Embed Size (px)
Citation preview

Journal of Critical Care (2012) 27, 681–687
Homeward bound: An analysis of patients discharged homefrom an oncologic intensive care unit☆,☆☆
Sanjay Chawla MDa,⁎, Rhonda L. D'Agostino ACNP-BC a, Stephen M. Pastores MDa,Raghukumar Thirumala MDa, Natalie Kostelecky RNa, Joanne F. Chou MPHb,Howard T. Thaler PhDb, Neil A. Halpern MDa
aCritical Care Medicine Service, Department of Anesthesiology and Critical Care Medicine, Memorial Sloan-KetteringCancer Center, New York, NYbDepartment of Epidemiology and Biostatistics, Memorial Sloan-Kettering Cancer Center, New York, NY
M
a
0h
Keywords:Discharge;Intensive care;Critical care;Home;Occupancy;Outcomes;Cancer
AbstractPurpose: The objectives of our studywere to evaluate the characteristics and outcomes of patients dischargedhome directly from an oncologic intensive care unit (ICU) and their 30-day hospital readmission patterns.Materials and Methods: We retrospectively reviewed ICU discharges over 3 years (2008-2010) andidentified patients who were discharged directly home. Demographic, clinical, ICU discharge, and 30-dayhospital readmission and mortality rates were analyzed.Results: Ninety-five patients (3.6%) were discharged home directly from the ICU (average annual rate of3.9%). ICU diagnoses primarily included respiratory insufficiency, sepsis, cardiac syndromes, andgastrointestinal bleeding. Home discharge occurred most commonly between Thursday and Saturday.Five (5.3%) patients, including 2 hospice patients, died within 30 days of ICU home discharge. Thirty(31.6%) patients were readmitted within 30 days of discharge. The unplanned 30-day readmission rate was23.2% (22/95) with a median time to hospital readmission of 13 (8-18) days. Most (64%) of the unplannedreadmissions were related to the initial ICU admission.Conclusions: Home discharge of ICU patients at our institution is infrequent but consistent. Almost onethird of these patients were readmitted to the hospital within 30 days. Enhancements to the ICU homedischarge process may be required to ensure optimal post-ICU care.© 2012 Elsevier Inc. All rights reserved.
☆ Financial Support: Department of Anesthesiology and Critical Careedicine.☆☆ No financial or other potential conflicts of interest exist for all listed
uthors.⁎ Corresponding author. Tel.: +1 212 639 6673; fax: +1 212 794 4333.E-mail address: [email protected] (S. Chawla).
883-9441/$ – see front matter © 2012 Elsevier Inc. All rights reserved.ttp://dx.doi.org/10.1016/j.jcrc.2012.05.009
1. Introduction
Caring for critically ill patients is costly, and hospitalsexpect maximal, yet optimal, utilization of their intensivecare units (ICU) [1,2]. Efficient hospital and ICU throughputdepends upon the expeditious admission and discharge ofICU patients [3]. However, when hospital occupancy is near

682 S. Chawla et al.
capacity, prompt discharge of ICU patients to ward beds maybe restricted. The resultant delays in ICU discharge not onlyartificially increase ICU occupancy rates, length of stay(LOS), and costs [4,5] but may also impede the admission ofnew ICU patients, potentially compromising their care [6,7].Professional society guidelines for ICU discharge werewritten well over a decade ago and do not address the distinctissues involved with ICU-to-home discharges [8]. Inaddition, it is not clear whether ICU-to-home dischargesare even appropriate given the national goal of avoidinghospital readmissions within 30 days, an outcome of caremeasure by the Centers for Medicare and Medicaid Servicesand patient safety organizations [9].
To our knowledge, beyond brief reports of direct ICU-to-home discharges for home hospice [10,11] or after drugoverdoses [12], and unpublished data from the AcutePhysiology and Chronic Health Evaluation (APACHE) IVdataset (Cerner Corporation, Kansas City, MO), there are nolong-term, descriptive studies that address patterns in homedischarges from adult ICUs in the United States. Theobjectives of this study were to evaluate the characteristicsand outcomes of patients who were discharged directly homefrom our ICU and to determine the rate, type (planned orunplanned) and causes of hospital readmission of thesepatients within 30 days.
2. Materials and methods
2.1. Data source and study setting
Using hospital and ICU databases, we identified andretrospectively analyzed all adult (N18 years of age) patientswho were discharged home from the 20-bed closed medical/surgical ICU at Memorial Sloan-Kettering Cancer Centerbetween January 1, 2008, and December 31, 2010. Thehospital is a 470-bed academic, tertiary-care referral cancercenter in New York City.
Our ICU is staffed with full time intensivists, pulmonaryand critical care fellows, and acute care nurse practitioners aswell as rotating anesthesiology house staff. All ICUadmissions, discharges, and rejections must be approvedby the critical care medicine attending of record, incollaboration with the primary admitting service attending.Intensive care unit bed capacity remained unchanged duringthe study period. However, hospital bed capacity increasedfrom 434 to 470 beds coincident with the opening of asurgical step-down/ventilator dependent unit (6-8 beds) inJanuary 2010.
2.2. Study population
The following demographic and clinical data werecollected on all study patients: age, gender, source of ICUadmission (Urgent Care Center [UCC], ward, post-anesthe-sia care unit (PACU)/operating room [OR], and other areas);
admitting hospital service (medical or surgical); cancerclassification (thoracic, gastrointestinal [GI], genitourinary[GU], head and neck, hematological, hematopoietic stem celltransplantation [HSCT], miscellaneous and no activecancer); primary critical care diagnosis; arterial lactatelevel and the Mortality Probability Model score on ICUadmission, version 2 (MPM0II) [13]; use of mechanicalventilation or vasopressors at any time during the ICU stay;need for isolation; Do Not Resuscitate (DNR) status onadmission and during ICU stay; and pre-ICU, ICU, and totalhospital LOS and hospital readmission and mortality rateswithin 30 days of ICU discharge.
We identified the date and day of week that ICUdischarge (home or ward) was planned and the date andday of week that ICU discharge home was actualized.Planned transfer or discharge was identified by reviewingthe critical care medicine attending notes for the firstdocumentation of intent to transfer or discharge. We alsoobtained the number of ICU and hospital discharges,inpatient days, average LOS and occupancy for each studyyear. Average hospital and ICU occupancy rates (obtainedfrom the inpatient midnight census/functioning beds thatday) were determined for each day of the week during eachof the study years.
We assessed the number of medications prescribed, themedical status at the time of home discharge (relativelyhealthy or hospice care), special follow-up home-care re-quirements (hospice care, visiting nurse, wound care,supplemental oxygen, or physical or occupational therapy),and whether post-home discharge clinic visits were sched-uled including the number of visits and number of days tothe first visit.
The charts of patients who were readmitted to our hospitalwithin 30 days of ICU discharge to home were evaluated.Two of the investigators (SC, NK) independently reviewedthe medical records to determine whether the cause of the 30-day hospital readmission was planned (scheduled surgicalprocedures or chemotherapy) or unplanned. In addition, ifthe readmission was unplanned, we determined if it waseither related (ie, if there was clinical progression orrecurrence of the ICU primary diagnosis) or unrelated (ie,development of a separate clinical condition distinct from theICU primary diagnosis) to the prior hospitalization and ICUadmission [14-16]. If a consensus was not achieved in thesedeterminations, then authors SC, RD, SP, NK, and NHreviewed both hospitalizations and a decision was reached byabsolute majority. The study was granted a limited waiver(Waiver #0093-09) of authorization and approved by ourinstitutional review board.
2.3. Statistical analysis
Data are presented as means ±SD, median (interquartilerange), absolute numbers, and percentages. Fisher's exacttest and the Wilcoxon rank sum test were used to examinecovariate differences between groups. SAS 9.2 (SAS
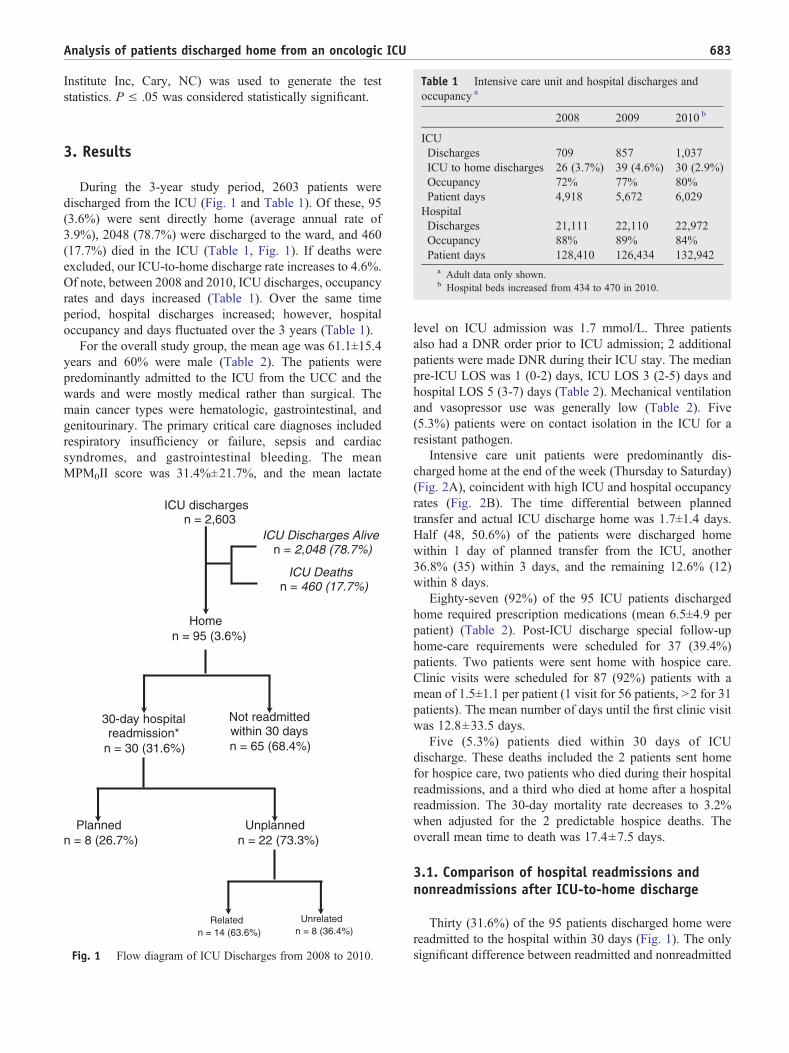
Table 1 Intensive care unit and hospital discharges andoccupancy a
683Analysis of patients discharged home from an oncologic ICU
Institute Inc, Cary, NC) was used to generate the teststatistics. P ≤ .05 was considered statistically significant.
2008 2009 2010 b
ICUDischarges 709 857 1,037ICU to home discharges 26 (3.7%) 39 (4.6%) 30 (2.9%)Occupancy 72% 77% 80%Patient days 4,918 5,672 6,029HospitalDischarges 21,111 22,110 22,972Occupancy 88% 89% 84%Patient days 128,410 126,434 132,942
a Adult data only shown.b Hospital beds increased from 434 to 470 in 2010.
3. Results
During the 3-year study period, 2603 patients weredischarged from the ICU (Fig. 1 and Table 1). Of these, 95(3.6%) were sent directly home (average annual rate of3.9%), 2048 (78.7%) were discharged to the ward, and 460(17.7%) died in the ICU (Table 1, Fig. 1). If deaths wereexcluded, our ICU-to-home discharge rate increases to 4.6%.Of note, between 2008 and 2010, ICU discharges, occupancyrates and days increased (Table 1). Over the same timeperiod, hospital discharges increased; however, hospitaloccupancy and days fluctuated over the 3 years (Table 1).
For the overall study group, the mean age was 61.1±15.4years and 60% were male (Table 2). The patients werepredominantly admitted to the ICU from the UCC and thewards and were mostly medical rather than surgical. Themain cancer types were hematologic, gastrointestinal, andgenitourinary. The primary critical care diagnoses includedrespiratory insufficiency or failure, sepsis and cardiacsyndromes, and gastrointestinal bleeding. The meanMPM0II score was 31.4%±21.7%, and the mean lactate
ICU dischargesn = 2,603
ICU Discharges Aliven = 2,048 (78.7%)
Homen = 95 (3.6%)
30-day hospital readmission*
n = 30 (31.6%)
Plannedn = 8 (26.7%)
Unplannedn = 22 (73.3%)
ICU Deaths n = 460 (17.7%)
Not readmitted within 30 days n = 65 (68.4%)
Relatedn = 14 (63.6%)
Unrelatedn = 8 (36.4%)
Fig. 1 Flow diagram of ICU Discharges from 2008 to 2010.
level on ICU admission was 1.7 mmol/L. Three patientsalso had a DNR order prior to ICU admission; 2 additionalpatients were made DNR during their ICU stay. The medianpre-ICU LOS was 1 (0-2) days, ICU LOS 3 (2-5) days andhospital LOS 5 (3-7) days (Table 2). Mechanical ventilationand vasopressor use was generally low (Table 2). Five(5.3%) patients were on contact isolation in the ICU for aresistant pathogen.
Intensive care unit patients were predominantly dis-charged home at the end of the week (Thursday to Saturday)(Fig. 2A), coincident with high ICU and hospital occupancyrates (Fig. 2B). The time differential between plannedtransfer and actual ICU discharge home was 1.7±1.4 days.Half (48, 50.6%) of the patients were discharged homewithin 1 day of planned transfer from the ICU, another36.8% (35) within 3 days, and the remaining 12.6% (12)within 8 days.
Eighty-seven (92%) of the 95 ICU patients dischargedhome required prescription medications (mean 6.5±4.9 perpatient) (Table 2). Post-ICU discharge special follow-uphome-care requirements were scheduled for 37 (39.4%)patients. Two patients were sent home with hospice care.Clinic visits were scheduled for 87 (92%) patients with amean of 1.5±1.1 per patient (1 visit for 56 patients, N2 for 31patients). The mean number of days until the first clinic visitwas 12.8±33.5 days.
Five (5.3%) patients died within 30 days of ICUdischarge. These deaths included the 2 patients sent homefor hospice care, two patients who died during their hospitalreadmissions, and a third who died at home after a hospitalreadmission. The 30-day mortality rate decreases to 3.2%when adjusted for the 2 predictable hospice deaths. Theoverall mean time to death was 17.4±7.5 days.
3.1. Comparison of hospital readmissions andnonreadmissions after ICU-to-home discharge
Thirty (31.6%) of the 95 patients discharged home werereadmitted to the hospital within 30 days (Fig. 1). The onlysignificant difference between readmitted and nonreadmitted
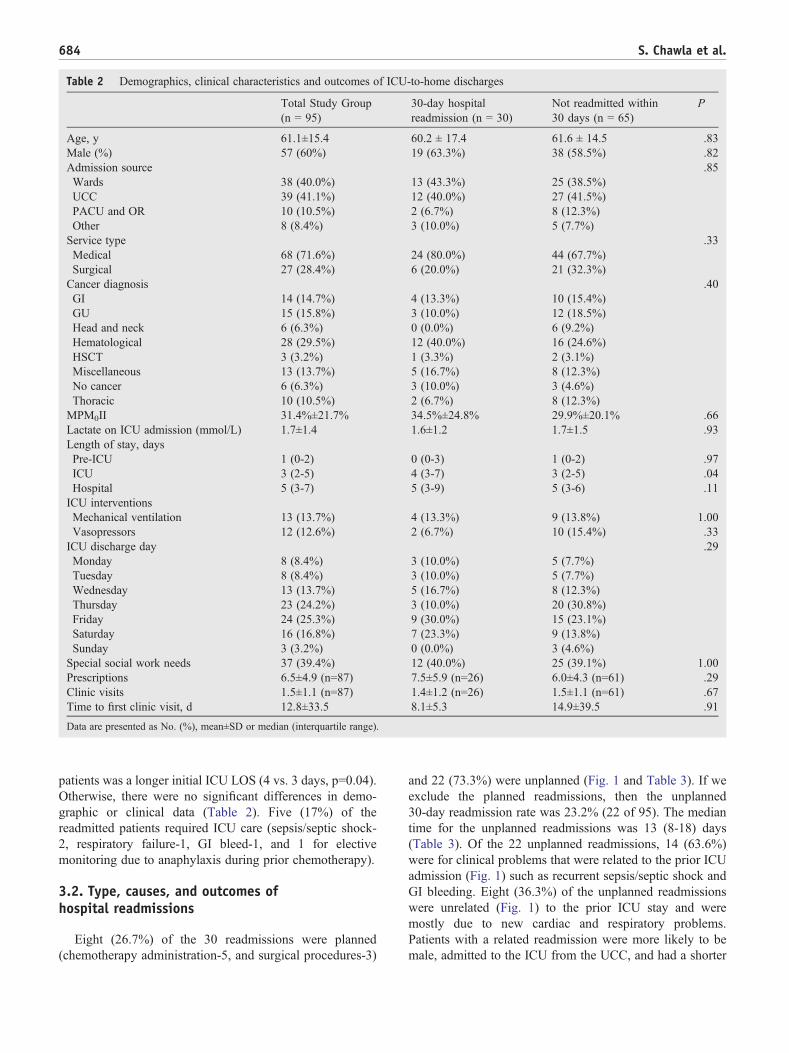
Table 2 Demographics, clinical characteristics and outcomes of ICU-to-home discharges
Total Study Group(n = 95)
30-day hospitalreadmission (n = 30)
Not readmitted within30 days (n = 65)
P
Age, y 61.1±15.4 60.2 ± 17.4 61.6 ± 14.5 .83Male (%) 57 (60%) 19 (63.3%) 38 (58.5%) .82Admission source .85Wards 38 (40.0%) 13 (43.3%) 25 (38.5%)UCC 39 (41.1%) 12 (40.0%) 27 (41.5%)PACU and OR 10 (10.5%) 2 (6.7%) 8 (12.3%)Other 8 (8.4%) 3 (10.0%) 5 (7.7%)Service type .33Medical 68 (71.6%) 24 (80.0%) 44 (67.7%)Surgical 27 (28.4%) 6 (20.0%) 21 (32.3%)Cancer diagnosis .40GI 14 (14.7%) 4 (13.3%) 10 (15.4%)GU 15 (15.8%) 3 (10.0%) 12 (18.5%)Head and neck 6 (6.3%) 0 (0.0%) 6 (9.2%)Hematological 28 (29.5%) 12 (40.0%) 16 (24.6%)HSCT 3 (3.2%) 1 (3.3%) 2 (3.1%)Miscellaneous 13 (13.7%) 5 (16.7%) 8 (12.3%)No cancer 6 (6.3%) 3 (10.0%) 3 (4.6%)Thoracic 10 (10.5%) 2 (6.7%) 8 (12.3%)MPM0II 31.4%±21.7% 34.5%±24.8% 29.9%±20.1% .66Lactate on ICU admission (mmol/L) 1.7±1.4 1.6±1.2 1.7±1.5 .93Length of stay, daysPre-ICU 1 (0-2) 0 (0-3) 1 (0-2) .97ICU 3 (2-5) 4 (3-7) 3 (2-5) .04Hospital 5 (3-7) 5 (3-9) 5 (3-6) .11ICU interventionsMechanical ventilation 13 (13.7%) 4 (13.3%) 9 (13.8%) 1.00Vasopressors 12 (12.6%) 2 (6.7%) 10 (15.4%) .33ICU discharge day .29Monday 8 (8.4%) 3 (10.0%) 5 (7.7%)Tuesday 8 (8.4%) 3 (10.0%) 5 (7.7%)Wednesday 13 (13.7%) 5 (16.7%) 8 (12.3%)Thursday 23 (24.2%) 3 (10.0%) 20 (30.8%)Friday 24 (25.3%) 9 (30.0%) 15 (23.1%)Saturday 16 (16.8%) 7 (23.3%) 9 (13.8%)Sunday 3 (3.2%) 0 (0.0%) 3 (4.6%)Special social work needs 37 (39.4%) 12 (40.0%) 25 (39.1%) 1.00Prescriptions 6.5±4.9 (n=87) 7.5±5.9 (n=26) 6.0±4.3 (n=61) .29Clinic visits 1.5±1.1 (n=87) 1.4±1.2 (n=26) 1.5±1.1 (n=61) .67Time to first clinic visit, d 12.8±33.5 8.1±5.3 14.9±39.5 .91
Data are presented as No. (%), mean±SD or median (interquartile range).
684 S. Chawla et al.
patients was a longer initial ICU LOS (4 vs. 3 days, p=0.04).Otherwise, there were no significant differences in demo-graphic or clinical data (Table 2). Five (17%) of thereadmitted patients required ICU care (sepsis/septic shock-2, respiratory failure-1, GI bleed-1, and 1 for electivemonitoring due to anaphylaxis during prior chemotherapy).
3.2. Type, causes, and outcomes ofhospital readmissions
Eight (26.7%) of the 30 readmissions were planned(chemotherapy administration-5, and surgical procedures-3)
and 22 (73.3%) were unplanned (Fig. 1 and Table 3). If weexclude the planned readmissions, then the unplanned30-day readmission rate was 23.2% (22 of 95). The mediantime for the unplanned readmissions was 13 (8-18) days(Table 3). Of the 22 unplanned readmissions, 14 (63.6%)were for clinical problems that were related to the prior ICUadmission (Fig. 1) such as recurrent sepsis/septic shock andGI bleeding. Eight (36.3%) of the unplanned readmissionswere unrelated (Fig. 1) to the prior ICU stay and weremostly due to new cardiac and respiratory problems.Patients with a related readmission were more likely to bemale, admitted to the ICU from the UCC, and had a shorter
A - Discharge by Day of Week
B - ICU & Hospital Occupancy
30%
24%
18%
12%
6%
0%
100%
80%
60%
40%
20%
0%
Per
cent
Dis
char
ged
Monday Tuesday WednesdayThursday Friday Saturday Sunday
Monday Tuesday WednesdayThursday Friday Saturday Sunday
ICU Hospital
Fig. 2 The bulk of the ICU discharges home occurred betweenWednesday and Saturday (A) coincident with the highest ICU andhospital occupancy rates (B).
685Analysis of patients discharged home from an oncologic ICU
ICU and hospital LOS during the index admission(Table 3).
4. Discussion
We report a nearly 4% average annual rate of ICU-to-home discharges between 2008 and 2010. Although our dataare culled from patients in an oncologic ICU, we believe ourfindings are broadly applicable given that approximately15% of patients admitted to US and European ICUs havemalignancies [17,18]. More importantly, our ICU-to-homedischarge rate is comparable to the 4% average rate per yearof ICU-to-home discharge over the identical time periodfrom the APACHE IV data set (Personal communication -Kramer AA. Critical Care Research, Cerner Critical Care,[email protected]) [19]. Our study findings and those ofthe APACHE IV data set highlight that ICU-to-homedischarges has become commonplace and should beacknowledged and addressed.
To date, ICU discharge guidelines [8] and recommenda-tions have been designed to minimize post-ICU dischargeproblems [20-22] for ICU patients transferred to inpatientwards. Specifics of the ICU-to-home discharge process havenever been formally addressed. Our study showed thatICU-to-home discharges were associated with considerableforward planning. This was represented by the over 90% ofpatients who required the ordering of a large number ofmedications and the scheduling of outpatient clinic visits. Inaddition, almost 40% of patients required arrangements forspecial services. Of particular concern was our finding thathome discharges usually occurred at the end of the week.This posed an organizational challenge for us as the home-care requirements had to be coordinated by Friday becausesocial workers and case managers were not routinelyavailable on weekends.
The greatest issue however, for an ICU dischargingtheir patients' home is the finality of the dischargeprocess. Intensive care unit to home discharges precludepost-ICU visits on the wards thus eliminating the innatehospital safety-net for such patients. Similarly, when ICUteams order discharge medications for the ward, they doso with the knowledge that the ward team will addresslong-term and home medication needs. Lastly, ICU-to-home discharges may be particularly concerning in“closed” ICUs such as ours, where the patients' primaryproviders may be less involved in ICU care and dischargeplanning than in open units. Therefore, the ICU team mustdiscuss the home discharge plans with the patients'primary providers to ensure continuity of care outsidethe hospital.
ICUs may be quite hesitant to discharge their patientshome even if seemingly appropriate because a hospitalreadmission within 30-days may trigger a quality review andpunitive actions [23]. Our overall 30-day hospital read-mission rate was rather high at 31.6%. However, theunplanned 30-day readmission rate was much lower at23.2%. A majority (64%) of the unplanned readmissionswere for problems that were related to the primary diagnosesof the prior ICU admission. This finding suggests that theunderlying clinical problems may not have been adequatelyaddressed prior to home discharge.
Our study has several limitations. First, it was beyondour scope in this small retrospective study to determinethe complicated, dynamic, and multifactorial real-timestatistical relationships that address ICU throughput,daily ICU and hospital bed availability, and thedischarge choices for ICU patients [24]. Second, wedid not develop a predictive model to assess which ICUpatients were best suited to be discharged home. Thiswould require a large multicenter study that analyzesICU discharge patterns, patient characteristics, ICU andhospital occupancy rates, and other variables that effectICU throughput [25,26]. Lastly, it was not possible todetermine if hospital readmissions occurred outside ofour healthcare network system.
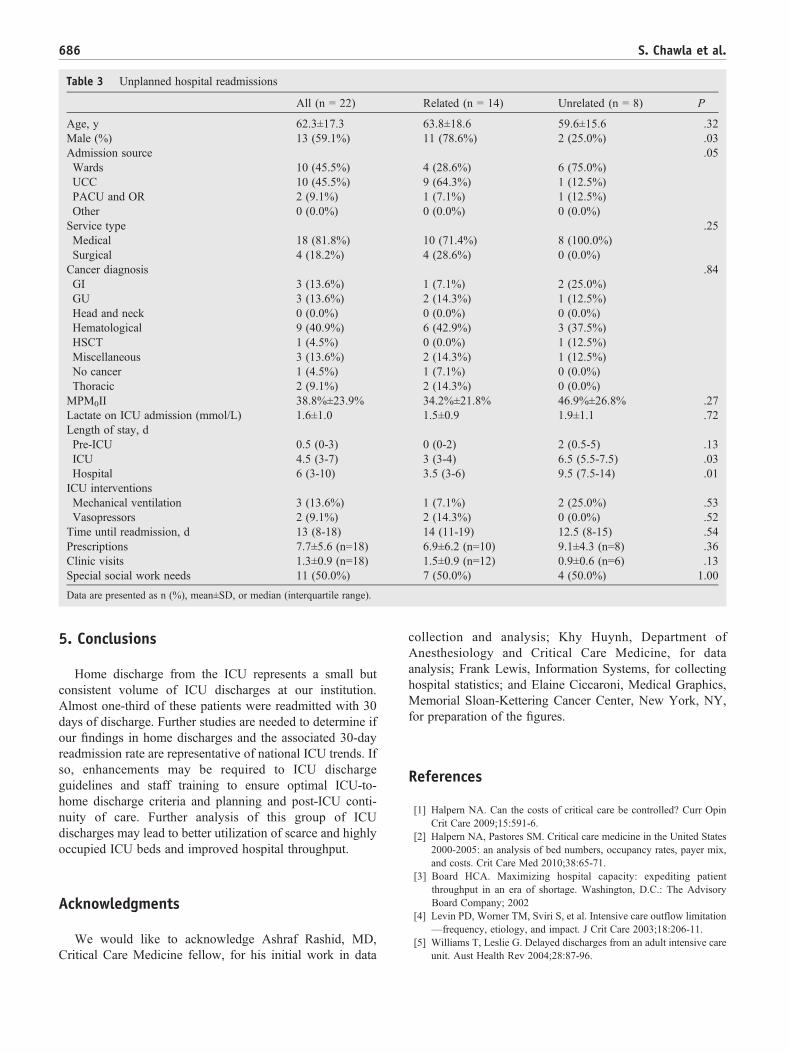
Table 3 Unplanned hospital readmissions
All (n = 22) Related (n = 14) Unrelated (n = 8) P
Age, y 62.3±17.3 63.8±18.6 59.6±15.6 .32Male (%) 13 (59.1%) 11 (78.6%) 2 (25.0%) .03Admission source .05Wards 10 (45.5%) 4 (28.6%) 6 (75.0%)UCC 10 (45.5%) 9 (64.3%) 1 (12.5%)PACU and OR 2 (9.1%) 1 (7.1%) 1 (12.5%)Other 0 (0.0%) 0 (0.0%) 0 (0.0%)Service type .25Medical 18 (81.8%) 10 (71.4%) 8 (100.0%)Surgical 4 (18.2%) 4 (28.6%) 0 (0.0%)Cancer diagnosis .84GI 3 (13.6%) 1 (7.1%) 2 (25.0%)GU 3 (13.6%) 2 (14.3%) 1 (12.5%)Head and neck 0 (0.0%) 0 (0.0%) 0 (0.0%)Hematological 9 (40.9%) 6 (42.9%) 3 (37.5%)HSCT 1 (4.5%) 0 (0.0%) 1 (12.5%)Miscellaneous 3 (13.6%) 2 (14.3%) 1 (12.5%)No cancer 1 (4.5%) 1 (7.1%) 0 (0.0%)Thoracic 2 (9.1%) 2 (14.3%) 0 (0.0%)MPM0II 38.8%±23.9% 34.2%±21.8% 46.9%±26.8% .27Lactate on ICU admission (mmol/L) 1.6±1.0 1.5±0.9 1.9±1.1 .72Length of stay, dPre-ICU 0.5 (0-3) 0 (0-2) 2 (0.5-5) .13ICU 4.5 (3-7) 3 (3-4) 6.5 (5.5-7.5) .03Hospital 6 (3-10) 3.5 (3-6) 9.5 (7.5-14) .01ICU interventionsMechanical ventilation 3 (13.6%) 1 (7.1%) 2 (25.0%) .53Vasopressors 2 (9.1%) 2 (14.3%) 0 (0.0%) .52Time until readmission, d 13 (8-18) 14 (11-19) 12.5 (8-15) .54Prescriptions 7.7±5.6 (n=18) 6.9±6.2 (n=10) 9.1±4.3 (n=8) .36Clinic visits 1.3±0.9 (n=18) 1.5±0.9 (n=12) 0.9±0.6 (n=6) .13Special social work needs 11 (50.0%) 7 (50.0%) 4 (50.0%) 1.00
Data are presented as n (%), mean±SD, or median (interquartile range).
686 S. Chawla et al.
5. Conclusions
Home discharge from the ICU represents a small butconsistent volume of ICU discharges at our institution.Almost one-third of these patients were readmitted with 30days of discharge. Further studies are needed to determine ifour findings in home discharges and the associated 30-dayreadmission rate are representative of national ICU trends. Ifso, enhancements may be required to ICU dischargeguidelines and staff training to ensure optimal ICU-to-home discharge criteria and planning and post-ICU conti-nuity of care. Further analysis of this group of ICUdischarges may lead to better utilization of scarce and highlyoccupied ICU beds and improved hospital throughput.
Acknowledgments
We would like to acknowledge Ashraf Rashid, MD,Critical Care Medicine fellow, for his initial work in data
collection and analysis; Khy Huynh, Department ofAnesthesiology and Critical Care Medicine, for dataanalysis; Frank Lewis, Information Systems, for collectinghospital statistics; and Elaine Ciccaroni, Medical Graphics,Memorial Sloan-Kettering Cancer Center, New York, NY,for preparation of the figures.
References
[1] Halpern NA. Can the costs of critical care be controlled? Curr OpinCrit Care 2009;15:591-6.
[2] Halpern NA, Pastores SM. Critical care medicine in the United States2000-2005: an analysis of bed numbers, occupancy rates, payer mix,and costs. Crit Care Med 2010;38:65-71.
[3] Board HCA. Maximizing hospital capacity: expediting patientthroughput in an era of shortage. Washington, D.C.: The AdvisoryBoard Company; 2002
[4] Levin PD, Worner TM, Sviri S, et al. Intensive care outflow limitation—frequency, etiology, and impact. J Crit Care 2003;18:206-11.
[5] Williams T, Leslie G. Delayed discharges from an adult intensive careunit. Aust Health Rev 2004;28:87-96.

687Analysis of patients discharged home from an oncologic ICU
[6] Cline SD, Schertz RA, Feucht EC. Expedited admission of patientsdecreases duration of mechanical ventilation and shortens ICU stay.Am J Emerg Med 2009;27:843-6.
[7] Young MP, Gooder VJ, McBride K, et al. Inpatient transfers to theintensive care unit: delays are associated with increased mortality andmorbidity. J Gen Intern Med 2003;18:77-83.
[8] Guidelines for intensive care unit admission, discharge, and triage.Task Force of the American College of Critical Care Medicine, Societyof Critical Care Medicine. Crit Care Med 1999;27:633-8.
[9] Jencks SF, Williams MV, Coleman EA. Rehospitalizations amongpatients in the Medicare fee-for-service program. N Engl J Med2009;360:1418-28.
[10] Huang YC, Huang SJ, Ko WJ. Going home to die from surgicalintensive care units. Intensive Care Med 2009;35:810-5.
[11] Ryder-Lewis M. Going home from ICU to die: a celebration of life.Nurs Crit Care 2005;10:116-21.
[12] Heyman EN, LoCastro DE, Gouse LH, et al. Intentional drugoverdose: predictors of clinical course in the intensive care unit.Heart Lung 1996;25:246-52.
[13] Lemeshow S, Teres D, Klar J, et al. Mortality Probability Models(MPM II) based on an international cohort of intensive care unitpatients. JAMA 1993;270:2478-86.
[14] Chawla S, Pastores SM, Hassan K, et al. ICU admissions after actual orplanned hospital discharge: incidence, clinical characteristics, andoutcomes in cancer patients. Chest 2009;136:1257-62.
[15] Chen LM, Martin CM, Keenan SP, et al. Patients readmitted to theintensive care unit during the same hospitalization: clinical featuresand outcomes. Crit Care Med 1998;26:1834-41.
[16] Rosenberg AL, Watts C. Patients readmitted to ICUs*: a systematicreview of risk factors and outcomes. Chest 2000;118:492-502.
[17] Zimmerman JE, Kramer AA, McNair DS, et al. Acute Physiology andChronic Health Evaluation (APACHE) IV: hospital mortalityassessment for today's critically ill patients. Crit Care Med 2006;34:1297-310.
[18] Taccone FS, Artigas AA, Sprung CL, et al. Characteristics andoutcomes of cancer patients in European ICUs. Crit Care 2009;13:R15.
[19] Kramer AA, Higgins TL, Zimmerman JE. Intensive care unitreadmissions in U.S. hospitals: patient characteristics, risk factors,and outcomes. Crit Care Med 2012;40:3-10.
[20] Williams TA, Leslie GD, Elliott N, et al. Introduction of discharge planto reduce adverse events within 72 hours of discharge from the ICU.J Nurs Care Qual 2010;25:73-9.
[21] Prinjha S, Field K, Rowan K. What patients think about ICU follow-upservices: a qualitative study. Crit Care 2009;13:R46.
[22] Chaboyer W, Thalib L, Foster M, et al. Predictors of adverse events inpatients after discharge from the intensive care unit. Am J Crit Care2008;17:255-63 [quiz 264].
[23] Rau J. Medicare rule would decrease payments to hospitals with highre-admission rates: The Washington Post, July 30, 2011. http://www.washingtonpost.com/national/health-science/medicare-rule-would-decrease-payments-to-hospitals-with-high-re-admission-rates/2011/07/28/gIQAYwDpjI_story.html.
[24] Halpern SD. ICU capacity strain and the quality and allocation ofcritical care. Curr Opin Crit Care 2011;17:648-57.
[25] Hansen LO, Young RS, Hinami K, et al. Interventions to reduce30-day rehospitalization: a systematic review. Ann Intern Med 2011;155:520-8.
[26] Allaudeen N, Schnipper JL, Orav EJ, et al. Inability of providers topredict unplanned readmissions. J Gen Intern Med 2011;26:771-6.