Embed Size (px)
Citation preview
Systematic Review and Meta-Analysis of Treatment of Latent TB Infection to
Reduce Progression to Multidrug-Resistant Tuberculosis
Suzanne M. Marks, Sundari R. Mase, Sapna Bamrah Morris
Brown Bag Presentation to CDC/DTBE,
August 20, 2015
Background• Current guidance is based on expert opinion
• Evidence-based recommendations are lacking because published data consist of small observational studies
• TB incidence in contacts treated for presumed MDR LTBI is unknown
• Treatment discontinuation due to adverse effects has not been systematically documented
Current Guidance• CDC. Management of Persons Exposed to Multidrug-resistant Tuberculosis. MMWR. 1992;41(RR-
11):59-71. – “no clinical data exist on the risks and benefits of regimens that do not include INH or RIF”– Persons at high-risk of progressing to TB (HIV+, immunosuppressed)
• treatment with ≥ 2 drugs since “efficacy of preventive monotherapy with alternative drugs has not been demonstrated”
– Persons who are not at high risk of progression, 2 options:• No preventive therapy and provide clinical follow up for signs and symptoms• Treatment with ≥ 2 drugs other than INH or RIF.
– If the source case strain is < 100% INH resistant, INH should be used– If the source case strain is < 100% RIF resistant, RIF should be used– Potential alternative regimens: 6-12 months (12 months for HIV+, immunosuppressed) of
treatment with ≥ 2 drugs to which the isolate of the presumed source case is susceptible• PZA/EMB (EMB to be used with caution in children) • PZA/FQ • FQ should only be used in children or pregnant females if potential benefits justify the
potential side effects• PAS, ETH, CYC are not recommended “because of their high frequency of side effects and
relatively low efficacy”
• CDC. Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection. MMWR. 2000;49(RR-6):36-37.– PZA/EMB or PZA/FQ for 6-12 months if the isolate is susceptible to these drugs– ≥ 2 drugs to which the isolate of the presumed source case is susceptible
Current Guidance• Curry National Tuberculosis Center. Drug-Resistant Tuberculosis: A Survival Guide for
Clinicians– LEV or MOX and a 2nd susceptible drug; LEV or MOX alone– “Young children with presumed MDR-LTBI should be treated with a 2 to 3 drug
regimen for 12 months, including a FQ if appropriate” (monitor for joint pain, swelling, or decreased range of motion)
• ECDC Guidance: Management of Contacts of MDR TB and XDR TB Patients– Cites 3 studies: Attamna, Kritski, and Schaaf– “it is not possible with the available evidence to support or reject preventive therapy”
• Bob Horsburgh: ATS/CDC/IDSA LTBI group– “Current recommendations for treatment of contacts of patients with MDR-TB are
based on expert opinion and do not meet GRADE criteria.[15,16] Therefore, we recommend neither for or against such treatment.”
• WHO Guidelines on the management of LTBI– “serious limitations of the quality of evidence prevent drawing any recommendations
on MDR-TB preventive therapy as a public health measure. Strict clinical observation and close monitoring for the development of active TB disease for at least two years is preferred over the provision of preventive treatment for contacts with MDR-TB cases.”
Study Objectives
• To assess, using systematic review and meta-analysis, whether MDR-LTBI treatment is significantly associated with lower TB incidence among persons having contact with infectious MDR-TB patients and evidence of or presumed LTBI, compared with no medical treatment
• To examine treatment completion and adverse effects (AE)
Study Methods (1)
• Conducted a systematic review in Dec. 2014 of published studies in English or Spanish of patients having contact with infectious MDR-TB cases, who had documented or presumed (for children <5 years of age or living with HIV) LTBI, treated or untreated MDR-TB LTBI
• Considered patients effectively treated if they were on ≥ one medication to which their MDR-TB strain was likely to be susceptible
Study Methods (2)• Abstracted TB incidence data from studies presenting data both on
patients treated and untreated, only on patients treated, and only on untreated patients. TB incidence was calculated as a proportion of persons treated versus untreated, and not by time, because only a few studies reported incidence by person-time.
• Selected studies that compared treatment versus non-treatment outcomes. We performed meta-analysis on data from studies reporting any TB incidence to estimate the pooled random effects relative risk (RR) of TB incidence and its 95% confidence using EpiSheet.
• Abstracted data on treatment completion, when available
• Abstracted data on adverse effects, and aggregated individual level adverse effect data by regimen, when available
Search Methods
• Searched publications through December 2014 in Pubmed, Embase, Cochrane Library, Google Scholar, Google
• Manually searched references of review articles
• Reviewed titles and abstracts, followed by reviewing full-texts of selected articles
Search Fields
("tuberculosis, multidrug-resistant"[MeSH Terms] OR ("tuberculosis"[All Fields] AND
"multidrug-resistant"[All Fields]) OR "multidrug-resistant tuberculosis"[All Fields] OR ("multidrug"[All Fields] AND "resistant"[All Fields] AND "tuberculosis"[All Fields]) OR "multidrug resistant tuberculosis"[All Fields]) AND contacts[All Fields] AND ("therapy"[Subheading] OR "therapy"[All Fields] OR "treatment"[All Fields] OR "therapeutics"[MeSH Terms] OR "therapeutics"[All Fields])
Systematic Literature ReviewInclusion Criteria
• Published journal articles that presented data on:
– contacts to patients with infectious MDR TB who have documented or assumed LTBI
– treatment of MDR TB LTBI
Exclusion Criteria
• Case reports with N < 10
• Studies only reporting on diagnosis or treatment of MDR TB disease
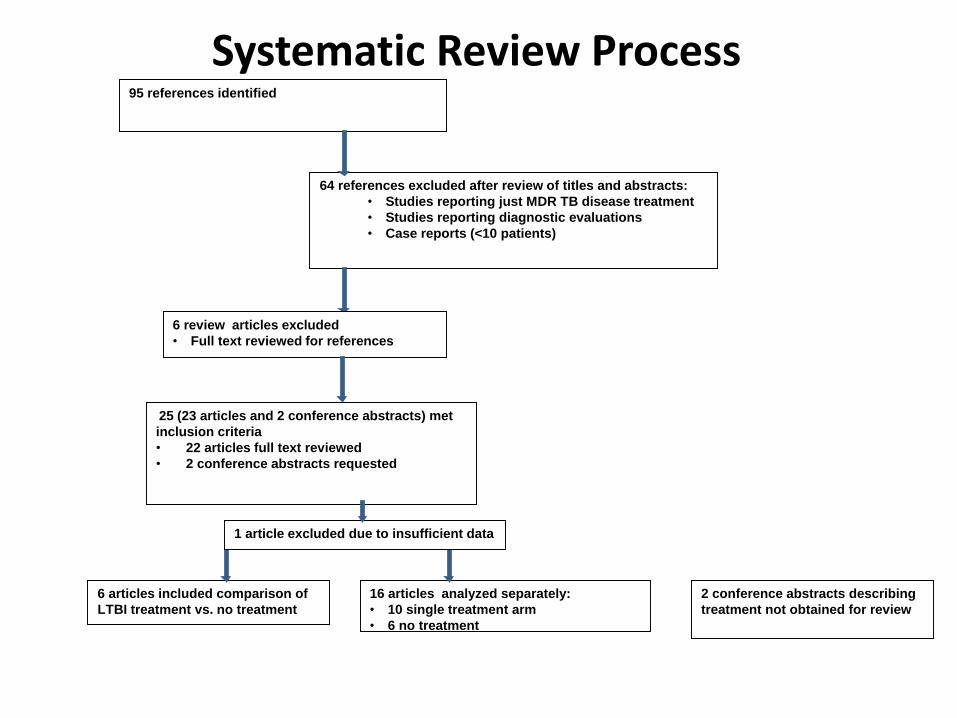
95 references identified
64 references excluded after review of titles and abstracts:
• Studies reporting just MDR TB disease treatment
• Studies reporting diagnostic evaluations
• Case reports (<10 patients)
25 (23 articles and 2 conference abstracts) met
inclusion criteria
• 22 articles full text reviewed
• 2 conference abstracts requested
6 articles included comparison of
LTBI treatment vs. no treatment
16 articles analyzed separately:
• 10 single treatment arm
• 6 no treatment
6 review articles excluded
• Full text reviewed for references
Systematic Review Process
2 conference abstracts describing
treatment not obtained for review
1 article excluded due to insufficient data
6 Excluded Review Articles:References Manually Search for Inclusion
1. CDC. Management of persons exposed to multidrug-resistant tuberculosis. MMWR Recomm Rep. 1992 Jun 19;41(RR-11):61-71.
2. European Centre for Disease Prevention and Control. Management of contacts of MDR TB and XDR TB patients. Stockholm: ECDC; 2012.
3. Fraser A, Paul M, Attamna A, et al. Drugs for preventing tuberculosis in people at risk of multiple-drug-resistant pulmonary tuberculosis. Cochrane Database Syst Rev 2006; CD005435.
6 Excluded Review Articles:References Manually Search for Inclusion
4. Fraser A, Paul M, Attamna A, Leibovici L. Treatment of latent tuberculosis in persons at risk for multidrug-resistant tuberculosis: systematic review. IJTLD 2006; 10:19–23.
5. Langendam MW(1), Tiemersma EW, van der Werf MJ, Sandgren A. Adverse events in healthy individuals and MDR-TB contacts treated with anti-tuberculosis drugs potentially effective for preventing development of MDR-TB: a systematic review. PLoS One. 2013:8(1): e53599. doi:10.1371/journal.pone.0053599.
6. Van der Werf MJ(1), Langendam MW, Sandgren A, Manissero D. Lack of evidence to support policy development for management of contacts of multidrug-resistant tuberculosis patients: two systematic reviews. IJTLD. 2012: 16(3):288–296.
10 Studies of Only LTBI Treatment1. Feja K, McNelley E, Tran C S, et al. Management of pediatricmultidrug-resistant
tuberculosis and latent tuberculosis infections in New York City from 1995 to 2003. Pediatr Infect DisJ 2008; 27: 907–912.
2. Freier G(1), Wright A, Nelson G et al. Multidrug-resistant tuberculosis in military recruits. Emerg Infect Dis. 2006;12(5):760-2.
3. Garcia-Prats AJ, Zimri K, Mramba Z, et al. Children exposed to multidrug-resistant tuberculosis at a home-based day care centre: a contact investigation. Int J Tuberc Lung Dis 2014; 18 (11):1292-98.
4. Horn DL, Hewlett D Jr, Alfalla C, et al. Limited tolerance of ofloxacin and pyrazinamide prophylaxis against tuberculosis. N Engl J Med. 1994 Apr 28;330(17):1241.
5. Lou H X, Shullo M A, McKaveney T P. Limited tolerability of levofloxacin and pyrazinamide for multidrug-resistant tuberculosis prophylaxis in a solid organ transplant population. Pharmacotherapy 2002; 22: 701–704.
6. Miramontes R, Lambert L, Haddad MB, et al. Public health response to a multidrug-resistant tuberculosis outbreak among Guatemalans in Tennessee, 2007. South Med J. 2010 Sep;103(9):882-6. doi: 10.1097/SMJ.0b013e3181eba488.
7. Papastavros T, Dolovich LR, Holbrook A, et al. Adverse events associated with pyrazinamide and levofloxacin in the treatment of latent multidrug-resistant tuberculosis. CMAJ 2002;167 (2) 131–136.
8. Ridzon R, Meador J, Maxwell R, et al. Asymptomatic hepatitis in persons who received alternative preventive therapy with pyrazinamide and ofloxacin. Clin Infect Dis. 1997 Jun;24(6):1264-5.
9. Seddon JA(1), Hesseling AC, Finlayson H, et al. Preventive therapy for child contacts of multidrug-resistant tuberculosis: a prospective cohort study. Clin Infect Dis 2013; 57:1676
10. Younossian AB(1), Rochat T, Ketterer JP, Wacker J, Janssens JP. High hepatotoxicity of pyrazinamide and ethambutol for treatment of latent tuberculosis. Eur Respir J. 2005 Sep;26(3):462-4.
6 Studies of No Effective LTBI Treatment1. Amanullah F, Ashfaq M, Khowaja S, et al. High tuberculosis prevalence in
children exposed at home to drug-resistant tuberculosis. IJTLD. 2014; 18:520.
2. Bayona J, Chavez-Pachas AM, Palacios E, et al. Contact Investigations as a Means of Detection and Timely Treatment of Persons with Infectious Multidrug-resistant Tuberculosis. IJTLD. 2003: 7(12):S501–S509
3. Becerra MC, Franke MF, Appleton SC, et al. Tuberculosis in Children Exposed at Home to Multidrug-resistant Tuberculosis. Pediatr Infect Dis J. 2013; 32:115
4. Kritski AL, Marques MJ, Rabahi MF, et al. Transmission of tuberculosis to close contacts of patients with multidrug-resistant tuberculosis. Am J RespirCrit Care Med. 1996:153(1):331-5.
5. Nitta AT(1), Knowles LS, Kim J, et al. Limited transmission of multidrug-resistant tuberculosis despite a high proportion of infectious cases in Los Angeles County, California. Am J Respir Crit Care Med. 2002 Mar 15;165(6):812-7.
6. Pineiro Perez R, Mellado Pena MJ, Mendez Echevvaria A, et al. Exposicion a tuberculosis multirresistente: estudio y seguimiento de nueve ninos. An Pediatr (Barc). 2008;68(5):490-5.
6 Studies Comparing LTBI Tx vs. No Effective Tx1. Bamrah S, Brostrom R, Fred D, et al. Treatment for Multidrug-Resistant
Latent Tuberculosis Infection—Federated States of Micronesia, 2009–2012. IJTLD. 2014:18(8):912-919.
2. Denholm JT(1), Leslie DE, Jenkin GA, et al. Long-term follow-up of contacts exposed to multidrug-resistant tuberculosis in Victoria, Australia, 1995-2010. IJTLD. 2012:16(10):1320-5.
3. Schaaf et al. Evaluation of Young Children in Contact with Adult Multidrug-resistant Pulmonary Tuberculosis: A 30-month Follow-up. Pediatrics. 2002; 109:765-771
4. Adler-Shohet et al. Management of Latent Tuberculosis Infection in Child Contacts of Multidrug-resistant Tuberculosis. Pediatric Infectious Disease Journal. 2014; 33:664
5. Attamna A, Chemtob D, Attamna S, et al. Risk of tuberculosis in close contacts of patients with multidrug resistant tuberculosis: a nationwide cohort. Thorax. 2009 Mar;64(3):271.
6. Williams B, Ramroop S, Shah P, et al. Management of Pediatric Contacts of Multidrug Resistant Tuberculosis in the United Kingdom, Pediatric Infectious Disease Journal. 2013;32: 926-7.
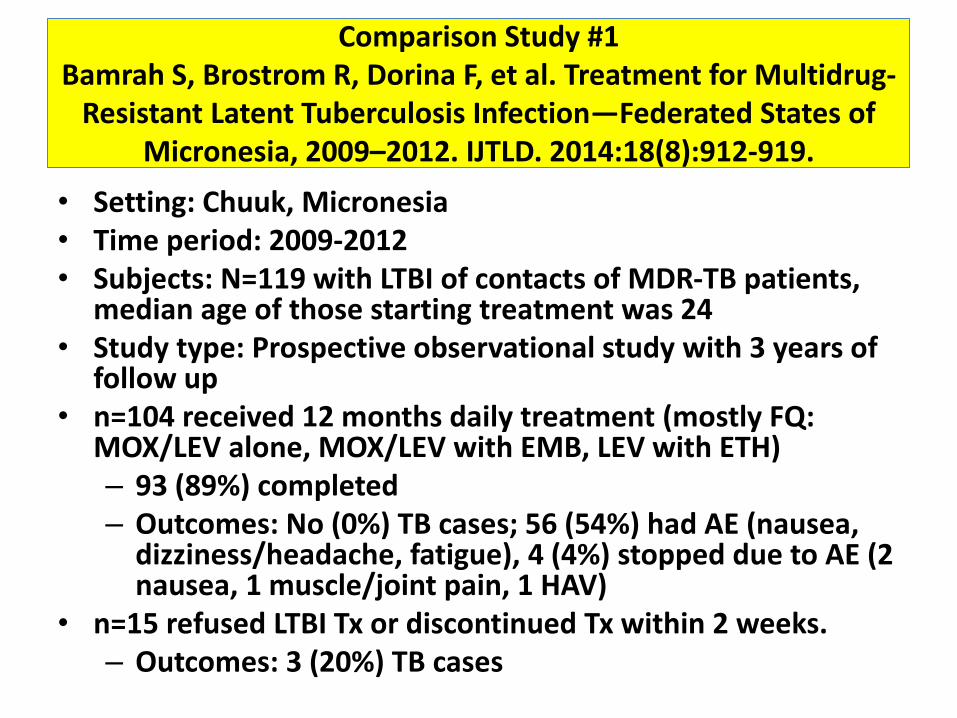
Comparison Study #1 Bamrah S, Brostrom R, Dorina F, et al. Treatment for Multidrug-
Resistant Latent Tuberculosis Infection—Federated States of Micronesia, 2009–2012. IJTLD. 2014:18(8):912-919.
• Setting: Chuuk, Micronesia• Time period: 2009-2012• Subjects: N=119 with LTBI of contacts of MDR-TB patients,
median age of those starting treatment was 24• Study type: Prospective observational study with 3 years of
follow up • n=104 received 12 months daily treatment (mostly FQ:
MOX/LEV alone, MOX/LEV with EMB, LEV with ETH) – 93 (89%) completed – Outcomes: No (0%) TB cases; 56 (54%) had AE (nausea,
dizziness/headache, fatigue), 4 (4%) stopped due to AE (2 nausea, 1 muscle/joint pain, 1 HAV)
• n=15 refused LTBI Tx or discontinued Tx within 2 weeks. – Outcomes: 3 (20%) TB cases
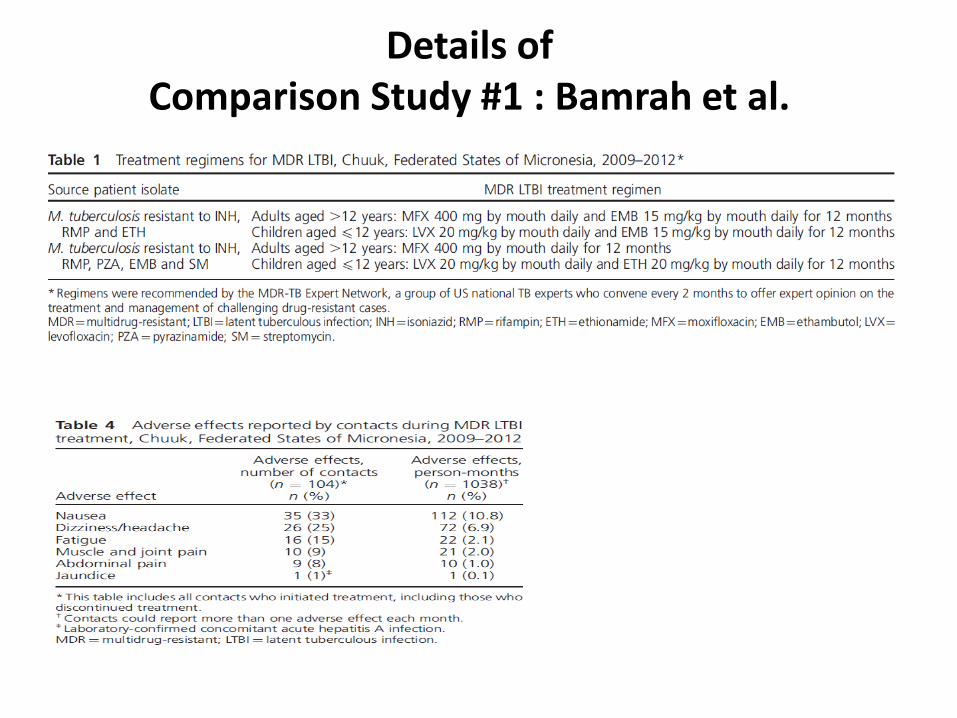
Details of Comparison Study #1 : Bamrah et al.
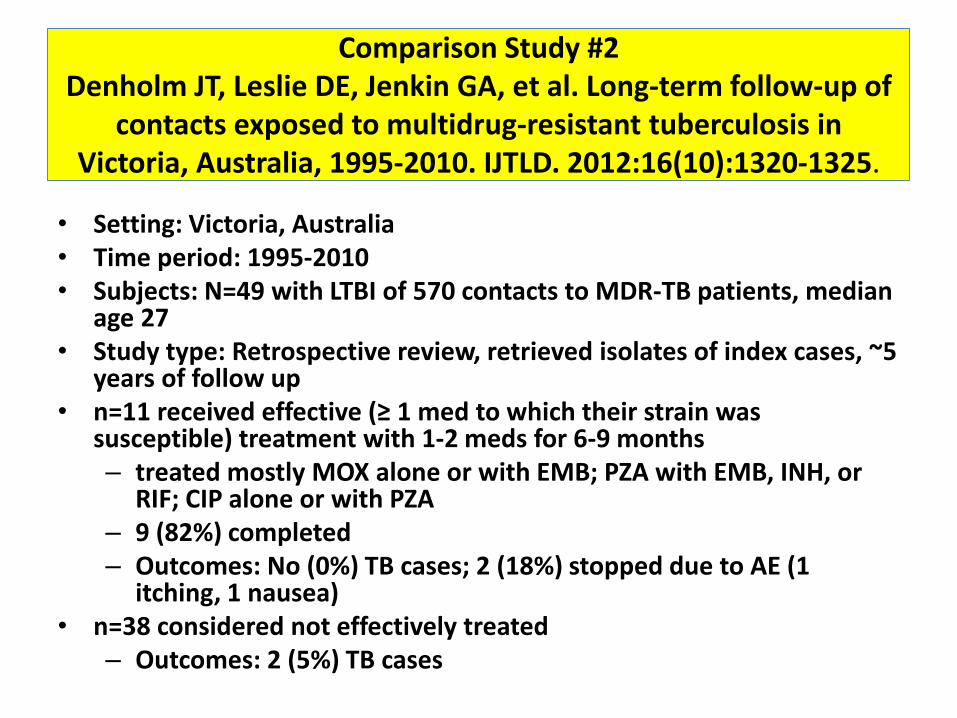
Comparison Study #2 Denholm JT, Leslie DE, Jenkin GA, et al. Long-term follow-up of
contacts exposed to multidrug-resistant tuberculosis in Victoria, Australia, 1995-2010. IJTLD. 2012:16(10):1320-1325.
• Setting: Victoria, Australia• Time period: 1995-2010• Subjects: N=49 with LTBI of 570 contacts to MDR-TB patients, median
age 27• Study type: Retrospective review, retrieved isolates of index cases, ~5
years of follow up• n=11 received effective (≥ 1 med to which their strain was
susceptible) treatment with 1-2 meds for 6-9 months– treated mostly MOX alone or with EMB; PZA with EMB, INH, or
RIF; CIP alone or with PZA– 9 (82%) completed – Outcomes: No (0%) TB cases; 2 (18%) stopped due to AE (1
itching, 1 nausea)• n=38 considered not effectively treated
– Outcomes: 2 (5%) TB cases
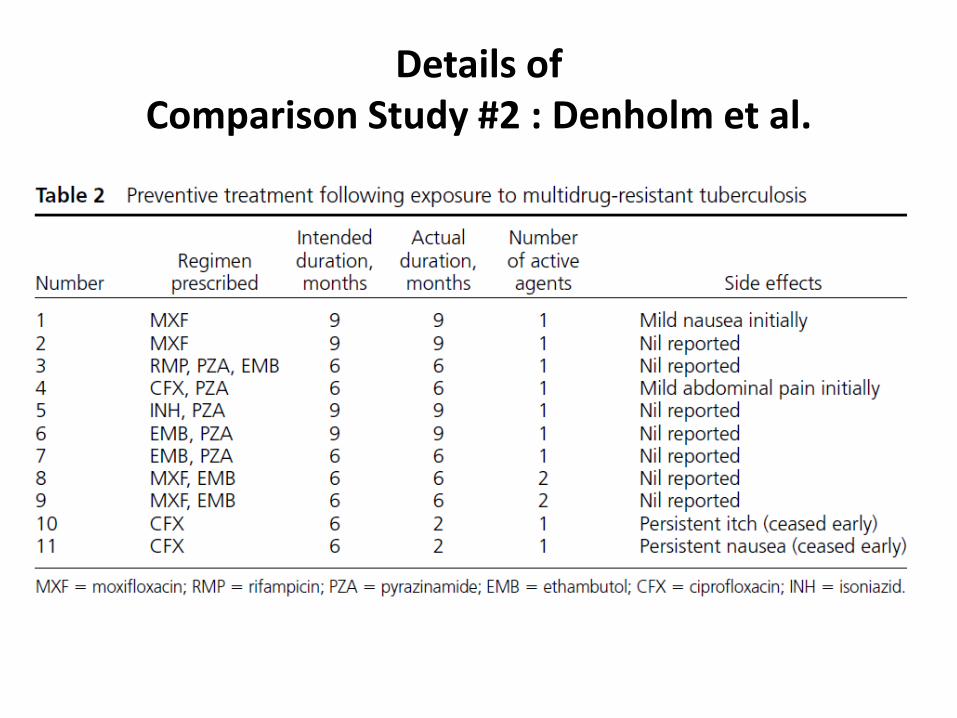
Details of Comparison Study #2 : Denholm et al.
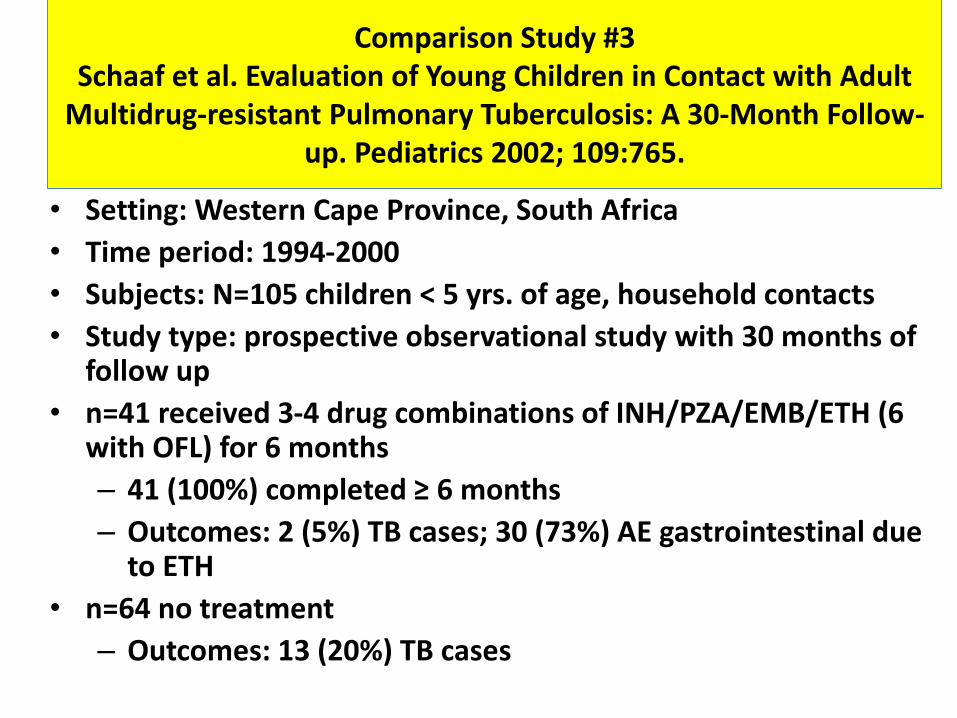
Comparison Study #3 Schaaf et al. Evaluation of Young Children in Contact with Adult
Multidrug-resistant Pulmonary Tuberculosis: A 30-Month Follow-up. Pediatrics 2002; 109:765.
• Setting: Western Cape Province, South Africa
• Time period: 1994-2000
• Subjects: N=105 children < 5 yrs. of age, household contacts
• Study type: prospective observational study with 30 months of follow up
• n=41 received 3-4 drug combinations of INH/PZA/EMB/ETH (6 with OFL) for 6 months
– 41 (100%) completed ≥ 6 months
– Outcomes: 2 (5%) TB cases; 30 (73%) AE gastrointestinal due to ETH
• n=64 no treatment
– Outcomes: 13 (20%) TB cases
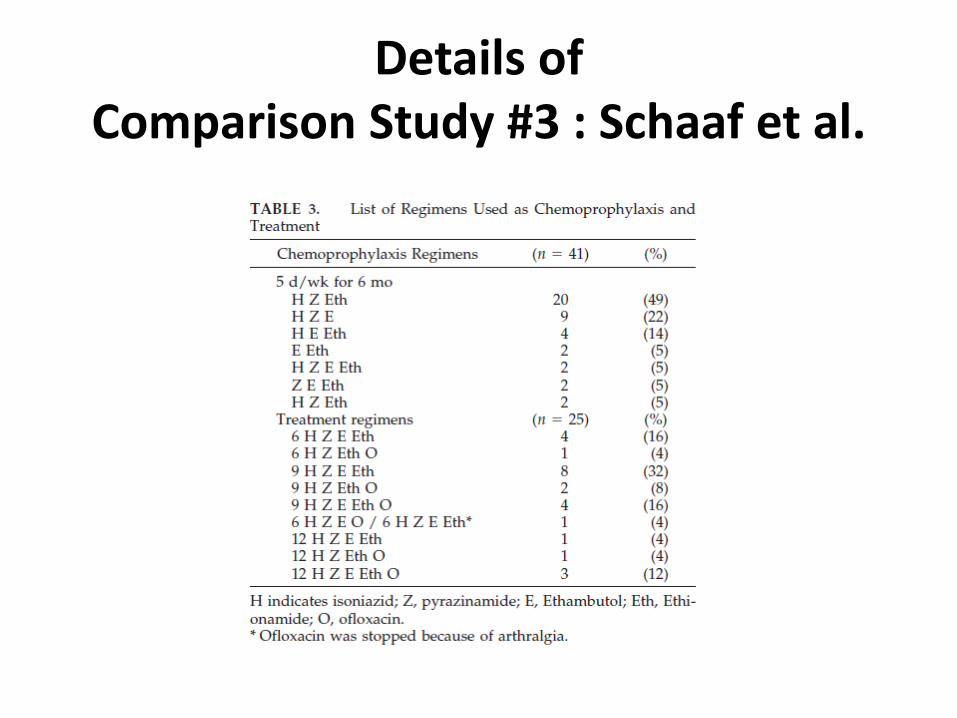
Details of Comparison Study #3 : Schaaf et al.
Comparison Study #4 Adler-Shohet et al. Management of Latent Tuberculosis Infection
in Child Contacts of Multidrug-resistant Tuberculosis. Pediatric Infectious Disease Journal. 2014; 33:664
• Setting: Orange County, California
• Time period: 2013-2014?
• Subjects: N=31 with LTBI
• Study type: prospective observational with 2 years of follow up
• n=26 LTBI treatment of LEV and PZA for 9 months
– 15 (57%) completed
– Outcomes: No (0%) TB cases; 26 (100%) AE, 11 (42%) stopped due to AE
• n=5 no treatment
– Outcomes: No (0%) TB cases
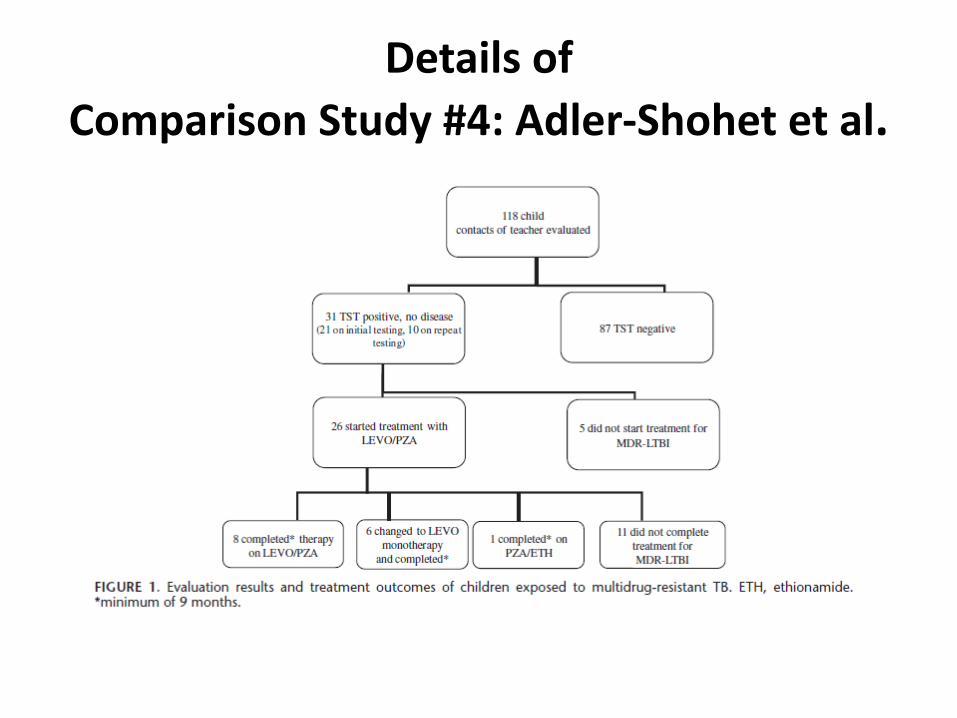
Details of
Comparison Study #4: Adler-Shohet et al.
Comparison Study #5 Attamna A, Chemtob D, Attamna S, et al. Risk of tuberculosis in
close contacts of patients with multidrug resistant tuberculosis: a nationwide cohort. Thorax. 2009 Mar;64(3):271.
• Setting: Israel
• Time period: 1998-2006
• Subjects: N=470 TST+ contacts, median age 29
• Study type: retrospective cohort matched to MDR TB registry to identify incident cases, median of 6 years of follow up
• n=12 LTBI treatment, mainly with CIP and PZA, Tx length?
– Completion unknown %
– Outcomes: No (0%) TB cases; no data on AE
• n=458 no treatment
– Outcomes: No (0%) TB cases
Comparison Study #6 Williams B, Ramroop S, Shah P, et al. Management of Pediatric
Contacts of Multidrug Resistant Tuberculosis in the United Kingdom, Pediatric Infectious Disease Journal. 2013;32: 926-7.
• Setting: UK
• Time period: 2006-2010
• Subjects: N=12 children with LTBI
• Study type: retrospective review with 2 years of follow up
• n=8 LTBI treatment with 2 effective drugs for 6-12 months
– 8 (100%) completion
– Outcomes: No (0%) TB cases; unknown AE
• n=4 no treatment
– Outcomes: No (0%) TB cases
Outcome of TB Incidence
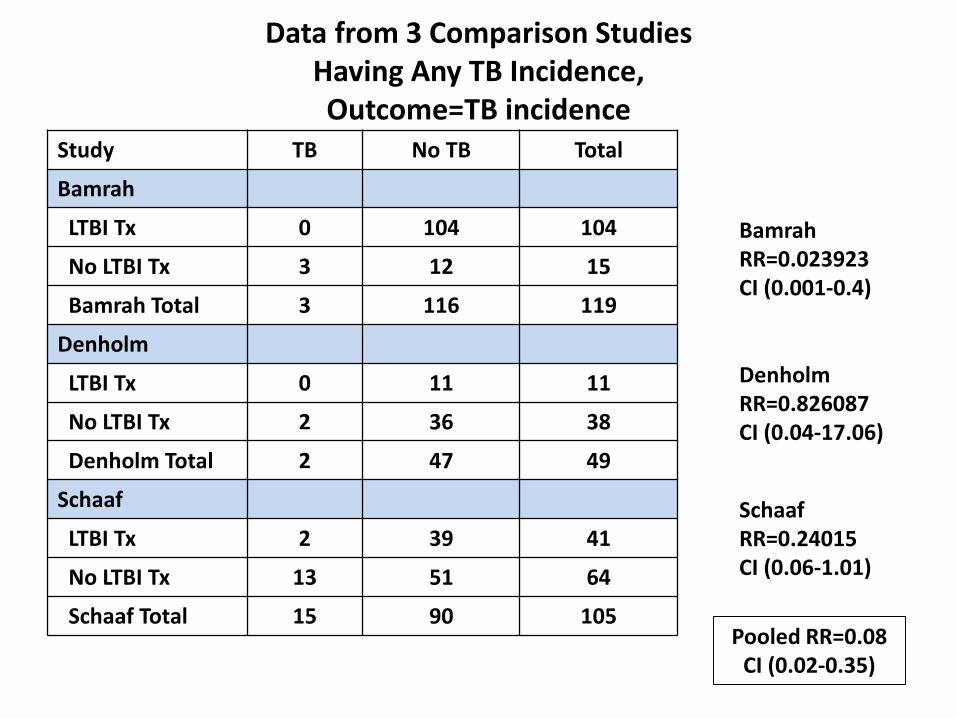
Data from 3 Comparison Studies Having Any TB Incidence, Outcome=TB incidence
Study TB No TB Total
Bamrah
LTBI Tx 0 104 104
No LTBI Tx 3 12 15
Bamrah Total 3 116 119
Denholm
LTBI Tx 0 11 11
No LTBI Tx 2 36 38
Denholm Total 2 47 49
Schaaf
LTBI Tx 2 39 41
No LTBI Tx 13 51 64
Schaaf Total 15 90 105
Bamrah RR=0.023923CI (0.001-0.4)
Denholm RR=0.826087CI (0.04-17.06)
SchaafRR=0.24015CI (0.06-1.01)
Pooled RR=0.08CI (0.02-0.35)
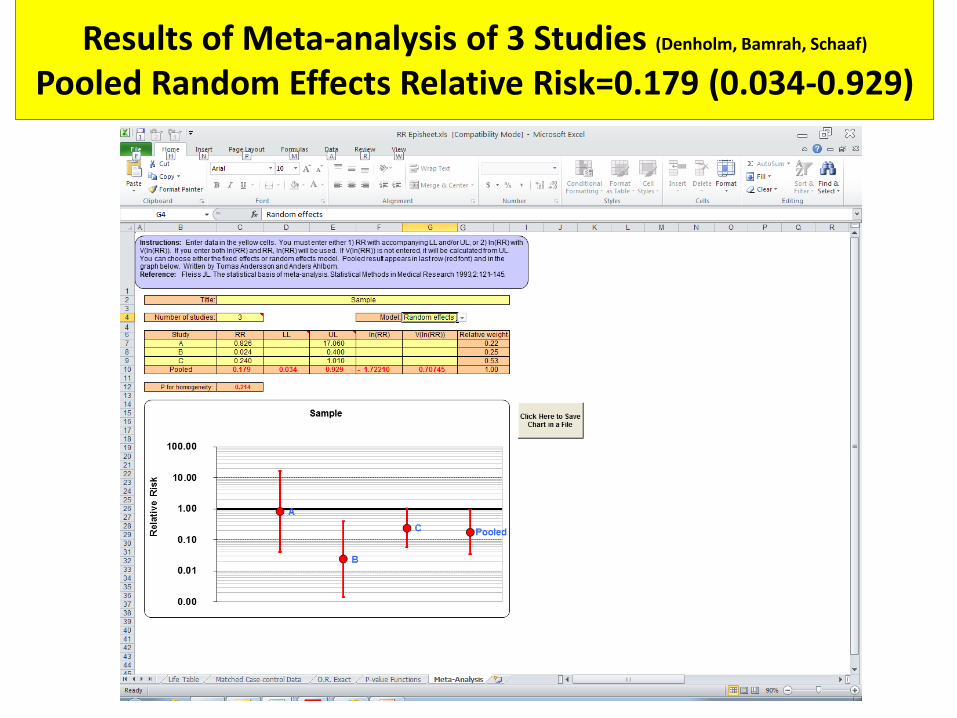
Results of Meta-analysis of 3 Studies (Denholm, Bamrah, Schaaf)
Pooled Random Effects Relative Risk=0.179 (0.034-0.929)
Assessment of Heterogeneity of the 3 Studies: p=0.214
• Assessment of Heterogeneity of the 3 Studies p=0.214: relatively homogenous
• Possible reasons for some heterogeneity:
– Sample size (49, 119, 105)
– Overall TB incidence:
• 4% Australia (Denholm)
• 3% Chuuk (Bamrah)
• 14% South Africa (Schaaf)
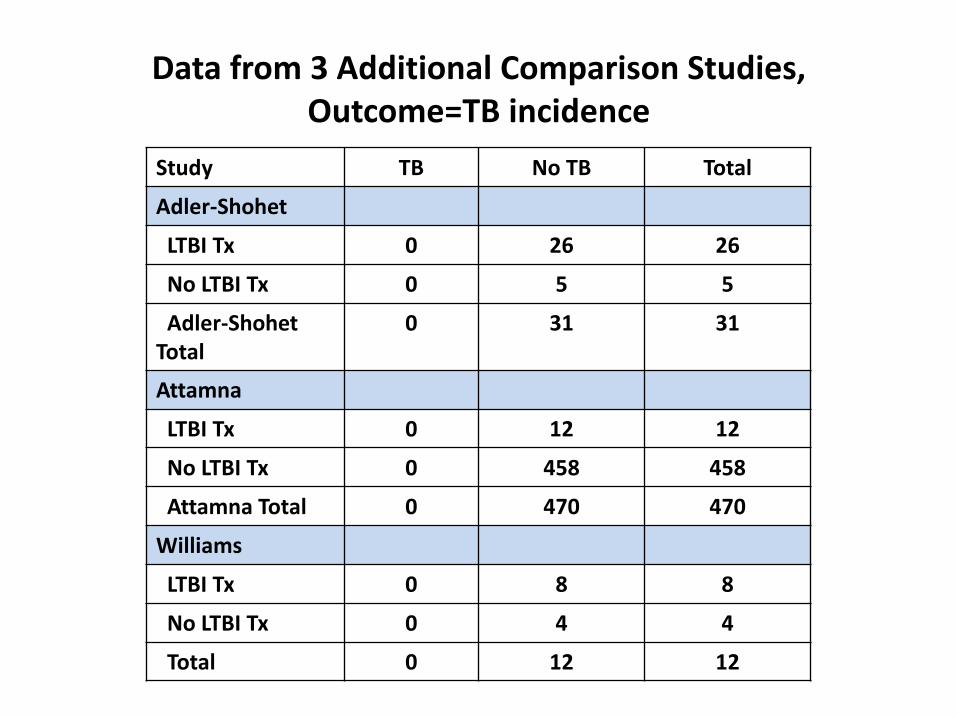
Data from 3 Additional Comparison Studies, Outcome=TB incidence
Study TB No TB Total
Adler-Shohet
LTBI Tx 0 26 26
No LTBI Tx 0 5 5
Adler-ShohetTotal
0 31 31
Attamna
LTBI Tx 0 12 12
No LTBI Tx 0 458 458
Attamna Total 0 470 470
Williams
LTBI Tx 0 8 8
No LTBI Tx 0 4 4
Total 0 12 12
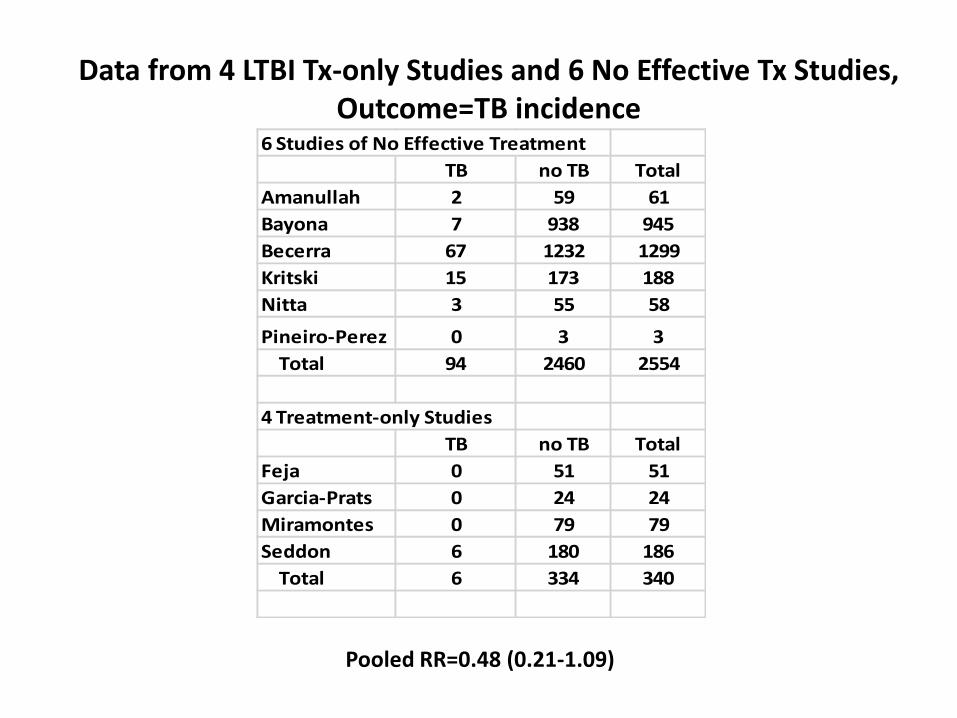
Data from 4 LTBI Tx-only Studies and 6 No Effective Tx Studies, Outcome=TB incidence
6 Studies of No Effective Treatment
TB no TB Total
Amanullah 2 59 61
Bayona 7 938 945
Becerra 67 1232 1299
Kritski 15 173 188
Nitta 3 55 58
Pineiro-Perez 0 3 3
Total 94 2460 2554
4 Treatment-only Studies
TB no TB Total
Feja 0 51 51
Garcia-Prats 0 24 24
Miramontes 0 79 79
Seddon 6 180 186
Total 6 334 340
Pooled RR=0.48 (0.21-1.09)
Outcome of Treatment Completion
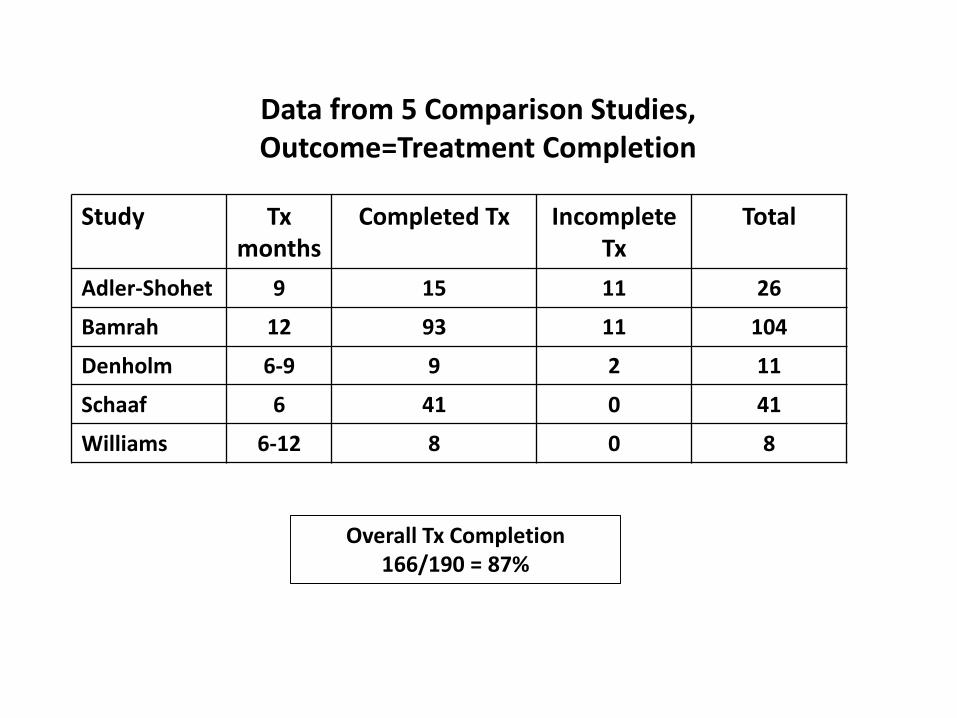
Study Txmonths
Completed Tx Incomplete Tx
Total
Adler-Shohet 9 15 11 26
Bamrah 12 93 11 104
Denholm 6-9 9 2 11
Schaaf 6 41 0 41
Williams 6-12 8 0 8
Overall Tx Completion 166/190 = 87%
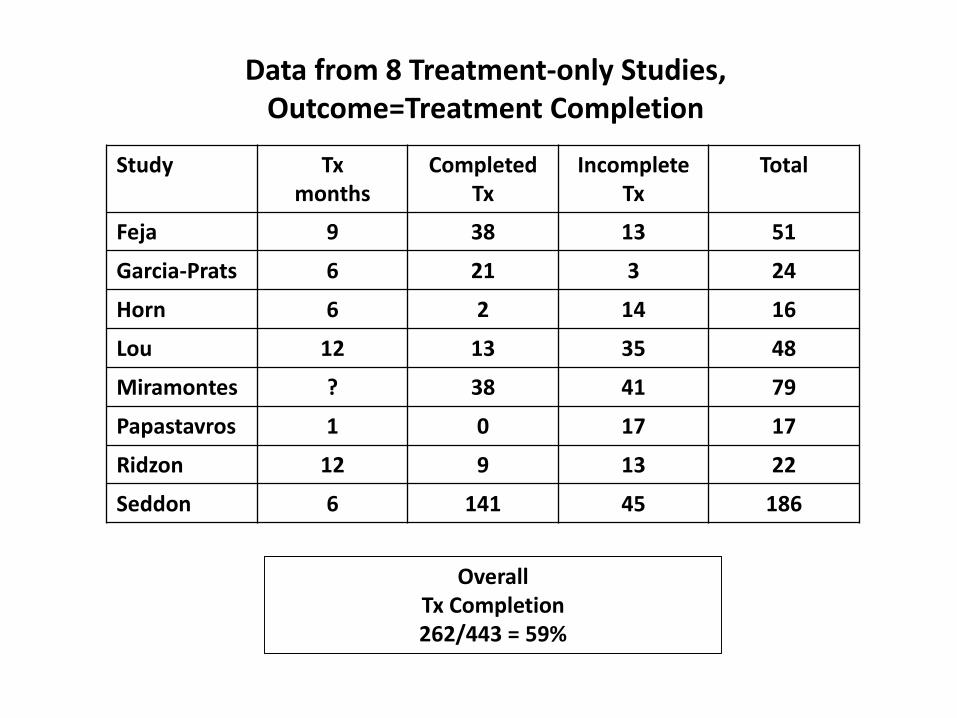
Data from 5 Comparison Studies, Outcome=Treatment Completion
Study Txmonths
CompletedTx
Incomplete Tx
Total
Feja 9 38 13 51
Garcia-Prats 6 21 3 24
Horn 6 2 14 16
Lou 12 13 35 48
Miramontes ? 38 41 79
Papastavros 1 0 17 17
Ridzon 12 9 13 22
Seddon 6 141 45 186
Overall Tx Completion 262/443 = 59%
Data from 8 Treatment-only Studies, Outcome=Treatment Completion
Outcome of Adverse Effects (AE)
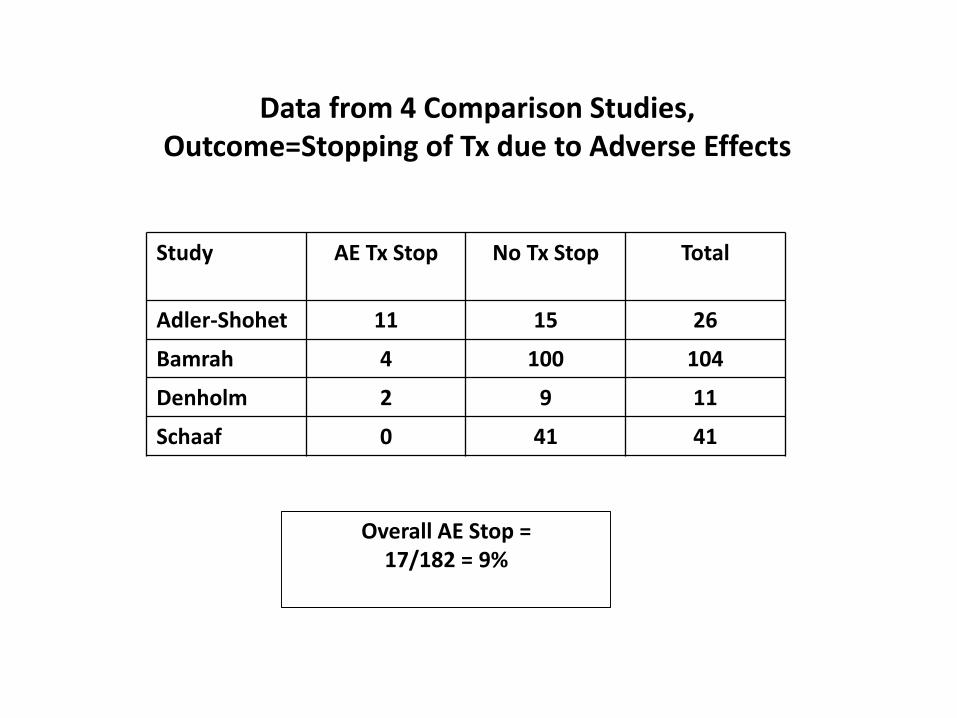
Study AE Tx Stop No Tx Stop Total
Adler-Shohet 11 15 26
Bamrah 4 100 104
Denholm 2 9 11
Schaaf 0 41 41
Overall AE Stop =17/182 = 9%
Data from 4 Comparison Studies, Outcome=Stopping of Tx due to Adverse Effects
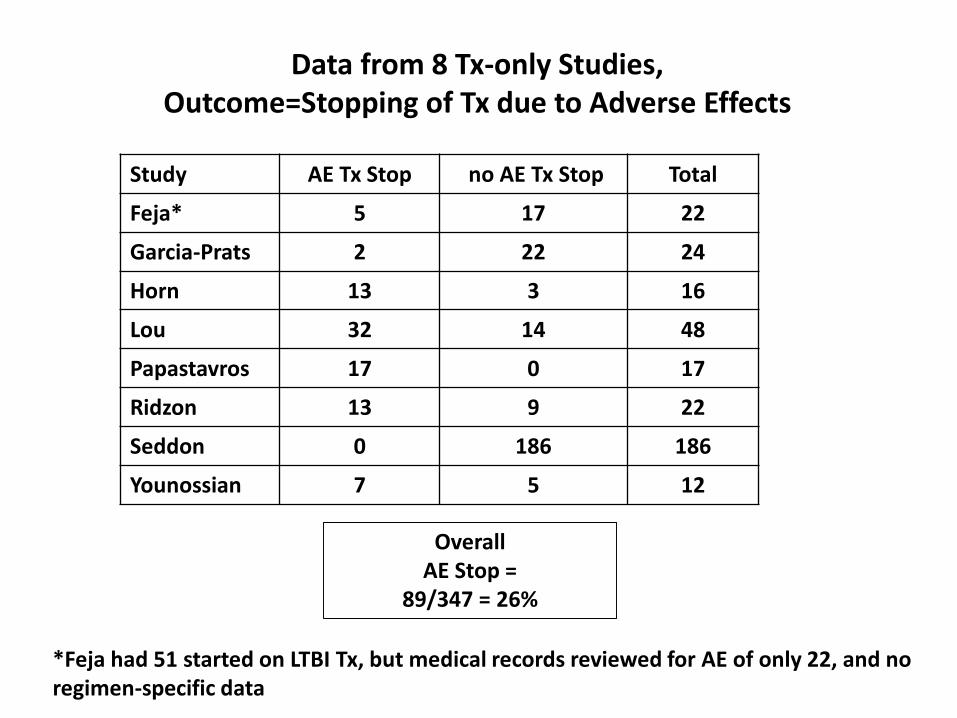
Study AE Tx Stop no AE Tx Stop Total
Feja* 5 17 22
Garcia-Prats 2 22 24
Horn 13 3 16
Lou 32 14 48
Papastavros 17 0 17
Ridzon 13 9 22
Seddon 0 186 186
Younossian 7 5 12
Overall AE Stop =
89/347 = 26%
Data from 8 Tx-only Studies, Outcome=Stopping of Tx due to Adverse Effects
*Feja had 51 started on LTBI Tx, but medical records reviewed for AE of only 22, and no regimen-specific data
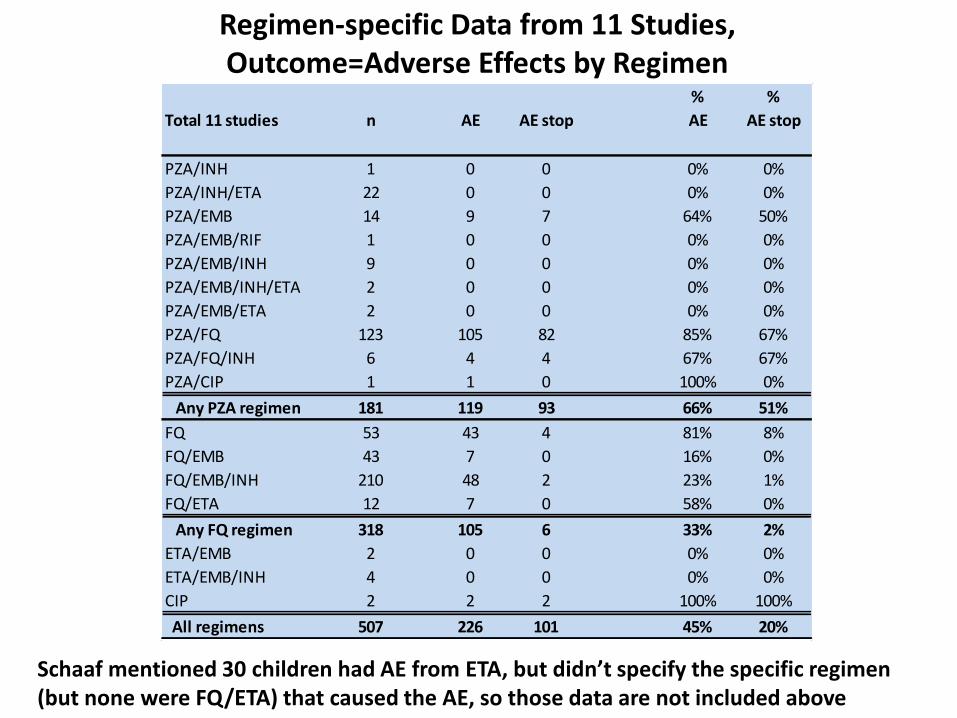
Regimen-specific Data from 11 Studies, Outcome=Adverse Effects by Regimen
% %
Total 11 studies n AE AE stop AE AE stop
PZA/INH 1 0 0 0% 0%
PZA/INH/ETA 22 0 0 0% 0%
PZA/EMB 14 9 7 64% 50%
PZA/EMB/RIF 1 0 0 0% 0%
PZA/EMB/INH 9 0 0 0% 0%
PZA/EMB/INH/ETA 2 0 0 0% 0%
PZA/EMB/ETA 2 0 0 0% 0%
PZA/FQ 123 105 82 85% 67%
PZA/FQ/INH 6 4 4 67% 67%
PZA/CIP 1 1 0 100% 0%
Any PZA regimen 181 119 93 66% 51%
FQ 53 43 4 81% 8%
FQ/EMB 43 7 0 16% 0%
FQ/EMB/INH 210 48 2 23% 1%
FQ/ETA 12 7 0 58% 0%
Any FQ regimen 318 105 6 33% 2%
ETA/EMB 2 0 0 0% 0%
ETA/EMB/INH 4 0 0 0% 0%
CIP 2 2 2 100% 100%
All regimens 507 226 101 45% 20%
Schaaf mentioned 30 children had AE from ETA, but didn’t specify the specific regimen (but none were FQ/ETA) that caused the AE, so those data are not included above
Adverse Effects, Stratified by Studies of Children Aged <15 versus Those of Other Ages
• From 11 studies presenting data on adverse effects by regimen:
– 4 were in children aged < 15 years
• 13/277 = 5% AE treatment stop
– 7 were in persons having a median age > 15 years of age
• 88/230 = 38% AE treatment stop
Limitations
• Overall quality of evidence was very low
• Few studies reported the outcomes of interest
Cost-effectiveness: Holland DP, Sanders GD, Hamilton CD, Stout JE. Strategies for Treating Latent Multiple-
Drug Resistant Tuberculosis: A Decision Analysis. PLoSONE. 2012;7(1):e30194.
• Decision analysis of 6 month MDR LTBI Tx regimens:– PZA/EMB– MOX– MOX/PZA– MOX/EMB– MOX/ETH– MOX/PA-824
• Efficacy estimates from mouse models; toxicity from various studies, but excluding Bamrah, and assumed toxicity for MOX and MOX/EMB
• Range of AE stop was 4%-67%• MOX alone was lowest cost; MOX/EMB was incrementally cost effective• Hypothetical regimen of low toxicity and modest efficacy was cost
effective vs. no MDR LTBI treatment
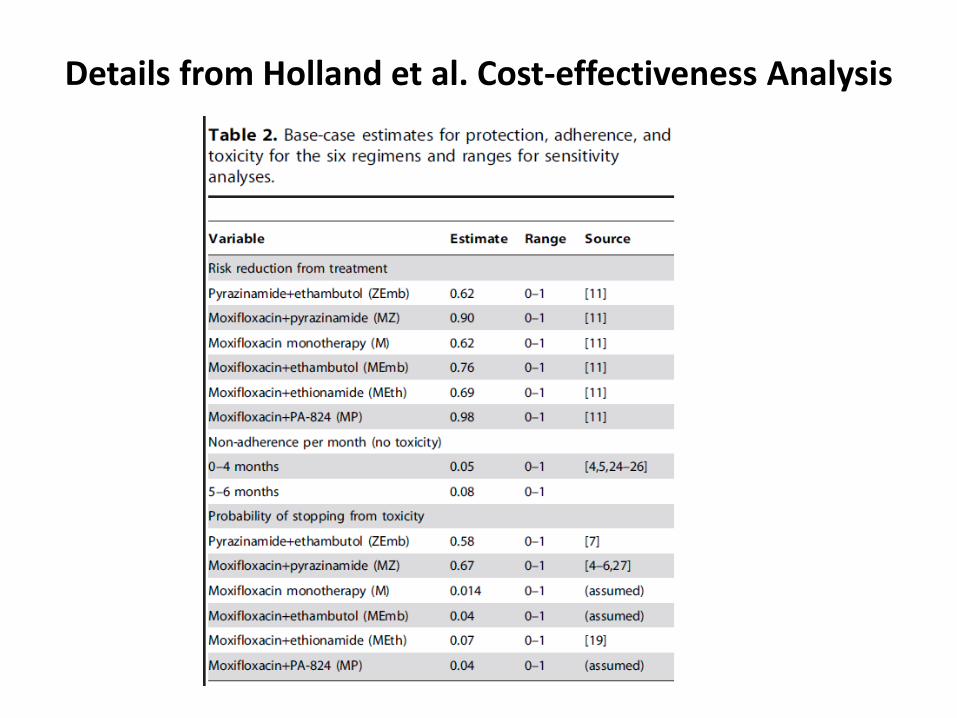
Details from Holland et al. Cost-effectiveness Analysis
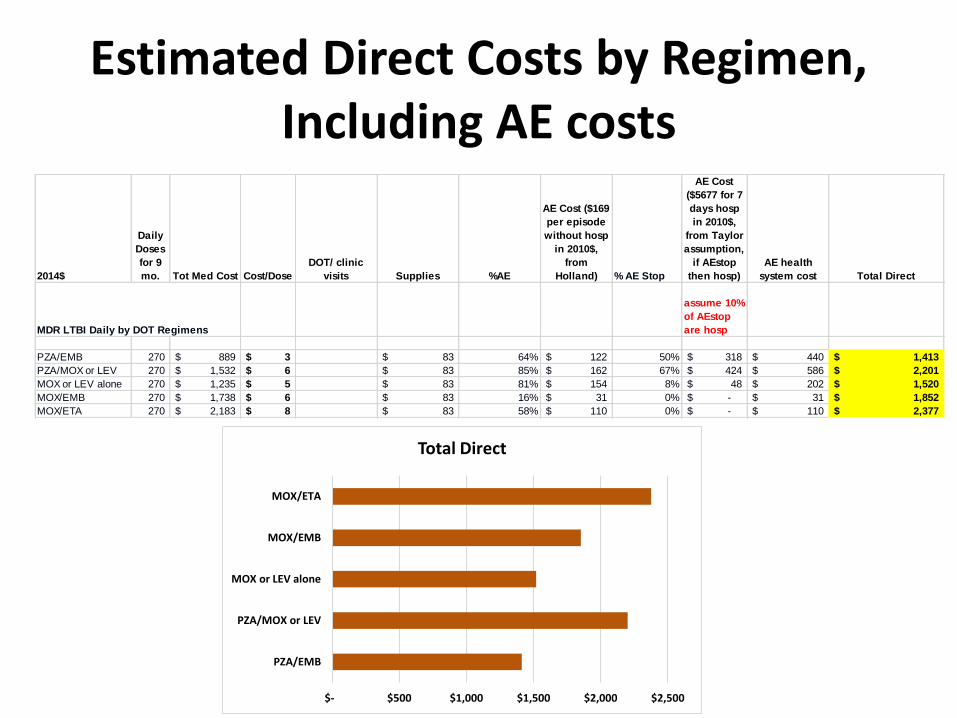
Estimated Direct Costs by Regimen, Including AE costs
2014$
Daily
Doses
for 9
mo. Tot Med Cost Cost/Dose
DOT/ clinic
visits Supplies %AE
AE Cost ($169
per episode
without hosp
in 2010$,
from
Holland) % AE Stop
AE Cost
($5677 for 7
days hosp
in 2010$,
from Taylor
assumption,
if AEstop
then hosp)
AE health
system cost Total Direct
MDR LTBI Daily by DOT Regimens
assume 10%
of AEstop
are hosp
PZA/EMB 270 889$ 3$ 83$ 64% 122$ 50% 318$ 440$ 1,413$
PZA/MOX or LEV 270 1,532$ 6$ 83$ 85% 162$ 67% 424$ 586$ 2,201$
MOX or LEV alone 270 1,235$ 5$ 83$ 81% 154$ 8% 48$ 202$ 1,520$
MOX/EMB 270 1,738$ 6$ 83$ 16% 31$ 0% -$ 31$ 1,852$
MOX/ETA 270 2,183$ 8$ 83$ 58% 110$ 0% -$ 110$ 2,377$
$- $500 $1,000 $1,500 $2,000 $2,500
PZA/EMB
PZA/MOX or LEV
MOX or LEV alone
MOX/EMB
MOX/ETA
Total Direct
Summary of Findings
• Very few studies met the inclusion criteria
• Results should be cautiously interpreted
• We found, by using meta-analysis, some empirical evidence suggesting effectiveness of LTBI treatment in preventing progression to MDR-TB disease
• We also found high discontinuation rates due to adverse effects and toxicity in those patients taking PZA containing MDR-LTBI regimens (especially PZA/FQ)
Discussion
• Trials are needed, but TB incidence in low incidence settings is too low
• Adverse effects by regimen: Nix PZA regimens?
• Cost effectiveness greatest with FQ or FQ/EMB
Detection of 1 Incident MDR TB Case
• ~100 MDR-TB cases in the U.S. per year
– ~80%=80 cases/year are infectious (pulmonary, sputum smear positive)
• ~ 20 contacts/case = 1600 MDR TB contacts– ~30% to 40% have LTBI = 480 to 640/year
– Estimated TB incidence is 0.00032/year (Walter) to 0.00084/year (Shea)
» MDR TB incidence = 0.15 to 0.54 cases per year
» So, it would take 2 to 7 years to detect one incident MDR TB case
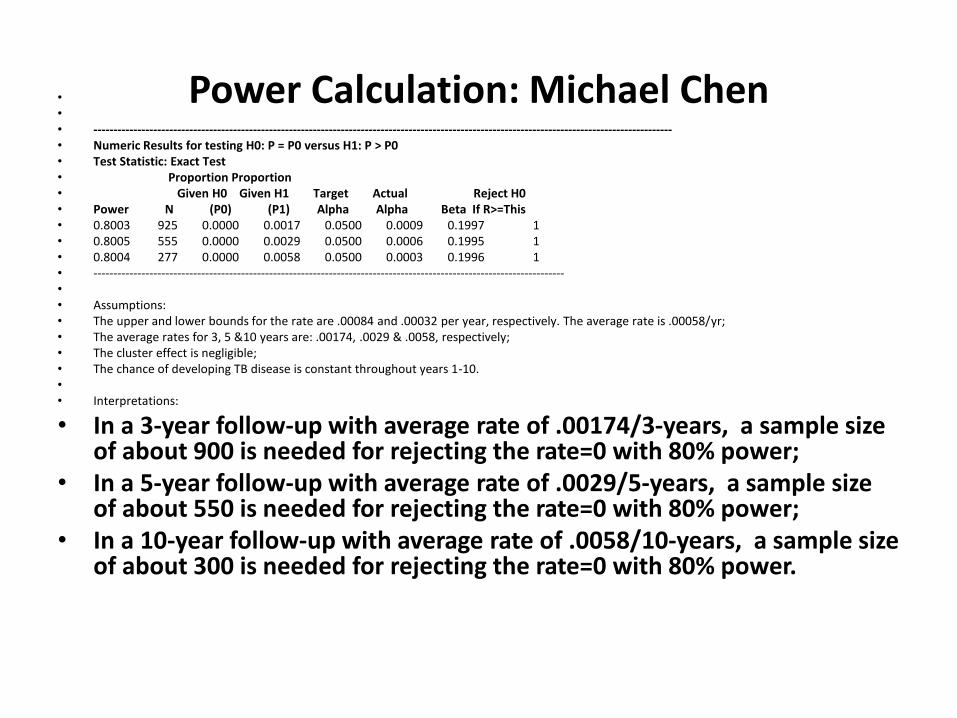
Power Calculation: Michael Chen•
•
• -------------------------------------------------------------------------------------------------------------------------------------------------• Numeric Results for testing H0: P = P0 versus H1: P > P0• Test Statistic: Exact Test• Proportion Proportion• Given H0 Given H1 Target Actual Reject H0• Power N (P0) (P1) Alpha Alpha Beta If R>=This• 0.8003 925 0.0000 0.0017 0.0500 0.0009 0.1997 1• 0.8005 555 0.0000 0.0029 0.0500 0.0006 0.1995 1• 0.8004 277 0.0000 0.0058 0.0500 0.0003 0.1996 1• ----------------------------------------------------------------------------------------------------------------------•
• Assumptions:• The upper and lower bounds for the rate are .00084 and .00032 per year, respectively. The average rate is .00058/yr;• The average rates for 3, 5 &10 years are: .00174, .0029 & .0058, respectively; • The cluster effect is negligible;• The chance of developing TB disease is constant throughout years 1-10.•
• Interpretations:
• In a 3-year follow-up with average rate of .00174/3-years, a sample size of about 900 is needed for rejecting the rate=0 with 80% power;
• In a 5-year follow-up with average rate of .0029/5-years, a sample size of about 550 is needed for rejecting the rate=0 with 80% power;
• In a 10-year follow-up with average rate of .0058/10-years, a sample size of about 300 is needed for rejecting the rate=0 with 80% power.