Embed Size (px)
Citation preview
Home Study JANUARY 2004, VOL 79, NO 1
Home Study Program Assertiveness training
t o prevent verbal abuse in the OR he article “Assertiveness training to prevent verbal abuse in the OR” is the basis for this AORN Journal independent study. The behavioral objectives and examination for this program were prepared by Rebecca Holm, RN, MSN, CNOR, clinical editor, with consultation from Susan Bakewell, RN, T MS, education program professional, Center for Perioperative Education.
Participants receive feedback on incorrect answers. Each applicant who suc- cessfully completes this study will receive a certificate of completion. The deadline for submitting this study is Jan 31,2007.
Complete the examination answer sheet and learner evaluation found on pages 169-170 and mail with appropriate fee to
AORN Customer Service c/o Home Study Program
2170 S Parker Rd, Suite 300 Denver, CO 80231-5711
or fax the information with a credit card number to (303) 750-3212.
You also may access this Home Study via AORN Online at www.aorn.org/journal/homestudy/default. htm.
BEHAVIORAL OBJEUIVES After reading and studying the article on assertiveness training to prevent
verbal abuse in the OR, the nurse will be able to
1. identify the dimensions of verbal abuse,
2. explain how episodes of abuse have evolved historically in the perioperative setting,
3. describe the effects of verbal abuse, and
4. discuss interventions that can be used to prevent and manage verbal abuse.
This
progmm meets criterio for CNOR and CRNFA recertification 0s well 0s other continuing education requirements.
A minimum score of 70% on the multiple- choice exominotion is necessary to earn 3 con- tact hours for this inde- pendent study.
Purpose/Goak To educote periopemtive nurses about the effeck of verbol obuse ond how to implement on assertiveness self-leorning module to prevent future episodes of verbol obuse.
147 AORN JOURNAL
JANUARY 2004, VOL 79, NO 1 Buback
Home Study Program Assertiveness training
t o prevent verbal abuse in t h e OR
Debra Buback, RN
erbal abuse is a common form of workplace violence in today’s V health care environment. Of 461
nurses surveyed in 1999,94% had expe- rienced some form of verbal abuse.’
DIMENSIONS OF VERBAL ABUSE The term verbal ubuse frequently is
defined as communication perceived by a person to be a harsh, condemnato- ry attack, either professional or person- al (Table 1). It may be conveyed with tone, manner, or nonverbal cues.2 Abuse in the health care arena consists of two dimensions, horizontal and ver- tical abuse. Horizontal abuse is abuse directed between two equally ranked coworkers, such as between two nurs- es. Vertical abuse is use of inappropri- ate power toward an actual or per- ceived subordinate. Vertical abuse
ABSTRACT THE HIGH INCIDENCE OF VERBAL ABUSE
directed toward perioperative nurses by surgeons has been the subject of recent research studies.
REPEATED INCIDENTS of verbal abuse in the OR contribute to increased incidence of errors, low morale, and high turnover among nursing staff members.
ASSERTIVENESS TRAINING that focuses on conflict resolution and communication skills is an effective method of coping with verbal abuse.
EACH MEMBER is a vital part of the perioper- ative team. Any disruption to the team, including verbal abuse, can compromise patient safety. Collaboration among team members is critical to ensure safe patient outcomes. A O W ] 79 (January 2004) 148-164.
occurs when a surgeon directs abuse toward a nurse. A nurse directing abuse toward a subordinate nurse or coworker (eg, scrub technician) or directing inappropriate behavior toward a patient also are examples of vertical abuse. Vertical abuse directed from the surgeon toward a nurse usu- ally is done in the presence of others. Vertical abuse between two nurses, on the other hand, usually occurs in a pri- vate area.
A recent study conducted in Veteran’s Health Administration hospi- tals noted that more than 50% of the physicians were unaware of the effects verbal abuse had on n ~ r s e s . ~ Other recent studies have shown a high inci- dence of verbal abuse directed at peri- operative nurses by surgeon^.'^
HISTORICAL PERSPECTIVE The perioperative setting can be very
stressful. A surgical team consists of the anesthesia care provider, the surgeon, an RN first assistant (RNFA) or a resi- dent physician, a scrub person, and a circulating nurse. With the exception of the anesthesia care provider and the cir- culating nurse, team members must remain within the sterile area and, therefore, are unable to leave when ver- bal abuse occurs. The anesthesia care provider continuously monitors the patient during the procedure and is required to be in the OR during the entire procedure. Although the circulat- ing nurse may leave the OR to retrieve supplies or medications, he or she must return quickly, and therefore, is almost as vulnerable to abuse as team members confined to the sterile area. The victims of abuse must stay and listen to the abu- sive comments until someone can pro- vide relief. If relief can be obtained at
148 AORN JOURNAL
JANUARY 2004, VOL 79, NO 1 Buback
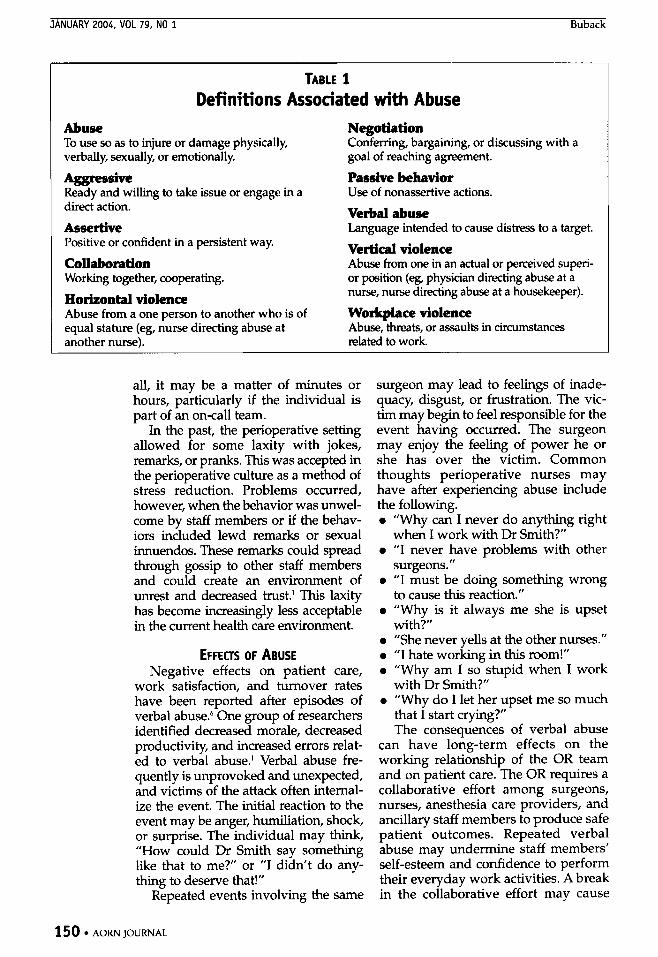
TABLE 1 Definitions Associated with Abuse
Abuse To use so as to injure or damage physically, verbally, sexually, or emotionally.
Aggressive Ready and willing to take issue or engage in a direct action.
Assertive Positive or confident in a persistent way.
Collaboration Working together, cooperating.
Horizontal violence Abuse from a one person to another who is of equal stature (eg, nurse directing abuse at another nurse).
Negotiation Conferring, bargaining, or discussing with a goal of reaching agreement.
Passive behavior Use of nonassertive actions.
Verbal abuse Language intended to cause distress to a target.
Vertical violence Abuse from one in an actual or perceived superi- or position (eg, physician directing abuse at a nurse, nurse directing abuse at a housekeeper).
Workplace violence Abuse, threats, or assaults in circumstances related to work.
all, it may be a matter of minutes or hours, particularly if the individual is part of an on-call team.
In the past, the perioperative setting allowed for some laxity with jokes, remarks, or pranks. This was accepted in the perioperative culture as a method of stress reduction. Problems occurred, however, when the behavior was unwel- come by staff members or if the behav- iors included lewd remarks or sexual innuendos. These remarks could spread through gossip to other staff members and could create an environment of unrest and decreased trust.’ This laxity has become increasingly less acceptable in the current health care environment.
EFFECTS OF ABUSE Negative effects on patient care,
work satisfaction, and turnover rates have been reported after episodes of verbal abuse: One group of researchers identified decreased morale, decreased productivity, and increased errors relat- ed to verbal abuse.’ Verbal abuse fre- quently is unprovoked and unexpected, and victims of the attack often intemal- ize the event. The initial reaction to the event may be anger, humiliation, shock, or surprise. The individual may think, ”How could Dr Smith say something like that to me?” or ”I didn’t do any- thing to deserve that!”
Repeated events involving the same
surgeon may lead to feelings of inade- quacy, disgust, or frustration. The vic- tim may begin to feel responsible for the event having occurred. The surgeon may enjoy the feeling of power he or she has over the victim. Common thoughts perioperative nurses may have after experiencing abuse include the following. 0 “Why can I never do anything right
0 “I never have problems with other
0 “I must be doing something wrong
0 “Why is it always me she is upset
0 “She never yells at the other nurses.” 0 “I hate working in this room!” 0 “Why am I so stupid when I work
with Dr Smith?” 0 “Why do I let her upset me so much
that I start crying?” The consequences of verbal abuse
can have long-term effects on the working relationship of the OR team and on patient care. The OR requires a collaborative effort among surgeons, nurses, anesthesia care providers, and ancillary staff members to produce safe patient outcomes. Repeated verbal abuse may undermine staff members’ self-esteem and confidence to perform their everyday work activities. A break in the collaborative effort may cause
when I work with Dr Smith?”
surgeons.”
to cause this reaction.”
with?“
150 AORN JOURNAL

other team members to feel they are taking on part of the victim's responsi- bilities. The victim may not care if the OR is prepared correctly for a sur- geon's procedure. The morale of the entire team may be affected. Decreased morale and productivity may con- tribute to errors caused in the OR.' Decreased morale ultimately may result in increased staff turnover rates. The remaining staff members may find themselves working longer hours and taking more on-call assignments. This contributes to decreased morale and job satisfaction.
A high turnover rate during the cur- rent nursing shortage can be costly. A cost-benefit analysis revealed an estimate of $64,900 per year was related to verbal abuse? For example, a portion of the cost of verbal abuse that results in the need to replace one nurse has been estimated at approximately $16,000.R An inexperi- enced nurse requires a lengthy orienta- tion, usually from six weeks to nine months, depending on the institution size and number of specialties involved.
An experienced nurse acts as a pre- ceptor for the novice perioperative nurse for a minimum of two weeks in each specialty before the novice nurse begins to work independently. The novice nurse requires a minimum of six weeks before he or she is able to func- tion independently of the preceptor and another six weeks before he or she can be assigned to the on-call team for emergency surgeries. The initial invest- ment by the institution is a minimum of three months before the novice is able to function as a staff nurse in the perioper- ative setting. It is important, therefore, to prevent verbal abuse to limit the cost of recruiting and retention.
PROACTIVE APPROACH Health care facilities should take a
proactive approach to dealing with ver- bal abuse. Key to prevention and man-
agement of verbal abuse is recognition of verbal abuse warning signs and doc- umentation and reporting of incidences of verbal abuse? One researcher recom- mends that institutions develop poli- cies and procedures to handle verbal abuse, such as having staff nurses attend a training session immediately after an incident has occurred and peri- odically thereafter, and tracking trends in verbal abuse.'O Ideally, the offender also should participate in the training, although policies- vary among hospitals.
One group of research- ers found that assertive- ness training and commu- nication skills training were effective in coping with verbal abuse.' Another group of re- searchers recommended early intervention, such as counseling or attending formal education pro- grams." One group of researchers noted that education and collabora- tion were paramount in reducing incidences of verbal abuse.' The Occupational Safety and Health Administration
Collaboration and education, such as work- place violence
prevention programs are paramount to
reducing verbal abuse.
recommends establishment of workplace violence prevention programs that include 0 written programs with clearly stated
0 a workplace risk analysis, 0 hazard prevention and control
practices, and 0 training and education for all
employees.' Collaboration among all team mem-
bers in the perioperative setting is nec- essary to ensure quality patient care. Perioperative team members can be compared to the components of the engine of a car. Every part of the engine,
goals and objectives,
AORN JOURNAL 153
JANUARY 2004, VOL 79, NO 1 Buback
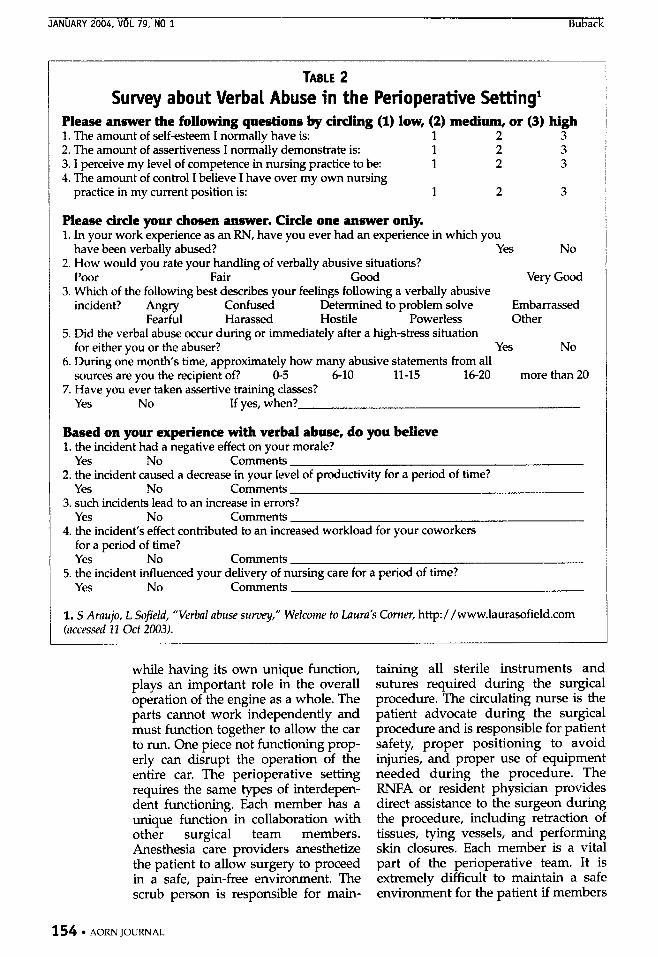
TABLE 2 Survey about Verbal Abuse in the Perioperative Setting’
Please answer the following questions by circling (1) low, (2) medium, or (3) high 1. The amount of self-esteem I normally have is: 1 2 3 2. The amount of assertiveness I normally demonstrate is: 1 2 3 3. I perceive my level of competence in nursing practice to be: 1 2 3
practice in my current position is: 3 2 3 4. The amount of control I believe I have over my own nursing
Please circle your chosen answer. Circle one answer only. 1. In your work experience as an RN, have you ever had an experience in which you
2. How would you rate your handling of verbally abusive situations?
3. Which of the following best describes your feelings following a verbally abusive
have been verbally abused? Yes No
Poor Fair Good Very Good
incident? Angry confused Determined to problem solve Embarrassed Fearful Harassed Hostile Powerless Other
5. Did the verbal abuse occur during or immediately after a high-stress situation for either you or the abuser? Yes No
6. During one month’s time, approximately how many abusive statements from all sources are you the recipient of? 0-5 6-10 11-15 16-20 more than 20
7. Have you ever taken assertive training classes? Yes No If yes, when?
Based on your experience with verbal abuse, do you believe 1. the incident had a negative effect on your morale?
Yes No Comments 2. the incident caused a decrease in your level of productivity for a period of time?
Yes No Comments 3. such incidents lead to an increase in errors?
Yes No Comments 4. the incident’s effect contributed to an increased workload for your coworkers
for a period of time? Yes No Comments
YeS No Comments 5. the incident influenced your delivery of nursing care for a period of time?
1. S Araujo, L Sojield, “Verbal abuse survey,” Welcome to Laura2 Corner, http:/ /www.laurasofield.com (accessed II Oct 2003).
while having its own unique function, plays an important role in the overall operation of the engine as a whole. The parts cannot work independently and must function together to allow the car to run. One piece not functioning prop- erly can disrupt the operation of the entire car. The perioperative setting requires the same types of interdepen- dent functioning. Each member has a unique function in collaboration with other surgical team members. Anesthesia care providers anesthetize the patient to allow surgery to proceed in a safe, pain-free environment. The scrub person is responsible for main-
taining all sterile instruments and sutures required during the surgical procedure. The circulating nurse is the patient advocate during the surgical procedure and is responsible for patient safety, proper positioning to avoid injuries, and proper use of equipment needed during the procedure. The RNFA or resident physician provides direct assistance to the surgeon during the procedure, including retraction of tissues, tying vessels, and performing skin closures. Each member is a vital part of the perioperative team. It is extremely difficult to maintain a safe environment for the patient if members
154 AORN JOURNAL
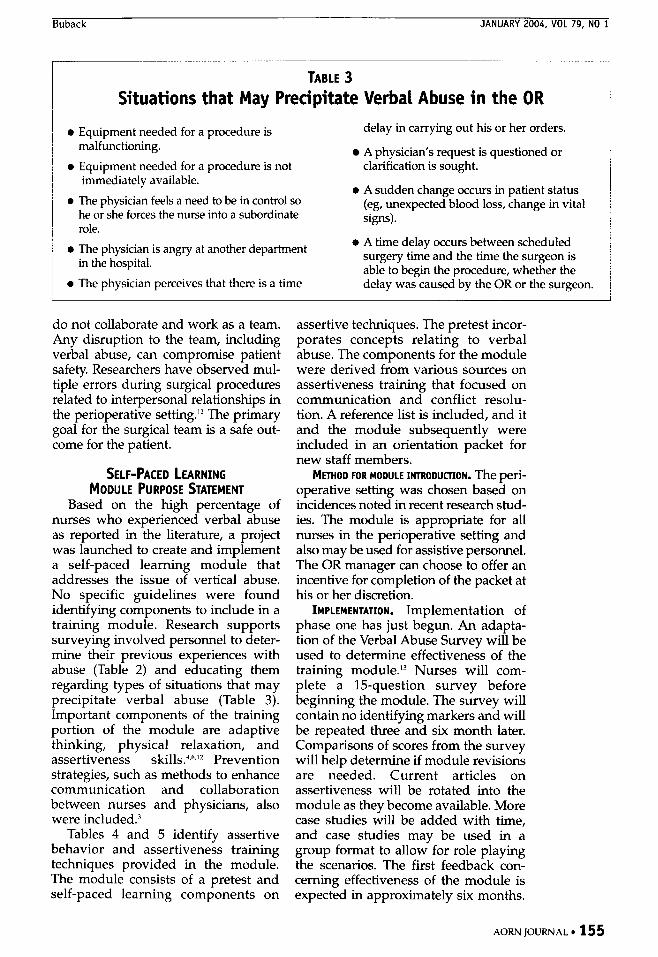
TABLE 3 Situations that May Precipitate Verbal Abuse in the OR
0 Equipment needed for a procedure is
0 Equipment needed for a procedure is not malfunctioning.
delay in carrying out his or her orders.
A physician’s request is questioned or clarification is sought.
immediately available. 0 The physician feels a need to be in control so
he or she forces the nurse into a subordinate role.
0 A sudden change occurs in patient status (eg, unexpected blood loss, change in vital signs).
0 A time delay occurs between scheduled 0 The physician is angry at another department surgery time and the time the surgeon is
able to begin the procedure, whether the in the hospital. 0 The physician perceives that there is a time delay wascaused by the OR or the surgeon.
do not collaborate and work as a team. Any disruption to the team, including verbal abuse, can compromise patient safety. Researchers have observed mul- tiple errors during surgical procedures related to interpersonal relationships in the perioperative setting.’* The primary goal for the surgical team is a safe out- come for the patient.
SELF-PACED LEARNING MODULE PURPOSE STATEMENT
Based on the high percentage of nurses who experienced verbal abuse as reported in the literature, a project was launched to create and implement a self-paced learning module that addresses the issue of vertical abuse. No specific guidelines were found identifying components to include in a training module. Research supports surveying involved personnel to deter- mine their previous experiences with abuse (Table 2) and educating them regarding types of situations that may precipitate verbal abuse (Table 3). Important components of the training portion of the module are adaptive thinking, physical relaxation, and assertiveness skills.‘.”l2 Prevention strategies, such as methods to enhance communication and collaboration between nurses and physicians, also were incl~ded.~
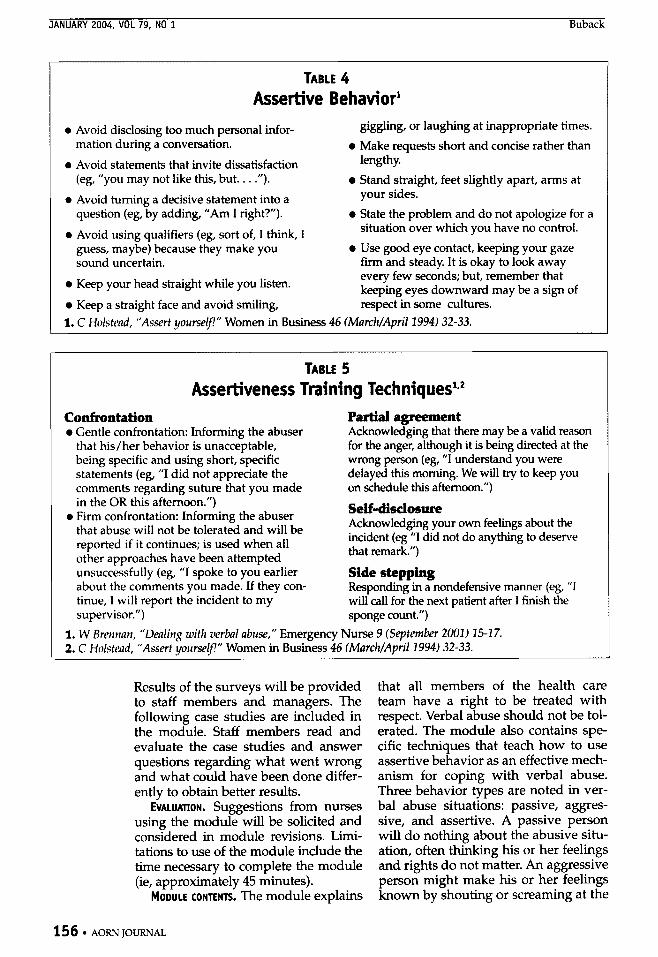
Tables 4 and 5 identify assertive behavior and assertiveness training techniques provided in the module. The module consists of a pretest and self-paced learning components on
assertive techniques. The pretest incor- porates concepts relating to verbal abuse. The components for the module were derived from various sources on assertiveness training that focused on communication and conflict resolu- tion. A reference list is included, and it and the module subsequently were included in an orientation packet for new staff members.
operative setting was chosen based on incidences noted in recent research stud- ies. The module is appropriate for all nurses in the perioperative setting and also may be used for assistive personnel. The OR manager can choose to offer an incentive for completion of the packet at his or her discretion.
IMPLEMENTATION. Implementation of phase one has just begun. An adapta- tion of the Verbal Abuse Survey will be used to determine effectiveness of the training module.I3 Nurses will com- plete a 15-question survey before beginning the module. The survey will contain no identifying markers and will be repeated three and six month later. Comparisons of scores from the survey will help determine if module revisions are needed. Current articles on assertiveness will be rotated into the module as they become available. More case studies will be added with time, and case studies may be used in a group format to allow for role playing the scenarios. The first feedback con- cerning effectiveness of the module is expected in approximately six months.
M ~ O D FOR MODULE INTRODUCTION. The peri-
AORN JOURNAL 15 5
JANUARY 2004, VOL 79, NO 1 Buback
TABLE 4 Assertive Behavior’
0 Avoid disclosing too much personal infor- mation during a conversation.
0 Avoid statements that invite dissatisfaction (eg, “you may not like this, but. . . .”).
0 Avoid turning a decisive statement into a question (eg, by adding, ”Am I right?”).
0 Avoid using qualifiers (eg, sort of, I think, I guess, maybe) because they make you sound uncertain.
0 Keep your head straight while you listen.
0 Keep a straight face and avoid smiling,
giggling, or laughing at inappropriate times. 0 Make requests short and concise rather than
lengthy. Stand straight, feet slightly apart, arms at your sides.
0 State the problem and do not apologize for a situation over which you have no control.
0 Use good eye contact, keeping your gaze firm and steady. It is okay to look away every few seconds; but, remember that keeping eyes downward may be a sign of respect in some cultures.
1. C Holstead, “Assert yourse!f!” Women in Business 46 (MarchlApril2994) 32-33.
TABLE 5 Assertiveness Training
Confrontation Partial agreement 0 Gentle confrontation: Informing the abuser Acknowledging that there may be a valid reason
for the anger, although it is being directed at the wrong person (eg, ’‘I understand you were delayed this morning. We will try to keep you on schedule this afternoon.”)
that his/her behavior is unacceptable, being specific and using short, specific statements (eg, ’‘I did not appreciate the comments regarding suture that you made
Self-disclosure Acknowledging your own feelings about the incident (eg “I did not do anything to deserve that remark.”)
in the OR this afternoon.”) 0 Firm confrontation: Informing the abuser
that abuse will not be tolerated and will be reported if it continues; is used when all other approaches have been attempted unsuccissfully (eg, ”I spoke to you earlier about the comments you made. If they con- tinue, I will report the incident to my supervisor.”) sponge count.”)
Side stepping Responding in a nondefensive manner (eg, ”I will call for the next patient after I finish the
1. W Brennan, “Denling with verbal abuse,” Emergency Nurse 9 (September 2002) 25-27. 2. C Holstead, “Assert yoursev’” Women in Business 46 fMarchlApril2994) 32-33.
Results of the surveys will be provided to staff members and managers. The following case studies are included in the module. Staff members read and evaluate the case studies and answer questions regarding what went wrong and what could have been done differ- ently to obtain better results.
EVALUATION. Suggestions from nurses using the module will be solicited and considered in module revisions. Limi- tations to use of the module include the time necessary to complete the module (ie, approximately 45 minutes).
MOOULE CONTENTS. The module explains
that all members of the health care team have a right to be treated with respect. Verbal abuse should not be tol- erated. The module also contains spe- cific techniques that teach how to use assertive behavior as an effective mech- anism for coping with verbal abuse. Three behavior types are noted in ver- bal abuse situations: passive, aggres- sive, and assertive. A passive person will do nothing about the abusive situ- ation, often thinking his or her feelings and rights do not matter. An aggressive person might make his or her feelings known by shouting or screaming at the
15 6 AORN JOURNAL
other person. This behavior might mimic the abuser's behavior. An assertive person makes his or her feel- ings known but remains in control of the situation.
Self-assertion is presented in the module as a method of learning about one's own limitations and strengths. Assertion develops power and control. Increasing personal security helps indi- viduals deal with anger. One researcher
notes seven steps to be- coming self-assirtive. The Self-assertion is individual should 0 acknowledge that the
situation made him or a method of her angry;I4 learning about 0 identifv his or her feel-
one's own 1 imitations
ings about the situa- tion, which reduces the power that the feelings have over the him or her;
and 0 develop a stronger
which helps sense i f personal id&- tity, which provides e a t e r control of the
develop power situation; 0 learn to. forgive and
forget to keep the doors to relationships
and control.
open; 0 practice physical cues that confirm
confidence and help regain control of the situation, such as a ensuring that facial expressions
correspond with their message, a learning to ignore distractions, 0 listening effectively to the other
person and understanding the other person's message before answering, standing straight,
a using good eye contact, e using relaxed and natural ges-
0 using a level, well-modulated
0 avoid reciprocating with aggressive
tures,
voice and speaking clearly;
behavior because it is ineffective; and 0 handle situations diplomatically
using active listening skills. Careful, attentive listening is critical because communication is the key for success. The assertive person stays calm, listens to both sides of a situation, and focuses attention on problem solv- ing. Willingness to negotiate and com- promise, when appropriate, helps regain control of an explosive situation.
An assertive person informs the abuser of his or her feelings, letting the abuser know that the abuse will not be tolerated. Individuals should learn to say "no" and use "I" statements, such as, "I did not appreciate the language you used today. Please do not use it again."15
Numerous case studies are presented in the module. Staff members read the case studies and answer a series of questions about the problems and suc- cesses presented in the case study. Two case studies are presented and an exam- ple of discussion sessions between the team members and the project modera- tor follow.
CASE STUDY ONE Nurse Friendly is assigned as the cir-
culating nurse in room two for Dr Rude. Dr Rude has five surgical cases, the first one scheduled to start at noon. New requirements of the Joint Commission on Accreditation of Healthcare Organ- izations (JCAHO) mandate that the sur- geon sign the informed consent and confirm the surgical site before the patient can be taken to the OR. The OR has been prepared for the first case, the patient is in the preoperative holding area, has been assessed by the anesthe- sia care provider, and is ready for sur- gery before Dr Rude arrives.
Nurse Shy is caring for the patient in the preoperative holding area. Nurse Friendly assesses the patient in the holding area, confirms the surgical site
158 AORN JOURNAL
Buback JANUARY 2004, VOL 79, NO 1
Dr Rude turned to Nurse Friendly saying? “Are you stupid too? Take the patient into the OR! I’m running late and you’re not helping.’’
with the patient, and notes that the informed consent is correct but that the surgeon has not signed or verified the consent with the patient. Nurse Friendly and the surgical team mem- bers then await Dr Rude’s arrival.
Dr Rude calls the holding area from his office next door at 12:lO I’M. Nurse Shy answers the telephone. Dr Rude shouts, “Tell them to take Mr Arm into the OR. I will be right there!” Nurse Shy answers, ”Yes, sir,” and hangs up the telephone.
Dr Rude’s request is relayed to the surgical team. Nurse Friendly then reminds Nurse Shy of the new JCAHO requirements regarding the informed consent and site verification by the sur- geon. Nurse Shy keeps the patient in the holding area as required.
Dr Rude storms into the holding area, dressed in scrubs, at 12:20 PM. He walks up to Nurse Shy and states “Why the $@#% isn‘t my patient in the OR? Didn’t I tell you to have them take him back? Can’t you relay simple orders?” Nurse Shy lowers her eyes and responds, “I’m sorry,” as she hurries off to her next patient.
Dr Rude then tums to Nurse Friendly. “Are you stupid too? Take the patient into the OR. I’m running late and you are not helping!” Nurse Friendly shoves the chart into Dr Rude’s hands. “We‘ve been waiting for you! The consent isn’t signed and the site hasn’t been verified. Do your part and we’ll take the patient into the OR!” Dr Rude stomps over to the patient, signs the consent form, and verifies the surgical site with the patient. The anes- thesia care provider and circulating nurse then take Mr Arm to the OR.
Mr Arm is induced under anesthesia, after which Dr Rude applies a tourni- quet. Nurse Friendly preps h4r Arm’s right hand, and surgical team members drape the surgical site. Surgery then is begun to repair a nerve injury.
The surgery proceeds without inci- dent until suddenly profuse bleeding begins at the surgical site. Dr Rude shouts “What the +!@# is going on? Doesn’t anything work around here? What is wrong with the tourniquet?” He tums to Nurse Friendly and bellows “Get off your butt and check it out. Can’t you do anything without me telling you first?”
Nurse Friendly checks the tourni- quet; finds the pressure is low and adjusts it to the correct pressure. She then returns to the desk in the comer of OR and thinks to herself ”What is his problem today? He put the tourniquet on and checked the pressure himself. I am tired of his attitude.” Surgery is completed without further incident. The patient suffered no ill effects from the tourniquet failure.
DISCUSSION. The preceding case study demonstrates unacceptable behaviors. Positive, assertive behavior can be developed by learning how to idenhfy negative and positive behaviors. In this case study, Dr Rude is seen as an aggressive party in all interactions with nursing staff members. He shouts and yells and demeans them. Nurse Shy dis- plays passive behavior with downcast eyes and the apology, ”I’m sorry.” Although Nurse Friendly displays assertive behavior in her reminder to Nurse Shy of the new requirements, her subsequent behavior toward Dr Rude in the preoperative area is aggressive. Nurse Friendly’s behavior during the tourniquet incident also could be seen as a positive behavior. She corrects the situation and keeps aggressive thoughts to herself regarding Dr Rude instead of verbalizing them during the procedure, which most probably would have served to escalate the situation.
The situation could have been han- dled differently. Nurse Shy should have reminded Dr Rude of the new chart requirements when he was on the
AORN JOLJFWAL 16 1
telephone. When he arrived, the chart could have been ready for his signa- ture so the patient could proceed to the OR without further delay.
One must assume that, based on AORN standards, Nurse Friendly checked the tourniquet while preparing the room. When the problem with the tourniquet occurred, Nurse Friendly should have notified Dr Rude of the action taken to correct the problem and informed him that the preoperative
Dr Handy notices Nurse Staple and asks, ”Why are you in here? I asked them not to put you in my room again-you are worthless!“
tourniquet
L A
check had occurred with- out complications but that the tourniquet would be sent for main- tenance after the case was completed. Ensur- ing that she was able to observe the sterile field from where she was sit- ting to complete her peri- operative charting might have made her more vis- ible to the individuals within the sterile field. This may have alleviated the impression Dr Rude expressed and also might have helped her see that a problem with the
pressure was occurring. After the ca’se was completed, Nurge Friendly should have acknowledged that she would keep a closer check on the tourniquet in the future but that, nevertheless, Dr Rude’s comments to her were not appreciated. If Dr Rude responds with continued abuse, Nurse Friendly should report the situation to her supervisor and the supervisor must follow up on the situation.
CASE STUDY Two Dr Handy has scheduled a total
nephrectomy in OR room three to begin at 730 AM. Nurse Stitch (ie, scrub per- son) and Nurse Staple (ie, circulating nurse) are scheduled as the OR team.
Working together, they prepare the OR according to the requests on Dr Handy’s preference card.
Upon entering the OR, Dr Handy notices Nurse Staple. He asks “Why are you in here? I asked them not to put you in my room again-you are worthless!” Nurse Staple with eyes downcast, states “I’m sorry, they did not have anyone else to do your proce- dure today. I will do my best, all right?” Dr Handy replies, “We’ll see. Just don’t screw anything up.”
Surgery proceeds without incident for approximately 45 minutes. While locating the renal vein and artery, Dr Handy inadvertently nicks a lumbar artery. He shouts, ”Give me a 5-0 polypropylene, STAT!” Nurse Stitch does not have one available on the ster- ile field. Nurse Staple rushes to the suture cart in the hall to obtain one.
Several minutes go by before Nurse Staple returns empty-handed because she was unsure of the type of needle to obtain. She calmly asks Dr Handy “What kind of needle do you want that on?” Dr Handy yells ”Just give me a %!#$ vascular stitch-anything, before this patient bleeds to death.” Turning to the anesthesia care provider, Dr Handy shouts, ”Get somebody in here who knows what the +!@$ they are doing!” The anesthesia care provider pages the supervisor. Nurse Staple obtains a polypropylene suture on a vascular needle and delivers it asepti- cally to Nurse Stitch.
Supervisor Bell enters the OR. Immediately Dr Handy shouts ”Don’t you have any nurses who know what the $@#$ they are doing? Are they all incompetent?” Supervisor Bell assesses the situation. She reviews the prefer- ence card with Nurse Staple. The pref- erence card requests a 5-0 polypropy- lene suture on a vascular needle be available in the OR for emergency, if needed. Supervisor Bells asks Nurse
16 2 AORN JOURNAL
Staple "Who checked the preference card and pulled suture?" Nurse Staple replies, "I checked the card for all sup- plies except the suture. Nurse Stitch always pulls her own suture. She knows the suture better than I do." Supervisor Bell turns to Dr Handy. "The suture was missed on your preference card. I will take steps to see the situation is avoided in the future."
The nephrectomy is completed with- out further incident. Before leaving the OR, Nurse Staple turns to Dr Handy. "I'm sorry. I keep messing up in your room. I deserved your anger today. I need to find a class on types of suture so I can be better prepared." Dr Handy replies "Good idea. Let me know if I can be of assistance."
Nurse Stitch and Nurse Staple meet with Supervisor Bell to review the situ- ation. Supervisor Bell asks Nurse Stitch why the vascular stitch was not avail- able if she was responsible for obtaining sutures. Nurse Stitch apologizes and explains that she simply forgot to pull the emergency stand-by sutures and would not fail to do so in the future. Nurse Staple requests a class on suture so that she does not have to depend on the scrub person in the future. Supervisor Bell agrees that this is a very good proactive step and schedules a class with the suture representatives for Nurse Staple for the following week.
DISCUSSION. Case study two shows Dr Handy in the role of a verbal abuser. He demeans the circulating nurse when he first enters the OR. In response to his attack, Nurse Staple shows passive behavior in both her nonverbal (eg, downcast eyes) and ver- bal (eg, "I'm sorry," "1'11 do my best, all right?") cues. Dr Handy verbally attacks the circulating nurse when a suture he has requested is not pro- duced immediately. When the supervi- sor arrives to assess the situation, the circulating nurse blames the missing
suture on the scrub person. Assertive behavior was displayed
by Supervisor Bell during her assess- ment of the situation and the subse- quent interaction and problem solving, although she did not discuss Dr Handy's behavior with him. Nurse Staple accepted responsibility for not knowing the suture types used during the procedure. Even though Dr Handy offered his assistance after Nurse Staple accepted responsibility for her actions, Supervisor Bell should have pulled Dr Handy aside
Improving after the procedure to discuss his behavior and, if need be, discuss it with her supervisor or the team member chief ofsurgery. communication
Improving team mem- ber c6mm&cation could avert future incidents. The circulating nurse and scrub person work as a team to prepare the room. Both should be aware of all preference card needs for a given procedure. The surgeon and other team members should be made aware of items that are not immediately available.
can help to avert future incidents of verbal abuse.
CONCLUSIONS Research has shown a high incidence
of verbal abuse in perioperative set- tings. Verbal abuse contributes to low job satisfaction, high staff member turnover, and increased errors. The use of assertiveness training as a compo- nent of conflict resolution has been shown to decrease the incidence of ver- bal abuse with subsequent improve- ment in job satisfaction, decreased staff member turnover, and fewer patient errors. This assertiveness training mod- ule was developed in response to the high percentage of perioperative nurses who have experienced verbal abuse in the OR. Preliminary results show that
AORN JOURNAL 163
the use of assertiveness training improves self-esteem and communica- tion skills. This contributes to a positive outcome in the OR environment for the patient and OR team members. 9
Debbie Buback, RN, MSN, CNOR, CRNFA, A”, is an adult nurse practi- tioner and RN first assistant at Urology Consultants, Ltd, St Louis, Mo.
NOTES 1. V Watson, M J Steiert, ”Verbal abuse and violence: The quest for harmony in the OR,” SSM 8 (August 2002) 16-22. 2. P Bruder, “Verbal abuse of female nurs- es: An American medical form of ender apartheid?” Hospital Topics 79 (Faf2001)
3. J A H Rosenstein, ”Nurse-physician rela- tionships: Impact on nurse satisfaction and retention,” American Journal of Nursing 102 (June 2002) 26-34. 4. W Brennan, “Dealing with verbal abuse,” Emergency Nurse 9 (September
5. J Cook, M Green, R Top? “Exploring the impact of physician verba abuse on peri- operative nurses,“ AORN Journal 74
30-34.
2001) 15-17.
(September 2001) 317-331. 6. M A Manderino, N Berkey, “Verbal abuse of staff nurses by physicians,” Journal of Professional Nursing 13 (January/Febru- ary 1997) 48-55. 7. R Michael, H J Jenkins, ”Work related trauma: The experiences of perioperative nurses,” Collegian 8 (January 2001) 19-25. 8. C Lybecker, L Sofield, “Verbal abuse,“ Sur ‘cal Services Management 6 (June 2000) 32-&. 9. J L Jacobs, “Preventing workplace vio- lence,” Surgical Services Management 6 (May 2000) 42-46. 10. L Cameron, ’‘Verbal abuse: A proactive approach,” Nursing Management 29 (August
11. C Anderson, M Stamper, “Workplace violence,” RN 64 (Februa 12. S L Espin, LA Lingarx “Time as a cata- lyst for tension in nurse-sur eon communi-
13. S Araujo, L Sofield, “Verbal abuse
~ ~ ~ w w . l a u r a s o f i e l d . c o m (accessed 11
1998) 34-36.
2001) 71-74.
cation,” AORN Journal 74 ( 8 ovember 2001) 672-682.
” Welcome to Laura’s Comer,
Oit 2003). 14. C J Chouvardas, “7 Steps to assertin vourself.” NursinP9I 21 (November 1998 i26-132.’ 15. C Holstead, ”Assert yourself!” Women in Business 46 (March/Aprill994) 32-33.
0
~~ ~
Publish an AORN Journal Home Study Program he AORN Journal editor i s seeking authors to submit manuscripts that qualify for AORN Journal
Home Study Programs. The content must include comprehensive and detailed descriptions of patient care activities, surgical processes, or descriptive patient care information. Content must describe disease processes or surgical procedures, nursing considerations, and patient care. Examples of proce- dure-specific content include 0 detailed anatomy and physiology: 0 preoperative care and interventions (eg, labora-
tory work, diagnostic studies); 0 patient and family member teaching: 0 patient-specific (eg, age, diagnosis, specific pro-
0 preparation for the procedure (eg, scheduling,
equipment and instrumentation needs, patient care needs);
0 intraoperative care and activities, including spe- cific responsibilities of team members;
0 postoperative care: and 0 discharge teaching, expected recovery, and reha-
bilitation (eg, office visits, physical therapy, return to work, reportable symptoms).
Author guidelines can be obtained online at http://www.aorn.ordjournal/guidelines. htm. Ideas can be discussed with the editor by calling (210) 567-5841 or by sending an e-mail to [email protected]. Home Study Programs whose authors include at least one R N AORN member qualify for the annual AORN Journal Writers Contest.
T
cedure) needs:
16 4 . AORN JOURNAL





























