. Influenceof training volume and acute physicalexercise on the homocysteine levels inendurance-trained men: interactionswith plasma folate and vitaminB12. Ann Nutr Metab 2003: 47:114–118.
Kuo HK, Yen CJ, Bean JF. Levels ofhomocysteine are inversely associatedwith cardiovascular fitness in women,but not in men: data from the NationalHealth and Nutrition ExaminationSurvey, 1999–2002. J Intern Med 2005:258: 328–335.
Leong T, Fitzgerald A, McGorrian C,Graham I. Homocysteine,apolipoprotein B/AI ratio and themetabolic syndrome are predictors of
cardiovascular risk using the SCOREsystem. Irish J Med Sci 2005:174(Suppl.): 58–59.
Mansoor MA, Kristensen O, Hervig T,Drablos PA, Stakkestad JA, Woie L,Hetland O, Osland A. Lowconcentrations of folate in serum anderythrocytes of smokers: methionineloading decreases folate concentrationsin serum of smokers and nonsmokers.Clin Chem 1997: 43: 2192–2194.
Muda P, Kampus P, Zilmer M, Zilmer K,Kairane C, Ristmae T, Fischer K,Teesalu R. Homocysteine and redblood cell glutathione as indices formiddle-aged untreated essentialhypertension patients. J Hypertension2003: 21: 2329–2333.
Nygard O, Nordrehaug JE, Refsum H,Ueland PM, Farstad M, Vollset SE.Plasma homocysteine levels andmortality in patients with coronaryartery disease. N Engl J Med 1997: 337:230–236.
Nygard O, Vollset SE, Refsum H,Stensvold I, Tverdal A, NordrehaugJE, Ueland M, Kvale G. Total plasmahomocysteine and cardiovascular riskprofile. The Hordaland HomocysteineStudy. JAMA 1995: 274: 1526–1533.
O’Callaghan P, Meleady R, Fitzgerald T,Graham I.The European COMACgroup. Smoking and plasmahomocysteine. Eur Heart J 2002: 23:1580–1586.
Paffenbarger Jr. RS, Hyde RT, Wing AL,Steinmetz CH. A natural history ofathleticism and cardiovascular health.JAMA 1984: 252: 491–495.
Pihl E, Jurimae T, Kaasik T. Coronaryheart disease risk factors in middle-aged former top-level athletes. Scand JMed Sci Sports 1998: 8: 229–235.
Pihl E, Zilmer K, Kullisaar T, Kairane C,Pulges A, Zilmer M. High-sensitiveC-reactive protein level and oxidativestress-related status in former athletesin relation to traditional cardiovascularrisk factors. Atherosclerosis 2003: 171:321–326.
Poddar R, Sivasubramanian N, DiBelloPM, Robinson K, Jacobsen DW.Homocysteine induces expression andsecretion of monocyte chemoattractantprotein-1 and interleukin-8 in human
Homocysteine and exercise in former athletes
365

aortic endothelial cells: implications forvascular disease. Circulation 2001: 103:2717–2723.
Rinder MR, Spina RJ, Ehsani AA.Enhanced endothelium-dependentvasodilation in older endurance-trainedmen. J Appl Physiol 2000: 88: 761–766.
Saltin B, Grimby G. Physiologicalanalysis of middle-aged and old former
athletes. Comparison with still activeathletes of the same age. Circulation1968: 38: 1104–1115.
Sen CK. Oxidants and antioxidants inexercise. J Appl Physiol 1995: 79:675–686.
Splaver A, Lamas GA, Hennekens CH.Homocysteine and cardiovasculardisease: biological mechanisms,
observational epidemiology, and theneed for randomized trials. Am Heart J2004: 148: 34–40.
Wald DS, Law M, Morris JK.Homocysteine and cardiovasculardisease: evidence and causality froma meta-analysis. JAMA 2002: 325:1202–1226.
Unt et al.
366
![A PATIENT’S GUIDE TO MEDICAL FOODS, SPECIALTY TOPICALS ... · Homocysteine levels Pyridoxal 5’-phosphate [active vitamin B 6] – Advanced glycation end products – Homocysteine](https://img.pdfslide.us/doc/110x75/5f87f6a15e09f21917510fa7/a-patientas-guide-to-medical-foods-specialty-topicals-homocysteine-levels.jpg)



![Homocysteine-lowering interventions for preventing … · 2018. 12. 15. · [Intervention Review] Homocysteine-lowering interventions for preventing cardiovascular events Arturo J](https://img.pdfslide.us/doc/110x75/5ff89452656730039f05d58a/homocysteine-lowering-interventions-for-preventing-2018-12-15-intervention.jpg)
























