Embed Size (px)
Citation preview

2823
REVIEW DOI: 10.5504/bbEq.2011.0147 Mb
MEDICAL bIOTECHNOLOGY
Biotechnol. & Biotechnol. eq. 26/2012/2
Biotechnol. & Biotechnol. eq. 2012, 26(2), 2823-2825Keywords: gastroesophageal reflux disease, oral cavity signs, dental recommendations
Oral Manifestations of Gastroesophageal Reflux Disease (GERD)Several gastrointestinal disorders affect the oral cavity, within tissues in or around the mouth (12, 13). Gastroesophageal reflux disease, or GERD, is a relatively common pathology. The gastric acid juice refluxes usually through the lower esophageal sphincter in the lower part of the esophagus or up to the oral cavity. It may cause different oral symptoms and signs.
The common symptoms of GERD are belching, heartburn, acid regurgitation, difficulty swallowing (dysphagia) and unexplained sour taste (1, 24). Other gastric atypical symptoms include posterior laryngitis, respiratory symptoms, noncardiac chest pain (24).
In silent GERD, however, the usual characteristic symptoms do not occur, and oral signs and symtoms may be the first clinical manifestation of GERD. So it is important that dental professionals can identify such patients and recommend appropriate measures to protect the long-term health of the dentition. Furthermore, dental professionals have the opportunity to recognize these pathologies (12, 13, 24).
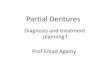
The oral manifestations of GERD are:Tooth erosionThe most frequent oral manifestation of GERD is erosion of tooth enamel (2, 3, 19, 23). The pH of the gastric acid is much lower than the critical pH of enamel dissolution, therefore, reflux of stomach contents into the oral cavity over an extended period of time can cause severe loss of tooth structure (15, 16). Enamel erosion (Fig. 1 and Fig. 2) by gastric acids also occurs in other reflux abnormalities: patients with hiatal hernia, wine drinking, chronic alcoholism and bulimia (5, 12, 13, 15, 16, 17).
Fig. 1. Enamel erosion in patients with GERD.
Fig. 2. Enamel erosion in patients with GERD.
The typical localisation of enamel erosion distinguishes the chemical erosions and erosions by reflux disease. The typical chemical erosion is observed usually on the vestibular tooth surfaces contrary to the erosions due to the gastric acid, witch are localized often on the palatinal surfaces of the maxillary dentition (12, 13). It is postulated that the dental expertise may be essential in distinguishing between differential diagnoses such as bulimia, attrition and abrasion (1, 15, 16).
Enamel erosions result in exposure of the underlying dentin, which is a softer, more yellow, material. The extent of erosion depends on the frequency and the quantity of асid exposure along with the duration of disease (24).
ORAL CAVITY AND SYSTEMIC DISEASES – GASTROESOPHAGEAL REFLUX DISEASE
Assya Krasteva1, Vladimir Panov2, Angelina Kisselova1, Zahary Krastev 3 1Medical University – Sofia, Faculty of Dental Medicine, Sofia, Bulgaria 2Medical University “Prof. Dr. P. Stoyanov”, Faculty of Dental Medicine, Varna, Bulgaria 3Medical University Sofia, Clinic of Gastroenterology “St. Ivan Rilski”, Sofia, BulgariaCorrespondence to: Assya KrastevaE-mail: [email protected]
ABSTRACTSeveral gastrointestinal disorders affect the oral cavity, and also the tissues around the mouth in the maxillo-facial region. In some cases, oral signs may be present in the absence of obvious gastrointestinal complaints or signs and also may suggest the disease. In this review we summarize some oral abnormalities in patients affected by the gastro-oesophageal reflux disease.

2824 Biotechnol. & Biotechnol. eq. 26/2012/2
Low pH in the oral cavityRegurgitation of gastric contents (pH 1-2) reduces the pH of the oral cavity below 5.5. Oral pH has been noted to be significantly lower in patients with GERD (22).
Low salivary buffer capacityGudmundsson et al. (11) found that the patients with GERD had low salivary buffer capacity.
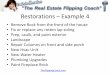
Oral mucosa lesionsIn patients with GERD oral erythema on the soft and hard palate mucosa has been found (9) (Fig. 3 and Fig. 4). this erythema and mucosal atrophy may be present as a result of chronic exposure of tissues to acid (5).
Fig. 3. Oral erythema in patients with GERD.
Oral complaints GERD patients often mention other oral complaints such as sensitation of burning or heat in the mouth, halitosis, xerostomia, dysgeusia – foul taste, and dental sensitivity related to hot or cold drinks or foods due to the erosions (5, 9, 18, 20).
Temporomandibular disordersIncreased temporomandibular disorders have been found in patients with GERD by Gharaibeh et al. (10). Other study mentions that patients with masticatory dysfunction have a higher incidence of gastrointestinal disorders including gastroesophageal reflux disease (21).
Fig. 4. Oral erythema in patients with GERD.
Dental Recommendations Tooth erosion, oral pH and salivary buffer capacity – practical dental recommendations
AnalysisThe first step is to recognise eventual medical circumstances that increase the risks of tooth wear. These include diseases that
affect the salivary glands or some medications that decrease the salivary function.
Remineralization procedureRemineralization therapy can be administered professionally and recommended as a part of a patient’s self-care routine. Not only will these treatments help patients with erosion due to acid reflux, but they will also help to control damage to the enamel from other demineralization factors, such as excessive ingestion of acidic foods and beverages (e.g., soda pop, sports drinks, tomato based products and citrus foods and drinks) (24).
The dentisrt can apply/recommend topical fluoride through varnish, rinses, and one-minute topical gel/foam for use in a disposable tray after completion of the prophylaxis (24).
Restorative procedure (4, 6, 7, 24) • Restorative options of the enamel erosion will depend
on the degree of tooth surface loss. • In early erosion, restorative options include use of
dentin bonding agents to protect exposed dentin, resin restorations retained with adhesive agents in surfaces not susceptible to heavy loads, and veneer restorations.
• In advanced erosion, which involves a large amount of dentin exposure and loss of vertical dimension, orthodontic extrusion and full coverage restorations may be necessary.
Other recommendations (8, 24)• Using toothpaste, preferably a low-abrasive formula;• Use of a protective occlusal guard if attrition due to
bruxism is present; • Use of a neutralizing agent such as sugar-free antacids
held in the mouth after acid exposure;• Oral health education and drink and food guidance
should be strengthened. The amount and frequency of intake of acidic food and drink should be reduced to promote oral health.
Oral complaints – practical dental recommendationsHalitosis, dysgeusia (5, 6, 12, 13).
• Wash your teeth twice a day – at least three minutes;• Use teeth floss;• Clean your tongue – thus reducing the number of
dead cells and bacteria;• Use a mouthwash;• Take probiotics – oral and systemic;• Chew gum, mint, cloves or fennel;• Mild baking soda mouthrinses are recommended to
minimize dysgeusia caused by acid reflux.
Xerostomia (14)• At least 2 liters of liquids intake a day (patient can
hold ice chips in his or her mouth to provide moisture

2825Biotechnol. & Biotechnol. eq. 26/2012/2
and possibly alleviate symptoms);• Products promoting salivary gland secretions –
cholinergic drugs such as pilocarpin, lemon juice, chewing gum;
• When conventional medical interventions do not provide satisfactory relief, it is recommended saliva substitutes and oral lubricants to be administered. The volume of stimulated and unstimulated saliva could also be measured.
ConclusionsOne way that dental professionals can be proactive in preserving and protecting the dental health of their patients is to be aware of any factors that may affect the dentition. Recognized oral manifestations (oral signs and symptoms) of gastrointestinal disease may be useful to the gastroenterologist in the diagnostic process for patients with gastrointestinal complaints. Good dental care, early recognition and patient education is the most effective behavior with these patients.
REFERENCES1. Ali D,. Brown R., Luciano O., et al. (2002) J. Am. Dent.
Assoc., 133, 734-737. 2. Barron P., Carmichael P., Marcon A., et al. (2003) J.
Can. Dent. Assoc., 69, 84-89. 3. Bassiouny M.A. (2010) Gen. Dent., 58, 244-255. 4. Bornstein M., Stocker L., Seemann R., et al. (2009) J.
Periodontol., 80, 24-31. 5. Bricker S., Langlais R., Miller C. (1994) Oral Diagnosis,
Oral Medicine and Treatment Planning, BC Decker Inc, Hamilton, Canada, 346-349.
6. Broliato A., Volcato B., Reston G., et al. (2008) Quintessence Int., 39, 131-137.
7. Corega C., Baciut M., Vaida L., et al. (2009) J. Gastrointestin. Liver Dis., 18, 497-499.
8. Chen G., Li X., Hu Y., et al. (2009) Hua Xi Kou Qiang Yi Xue Za Zhi., 27, 565-567.
9. Di Fede O., Di Liberto C., Occhipinti G., et al. (2008) J. Oral Pathol. Med., 37, 336-340.
10. Gharaibeh M., Jadallah K., Jadayel A. (2010) J. oral Maxillofac. Surg., 68, 1560-1564.
11. Gudmundsson K, Kristleifsson G., Theodors A., et al. (1995) Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod., 79, 185-189.
12. Krastev Z., Kisselova A. (2009) In: Oral Medicine, I. Sapunjiev EOOD, Sofia, 334- 345 (in Bulgarian).
13. Krasteva A., Kisselova A., Panov Vl., et al. (2011) oral Lesions, I. Sapunjiev EOOD, Sofia (in Bulgarian).
14. Krasteva A., Panov Vl., Krasteva A., Kisselova A. (2011) Biotechnol. Biotech. eq., 25, 2305-2309.
15. Lazarchik A., Frazier B. (2009) Gen Dent., 57, 151-158.16. Lazarchik A., Filler S. (1997) Am. J. Med., 103,
107S-113S.17. Little W. (2002) Oral Surg. Oral Med. Oral Pathol. Oral
Radiol. Endod., 93 138-143.18. Madani A., Wong E., Sowerby L., et al. (2010) J. Fam.
Pract., 59, 102-107. 19. Moazzez R., Bartlett D., Anggiansah A. (2004) J. Dent.,
32, 489-494.20. Moshkowitz M., Horowitz N., Leshno M., et al. (2007)
Oral Dis., 13, 581-585.21. Togawa R., Ohmure H., Sakaguchi K., et al. (2009) Am.
J. Orthod. Dentofacial Orthop., 136, 10-11. 22. Van der Waal R.I., Buter J., van der Waal I. (2003) Br. J.
Oral Maxillofac. Surg., 41, 3-6.23. Vigner S., Russo L., Fedele S., et al. (2008) J. Oral Pathol.
Med., 3, 336-340.24. Yang V., Wehbi M. (2005) PennWell Continuing Education
Courses, www.ineedce.com/PDF%20files/ACID%20REFLUX.pdf