Embed Size (px)
Citation preview

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Neurology Vol 2 July 2003 http://neurology.thelancet.com 425
Rapid reviewHomocysteine and AD
Lancet Neurology 2003: 2: 425–28
A link between hyperhomocysteinaemia or B-group-vitamindeficiency and dementia are logical extensions of the well-established connection between homocysteine and vasculardisease.1,2 However, reports of a connection between B-group-vitamin deficiency and cognitive dysfunctionappeared in the literature long before homocysteine gainedprominence as a cardiovascular risk factor in the 1990s.Early reports noted a high occurence of vitamin-B12deficiency in psychogeriatric populations3 and a highprevalence of hyperhomocysteinaemia in elderly patientswith dementia.4–6 Critics of the hypothesis that B-group-
vitamin deficiency causes dementia have suggested thatdemented patients’ inability to care for themselves explainsthe B-group-vitamin deficiency; however, studies of otherindicators of nutritional status showed that this was not thecause.7–9 Although several studies involved non-demented,community-dwelling elderly patients,10–13 results may beapplicable to the relation between hyperhomocysteinaemiaand AD, because non-demented people who do poorly intests of cognitive-function can have preclinical AD. Indeed,the disease has been described as the endpoint of a steadydecline in cognitive and psychosocial function.14
Some studies of hyperhomocysteinaemia and poorcognitive function found no link,15 and those that did couldnot rule out covert vascular disease as the true cause of poorcognitive ability in patients with hyperhomocysteinaemia.
The early studies raised several questions abouthyperhomocysteinaemia to which epidemiological studymight be applied: Firstly, does it cause AD? Secondly, does itcause dementia? And thirdly, does hyperhomocysteinaemiaconcomitant with AD result in more severe dementia or afaster decline?
Recent epidemiological studies ofhomocysteine and ADA study of 43 volunteers diagnosed with probable or possibleAD and 37 controls from the same population of outpatientssuggested that hyperhomocysteinaemia was not related toAD.16 Any apparent link was explained by the coexistence ofthe AD and vascular disease. Nevertheless, after accountingfor history of clinically evident vascular events, the patientswith AD in this small study were more than twice as likely ascontrols to be hyperhomocysteinaemic, and the confidenceinterval for the odds ratio indicated consistency with a valueas high as 16 (table).17,18,19 These findings were similar to thosepreviously obtained by Clarke and colleagues,20 who found aneven stronger association when analyses were restricted tocases of dementia confirmed as AD at autopsy. Furthermore,results of a small case-control study of volunteers could notnegate the independent link between homocysteineconcentration and AD among more than 1000 patients in theFramingham Study.8 The researchers estimated that 16% of
MSM is at Jean Mayer United States Department of AgricultureHuman Nutrition Research Center on Aging at Tufts University,Boston, MA, USA.
Correspondence: Dr Martha Savaria Morris, JM-USDA HNRCA,Tufts University, 711 Washington Street, Boston, MA 02111, USA. Phone +1 617 556 3302; fax +1 617 556 3344; email [email protected]
Homocysteine and Alzheimer’s disease
Martha Savaria Morris
BackgroundA high circulating concentration of the amino acid homocysteineis an independent risk factor for stroke. Alzheimer's disease (AD)commonly co-occurs with stroke. Epidemiological studies foundassociations between hyperhomocysteinaemia and bothhistologically confirmed AD and disease progression andrevealed that dementia in AD was associated with evidence ofbrain infarcts on autopsy. Thus, hyperhomocysteinaemia and ADcould be linked by stroke or microvascular disease. However,given known relations between B-group-vitamin deficiency andboth hyperhomocysteinaemia and neurological dysfunction,direct causal mechanisms are also plausible.
Recent developments A recent prospective study (S Seshadri and colleagues N Engl JMed; 2002 346: 476–83) showed hyperhomocysteinaemia to bea strong, independent risk factor for dementia and AD. Theresearchers found a graded increase in risk of both outcomeswith rising plasma concentration of homocysteine aftermultivariate control for putative risk factors for AD. In conjunctionwith demonstration of a fall in homocysteine concentrations inresponse to increasing B-group-vitamin status, these findingsgive hope that mental decline, or AD itself, could be prevented bydietary modification or food fortification.
Where next?25% of dementia cases are attributed to stroke. The possibilitythat some of the other 75% might be prevented by the loweringof homocysteine concentrations greatly increases the hope ofmaintaining self-sufficiency into old age. If homocysteinelowering can reduce the incidence of dementia or AD, decreasedincidence of these disorders may be seen in Canada and theUSA, where government-mandated folate-fortificationprogrammes are in effect. Future research should focus on earlydetection of AD and on the possibility that the disease itself, or itsprimary symptom, could be prevented by folatesupplementation.

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Neurology Vol 2 July 2003 http://neurology.thelancet.com426
AD in the Framingham cohort was attributable tohyperhomocysteinaemia. Results of another early7 and arecently published9 case-control study also support theconclusion that AD and hyperhomocysteinaemia areconnected. After multivariate control for potentiallyconfounding factors and nutritional status indicators, McIlroyand colleagues9 found that hyperhomocysteinaemia was moreprevalent in patients with vascular dementia, those with AD,and non-demented patients with stroke than it was in healthycontrol individuals. This association was statisticallysignificant for patients with dementia and AD, but was notsignificant for non-demented patients with stroke when othervascular disease was controlled for.
A recent prospective study assessed the possiblecontribution of B-group-vitamin deficiency to AD risk.21 Lowfolate or vitamin B12 status at baseline in non-dementedresidents of Stockholm was associated with double the risk ofbeing diagnosed with AD 3 years later, even when vasculardiseases were accounted for. The researchers offered noexplanation for the unexpected finding that the associationwas confined to participants with high cognitive function testscores at baseline. However, the number of individuals in thepost-hoc analysis was small, and whether the statisticalinteraction had been formally tested was unclear.
Studies of homocysteine and early temporal-lobe changesAn investigation prompted by the finding of a relationbetween atrophy of the temporal medial lobe and
hyperhomocysteinaemia in AD sought to determine whetherhippocampal width, which is known to decrease with age, wasrelated to plasma concentrations of homocysteine incommunity-dwelling elderly people.22 The individuals had noclinical memory problems, and cognitive function tests wereused to screen out volunteers with mental impairment. Thestudy found that hippocampal width decreased significantlywith increasing homocysteine concentration—a result thatwas due to neither age nor to body mass index, both of whichare known correlates of the outcome. The researchersinterpreted their findings as suggestive of a damaging effect ofhyperhomocysteinaemia on the hippocampus, which wasseen as the proximal cause of the memory deficits.
More recently, plasma concentration of homocysteinewas found to be inversely related to hippocampal andcortical volume as determined by MRI.23 Homocysteine wassignificantly associated with the early markers of AD aftercarotid atherosclerosis or white-matter lesions—which aresymptomatic of small-vessel disease—were controlled for.
Possible mechanisms for the associationbetween hyperhomocysteinaemia and ADThe Nun Study,24 a longitudinal study of ageing and AD, foundthat dementia was worse in the presence of brain infarcts,therefore, hyperhomocysteinaemia may contribute to ADdementia by induction of vascular changes. However,homocysteine was directly excitotoxic to cortical neurons incell culture, which suggests a causal role for the amino acid inthe cholinergic deficit characteristic of AD.25 Alternatively,
Rapid review Homocysteine and AD
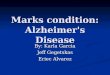
Recently published epidemiological studies investigating the relationship between homocysteine and AD
Reference Study design Diagnostic criteria Effect measure Covariates Results(patients/non-cases)
McCaddon7 Case-control (30/30) DSM-III-R for senile Difference in mean Gender, age, smoking, hypertension, and Patients; 21·9 �mol/Ldementia of Alzheimer serum tHcy concentrations of B12 and folate Controls, 12·2 �mol/Ltype p <0·0001
Seshadri8 Prospective (44/636) NINCDS-ADRDA for RR per one SD Gender, age, ApoE genotype, plasma RR (95% CI), definite, probable, or increase in the B vitamin concentrations, education, 1·8 (1·3–2·5)possible AD log-transformed systolic blood pressure, smoking status,
plasma tHcy alcohol intake, presence of diabetes, BMI, and stroke history
McIlroy9 Case-control (83/71) NINDS-ADRDA for OR for plasma Gender, age, hypertension, cholesterol, OR (95% CI), probable AD tHcy �13·3 �mol/L adult and childhood socioeconimic status, 2·9 (1·0–8·1)
vs a lower value education, smoking, BMI, MNA, concentrations of creatinine, B12, folate, pyridoxal phosphate, and pyridoxal
Miller16 Case-control (43/37) NINDS-ADRDA for OR for plasma tHcy Gender, age, folate concentration in OR (95% CI), possible or probable >12 �mol/L vs a erythrocytes, plasma concentration of 2·2 (0·31–16·00)AD lower value B12, serum creatinine, and serum TSH
Clarke17 Case-control (164/108) CERAD for definite or OR for top third Gender, age, smoking, socioeconomic OR (95% CI) for probable AD, autopsy vs bottom third class, and ApoE �4 concentration confirmed, 4·5 (2·2–9·2);confirmation of 76 of for serum tHcy OR for clinically 103 deceased diagnosed, 2·0 (1·1–3·4)
Wang18 Prospective (59/310) DSM-III-R for gradual RR for serum B12 Gender, age, and education RR (95% CI), onset and progressive �150 pmol/L or folate 2·1 (1·2–3·5)deterioration of �10 nmol/L vs normaldementia and exclusion higher concentrations of other specific causes of both vitamins
tHcy=total homocysteine; DSM-III-R=Diagnostic and Statistical Manual of Mental Disorders (3rd edn-revised);17 NINDS-ADRDA=National Institute of Neurological Disorders and
Stroke–Alzheimer’s Disease and Related Disorders Association;18 CERAD= Consortium To Establish A Registry For Alzheimer’s Disease;19 OR=odds ratio; RR=relative risk; BMI=body
mass index; TSH=thyroid-stimulating hormone; MNA=mini-nutritional assessment.

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Neurology Vol 2 July 2003 http://neurology.thelancet.com 427
neuronal death through apoptosiscould result from folate deficiency via S-adenosyl-methionine (SAM) de-pletion and resultant hypomethylation,and hyperhomocysteinaemia may be anepiphenomenon.26
Amyloid-� peptide (A�), whichaggregates to form senile plaques in AD,has long been suspected to contribute todisease progression by inducingoxidative stress.27 More recently,McCaddon and colleagues28,29 proposedthat folate deficiency, hyperhomo-cysteinaemia, and cognitive deficitsassociated with AD were caused by theeffects of oxidative stress on themetabolism of methionine. In a studyof 50 patients with AD and 57 healthy volunteers, the glutathioneconcentrations in patients and controlswere similar. However, in the patients,low glutathione concentrations wereassociated with worse cognitive scores,but hyperhomocysteinaemia was not.When compared with controls, thepatients had high concentrations ofboth homocysteine and cysteine, whichled McCaddon and colleagues toconclude that transsulphuration ofhomocysteine to cysteine was intact butremethylation of homocysteine to methionine was disturbedin the patients with AD (figure). Although transsulphuration isa disposal pathway for homocysteine, it is stimulated by SAM,which would be in short supply under conditions of reducedhomocysteine remethylation. Consequently, excesshomocysteine would be exported to the bloodstream, resultingin hyperhomocysteinaemia. This scenario was consistent withthe vulnerability of the vitamin-B12-dependent enzymemethionine synthase to oxidative stress and previous reports ofincreased transsulphuration in an oxidative environment andlow concentrations of SAM in AD. McCaddon and colleaguessuggested that excess cerebral oxidative stress might result indepleted glutathione stores—a possible explanation for thecross-sectional association they found between low glutathioneconcentrations and indicators of AD progression.Alternatively, low glutathione concentrations might reflect aninability to compensate for potential oxidative damage causedby folate deficiency or excess homocysteine.27 This hypothesisexplains the low serum concentration of folate in AD as aconsequence of the methyl folate trap.
Normally, folate is retained in cells as polyglutamate.However, methionine synthase inactivation results in thetrapping of folate in the monoglutamate form, which leaksout of cells. A recent study showed that the efficiency ofrenal 5-methyltetrahydopteroylglutamate excretion in ratsincreases in response to high concentrations of folate in theplasma,30 supporting McCaddon and colleagues’ suggestionthat the failure of polyglutamation leads to folatedepletion.
Some theorists favour the hypothesis that the connectionbetween folate deficiency and AD is causal, with either highhomocysteine or decreased SAM as an intermediary. In arecent study by Kruman and colleagues,26 culture in a mediumdeficient in folic acid and methionine or rich in homocysteinecaused the death of hippocampal neurons and increased A�-induced death. Furthermore, neurons incubated inhomocysteine alone had more DNA damage than neuronsincubated in a control medium (although this damage wasreversible). Neither deficiency of folate or methionine nor A�resulted in more DNA damage than was seen in the controlmedium. However, A� combined with either homocysteine,folate, or methionine deficiency resulted in more DNA damagethan A� alone; this damage was not reversible. Furtheranalyses showed that A� alone caused reversible oxidativedamage involving an increase in 8-oxyguanine, but that cellsincubated in a folate or methionine deficient medium couldnot repair DNA after exposure to A�. Addition to the culturesof an enzyme that removes misincorporated uracil showed thatthe effect of the folate-deficient or methionine-deficient mediawas a highly significant increase in uracil misincorporation.Moreover, addition of purines and thymidine to the mediumresulted in less cell death. Kruman and colleagues concludedthat methyl-donor deficiency and homocysteine affect theavailability of purines and thymidine for DNA repair and thuspromote the accumulation of DNA damage caused byoxidative stress. That the combination of A� deposits withfolate deficiency or hyperhomocysteinaemia results inneuronal death was supported by in vivo experiments showing
SAMcycle
Folatecycle
Trans-sulphurationpathway
Methionine THF
ATP Serine
Serine
GlycineSAM
Homocysteine
Cystathionine
Methylene-THF
Methyl-THF
SAH
MS
MTHFR
Acceptor
Methylatedacceptor
CBS
Cysteine
Glutathione
SAM
SAM
SAHhydrolase
Cystathionase
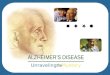
Two cycles in the metabolism of homocysteine. Methyl transfer from methyl-THF to homocysteine,which is catalysed by vitamin-B12-dependent methionine synthase, produces methionine andtetrahydrofolate (THF). Methionine is then activated by ATP to produce SAM, which donates a methylgroup to an acceptor molecule to produce S-adenosylhomocysteine (SAH). Finally, SAH hydrolasecatalyses the conversion of SAM into homocysteine. Vitamin-B6-dependent carbon exchange fromserine to free THF produces methylene-THF and glycine. Reduction of methylene-tetrahydrofolate bymethylene tetrahydrofolate reductase (MTHFR)—which is inhibited by SAM—produces methyl-THF.Vitamin-B6-dependent cystathionine-�-synthase (CBS)—which is activated by SAM—catalyses theconversion of homocysteine to cysathionine. Cysathionase catalyses the conversion of cystathione tocysteine, which is a precusor of glutathione.
Rapid reviewHomocysteine and AD

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Neurology Vol 2 July 2003 http://neurology.thelancet.com428
that the extent of neuronal death was significantly greater inmutant transgenic mice with A� deposits maintained on a folicacid, homocysteine-raising diet than among mutant micemaintained on a normal diet or wild-type mice maintained oneither diet.
To explain what processes might link deficient DNA-repairmechanisms to neuronal death Kruman and colleagues26 pointout that, when DNA damage cannot be repaired, factors thatnormally shift a dividing cell’s activities from mitosis to repaircan also trigger apoptosis. The finding of proteins that controlcell division in the cerebral cortex of patients with ADprompted an investigation into whether hyperhomocys-teinaemia in patients with AD is related to expression of cyclinE and cyclin B, which indicate re-entry into the cell-divisioncycle and progression to the G2 phase, respectively.31
Independent of known risk factors for hyperhomocys-teinaemia, total serum concentration of homocysteine washigher in patients whose hippocampal neurons expressed cyclinE than it was in patients in who did not have hippocampalexpression of cyclin E. No such relation was found betweenhomocysteine concentration and expression of cyclin B. Theauthors suggested that hyperhomocysteinaemia might triggerthe production of cell division proteins, which, in the absence ofdivision, result in pathology or death. Alternatively, the cell-division proteins might be markers of failure of DNA repair inthe presence of hyperhomocysteinaemia and a consequent shiftof activities from repair to apoptosis.
ConclusionAn association between hyperhomocysteinaemia and AD iswell established. Furthermore, the follow-up study by Seshadri
and colleagues8 showed that high homocysteine concentrationpreceded the diagnosis of AD. Because the diagnosis wouldlikely have been made long after disease onset, reversecausation might seem plausible. However, homocysteinemeasurements taken 8 years earlier in a subset of patients gavesimilar results. Studies relating changes in the temporal lobe tohyperhomocysteinaemia lend support to the view that thissymptom precedes the onset of disease, and several studieshave shown the association to be independent of vasculardisease. Some studies found associations between vitamin-Bdeficiency and AD. However, in the Framingham cohort, suchassociations were not independent of homocysteine.
The links between homocysteine, folate, and AD are likelyto be complex. However, complete understanding of themechanisms involved is not necessary for prevention. Studiesof folate supplementation in depression, one of severalneuropsychiatric diseases also associated with low folate status,have shown benefits even when folate status was not low.32 Thismay be because serum folate concentrations do not reflectconcentrations in the CNS or, as Shea and Rogers33 havesuggested, folate requirements are increased inneuropsychiatric diseases. Whether AD is more likely to resultfrom homocysteine toxicity or a deficiency of folate or SAM,folate-supplementation trials should continue.
Conflict of interestI have no conflicts of interest.
Role of the funding sourceThis review is based upon work supported by the US Department ofAgriculture, under agreement number 58-1950-9-001.
Rapid review Homocysteine and AD
References1 Boushey CJ, Beresford SA, Omenn GS,
Motulsky AG. A quantitative assessment of plasmahomocysteine as a risk factor for vascular disease:probable benefits of increasing folic acid intakes.JAMA 1995; 274: 1049–57.
2 Refsum H, Ueland PM, Nygard O, Vollset SE.Homocysteine and cardiovascular disease. Annu RevMed 1998; 49: 31–62.
3 Nilsson K, Gustafson L, Faldt R, et al.Hyperhomocysteinaemia: a common finding in apsychogeriatric population. Eur J Clin Invest 1996;26: 853–59.
4 Bell IR, Edman JS, Selhub J, et al. Plasmahomocysteine in vascular disease and in nonvasculardementia of depressed elderly people. Acta PsychiatrScand 1992; 86: 386–90.
5 Leblhuber F, Walli J, Artner-Dworzak E, et al.Hyperhomocysteinemia in dementia. J NeuralTransm 2000; 107: 1469–74.
6 Gottfries CG, Lehmann W, Regland B. Earlydiagnosis of cognitive impairment in the elderlywith the focus on Alzheimer’s disease. J NeuralTransm 1998; 105: 773–86.
7 McCaddon A, Davies G, Hudson P, Tandy S,Cattell H. Total serum homocysteine in seniledementia of Alzheimer type. Int J Geriatr Psychiatry1998; 13: 235–39.
8 Seshadri S, Beiser A, Selhub J, et al. Plasmahomocysteine as a risk factor for dementia andAlzheimer’s disease. N Engl J Med 2002; 346:476–83.
9 McIlroy SP, Dynan KB, Lawson JT, Patterson CC,Passmore AP. Moderately elevated plasmahomocysteine, methylenetetrahydrofolate reductasegenotype, and risk for stroke, vascular dementia,and Alzheimer disease in Northern Ireland. Stroke2002; 33: 2351–56.
10 Riggs KM, Spiro A 3rd, Tucker K, Rush D. Relationsof vitamin B-12, vitamin B-6, folate, andhomocysteine to cognitive performance in theNormative Aging Study. Am J Clin Nutr 1996; 63:306–14.
11 Ravaglia G, Forti P, Maioli F, et al. Homocysteine
and cognitive function in healthy elderlycommunity dwellers in Italy. Am J Clin Nutr 2003;77: 668–73.
12 Morris MS, Jacques PF, Rosenberg IH, Selhub J.Hyperhomocysteinemia associated with poor recallin the third National Health and NutritionExamination Survey. Am J Clin Nutr 2001; 73:927–33.
13 Budge MM, de Jager C, Hogervorst E, Smith AD.Total plasma homocysteine, age, systolic bloodpressure, and cognitive performance in older people. J Am Geriatr Soc 2002; 50: 2014–18.
14 Burns A, Zaudig M. Mild cognitive impairment inolder people. Lancet 2002; 360:1963–65.
15 Kalmijn S, Launer LJ, Lindemans J, Bots ML,Hofman A, Breteler MM. Total homocysteine andcognitive decline in a community-based sample ofelderly subjects: the Rotterdam Study.Am J Epidemiol 1999; 150: 283–89.
16 Miller JW, Green R, Mungas DM, Reed BR, JagustWJ. Homocysteine, vitamin B6, and vascular diseasein AD patients. Neurology 2002; 58: 1471–75.
17 American Psychiatric Association: Diagnostic andStatistical Manual for Mental Disorders, 3rd edn.Washington: American Psychiatric Press, 1987.
18 McKhann G, Drachman D, Folstein M, Katzman R,Price D, Stadlan EM. Clinical diagnosis ofAlzheimer's disease: report of the NINCDS-ADRDAWork Group under the auspices of Department ofHealth and Human Services Task Force onAlzheimer’s Disease. Neurology 1984; 34: 939–44.
19 Mirra SS, Heyman A, McKeel D, et al. TheConsortium to Establish a Registry for Alzheimer'sDisease (CERAD). Part II. Standardization of theneuropathologic assessment of Alzheimer’s disease.Neurology 1991; 41: 479–86.
20 Clarke R, Smith AD, Jobst KA, Refsum H, Sutton L,Ueland PM. Folate, vitamin B12, and serum totalhomocysteine levels in confirmed Alzheimer disease.Arch Neurol 1998; 55: 1449–55.
21 Wang HX, Wahlin A, Basun H, Fastbom J,Winblad B, Fratiglioni L. Vitamin B(12) and folatein relation to the development of Alzheimer’sdisease. Neurology 2001; 56: 1188–94.
22 Williams JH, Pereira EA, Budge MM, Bradley KM.Minimal hippocampal width relates to plasmahomocysteine in community-dwelling older people.Age Ageing 2002; 31: 440–44.
23 den Heijer T, Vermeer SE, Clarke R, et al.Homocysteine and brain atrophy on MRI of non-demented elderly. Brain 2003; 126: 170–75.
24 Snowdon DA, Greiner LH, Mortimer JA, Riley KP,Greiner PA, Markesbery WR. Brain infarction andthe clinical expression of Alzheimer disease: TheNun Study. JAMA 1997; 277: 813–17.
25 Ho PI, Ortiz , Rogers E, Shea TB. Multiple aspects ofhomocysteine neurotoxicity: glutamateexcitotoxicity, kinase hyperactivation and DNAdamage. J Neurosci Res 2002; 70: 694–702.
26 Kruman, II, Kumaravel TS, Lohani A, et al. Folicacid deficiency and homocysteine impair DNArepair in hippocampal neurons and sensitize themto amyloid toxicity in experimental models ofAlzheimer’s disease. J Neurosci 2002; 22: 1752–62.
27 Mattson MP, Shea TB. Folate and homocysteinemetabolism in neural plasticity andneurodegenerative disorders. Trends Neurosci 2003;26: 137–46.
28 McCaddon A, Hudson P, Hill D, et al. Alzheimer’sdisease and total plasma aminothiols. Biol Psychiatry2003; 53: 254–60.
29 McCaddon A, Regland B, Hudson P, Davies G.Functional vitamin B(12) deficiency and Alzheimerdisease. Neurology 2002; 58: 1395–99.
30 Han YH, Kato Y, Kusuhara H, et al. Kinetic profileof overall elimination of 5-methyltetrahydropteroyl-glutamate in rats. Am J Physiol 1999; 276: E580–87.
31 Nagy ZS, Smith MZ, Esiri MM, Barnetson L, SmithAD. Hyperhomocysteinaemia in Alzheimer’s diseaseand expression of cell cycle markers in the brain.J Neurol Neurosurg Psychiatry 2000; 69: 565–66.
32 Passeri M, Cucinotta D, Abate G, et al. Oral 5’-methyltetrahydrofolic acid in senile organic mentaldisorders with depression: results of a double-blindmulticenter study. Aging (Milano) 1993; 5: 63–71.
33 Shea TB, Rogers E. Homocysteine and dementia. N Engl J Med 2002; 346: 2007.