Embed Size (px)
Citation preview

HYPERTHYROIDISM
The Dietary Supplement Tiratricol (3,3,5′-Triiodothy-roacetic Acid) Can Cause Symptoms ofHyperthyroidism ..................................................................41
The Serum Free Triiodothyronine to Free ThyroxineRatio and the Peripheral Blood Eosinophil to MonocyteRatio Help to Distinguish between Graves’ Disease andThyroiditis as a Cause of Thyrotoxicosis ........................42
GRAVES’ DISEASE
Concordance of Graves’ Disease Is Greater in Monozy-gotic than Dizygotic Twins ................................................43
Shedding of Part of the Thyrotropin Receptor May BeImportant in the Pathogenesis of Hyperthyroidism inGraves’ Disease ....................................................................44
Neonatal Hyperthyroidism Occurs Only in InfantsWhose Mothers Have Very High Serum Thyrotropin Receptor-Stimulating Antibody Concentrations ............45
GRAVES’ OPHTHALMOPATHY
Patients with Graves’ Ophthalmopathy May Have Long-Term Impairment in Vision and Quality of Life............46
HYPOTHYROIDISM
Germline Loss-of-Function Mutations of theThyrotropin-Receptor Gene Are a Cause of SubclinicalHypothyroidism ....................................................................47
Progression from Subclinical to Overt HypothyroidismIs Most Likely in Women with Higher Serum TSHConcentrations and High Serum Antithyroid AntibodyTiters ......................................................................................48
Serum Concentrations of Multiple Enzymes May BeHigh in Patients with Hypothyroidism ............................49
Thyroxine Inhibits Thyrotropin Secretion in Patientswith Central Hypothyroidism ............................................50
NODULAR GOITER
Thyroxine Therapy Does Not Reduce the Size of BenignSolitary Thyroid Nodules: Systematic Analysis ofMultiple Studies ....................................................................51
THYROID CANCER
Completion Thyroidectomy Can Be Done Safely afterThyroid Lobectomy in Patients with ThyroidCarcinoma..............................................................................52
Changes in Surgical Practice and Use of PostoperativeRadioiodine Therapy Have Had Limited Effect on Out-come in Patients with Papillary Thyroid Carcinoma ......53
Fertility Is Not Impaired after Radioiodine Therapy inMen with Thyroid Carcinoma ............................................54
High Serum Antithyroglobulin Concentrations afterInitial Therapy Are Associated with Recurrence inPatients with Thyroid Carcinoma ......................................55
THYROID FUNCTION IN PREGNANCY
Some Women with Hyperemesis Gravidarum HaveTransient Hyperthyroidism ................................................56
CONGENITAL HYPOTHYROIDISM
Discordance of Thyroid Dysgenesis in MonozygoticTwins ......................................................................................57
NONTHYROIDAL ILLNESS
Thyroid Abnormalities in Recipients of Bone MarrowTransplants Are Usually Associated with Chronic Graft-versus-Host Disease ............................................................58
3,5-Diiodothyropropionic Acid Has Favorable Short-Term Effects on Cardiac Hemodynamics in Patients withCongestive Heart Failure ....................................................59
IODINE METABOLISM
Recurrence of Mild Iodine Deficiency in Tasmania ......60
VOLUME XIV ● ISSUE 3 NOVEMBER 2002
CLINICALTHYROIDOLOGY
A publication of the American Thyroid Association

CLINICALTHYROIDOLOGYVOLUME XIV ● ISSUE 3 NOVEMBER 2002
Editor-in-ChiefRobert D. Utiger, M.D.Thyroid DivisionDepartment of MedicineBrigham & Women’s Hospital 77 Avenue Louis Pasteur Boston, MA 02115(617) 525-5171 Telephone (617) 731-4718 Fax [email protected]
PresidentCarole A. Spencer, Ph.D.
Secretary Paul W. Ladenson, M.D.
President Elect Peter A. Singer, M.D.
Treasurer David S. Cooper, M.D.
Publications Committee ChairMartin I. Surks, M.D.
Director of Public AffairsEdie Stern
Executive DirectorBarbara R. Smith, C.A.E.American Thyroid Association6066 Leesburg Pike, Suite 650Falls Church, VA 22041Telephone: 703-998-8890Fax: 703-998-8893Email: [email protected]
Designed BySaratoga Graphics7 Kaatskill WayBallston Spa, NY 12020Telephone: (518) 583-0243Kandra L. Files, Art DirectorEmail: [email protected]
Clinical ThyroidologyCopyright © 2002American Thyroid Association, Inc.Printed in the USA. All rights reserved.
Clinical Thyroidology is now availableon the ATA web site (www.thyroid.org).
ATA News
Future Meetings
75th Annual MeetingSeptember 16 to 21, 2003The BreakersPalm Beach, FL
76th Annual MeetingSeptember 29 to October 3, 2004Westin Bayshore Resort and MarinaVancouver, British Columbia, Canada
13th International Thyroid CongressOctober 30 to November 4, 2005Buenos Aires, Argentina

SUMMARY
Background Tiratricol (3,5,3′-triiodothyroacetic acid, ortriac) is a metabolite of thyroxine (T4) that has some intrin-sic thyromimetic activity. It is marketed in health food storesand on the Internet as a substance that accelerates metab-olism and burns fat. This paper describes a patient in whomtiratricol caused symptoms of hyperthyroidism.
Case Report The patient was an 87-year-old woman whowas referred to the Mayo Clinic in May 2001. Four monthsearlier she was told by a chiropractor that she had a mildanemia, and she had been advised to take multiple dietarysupplements (Osteo-Genics, Hemagenics, Serenagen, BioPure Protein, Acida-Zyme, Therazyme, Ginkgo biloba, multi-vitamins, and tiratricol). The dose of tiratricol was three1000-µg tablets daily. Two months later, she noted the onsetof persistent nervousness, insomnia, tremor, fatigue, andweight loss. Physical examination, including examination ofthe thyroid, was normal. Her serum thyrotropin (TSH) con-
centration was 0.015 mU/L (normal, 0.3 to 5.0), her serumfree T4 concentration was low (0.6 ng/dL [7.7 pmol/L]),and her serum triiodothyronine (T3) concentration was high(293 ng/dL [4.5 nmol/L]). Tiratricol was not tested, but3,5,3′-triiodothyropropionic acid had 33 percent cross-reac-tivity in the serum T3 assay. (Six months earlier her serumTSH concentration had been 2.9 mU/L and her serum totalT4 concentration 6.2 µg/dL ([80 nmol/L]).
The patient was advised to stop taking all the dietary sup-plements. Her symptoms disappeared, and four weeks laterher serum TSH concentration was 5.9 mU/L and her serumfree T4 and T3 concentrations were normal. She thenresumed taking all the supplements except tiratricol. Hersymptoms did not recur, and six weeks later the tests of thy-roid function were normal.
Conclusion Tiratricol is a thyroid hormone analogue thatcan be purchased as a dietary supplement and can causesymptoms of hyperthyroidism.
HYPERTHYROIDISM
The dietary supplement tiratricol (3,5,3′-triiodothyroacetic acid) can causesymptoms of hyperthyroidism
Bauer BA, Elkin PL, Erickson D, Klee GG, Brennan MD. Symptomatic hyperthyroidism in a patient taking the dietarysupplement tiratricol. Mayo Clin Proc 2002;77:587-90.
CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3 ● 41
COMMENTARY
There is a long list of natural prod-ucts euphemistically called dietary ornutritional supplements that affect thy-roid hormone production or action, andthat therefore can cause hypothyroidismor hyperthyroidism. One group of prod-ucts are those that contain large amountsof iodine, such as kelp, that can increaseor decrease thyroid hormone productionin patients with different thyroid disor-ders. A second consists of products richin tyrosine. These are marketed on thegrounds that tyrosine is an essential sub-strate for thyroid hormone production,and therefore an increase in tyrosineintake will increase thyroid hormone pro-duction. This is a classic half-truth; tyro-sine is of course needed for thyroid hor-mone production, but there is no evi-dence that feeding tyrosine increases thy-roid hormone production in anybody. Athird consists of crude thyroid extractsand purified T4 analogs such as tiratricol.These substances are marketed not onlyas dietary or nutritional supplements, butalso as fat burners. They have thy-romimetic actions, and therefore can
cause hyperthyroidism, if taken in suffi-cient quantities (1), but they can hardlybe called dietary or nutritional supple-ments, and there is no evidence that theystimulate fat catabolism, as they areadvertised to do.
Tiratricol binds well to thyroid hor-mone receptors in vitro, but has about 5to 10 percent of the calorigenic activityof T3 in vivo. In studies in patients withthyroid carcinoma and severe hypothy-roidism, the mean doses of T4 and tira-tricol needed to reduce serum TSH con-centrations to just below 0.1 mU/L were2.2 µg/kg/day and 48 µg/kg/day (ratio,1:22), respectively (2). As compared withT4, tiratricol had similar effects on a thy-rotoxicosis symptom score, body weight,resting metabolic rate, fat oxidation, andurinary nitrogen excretion, but it had rel-atively greater effects on the liver andskeleton (2). The patients given tiratricolhad undetectable serum free T4 concen-trations.
Tiratricol is undeniably a naturalproduct, but to call it a dietary or nutri-tional supplement is surely a misnomer.The FDA has banned several tiratricolproducts, but as of November 4, 2002,
it remains available at at least one Website (www.muscleshop.net/TriCuts.htm).There, ninety 1000-µg tablets of tiratricolcan be purchased for $79.99. The sug-gested dose is 3000 µg daily. This isenough to provide a 62.5-kg person withthe 48 µg/kg/day needed to cause atleast mild hyperthyroidism. There is noreason to think that tiratricol has uniqueproperties as a “fat burner”; it is justanother way of selling thyroid hormoneand at the same time evading regulationby the Food and Drug Administration.
Robert D. Utiger, M.D.
References
1. Eliason BC, Doenier JA, NuhlicekDN. Desiccated thyroid in a nutritionalsupplement. J Fam Pract 1994;38:287-8.
2. Sherman SI, Ringel MD, Smith MJ, etal. Augmented hepatic and skeletal thy-romimetic effects of tiratricol in compar-ison with levothyroxine. J Clin Endo-crinol Metab 1997;82:2153-8.

SUMMARY
Background Differentiating between thyrotoxicosiscaused by silent (painless) thyroiditis and Graves’ disease isimportant, because the natural history and treatment of thetwo disorders differ. They can be differentiated on the basisof measurements of thyroid radioiodine uptake and thy-rotropin (TSH)-receptor antibodies in serum, but simplertests are needed. This study evaluated the efficacy of meas-urements of the molar ratio of free triiodothyronine (T3) tofree thyroxine (T4) in serum and the ratio of peripheralblood eosinophils to monocytes to differentiate betweensilent thyroiditis and also subacute thyroiditis and Graves’disease as causes of thyrotoxicosis.
Methods The study subjects were 111 patients with thyro-toxicosis. They included 69 patients (52 women, 17 men;mean [±SD] age, 37±13 years) with Graves’ disease, 21patients (17 women, 4 men; mean age, 41±14 years) withpainless thyroiditis, and 21 patients (17 women, 4 men;mean age, 48±7 years) with subacute (painful) thyroiditis.All the patients had high serum free T3 and free T4 concen-trations. The diagnosis of Graves’ disease was based on apositive test for TSH receptor antibodies or a high thyroidradioiodine uptake. Painless thyroiditis was diagnosed onthe basis of high serum free T3 and free T4 concentrationsfor less than three months, and a low thyroid radioiodineuptake or later development of transient hypothyroidism.Subacute thyroiditis was diagnosed on the basis of neckpain and tenderness, fever, neck swelling, a high serumC-reactive protein or low thyroid radioiodine uptake value,and spontaneous remission of thyroid dysfunction. Serumfree T3 and free T4 were measured by radioimmunoassayand blood eosinophils and monocytes by an automatedmethod before any treatment was given.
Results The mean serum free T3 and free T4 concentra-tions in the patients with Graves’ disease were 1.3±0.6 ng/dL (20±10 pmol/L) and 4.0±1.9 ng/dL (51±25pmol/L), respectively, as compared with 0.8±0.5 ng/dL
(12±8 pmol/L) and 3.0±2.4 ng/dL (39±31 pmol/L,respectively, in the patients with painless thyroiditis. The val-ues in the patients with subacute thyroiditis were similar tothose in the patients with painless thyroiditis. The serumfree T3:free T4 molar ratio was higher in the patients withGraves’ disease (0.40±0.09) than in the patients with eitherpainless thyroiditis (0.30±0.07, P<0.01) or subacute thy-roiditis (0.34±0.06, P<0.01). Among the 28 patients withthyrotoxicosis who had a serum free T3:free T4 molar ratio<0.3, 22 (79 percent) had silent or subacute thyroiditis(Table).
The mean percentage of eosinophils was 3.5 in the patientswith Graves’ disease, as compared with approximately 1.4 inthe patients with silent thyroiditis (P<0.01) and 1.1 in thepatients with subacute thyroiditis (P<0.01). The meaneosinophil:monocyte ratios were 0.8±0.8 in the patientswith Graves’ disease, 0.3±0.2 in the patients with silent thy-roiditis (P<0.01), and 0.2±0.2 in the patients with subacutethyroiditis (P<0.01). Among the 24 patients with thyrotox-icosis who had an eosinophil:monocyte ratio <0.2, 22 (92percent) had silent or subacute thyroiditis (Table).
Conclusion Measurements of the serum free T3:free T4molar ratio and the peripheral blood eosinophil:monocyteratio distinguish between Graves’ disease and silent thy-roiditis or subacute thyroiditis as causes of thyrotoxicosis.
HYPERTHYROIDISM
The serum free triiodothyronine to free thyroxine ratio and the peripheralblood eosinophil to monocyte ratio help to distinguish between Graves’ dis-ease and thyroiditis as a cause of thyrotoxicosis
Izumi Y, Hidaka Y, Tada H, Takano T, Kashiwai T, Tatsumi K, Ichihara K, Amino N. Simple and practical parametersfor differentiation between destruction-induced thyrotoxicosis and Graves’ thyrotoxicosis. Clin Endocrinol 2002;57:51-8.
42 ● CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3
COMMENTARY
Distinguishing between Graves’ dis-ease and silent thyroiditis, whether itoccurs postpartum or unrelated to preg-nancy, as a cause of thyrotoxicosis maybe difficult, and simple blood tests thatdistinguished between the two disorderswould be useful.
The evaluation of eosinophil andmonocyte counts as indicators of the
cause of thyrotoxicosis was based on theassociation between Graves’ disease andhumoral immunity (Th2-cell predomi-nance), which is associated witheosinophilia, and the association betweensilent thyroiditis and subacute thyroiditiswith cellular immunity (Th1-cell predom-inance), which is associated with mono-nuclear cells. It is easy to count thesecells, but the differences in cell countsand the eosinophil:monocyte ratio were
small, and no information about the day-to-day reproducibility of the counts wasprovided. Also, thyroid radioiodineuptake was not measured routinely, sothat the hormone and cell count ratioscannot be compared with the test usedmost widely to distinguish between thesedisorders.
Robert D. Utiger, M.D.
Table. Test Results Distinguishing Thyrotoxicosis Caused by Graves’ Disease andThyrotoxicosis Caused by Painless or Subacute Thyroiditis.
Cutoff Graves’ Thyroiditis Proportion with ProportionValue Disease (n=42) Graves’ with
(n=69) Disease Thyroiditis
Serum free T3: <0.3 6 22 21% 79%free T4 ratio
Eosinophil: >1.0 15 0 100% 0%monocyte ratio <0.2 2 22 8% 92%

SUMMARY
Background There is strong evidence for genetic suscep-tibility to Graves’ disease, based on studies of twins, familyclustering, and gene linkage, but the extent of heritabilityhas varied in different studies. In this study the heritabilityof Graves’ disease was determined in a large cohort ofmonozygotic and dizygotic twins.
Methods The California Twin Program was created as afile of all twins born in the state from 1908 to 1982. Thisfile was linked to the state’s file of people who had activedriver’s licenses in 1991, which yielded 102,000 twins. Aquestionnaire was sent to the 36,244 twins aged 40 years orolder. The twins were asked about their personal character-istics and medical history, including questions about Graves’disease and other thyroid disorders in themselves, their co-twins, and other family members, including spouses. Usablequestionnaires were returned by 19,378 subjects (53 per-cent), representing 13,708 twin pairs. Based on the self-reports of these respondents, 32 percent were monozygot-ic twins (50 percent women, 50 percent men), 37 percentwere like-sex dizygotic twins (17 percent women, 20 percentmen), and 31 percent were unlike-sex dizygotic twin pairs.The mean ages of these five groups ranged from 44 to 50years.
The subjects reporting a diagnosis of Graves’ disease orother thyroid disorder were interviewed by telephone, atwhich time they were asked detailed questions about symp-toms and signs of hyperthyroidism, the basis for diagnosis,treatment, and course, and also the presence of Graves’ophthalmopathy in themselves, their twins, and other fami-ly members. An investigator who was unaware of individual
identity and twin status reviewed each questionnaire andconfirmed the diagnosis of Graves’ disease.
Results On the basis of the initial questionnaire, a diagno-sis of Graves’ disease was suggested in 118 members of 110twin pairs. Information was available from both twins of 62twin pairs, of whom 70 reported Graves’ disease, and onetwin of 48 twin pairs, of whom 35 reported Graves’ diseasein themselves and 13 in their twin.
Among these 118 subjects, 106 (77 women, 29 men) wereconfirmed to have Graves’ disease after the telephone inter-view. Ten of these subjects had no twin at risk, because ofdeath or thyroidectomy. There were 89 twin pairs in whichone or both twins were confirmed to have Graves’ disease.They included 35 pairs of monozygotic twins, among which6 pairs (17 percent) were concordant for Graves’ disease(5 female pairs, 1 male pair), and 54 pairs of dizygotic twins,among which 1 twin pair (2 percent) was concordant forGraves’ disease (1 female, 1 male). The mean age at diagno-sis in the concordant pairs was 33 years (range, 12 to 46),and the mean interval between diagnosis in each member ofa pair was 12 years. In 5 of the 35 monozygotic twin pairs(14 percent) and 1 of the 54 dizygotic twin pairs (2 percent),one twin had Graves’ disease and the other twin had chron-ic autoimmune thyroiditis.
Among the twins with Graves’ disease, none had a spousereported to have Graves’ disease, but 19 of 488 first-degreerelatives (4 percent) did have the disease.
Conclusion Among twins in California, Graves’ diseasewas more common in monozygotic than dizygotic twins,confirming that the disease has a heritable component.
GRAVES’ DISEASE
Concordance of Graves’ disease is greater in monozygotic thandizygotic twins
Ringold DA, Nicoloff JT, Kesler M, Davis H, Hamilton A, Mack T. Further evidence for a strong genetic influence onthe development of autoimmune thyroid disease: the California Twin Study. Thyroid 2002;12:647-53.
CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3 ● 43
COMMENTARY
The results of this study mirrorthose of a 1998 study of twins in Den-mark (pairwise concordance rate, 22 per-cent for monozygotic twins, 0 percentfor dizygotic twins) (1); in earlier studiesthe rates in both types of twins werehigher (reviewed in 1). Some of the vari-ations can be explained by variations inthe ages of the twins when surveyed;accuracy of recall; variations in question-naires; criteria for diagnosis; and extentof documentation of diagnosis. Ofcourse, Graves’ disease is not synony-mous with hyperthyroidism, but it isnearly enough so in common parlancethat asking about Graves’ disease can be
considered asking about hyperthyroidism,and vice-versa, at least in the UnitedStates.
The nature of the genetic suscepti-bility to Graves’ disease revealed by twinand other studies is not known. The dis-ease has been linked to genes that affectthe thyroid and genes that affect immuneregulation. Therefore, the heritable com-ponents of the disease are almost cer-tainly polygenic. The nature of the non-heritable contributions to the disease,whether as risk factors or actual precipi-tating factors, is equally if not more un-certain, and they too are surely multiple.
Robert D. Utiger, M.D.
Reference
1. Brix TH, Kyvik KO, Hegedus L. Whatis the evidence of genetic factors in theetiology of Graves’ disease? A briefreview. Thyroid 1998;8:627-34.

SUMMARY
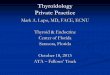
Background The proximate cause of hyperthyroidism inpatients with Graves’ disease is activation of thyrotropin(TSH) receptors on thyroid follicular cells by TSH receptor-stimulating antibodies (TSHR-SAb). These receptors arecomposed of an extracellular amino-terminal domain and atransmembrane and intracellular domain. After insertioninto the cell membrane the extracellular domain can becleaved in two places, forming an A subunit (Figure) and aB subunit, which are joined by disulfide bonds, and theintervening C peptide region is deleted. The binding site(and epitope) for TSHR-SAb and the binding site for TSHoverlap each other at the amino-terminal end of the A sub-unit. The A subunit is shed from the receptor into the extra-cellular fluid. This study was done to determine the reactiv-ity of different forms of the receptor with TSH, TSHR-SAb, and TSH receptor-blocking antibodies (TSHR-BAb).
Methods Intact uncleaved TSH receptors (TSHR cells) orthe extracellular domain of the receptor anchored to the cellmembrane with glycosylphosphatidylinositol (ECD-TSHRcells) were expressed in hamster ovary cells. The cells wereincubated with a monoclonal antibody (3BD10) that reacts
with the amino terminus of the A subunit (amino acidresidues 25-51), a monoclonal antibody (2C11) that reactswith the C peptide region (amino acids 354-359), and serumsamples from 20 patients with Graves’ hyperthyroidismcontaining TSHR-SAb, 7 patients with hypothyroidism con-taining TSHR-BAb, and 9 normal subjects. The cells werethen incubated with fluorescein-labeled antimouse or anti-human immunoglobulin and the extent of binding meas-ured by flow cytometry. The ability of free A subunit toinhibit binding was also tested.
Results The ECD-TSHR cells bound more 3BD10 anti-body than did the TSHR cells, suggesting that the epitopefor the 3BD10 antibody was more exposed in the ECD-TSHR cells. In contrast, the TSHR cells bound more 2C11antibody, because these cells contained more receptor thandid the ECD-TSHR cells, as documented by binding ofradiolabeled TSH. Serum from 17 of the 20 patients withGraves’ hyperthyroidism bound to ECD-TSHR cells betterthan to TSHR cells, despite the greater number of receptorson the TSHR cells. In contrast, serum from patients withhypothyroidism bound equally well to both types of cells.Serum from normal subjects did not bind to either type ofcell. Preincubation of A subunit with serum from patientswith Graves’ hyperthyroidism abolished serum binding tocells, whereas the effect of preincubation of A subunit withserum from patients with hypothyroidism was variable.
Conclusion TSHR-SAb in serum from patients withGraves’ hyperthyroidism bind preferentially to exposedTSH receptors, as compared with intact receptors, andbinding is readily inhibited by the A subunit. Exposure to Asubunit as a result of its natural shedding into extracellularfluid may be important in the pathogenesis of the disease.
Figure. Schematic Diagram of TSH Receptors Showing the Intact Receptor(TSHR) (Left), the Extracellular Domain Anchored to Cells (ECD-TSHR) (Mid-dle), and the Free A Subunit (Right). (Drawing kindly supplied by the authors.)Black ovals, TSHR-SAb epitope; horizontal lined triangles, A subunit.
GRAVES’ DISEASE
Shedding of part of the thyrotropin receptor may be important in thepathogenesis of hyperthyroidism in Graves’ disease
Chazenbalk GD, Pichurin P, Chen CR, Latrofa F, Johnstone AP, McLachlan SM, Rapoport B. Thyroid-stimulatingautoantibodies in Graves’ disease preferentially recognize the free A subunit, not the thyrotropin holoreceptor. J ClinInvest 2002;110:209-17.
44 ● CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3
COMMENTARY
Previous studies of the reactivity ofTSHR-SAb have suggested that the anti-bodies bind primarily to discontinuoussegments of the amino-terminal domainof the TSH receptor (1), indicating thatboth conformation of the receptor andits amino-acid sequence are determi-nants of antibody reactivity; in otherwords the epitopes are conformationaland structural. The present work extendsthis suggestion, by demonstrating differ-ences in TSHR-SAb reactivity with cellsin which the amino-terminal end of thereceptor had a different conformation.
What is perhaps surprising was thatcells with intact receptors bound TSHR-SAb less well than cells with incompletebut possibly more exposed receptors.These results, plus the neutralizationstudies, plus the fact that the A subunit isshed and therefore has easy access toantigen-processing cells, all support avery prominent role for the A subunit inthe generation and continued productionof TSHR-SAb. As the authors note, fur-ther support for a prominent role for theshed A subunit comes from the fact thatamong the receptors for glycoproteinhormones (TSH, luteinizing hormone,follicle-stimulating hormone, chorionic
gonadotropin), only TSH receptor arecleaved and shed, and there are no disor-ders of the gonads or placenta character-ized by production of antibodies thatactivate the receptors for the gonado-tropins.
Robert D. Utiger, M.D.
Reference
1. Rapoport B, Chazenbalk GD, JaumeJC, et al. The thyrotropin (TSH) recep-tor: interaction with TSH and autoanti-bodies. Endocr Rev 1998;19:673-716.

SUMMARY
Background Fetuses and neonates of mothers who havehyperthyroidism caused by Graves’ disease may have hyper-thyroidism, caused by the transplacental passage of thy-rotropin (TSH) receptor-stimulating antibodies. This studywas done to determine the relationship between maternalserum concentrations of these antibodies and the likelihoodof fetal or neonatal hyperthyroidism.
Methods From 1986 to 1995, serum TSH receptor-stimu-lating antibodies (in the form of thyroid-stimulatingimmunoglobulins) were measured in 61 pregnant women ina single laboratory. These measurements were done at thediscretion of the patient’s physician, using a bioassay inwhich immunoglobulins extracted from serum were incu-bated with cultured rat thyroid cells and the amount ofcyclic AMP generated was determined. The results wereexpressed as index units; 1 index unit was defined as theamount of cyclic AMP generated in the presence of a poolof serum immunoglobulins from normal subjects, and anindex value >1.3 (representing a >130 percent increase) wasconsidered a positive response.
Forty-nine women (80 percent) had positive serum indexvalues. Complete prenatal and delivery records were avail-able for review in 29 of these women, and they formed thebasis for the study. The fetuses were not evaluated system-atically. Fetal hyperthyroidism was defined as persistenttachycardia (>160 beats/minute), goiter, or hydrops; highfetal serum free thyroxine (T4) concentrations alone werenot considered to indicate fetal hyperthyroidism. All theneonates were evaluated for hyperthyroidism, and given adiagnosis of hyperthyroidism if they had symptoms andsigns of hyperthyroidism (tachycardia, goiter, irritability,hyperphagia, heart failure) and high serum free T4 and lowserum TSH concentrations.
Results The 29 women (mean age, 29 years; range, 18 to40) had 35 singleton pregnancies ending with live births.
During these 35 pregnancies; 11 of the women were treat-ed with propylthiouracil; 8 women were treated with T4, forradioiodine- or surgery-induced hypothyroidism; 6 receivedpropylthiouracil and T4; and the remainder received neither.The serum thyroid-stimulating immunoglobulin measure-ments were done during the second trimester in all the preg-nancies. The index values ranged from 1.1 to 15.0 (extrapo-lated from Figure 1).
Cordocentesis was done in seven fetuses at 24 to 35 weeksof gestation; their mothers had index values ranging from3.3 to 15.0. Four of the fetuses had high serum free T4 con-centrations. One had neonatal hyperthyroidism at birth aweek later. The other three infants were normal at birth; themothers of two had been taking propylthiouracil and weregiven a higher dose. Among the three fetuses with normalserum free T4 concentrations, one had neonatal hyperthy-roidism at birth three weeks later.
Overall, 29 of the 35 infants (83 percent) were deliveredvaginally, and 6 (17 percent) by cesarean section. Nineinfants (26 percent) were born preterm (<37 weeks), and 6(17 percent) had intrauterine growth restriction. Six infants(17 percent) had neonatal hyperthyroidism, including twoinfants delivered by each of two mothers. Five of these 6infants had tachycardia and 2 had heart failure; all weretreated with propylthiouracil. The mothers’ serum thy-roid-stimulating immunoglobulin index values ranged from5.8 to 15.0; one mother was taking T4 and two were takingpropylthiouracil. Among the 29 normal infants, the mothersof six (21 percent) had serum index values >5.0. The sensi-tivity and specificity of a serum index value ≥5 for predict-ing neonatal hyperthyroidism were 100 percent and 79 per-cent, respectively. The positive predictive value was 40 per-cent and the negative predictive value was 100 percent.
Conclusion Among pregnant women with hyperthy-roidism caused by Graves’ disease, only those with very highserum thyroid-stimulating immunoglobulin index valueshave fetuses and neonates at risk for hyperthyroidism.
GRAVES’ DISEASE
Neonatal hyperthyroidism occurs only in infants whose mothers have veryhigh serum thytropin receptor-stimulating antibody concentrations
Peleg D, Cada S, Peleg A, Ben-Ami M. The relationship between maternal serum thyroid-stimulating immunoglobulinsand fetal and neonatal thyrotoxicosis. Obstet Gynecol 2002;99:1040-3.
CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3 ● 45
COMMENTARY
Virtually all pregnant women whohave hyperthyroidism have as its causeGraves’ disease, whether the hyperthy-roidism preceded or began during thepregnancy. Among these women, it isnow clear, as reported by Peleg et al. andothers (1), that only those who have veryhigh serum concentrations of TSHreceptor-stimulating antibodies are likelyto have fetuses and neonates who havehyperthyroidism.
Should these antibodies be measured
in all pregnant women with any historyof Graves’ disease at about 15 weeks ofgestation, when the fetal thyroid isresponsive to thyroid stimulators? Thatseems inappropriate, and could be mis-leading. The values are not often high,and even if they are, the fetus andneonate may not have hyperthyroidism. Itseems more appropriate to monitor fetalgrowth, thyroid size, heart rate, and activ-ity clinically and by ultrasonography. Inthe unlikely event there are unequivocalsigns of fetal hyperthyroidism (poor fetal growth, goiter, hyperactivity),
then—depending on the proximity toterm—measure serum free T4 and TSHin serum obtained by cordocentesis orvery soon after delivery.
Robert D. Utiger, M.D.
Reference
1. Tamaki H, Amino N, Aozasa M, et al.Universal predictive criteria for neonatalovert thyrotoxicosis requiring treatment.Am J Perinatol 1988;5:152-8.

GRAVES’ OPHTHALMOPATHY
Patients with Graves’ ophthalmopathy may have long-term impairment invision and quality of life
Terwee C, Wakelkamp I, Tan S, Dekker F, Prummel MF, Wiersinga W. Long-term effects of Graves’ ophthalmopathy onhealth-related quality of life. Eur J Endocrinol 2002;146:751-7.
46 ● CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3
COMMENTARY
This study confirms that patientswith Graves’ ophthalmopathy severeenough to warrant glucocorticoid ororbital radiation are likely to have persist-ent visual deficits that adversely affecttheir quality of life.
As acknowledged by the authors,there are many difficulties with the inter-pretation of data from this study. Refer-ral bias resulted in preselection ofpatients with more severe eye disease,limiting the applicability of the findings.
The patients with Graves’ ophthalmopa-thy were older and less educated than thereference population, both of whichdiminish general quality-of-life scores.
Several questions go unanswered.What were the quality-of-life scores inpatients in whom eye appearance andfunction were restored to normal by glu-cocorticoid or radiation therapy? Arethere lingering psychological effects asso-ciated with the illness and therapy apartfrom a persistent visual deficit or alteredappearance?
Despite the limitations of the study,
the authors found that both previouslytreated and currently treated patients withGraves’ ophthalmopathy have lower qual-ity-of-life scores than a reference popula-tion. Demonstration of an improvementin these important subjective changesmay therefore become a useful measureof successful therapy.
Henry B. Burch, M.D.Walter Reed Army Medical Center
Washington, D.C.
Table 2. Scores on the General and Graves’ Ophthalmopathy Quality-of-LifeQuestionnaires.
Treated Patients Patients Being Normal Subjects (n=163) Treated (n=204) (n=750)
Mobility—good/poor (%) 61/39 66/34 95/5Usual activities—yes/no 59/41 34/66 86/14Pain/discomfort—
no/yes (%) 42/58 30/70 68/32Anxiety/depression—
no/yes (%) 68/32 46/54 84/16Visual function* 78±24 58±28Appearance of eyes* 77±22 58±25
*Mean (±SD) score on scale of 0 to 100 (marked limitation or abnormality tono limitation or abnormality).
Table 1. Characteristics of Patients with Graves’ Ophthalmopathy.Treated Patients Patients Being Treated
(n=168) (n=206)Age—yr (±SD) 58±13 50±12Women/men (%) 78/22 83/17Radiation/prednisone/both—(%) 13/32/55 5/29/16Current eye findings (n=154) (n=206)Soft tissue changes—no/yes (%) 87/13 16/84Proptosis—≤19 mm/≥20 mm (%) 40/60 62/38Diplopia—no/yes (%) 49/51 37/63Visual acuity—normal/impaired (%) 72/28 78/22
SUMMARY
Background Patients with Graves’ ophthalmopathy mayhave persistent changes in the appearance and function oftheir eyes, and these changes may lead to long-term psycho-logical problems and limitations in physical and psychoso-cial activities. In this study the long-term effects of Graves’ophthalmopathy on general and visual quality of life and onvisual function were assessed.
Methods The main study group consisted of patients withGraves’ ophthalmopathy treated with external-beam radia-tion, prednisone, or both, at a referral center between 1982and 1992; the patients were studied in 1999-2000. Otherstudy groups were patients with Graves’ ophthalmopathystudied at the time of radiation therapy or orbital surgery in1997-1998, and subjects from the general population(results from the literature). The study subjects completedone or more of several questionnaires relating to quality oflife, and the patients with ophthalmopathy also completed aGraves’ ophthalmopathy quality-of-life questionnaire andwere evaluated by an ophthalmologist.
Results The previously treated ophthalmopathy groupconsisted of 247 patients, of whom 34 (14 percent) haddied, 45 (18 percent) declined to participate, and 168 (68percent) were studied 7 to 23 years (median, 12) after ther-apy (Table 1). The patients studied while being treated weresimilar, except with respect to some eye findings.
Both groups of patients with ophthalmopathy scored lowerthan the normal subjects on several components of thegeneral quality-of-life questionnaire, and the scores on theGraves’ ophthalmopathy quality-of-life questionnaire werelower in the patients being treated than in those previouslytreated (Table 2).
In the previously treated patient group, those who werenon-smokers had higher scores on the Graves’ ophthal-
mopathymopathy quality-of-life score than smokers.Patients treated with radiation tended to score lower on thegeneral quality-of-life questionnaires. Patients considered tohave responded to radiation or prednisone therapy(decreased soft-tissue changes, proptosis, and diplopia;increased visual acuity) scored higher on both question-naires.
Conclusion Patients with Graves’ ophthalmopathy mayhave persistent impairment in the appearance and functionof their eyes and a decreased quality of life.

SUMMARY
Background Patients who have germline loss-of-functionmutations in both alleles of the thyrotropin (TSH)-receptorgene may have either overt or subclinical hypothyroidism,and those who have a mutation in one allele may be normalor have subclinical hypothyroidism. In this study mutationsof the TSH receptor were sought in patients with subclini-cal hypothyroidism who had no evidence of autoimmunethyroid disease.
Methods The study subjects were 10 patients (4 femaleand 6 male; age range, 23 days to 25 years) with subclinicalhypothyroidism (initial serum TSH concentration, 6.6 to46.0 mU/L, normal serum free thyroxine [T4] concentra-tions) and their parents and siblings. All the patients hadnormal serum antithyroid peroxidase, antithyroglobulin,and anti-TSH receptor antibody concentrations. Three ofthe five patients who had been tested for hypothyroidism asneonates had high blood-spot TSH values. Ultrasonographyrevealed thyroid hypoplasia in two patients and a normalthyroid gland in eight patients.
DNA was extracted from peripheral blood leukocytes, andthe entire coding sequence and exon-intron boundaries ofthe TSH-receptor gene were sequenced (the receptor iscomposed of an N-terminal extracellular domain, a trans-membrane domain, and a C-terminal intracellular domain).The DNA substitutions found in the patients were intro-duced into the wild-type TSH-receptor gene by site-direct-ed mutagenesis. Wild-type and mutated DNA was insertedinto cells and the cells were cultured for 48 hours. Intactcells and cells rendered permeable to antibodies then wereexamined by flow cytometry using anti-TSH receptor anti-bodies. In addition, cyclic AMP production was measured intransfected cells incubated without and with bovine TSH.
Results Five different mutations in the TSH-receptor genewere detected in 4 of the 10 patients. One patient
(age 25 years) was a compound heterozygote, with a muta-tion in the extracellular domain of the receptor in one alleleof the gene and a mutation in the transmembrane domainin the other allele (serum TSH concentrations, 31.5 to 46.0mU/L). The parents and brother of this patient had onemutated and one wild-type allele, and each had normal orslightly high serum TSH concentrations on different occa-sions (3.5 to 6.2 mU/L). The other three patients (aged 23days, 30 days, and 5 years) were heterozygotes, with onewild-type allele and a mutation in either the extracellulardomain or the transmembrane domain of the other allele. Aparent or sibling of two of these three patients carried thesame allele (and had slightly high serum TSH concentra-tions). The third patient had a normal mother and sibling;her father was not tested.
Similar quantities of TSH receptors were detected in per-meabilized cells transfected with wild-type and mutantTSH-receptor DNA, but fewer TSH receptors were detect-ed on intact cells transfected with mutant DNA as com-pared with cells transfected with wild-type DNA. Theseresults indicate that the cells synthesized similar amounts ofTSH receptors, but the mutated receptors were not insertedinto the cell membrane. As compared with cells transfectedwith wild-type TSH-receptor DNA, cells transfected withmutant DNA produced little cyclic AMP, both basally andin response to TSH.
Serum TSH concentrations were high (6.1 to 26.7 mU/L) ina parent and one or more siblings of four of the six patientsin whom no mutation was detected.
Conclusion Germline loss-of-function mutations in oneor both alleles of the TSH-receptor gene can cause subclin-ical hypothyroidism.
HYPOTHYROIDISM
Germline loss-of-function mutations of the thyrotropin-receptor gene are acause of subclinical hypothyroidism
Alberti L, Proverbio MC, Costagliola S, Romoli R, Boldrighini B, Vigone MC, Weber G, Chiumello G, Beck-Peccoz P,Persani L. Germline mutations of TSH receptor gene as cause of nonautoimmune subclinical hypothyroidism. J ClinEndocrinol Metab 2002;87:2549-55.
CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3 ● 47
COMMENTARY
These results document that thepresence of one normal allele of theTSH-receptor gene does not necessarilyprovide thyroid cells with enough recep-tors to allow normal thyroid secretion.
The results also raise the possibilitythat genetic disorders may be a cause ofsubclinical hypothyroidism in the general
population, not just in infants with con-genital hypothyroidism. In most patientssubclinical hypothyroidism is attributedto chronic autoimmune thyroiditis, whichseems reasonable enough in patients withhigh serum antithyroid antibody concen-trations. But what about those in whomthe serum antibody concentrations arenot high? Might not some of them havea mutation reducing TSH receptors or a
step in intracellular TSH signaling? As afirst step in investigating this possibility,serum TSH could be measured in par-ents, siblings, and offspring of a group ofadults with subclinical hypothyroidism.
Robert D. Utiger, M.D.

SUMMARY
Background Subclinical hypothyroidism (high serum thy-rotropin [TSH] and normal serum thyroid hormone con-centrations) is common, and some patients later have overthypothyroidism. This study was undertaken to determinethe rate of progression of subclinical hypothyroidism toovert hypothyroidism (high serum TSH and low serum freethyroxine [T4] concentrations) and to identify the risk fac-tors for progression.
Methods The study subjects were 82 women (mean age, 51years) with subclinical hypothyroidism on two occasionsone month apart. They included 42 women with a history ofhyperthyroidism caused by Graves’ disease, of whom 32had been treated with radioiodine 1 to 28 years earlier(median, 7) and 10 by surgery; 29 women with chronicautoimmune thyroiditis; and 11 with nontoxic goiter, all pre-viously treated by surgery. The women were evaluated byclinical examination, including assessment of hypothyroidsymptoms by two scoring systems (Billewicz, Zulewski), andmeasurements of serum TSH, free T4, antithyroid microso-mal (peroxidase) antibodies, lipids, and creatine kinase atyearly intervals. The study end points were overt hypothy-roidism on two occasions (interval not stated), or initiationof T4 therapy for Graves’ ophthalmopathy, prevention ofrecurrent goiter after thyroidectomy, depression, hypercho-lesterolemia, or infertility.
Results The mean follow-up period was 9 years (range, 0.5to 26), during which there were no changes in mean symp-tom scores, serum lipid or creatine kinase concentrations, orserum free T4 concentrations, whereas the mean (±SE)serum TSH concentration increased from 12.0±1.1 to18.9±2.7 mU/L. At base line, 21 women (26 percent) hadserum TSH concentrations >4.0 to 6.0 mU/L, 36 women(44 percent) had values of >6 to 12 mU/L, and 25 women(30 percent) had values of >12 mU/L. The mean base-line
and final serum TSH concentrations in these three groupswere, respectively, 5.0 and 6.0 mU/L, 8.6 and 15.9 mU/L,and 22.9 and 34.1 mU/L. The base-line and final values forthe symptom scores and other measurements, includingserum free T4 concentrations, were similar in all three sub-groups, as they were in all 82 women.
During follow-up 23 women (28 percent) developed overthypothyroidism, 56 (68 percent) had persistent subclinicalhypothyroidism, and 3 (4 percent) became euthyroid. Thelikelihood of overt hypothyroidism increased as a functionof the base-line serum TSH concentration; as determinedby Kaplan-Meier analysis, the 10-year risk was 0 percent inthe women with base-line serum TSH concentrations >4 to6 mU/L, 43 percent (3 percent/year) in the women withbase-line concentrations >6 to 12 mU/L, and 77 percent(11 percent/year) in the women with base-line concentra-tions >12 mU/L. Among the 56 women who had persist-ent subclinical hypothyroidism, 17 (30 percent) were treatedwith T4, and they were then excluded from furtherfollow-up.
A high serum antithyroid microsomal antibody titer at baseline was an additional risk factor for overt hypothyroidism.The cumulative incidence of overt hypothyroidism was 23percent among the 40 women with normal serum antibodytiters and 58 percent among the 42 women with high serumantibody titers.
The likelihood of overt hypothyroidism was similar in the32 women who had Graves’ hyperthyroidism and had beentreated with radioiodine and the 29 women with chronicautoimmune thyroiditis.
Conclusion Among women with subclinical hypothy-roidism the risk of overt hypothyroidism is higher in thosewith higher serum TSH concentrations and high serumantithyroid microsomal antibody titers.
HYPOTHYROIDISM
Progression from subclinical to overt hypothyroidism is most likely inwomen with higher serum TSH concentrations and high serum antithyroidantibody titers
Huber G, Staub J-J, Meier C, Mitrache C, Guglielmetti M, Huber P, Braverman LE. Prospective study of thespontaneous course of subclinical hypothyroidism: prognostic value of thyrotropin, thyroid reserve, and thyroidantibodies. J Clin Endocrinol Metab 2002;87:3221-6.
48 ● CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3
COMMENTARY
Whether people with subclinicalhypothyroidism should be treated withT4 is controversial. One argument fortreatment is to prevent progression toovert hypothyroidism, but how oftendoes that occur and can it be predicted?The answers from both this and otherstudies is that it does occur, and that itcan to some extent be predicted. Some
of the studies, like this one, were of peo-ple known to have thyroid disease, butothers, like the 20-year Whickham,United Kingdom study, were community-based (1).
Robert D. Utiger, M.D.
Reference
1. Vanderpump MP, Tunbridge WM,
French JM, et al. The incidence of thy-roid disorders in the community: a twen-ty-year follow-up of the Whickham Sur-vey. Clin Endocrinol 1995;43:55-68.

HYPOTHYROIDISM
Serum concentrations of multiple enzymes may be high in patients withhypothyroidism
Saha B, Maity C. Alteration of serum enzymes in primary hypothyroidism. Clin Chem Lab Med 2002;40:609-11.
SUMMARY
Background Some patients with primary hypothyroidismhave high serum concentrations of creatine kinase, aspar-tate aminotransferase, and other enzymes, but the relation-ships between the elevations and the severity of hypothy-roidism, as determined by measurements of serum thy-rotropin (TSH), are not clear. In this study these and otherenzymes were measured and the results correlated withserum thyrotropin (TSH) concentrations in a large group ofpatients with primary hypothyroidism.
Methods The study subjects were 114 patients, aged 7 to65 years, with spontaneously occurring primary hypothy-roidism, with or without thyroid enlargement, as defined bya serum TSH concentration >14 mU/L; serum thyroxinewas not measured. Patients with a history of other thyroiddiseases or treatment for thyroid disease, other illnesses, ortreatment with any drug that affects thyroid function, andpregnant women were excluded. Fasting blood sampleswere collected before and 3 weeks to 11 months after theinitiation of thyroxine therapy for measurements of serumTSH, creatine kinase, aspartate aminotransferase, alanineaminotransferase, alkaline phosphatase, and amylase. Noage- and sex-matched normal subjects were studied at thesame time.
Results Forty-seven of the 114 patients (41 percent) hadnormal serum concentrations of all five enzymes. Among
the other patients, 8 (7 percent) had high serum concentra-tions of creatine kinase, aspartate aminotransferase, alanineaminotransferase, and amylase, and the remainder had highserum concentrations of one to three of these enzymes.Among the individual enzymes, high values were found infrom 3 percent to 37 percent of the patients (Table).
Fifty-three patients had serum TSH concentrations <100mU/L, of whom 38 (72 percent) had normal serum con-centrations of all five enzymes. In this group there was nocorrelation between serum TSH concentrations and theserum concentrations of any of the enzymes.
Serum creatine kinase concentrations decreased from highto normal or decreased within the normal range during thy-roxine therapy. The patterns of change in the otherenzymes were similar.
Conclusions Among several serum enzymes, the concen-trations of creatine kinase are most often high in patientswith hypothyroidism, but there is little correlation betweenserum enzyme and TSH concentrations.
COMMENTARY
The serum enzymes measured inthese patients with hypothyroidism origi-nate in different tissues, and they may becleared from the circulation by differenttissues as well. In the case of creatinekinase, the increases are in the MMisoenzyme that predominates in skeletalmuscle, and the high serum concentra-tions are caused by the increased perme-ability of skeletal muscle cells, but it islikely that clearance of the enzyme isslowed as well. A combination ofincreased release from tissues as diverseas the liver, pancreas, salivary glands, andskeleton, and slowed clearance probablyexplains the increased serum concentra-tions of the other enzymes as well.Physicians who order serum enzymemeasurements should be aware thathypothyroidism can cause elevations notonly of serum creatine kinase but alsoother enzymes.
High serum creatine kinase concen-trations occur not only in patients withovert hypothyroidism, but also in thosewith subclinical hypothyroidism. In astudy of 104 patients with widely varyingserum TSH concentrations serum crea-tine kinase (and myoglobin) and TSHconcentrations were positively correlated,and the mean serum creatine kinase con-centration in the patients with overthypothyroidism was seven times that inthe normal subjects (579 versus 86 U/L)(1). The relationship between muscle dys-function and serum creatine kinase con-centrations in patients with hypothy-roidism varies. Patients with myopathyusually have high concentrations (2), andmassive elevations have been found in afew patients, for example to 29,160 U/Lin a man with marked proximal myopa-thy that responded well to thyroxine ther-apy (3). Other patients with high serumcreatine kinase concentrations do not
have overt myopathy, but it probably isn’tlooked for very diligently.
Robert D. Utiger, M.D.
References
1. Staub JJ, Althaus BU, Engler H, et al.Spectrum of subclinical and overthypothyroidism: effect on thyrotropin,prolactin, and thyroid reserve, and meta-bolic impact on peripheral target tissues.Am J Med 1992;92:631-42.
2. Rodolico C, Toscano A, Benvenga S,et al. Myopathy as the persistently isolat-ed symptomatology of primary autoim-mune hypothyroidism. Thyroid1998;8:1033-8.
3. Scott KR, Simmons Z, Boyer PJ.Hypothyroid myopathy with a strikinglyelevated serum creatine kinase level.Muscle Nerve 2002;26:141-4.
CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3 ● 49
Table. Serum Enzyme Concentrations in Patients with HypothyroidismCreatine Aspartate Alanine Amylase AlkalineKinase Amino- Amino- Phosphatase
transferase transferasePatients with 42 (37%) 40 (35%) 33 (29%) 17 (15%) 3 (3%)
high values

SUMMARY
Background Patients with central hypothyroidism typical-ly have normal or low serum thyrotropin (TSH) concentra-tions and low serum thyroxine (T4) concentrations. Theefficacy of treatment with T4 in these patients is usuallyassessed by measurements of serum free T4, and there hasbeen little study of the relationship between their serumTSH and free T4 concentrations before and during T4 treat-ment. This retrospective study was undertaken to evaluatethis relationship, with the hypothesis that TSH secretion inthese patients is sensitive to changes in serum free T4 con-centrations, but is lower at all serum free T4 concentrationsthan it is in normal subjects or patients with primaryhypothyroidism.
Methods The study subjects were 41 patients (17 women,24 men; mean age, 48 years [range, 16 to 77]). All had adult-onset hypothalamic-pituitary disease and low serum free T4concentrations; their serum TSH concentrations were low,normal, or slightly high. The hypothalamic-pituitary dis-eases were: nonsecreting pituitary adenoma, 16 patients;somatotroph adenoma, 6 patients; prolactinoma, 5 patients;and craniopharyngioma, pituitary apoplexy, histiocytosis X,hypophysitis, sellar cyst, meningioma, and empty sella, 3 orfewer patients each. Thirty patients had been treated surgi-cally, and 18 had received radiation therapy. Thirty-threepatients were taking glucocorticoids, 22 estrogen or testos-terone, and 9 vasopressin.
The patients were treated with 50 to 150 µg of T4 daily(mean, 1.15 µg/kg/day). The initial dose was increased inincrements of 25 µg until the patient was clinically euthyroidand had a normal serum free T4 concentration (intervalbetween dose changes not given). Serum free T4 and TSH(assay sensitivity, 0.005 mU/L) were measured at multipletimes in each patient during a mean follow-up period of 7years (range, 0.5 to 23). The results in 20 patients who hadat least three consecutive measurements before and duringtreatment were compared with similarly obtained results in17 patients with primary hypothyroidism.
Results The mean (±SE) pretreatment serum TSH con-centration in the patients with central hypothyroidism was2.0±0.2 mU/L (range, 0.06 to 5.8); five patients had values>4.0 mU/L, and 9 had values <0.5 mU/L. The changes inserum TSH and free and total T4 concentrations duringtreatment are shown in the Table.
During treatment, 92 percent of patients who had serumTSH concentrations <0.1 mU/L had normal serum free T4concentrations, as compared with only 34 percent ofpatients who had serum TSH concentrations >1 mU/L.
The mean pretreatment serum TSH concentration in thepatients with primary hypothyroidism was 75.5±19.6mU/L, and the final concentration was 5.4±2.2 mU/L. Theslopes of the regression lines for the logarithm of theserum TSH concentrations as a function of the serum freeT4 concentrations before and during treatment in the 20patients with central hypothyroidism and 17 patients withprimary hypothyroidism were parallel, but at a zero serumfree T4 concentration the serum TSH concentration wasapproximately three log units lower in the patients with cen-tral hypothyroidism.
Conclusion Serum TSH concentrations vary inverselywith serum free T4 concentrations in patients with centralhypothyroidism, indicating that T4-mediated negative feed-back is preserved, but at a considerably lower set point thanin patients with primary hypothyroidism.
HYPOTHYROIDISM
Thyroxine inhibits thyrotropin secretion in patients with centralhypothyroidism
Shimon I, Cohen O, Lubetsky A, Olchovsky D. Thyrotropin suppression by thyroid hormone replacement is correlatedwith thyroxine level normalization in central hypothyroidism. Thyroid 2002;12:823-7.
50 ● CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3
COMMENTARY
Shimon et al. have clearly demon-strated that TSH secretion in patientswith central hypothyroidism is sensitiveto changes in serum free T4 concentra-tions, albeit in a quantitatively abnormalway. The set point of TSH secretion islowered. As compared with normal sub-jects, not only is the patients’ TSH secre-
tion low relative to the ambient serumfree T4 concentration, but also it is muchmore easily inhibited by small increases inserum free T4 concentrations. While rela-tively normal serum TSH concentrationsin patients with central hypothyroidismbeing treated with T4 suggest that treat-ment was inadequate, the slopes of theserum TSH-free T4 plots were differentin different patients, so that it is doubtful
that measurements of serum TSH, evenif done using a very sensitive assay, cansupplant measurements of serum free T4as an indicator of the adequacy of treat-ment in patients with central hypothy-roidism.
Robert D. Utiger, M.D.
Table. Serum TSH and Thyroid Hormone Concentrations in Patients withCentral Hypothyroidism during T4 Treatment.
Base Line 6 Months 28 Months LastT4 dose (µg/day) 0 58±5 81±5 86±6Serum TSH (mU/L) 2.0±0.2 1.0±0.2 0.6±0.2 0.5±0.2Serum free T4 (ng/dL)* 0.6±0.04 0.9±0.1 1.1±0.1 1.2±0.1Serum T4 (µg/dL)* 4.4±0.2 8.1±0.4*To convert serum free T4 and T4 values to pmol/L and nmol/L, respectively,multiply by 12.9.

NODULAR GOITER
Thyroxine therapy does not reduce the size of benign solitary thyroid nod-ules: systematic analysis of multiple studies
Castro MR, Caraballo PJ, Morris JC. Effectiveness of thyroid hormone suppressive therapy in benign solitary thyroidnodules: a meta-analysis. J Clin Endocrinol Metab 2002;87:4154-9.
SUMMARY
Background Patients with a benign solitary thyroid noduleare often treated with thyroxine (T4) to reduce nodule size,but the efficacy of this therapy is uncertain. This study wasa meta-analysis of controlled clinical trials of T4 therapy inpatients with benign solitary thyroid nodules.
Methods The literature was searched to identify trials ofT4 therapy in patients with a thyroid nodule. To be includedin the analysis, the trial had to be a randomized controlledtrial of patients with a single thyroid nodule, as detected bypalpation, proven to be benign by fine-needle aspirationbiopsy. Other inclusion criteria were measurements of nod-ule volume by ultrasonography, with a response to therapybeing defined as a >50 percent decrease in volume; docu-mentation of suppression of thyrotropin (TSH) secretionby T4; and duration of treatment of at least six months.
Results Thirteen trials of T4 therapy in patients with abenign solitary thyroid nodule were identified. Amongthem, six met the inclusion criteria and were thereforeincluded in the meta-analysis. One of the excluded trialsdescribed the same patients after treatment for five years;the others were excluded because they did not meet theinclusion criteria in one or more ways.
The six trials included 346 patients (313 women, 33 men),all of whom had normal thyroid function. The mean ageranged from 34 to 48 years. Most trials included onlypatients with a solid nodule or a nodule that was ≤20 per-cent cystic. At base line, the patients in the T4-treatment andcontrol groups in each study were well matched in clinicalcharacteristics, thyroid-function test results, and nodule vol-ume. The mean nodule volumes in individual studies variedconsiderably, from 3.0 and 2.6 mL in the T4-treatment and
control groups, respectively, in study 1 (Table) to 16.4 and13.6 mL in the respective groups in study 5. The duration oftreatment varied from 6 to 12 months. The doses of T4ranged from 1.5 to 3 µg/kg; in some studies the dose wasfixed, but in others it was adjusted to meet a specific serumTSH target, usually just below the lower limit of the normalrange. The control group received a placebo in four trialsand nothing in two. The investigators who measured nodulevolume were not aware of treatment-group assignment inall trials.
Overall, nodule volume decreased by more than 50 percentin 22 percent of the T4-treated patients and by 10 percentin the control patients; in only one trial was the differencestatistically significant. The relative risk (likelihood) of a>50 percent decrease in nodule volume in the T4-treatmentgroup, as compared with the control group, is shown in theTable. The mean nodule volume was similar in the T4-treat-ment and control groups at the end of each trial, excepttrial 4.
Conclusion In patients with a benign solitary thyroid nod-ule, T4 therapy for 6 to 12 months does not result in a sub-stantial decrease in nodule size.
COMMENTARY
The results of this meta-analysis ofT4 treatment in patients with a benignsolitary nodule were similar to those of apreceding one (1). The first meta-analysisincluded seven trials (413 patients); nod-ule volume decreased by >50 percent in26 percent of the T4-treated patients and12 percent of the control patients(P<0.05). Five of these trials were includ-ed in this new analysis, two were exclud-ed because they were not randomized,and one new trial was included. Thesetrials were heterogeneous, in that nodulesize, cystic content of the nodules, anddose of T4 varied. The pathology of the
nodules and their content of TSH recep-tors, presumably a key determinant ofthe efficacy of T4 therapy, surely variedtoo.
Even if T4 therapy does notdecrease nodule size, it might preventnodule growth. Summary data on thispoint can be found in reference 1; in fourtrials (trials 1, 3, 4, and 5) nodule volumeincreased by >50 percent in 8 percent ofthe T4-treated patients and 17 percent ofthe control patients (P<0.05).
Any continued use of T4 in thesepatients rests primarily on the lack ofsimple alternative treatments. Thyroidnodules can be destroyed by injections ofethanol, but the treatment is not simple.
As for T4 therapy, the benefit, if any, isso marginal, and the hazards, howeversmall, of the subclinical hyperthyroidismthat results from the therapy are suchthat doing nothing seems wiser.
Robert D. Utiger, M.D.
Reference
1. Zelmanovitz F, Genro S, Gross JL.Suppressive therapy with levothyroxinefor solitary thyroid nodules: a double-blind controlled clinical study and cum-ulative meta-analysis. J Clin EndocrinolMetab 1998;83:3881-5.
CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3 ● 51
Table. Relative Risk (Likelihood) of a >50 Percent Decrease inNodule Volume during T4 Treatment.Trial No. of Patients Location Relative Risk
(95% Confidence Interval)1 53 USA 0.7 (0.2-2.4)2 40 Spain 1.3 (0.3-5.2)3 101 Italy 3.3 (1.0-11.2)4 45 Italy 18.2 (1.1-295.2) 5 45 Brazil 3.4 (0.8-15.2)6 62 Iran 1.4 (0.4-4.5)Total 346 1.9 (1.0-3.8)

SUMMARY
Background Patients with a thyroid nodule in whom abiopsy reveals a follicular tumor or is nondiagnostic areoften treated by unilateral thyroid lobectomy. If the noduleproves to be a follicular or papillary carcinoma, the patientsare usually advised to undergo contralateral thyroid lobecto-my—so-called completion thyroidectomy. One rationale forcompletion thyroidectomy is that the remaining lobe maycontain one or more microscopic thyroid carcinomas.Another is that it is difficult to destroy a normal thyroidlobe with radioiodine (I-131), and the presence of normalthyroid tissue reduces the value of measurements of serumthyroglobulin as a tumor maker and makes it difficult if notimpossible to treat recurrent tumor with I-131. This retro-spective case study was done to determine the safety ofcompletion thyroidectomy.
Methods The study subjects were all 36 patients whounderwent thyroid lobectomy and then completion thy-roidectomy by one surgeon between 1997 and 2000. Therewere 32 women and 4 men; mean age, 44 years (range, 19 to59). The completion operation was performed via a low-collar incision, with excision of the scar from the previousthyroid lobectomy. Parathyroid and laryngeal- nerve func-tion were routinely assessed pre- and postoperatively.
Results All patients underwent fine-needle aspirationbiopsy before their initial operation. The biopsy diagnoseswere follicular tumor in 32 patients (89 percent) and
Hurthle-cell tumor in 1 patient (3 percent); the biopsy wasnondiagnostic in 3 patients (8 percent). The findings at theinitial thyroid lobectomy were follicular variant of papillarycarcinoma in 29 patients (80 percent), follicular carcinomain 6 patients (17 percent), and Hurthle-cell carcinoma in 1patient (3 percent). Two patients (6 percent) had transienthypocalcemia postoperatively.
Completion thyroidectomy, done between 2 and 103 days(mean, 43) after the initial thyroid lobectomy, revealed thy-roid carcinoma in 20 of the 36 patients (56 percent). Thepathological diagnosis was follicular variant of papillary car-cinoma in 18 patients (50 percent), follicular carcinoma in 1patient (3 percent), and Hurthle-cell carcinoma in 1 patient(3 percent). No tumor was found in 16 patients (44 percent).Five patients (14 percent) had transient hypocalcemia, butnone had permanent hypocalcemia. No patient had recur-rent laryngeal-nerve injury, as assessed by nasopharyngo-laryngoscopy, after the initial or completion thyroidectomy.
Conclusion In patients with thyroid nodules that prove atsurgery to be thyroid carcinomas, completion thyroidecto-my can be performed safely a few days or many weeks afterinitial surgery and reveals thyroid carcinoma in approxi-mately 50 percent of patients.
THYROID CANCER
Completion thyroidectomy can be done safely after thyroid lobectomy inpatients with thyroid carcinoma
Kupferman ME, Mandel SJ, DiDonato L, Wolf P, Weber RS. Safety of completion thyroidectomy following unilaterallobectomy for well-differentiated thyroid cancer. Laryngoscope 2002;112:1209-12.
52 ● CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3
COMMENTARY
The need for completion thyroidec-tomy in patients who present with a thy-roid nodule is based not only on the lim-itations of fine-needle-aspiration biopsyand frozen-section diagnosis at the timeof surgery, but also on the patient’s orsurgeon’s hope that the nodule will proveto be benign, obviating the need forremoval of the contralateral lobe of thethyroid and therefore the need for life-long thyroxine therapy. This hope is sus-tained by the fact that the majority ofpatients in whom biopsy reveals a follicu-lar or Hurthle-cell tumor do not have afollicular or Hurthle-cell carcinoma. Inthem, unilateral thyroid lobectomy is ade-quate treatment. In patients in whom thenodule proves to be a carcinoma on
examination of permanent microscopicsections, a recommendation for comple-tion thyroidectomy is based on the beliefthat bilateral thyroid lobectomy (usuallynear-total thyroidectomy) is a more effec-tive treatment for papillary or follicularthyroid carcinoma than is a unilaterallobectomy. This belief is based on thefact that the contralateral lobe often con-tains one or more foci of carcinoma, aswas the case in 56 percent of thepatients in this study, and that some ofthese foci are clinically important, basedon the results of studies demonstratingthe superiority of near-total thyroid-ectomy over unilateral lobectomy astreatment for thyroid carcinoma (seepage 53).
The question of the optimal timingof completion thyroidectomy was not
addressed in this study, but in a recentstudy of 100 consecutive patients under-going this operation, the frequency ofpostoperative complications was low, andnot related to the timing of the comple-tion operation (1).
Robert D. Utiger, M.D.
Reference
1. Tan MP, Agarwal G, Reeve TS, et al.Impact of timing on completion thy-roidectomy for thyroid cancer. Br J Surg2002;89:802-4.

SUMMARY
Background There has been continued debate regardingthe most appropriate surgical treatment and the value ofpostoperative radioiodine (I-131) therapy for patients withpapillary thyroid carcinoma. This study determined thetemporal trends in therapy and the cause-specific mortalityand tumor recurrence rates in a large cohort of patientswith papillary carcinoma.
Methods The study subjects were all 2444 patients (1648females, 796 males; median age, 46 years [range, 4 to 90])with papillary carcinoma who underwent surgery at theMayo Clinic from 1940 to 1999. The median follow-up was15 years (longest, 60 years). Among the 2444 patients, 2305(94 percent) were considered cured, because resection wasthought to be complete or no metastases were detectedwithin 30 days after surgery.
Results The mean tumor size was 2.1 cm (range, 0.1 to15.0). At surgery, 693 patients (28 percent) had multicentrictumors, 328 patients (13 percent) had locally invasivetumors, and 983 patients (40 percent) had regional lymphnode metastases. Based on the MACIS scoring system (dis-tant Metastases [0, 3], Age [3.1 if age ≤39 years, 0.08 × ageif older], Completeness of resection [0, 1], local invasion[0, 1], and tumor Size [0.3 × tumor size], 2038 patients(83 percent) were considered low risk (score, <6) and 406(17 percent) were high risk (score, ≥6).
The initial operation was a near-total or total thyroidectomyin 1905 patients (78 percent), bilateral subtotal lobectomy in215 patients (9 percent), unilateral lobectomy in 284patients (12 percent); the remainder had lesser operations.Postoperatively, 774 patients (33 percent) received I-131therapy for remnant destruction. I-131 was not given during
the 1940s; the rates in subsequent decades are shown in theTable. Risk status was not a determinant of I-131 therapy;for example, in the 1980s, 57 percent of low-risk patientsand 50 percent of high-risk patients received I-131, and inthe 1990s the respective percentages were 42 percent and 49percent.
Among the 2305 patients thought to have compete resec-tions, 673 (29 percent) died, a rate similar to that expectedfor people living in the same region. The cancer-specificmortality rates were 4 percent at 10 years and 5 percent at15, 20 and 25 years. The tumor recurrence rates at thesetimes were 11, 12, 13, and 14 percent, respectively. The 10-year cancer-specific mortality and recurrence rates bydecade are shown in the Table.
Despite the differences in extent of surgery and frequencyof I-131 therapy, the 10-year cancer-specific mortality andrecurrence rates did not vary in either the low-risk or high-risk patients during the five decades from 1950 to 1999.
Conclusion Among patients with papillary thyroid carci-noma, cancer-specific death rates and recurrence rates havechanged little since 1950, despite the increasing extent ofsurgery and the increasing frequency of postoperative I-131therapy.
CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3 ● 53
THYROID CANCER
Changes in surgical practice and use of postoperative radioiodine therapyhave had limited effect on outcome in patients with papillary thyroidcarcinoma
Hay ID, Thompson GB, Grant CS, Bergstralh EJ, Dvorak CE, Gorman CA, Maurer MS, McIver B, Mullan BP, ObergAL, Powell CC, van Heerden JA, Goellner JR. Papillary thyroid carcinoma managed at the Mayo Clinic during sixdecades (1940-1999): temporal trends in initial therapy and long-term outcome in 2444 consecutively treated patients.World J Surg 2002;26:879-85.
COMMENTARY
There has been a long-runningdebate about the value of postoperativetreatment with I-131 for the purpose ofdestroying any thyroid tissue remainingafter surgery in patients with papillarycarcinoma (remnant ablation). The mainreason the debate continues is that all thestudies of this treatment have been ret-rospective and observational, with inher-ent biases, especially selection bias.
In some studies, remnant ablation
was associated with decreased mortalityand recurrence rates in patients with allbut the smallest tumors. In contrast, inthis study by Hay et al. remnant ablationhad little effect on mortality or recur-rence rates in both low-risk and high-riskpatients. However, the results may not beas compelling as they seem. Many of theresults are given as percentages, andoften the numbers of patients on whomthese percentages are based are notgiven. This is particularly a problem withrespect to the long-term follow-up
results; the number of patients treated inthe 1980s and 1990s and followed up for10 or more years is likely to be small.Nonetheless, the results provide a strongargument for reconsidering the use ofremnant ablation, especially in low-riskpatients.
Richard J. Robbins, M.DMemorial Sloan-Kettering Cancer Center
New York, NY
Table. Rates of Bilateral Surgery, I-131 Therapy, Cancer-Specific Mortality,and Tumor Recurrence in 2305 Patients with Papillary Carcinoma, by Decade.
Decade of Diagnosis1940-49 1950-59 1960-69 1970-79 1980-89 1990-99
Bilateral surgery (%)* 30 78 94 97 96 91I-131 therapy (%)* 0 4 2 18 57 46Mortality—10-yr (%) 7 4 6 3 2 2Recurrence—10-yr (%) 18 9 8 10 8 10
*Extrapolated in part from Figure 2 of article.

SUMMARY
Background Some men with thyroid carcinoma have tran-sient decreases in spermatogenesis after radioiodine (I-131)therapy, but whether long-term fertility is reduced is notknown. In this study the fertility of men with papillary orfollicular thyroid carcinoma treated with varying doses ofI-131 was determined, and radiation doses to the testes andserum follicle-stimulating hormone (FSH) concentrationswere measured serially after I-131 therapy in subgroups ofthe men.
Methods The study subjects were 122 men with thyroidcarcinoma who were less than 40 years old (median, 35;range, 23 to 39) when treated between 1949 and 1997; oldermen were excluded because most had completed their fam-ilies. In 97 men the disease was limited to the thyroid, 22 hadlymph node involvement, and 3 had metastases. All weretreated surgically; 78 men then received 81 mCi (3 GBq)of I-131 to destroy remaining normal thyroid tissue, and 44men received 230 to 1280 mCi (8.5 to 47.3 GBq) of I-131for that purpose and to treat persistent, recurrent, ormetastatic disease.
Information about fertility was obtained from the men atthe time of follow-up visits or by mail. The men were askedif they had all the children they wished to have, and if theyhad not had children whether this was by choice. Theradiation dose to each testis was measured by placement ofa small thermoluminescent detector on the scrotum in 14men. Serum FSH was measured before and at 1, 3, 6, 9, and12 months after I-131 therapy in 14 men.
Results Among the 122 men, 29 had died or were lost tofollow-up (median follow-up period, 21 years; range, 3 to
39). Among the remaining 93 men, 34 (37 percent) had notwished to have children, including three men who initiallywished to have children but changed their minds because ofthe perceived risk of congenital anomalies in any offspring.The remaining 59 men (63 percent) had fathered 106 chil-dren 3.5 to 18 years after I-131 therapy. These 59 menincluded 12 men who received a single 81 mCi (3 GBq) doseof I-131 and had fathered 20 children, 19 men who received>81 to <380 mCi (3 to 14 GBq) and had fathered 36 chil-dren, and 28 men who received 380 to 1190 mCi (14 to 44GBq) and had fathered 50 children. The interval betweenthe last dose and fathering is not stated. None of the chil-dren had any major malformation.
The estimated mean radiation doses to each testis rangedfrom 6.4 cGy (64 rad) in seven men treated once with 81mCi (3 GBq) of I-131 to 21.2 cGy (212 rad) in seven mentreated two or more times with cumulative doses of 150mCi (5.5 GBq) to 250 mCi (9.2 GBq) of I-131.
In seven men given 81 mCi (3 GBq) of I-131, serum FSHconcentrations increased twofold or threefold one monthafter treatment, and returned to base line by 9 months. Inseven other men who received two doses of I-131, serumFSH concentrations increased slightly more after the seconddose than after the first dose, and returned to base line by12 months. Two men had small transient increases in serumluteinizing hormone concentrations after therapy, but nochange in serum testosterone concentrations.
Conclusion I-131 therapy does not reduce fertility in menwith thyroid carcinoma.
54 ● CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3
THYROID CANCER
Fertility is not impaired after radioiodine therapy in men with thyroidcarcinoma
Hyer S, Vini L, O’Connell M, Pratt B, Harmer C. Testicular dose and fertility in men following I131 therapy for thyroidcancer. Clin Endocrinol 2002;56:755-8.
COMMENTARY
The largest previous studies of theeffects of I-131 therapy in men with thy-roid carcinoma contained more detailedhormonal analyses in more men, withsimilar results—a rise and fall in serumFSH concentrations and little change inserum LH and testosterone concentra-tions (1,2). The fact that serum FSHconcentrations rise transiently after singledoses of I-131—and are persistently highin some men after repeated doses (1)—isstrong evidence that I-131 can reducespermatogenesis, although there havebeen no systematic studies of sperm pro-duction in these men. In one study, 11men had fathered children, and single
semen analyses in eight men revealeddecreased numbers of motile sperm (1).
Hyer at al. found that men with thy-roid carcinoma who have been treatedwith I-131 are fertile, but they may notbe normally fertile. No man who wantedto father a child was unable to do so, butthe men apparently were not askedwhether the fathering took longer thanexpected or if they wished to have morechildren. And we do not know what themen had been told about fertility at thetime of treatment, which may well haveinfluenced their later desire not to havechildren. Nonetheless, given the availableinformation, men who are to be treatedwith I-131 can be told that they shouldbe fertile in the long term, unless they
are treated repeatedly, but their fertilitymay be impaired in the first months afterI-131 therapy.
Robert D. Utiger, M.D.
References
1. Pacini F, Gasperi M, Fugazzola L, etal. Testicular function in patients withdifferentiated thyroid carcinoma treatedwith radioiodine. J Nucl Med1994;35:1418-22.
2. Wichers M, Benz E, Palmedo H, et al.Testicular function after radioiodine ther-apy for thyroid carcinoma. Eur J NuclMed 2000;27:503-7.

SUMMARY
Background Some patients with differentiated thyroidcarcinoma have high serum antithyroglobulin antibodyconcentrations not only before but also after surgical andradioiodine therapy, and persistently high values may beassociated with recurrence of carcinoma. This study wasdone to determine the relationship between high serumantithyroglobulin antibody concentrations after initialtreatment and outcome in patients with thyroid carcinoma.
Methods The study subjects were 226 patients with dif-ferentiated thyroid carcinoma treated by surgery andradioiodine who subsequently had no detectable thyroidremnants and serum thyroglobulin concentrations <1ng/mL (independent of their serum thyrotropin concen-trations at that time). Serum antithyroglobulin antibodieswere measured then and during subsequent follow up ineach patient, and the patients were evaluated for recurrenceby imaging procedures or surgery. Serum thyroglobulin wasmeasured by an immunoradiometric assay (sensitivity, <0.8ng/mL; recovery of thyroglobulin, 93 to 133 percent), andserum antithyroglobulin antibodies were measured by aradioimmunoassay (values <100 U/mL were considerednegative). Autoimmune thyroid disease was diagnosed byhistology at initial surgery.
Results The initial serum antithyroglobulin antibody con-centrations were <100 U/mL in 175 patients (77 percent),of whom 6 patients (3 percent) had a recurrence duringfollow-up (duration of follow-up not given) (Table). Serumantithyroglobulin concentrations were ≥100 U/mL in 51patients (23 percent), of whom 25 (49 percent) had a recur-rence after a mean (±SD) disease-free interval of 52±56months, and 26 (51 percent) had no recurrence during a
mean follow-up period of 25±13 months. Among the 31patients who had recurrences, 4 had local recurrences, 21had lymph node metastases, and 6 had lung or bone meta-stases.
In the 51 patients with high serum antithyroglobulin anti-body concentrations, the initial values were higher in the 25patients who had a recurrence than in the 26 patients whodid not (1124±1879 vs. 520±724 U/mL). Fourteen ofthese 25 patients responded to surgical or radioiodine ther-apy; serum antithyroglobulin antibody concentrationsdecreased in 10 and did not change or increased in 4.Serum antithyroglobulin antibody concentrations decreas-ed in 19 of the 26 patients (73 percent) (to values <100U/mL in 12 patients) who did not have a recurrence dur-ing follow-up; the values did not change in 3 patients andincreased progressively in 4 patients.
Conclusion Patients with differentiated thyroid carcino-ma who have high serum antithyroglobulin antibody con-centrations after surgical and radioiodine therapy are morelikely to have recurrent carcinoma than those with low con-centrations.
THYROID CANCER
High serum antithyroglobulin concentrations after initial therapy areassociated with recurrence in patients with thyroid carcinoma
Chung JK, Park YJ, Kim TY, So Y, Kim SK, Park DJ, Less DS, Lee MC, Cho BY. Clinical significance of elevated level ofserum antithyroglobulin antibody in patients with differentiated thyroid cancer after thyroid ablation. Clin Endocrinol2002;57:215-21.
CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3 ● 55
COMMENTARY
Patients were selected for this studyif they had very low serum thyroglobulinconcentrations several years after surgeryand administration of radioiodine forthyroid remnant destruction. The pres-ence of high serum antithyroglobulinantibody concentrations at that time in23 percent of the patients, however,implies that that some thyroglobulin was(or had recently been) present. If so, itwas probably being produced by residualmicroscopic foci of thyroid carcinomacells rather than normal thyroid cells. Ifthis hypothesis is correct, then it is notsurprising that patients with high serum
antithyroglobulin antibody concentrationsare likely to have clinically evident recur-rences at some later time; indeed, it issurprising that the recurrence rate in thisgroup was not higher. And of course itmight be as the patients are followedlonger; note that the patients who didnot have a recurrence were followed foronly about half as long as those who hada recurrence (25 vs. 52 months). Con-versely, in patients with no remaining thy-roid tissue at all, serum antithyroglobulinconcentrations would be expected to below, and of course the recurrence rateshould be low. And it was.
However one may speculate aboutthe pathophysiology of antithyroglobulin
antibody production in patients with thy-roid carcinoma, the practical reality isthat the presence of the antibodies com-plicates follow-up of the patients. Theyinterfere with measurements of serumthyroglobulin, although the extent of theinterference and whether it can be cor-rected for by recovery studies is debated.If they predict recurrence, then patientswith high serum antibody concentrationsmay need closer, and more complicated,follow-up.
Robert D. Utiger, M.D.
Table. Clinical Characteristics of Patients with Thyroid Carcinoma with Low(Negative) and High Serum Antithyroglobulin Antibody Concentrations.
Serum SerumAntithyroglobulin Antithyroglobulin
<100 U/mL (n=175) ≥100 U/mL (n=51)Age (mean [±SD] yr) 44±13 44±13Women/men 158/17 46/5Histology (papillary/follicular) 163/12 51/0Time after radioiodine therapy 3.3±3.7 3.5±4.2
(mean [±SD] yrs)Recurrence 6 (3%) 25 (49%)Autoimmune thyroid disease 14 (8%) 16 (31%)

THYROID FUNCTION IN PREGNANCY
Some women with hyperemesis gravidarum have transient hyperthyroidism
Tan JY, Loh KC, Yeo GS, Chee YC. Transient hyperthyroidism of hyperemesis gravidarum. BJOG 2002;109:683-8.
56 ● CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3
COMMENTARY
The hyperthyroidism that occurs insome women with hyperemesis gravi-darum is true hyperthyroidism. Com-pared with normal pregnant women,their serum free T4 concentrations arehigher and their serum TSH concentra-tions are lower. Their thyroid secretionmust be increased more and the increaselasts longer. The increase in thyroidsecretion in both groups is caused bychorionic gonadotropin, and there is apositive correlation between serum chori-onic gonadotropin concentrations andserum free T4 concentrations in bothnormal pregnant women and women
with hyperemesis gravidarum (1).The hyperthyroidism in these
women is not, however, clinically impor-tant. The women do not have any clinicalmanifestations of hyperthyroidism orthyroid enlargement, presumably becausethe increase in thyroid secretion is smalland transient, and the illness is dominat-ed by the hyperemesis and the attendantabnormalities in serum electrolyte con-centrations. The hyperemesis is probablydue to excess estrogen production causedby the excess production of chorionicgonadotropin. Conversely, pregnantwomen with hyperthyroidism caused byGraves’ disease do have clinical manifes-tations of hyperthyroidism and often thy-
roid enlargement, they have more severebiochemical hyperthyroidism, and theydo not have hyperemesis. It is on thebasis of these differences that these twocauses of gestational hyperthyroidismcan be distinquished.
Robert D. Utiger, M.D.Reference
1. Goodwin TM, Montoro M, MestmanJH, et al. The role of chorionicgonadotropin in transient hyperthy-roidism of hyperemesis gravidarum. JClin Endocrinol Metab 1992;75:1333-7.
SUMMARY
Background Pregnant women have transient increases inthyroid secretion, manifested by a small increase in serumfree thyroxine (T4) concentrations and a small decrease inserum thyrotropin (TSH) concentrations, from approxi-mately 6 to 16 weeks of gestation, caused by the thyroid-stimulating action of chorionic gonadotropin. Thesechanges are exaggerated in women with hyperemesis gravi-darum, sometimes so much so that they may be thought tohave hyperthyroidism caused by Graves’ disease (and toneed antithyroid-drug therapy). This case study was done todefine the clinical and biochemical characteristics andcourse of women with hyperemesis gravidarum who hadhyperthyroidism, and to compare the findings in thesewomen with the findings in pregnant women with Graves’hyperthyroidism.
Methods The study subjects were women with hypereme-sis gravidarum, defined as persistent vomiting beginningbefore 13 weeks of gestation that was so severe that thewoman could not retain solids or liquids and needed to behospitalized for intravenous hydration for more than threedays or on more than one occasion. The women were eval-uated by clinical examination; pelvic ultrasonography (toexclude trophoblastic disease); and measurements of serumTSH, free T4, TSH receptor antibodies, thyroid peroxidaseantibodies, electrolytes, alanine and aspartate aminotrans-ferases, and bilirubin. Many of these tests were done week-ly until normal. Hyperthyroidism was defined as a serumTSH concentration <0.1 mU/L and a serum free T4 con-centration >2.0 ng/dL (26 pmol/L).
Results Among 78 women hospitalized for treatment ofhyperemesis gravidarum, 39 had transient hyperthyroidism.Their mean age was 30 years (range, 19 to 40); the meanduration of gestation was 9 weeks (range, 6 to 13); 35 had
singleton pregnancies and 4 twin pregnancies; and 19 hadone admission, 8 had two admissions, and 12 had three ormore admissions. Twenty-two women (56 percent) had lost>5 percent of their prepregnancy weight. None had clinicalmanifestations of hyperthyroidism or Graves’ disease. Atfirst admission, 26 of the 39 women (67 percent) hadhyponatremia, 23 (59 percent) had hypokalemia, 22 (56 per-cent) had high serum aminotransferase concentrations, and5 (13 percent) had hyperbilirubinemia. None had a highserum concentration of TSH receptor antibodies, and 2 (5percent) a high serum antithyroid peroxidase antibody con-centration.
The peak mean serum free T4 concentration in these 39women was 3.1 ng/dL (40 pmol/L) at 9 weeks of gestation,after which the values fell progressively; all the women hadnormal serum free T4 concentrations by 15 weeks. SerumTSH concentrations increased more slowly, but all thewomen had serum TSH concentrations ≥0.1 mU/L by 19weeks. One woman had a spontaneous abortion at 15weeks; the remainder delivered at term. The infants ofwomen who had lost >5 percent of their prepregnancyweight were slightly smaller than the infants of the womenwho lost less or no weight (2915 vs. 3115 g, P = 0.09). Theratio of female to male infants was 2.6:1.
Five women were thought to have Graves’ hyperthyroidism,based on the presence of persistent tachycardia, goiter, orophthalmopathy, and high serum concentrations of TSHreceptor antibodies or antithyroid peroxidase antibodies.Three of these women were not treated, and improvedspontaneously, and two were treated with propylthiouracil.
Conclusion Some women with hyperemesis gravidarumhave transient hyperthyroidism, which subsides during thesecond trimester, and thereafter their pregnancies and deliv-eries are normal.

CONGENITAL HYPOTHYROIDISM
Discordance of thyroid dysgenesis in monozygotic twins
Perry R, Heinrichs C, Bourdoux P, Khoury K, Szots F, Dussault JH, Vassart G, Van Vliet G. Discordance of monozy-gotic twins for thyroid dysgenesis: implications for screening and for molecular pathophysiology. J Clin EndocrinolMetab 2002;87:4072-7.
SUMMARY
Background Thyroid dysgenesis, in the form of thyroidagenesis, hypoplasia, or ectopy, accounts for approximately85 percent of cases of congenital hypothyroidism in iodine-sufficient regions of the world. The remainder have defectsin thyroid hormone biosynthesis (dyshormonogenesis),which are inherited as autosomal recessive traits. The caus-es of thyroid dysgenesis are not known. A few infants havehad homozygous mutations in the gene for one of the thy-roid transcription factors or the thyrotropin (TSH) receptor,and approximately 2 percent of cases are familial. In thisstudy the concordance of congenital hypothyroidismamong twins was evaluated, and in addition the possibilitythat mixing of blood among twins might alter the results ofscreening for congenital hypothyroidism was studied.
Methods The initial study subjects were monozygotictwins born in Quebec in 2000 who were discordant for con-genital hypothyroidism. The affected twin had only a slight-ly high screening blood TSH concentration (22 mU/L).Eleven days later this infant had a very high serum TSHconcentration (444 mU/L) and a low serum free thyroxine(T4) concentration (0.3 ng/dL [3.4 pmol/L]). The multi-year records of the Quebec, Canada and Brussels, Belgiumscreening programs were searched to identify twins withcongenital hypothyroidism, and the infants’ records werethen reviewed. In addition, pediatric endocrinologists inQuebec and Brussels were surveyed to determine if theyknew of any twins with congenital hypothyroidism missedby the screening programs.
Results During the study interval, the frequency of con-genital hypothyroidism was 1 in 2971 infants in Quebec and1 in 3167 infants in Brussels. Sixteen pairs of twins wereidentified in the two regions, of which five were monozy-gotic twins and 11 were dizygotic twins. All the twin pairs
were discordant for congenital hypothyroidism. The causesof the hypothyroidism were thyroid dysgenesis in one infantin each of five monozygotic pairs and one infant in each ofseven dizygotic pairs, and dyshormonogenesis in one infantin each of four dizygotic pairs. Thyroid ultrasonography,done in the normal twin of four twin pairs, was normal. Themothers of all the infants had normal thyroid function, andthere was only one case of congenital hypothyroidism ineach family. The survey of pediatric endocrinologists didnot reveal any twins missed by the neonatal screening pro-grams.
Exact values for screening blood TSH concentrations andfollow-up serum values at the time of recall were availablefor four infants with congenital hypothyroidism from pairsof monozygotic twins. The results in these four infants and16 singleton infants with congenital hypothyroidismmatched for age at screening and diagnosis and serum TSHvalues at diagnosis suggest that mixing of blood betweenaffected and unaffected twins lowers screening blood TSHvalues in affected twins (65 versus 160 mU/L) (Table).
Conclusion Monozygotic twins are rarely concordant forcongenital hypothyroidism caused by thyroid dysgenesis.Fetal blood mixing may mask congenital hypothyroidism inaffected twins.
CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3 ● 57
COMMENTARY
The success of newborn screeningprograms for congenital hypothyroidismhas not been matched by comparablesuccess in understanding of the causes ofcongenital hypothyroidism. This is partic-ularly true for its most common cause,thyroid dysgenesis. This is an all-purposeterm that encompasses multiple abnor-malities in thyroid development, fromcomplete absence of thyroid tissue (agen-esis), to a decreased amount of thyroidtissue in an abnormal location (ectopia),to an inadequate amount of thyroid tis-
sue in the normal location (hypoplasia).This study does not provide evidence fora major genetic component in the causa-tion of thyroid dysgenesis, but not manytwin pairs were identified. Other evi-dence, however, does support the possi-bility of a genetic contribution. In astudy of 241 first-degree relatives of 84infants with congenital hypothyroidism,21 thyroid developmental abnormalitieswere detected by ultrasonography in 19relatives (8 percent). as compared with 2of 217 subjects (1 percent) from familieswith no thyroid disorder (1). Detailedanalysis of these results suggested that in
some families thyroid dysgenesis is trans-mitted as an autosomal dominant trait. Inthe majority, however, it is an isolatedevent, probably caused by an early somat-ic mutation or an environmental insult..
Robert D. Utiger, M.D.
References
1. Leger J, Marinovic D, Garel C, et al.Thyroid developmental anomalies in firstdegree relatives of children with congeni-tal hypothyroidism. J Clin EndocrinolMetab 2002;87:575-80.
Table. Times of Testing and Blood and Serum TSH Values (Range) of Mono-zygotic Twins with Congenital Hypothyroidism and Matched Singleton Infantswith Congenital Hypothyroidism.
Monozygotic Twins (n=4) Singleton Infants (n=16)Mean age at screening (days) 3 (2-5) 3 (2-5)Blood TSH value at 65 (22-204) 160 (29-499)
screening (mU/L)Age at diagnosis (days) 19 (14-22) 14 (9-23)Serum TSH at 519 (406-985) 532 (368-999)
diagnosis (mU/L)

NONTHYROIDAL ILLNESS
Thyroid abnormalities in recipients of bone marrow transplants are usuallyassociated with chronic graft-versus-host disease
Tauchmanova L, Selleri C, De Rosa G, Pagano L, Orio F, Lombardi G, Rotoli B, Colao A. High prevalence of endocrinedysfunction in long-term survivors after allogeneic bone marrow transplantation for hematologic diseases. Cancer2002;95:1076-84.
SUMMARY
Background Bone marrow transplantation is an effectivetherapy for several hematologic diseases, but has numerouscomplications. They include endocrine dysfunction, causedby the pretransplant conditioning regimen, graft-versus-host disease (GVHD), or immunosuppressive therapy. Inthis study endocrine function was evaluated in a group ofpatients who had received allogeneic bone marrow trans-plants.
Methods The study subjects were 40 patients (21 women,19 men; age at the time of transplantation, 29 years [range,13 to 45]) with hematologic disease who received bone mar-row-derived stem cells from HLA-identical siblings andwho were disease-free one or more years after transplanta-tion. Twenty-two patients had acute leukemia, 16 hadchronic leukemia, and 2 had aplastic anemia. The pretrans-plant conditioning regimen consisted of busulfan andcyclophosphamide (no patient received radiation).Cyclosporine and methotrexate were given as prophylaxisagainst acute GVHD. Acute GVHD was treated with highdoses of glucocorticoids, and chronic GVHD with highdoses of glucocorticoids and cyclosporine. Thirteenpatients (32 percent) had acute GVHD, and 26 patients (65percent) had chronic GVHD. The median duration of fol-low-up was 38 months (range, 12 to 62).
Results Pituitary-Thyroid Function Twenty patientswere known to have normal thyroid function before trans-plantation. After transplantation, 20 patients were studiedonce and 20 on several occasions. Twelve patients (30 per-cent) had some abnormality in thyroid function. Fourpatients with chronic GVHD 12 to 48 months after trans-plantation had low serum free triiodothyronine concentra-tions and normal serum free thyroxine and thyrotropin(TSH) concentrations, findings considered to be caused bytheir nonthyroidal illness. Six patients had subclinical hyper-thyroidism when first studied 12 to 18 months after trans-plantation; the three patients studied again 4 to 7 monthslater had normal serum TSH concentrations. Two patients
had subclinical hypothyroidism 5 and 6 years after trans-plantation. Four of the patients with subclinical hyperthy-roidism and both patients with subclinical hypothyroidismhad chronic GVHD. One patient had a thyroid lymphoma8 months after transplantation.
Pituitary-Gonadal Function Among the 21 women, 20(95 percent) had amenorrhea, and 1 (5 percent) polymenor-rhea. All had high serum follicle-stimulating hormone(FSH) and luteinizing hormone (LH) concentrations, lowserum estradiol concentrations, and normal serum prolactinconcentrations. Two women recovered; the others wereconsidered to have permanent primary hypogonadism. The19 men had normal serum LH and testosterone concentra-tions, but 9 (47 percent) men had high serum FSH concen-trations; all 3 men who were tested had azoospermia.
Pituitary-Adrenal Function All 40 patients received glu-cocorticoid therapy; the median dose was 10 g/m2 of pred-nisone or its equivalent (range, 0.9 to 24), and the medianduration of therapy was 9 months (range, 3 to 36). Fourpatients (10 percent) had secondary adrenal insufficiencywhen studied 10 to 30 days after the cessation of glucocor-ticoid therapy; all had normal adrenal function 6 to 18months later. The other 36 patients (90 percent) had normaladrenal function when studied 30 to 180 days after the ces-sation of glucocorticoid therapy.
Growth Hormone-Insulin-Like Growth Factor I Allpatients had normal serum growth hormone concentra-tions, measured in six samples collected at 20-minute inter-vals for two hours. Serum insulin-like growth factor I con-centrations were lower than in age-matched normal subjectsin 10 of the 26 patients (38 percent) with chronic GHVD,but only 1 of the 14 other patients (7 percent).
Conclusion Among patients with hematologic diseasestreated with allogeneic bone marrow transplantation,endocrine dysfunction is common, especially in patientswith chronic GVHD.
58 ● CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3
COMMENTARY
Endocrine dysfunction was mostcommonly found in the patients withGVHD, but were the abnormalitiescaused by the GVHD or by the highdoses of glucocorticoids or otherimmunosuppressive drugs given to treatGVHD?
Acute or chronic GVHD alone
would be expected to cause the samechanges in thyroid function as any otherillness, namely low serum free triiodothy-ronine concentrations alone, low serumTSH concentrations alone (transient sub-clinical hyperthyroidism), or both. Highdoses of glucocorticoids have similareffects. GVHD alone might also causethyroid dysfunction, if the donor cellsrecognized recipient thyroid cells as non-
self, causing thyroid inflammation.
Robert D. Utiger, M.D.

COMMENTARY
DITPA increased cardiac output,presumably by improving diastolic func-tion and decreasing peripheral vascularresistance, in patients with congestiveheart failure. Its prolonged administra-tion would be expected to result inimprovement in symptoms and function-al class, if the increase were sustainedand no harmful chronotropic effects
occurred. The authors suggest that it didnot increase myocardial oxygen con-sumption, because the product of theheart rate times the mean arterial pres-sure did not increase. However, DITPAcan hardly be said to have specific car-diac effects; it inhibited TSH secretionand lowered serum lipid concentrations.The search for cardiac-specific and otherorgan-specific thyroid hormone analogswill continue, now spurred by recogni-
tion that there are several nuclear recep-tors for thyroid hormone with differenttissue distributions.
Robert D. Utiger, M.D.
NONTHYROIDAL ILLNESS
3,5-Diiodothyropropionic acid has favorable short-term effects on cardiachemodynamics in patients with congestive heart failure
Morkin E, Pennock G, Spooner PH, Bahl JJ, Underhill Fox K, Goldman S. Pilot studies on the use of 3,5-diiodothyro-propionic acid, a thyroid hormone analog, in the treatment of congestive heart failure. Cardiology 2002;97:218-225.
SUMMARY
Background Patients with congestive heart failure oftenhave low serum triiodothyronine (T3) concentrations, whichmay contribute to their decreased cardiac contractility andincreased peripheral resistance. Thyroid hormones increasecardiac contractility and decrease peripheral resistance, buthave many other actions; these actions may to some extentbe dissociated in some thyroid hormone analogs. This studyevaluated the effects of 3,5-diiodothyropropionic acid(DITPA), a thyroid hormone analog that in animals has rel-atively greater inotropic than chronotropic and metaboliceffects, in normal subjects and patients with congestiveheart failure.
Methods The study subjects were seven normal men (agerange, 18 to 65 years) and 21 patients with congestive heartfailure (numbers of women and men not given; age range,47 to 67 years). All the patients had symptoms of heart fail-ure, sinus rhythm, a cardiac ejection fraction <35 percent,and a New York Heart Association functional class of II orIII; 20 patients had ischemic cardiomyopathy and 1 patienthad dilated cardiomyopathy. They could be taking digoxin,an angiotensin-converting enzyme inhibitor, and a diuretic,but not a β-adrenergic antagonist.
The normal subjects were given 1.875 mg/kg of DITPA intwo divided doses daily for two weeks and then 3.75 mg/kgdaily for two weeks. The patients with heart failure wererandomly assigned to receive 1.875 mg/kg of DITPA individed doses daily for two weeks and then 3.75 mg/kg dailyfor two weeks, or placebo. Body weight, heart rate, bloodpressure, and serum thyroxine (T4) and thyrotropin (TSH)were measured before and at the end of each treatmentperiod. Serum T3 was not measured at base line in thepatients with heart failure, and it was not measured duringDITPA treatment because it cross-reacted in the T3 assay.The patients underwent cardiac catheterization, echocardio-graphy, and measurements of ejection fraction by radio-nuclide imaging at base line and four weeks.
Results Normal Subjects There were no changes inweight, heart rate, or blood pressure after administration ofDITPA for two and four weeks. The mean serum TSH con-centration fell from 3.5 mU/L to 0.4 mU/L at four weeks;the mean serum T4 concentrations at these times were 8.7µg/dL (112 nmol/L) and 5.9 µg/dL (76 nmol/L), respec-tively, but the mean serum free T4 concentration did notchange.
Patients with Congestive Heart Failure Nineteenpatients completed the study, 9 in the DITPA-treatmentgroup and 10 in the placebo group. At base line, the DITPAand placebo groups were similar, except that the mean ejec-tion fraction was lower in the DITPA group (18 vs. 29 per-cent). During treatment, there were no changes in weight,heart rate, or blood pressure in either group. The meanserum TSH concentration decreased from 2.5 mU/L to0.02 mU/L in the DITPA-treatment group, but the meanserum free T4 concentration did not change; there were nochanges in either hormone in the placebo group. The meanserum low-density-lipoprotein cholesterol and triglycerideconcentrations decreased in the DITPA-treatment group,but did not change in the placebo group.
There were no changes in functional class, ejection fraction,and echocardiographic measurements (fractional shorten-ing, velocity of circumferential fiber shortening, and ratio ofearly to late diastolic filling) in either group, except for adecrease in the velocity of circumferential fiber shorteningin the DITPA-treatment group. Similarly, there were nochanges in pulmonary artery, right atrial, or mean arterialpressure in either group. The mean cardiac index increasedby 17 percent (P = 0.04) and the mean systemic vascularresistance index decreased by approximately 15 percent(extrapolated from Figure 2, P = 0.02) in the DITPA-treat-ment group; these measurements did not change in theplacebo group.
Conclusion The thyroid hormone analog DITPA increas-es cardiac output and decreases peripheral vascular resist-ance in patients with congestive heart failure.
CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3 ● 59

IODINE METABOLISM
Recurrence of mild iodine deficiency in Tasmania
Guttikonda K, Burgess JR, Hynes K, Boyages S, Byth K, Parameswaran V. Recurrent iodine deficiency in Tasmania,Australia: a salutary lesson in sustainable iodine prophylaxis and its monitoring. J Clin Endocrinol Metab 2002;87:2809-15.
SUMMARY
Background Endemic goiter was common in Tasmaniabefore 1950. Iodine supplementation began that year withthe distribution of potassium iodide tablets to schoolchild-ren. In 1966 this was replaced by the addition of potassiumiodate to bread. During the 1960s the presence of iodine inmilk, due to the use of iodine-containing disinfectants indairy cattle, led to a further increase in iodine intake. A max-imum (but no minimum) limit was then mandated foriodine content in milk, and addition of potassium iodate tobread was discontinued. From the late 1960s to the mid-1980s, iodine intake was considered adequate, based onmeasurements of urinary iodine. Monitoring of the iodinecontent of milk lapsed in the late 1980s. By the 1990s, asdairy-farming practices changed, some children had urinaryiodine values <50 µg/L, indicative of moderate dietaryiodine deficiency. This study was undertaken to evaluatecontemporary iodine nutrition in Tasmania 50 years afteriodine supplementation was introduced.
Methods The study subjects were 225 children (99 girls,126 boys; mean age, 11 years [range, 4 to 17]). Morningurine samples were collected for the measurement ofiodine, and thyroid volume was measured by ultrasonogra-phy. Thyroid volume, corrected for age and body surfacearea, was classified as normal or increased according touncorrected and corrected standards of the World Health
Organization/International Council for the Control ofIodine Deficiency Disorders (WHO/ICCIDD).
Results The median urinary iodine excretion in the 225children was 84 µg/L (interquartile range, 57 to 110); 20percent of the children had values of 50 µg/L or lower,indicative of moderate iodine deficiency. The median valueswere similar in girls and boys (81 vs. 84 µg/L). There wassome regional variation within the state, but not among chil-dren of differing socioeconomic status.
The prevalence of thyroid enlargement in the girls was 3.5percent based on age and on body-surface area in relation tothe uncorrected WHO/ICCIDD standards, and it was 21percent based on age and body-surface area in relation tothe corrected standards. For the boys, the prevalence of thy-roid enlargement was 5 percent based on age and 6 percentbased on body-surface area in relation to the uncorrectedstandards, and 25 percent based on age and 22 percentbased on body-surface area in relation to the corrected stan-dards. There were no differences in thyroid volume in thegirls and boys, or among children living in different areas ofthe state or having different socioeconomic status.
Conclusion Among school children in Tasmania, the val-ues for urinary iodine excretion and the percentages withthyroid enlargement indicate the recurrence of mild iodinedeficiency.
60 ● CLINICAL THYROIDOLOGY ● VOLUME XIV ● ISSUE 3
COMMENTARY
The standard measures of iodinenutrition are the presence or absence ofgoiter, preferably determined by ultra-sonography, and urinary iodine excretion.In many studies around the world themeasurements of thyroid volume werecompared with those of iodine-sufficientEuropeans, but there has been increasingrecognition that the values are lower iniodine-sufficient people living elsewhere,due at least in part to differences in bodysize. A correction factor has been intro-duced to adjust for these differences.Correction of values nearly always leadsto an increase in the frequency of goiter,as in this study. Urinary iodine excretionclosely reflects iodine intake, but can varyfrom day to day.
The history of the ups and downsof iodine supplementation in Tasmaniaprovides important lessons on the factorsthat can affect iodine intake in different
populations, and these lessons areundoubtedly applicable to other coun-tries. In Tasmania, the introduction ofiodine-containing disinfectants in thedairy industry and the subsequent reduc-tion in the use of these products hadmajor impacts on iodine nutrition.
The same thing has happened in theUnited States. In 1971-1974, the medianurinary iodine excretion was 320 µg/L,whereas in 1988-1994 it was 145 µg/L(1). And at the latter time urinary iodineexcretion was <50 µg/L in 12 percent ofthe population, including 15 percent ofpregnant women. The causes of thismarked decrease in urinary iodine excre-tion include decreased use of salt, includ-ing iodized salt, in home cooking;decreased use of iodized salt in manufac-tured foods and restaurants; cessation ofuse of potassium iodate in the bakingindustry; and decreased use of iodine-containing animal feeds and iodine-con-taining disinfectants in animals.
The important point is that changesin iodine intake can be caused by changesin farming or food industry practices thathave little to do with iodine nutrition inhumans, as well by variations in the con-tent of iodine occurring naturally in foodand water. Iodine deficiency should neverbe considered to be permanently elimi-nated, and iodine intake should be con-tinually monitored in all countries.
Robert D. Utiger, M.D.
References
1. Hollowell JG, Staehling NW, HannonWH, et al. Iodine nutrition in the UnitedStates. Trends and public health implica-tions: iodine excretion data from Nation-al Health and Nutrition ExaminationSurveys I and III (1971-1974 and 1988-1994). J Clin Endocrinol Metab 1998;83:3401-8.

Thyroid Review Articles
Klein RZ, Mitchell ML. Maternal hypothyroidism and cognitive development ofthe offspring. Curr Opin Pediatr 2002;14:443-6.
Langton JE, Brent GA. Nonthyroidal illness syndrome: evaluation of thyroid function insick patients. Endocrinol Metab Clin North Am 2002;31:159-72.
Malik R, Hodgson H. The relationship between the thyroid gland and the liver. Q J Med 2002;95:559-69.
Stagnaro-Green A. Postpartum thyroiditis. J Clin Endocrinol Metab 2002;87:4042-7.

CL
INIC
AL
TH
YR
OID
OL
OG
YAmerican Thyroid AssociationP.O. Box 1836Falls Church, VA 22041
CLINICAL THYROIDOLOGY
is supported by an unrestricted educational grant fromMONARCH PARMACEUTICALS, a wholly owned subsidiary of KING PHARMACEUTICALS, INC.Bristol, Tennessee
NONPROFIT ORG.US POSTAGE
PAIDALBANY NYPERMIT #164
Special Symposium—February 28, 2003
Public Health Strategies for Protecting the Thyroid withPotassium Iodide in the Event of a Nuclear Incident
A symposium of the American Thyroid AssociationCME sponsored by the Johns Hopkins University in conjunction with
the American Thyroid Association
Supported by the American Thyroid Association andthe American Association of Clinical Endocrinologists
Hyatt Regency Washington on Capitol HillWashington, DC
To register online:http://www.hopkinsmedicine.org/cme/events/PubHlthThyroid.html
For registration information:telephone: 410-955-2959
fax: 410-955-0807e-mail: [email protected]