Embed Size (px)
Citation preview
















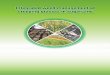
Intracanalicular (0 mm) 10 mm
20 mm 30 mm

Translabyrinthineapproach
Retrosigmoidapproach
Middle Fossa Approach

The Effect of Age on Acoustic NeuromaSurgery Outcomes
John S. Oghalai, James L. Buxbaum, Lawrence H. Pitts, and Robert K. Jackler
Departments of Otolaryngology–Head and Neck Surgery and Neurosurgery, University of California SanFrancisco. San Francisco, California, U.S.A.
Objectives: To ascertain the effect of age on hearing preser-vation, facial nerve outcome, and complication rates afteracoustic neuroma surgery.Study Design: Retrospective chart review. Two study armswere used: a comparison of the authors’ oldest patients withtheir youngest patients (extremes of age arm) and an analysis ofall middle fossa surgical procedures (middle fossa arm).
Setting: Tertiary referral centerPatients: Total of 329 patients. For the extremes of age arm,205 patients were studied in two cohorts with 150 older patients(>60 years) compared with 55 younger patients (<40 years).The approaches included 21 middle fossa (MF), 38 retrosig-moid (RS), and 91 translabyrinthine (TL) procedures in theolder group versus 25 MF, 17 RS, and 13 TL in the younger.For the middle fossa arm, there were 170 patients (age range15–76 years) who underwent the MF approach for an attempt athearing preservation.
Main Outcome Measures: Hearing preservation was definedas the maintenance of either class A or class B hearing (AAO-HNS class). Good facial nerve outcome was considered themaintenance of either grade 1 or 2 (House-Brackmann scale).
Cerebrospinal fluid leak rates and other postoperative compli-cations were also tabulated.Results: After adjustment for tumor size and surgical approachusing multiple logistic regression analysis, the extremes of agestudy arm demonstrated that there is a lower chance of pre-serving good hearing in older patients (p � 0.048, odds ratio �0.30). Age was not associated with a difference in the rate of goodfacial nerve outcome (p � 0.2). There was a trend toward slightlyhigher rates of cerebrospinal fluid leak in the older patient group(p � 0.07) but no difference in the rate of other complications (p� 0.9). The middle fossa study arm, after adjustment for tumorsize and surgical approach, demonstrated that older patient age isassociated with a lower rate of preservation of good hearing (p� 0.01, O.R.�1.044). There was no association between ageand good facial outcome (p � 0.7).Conclusions: Older patient age lowers the chance of hearingpreservation but does not affect facial outcomes. There is atrend toward a higher rate of cerebrospinal fluid leak in olderpatients, but no increased risk of other complications. KeyWords: Vestibular schwannoma—Acoustic neuroma—Middlefossa approach—Hearing preservation—Skull base surgery.Otol Neurotol 24:473–477, 2003.
Acoustic neuromas (AN) in young and middle-agedpatients are usually treated surgically. The rates of hear-ing preservation, facial nerve function, and complica-tions after tumor resection in the general population havebeen well described by multiple retrospective reviews(1–5). However, because of perceived increases in sur-gical risk and shorter expected patient life span, the trendin managing these tumors in patients over 60 years oldhas been toward nonoperative strategies. Consequently,the literature on AN in the elderly tends to focus more onoperative versus nonoperative management (6–11). Be-cause the aging baby boomer cohort has improved healthand a lengthened life expectancy in comparison with
earlier generations (12–14), the role of age in the surgicalmanagement of AN needs to be evaluated carefully.Functional outcomes are particularly important in thisactive and vibrant patient population (15). It is possible,however, that older age may diminish the ability of thecochlear or the facial nerve to tolerate the surgical ma-nipulation necessary to resect an AN. We sought to as-certain the effect of age on hearing preservation, facialnerve outcome, and complication rates after AN surgery.
MATERIALS AND METHODS
Study Design and Patient PopulationOur retrospective study of 329 patients included two arms to
evaluate for an effect of age on AN surgical outcomes. The firstwas a comparison of our oldest patients versus our youngestpatients (extremes of age study arm). This was because wehypothesized that any major differences in surgical outcomes
Address correspondence and reprint requests to Dr. John S. Oghalai,Department of Otolaryngology–Head and Neck Surgery, 400 ParnassusAvenue, Suite A-730, University of California San Francisco, SanFrancisco, CA 94143–0342, U.S.A.; Email: [email protected]
Otology & Neurotology24:473–477 © 2003, Otology & Neurotology, Inc.
473

based on age would be most easily detectable using patients atthe extremes of age. The second was an analysis of all middlefossa surgery outcomes (middle fossa arm). This study arm wasused to evaluate for subtle effects of age on hearing and facialnerve outcomes, because the middle fossa route is our usualapproach for hearing conservation surgery.
The extremes of age study arm was a retrospective studycomparing older and younger patients (total n � 205). Allpatients over 60 years of age who underwent surgical excisionof an AN were compared with those patients under than 40years of age. The details of the two groups of patients are givenin Table 1. The expected patient life span was determined froman actuarial table (16). Tumor size was measured as millimetersin the cerebellopontine angle (CPA). Tumors wholly confinedto the internal auditory canal were categorized as intracanali-cular (0 mm).
The average tumor size in the patients undergoing the middlefossa approach was much smaller than that in the patients un-dergoing the retrosigmoid approach. This reflects our philoso-phy of using the middle fossa approach as our primary strategytoward hearing preservation, while reserving the retrosigmoidapproach only for hearing conservation attempts for tumorsmeasuring 15 to 25 mm in the CPA (17). Older patients un-dergoing the translabyrinthine approach also tended to havelarger tumors, because our usual policy for older patients withsmall tumors and poor hearing is to either monitor them withserial magnetic resonance imaging or treat them with stereo-tactic radiotherapy.
The middle fossa study arm was a retrospective review of allpatients who underwent the middle fossa approach for resectionof an AN, regardless of age. This included patients at the ageextremes as well as those 40 to 60 years old (total n � 170,Table 1). This larger patient population permitted us to studythe effect of patient age on hearing preservation with greaterpower than did the extremes of age study arm. The averagepatient age was 45 ± 10 years (mean ± SD), and the averagetumor size was 5 ± 6 mm (mean ± SD) in the CPA.
Main Outcome MeasuresGood hearing preservation was defined as postoperative
AAO-HNS class A or B hearing (18). We did not includepatients in this analysis who had class C or D hearing preop-eratively. We measured postoperative hearing at least 3 months
after surgery. Good postoperative facial function was consid-ered House-Brackmann grade 1 or 2 (19). We did not includepatients in this analysis who had grade 3 or worse facial func-tion preoperatively. Postoperative facial weakness was nottabulated unless it was present 1 year after surgery.
Postoperative complications were also tabulated. Cerebro-spinal fluid (CSF) leaks were identified separately from othercomplications. This included all postoperative leaks identified,whether they required lumbar subarachnoid drain and/or reop-eration. Fewer than 5% of patients with leaks required opera-tive intervention (20).
Statistical AnalysisSPSS (version 10.0; SPSS, Inc., Chicago) was used for sta-
tistical analysis. All averages are reported as mean ± standarddeviation. We used the two-tailed t test to compare continuousvariables (patient age and tumor size). Multiple logistic regres-sion analysis was performed to account for confounding vari-ables in the comparison of discrete variables (hearing preser-vation, good facial function, CSF leak, other complications).This technique was also used for the continuous variables toverify the t test results. A stepwise entry methodology wasused. For all analyses, statistical significance was determined ifp � 0.05.
RESULTS
Extremes of Age Study ArmThis first arm was designed to compare patients at the
extremes of age for each of the three surgical approachesto identify major differences that might be associatedwith patient age. The main outcome measures are pre-sented in Table 2. The rate of hearing preservation waslower in the older patient group than in the youngerpatient group for both the middle fossa (29% vs. 60%)and the retrosigmoid (8% vs. 15%) approaches. Multiplelogistic regression analysis was performed to identify aneffect of age on hearing preservation, while accountingfor surgical approach and tumor size. This demonstratedthat patients older than 60 years were less likely to have
TABLE 1. Patient population stratified by surgical approach and age group
Surgical approach Group N Age (yr) Expected lifespan (yr)Tumor sizea
(mm in CPA) Study arm
Middle fossa <40 yr 25 32 ± 7 46 ± 6 5 ± 6 Extremes of age,[15–39] [40–62] [0–18] middle fossa
40–60 yr 124 51 ± 5 30 ± 2 5 ± 6 Middle fossa[41–59] [22–39] [0–18]
>60 yr 21 66 ± 4 17 ± 3 7 ± 5 Extremes of age,[60–76] [11–22] [0–18] middle fossa
Retrosigmoid <40 yr 17 32 ± 6 46 ± 6 21 ± 3 Extremes of age[20–39] [40–58] [15–25]
>60 yr 31 68 ± 6 16 ± 4 21 ± 11 Extremes of age[60–89] [5–22] [0–50]
Translabyrinthine <40 yr 16 33 ± 5 45 ± 5 22 ± 15 Extremes of age[22–38] [41–57] [0–40]
>60 yr 68 68 ± 6 16 ± 4 20 ± 12 Extremes of age[60–86] [6–22] [0–45]
All values are mean ± standard deviation. The range is in brackets.Expected lifespan was calculated from actuarial data (25).aIntracanalicular tumors recorded as 0 mm in the cerebellopontine angle.
474 J. S. OGHALAI ET AL.
Otology & Neurotology, Vol. 24, No. 3, 2003

preserved good hearing than those younger than 40 years(p � 0.048, odds ratio � 0.30).
The rate of good postoperative facial function did notseem to be dramatically different between the older andthe younger age groups for any of the surgical ap-proaches (87–100%). Multiple logistic regression analy-sis accounting for surgical approach and tumor size dem-onstrated that there was no effect of age grouping onfacial outcomes (p � 0.2). There was a trend towardslightly higher rates of CSF leak (0–15%) in the olderpatient group (p � 0.07), but there was no statisticallysignificant difference in the rate of other complications(0–7%, p � 0.8) between the age extremes.
Middle Fossa Study ArmThis second arm was a review of all patients who
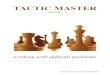
underwent the middle fossa approach. It was designed toidentify subtle associations of age with hearing and facialnerve outcomes in our primary hearing preservation ap-proach. First, we compared the average patient age andtumor size for patients in whom we were and were notable to preserve hearing and maintain good facial nervefunction (Fig. 1.). Patients in whom hearing was pre-served were younger than those in whom hearing was notpreserved (A, preserved: 48 ± 11 years, n � 75 vs. notpreserved: 52 ± 9 years, n � 88, p � 0.01). Addition-ally, there was a trend toward patients with a smallertumor size having an improved rate of hearing preserva-tion (B, preserved: 4 ± 5 mm, n � 74 vs. not preserved:6 ± 6 mm, n � 88, p � 0.08). Neither younger patientage (C, good facial function: 50 ± 10 years, n � 155 vs.poor facial function: 51 ± 7 years, n � 10, p � 0.8) nortumor size (D, good facial function: 5 ± 6 mm, n � 154
vs. poor facial function: 6 ± 5 mm, n � 10, p � 0.7)were correlated with good facial function.
Because larger tumor size can be associated withlower hearing preservation rates and worse facial nerveoutcomes, it is important to distinguish between the ef-fects of patient age and the effects of tumor size. Mul-tiple logistic regression analysis was then performed toaccount for tumor size as a confounding variable. Thisrevealed that older age was associated with poorer ratesof hearing preservation (p � 0.01; odds ratio � 1.044).This means that the odds of hearing preservation de-creases by 4.4% per year. However, older age was not anindependent predictor of poor facial function (p � 0.7).
DISCUSSION
Both arms of the study demonstrate that older patientshave a decreased rate of hearing preservation when tu-mor size was controlled for. Additionally, there was alsoa trend toward higher CSF leak rates in older patients,but there was no statistically significant effect of age onother complications or facial nerve function. However,our facial function results may be biased toward betterpreservation rates in older patients because we typicallyare less aggressive in trying to achieve total tumor re-moval in this population. We may leave a small bit oftumor on the facial nerve to reduce trauma and subse-quent morbidity. A near-total resection means leaving ascrap of tumor no larger than 25 mm2 (5 × 5 mm) and 2mm thick, and a subtotal resection means leaving anylarger piece. It is likely that without our altered surgicaltechnique for older patients, there would have been asignificantly reduced rate of good postoperative facial
TABLE 2. Outcome measures stratified by surgical approach and age group
Surgical approach Group Good hearing (%)Good facialfunction (%) CSF leak (%)
Rate of othercomplications (%) Other complications
Middle fossa <40 yr 15/25 (60) 24/25 (96) 4/25 (16) 0/25 (0)40–60 yra 55/121 (46) 115/124 (93) 12/124 (10) 1/124 (0) Deep venous thrombosis,
treated with inferior venacava filter (1)
>60 yr 5/17 (29) 16/16 (100) 5/21 (24) 0/21 (0)Retrosigmoid <40 yr 2/13 (15) 16/16 (100) 1/16 (6) 0/16 (0)
>60 yr 1/12 (8) 25/28 (89) 6/38 (16) 1/38 (3) Postoperative communicatinghydrocephalus that resolvedspontaneously (1)
Translabyrinthine <40 yr n/a 12/13 (92) 0/13 (0) 0/16 (0)>60 yr n/a 64/74 (87) 14/91 (15) 6/91 (7) Wound infections that
resolved with local wound careand antibiotics (3), non-communicating hydrocephalussecondary to intraventricularhemorrhage that requiredventriculoperitoneal shunt (1),diplopia (1), postoperativemyocardial infarction withgood recovery (1)
The number of patients in each category may be less than the total number of patients studied. Only patients with preoperative AAO-HNS classA or B hearing or preoperative House-Brackmann grade 1 or 2 facial function were included in the analysis.
aThis middle age group of patients was not use for the extremes of age study arm, but was included in the middle fossa study arm.CSF, cerebrospinal fluid; n/a, not applicable.
475EFFECT OF AGE ON ACOUSTIC NEUROMA OUTCOMES
Otology & Neurotology, Vol. 24, No. 3, 2003

function (as there was with the rate of hearing preserva-tion). We did not have enough patients to perform aquantitative analysis of the effect of the completeness ofsurgical resection on hearing and facial nerve function.
Our hearing and facial nerve preservation findingsconcur with and expand on those of other investigators.Brackmann et al. (3) found that the average age of pa-tients who lost hearing postoperatively with the middlefossa approach was slightly higher than in patients whodid not, although the difference was not significant.Ramsay and Luxford (6) found similar postoperative fa-cial nerve function in patients older than 70 years andyounger than 70 years of age, all of whom were treatedwith the translabyrinthine approach.
Certainly, there is a generalized increased risk of sur-gical complications in older patients in all types of sur-gery. This is predominantly due to the steady decline inorgan system functioning during aging (21). One mightreasonably suspect that complications during AN surgeryshould occur more frequently in older patients. However,older patient age has not been shown to be associatedwith increased complications in AN surgery (22,23). Ourdata support these studies, in that we saw no effect ofolder age on complication rates. The middle fossa ap-proach is thought to be more technically challenging inolder patients because of thinning and adhesions of thedura. Indeed, patient age greater than 60 years has beensuggested as a relative contraindication to the middlefossa approach (24,25). Our philosophy has been to base
our surgical approach on tumor size, location, and re-sidual hearing, and we do not believe that older patientage is a contraindication to the middle fossa approach.Meticulous surgical technique in raising the craniectomybone flap, suture repair of any dural tears, and carefulbipolar cautery of any bleeding vessels is critical to thesuccessful prevention of technical complications. Alsolarger tumor size is probably not associated with an in-creased rate of CSF leak (20).
The dilemma in treating older patients is whether toremove a small AN to preserve potential hearing loss inthe years to come. Our philosophy on the management ofAN in patients older than 60 years is to treat with eithersurgery or stereotactic radiation only if the patient has alarge tumor with substantial brainstem compression, hasprogressive worsening of symptoms (particularly failingbalance), or demonstrates tumor growth at a rate that willeventually lead to serious brainstem compression withinthe patient’s predicted life span. By far the majority ofolder patients with tumors smaller than 2 cm in the CPAundergo a period of observation with serial magneticresonance imaging to determine tumor growth rate, be-fore intervention strategies are decided on. The risk oftumor progression and hearing loss (with either no treat-ment or stereotactic radiation) and the risk of the devel-opment of a radiation-induced malignancy (with stereo-tactic radiation) during an expected life span of 15 to 20years should be weighed against the risks and benefits oftumor removal in consultation with the patient.
FIG. 1. The effect of patient ageand tumor size on surgical out-comes with the middle fossa ap-proach. Patients in whom hearing(A, B) or good facial nerve func-tion (C, D) were able to be pre-served were compared with thosein whom they could not be pre-served. The box and whisker plotsdemonstrate the 25th and 75thpercentiles of the samples (bot-tom and top of the boxes), the me-dians (line in the middle of theboxes), and the extent of thesample (whiskers above and be-low the boxes). Outliers more than1.5 times the interquartile rangeaway from the top or bottom of thebox are identified (o). Younger pa-tient age (A, 48 ± 11 years, n = 75,vs. 52 ± 9 years, n = 88, p = 0.01)was correlated with hearing pres-ervation. There was a trend to-ward hearing preservation in pa-tients with smaller tumors (B, 4 ± 5mm, n = 74, vs. 6 ± 6 mm, n = 88,p = 0.08). The number of patientsis less than the total number of pa-tients studied because only pa-tients with preoperative AAO-HNSclass A or B hearing were ana-lyzed. Neither younger patient age
(C, 50 ± 10 years, n = 155, vs. 51 ± 7 years, n = 10, p = 0.8) nor tumor size (D, 5 ± 6 mm, n = 154, vs. 6 ± 5 mm, n = 10, p = 0.7) wascorrelated with good facial function.
476 J. S. OGHALAI ET AL.
Otology & Neurotology, Vol. 24, No. 3, 2003

REFERENCES
1. Slattery WH 3rd, Brackmann DE, Hitselberger W. Middle fossaapproach for hearing preservation with acoustic neuromas. Am JOtol 1997;18:596–601.
2. Irving RM, Jackler RK, Pitts LH. Hearing preservation in patientsundergoing vestibular schwannoma surgery: comparison of middlefossa and retrosigmoid approaches. J Neurosurg 1998;88:840–5.
3. Brackmann DE, Owens RM, Friedman RA, et al. Prognostic fac-tors for hearing preservation in vestibular schwannoma surgery.Am J Otol 2000;21:417–24.
4. Holsinger FC, Coker NJ, Jenkins HA. Hearing preservation inconservation surgery for vestibular schwannoma. Am J Otol 2000;21:695–700.
5. Wiet RJ, Mamikoglu B, Odom L, et al. Long-term results of thefirst 500 cases of acoustic neuroma surgery. Otolaryngol HeadNeck Surg 2001;124:645–51.
6. Ramsay HA, Luxford WM. Treatment of acoustic tumors in elder-ly patients: is surgery warranted? J Laryngol Otol 1993;107:295–7.
7. Silverstein H, Rosenberg SI, Flanzer JM, et al. An algorithm forthe management of acoustic neuromas regarding age, hearing, tu-mor size, and symptoms. Otolaryngol Head Neck Surg 1993;108:1–10.
8. Pulec JL. Acoustic neuroma surgery in geriatric patients. Ear NoseThroat J 1999;78:429–30, 33–6, 38–40 passim.
9. Rosenberg SI. Natural history of acoustic neuromas. Laryngoscope2000;110:497–508.
10. Shin YJ, Fraysse B, Cognard C, et al. Effectiveness of conservativemanagement of acoustic neuromas. Am J Otol 2000;21:857–62.
11. Perry BP, Gantz BJ, Rubinstein, JT. Acoustic neuromas in theelderly. Otol Neurotol 2001;22:389–91.
12. Schneider EL, Guralnik JM. The aging of America: impact onhealth care costs. JAMA 1990;263:2335–40.
13. Cornman JM, Kingson ER. Trends, issues, perspectives, and val-
ues for the aging of the baby boom cohorts. Gerontologist 1996;36:15–26.
14. Tuljapurkar S, Li N, Boe C. A universal pattern of mortality de-cline in the G7 countries. Nature 2000;405:789–92.
15. Robine JM, Romieu I, Cambois E. Health expectancy indicators.Bull World Health Organ 1999;77:181–5.
16. Center for Disease Control. National Vital Statistics Report. Avail-able at: Statistics, NCfH.
17. Satar B, Jackler RK, Oghalai JS, et al. Risk benefit analysis ofusing the middle fossa approach for acoustic neuromas with >10mm cerebellopontine angle component. Laryngoscope 2002;112:1500–6.
18. Committee on Hearing and Equilibrium guidelines for the evalu-ation of hearing preservation in acoustic neuroma (vestibularschwannoma). American Academy of Otolaryngology-Head NeckSurgery Foundation, Inc. Otolaryngol Head Neck Surg 1995;113:179–80.
19. House JW, Brackmann DE. Facial nerve grading system. Oto-laryngol Head Neck Surg 1985;93:146–7.
20. Becker SS, Jackler RK, Pitts LH. Cerebrospinal fluid leak afteracoustic neuroma surgery: a comparison of the translabyrinthine,middle fossa, and retrosigmoid approaches. Otol Neurol 2003;24:107–12.
21. Zenilman, ME. Preoperative assessment of the elderly patient. In:Cameron JL, ed. Current Surgical Therapy. 5th ed. St. Louis: C.V.Mosby, 1995:928–32.
22. Samii M, Tatagiba M, Matthies C. Acoustic neurinoma in theelderly: factors predictive of postoperative outcome. Neurosurgery1992;31:615–9; discussion 9–20.
23. Slattery WH 3rd, Francis S, House KC. Perioperative morbidity ofacoustic neuroma surgery. Otol Neurotol 2001;22:895–902.
24. Coker NJ, Jenkins HA. Atlas of Otologic Surgery. Philadelphia:W.B. Saunders, 2001.
25. Centers for Disease Control. National Vital Statistics Report.Available at: http://www.cdc.gov/nchs/products/pubs/pubd/nvsr/nvsr.htm. Accessed October 2001.
477EFFECT OF AGE ON ACOUSTIC NEUROMA OUTCOMES
Otology & Neurotology, Vol. 24, No. 3, 2003

The fate of the tumor remnant after less-than-completeacoustic neuroma resectionDOV C. BLOCH, MD, JOHN S. OGHALAI, MD, ROBERT K. JACKLER, MD, MONICA OSOFSKY, MD, and LAWRENCE H. PITTS, MD,San Francisco, California
OBJECTIVES: We sought to determine the recur-rence rate after near-total and subtotal resection ofacoustic neuroma.STUDY DESIGN, SETTING, AND PATIENTS: We con-ducted a retrospective chart review of a total of 79patients: 50 with near-total resections (remnant <25mm2 and <2 mm thick) and 29 with subtotal resec-tions (any larger remnant). Surgical approach in-cluded 5 middle fossa, 17 retrosigmoid, and 57translabyrinthine.MAIN OUTCOME MEASURES: Recurrence was de-fined as documented tumor growth by serial imag-ing or the recommendation for further treatmentafter a single scan. No recurrence was defined asno visible tumor on imaging for a minimum fol-low-up time of 3 years or tumor remnants that re-mained unchanged on serial scans (mean, 5-yearfollow-up).RESULTS: Fifty-two patients were included in thestudy group. Recurrences were seen in 1 (3%) of 33patients who had a near-total resection comparedwith 6 (32%) of 19 patients who had a subtotal re-section. After adjustment for follow-up time andlarge tumor size, the odds ratio for recurrence was12 times larger for subtotal than for near-total re-sections (P � 0.033). All recurrences were seen fol-lowing the translabyrinthine approach in the mid-cerebellopontine angle. None were encountered inthe internal auditory canal. The mean time intervalfrom surgery to the detection of a recurrence was 3years (range, 1 to 5 years).
CONCLUSIONS: The recurrence rate when perform-ing a near-total resection is low but is substantiallyhigher with a subtotal resection. Recurrences canbe detected within the first 5 postoperative years.We recommend near-total resection in any patientif needed to preserve neural integrity. Subtotal re-section is best avoided whenever possible; how-ever, adjunctive treatment with stereotactic radio-therapy may be considered. (Otolaryngol HeadNeck Surg 2004;130:104-12.)
The goals of acoustic neuroma (AN) surgery aretumor control and preservation of cranial nerves,including the facial nerve and at times the auditorynerve. Balancing the priority of these goals isinfluenced by other considerations such as patientage and life expectancy, overall health and comor-bidities, and tumor adherence and size. Microsur-gical gross total tumor removal is by far the mostcommon result of AN surgery. Less-than-com-plete resection most commonly involves an intra-operative decision to leave tumor remnants behindas a concession to neural integrity. Elderly ordebilitated patients may have a subtotal removalplanned preoperatively to minimize the morbidityand mortality associated with a more extensiveand lengthy procedure. The aim of the presentstudy was to determine the risk of tumor recur-rence with incomplete AN resection.
METHODSSeventy-nine patients with incomplete AN re-
sections from 1978 to 1999 were identified, ac-counting for less than 10% of the patients whounderwent AN surgery at our institution. At theUniversity of California–San Francisco (UCSF), ateam composed of a neurotologist and a neurosur-geon perform the procedure. A retrospective chartreview was performed from records kept by bothdepartments and entered into a computerized da-tabase. The study protocol was approved by theUCSF Committee on Human Research.
Clinical parameters, including patient age, gen-der, symptoms, surgical approach, and postopera-
From the Departments of Otolaryngology–Head and NeckSurgery (Drs Bloch, Oghalai, Jackler, Osofsky, and Pitts)and Neurosurgery (Drs Pitts and Jackler), University ofCalifornia–San Francisco.
Presented at the Annual Meeting of the American Academyof Otolaryngology–Head and Neck Surgery, San Diego,CA, September 22-25, 2002.
Reprint requests: John S. Oghalai, MD, Department of Oto-rhinolaryngology and Communicative Sciences, One Bay-lor Plaza, NA102, Houston, TX 77030; e-mail,[email protected].
0194-5998/$30.00Copyright © 2004 by the American Academy of Otolaryn-
gology–Head and Neck Surgery Foundation, Inc.doi:10.1016/S0194-5998(03)01598-5
104

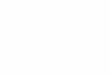
tive complications, were recorded. Tumor size,based on the greatest dimension within the cer-ebellopontine angle (CPA), was obtained frompreoperative imaging data. The surgeons’ noteswere examined to ascertain the indication for per-forming an incomplete resection whenever possi-ble. As opposed to defining residual tumor as apercentage of the original tumor, near-total resec-tions were defined by tumor remnants no greaterthan 25 mm2 and 2 mm thick; subtotal resectionsincluded anything larger1 (Fig 1). Facial nerveoutcomes with a minimum of 1-year follow-up
were recorded, based on the House-Brackmann(HB) grading system.
Our routine protocol for postoperative tumorsurveillance consists of imaging at 1 and 3 yearsfor tumors that have been totally removed. In-completely resected tumors are followed annu-ally with a gradual lengthening of the time be-tween scans when there is no evidence ofrecurrence. Because UCSF is a tertiary referralcenter, some patients receiving longitudinal fol-low-up care at other institutions had differentimaging regimens. The modality most com-
Fig 1. (A) The 2 types of incomplete tumor resection strategies. Near-total resections were defined by tumor remnants nogreater than 25 mm2 and 2 mm thick; subtotal resections included anything larger. (B) Surgical dissection of the mostadherent area of the tumor off of the facial nerve.
Otolaryngology–Head and Neck SurgeryVolume 130 Number 1 BLOCH et al 105

monly used was magnetic resonance imaging(MRI), although a few patients early in the studyperiod had computed tomography (CT). All pa-tients, except for 1, had an MRI study at somepoint in their follow-up.
The results of all postoperative follow-up im-aging were recorded to identify residual and/orrecurrent tumor. No tumor recurrence was definedby the absence of visible tumor on imaging after aminimum follow-up of 3 years or if stable residualtumor was present. Stable residual tumor wasdefined as a tumor remnant that remained un-changed on serial imaging. Recurrent tumor wasdefined as tumor growth on serial imaging. Addi-tionally, tumor recurrence was defined as whenthe patient underwent additional treatment (eitherstereotactic radiation or repeat surgery) after onlya single scan because of the large tumor size.
Statistical AnalysisStata (version 7.0; Stata Corp, College Station,
TX), SPSS (version 10.0; SPSS, Inc, Chicago, IL),and StatXact (version 3.0; Cytel Software, Cam-bridge, MA) were used for statistical analysis.Fisher exact test and 2-sided t test were used toevaluate bivariate relationships. Logistic regres-sion was performed on recurrence and good facialnerve function (HB I or II) to assess the influenceof subtotal versus near-total resection, age, large
tumor size (�25 mm), and other predictors. Oddsratios were calculated and statistical significancewas determined if P � 0.05. Logistic regressionwas followed by statistical analyses using exactstratified contingency table analysis to check thestability of the logistic regression results.
RESULTSPatient Population
There were 50 patients (63%) with near-totalresections and 29 patients (37%) with subtotalresections (Table 1). The mean age was 59 years(range, 21 to 81 years). Patients who underwentsubtotal resections tended to be older than thenear-total group (mean, 62 versus 57 years; P �0.10). The mean tumor size was significantlygreater in the subtotal resection group than in thenear-total resection group (31 mm versus 24 mm,P � 0.005). The predominant approach used inthis group of patients was the translabyrinthine(TL), accounting for 72% of the operations. Theaverage tumor size was greatest for the TL ap-proach (26 mm) followed by the retrosigmoid(RS) (22 mm) and the middle fossa (MF) (7 mm)approaches. A comparison between the near-totaland subtotal groups showed no significant differ-ence in terms of gender, approach, and follow-upperiod. Postoperative complications are presentedin Table 2. The cerebellar peduncular infarcts
Table 1. Patient populations
Near-total (n � 50; 63%) Subtotal (n � 29; 37%)
GenderMale 23 15Female 27 14
Tumor size inCPA,*mean � SD (mm) 24 � 10 31 � 12(P � 0.005) (range, 0 to 45) (range, 7 to 65)Surgical approach
Translabyrinthine 34 (68%) 23 (79%)Mean (mm) 26 (range, 12 to 45) 31 (range, 7 to 65)
Retrosigmoid 12 (24%) 5 (17%)Mean (mm) 22 (range, 0 to 37) 33 (range, 18 to 45)
Middle fossa 4 (8%) 1 (4%)Mean (mm) 7 (range, 0 to 12) 15
AgeMean � SD (yr) 57 � 13 62 � 13(P � 0.10) (range, 21 to 78) (range, 34 to 81)
*Largest diameter dimension in the CPA. Intracanalicular tumors recorded as 0 mm.CPA, Cerebellopontine angle.
Otolaryngology–Head and Neck Surgery
106 BLOCH et al January 2004

were areas of distal anterior inferior cerebellarartery ischemia (with minimal symptomatology),not major strokes.2 There were no known tumor-related deaths, but there were 4 unrelated deathsseen on long-term follow-up.
Indications for Incomplete ResectionAlthough all patients had an incomplete resec-
tion to preserve facial nerve integrity, there wereadditional indications for this technique in a fewpatients. One patient had a near-total resectionafter experiencing bradyarrhythmias during dis-section of the tumor from the brain stem. Fourpatients had planned incomplete resections forother reasons, including advanced age and medicalcomorbidities. Finally, 4 patients had subtotal re-sections after initial treatment with stereotacticradiotherapy failed. Of these, 3 patients had aventriculoperitoneal shunt placed preoperativelyto treat hydrocephalus and subsequently under-went a planned subtotal resection for brain stemdecompression. The time interval between failedradiotherapy and operative intervention was from3 to 17 months. Three of 4 of these patients had noevidence of recurrence at 3 years (the fourth pa-tient was lost to follow-up).
Facial Nerve OutcomesGood facial nerve function at 1 year postoper-
atively, defined as HB grade I or II, was seen in 57(81%) of the 65 patients (Table 3). There were nodetectable associations between good facial nervefunction and tumor size (P � 0.98), age (P �0.41), or approach (P � 0.66). Logistic regressionanalysis demonstrated no statistically significantdifference in good facial nerve function betweenthe near-total and subtotal groups when control-ling for age, tumor size, and operative approach (P� 0.1).
Radiographic ImagingSixty-four patients had imaging available for at
least 1 year postoperatively, with a mean radio-graphic follow-up period of 4.3 years (range, 1 to13 years). Imaging revealed the residual tumor inapproximately 20% of patients in the near-totalgroup and 80% of patients in the subtotal group(Figs 2 and 3). The proportion of scans at eachyear that revealed tumor remained relatively stableover the study period.
Recurrence RiskThe risk of developing a tumor recurrence was
determined in a subgroup of 52 patients who metthe criteria for adequate follow-up, as described inMethods. The mean follow-up time for these pa-tients was 5 years (maximum, 13 years). Recur-rences were seen in 1 (3%) of 33 patients who hada near-total resection compared with 6 (32%) of19 patients who had a subtotal resection. Multiplelogistic regression analysis was then performed toadjust for differences in follow-up time and largetumor size (�25 mm). From this analysis, theodds ratio for recurrence was found to be 12 timeslarger for subtotal than for near-total resections (P� 0.033) (Fig 4).
Seven patients had recurrent tumors (Table 4).All recurrences were seen following the TL ap-proach (Fig 5). The locations of the recurrenceswere in the mid-CPA, and none were encounteredin the internal auditory canal. The recurrent tu-mors were all large at the initial operation (mean,37 mm; P � 0.001); however, large size as a riskfactor for recurrence was not significant whencontrolling for subtotal resections (P � 0.32).There was no association between patient age andrecurrence risk (P � 0.19). The mean time intervalfrom surgery to the detection of a recurrence was3 years (range, 1 to 5 years). Stereotactic radiationtreatment was recommended in 5 patients. Theremaining 2 patients underwent a repeat incom-plete resection with the RS approach (1 NT and 1ST).
DISCUSSIONThe rationale for using an incomplete tumor
dissection technique is dictated by the risk/benefitratio for the patient. Our data suggest that the riskof tumor recurrence after a near-total resection is
Table 2. Complications
ComplicationNear-total(n � 50)
Subtotal(n � 29)
Cerebrospinal fluid leak* 8 1Meningitis (aseptic) 2 1Wound infection 3 0Cerebellar peduncular infarct 2 0Deaths 0 0
*Two required surgery, and 7 were treated with a lumbar drain.
Otolaryngology–Head and Neck SurgeryVolume 130 Number 1 BLOCH et al 107

quite low. Although we did not perform a random-ized controlled trial to determine the degree ofimprovement in facial nerve outcomes, it seemslogical to conclude that any further tumor removalwould have compromised facial nerve function.Every patient in our study was selected because ofa particularly high level of tumor adherence. Com-parisons with stratified control patients who un-derwent a complete tumor resection would be in-herently flawed, because these patients did nothave tumors that were as difficult to dissect.
In our experience, substantial adherence of thetumor to the facial nerve has a high risk of a poorfacial nerve outcome. Near-total resection in-volves leaving a small rind of tumor to betterpreserve the facial nerve. Incomplete resection ishelpful in preserving facial nerve integrity becauseas the tumor enlarges, it compresses the facialnerve and the tumor–arachnoid mater plane islost.3 Difficulty in identifying a plane between thetumor and the facial nerve most commonly oc-curred just medial to the porus acousticus (Fig 1).The facial nerve, which follows the shape of the
tumor, often becomes splayed and thinned in thisregion, possibly accounting for the adherence.
Subtotal resection, in contrast, leads to a 12-time higher risk of recurrence. This may beexplained merely by the larger initial tumor sizein the subtotal group compared with the near-total group (P � 0.005), resulting in a moretenuous and adherent facial nerve. However,another explanation may be distinct variationsin AN biological behavior. Although most tu-mors are slow growing (approximately 2 mmper year),3,4 a small subset demonstrate rapidgrowth.5 One patient illustrating an aggressivevariant had a subtotal resection for a 25-mmtumor. She subsequently had 2 large symptom-atic cystic recurrences after a 2- to 3-year inter-val. We use the subtotal resection techniquewith large tumors that have a large area of tumorstuck to the facial nerve and/or brain stem or tominimize other complications, particularly inelderly or debilitated patients. Rarely, an intra-operative event is the indication for a subtotalresection.3 We favor a conservative approach
Table 3. Facial nerve function 1 year after surgery
House-Brackmann grade
I II III IV V VI
Near-total (n � 44) 23 (50%) 14 (30%) 8 (17%) 0 1 (2%) 0Subtotal (n � 21) 13 (54%) 7 (29%) 2 (8%) 1 (4%) 0 1 (4%)
Fig 2. (A) Near-total residual (arrow) seen in mid-CPA on MRI 1 year after an RS resection. The patient had been previouslytreated at another institution with an RS resection and presented with brain stem compression and a recurrence involvingthe internal auditory canal. (B) Subtotal residual seen on MRI following a TL resection. A thin rind (arrow) is seen alongthe brain stem extending to the porus acousticus.
Otolaryngology–Head and Neck Surgery
108 BLOCH et al January 2004

and often use the subtotal technique to treatpatients for whom stereotactic radiation hasfailed. This is done to minimize the attendantrisks engendered from radiation-induced
changes. Microsurgery is often difficult due toinflammation and fibrosis that interfere with theidentification of normal dissection planes, lead-ing to poorer facial nerve outcomes.6
Fig 3. Frequency of visible tumor remnants on postoperative enhanced MRI. A cross-sectional plot of patients at 1-, 3-, and�3-year MRI. Roughly 20% of the patients with near-total tumor resections had visible tumor on follow-up MRI, as opposedto the 80% of patients with subtotal resections. Because not all patients followed the recommended protocol of an annualscan, the number of patients at each time frame varies. Most studies were MRI (1 year: 53 MRI, 2 CT; 3 years: 26 MRI, 2 CT;�3 years:32 MRI, 1 CT). The average follow-up time for the patients in the �3-year category was 6.3 years.
Fig 4. Recurrence rates of near-total versus subtotal residuals (n � 52). Recurrence was determined by documentedgrowth or recommended treatment. No recurrence was defined by tumor that was stable on serial scans or not visible fora minimum of 3 years. The mean follow-up time was 5 years. There was a substantially higher risk of developing arecurrence if a subtotal resection (32%) was performed compared with a near-total resection (3%) (odds ratio, 12; P �0.033; details of multiple logistic regression analysis given in text).
Otolaryngology–Head and Neck SurgeryVolume 130 Number 1 BLOCH et al 109

However, we have a particular concern aboutperforming a subtotal resection in tumors withlarge cystic components. The cyst should not sim-ply be marsupialized; the wall needs to be care-fully microdissected from the surrounding normalstructures and removed. A tendency exists for theresidual cyst wall to reseal. Brain stem compres-sion may result from the cyst recurrence eventhough the solid (neoplastic) residual has notgrown. Stereotactic radiosurgery is not very effec-tive in such cystic recurrences because it is not
caused by rapid cell division. It is possible thatradiosurgery may even stimulate further cyst ex-pansion in such patients. Thus, a cystic recurrencelikely necessitates reoperation.
ANs do not have true capsules. The histopathol-ogy includes compressed neoplastic cells at themargin of the tumor surrounded by connectivetissue only a few micrometers in thickness.7 Theentire mass contains viable tumor cells that carrythe potential for recurrence. Thus, “complete re-section leaving only a small amount of capsule” is
Table 4. Characteristics of patients with recurrent tumors
Age*(yr)
Initial tumorsize† (mm) Resection Approach
Yearrecurred/treated Treatment Reason for retreatment
ST NT
72 25 X TL 3/8 SR Growth continued (18 mm)54 40 X TL 5/5 SR66 32 X TL 5/5 MS Hydrocephalus (31 mm)51 65 X TL 3/5 SR Growth continued (21 mm)70 35 X TL 1/1 Proton therapy Hydrocephalus (40 mm)67 35 X TL 3/3 SR78 25 X TL 2/2 MS 30 mm, then developed another
35 mm recurrence (3 yearslater)
*P � 0.19; †P � 0.001; ST, Subtotal; NT, near-total; TL, translabyrinthine; SR, stereotactic radiation; MS, microsurgical (retrosigmoid approachused in both cases).
Fig 5. (A) Near-total recurrence (arrow) seen on MRI 8 years after a TL resection. The tumor recurrence was detected ona 3-year scan and has continued to grow asymptomatically from 3 mm to 18 mm at 8 years after surgery (first patient,Table 4). (B) Subtotal recurrence (arrow) in the mid-CPA seen on MRI 3 years after a TL resection (sixth patient, Table 4).
Otolaryngology–Head and Neck Surgery
110 BLOCH et al January 2004

really incomplete tumor removal. Based on thevolume of tumor and “capsule” remaining, it isbest defined as a near-total or subtotal removal.Every effort should be made to remove as much ofthe tumor as possible while only leaving a smallrind at areas with difficult planes of dissection.Limiting the gross volume of residual tumor hasbeen shown to improve outcome.8 One of thepitfalls in performing an incomplete resection oc-curs with the RS approach when tumors are trun-cated at the internal auditory canal without drillingout the intracanalicular component. We do notrecommend this technique because these extensiveresiduals carry a high risk of recurrence. Indeed,even the need to perform a “blind sweep” of thefundus after a proper internal auditory canal drill-out with the RS approach carries a higher inci-dence of tumor recurrence.9
In contrast, all of the recurrences in our studywere centered in the CPA and followed a TLresection. Because the majority of the near-totalremnants and some of the subtotal remnants re-mained undetectable on serial follow-up imaging,we suspect that there was postoperative tumorregression. Other plausible explanations includetumor necrosis, detection limitations of the MRI,or an interruption of the blood supply preventingcontrast enhancement. Residual remnants havebeen shown to be relatively avascular in a studylooking at tumors managed with staged proce-dures.3 Nonetheless, the bipolar electrocauteryshould be used to coagulate the remnant to causefurther devascularization. The location of remnantappears to influence the recurrence risk. The bloodsupply of the internal auditory canal and brainstem may lead to an increased propensity for re-currence in these locations compared with rem-nants along the facial nerve in the mid-CPA thathave a poor vascular supply.
The mean time interval between surgery andtumor recurrence was 3 years (range, 1 to 5 years).All recurrences were seen on either the initialpostoperative scan or serial scans that demon-strated growth. No patients had a clinical recur-rence after an established quiescent period. This iscontrasted by a study that revealed tumor growthin 17 patients after a median of 3.6 years with noevidence of tumor growth.8 These conflicting ob-servations may be explained by the use of lower-
sensitivity CT scanning for follow-up in the otherstudy. Consistent with our findings was that oncegrowth was identified, it continued unabated untilinstitution of treatment.8
AN recurrences are often asymptomatic due tothe typical postoperative sequelae of hearing lossand vestibular ablation. It is imperative to followthese patients diligently with other diagnostic mo-dalities that permit early detection and interven-tion before the need for urgent decompressionsurgery. The pre– and post–gadolinium enhancedT1-weighted MRI with fat saturation is the imag-ing of choice due to signal characteristics thatallow the differentiation of postoperative scarring,blood, and fat graft from tumor.10
Treatment options for a recurrent tumor includestereotactic radiosurgery or reoperation typicallydone via a different approach. In this series, allrecurrences followed TL removals, presumably be-cause this is the method typically used for tumors inthe size range where less-than-complete removal ismost likely to be chosen. When a reoperation isneeded following the TL approach, we choose theRS method to avoid having to dissect the fat graft offof the facial nerve. Similarly, we use the TL ap-proach to manage recurrences after other surgeonshave left tumor (particularly in the internal auditorycanal) during an RS approach to avoid the region ofsurgical scarring.
CONCLUSIONThere has been an evolution in the management
of ANs reflecting advances made in medical tech-nology and an improved understanding of the nat-ural progression of the disease. Historically, thegoal of complete tumor removal took precedenceover other considerations. Patients often presentedwith advanced disease, leading to unacceptabledeath rates. Today, high-quality imaging oftenleads to the diagnosis in patients with less severesymptoms and smaller tumors. A therapeutic di-lemma arises when balancing the risk and benefitsof a complete versus a less-than-complete resec-tion of a benign tumor. Near-total resection has alow risk of recurrence and may be used in anypatient as a concession to neural integrity. There isa substantially higher risk of recurrence with sub-total resections. Meticulous attention is needed tothin the tumor remnant as much as possible, limit
Otolaryngology–Head and Neck SurgeryVolume 130 Number 1 BLOCH et al 111

it to the CPA, and coagulate it with the electro-cautery. The postoperative management should in-clude vigilant surveillance with serial MRI to de-tect early recurrence. Detection of recurrenttumors was evident relatively early within the first5 years after surgery.
The authors extend their appreciation to Charles McCul-loch, PhD, for statistical analysis.
REFERENCES1. Jackler RK. Atlas of neurotology and skull base surgery.
St Louis: Mosby; 1996, p 306.2. Hegarty JL, Jackler RK, Rigby PL, et al. Distal anterior
inferior cerebellar artery syndrome after acoustic neu-roma surgery. Otol Neurotol 2002;23:560-71.
3. Comey CH, Jannetta PJ, Sheptak PE, et al. Staged re-moval of acoustic tumors: techniques and lessons learnedfrom a series of 83 patients. Neurosurgery 1995;37:915-20; discussion 20-1.
4. Schessel DA, Nedzelski JM, Kassel EE, et al. Recurrencerates of acoustic neuroma in hearing preservation sur-gery. Am J Otol 1992;13:233-5.
5. Bederson JB, von Ammon K, Wichmann WW, et al.Conservative treatment of patients with acoustic tumors.Neurosurgery 1991;28:646-50; discussion 50-1.
6. Battista RA, Wiet RJ. Stereotactic radiosurgery foracoustic neuromas: a survey of the American Neurotol-ogy Society. Am J Otol 2000;21:371-81.
7. Kuo TC, Jackler RK, Wong K, et al. Are acoustic neu-romas encapsulated tumors? Otolaryngol Head NeckSurg 1997;117:606-9.
8. El-Kashlan HK, Zeitoun H, Arts HA, et al. Recurrence ofacoustic neuroma after incomplete resection. Am J Otol2000;21:389-92.
9. Roberson JB Jr, Brackmann DE, Hitselberger WE.Acoustic neuroma recurrence after suboccipital resection:management with translabyrinthine resection. Am J Otol1996;17:307-11.
10. Battista RA, Bojrab DI, Wang AM. Evaluation of resid-ual acoustic schwannoma using gadolinium-DTPA en-hanced magnetic resonance imaging with the fat suppres-sion technique. Am J Otol 1995;16:628-33.
Otolaryngology–Head and Neck Surgery
112 BLOCH et al January 2004

Is It Worthwhile to Attempt Hearing Preservation inLarger Acoustic Neuromas?
*Philip D. Yates, *†Robert K. Jackler, *Bulent Satar, *†Lawrence H. Pitts, and*John S. Oghalai
Departments of *Otolaryngology-Head and Neck Surgery and †Neurologic Surgery, University ofCalifornia, San Francisco, California, U.S.A.
Objective: To determine the hearing outcome in patients un-dergoing surgery via the retrosigmoid approach for acousticneuromas with a substantial component in the cerebellopon-tine angle.Study Design: Retrospective case review.Setting: Tertiary referral center.Patients: The medical records of all patients undergoing acous-tic neuroma removal via the retrosigmoid approach at a tertiaryreferral center were retrospectively reviewed. Sixty-four pa-tients with both cerebellopontine angle component �15 mmand preoperative audiometry of class A or B (American Acad-emy of Otolaryngology–Head and Neck Surgery) were identified.Main Outcome Measures: Postoperative average pure tonethreshold and word recognition scores, categorized accordingto the classification of the American Academy of Otolaryn-gology–Head and Neck Surgery, were used to assess hearingoutcome.Results: Overall, only 6.3% (4 of 63) retained good hearing(class A or B) postoperatively. Hearing preservation rate in thesmallest (15- to 19-mm) group was 17.6% (3 of 17), which wasbetter than that for the larger groups. No successful hearing
preservation was achieved in tumors with �25 mm cerebel-lopontine angle component (0 of 23).Conclusions: Surgeon and patient alike would always choose ahearing preservation technique if there was no potential forincreased morbidity in making the attempt. When comparedwith the non–hearing preservation translabyrinthine approach,the retrosigmoid approach had a higher incidence of persistentheadache. In addition, efforts to conserve the auditory nerveprolong operating time, increase the incidence of postoperativevestibular dysfunction, and carry a slightly higher risk of tumorrecurrence. Nevertheless, even though the probability of suc-cess is disappointingly small, when excellent hearing is presentwe favor offering the option of a hearing conservation attemptwhen the patient has been well informed of the pros and consof the endeavor. Factors weighing against undertaking this ef-fort include larger cerebellopontine angle component (�25mm), deep involvement of the fundus, wide erosion of theporus, and marginal residual hearing. Key Words: Acousticneuroma (vestibular schwannoma)—Hearing preservation—Retrosigmoid approach.Otol Neurotol 24:460–464, 2003.
The three principal surgical approaches for acousticneuroma (AN) removal are the translabyrinthine (TL),retrosigmoid (RS), and middle fossa (MF) approach.Only the latter two approaches provide the possibility ofhearing preservation. The results of hearing preservationsurgery have been shown to be superior for small tumorswhen the MF approach is used (1). However, the MFapproach is only practicable in tumors with a limitedcerebellopontine angle (CPA) extension. This leaves theRS approach as the only alternative when attempting topreserve hearing in larger ANs. Because tumor size is themost important variable influencing hearing outcome,the question arises as to whether hearing preservationsurgery should still be attempted via the RS approach inpatients with large tumors but serviceable hearing (2–5).
Tumor size itself should not be a criterion in choosingbetween the RS and TL approach, because both ap-proaches provide adequate exposure, but the potentialhigher morbidity associated with the RS approach doesneed to be taken into account. This study was undertakento determine the rate of hearing preservation in patientswith ANs that have a substantial CPA component (� 15mm) so that patients can be appropriately counseled be-fore choosing between a RS and TL approach.
PATIENT POPULATION
This study is a retrospective review of the medical records ofpatients who have had surgical removal of a histologically con-firmed AN in a single tertiary referral center between the years1984 and 2001. Selection criteria for inclusion in the studywere tumor removal via the RS approach, �15 mm CPAcomponent, and preoperative hearing of class A or B. Becausenot every patient with a �15 mm AN and preoperative hearing
Address correspondence and reprint requests to Robert K Jackler,M.D., University of California Hospital, 400 Parnassus Avenue, Ste.A-730, San Francisco, CA 94143–0342, U.S.A. Email: [email protected]
Otology & Neurotology24:460–464 © 2003, Otology & Neurotology, Inc.
460

of class A or B was operated on via the RS approach in theinstitutional series, some selection bias may be present. Severalotherwise qualified patients underwent TL removal, especiallywhen adverse predictors, such as deep penetration of the fundusof the internal acoustic canal (IAC) or wide erosion of the porusacousticus, were present. These criteria would have been ana-lyzed in the present study were the data available in our medi-cal records more complete. Arbitrary patient preference wasalso sometimes a factor in the choice of operative approach.
Hearing class was documented as recommended by theCommittee on Hearing and Equilibrium of the American Acad-emy of Otolaryngology–Head and Neck Surgery (AAO-HNS)(6). Tumor size was defined as the largest diameter of the CPAportion of the tumor measured from axial magnetic resonanceimaging (MRI) scan or axial computerized tomography (CT)scan if MRI was not available. The patients were divided intothe following four groups according to tumor size: 15 to 19mm, 20 to 24 mm, 25 to 29 mm, and �30 mm. The pure tonethresholds at 0.5, 1, 2, and 3 kHz (4 kHz was used when 3kHzwas not recorded) were averaged, and this pure tone average(PTA) was used along with the best speech discriminationscore (SDS) to determine hearing class according to the nomo-gram provided in the AAO-HNS guidelines. SDS is reported atsensation levels of up to 40 dB or maximum comfortable loud-ness, whichever is less. This system was used to classify bothpreoperative and postoperative hearing results.
Several other parameters were recorded at the time of datacollection, including age, sex, side of tumor, extent of tumorresection, and facial nerve function. The extent of tumor resec-tion was categorized as total, near total (indicating a small areaof tumor capsule no more than 2 mm thick and 5 mm in di-ameter was left to protect a splayed and adherent facial nerve),or subtotal (indicating a larger remnant of tumor). Postopera-tive facial nerve outcome was reported according to the House-Brackmann grading system (7).
Statistical analysis was performed in SPSS program for Win-dows (Release 7.5, 1996), and statistical significance was set atp < 0.05. Each tumor-size category was compared with theothers in paired comparisons. Age, preoperative PTA and SDS,and postoperative PTA and SDS were compared using Mann-Whitney U test. Intergroup comparison of preoperative andpostoperative hearing class was made using Pearson’s �2 test.
To compare our results with those of other centers perform-ing AN surgery, a review of the literature was performed. Aliterature search was performed on MEDLINE using the key-words acoustic neuroma, hearing preservation, and retrosig-moid approach. If more than one series had been published bya single center, the most recent results were reviewed.
Approval for the study design was obtained from the Uni-versity of California, San Francisco Committee on Human Re-search.
RESULTS
Sixty-four patients with unilateral AN met the inclu-sion criteria, only one of whom had to be excluded be-cause of inadequate follow-up. The series included 39female and 24 male patients. The tumor was left-sided in38 cases and right-sided in 25 cases. We suspect thesetwo numerical asymmetries to have occurred by chance.Total tumor resection was achieved in 49 cases, and neartotal removal in 14 cases. No tumors were subtotallyremoved. The mean age of the patients was 45 years
(range, 17 to 70). The facial nerve outcomes at 1 yearwere as follows: grade 1 or 2 � 54 (86%), grade 3 or 4� 6 (10%), and grade 5 or 6 � 3 (5%).
Postoperative hearing was compared with preopera-tive hearing for each tumor size group (Table 1). Goodhearing (class A or B) was preserved in only 6.3% (4 of63) of patients. All of the successes in hearing conser-vation came in the smaller size groups. No patient with atumor �25 mm in CPA diameter retained hearing in thisstudy. The most favorable results were obtained in thesmallest (15 to 19 mm) size group, in which 17.6% (3 of17) retained good hearing.
No statistical significance was observed between anyof the tumor size groups when comparing age and pre-operative SDS. The preoperative PTA in the �30 mmgroup was significantly better than in the 15- to 19-mmgroup (p � 0.043). The postoperative PTA in the 15- to19-mm group was significantly better than in the 20- to24-mm group (p � 0.042), the 25- to 29-mm group (p �0.024), and the �30-mm group (p � 0.031). The post-operative SDS was significantly better in the 15- to 19-mm group than in the 25- to 29-mm group (p � 0.044),but no significant difference was observed in other groupcomparisons. When comparisons were made for preop-erative hearing class between groups, no statistically sig-nificant difference was observed. There was also no dif-ference observed when hearing preservation rates (i.e.,numbers of postoperative class A or B results) were com-pared across groups.
DISCUSSION
The aim of AN surgery is tumor removal with minimalassociated morbidity. The rate of functional preservationof the cochlear nerve has increased with the developmentof modern microsurgical techniques and intraoperativenerve monitoring. Hearing conservation is possible, incertain cases, using either the MF or RS approach. Fortumors with limited extension into the CPA, the MFapproach has become the method of choice in severalmajor centers. A recent study carried out in our depart-ment has demonstrated that more than 60% of tumorswith less than 10 mm of CPA extension operated on bythe MF approach will retain functional hearing (class Aor B), and approximately 95% of these patients will
TABLE 1. Cross-reference of preoperative andpostoperative hearing [AAO-HNS class (9)]
Intracranialsize (mm) (n)
Preoperativeclass
Postoperative hearing (n)
A B C D
15–19 (%) (17) A 0 11.8 (2) 0 35.3 (6)B 0 5.9 (1) 11.8 (2) 35.3 (6)
20–24 (%) (23) A 0 4.3 (1) 0 47.8 (11)B 0 0 0 47.8 (11)
25–29 (%) (12) A 0 0 0 50 (6)B 0 0 0 50 (6)
�30 (%) (11) A 0 0 0 81.8 (9)B 0 0 0 18.2 (2)
461ACOUSTIC NEUROMA: HEARING PRESERVATION SURGERY
Otology & Neurotology, Vol. 24, No. 3, 2003

maintain good (grade 1 or 2) facial nerve function. Tu-mors with a larger CPA component (10 to 19 mm) had asignificantly lower rate of hearing preservation (34%),along with a lower rate of good facial nerve outcome(81%) (8). Because the MF approach is not suitable forremoval of tumors with more than minor brainstemcontact, attempts at hearing conservation in tumors ex-ceeding approximately 18 mm are feasible only via theRS approach.
In an earlier study, a comparative analysis between theMF and RS approaches for small ANs (<10 mm CPAcomponent) revealed markedly greater success for theMF approach in these small tumors (1). Compared withour results using the MF approach (for smaller tumors),hearing preservation rates after RS procedures can onlybe described as disappointing. In the present study, goodhearing (A or B) was retained in only 10% of tumorsmeasuring 15 to 24 mm and in no tumors with �25 mmin the CPA.
A review of the literature identified a total of 21 stud-ies that contained data on a significant number of tumorsof �15 mm and focused on hearing preservation surgeryby the RS approach (2,4,9–27). Unfortunately, many ofthese studies provide insufficient data to undertake ananalysis stratified by tumor according to the AAO-HNShearing classification. Among those that do, some adhereto the AAO-HNS guidelines by reporting tumor size inthe CPA (Table 2), whereas others report size of theentire tumor, including the IAC portion (Table 3)(2,9,13–15,22–24,26). The latter method may overesti-mate tumor size by as much as 10 mm. The data fromone study is presented by virtue of its large patient popu-lation despite its use of noncomparable measures forboth hearing and tumor size (Table 4) (24). An importantlimitation of this particular study was that SDSs were
only available in 76% of cases preoperatively and in only50% of patients with some hearing postoperatively.
All of the studies demonstrated decreasing success inhearing preservation with larger tumor sizes. Amongthose studies reporting CPA diameter, most results aremore or less comparable with our own for smaller tu-mors, except for the Mount Sinai series, which, althoughsmall in numbers of patients, is somewhat better (Table2) (23). Results for larger tumors (�30 mm) are gener-ally modest, although, in contrast to our own experience,a few successes were recorded. Reviewing the four serieswith a �30 mm category, 9.1% (3 of 33) of these largetumors retained hearing of class A or B. It is of interestto consider studies using the entire tumor diameter (in-cluding the IAC), because, in aggregate, they represent asizable patient population (Table 3). However, the dif-ferent method of measurement precludes meaningfulcomparison.
Both surgeon and patient alike would always select ahearing-conservative approach, no matter how remote
TABLE 4. Hearing preservation via the retrosigmoidapproach in patients with good preoperative hearing using
the new Hannover hearing classification and tumormeasurement system
StudyTumor size*
(n)
Postoperative hearing†(% (n)]
H1 or 2 H3, 4, or 5
Samii et al. (11) T2 (65) 36.9 (24) 63.1 (41)T3 (162) 24.7 (40) 75.3 (122)T4 (81) 4.9 (4) 95.1 (77)
*New Hannover classification for tumor extension (11): T1, purelyintrameatal; T2, intrameatal and extrameatal; T3a, filling the cerebel-lopontine cistern; T3b, reaching the brain stem; T4a, compressing thebrain stem; T4b, severely dislocating the brain stem and compressingthe fourth ventricle.
†New Hannover classification for hearing: H1, 0 to 30 dB and 100%to 70% SDS; H2, 31 to 50 dB and 69% to 50% SDS; H3, 51 to 90 dBand 49% to 5% SDS; H4, 91 to 120 dB and 4% to 1% SDS; H5, �120dB and 0% SDS.
TABLE 2. Hearing preservation via the RS approach inpatients with good preoperative hearing (class A or B);
studies in which tumor measurement was reported in termsof the diameter of the CPA component
StudyTumor size[mm (n)]
Postoperative hearing class (% n)
A or B C or D
Present study 15–19 (17) 17.6 (3) 82.4 (14)20–24 (23) 4.3 (1) 95.7 (22)25–29 (12) 0 100 (12)
�30 (11) 0 100 (11)Wiet et al (8) 16–20 (12) 16.7 (2) 83.3 (10)
21–25 (11) 0 100 (11)26–30 (7) 14.3 (1) 85.7 (6)
�30 (2) 0 100 (2)Gormley et al (12) 20–39 (24) 25 (6) 75 (18)
�40 (3) 0 100 (3)Post et al (14) 15–19 (15) 40 (6) 60 (9)
20–24 (9) 11.1 (1) 88.9 (8)25–29 (7) 14.3 (1) 85.7 (6)
�30 (7) 28.6 (2) 71.4 (5)Cohen et al (15) 15–19 (37) 18.9 (7) 81.1 (30)
20–24 (10) 0 100 (10)25–29 (11) 0 100 (11)
�30 (13) 7.7 (1) 92.3 (12)
TABLE 3. Hearing preservation via the RS approach inpatients with good preoperative hearing (class A or B);
series in which tumor measurement was reported as entiretumor size including both IAC and CPA components
StudyTumor size[mm (n)]
Postoperative hearing [% (n)]
A or B C or D
Moffat et al (9) 15–24 (19) 5.3 (1) 94.7 (18)25–34 (6) 16.7 (1) 83.3 (5)35–44 (4) 0 100 (4)
�45 (1) 0 100 (1)Fahlbusch et al (10) 20–24 (7) 28.6 (2) 71.4 (5)
25–29 (13) 7.7 (1) 92.3 (12)�30 (29) 17.2 (5) 82.8 (24)
Arriaga et al (13) 15–19 (10) 70 (7) 30 (3)20–24 (4) 25 (1) 75 (3)25–29 (2) 50 (1) 50 (1)
�30 (2) 50 (1) 50 (1)Fischer et al (16) 20–29 (39) 5 (2) 95 (37)
�30 (30) 10 (3) 90 (27)
462 P. D. YATES ET AL.
Otology & Neurotology, Vol. 24, No. 3, 2003

the chance of success, were there not some additionalmorbidity from having made the attempt. In this case,intelligent clinical decision making requires a quantita-tive assessment of associated morbidities such as facialfunction, balance, cerebrospinal fluid (CSF) leak, persis-tent headache, operating time, and tumor recurrence.
Facial function is widely considered to be a most im-portant criterion for success in AN surgery. An earlieranalysis of size-matched tumors comparing the RS andTL approaches in our own series detected no differencein outcome (28). These findings are supported by severalother studies on this subject (26,29,30). Although theultimate results may be similar, preserving the auditorynerve occasionally makes the facial nerve dissectionmore tedious and time consuming. A clean proximal (atthe brain stem exit) and distal (in the IAC) division of theentire eighth nerve helps to establish the facial nervedissection plane and thus facilitates more rapid removal.During dissection from the region of greatest adherence,typically just outside of the porus acousticus, visualiza-tion of the facial nerve can be obscured by overlyingsplayed and sometimes adherent fibers of the eighthnerve. Thus, although choice of a hearing conservationRS approach may not alter facial nerve functional out-come, it may prolong surgery.
The RS approach requires a greater degree of cerebel-lar retraction than the TL approach. Although postopera-tive T2-weighted MRI images often show a greater de-gree of cerebellar encephalomalacia after a RS approach,we have not noted a particular tendency toward ataxia.Another factor on balance outcome is the effect of leav-ing residual vestibular nerve fibers in the course of ahearing conservation attempt. To maximize the possibil-ity of hearing preservation, most surgeons leave intactfibers of the eighth nerve that are not involved by tumor.These vestibular nerve remnants may generate perverseimpulses that hinder vestibular compensation. It is ouranecdotal impression that patients undergoing hearingconservation attempts are at higher risk of suffering per-sistent vestibular symptoms, although our results haveyet to be studied formally.
A recent retrospective study conducted in our depart-ment compared CSF leak rates among the different ap-proaches used for AN surgery (31). With 100 surgeries ineach cohort, this study identified no statistically signifi-cant difference in CSF leakage rates between the RS(10%) and TL (13%) approaches. Equally, there was nodifference in the requirement for surgical closure of theCSF leak (3% of RS and 4% of TL patients). The findingthat there is no difference seen in CSF leaks betweenthese approaches is supported by data published in arecent study by Brennan et al. (32).
Prolonged postoperative headache is a recognizedcomplication of AN surgery that may have significantmorbidity for the patient (33–35). A recent study byLevo et al. (36) demonstrated that the RS approach car-ried a 3.8-times higher risk than the TL approach forpostoperative headache. A study performed in our de-partment has also confirmed a substantially higher inci-
dence of postoperative headache after RS surgery com-pared with the TL approach (unpublished data). Attemptshave been made to reduce the rate of postoperative head-ache after the RS approach by performing craniotomyinstead of craniectomy. Although this technique has beenshown to produce significantly reduced postoperativeheadache rate, a study by Ruckenstein et al. (38) dem-onstrated that, despite the performance of a cranioplasty,patients undergoing RS craniotomies experience signifi-cantly more postoperative pain than those patients hav-ing undergone TL resections (37–39).
The RS approach seems to have a higher rate of tumorrecurrence that the TL. Although the TL method affordsdirect microsurgical exposure of the entire length of theIAC, when attempting hearing conservation via the RSapproach, it is possible to visualize only approximatelythe medial two thirds of the canal (40). Although thefundus could be visualized directly via the RS route, thisnecessitates removal of a portion of the inner ear and thusprecludes hearing preservation. When the lateral onethird of the IAC is involved with tumor, the surgeon mayelect to blindly dissect the portion in the fundus usingangled instruments that reach beneath the overhanginginner ear. In such cases, a small button of tumor caneasily be left in the canal’s distal recess. Because such aremnant has an intact blood supply, it has the potential togenerate a recurrence. Indeed, this phenomenon of re-growth from residual tumor left in the fundus during aRS hearing conservation approach is well-known (41).The incidence of its occurrence, however, is not known.Endoscopic inspection of the fundus has been proposedas a means of reducing this risk (42). Because of thisheightened risk of recurrence, we consider tumor in-volvement of the lateral one third of the IAC to be afactor weighing against choice of the RS technique.
It is our hope that the outcome data provided in thisstudy, together with those of others, will help surgeonsand patients with larger ANs to select an approach totheir tumor that maximizes the probability of favorableoutcome. To some extent, it depends on the valuation thepatient places on his or her residual hearing. To helpdetermine this, we encourage patients to wear an earplugin the tumor ear for a few days, to assess how muchdifficulty this poses in day-to-day life. If it has littleimpact, then the RS hearing conservation approach isprobably not worth attempting because of the potentialgreater morbidity. Because of the numerous outcomevariables involved, as well as the vicissitudes of patientpreference, it is not practical to adhere to a formula-driven decision tree. By way of illustration, we wouldencourage using the RS approach to attempt hearingpreservation for a 20-mm tumor with normal hearing,minimal involvement of the proximal IAC, and no poruserosion and discourage its use for a 35-mm tumor withmarginal class B hearing that deeply invades the fundusand widely erodes the porus. A special circumstance,worthy of mention, is a CPA tumor that is suspected ofbeing other than an AN (e.g., meningioma). In suchcases, hearing preservation is much more probable than
463ACOUSTIC NEUROMA: HEARING PRESERVATION SURGERY
Otology & Neurotology, Vol. 24, No. 3, 2003

with eighth nerve tumors, and the RS approach is welljustified.
Finally, we would like to make mention of the diffi-culty encountered in performing meaningful meta-analysis of the published literature in this field. Thelimitations posed by use of noncomparable data presen-tations highlight the need for investigators to use com-parable minimal reporting standards (such as thoseadopted by the AAO-HNS) when conveying results afteracoustic neuroma surgery.
Acknowledgments: Philip Yates’ fellowship at Departmentof Otolaryngology-Head and Neck Surgery, University of Cali-fornia, San Francisco, was funded by the TWJ Foundation.
REFERENCES
1. Irving RM, Jackler RK, Pitts LH. Hearing preservation in patientsundergoing vestibular schwannoma surgery: comparison of middlefossa and retrosigmoid approaches. J Neurosurg 1998;88:840–5.
2. Cohen NL, Lewis WS, Ransohoff J. Hearing preservation in cer-ebellopontine angle tumor surgery: the NYU experience 1974–1991. Am J Otol 1993;14:423–33.
3. Dornhoffer JL, Helms J, Hoehmann DH. Hearing preservation inacoustic tumor surgery: results and prognostic factors. Laryngo-scope 1995;105:184–7.
4. Nadol JB Jr, Chiong CM, Ojemann RG, et al. Preservation ofhearing and facial nerve function in resection of acoustic neuroma.Laryngoscope 1992;102:1153–8.
5. Shelton C. Hearing preservation in acoustic tumor surgery. Oto-laryngol Clin North Am 1989;25:609–621.
6. Committee on Hearing and Equilibrium. Committee on Hearingand Equilibrium guidelines for the evaluation of hearing in acous-tic neuroma (vestibular schwannoma). Otolaryngol Head NeckSurg 1995;115:179–80.
7. House JW, Brackmann DE. Facial nerve grading system. Oto-laryngol Head Neck Surg 1985;93:146–7.
8. Satar B, Jackler RK, Oghalai JS, et al. Risk-benefit analysis ofusing the middle fossa approach for acoustic neuromas with >10mm cerebellopontine angle component. Laryngoscope 2002;112:1500–06.
9. Arriagia MA, Chen DA, Fukushima T. Individualizing hearingpreservation in acoustic neuroma surgery. Laryngoscope 1997;107:1043–7.
10. Baldwin DL, King TT, Morrison AW. Hearing conservation inacoustic neuroma surgery via the posterior fossa. J Laryngol Otol1990;104:463–7.
11. Cerullo LJ, Grutsch JF, Heiferman K, et al. The preservation ofhearing and facial nerve function in a consecutive series of unilat-eral vestibular nerve schwannoma surgical patients (acoustic neu-roma). Surg Neurol 1993;39:485–93.
12. Ebersold MJ, Harner SG, Beatty CW, et al. Current results of theretrosigmoid approach to acoustic neurinoma. J Neurosurg 1992;76:901–9.
13. Fahlbusch R, Neu M, Strauss C. Preservation of hearing in largeacoustic neurinomas following removal via suboccipito-lateral ap-proach. Acta Neurochir 1998;140:771–8.
14. Fischer G, Fischer C, Remond J. Hearing preservation in acousticneurinoma surgery. J Neurosurg 1992;76:910–7
15. Gormley WB, Sekhar LN, Wright DC, et al. Acoustic neuromas:results of current surgical management. Neurosurgery 1997;41:50–8.
16. Harner SG, Fabry DA, Beatty CW. Audiometric findings in pa-tients with acoustic neuroma. Am J Otol 2000;21:405–11.
17. Holsinger FC, Coker NJ, Jenkins HA. Hearing preservation inconservation surgery for vestibular schwannoma. Am J Otol 2000;21:695–700.
18. Kaylie DM, Gilbert E, Horgan MA, et al. Acoustic neuroma sur-gery outcomes. Otol Neurotol 2001;22:686–9.
19. Kemink JL, LaRouere MJ, Kileny PR, et al. Hearing preservation
following suboccipital removal of acoustic neuromas. Laryngo-scope 1990;100:597–602.
20. Levo H, Blomstedt G, Pyykko I. Is hearing preservation worth-while in vestibular schwannoma surgery? Acta Otolaryngol Suppl2000;543:26–7.
21. Mazzoni A, Calabrese V, Danesi G. A modified retrosigmoid ap-proach for direct exposure of the fundus of the internal auditorycanal for hearing preservation in acoustic neuroma surgery. Am JOtol 2000;21:98–109.
22. Moffat DA, da Cruz MJ, Baguley DM, et al. Hearing preservationin solitary vestibular schwannoma surgery using the retrosigmoidapproach. Otolaryngol Head Neck Surg 1999;121:781–88.
23. Post KD, Eisenberg MB, Catalano PJ. Hearing preservation investibular schwannoma surgery: what factors influence outcome? JNeurosurg 1995;83:191–6.
24. Samii M, Matthies C. Management of 1000 vestibular schwanno-mas (acoustic neuromas): hearing function in 1000 tumor resec-tions. Neurosurgery 1997;40:248–60.
25. Torrens M, Maw R, Coakham H, et al. Facial and acoustic nervepreservation during excision of extracanalicular acoustic neuromasusing the suboccipital approach. Br J Neurosurg 1994;8:655–65.
26. Wiet RJ, Mamikoglu B, Odom L, et al. Long-term results of thefirst 500 cases of acoustic neuroma surgery. Otolaryngol HeadNeck Surg 2001;124:645–51.
27. Yokoh A, Kobayashi S, Tanaka Y, et al. Preservation of cochlearnerve function in acoustic neurinoma surgery. Acta Neurochir(Wein) 1993;123:8–13.
28. Lalwani AK, Butt FY, Jackler RK, et al. Facial nerve outcome afteracoustic neuroma surgery: a study from the era of cranial nervemonitoring. Otolaryngol Head Neck Surg 1994;111:561–70.
29. Arriaga MA, Chen DA. Facial function in hearing preservationacoustic neuroma surgery. Arch Otolaryngol Head Neck Surg2001;127:543–6.
30. Nissen AJ, Sikand A, Welsh JE, et al. A multifactorial analysis offacial nerve results in surgery for cerebellopontine angle tumors.Ear Nose Throat J 1997;76:37–40.
31. Becker SS, Jackler RK, Pitts LH. CSF leak after acoustic neuromasurgery: a comparison of the translabyrinthine, middle fossa andretrosigmoid approaches. Otol Neurotol (in press).
32. Brennan JW, Rowed DW, Nedzelski JM, et al. Cerebrospinal fluidleak after acoustic neuroma surgery: influence of tumor size andsurgical approach on incidence and response to treatment. J Neu-rosurg 2001;94:217–23.
33. Harner SG, Beatty CW, Ebersold MJ. Headache after acousticneuroma excision. Am J Otol 1993;14:552–5.
34. Schessel DA, Rowed DW, Nedzelski JM, et al. Postoperative painfollowing excision of acoustic neuroma by the suboccipital ap-proach: observations on possible cause and amelioration. Am JOtol 1993;14:491–4.
35. Soumekh B, Levine SC, Haines SJ, et al. Retrospective study ofpostcraniotomy headaches in suboccipital approach: diagnosis andmanagement. Am J Otol 1996;17:617–9.
36. Levo H, Pyykko I, Blomstedt. Postoperative headache after sur-gery for vestibular schwannoma. Ann Otol Rhinol Laryngol 2000;109:853–8.
37. Koperer H, Deinsberger W, Jodicke A, et al. Postoperative head-ache after the lateral suboccipital approach: craniotomy versuscraniectomy. Minim Invasive Neurosurg 1999;42:175–8.
38. Ruckenstein MJ, Harris JP, Cueva RA, et al. Pain subsequent toresection of acoustic neuromas via suboccipital and translabyrin-thine approaches. Am J Otol 1996;17:620–4.
39. Wazen JJ, Sisti M, Lam, SM. Cranioplasty in acoustic neuromasurgery. Laryngoscope 2000;110:1294–7.
40. Blevins NH, Jackler RK. Exposure of the lateral extremity of theinternal auditory canal through the retrosigmoid approach: a radio-anatomic study. Otolaryngol Head Neck Surg 1994;111:81–90.
41. Roberson JB Jr, Brackmann DE, Hitselberger WE. Acoustic neu-roma recurrence after suboccipital resection: management withtranslabyrinthine resection. Am J Otol 1996;17:307–11.
42. McKennan KX. Endoscopy of the internal auditory canal duringhearing conservation acoustic tumor surgery. Am J Otol 1993;14:259–62.
464 P. D. YATES ET AL.
Otology & Neurotology, Vol. 24, No. 3, 2003

The LaryngoscopeLippincott Williams & Wilkins, Inc., Philadelphia© 2002 The American Laryngological,Rhinological and Otological Society, Inc.
Risk–Benefit Analysis of Using the MiddleFossa Approach for Acoustic Neuromas With�10 mm Cerebellopontine Angle Component
Bulent Satar, MD; Robert K. Jackler, MD; John Oghalai, MD; Lawrence H. Pitts, MD; Philip D. Yates, MD
Objectives: To evaluate hearing preservation andfacial nerve (FN) outcome in the middle fossa (MF)approach for acoustic neuromas with a cerebellopon-tine angle (CPA) component >10 mm. Study Design:Retrospective review of 193 patients. Patient Popula-tion: Patients were grouped according to tumor size:intracanalicular tumors (IC; 64), 1 to 9 mm CPA ex-tension (42), and 10 to 18 mm CPA extension (47).Additionally, a group of 40 patients (tumor size 10–18mm CPA extension) who had undergone a translaby-rinthine (TL) approach was studied to assess compar-ative FN outcome. Hearing and FN function weremeasured 1 year postoperatively. We defined the suc-cess at functional hearing preservation as AAO–HNSclass B or better and good FN outcome as House-Brackmann grade II or better. Results: For IC tumorsand those with up to 9-mm CPA extension, there wasno significant difference in the rate of functionalhearing preservation (62.2% vs. 63.1%, P � .931) andgood FN outcome (93.7% vs. 97.6%, P � .358). For tu-mors of 10- to 18-mm CPA extension, the rate of hear-ing preservation (34%) was lower than the othergroups (P � .006 and P � .009). In this group, the rateof good FN outcome was lower compared with the ICand 1- to 9-mm tumors (80.8% vs. 93.7%, P � .037 and97.6%, P � .012). The rate of good FN outcome follow-ing the TL approach in a comparable cohort of pa-tients was 100% (P � .003 in comparison with 10–18mm tumor resected with the MF approach). Conclu-sions: When considering surgical options, patientswith >10-mm tumors should be advised that choosingthe MF approach for hearing preservation carries asomewhat higher risk of persistent FN dysfunction.Key Words: Acoustic neuroma (vestibular schwanno-ma), middle fossa approach, hearing preservation, fa-cial nerve.
Laryngoscope, 112:1500–1506, 2002
INTRODUCTIONSurgeons who manage acoustic neuroma (AN) want
to select an operative approach that optimizes both tumorcontrol and functional outcome. Until relatively recently,the vast majority of AN surgery conducted around theworld used either the retrosigmoid (RS) or translabyrin-thine (TL) approach. Traditionally, the middle fossa (MF)approach has been reserved for small tumors confined tothe internal auditory canal (IAC). Over the last two de-cades, two teams (one each in Germany and Japan) haveadvocated for the use of the MF technique for larger tu-mors possessing a substantial component in the cerebel-lopontine angle (CPA).1,2 Over the last 5 years, the MFapproach has undergone a marked resurgence as a resultof its proven superiority over the RS approach in hearingconservation.3,4 The MF approach is currently used inbetween 30% and 50% of AN microsurgeries in certainmajor American centers.5
The use of the MF approach in tumors of 10 to 20 mmin diameter within the CPA remains controversial, be-cause few data exist concerning hearing preservation andfacial nerve function for tumors in this larger size range.Because the facial nerve (FN) lies in a surgically lessfavorable orientation when viewed from above (MF) asopposed to from the lateral perspective (TL or RS), concernhas been raised as to whether FN functional outcome isadversely affected. In an earlier study, we demonstratedthat choice of the MF approach for hearing preservationfor smaller tumors (�10 mm in diameter in the CPA)carries an increased risk of transient FN dysfunction, butthat that long-term outcome was similar to that with theRS approach.3 The intention of the present study is toascertain whether the enhanced hearing preservation ca-pability of the MF approach has an impact on long-termfacial function in larger tumors (�10 mm).
Patient PopulationThe primary study population consisted of a retro-
spective chart review of 153 MF resections for AN. Be-cause 3 patients with neurofibromatosis type 2 underwentstaged, bilateral approaches, the primary study group in-cluded 150 individuals. There were 76 female and 74 malepatients. All patients had a confirmed histopathologic di-
From the Departments of Otolaryngology–Head and Neck Surgery(B.X., R.K.J., J.O., L.H.P., R.D.Y.) and Neurosurgery (R.K.J., L.H.P.), University ofCalifornia, San Francisco, California, U.S.A.
Editor’s Note: This Manuscript was accepted for publication April 1,2002.
Send Correspondence to Robert K. Jackler, MD, Department of Oto-laryngology, University of California, San Francisco, 400 Parnassus Ave.Ste. A-730, San Francisco, CA 94143-0342, U.S.A. E-mail:[email protected]
Laryngoscope 112: August 2002 Satar et al.: Middle Fossa Approach for Acoustic Neuromas �10 mm
1500

agnosis of AN and had completed at least 1-year follow-up.Complying with the recommendations of the Committeeon Hearing and Equilibrium of the American Academy ofOtolaryngology–Head and Neck Surgery, tumor size wasestimated on axial enhanced-T1 magnetic resonance im-ages (MRI) by excluding the intracanalicular segment andmeasuring only the size of the CPA component.6 Tumorscompletely confined to the IAC were reported as an intra-canalicular (IC) tumor. For tumors extending out of theIAC, the largest linear diameter was measured in a direc-tion either parallel or perpendicular to the petrous ridge.Tumors were stratified into three size categories: IC (64),1–9 mm CPA (42), or 10–18 mm CPA (47). Tumor resec-tion was total in 93.4% (143 of 153) patients, near total in5.2% (8 of 153), and subtotal in 1.3% (2 of 153) (Table I).Near-total resection refers to leaving only a miniscule partof the tumor surface no more than 2 mm thick and 5 mmin diameter. Subtotal resection refers to any remnantlarger than this.
Auditory function was assigned classification (A, B,C, or D) through pure-tone average and speech discrimi-nation scores (SDS) according to the guidelines describedby the American Academy of Otolaryngology–Head andNeck Surgery (AAO–HNS).6 Pure-tone threshold average(PTA) was reported as an average of the air-conductionthresholds at 0.5, 1, 2, and 3 kHz (4 kHz when the thresh-old at 3 kHz was not determined). SDSs were obtained atpresentation levels of up to 40-dB sensation level. Mea-surable hearing preservation was described as a PTA �90dB hearing loss with any SDS. Rate of the functionalhearing preservation was described as the ratio of thepostoperative AAO–HNS class B and better results topreoperative class B and better hearing.
FN function was graded according to the House-Brackmann system as recommended by the AAO–HNSand reported as early (within 48 h) and late (1 y postop-eratively) outcome.7 The rate of good FN function wasexpressed as the percentage of grade II and better result.A secondary study population was created to serve as amatched comparison for the largest MF subset when as-sessing facial function. This consisted of a group of 40patients (tumor size 10–18 mm CPA) who had undergoneTL resection by the same skull base team over the sametime frame as the MF study population. The patients inthis control group were age- and tumor size-matched tothe MF study population by random selection (to minimizebias) from our acoustic neuroma database.
The surgical technique of MF craniotomy was modi-fied from that classically described by House.8 To enhanceexposure, the bone anterior and posterior to the IAC waswidely removed and a specialized MF retractor was used.9
In 2 cases, the superior petrosal sinus was occluded andtransected. Closure of the operative field in the IAC wasperformed with a locally harvested muscle graft for casesearlier than 1998 and an abdominal adipose graft there-after. Cranial nerve monitoring, including electromyogra-phy, evoked electromyography, and auditory brainstemresponse testing, was used in all operations.
Statistical analysis of the data was performed usingthe SPSS program for Windows (release 7.5, 1996; SPSS,Inc., Chicago, IL). Statistical significance was set at P�.05. In evaluation of the hearing preservation and FNoutcome following the MF approach, each tumor-size cat-egory was compared with each other in paired compari-sons using Pearson’s �2 test. FN outcome in 47 cases(tumor size 10–18 mm) that had undergone the MF ap-proach was compared with that of 40 cases (tumor size-matched) who had undergone the TL approach using thesame statistical test. Results of the 15- to 18-mm tumorsubset removed with the MF approach were reported sep-arately without statistical analysis resulting in a smallsample size. Patient ages and the length of the recoverytime for FN function achieved were compared among thetumor-size categories using a two-tailed independent-samples t test. The correlation of tumor size with hearingresult and FN outcome and the correlation of hearingoutcome with FN function were analyzed with Pearson’sbivariate correlation test.
RESULTS
Auditory FunctionAnatomic integrity of the cochlear nerve was pre-
served in 90.8% (139 of 153) of cases. The rate of cochlearnerve integrity preservation was slightly better for ICtumors (93.8%) than it was for 1- to 9-mm (90.5%) and 10-to 18-mm (87.2%) tumors. There was no significant differ-ence in preoperative PTA and SDS among the tumor-sizecategories (Table II). There was a strong correlation ob-served between tumor size and postoperative PTA (R �0.226, P �.01). SDS was also inversely correlated withtumor size (R � -0.197, P �.05).
The rate of postoperative functional hearing preser-vation (class A/B) was 53.3% overall (72 of 135 patients
TABLE I.Patient Age and Extent of Tumor Removal.
ApproachTumor Size
Categories (no.)Age mean � SD
(range)Tumor Size in CPA
(mean � SD)
CompleteResection(no., %)
Near TotalResection(no., %)
SubtotalResection(no., %)
Middle fossa approach Intracanalicular (64) 48.8 � 10.4 (16–69) — 61 (95.3%) 3 (4.7%) —
1–9 mm (42) 48.5 � 9.7 (15–72) 5 � 2.4 39 (92.9%) 3 (7.1%) —
10–18 mm (47) 50.5 � 10.7 (28–73) 12.2 � 2.5 43 (91.4%) 2 (4.3%) 2(4.3%)
Translabyrinthine approach 10–18 mm (40) 56 � 10.8 (29–77) 13.9 � 2.9 33 (82.5%) 7 (17.5%) —
SD � standard deviation; CPA � cerebellopontine angle.
Laryngoscope 112: August 2002 Satar et al.: Middle Fossa Approach for Acoustic Neuromas �10 mm
1501

with A or B preoperatively). The 10- to 18-mm CPA grouphad significantly poorer rates of hearing than the twosmall tumor size groups (Table II). No significant differ-ence in hearing outcome was observed between the IC andsmall CPA component (1–9 mm) groups. Pre- and postop-erative hearing levels are presented in greater detail,categorized according to tumor size and AAO–HNS hear-ing class, in Table III. A statistical analysis of these cat-egorical data also demonstrated poorer hearing in thelargest tumor size group (Table IV). Hearing improvementsufficient to alter AAO–HNS class (from B to A) wasobserved in only 2 patients (one each IC and 1–9 mm). Noears with either class C or D hearing preoperativelyachieved good hearing (A or B) postoperatively.
Because our primary interest is with tumors �10 mmin CPA diameter, special mention will be made of theresults in this group. Only 15 of 44 ears (34%) with pre-operative A or B hearing maintained this level followingtumor removal. This is only approximately one half of thesuccess rate achieved with the IC (62.2%) and 1- to 9-mm(63.1%) groups. To screen for size effect within the 10- to18-mm cohort, we separately considered the 11 patientswith tumor diameter of 15 to 18 mm in the CPA. Preop-erative hearing was class A7 and B4 of whom 36.4% (4 of11) retained good hearing (A or B) postoperatively. Thisresult is similar to that of the entire 10- to 18-mm group.
Facial Nerve FunctionIn the MF approach, the rate of anatomic FN preser-
vation was 96% (147 of 153) overall: IC � 96.9%, 1–9 mm� 97.6%, and 10–18 mm � 93.6%. With the TL approach(tumors 10–18 mm), the FN was preserved in all 40 cases(100%). The early and late FN outcome in all MF sizecategories as well as the comparison TL series appears inTable V. The most important measure of success is long-term functional outcome. Good FN function (grade I/II) at1 year postoperatively was achieved in 90.8% (139 of 153)of MF patients compared with 100% (40 of 40) of TL cases.A statistical analysis (�2) of comparisons between MF andTL results as well as among the various MF tumor sizegroups is presented in Table VI. In sized-matched cohorts(each 10–18 mm in CPA), the long-term MF FN outcomewas significantly worse than the TL. Among the three MFsize groups, FN outcome in the largest tumor size group
(10–18 mm) was significantly less favorable than the twosmall groups. The rate of good facial function for the 15- to18-mm tumor subset (11 patients) was 45.5% and 100%for early and late time frames, respectively. A Pearson’sbivariate correlation analysis of late FN function withtumor size in the 153 MF patients demonstrated a signif-icant (R � 0.182, P �.05) correlation.
Linkage Between Auditory Function and FacialNerve Outcome
A linkage was observed between late FN function andhearing outcome (Table VII). Patients with success athearing preservation were more likely to have a favorableFN outcome. This relationship was present for all threesize categories.
A Pearson’s bivariate correlation analysis of the 153MF patients showed a correlation between hearing andfacial outcome (R � 0.305, P �.01). The same correlationwas found for tumors �10 mm in the CPA (including ICtumors; R � 0.210, P �.05) and tumors 10 to 18 mm (R �0.306, P �.05).
DISCUSSIONWidespread use of magnetic resonance imaging has
resulted in an increased detection of small-sized AN andan increased number of interventions for hearing preser-vation. As major centers have accumulated considerableexperience in hearing conservation in recent years, suc-cess rates in preserving useful hearing have improvedsubstantially. A well-established trend has been the in-creased use of the MF approach and its application intumors with extracanalicular components in the CPA. Theliterature concerning outcomes for MF approaches in tu-mors larger than 10 mm in the CPA is limited. Manyteams have been hesitant to adopt this method for largertumors because of concerns regarding the unfavorableposition of the facial nerve, limited access to the inferioraspect of the CPA, and the need for lengthy and moreforceful retraction of the temporal lobe. Other teams, par-ticularly those who have had favorable experiences withsmaller tumors, have begun to explore using this methodin larger lesions. It is generally accepted that the uppersize limit for the MF approach is in the range of 16 to 20mm in CPA component. The reason that the upper limit is
TABLE II.Mean Pre- and Postoperative Pure-Tone Threshold Average (PTA) and Speech Discrimination Score (SDS) in Intracanalicular (IC) Tumors
and Those With a Component in Cerebellopontine Angle (CPA).
Tumor Size Categories (no.)
PTA (dB HL) � SD SDS (%) � SD
Preoperative Postoperative Preoperative Postoperative
IC (64) 34 � 17.6 58 � 35.3 81 � 23.4 55 � 42
1–9 mm in CPA (42) 33 � 16.8 54 � 34.4 89 � 13.1 62 � 38.2
10–18 mm in CPA (47) 32 � 15.7 79 � 34.2 86 � 18.2 33 � 40.8
Statistical Analysis
P (IC vs 1–9 mm) .928 .574 .065 .395
P (IC vs 10–18 mm) .689 .002 .303 .006
P (1–9 mm vs 10–18 mm) .776 .001 .357 .001
HL � hearing loss; SD � standard deviation.
Laryngoscope 112: August 2002 Satar et al.: Middle Fossa Approach for Acoustic Neuromas �10 mm
1502

not a fixed number is explained by the variable geometryof the CPA itself. As a general rule of thumb, we think itunwise to undertake MF approaches to AN when morethan minor brainstem contact has occurred.
In terms of osseous exposure, some authors haveargued that a family of MF approaches are used to addressAN with the “standard” approach for IC and an “enlarged”approach for tumors with a significant CPA compo-nent.1,10 As we have done more MF cases, we have foundthat it is beneficial to make a fairly wide exposure of theIAC and adjacent posterior fossa dura regardless of thetumor size. In the TL approach, it is generally acknowl-edged that there is but one fundamental technique usedfor AN of all sizes. Admittedly, the opening is made some-what wider for larger tumors, but this is a variation on thesame theme. We think the same principle applies to theMF approach.
In the present study, the maximum diameter of thetumor resected using the MF approach was 18 mm. Therewere 11 cases with a tumor in the 15- to 18-mm range and47 larger than 10 mm in the CPA. Our primary reason for
undertaking this study was to determine the degree ofsuccess in hearing preservation for these larger tumorsand to ascertain whether undertaking this effort carries acost in terms of long-term FN outcome. There are threemeans of measuring “success” in hearing conservationsurgery: integrity of the cochlear nerve, presence of anydegree of measurable hearing, and maintenance of usefullevels of hearing. Because we think the latter measure isby far the most valid indicator of success, our analysis willemphasize this measure. In the present study, of 135 MFpatients with good preoperative hearing (class A/B) (in-cludes tumors of all sizes), 53.3% maintained good hearingafter tumor resection. When examined according to tumorsize, larger tumors (10–18-mm CPA) retained good hear-ing (A or B) approximately half as often (34%) as the IC(62.2%) and �9-mm CPA (63.1%). There is a paucity ofdata on hearing outcomes in the MF approach to tumorswith substantial extracanalicular components. The earlierliterature includes 156 patients (239 patients for evalua-tion of FN function) with a 10- to 20-mm CPA componentfrom four studies.4,10–12 In these, the rate of good hearing(A or B) preservation was 33.3% (Table VIII). These dataare similar to our own. Only studies with sufficient detailcould be tabulated in this manner. Much of the literaturewas not suitable for comparison as a result of inconsistentmethods of reporting tumor size and hearing outcome. Anumber of studies reported overall tumor size, includingthe IAC component. This tends to overestimate the size ofthe tumor by as much as 10 mm, a huge factor whenevaluating small tumor components within the CPA. Inthe future, we are hopeful that every study will includedata in a standardized format, such as that recommendedby the AAO–HNS, to facilitate meta-analyses.6
It seems worthwhile to make mention of the points inoperative technique which enhance the possibility of hear-
TABLE III.Cross-referencing Data of Pre- and Postoperative Hearing Levels (AAO-HNS classification).
Tumor SizeCategories Preoperative Class (no.)
Postoperative Class (no., %)
A B C D
Intracanalicular A (26) 13 (50%) 5 (19.2%) 1 (3.9%) 7 (26.9%)
B (27) 1 (3.7%) 14 (51.9%) 5 (18.5%) 7 (25.9%)
C (4) — — 1 (25%) 3 (75%)
D (7) — — — 7 (100%)
Total (64) 14 (21%) 19 (29%) 7 (11%) 25 (39%)
1–9 mm in CPA A (17) 9 (52.9%) 3 (17.6%) 2 (11.8%) 3 (17.6%)
B (21) 1 (4.8%) 11 (52.4%) 4 (19%) 5 (23.8%)
C (3) — — 2 (66.7%) 1 (33.3%)
D (1) — — — 1 (100%)
Total (42) 10 (23.8%) 14 (33.4%) 8 (19.1%) 10 (23.8%)
10–18 mm in CPA A (21) 6 (28.6%) 2 (9.5%) — 13 (61.9%)
B (23) — 7 (30.4%) 3 (13%) 13 (56.5%)
C (1) — — — 1 (100%)
D (2) — — — 2 (100%)
Total (47) 6 (12.7%) 9 (19.2%) 3 (6.3%) 29 (61.8%)
CPA � cerebellopontine angle.
TABLE IV.Chi-square (P values given) of the Data in Table III.*
Preoperative Postoperative
1–9 mmin CPA
10–18 mmin CPA
1–9 mmin CPA
10–18 mmin CPA
Intracanalicular .268 .090 .931 .006
10–18 mmin CPA
.583 .009
* Tumor size categories are compared with reference to the rate offunctional hearing preservation (postoperative class A and B/preoperativeclass A and B).
CPA � cerebellopontine angle.
Laryngoscope 112: August 2002 Satar et al.: Middle Fossa Approach for Acoustic Neuromas �10 mm
1503

ing conservation. Several points are often mentioned bysurgeons in the field with sufficient regularity to consti-tute conventional wisdom: work only medial to lateral toavoid traction of the fragile eighth nerve entering themodiolus, cut the vestibular nerves early, avoid usingbipolar cautery, and work “underwater” using copious ir-rigation.10,13,14 Even though our hearing results are atleast comparable to the best reported in the literature, ourpractice is often at variance to these pearls of conventionalwisdom. First of all, with the viewpoint provided by theMF approach, it is difficult to dissect medial to lateralduring the entire tumor dissection. The key point is thattraction on the cochlear fibers must be avoided to thegreatest extent possible. This may require sharp dissec-tion of the tumor–nerve interface. For the second point, wethink hearing preservation is enhanced when every eighthnerve fiber not infiltrated by tumor is preserved. Leavingsome vestibular fibers lends mechanical support to thecochlear nerve and helps to avoid injury to the tributariesof the internal auditory artery. A possible trade-off on thistechnique is a higher possibility of postoperative vestibu-lar symptoms. Concerning potential deleterious effects ofcautery, we regularly use the irrigating microbipolar atlow power settings. This should be done judiciously, aimedprecisely at the offending vessel, and not in the immediatevicinity of facial or auditory nerves. Meticulous hemosta-sis facilitates orderly microdissection. A final technicalpoint is that hearing is often lost during dissection oftumor from the fundus of the IAC. Because of overhang ofthe transverse crest and FN, dissection of its deepest
recesses must often be done blindly.15,16 Use of long an-gled instruments (e.g., curettes, hooks, and ball-hooks) ishelpful.
For any size of AN, preservation of the FN is techni-cally more challenging using the MF approach. Often thenerve is located on the superior surface of the tumorinterposed between the tumor and the surgeon’s point ofview. Thus, the surgeon must work past the nerve, and itmust be manipulated from side to side during tumor dis-section. By contrast, in the RS and TL approaches, the FNcan remain undisturbed in its deflected course and thussustains a lesser degree of trauma. In an earlier study, wefound that although transient FN dysfunction was sub-stantially higher in small tumors (�10 mm CPA), long-term outcome was the same as with other approaches.17 Inthe present study, it has become clear that with largertumors (10–18-mm CPA) the MF approach carries a sig-nificantly higher risk of long-term residual FN dysfunc-tion, the most informative comparison in the 10- to 18-mmCPA size group between the MF and TL approaches. Withthe MF, good long-term FN function (grade I/II) wasachieved in only 80.9% (38 of 47) of cases, whereas in TL100% (40 of 40) achieved this result. This difference wasstatistically significant (P � .003). A potential source ofbias should be noted in these data. Less-than-completetumor resection was performed in 8.6% of MF cases and17.5% of TL. This more conservative resection could haveboosted the FN outcome in the TL group. Two earlierstudies on the MF approach contain long-term FN out-come data in the size range of interest. In these, good FNfunction (1 or 2) was achieved in 85.2% (167 of 196).4,10 Itis interesting that a concurrence was found between goodFN function and functional hearing outcome (Table VII).The linkage between either good or bad outcome for bothfunctions probably relates to the biologic properties of thetumor such as the tendency to have an adhesive tumor–nerve interface.
The results of this risk–benefit analysis are useful inadvising AN patients with good hearing and a sizable CPAcomponent. For patients with tumors �10 mm in diame-ter, the MF approach is clearly superior because it has anequivalent long-term FN result (compared with RS andTL approaches) and allows for a �60% retention of goodhearing. For patients with good hearing and a tumor inthe 10- to 18-mm CPA range, the deliberation is more
TABLE V.Early (within first 2 days) and Late (1 year) Facial Nerve Outcome.
Approach Tumor-Size (no.) I II III IV V VI
MF approach Intracanalicular (64) 21 (32.8%) 12 (18.8%) 6 (9.4%) 4 (6.3%) 4 (6.3%) 17 (26.6%)
Early 1–9 mm in CPA (42) 18 (42.9%) 8 (19%) 4 (9.5%) 4 (9.5%) 1 (2.4%) 7 (16.7%)
10–18 mm in CPA (47) 9 (19.1%) 5 (10.6%) 6 (12.8%) 2 (4.3%) 2 (4.3%) 23 (48.9%)
TL approach 10–18 mm in CPA (40) 16 (40%) 7 (17.5%) 1 (2.5%) 5 (12.5%) 2 (5%) 9 (22.5%)
MF approach Intracanalicular (64) 55 (85.9%) 5 (7.8%) 4 (6.3%) — — —
Late 1–9 mm in CPA (42) 40 (95.2%) 1 (2.4%) 1 (2.4%) — — —
10–18 mm in CPA (47) 30 (63.8%) 8 (17%) 7 (14.9%) 1 (2.1%) — 1 (2.1%)
TL approach 10–18 mm in CPA (40) 35 (87.5%) 5 (12.5%) — — — —
MF � middle fossa; TL � translabyrinthine; CPA � cerebellopontine angle.
TABLE VI.Chi-square (P values given) of the Data in Table V.*
Approach Tumor Size
FacialFunction
Early Late
Among the MF Categories IC vs 1–9 mm .294 .358
IC vs 10–18 mm .022 .037
1–9 mm vs 10–18 mm .002 .012
MF vs TL 10–18 mm vs 10–18 mm .009 .003
* Tumor size categories are compared with reference to the rate ofgood facial nerve function (grade I/II) at early and late time frames.
MF � middle fossa; TL � translabyrinthine.
Laryngoscope 112: August 2002 Satar et al.: Middle Fossa Approach for Acoustic Neuromas �10 mm
1504

complicated. Although good hearing can be preserved inover one third of patients, cosmetically significant long-term FN dysfunction (grade III, 15%; IV, 2%; VI, 2%) ishigher than with the TL or RS methods. Earlier, we haveshown that long-term FN results are equivalent betweenthe RS and TL techniques.17 Recently, we have observedthat the RS approach is only approximately half as suc-cessful in preserving hearing for tumors in this sizerange.18 With its superior FN results compared with theMF approach, this may seem a reasonable alternative.However, the RS approach does not permit adequate ac-cess of the fundus of the IAC without removing a portionof the vestibule and common crus, a maneuver incompat-ible with hearing preservation.19 The RS approach is alsoassociated with a significantly higher incidence of persis-tent postoperative headache.20 For these reasons, whentumor extends deep into the fundus of the IAC, we tend toavoid the RS approach.
The results of this study have altered our recommen-dations to patients. Formerly, we recommended the MFapproach for all tumors with good hearing up to 18 mmdiameter in the CPA. Our current practice is to informpatients with 10- to 18-mm CPA components that whilethe MF approach is clearly superior for hearing, it carrieswith it a somewhat higher incidence of persistent facialparesis and synkinesis. We explain the probabilities in-volved and allow the patient to judge the relative impor-tance of hearing and facial function. The surgeon shouldnot assume that patients would automatically choose alowered risk of facial neuropathy over a possibility ofsaving hearing. In an earlier study of patient-perceivedoutcomes following AN surgery, we were surprised to note
that many patients with both facial dysfunction and uni-lateral deafness actually rated the auditory deficit as morelife disturbing.21
It should be noted that certain other factors (notquantified in the present study as a result of incomplete-ness of the available data) are also considered in riskstratification. For example, we suspect that extensive os-seous erosion of the porus acusticus and deep penetrationof the fundus are adverse predictors of success in hearingpreservation. The limited hard data available and com-plexity of the variables involved makes it difficult to codifysuch factors into an explicit set of rules. To illustrate howthese factors come into play in our advice to patients, wewould be more enthusiastic in our recommendation for ahearing conservation approach in a 12-mm CPA tumorwith normal hearing, an empty fundus, and a narrowporus than we would be in an 18-mm CPA tumor withmarginal class B hearing, deep fundus involvement, and awidely eroded porus acousticus.
Because of the technical challenges faced in obtainingadequate exposure and conducting an effective dissection,we recommend that microsurgical teams not undertakethe MF approach to tumors with sizable CPA componentsuntil they have become facile with smaller lesions.
CONCLUSIONWhen considering surgical options, patients with
�10-mm tumors should be advised that choosing the MFapproach for hearing preservation carries a somewhathigher risk of persistent FN dysfunction than the TLapproach.
TABLE VII.Concurrence of Good Facial Function and Functional Hearing Preservation.
Facial Nerve Function (�1 y)
Hearing Results
Intracanalicular 1–9 mm in CPA 10–18 mm in CPA
Class A/B Class C/D Class A/B Class C/D Class A/B Class C/D
Grade I–II 33 (100%) 27 (87.1%) 24 (100%) 17 (94.4%) 14 (93.3%) 24 (75%)
Grade III–VI (0%) 4 (12.9%) (0%) 1 (5.6%) 1 (6.7%) 8 (25%)
CPA � cerebellopontine angle.
TABLE VIII.Rates of Functional Hearing Preservation (class A/B) and Good Long-term Facial Function (grade I/II) in Selected Series of the Middle
Fossa Approach for Tumors Larger Than 10 mm.
Study Institution YearCPA
Component Patients Good Hearing Good Facial Function
Dornhoffer et al.11 Wuerzburg 1995 10–15 mm 17 47% NA
Staecker et al.4 Harvard 2000 10–15 mm 4 75% 75%*
Gjuric et al.10 Erlangen 2001 10–19 mm 109 28.4% 85% in 192 patients†
Kanzaki et al.12 Keio 2001 11–20 mm 26 30.7% NA
Satar et al. UCSF 2002 10–18 mm 44 34% 80.8% in 47 patients†
* 3 months postoperatively.† 1 year postoperatively and includes also preoperative class C/D patients.CPA � cerebellopontine angle; NA � data not available.
Laryngoscope 112: August 2002 Satar et al.: Middle Fossa Approach for Acoustic Neuromas �10 mm
1505

AcknowledgmentsThe TWJ Foundation funded Philip Yates’ fellowship
at the Department of Otolaryngology–Head and Neck Sur-gery University of California, San Francisco.
BIBLIOGRAPHY1. Haid CT, Wigand ME. Advantages of the enlarged middle
cranial fossa approach in acoustic neurinoma surgery. ActaOtolaryngol (Stockh) 1992;112:387–407.
2. Kanzaki J, Shiobara R, Toya S. Classification of the extendedmiddle cranial fossa approach. Acta Otolaryngol (Stockh)1991;Suppl 487:6–16.
3. Irving RM, Jackler RK, Pitts LH. Hearing preservation inpatients undergoing vestibular schwannoma surgery: com-parison of middle fossa and retrosigmoid approaches.J Neurosurg 1998;88:840–845.
4. Staecker H, Nadol JB Jr, Ojeman R, Ronner S, McKennaMJ. Hearing preservation in acoustic neuroma surgery:middle fossa versus retrosigmoid approach. Am J Otolar-yngol 2000;21:399–404.
5. Jackler RK. Editorial comment. Otol Neurotol 2001;22:230–231.
6. Committee on Hearing and Equilibrium. Committee on Hear-ing and Equilibrium guidelines for the evaluation of hear-ing in acoustic neuroma (vestibular schwannoma). Otolar-yngol Head Neck Surg 1995;115:179–180.
7. House JW, Brackmann DE. Facial nerve grading system.Otolaryngol Head Neck Surg 1985;93:146–150.
8. Jackler RK, Gladstone HB. Locating the internal auditorycanal during the middle fossa approach: an alternativetechnique. Skull Base Surgery 1995;5:63–67.
9. Driscoll CLW, Jackler RK, Pitts LP, Banthia V. Extraduraltemporal lobe retraction in the middle fossa approach tothe internal auditory canal: a biomechanical analysis.Am J Otolaryngol 1999;20:373–380.
10. Gjuric M, Wigand ME, Wolf SR. Enlarged middle fossa ves-tibular schwannoma surgery: experience with 735 cases.Otol Neurotol 2001;22:223–231.
11. Dornhoffer JL, Helms J, Hoehmann DH. Hearing preserva-tion in acoustic tumor surgery: results and prognostic fac-tors. Laryngoscope 1995;105:184–187.
12. Kanzaki J, Inoue Y, Ogawa K. The learning curve in post-operative hearing results in vestibular schwannoma sur-gery. Auris Nasus Larynx 2001;28:209–221.
13. Brackmann DE, House JR III, Hitselberger WE. Technicalmodifications to the middle fossa craniotomy approach inremoval of acoustic neuromas. Am J Otolaryngol 1994;15:614–619.
14. Slattery WH III, Brackmann DE, Hitselberger W. Middlefossa approach for hearing preservation with acoustic neu-romas. Am J Otolaryngol 1997;18:596–601.
15. Driscoll CL, Jackler RK, Pitts LH, Banthia V. Is the entirefundus of the internal auditory canal visible during middlefossa approach for acoustic neuroma? Am J Otolaryngol2000;21:382–388.
16. Haberkamp TJ, Meyer GA, Fox M. Surgical exposure of thefundus of the internal auditory canal: anatomic limits ofthe middle fossa versus the retrosigmoid transcanal ap-proach. Laryngoscope 1998;108:1190–1194.
17. Lalwani AK, Butt FYS, Jackler RK, Pitts LH. Facial nerveoutcome after acoustic neuroma surgery: a study from theera of cranial nerve monitoring. Otolaryngol Head NeckSurg 1994;111:561–570.
18. Yates PD, Jackler RK, Satar B, Pitts LH, Oghalai J. Is itworthwhile to attempt hearing preservation in largeracoustic neuromas. Otol Neurotol 2002 (in press).
19. Blevins NH, Jackler RK. Exposure of the lateral extremity ofthe internal auditory canal through the retrosigmoid ap-proach: a radioanatomic study. Otolaryngol Head NeckSurg 1994;111:81–90.
20. Levo H, Blomstedt G, Pyykko I. Is hearing preservationworthwhile in vestibular schwannoma surgery? Acta Oto-laryngol Suppl 2000;543:26–27.
21. Rigby PL, Shah SB, Jackler RK, Chung JH, Cooke DD.Acoustic neuroma surgery: outcome analysis of patient-perceived disability. Am J Otolaryngol 1997;18:427–435.
Laryngoscope 112: August 2002 Satar et al.: Middle Fossa Approach for Acoustic Neuromas �10 mm
1506