Embed Size (px)
Citation preview
1
Home Care Basics: Getting Started in Home Health
EILEEN BACH PT, M.ED, DPT, COS-C, CHC
© Eileen Bach
Provider Disclaimer
• Allied Health Education and the presenter of this
webinar do not have any financial or other
associations with the manufacturers of any products
or suppliers of commercial services that may be
discussed or displayed in this presentation.
• There was no commercial support for this
presentation.
• The views expressed in this presentation are the
views and opinions of the presenter.
• Participants must use discretion when using the
information contained in this presentation.
Home is the Place where….Course Description
• Home health is a growing post-acute care practice area for rehabilitation therapists. Home is the location most older adults choose to be even if health care is needed. Working in home care provides the rehab clinician with the opportunity to work one-one-one with each client and to provide services in the most functional setting. Home care offers both pros and cons to the rehab clinician; getting started in the home health setting can be an easier transition when the clinician is well prepared for this work.
• This lecture based webinar will cover the key regulatory elements of Home
Health as well as the knowledge, skills and abilities to help the new clinician to
home care thrive. Strategies to increase caseload organization, time
management, patient engagement and practice tips will be covered. Examples
illustrating care expectations and documentation processes will be discussed.
Resources are provided to connect the rehabilitation clinician with source
references for the Home Health setting.
2
Course Objectives
At this end of this seminar, the participant will be able to independently:
1. Explain Home Health regulations including the Center for Medicare and Medicaid Services (CMS) Home Health standards.
2. Define 3 clinical competencies needed to demonstrate effective service provision in the home health setting.
3. Identify the Medicare criteria for skilled care and homebound status, including documentation required.
4. Discuss 2-3 strategies to assist in caseload management and to improve patient outcomes.
Survey Question
Your Speaker – Eileen Bach
I have worked in the home health setting for the past 33 years. In addition to
field experience, I have served as a rehabilitation manager for both hospital
based and non-profit community based agencies.
My roles have included managing and directing interdisciplinary staff,
agency wide education and training, program development, quality and
accreditation leadership. I am a certified OASIS clinical specialist and
currently work in Home Health Compliance.
3
Course Agenda
•Introduction, course framework and CE requirements
•Home Health setting regulatory requirements; Medicare criteria for
Home Health; standards for therapy plan of care and goals
•Providing skilled care and related elements: assessments, plans of care,
documentation, care management and transitions
•Caseload management: organizing, prioritizing, scheduling, and
timeliness
•Patient centric care; outcomes and patient satisfaction in home health
•Review of resources and references; final Q&A
My Definition - Home Health Care Is…
Care at home that:
Supports individuals and families
Creates an environment for healing
Maximizes functional abilities
Home Care is…. Post-Acute Care
•Post acute care is any health care provided after inpatient hospitalization and includes:
In Patient Rehabilitation
Home Health Care
Skilled Nursing Facilities
Outpatient Care
4
Home Health Care Data
•In 2014, CDC reported 12,400 home health agencies 80% of agencies are For-Profit
•People receiving home health services – 4.9 million
•Services received: RN -84%, PT-40%, OT-14% 37% are noted to need assistance with ADL’s
• Source: http://www.cdc.gov/nchs/fastats/home-health-care.htm
Certified Home Health Care
•Only type of home care approved by the Centers for Medicare and Medicaid Services (CMS) to bill Medicare for services [Part A]
•To become Medicare Certified, a home care agency must: Offer multiple services (e.g. RN, PT, OT, aide)
Comply with all Conditions of Participation
Use standardized assessment and billing processes
Meet all state regulations for Home Health care
•Optional – Quality Accreditation such as accreditation from Joint Commission or CHAP (Community Health Accreditation Partner)
Understanding Medicare
•Many private and managed payers follow the Medicare established criteria for home health.
•Medicare WANTS all providers to understand home health requirements and issues
•Recommendation –please bookmark - www.cms.gov/center/hha.asp
This website provides multiple links to CMS reports, proposed changes, manuals, transmittals, billing information, home health compare and more
5
Medicare Home Health Care Framework
•60 day episode of care
Unlimited number of episodes under
Medicare
Home Care is a Medicare Part A
benefit and does not require any
hospital stay prior to home care
•Physician orders and a face-to-face
encounter with physician required
•Prospective payment system for
Medicare Home care
Prospective Payment System (PPS)
•PPS is used in key post-acute care settings regulated by CMS Home Health Care
Skilled Nursing Facility
In Patient Rehab
•PPS - determination by CMS of payment amount for healthcare provided, related quality indicators and adverse events reporting
•The IMPACT Act of 2014 – standardized data sets related to quality, resources used and other measures across post-acute
Home Health Medicare Payment under PPS
•Case Mix Model used which recognizes that different types of patients require different levels of resources
Each patient has a Clinical, Functional and Service score (called HHRG score) that reflects case payment
Other factors such as regional wage index or rural vs. urban agency considered
•Home Care PPS quantifies the relationship between patient characteristics and amount or type of resource utilization
Increased payment for select Diagnoses, services or needs
Rehabilitation therapy services payment levels
6
Discussion: Patient Populations Seen in Home Care
•Diverse socioeconomics
•Multilingual
•Ages - birth to centenarians
•Acute and Long term care needs
• Complex medical conditions
• Polypharmacy
• Typical history - acute hospital stay in previous months
• Variable health literacy
Medicare Criteria for Home Care
Patient under a physician’s care (including Face-to-Face documentation) and
Care provided is:
•Reasonable & Necessary
•Homebound
•Skilled and Intermittent
Discussion: Reasonable and Necessary
7
Discussion: Homebound
CMS Homebound Clarification - 2 criteria
must be met
•Criteria 1 – individual must meet ONE
Due to illness or injury, need for device (cane, walker, W/C), need for assist of a person, or need special transportation to leave the home
OR - has condition where leaving home is medically contraindicated
•Criteria 2 – individual must meet BOTH
Must exist a normal inability to leave the home
AND – leaving home must require considerable and taxing effort
Medicare Learning Network - http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/MM8444.pdf
Change Request 8444 - http://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R172BP.pdf
Discussion: Skilled and Intermittent
8
Skilled Care Is…
Hands on CareSpecifically selected to
meet care needs
Goal Oriented
Builds/transfers
knowledge and
abilities
Standardized Assessment in HC
•All Certified Home Health Care agencies in the US use a standardized assessment document -OASIS (Outcomes ASsessment
Information Set)
Current version is OASIS C-1 (next version C-2 is effective January 1, 2017)
•OASIS is a tool that includes key data sets such as demographics, diagnoses, cognition, function, pain, caregivers and more to create the case mix for PPS
Agency adds comprehensive assessment items to complete information needed for care plan
OASIS Tool
•OASIS assessment is completed at key time points such as admission, recertification, transfer to hospital or discharge from home care
•Specific items are used for PPS case mix payment and/or for quality indicators
•Process Measures may be tracked from initial assessment through re-certification and to discharge
•Electronic version easier to use than paper version
9
OASIS Timepoints (Types)
1. Initial Assessment (Start of Care)
4. Recertification – subsequent care episodes
>Transfer to Inpatient facility
6. Transfer, No discharge (Medicare/ Medicaid)
7. Transfer, Discharge (Other payors)
3. Resumption of Care
5. Other Follow-up
8. Death at Home
9. Discharge from agency
Process Measures in OASIS
Once Start of Care assessment is completed, process measures look to confirm:
•Timeliness - assessment, medication reconciliation
•Interventions indicated are implemented
•Education is provided to patient/caregiver
• Depression
• Diabetic foot care
• Pain
• Heart Failure
• Pressure Ulcers treatment & prevention
• Falls Prevention
• Medication reconciled with MD, meds taught
Understanding OASIS Documentation-Resources
•CMS.gov – User manuals
•https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HomeHealthQualityInits/HHQIOASISUserManual.html
•Chapter 3 – every OASIS item has the following info from CMS:
Item, Intent of item, Time points when item is required, Specific instructions in answering each item and data sources/resources
The tips and instructions to answer each item are VERY helpful!!
Current OASIS C1 and new version OASIS C2 effective 1/1/2017 available
Also available – OASIS Q&A [CMS answers to questions from OASIS users] http://www.oasisanswers.com/aboutoas_links.htm
10
Example of an OASIS C-2 Item
(M1800) Grooming: Current ability to tend safely to personal hygiene needs (specifically: washing face and hands, hair care, shaving or make up, teeth or denture care, fingernail care).
⃞ 0 - Able to groom self unaided, with or without the use of assistive devices or adapted methods.
⃞ 1 - Grooming utensils must be placed within reach before able to complete grooming activities.
⃞ 2 - Someone must assist the patient to groom self.
⃞ 3 - Patient depends entirely upon someone else for grooming needs.
To answer - Enter Level [where clinician enters one number from 0 to 3]
Functional Domain – OASIS Items
•Level of function is based on: Reported/observed functional ability [not “patient preferred” or willingness]
Direct observation is Preferred
Assistance [consider if equipment, hands on, verbal or tactile cues…] needed Caregiver help is not scored as part of ability
SAFETY – any unsafe performance affects your rating
•Read each item carefully Items may contain multiple tasks or actions; use CMS guidance for accuracy
•Related functions should be comparable: i.e. toilet hygiene/dressing
Example of OASIS Process Measures
•(M1240) Has this patient had a formal Pain Assessment using a standardized pain assessment tool (appropriate to the patient’s ability to communicate the severity of pain)?
⃞ 0 - No standardized assessment conducted
⃞ 1 - Yes, and it does not indicate severe pain
⃞ 2 - Yes, and it indicates severe pain
•(M1242) Frequency of Pain Interfering with patient's activity or movement:
⃞ 0 - Patient has no pain
⃞ 1 - Patient has pain that does not interfere with activity or movement
⃞ 2 - Less often than daily
⃞ 3 - Daily, but not constantly
⃞ 4 - All of the time
11
Tips to master …OASIS Documentation
•Take advantage of your HC agency’s orientation and training sessions•Review the OASIS user manual Chapter 3 – especially the intent of key items and the specific instructions/tips for how to select the answer
Download/print the sections you are likely to want to review over and over again such as Integumentary, ADLs, medications….
•Ask to observe an experienced clinician complete an OASIS - start of care and discharge will be the ones most often completed.
•At team meetings, or when meeting with supervisor, ask for OASIS resources – your agency may have items such as tips sheets, How to Q&A, wound assessment elements and more
Skilled Interventions: Therapy Source- Conditions of participation, CMS
Therapy services. 484.32
Any therapy services offered by the HHA directly or under arrangement are given by a qualified therapist or by a qualified therapy assistant under the supervision of a qualified therapist and in accordance with the plan of care. The qualified therapist assists the physician in evaluating level of function, helps develop the plan of care(revising it as necessary), prepares clinical and progress notes, advises and consults with the family and other agency personnel, and participates in in-service programs
https://www.cms.gov/CFCsAndCoPs/
CMS: Covered Therapy Services
“There must be an expectation that the beneficiary’s condition will improve materially in a reasonable (and generally predictable) period of time based on the physician’s assessment of the beneficiary’s restoration potential & unique medical condition, or the services must be necessary to establish a safe & effective maintenance program required in connection with a specific disease, or the skills of a therapist must be necessary to perform a safe & effective maintenance program.
If the services are for the establishment of a maintenance program, they may include the design of the program, the instruction of the beneficiary, family, or home health aides, and the necessary infrequent reevaluations of the beneficiary and the program to the degree that the specialized knowledge and judgment of a physical therapist, speech-language pathologist, or occupational therapist is required.”
33
12
CMS Example of Maintenance Therapy
“Maintenance therapy, when the specialized knowledge and judgment of a qualified therapist is required to design and establish a maintenance program based on an initial evaluation and periodic reassessment of the patient’s needs, and consistent with the patient’s capacity and tolerance.
For example, a patient with Parkinson’s disease who has not been under a rehabilitation regimen may require the services of a qualified therapist to determine what type of exercises will contribute the most to the maintenance of his present level of functioning.”
Maintenance therapy is:
•Designing & setting up a safe and effective maintenance program to maintain function and/or prevent regression for specific illness/injury
•Instructing patient, family and HHaides in the program (not HHaide only)
•Infrequently re-evaluating the program and/or the patient
http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/Downloads/MM8458.pdf
REQUIRES the specialized knowledge and judgement of the therapist (OT, PT, ST)
Improvement Standard: CMS Updated Guidance effective 1/7/14; additional guidance expected 2016-7
Restorative/Rehabilitative therapy (…where goal and/or treatment purpose is to reverse, in whole or in part, a previous loss of function), it would be entirely appropriate to consider the beneficiary’s potential for improvement from the services.
Maintenance therapy. Even if no improvement is expected, skilled therapy services are covered when an individualized assessment of the patient’s condition demonstrates that skilled care is necessary for the performance of a safe and effective maintenance program to maintain the patient’s current condition or prevent or slow further deterioration and the services cannot be safely and effectively carried out by the beneficiary personally or with the assistance of non-therapists, including unskilled caregivers.
13
Medicare Therapy Requirements Resource: www.cms.gov/center/hha.asp
Plan of Care describes Treatment & goals consistent with functional evaluation Therapy goals created by qualified therapist with physician collaboration
Goals are measurable; relate to illness or impairment
Initial assessment by therapist; reassessment on or before 30th day by therapist
Clinical record reflects: How therapy treatment is within accepted standards of clinical practice
Function assessed via objective measurements enabling comparison measurements to determine effectiveness of therapy goals. (progress towards goals)
G Codes: Visit billing (G codes) for home care include:
1. Visit type -Care visit or maintenance therapy visit (codes for OT, PT, ST)
2. Exact provider - visit from therapist (codes for OT, PT, ST) OR an assistant (codes for PTA, COTA)
3. Location – where patient received home care services (codes for home, assisted living, other)
Skilled Therapy Services Are:
•Considered accepted professional practice
•Specific, safe and effective treatment for patient condition
•Necessary (medically justified)
•Documented with objective evidence that shows: Improvement (restorative)
OR
Prevention of decline and/or stabilization in patient condition (maintenance)
Recommendations to Meet Therapy Requirements
•Stay current in best clinical practice for your discipline
•Use evidence based information and protocols
•Become proficient in administering and interpreting standardized tests and measures
•Manage the therapy plan of care on every visit – update treatment plan, equipment used, education provided and goal status
•Develop ability to discuss clear explanations of:
Skilled therapy, Maintenance, Homebound status, Outcomes ….
14
Clinical Standards in Home Care
•Certified agencies follows Medicare Conditions of Participation scope of practice information [covered RN, OT, PT, ST, SW services]
•Agency leadership and Quality staff provide direction through:
Policies and Procedures
Operational processes or care pathways
•Clinicians should follow professional standards from their respective discipline as well as scope of practice from their state professional licensing division
Discussion: Therapy Standards
•Care standards in home care are not different from any other healthcare setting
The standards represent the clinical knowledge, skills, best practices and agency expected practices
•Evidence based practice such as Falls screening and interventions, Vital sign monitoring, Exercise and activity guidelines are available and easily used in the home care setting
•Modalities are rarely used by OT or PT in the home setting
Benefits of Rehab Services in Home Care
•Rehabilitation services are all about function
OT, PT and/or SLP assessment leads to an individualized treatment plan and interventions with an overall purpose of achieving maximal functional abilities
•Rehabilitation care at home usually involves family caregivers for support and/or to carry-out needed care
•HC patients receiving therapy have lower re-hospitalization rates and higher ratings on functional outcomes
15
Best Practice Recommendations: Home Care
•Complete assessment AND start treatment during 1st patient visit
•Know and Execute the plan of care – visit frequency and duration
•Establish reasonable timeframes for therapy care:
Prioritize treatments needed and provided
Identify achievable goals
•Seek continuous learning to ensure:
Knowledge of medical conditions and surgical procedures
Emergency parameters and actions associated with each finding
Understanding of “normal” aging processes – avoid ageism
•Sharpen your cultural competencies
Skills that increase your Success in Home Care
•Listening
•Observation
•Customer Service
•Motivational abilities
• Teaching
• Coaching
• Time Management
• Organization
Strategies for Effective Communication
LISTENING
Be fully present
StopLook
Listen
Be empathetic
Ask questions
PERCEIVING
Analyze your “own” perceptions
Observe carefully and attentively
Interpret consciously [stop bias]
Focus on others
16
Discussion: Setting Up Therapy Visit Frequency
• Create an appropriate visit frequency – Visits per week over the 60 day episode [9 weeks] is frequency; in
some cases, therapy added in midst of episode – then shorter timeframe
ALWAYS based on MD orders (therapist confirms plan with MD)
Usually, visits are highest in 1st weeks, then taper as established therapy home plan and patient improvement or stabilization occurs
Example – 3x week for 2 weeks, 2xweek for 1 week, 1x week x 1 week
Maintenance frequency may be weekly or monthly
Example – 1-2x month for 2 months
• Front loading therapy visits in initial 2 weeks has been shown to decrease re-hospitalization and increase outcomes in transitional care studies.
Establishing a Home Program (HEP)
•ALWAYS event – a Therapy Home program for exercise, activity or both
Considerations in creating the HEP:
Visual and learning needs [i.e. large font, illustrated, written vs. video…] Progression potential to be included in HEP
Safety
•Use Teach Back method - patient in their own words/actions can show their understanding and learning
Resourceshttp://www.teachbacktraining.org/ http://www.plainlanguage.gov/howto/guidelines/bigdoc/TOC.cfm
Clinical Skills and Competencies for Home Care
•Interpretation of assessment/observation findings
•Proficiency with Vital Signs – B/P, HR, RR, temperature
Pain and Gait Speed as 5th and 6th vital signs
•Appropriate use and selection of valid, reliable objective measures
Tests & Measures - reflect skill and patient needs from Visit 1 to discharge visit
•Ability to report and document concisely and comprehensively
•Prioritization/organization – i.e. visit schedule, treatments, follow-up done
17
Resources for Best Practice and Competencies
•Experienced team members at your agency
•Professional associations - AOTA, APTA, ASHA, VNAA, NAHC…
•National Clinical and Quality groups– AHRQ, CMS, NIH…
•Accreditation organizations – Joint Commission, CHAP….
•Disease specific organizations (i.e. MS, ALS, PD, AHA…)
Vital Signs Assessment – Temp, RR, HR, B/P
Best Practice for therapists – take temperature at start of visit and HR, RR, B/P at both rest and after maximal exertion –EVERY visit
Resources – links below and websites such as AHA, NIH…
http://www.heart.org/HEARTORG/Conditions/HighBloodPressure/AboutHighBloodPressure/Understanding-Blood-Pressure-Readings_UCM_301764_Article.jsp
https://meded.ucsd.edu/clinicalmed/vital.htm
Auscultation listening skills -heart, lung – see links at http://acousticheart.com/learning_heart_and_lung_sounds.html
Vital Signs in Home Care
Best Practice for therapists – take temperature at start of visit and HR, RR, B/P at both rest and after maximal exertion – EVERY visit
Many experts consider 2 additional “vital signs” to be essential data for assessing and providing intervention.
Pain – the presence of pain can be addressed by appropriate non-pharmacological interventions
Gait Speed – studies show that slow gait speed is correlated with increased falls with injuries and decreased self-care skills as well as related to cognitive decline and mortality
18
Pain Assessment
•Use a standardized pain assessment tool appropriate to the patient
•Standardized pain tools examples: Numerical scale
Visual analog scale (VAS)
Wong-Baker FACES
Pain AD (dementia)
Resource – on website - select Health Professionals, then Practice tools
http://www.partnersagainstpain.com/measuring-pain/assessment-tool.aspx
Gait Speed Assessment
•Gait speed can be measured in several methods such as 10ft or 30ft distance, or steps per minute
Resources:
5 meter test –
http://geriatrictoolkit.missouri.edu/gaitspeed/Gait-Speed.pdf
10 meter test -http://www.rehabmeasures.org/Lists/RehabMeasures/DispForm.aspx?ID=901
Steps per minute/older adult full text article -http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3169444/
Gait Speed Tidbits
•Normal adult stride length is 2-2.5 feet
•Men usually have a faster gait speed than women
•67 steps per minute is a measure of slow walking
•Studies show community access requires walking 200 - 600 meters
•Crossing a 2 lane street safely is estimated to need a walking speed of 1.1m/second [using 4 meters for each lane]; need to step up/down on a curb would add additional time.
19
Vital Signs – Practical Tips for Home Care
•Make sure your blood pressure equipment is in working order (calibrated)
•In your field bag-
Have a measuring tape/pre-measured cord to measure distance for gait speed
If not in electronic record, print Standardized Pain assessment tools such as Pain AD
Keep a roll of painter’s tape
•Take advantage of any skills labs at your HC agency so you can complete
competencies in collection of vital sign data
•Know your agency’s processes (policies, documentation standards) covering assessment and interpretation of vital signs, especially
the established parameters from MD of high and low points and when to contact
MD or initiate emergent care
Discussion - Competencies – Vital Signs
•Blood Pressure Precautions – do not take on painful, post-surgical or arm with IV
Remove clothing, position cuff correctly
•Respiratory Rate Observe respiration for 30 seconds; note any irregular
patterns
•Heart Rate Usually, radial pulse is measured [know alternate sites]
Note rhythm, pulse strength, any irregularity
•Temperature Usually, electronic thermometer used; follow directions (covers, timing)
•Pulse Oximetry – use depends on agency policy; may require MD order
Discussion - Competencies –Assessment
•Observation General Movement Posture Skin Environment
•Hands-on Assessment 6 Vital Signs OT or PT initial evaluation based
Strength, Range of Motion, Sensation, Goniometry, Cognition, Self-Care, Balance, Gait…
•Interview with patient and caregivers
20
Competencies – Objectively Measuring Function
•Use standardized assessment tools whenever possible – following the
instructions for use; examples – Katz Index of ADLs, Barthel ADL Index, Mini-Cog, Montreal Cognitive Assessment [MOCA]
•If not standardized, on team or agency level create a standard definition for
minimum, moderate, maximum that defines amount of patient participation
and therapist assistance.
•Once created, all therapists use
Resources
http://www.rehabmeasures.org/rehabweb/allmeasures.aspx?View=%7b0C859D90%2d7478%2d4C9B%2d9575%2d7
84C4A9A2D85%7d&PageView=Shared
http://geriatrictoolkit.missouri.edu/
http://www.mocatest.org/
Rehabilitation Therapy in Homecare Workflow
Evaluation and creation- intervention/Plan
(Strength, balance, ADL, breathing…)
Support Patient in self-care management
Education & training for Family/Caregivers
(Home program, coaching, repetition…)
Discharge Plan: Recommendations
(Self-care, assist from family, outpatient…)
Care Planning Determinations
•Is therapy care restorative or maintenance level?
•Is therapy care primarily addressing new, acute condition or chronic conditions?
Does the care plan need to address both acute and chronic needs?
•Will therapy care need to address aging/geriatric issues as well?
21
Enhanced Guidance - Skilled Care Documentation
“the Home Health clinical notes must document as appropriate
•History and physical exam pertinent to care (including response or changes to behavior from
previously provided skilled services)
•Skilled services provided on current visit
•Patient/caregiver immediate response to skilled services on current visit
•Plan for next visit based on rationale of prior results
•Detailed rationale explaining the need for skilled services in light of patient overall medical
condition and experiences
•Complexity of the service performed
•Any pertinent characteristics of the beneficiary or the home
Source CMS
CMS Guidance Documentation -continued
“Clinical notes should be written to adequately describe the reaction of a patient to skilled care. Clinical notes should also provide a clear picture if the treatment as well as next steps to be taken. Vague or subjective descriptions of the patient’s care should not be used. Examples of insufficient terminology to describe need for skilled care – “Patient tolerated treatment well”; “Continue with POC”; “Caregiver instructed in medication management”.
“Objective measurements of physical outcomes of treatment should be provided and clear descriptions of changed behaviors due to education programs provided should be recorded so all concerned can follow the results of the applied services.”
Factors Influencing Rehabilitation at Home
•Patient’s mental status, including cognition, motivation, and anxiety
•Caregiver’s abilities, including physical and emotional demands and time available to provide necessary care
•Overall prognosis and care needs
22
Home Care Skill Set –Assessment/Re-evaluation
•Pain
•Fatigue
•Diagnoses - Primary and comorbidities
•Precautions and/or restrictions
•Cognition
•Psychosocial Issues
Determine Ability to Participate
Documentation - Justifying Homebound Status
•Mobility Gait pattern [specify deficits]
Device needed, assist levels
Environmental – stairs, curbs…. Walk distance to leave home
•Function
Strength [especially in upright]
Balance [especially dynamic]
Environmental – doors, lighting… Fatigue-based – time rest periods..
• Transfers• Assist level – be specific
• Device needed
• Specific issues – bed, bathroom, car, wound sites…
• Safety – related areas include:• Falls risk -date of recent fall if applicable
• Cognitive issues – specify
• Judgement impairments - specify
Documentation – Supervision/Assist Needed
•Minimum, moderate, maximum = not helpful…. Need to document what each level means OR
Use standard scale in agency documentation
•Physical assistance
Need to specify task details
•Cues assistance
Verbal, tactile or both – specify tasks needed
•Standby/observation
Explain why needed
23
Tips for Home Visit Documentation
Every Visit Note should address:
•Current patient clinical status
•Treatment provided
•Patient response to treatment
•Patient need for continued services
•Progress towards Goals as well as interventions on each visit – Use the Plan of Care for therapy
•Document teaching – patient, family, caregivers
•Specify plan for next visit or next contact
•Evaluate progress objectively based on goals
Goal Oriented Charting Tips
•Patient focused
•Clear and concise
•Observable, specific and measurable
•Time Limited
•Realistic
•Recommendation: Capture Patient stated goal
Will help Therapist with goal agreement and validate expectations
Creating Measurable Goals …..
•Patient to improve ADL in 6 weeks.
OR
Patient to improve self care as measured by bathing in tub with standby assistance in 6 visits.
Patient to increase self-care dressing skills due to increased shoulder flexion to 90degrees or greater in 4 weeks
• Patient will walk with cane 100ft in 8 weeks.
OR
Patient to improve gait cycle in step length and walk 100ft with cane and verbal cues in 9 visits.
Patient to gain safe mobility with cane in community as measured by the 2 minute walk test in 5 weeks.
24
More Goal Examples
•Short term OT – Patient will perform upper extremity dressing in wheelchair
with clothing set-up and moderate assist in 3 visits.
PT - In 4 visits, patient will increase standing balance and strength as measured by single limb stance to 6 seconds.
•Long Term OT – Patient will demonstrate improvement in cognitive deficits
as measures by a Montreal Cognitive Assessment (MOCA) test score of 22/30 in 8 visits.
PT – In 9 visits, patient will show decreased falls risk as measured by Timed Up and Go (TUG) test score of 16 seconds or less.
Tips for Documenting During the Home Visit
The argument to document in real time as much as possible:
•Evidence shows that adult retention decreases quickly – Writing notes hours later, or days later means that details will be
forgotten
•Telling a patient what you are documenting – and why it is important – increases patient engagement and participation in the plan of care
Strategies:•Have note or electronic record open and ready for input•Use patient rest periods or independent activity time to enter info
•Take 3-5 minutes at end of visit to document key info from that visit
Patient Satisfaction is measured by - HHCAPS Consumer Assessment of Healthcare Providers & Systems
•DHHS Transparency Initiative
•Survey developed by Agency for Healthcare Research and Quality
•Consumer Assessment of Healthcare Providers & Systems Program (CAHPS) in multiple settings (hospital, home care, MD practice, etc)
• 34 questions (10 optional questions)
• For public reporting –composite measures
• Linked to Pay-for-Performance; penalty if not submitted
www.homehealthcahps.org
25
Sample HHCAHPS Items
•Did someone talk with you about how to set up your home so you can move around safely?
•Did home health providers seem informed and up-to-date about all the care or treatment you got at home?
•Did your providers talk with you about -
Pain?
Medication?
Patient Satisfaction in Practice -Examples
•Keeping Patient Informed After team meeting or case discussion with RN and/or MD, let the
patient know that you had a conversation and what was the outcome
Ask your patient if they have any feedback for you or the team
•Hand-on Care If an intervention may be uncomfortable, address that 1st and identify
what you will do to lessen discomfort or pain
Be sure to demonstrate respect and courtesy 100% of the time. Examples – draping, touching, ask may I?, check to see what patient would prefer…
•Planning Discuss discharge on Visit 1 and at least weekly; identify next steps in
advance
CMS STARS Ratings
•Agencies are ranked according to score on nine measures then scores are divided into ten categories.
Scores for each measure are adjusted using a statistical significance test and the national median for the specific measure.
Adjustments will be factored for patient mix, scores will then be rounded to the nearest 0.5 and placed in the associated cluster groups. The groups are assigned stars from one through five.
•Agency data is available on -
https://www.medicare.gov/homehealthcompare/search.html
26
Home Care Star ratings – measures used
•Process Measures – Timely Initiation of Care
Drug Education on all Medications
Influenza Immunization [current season]
•Patient Experience– Care Related Items
Communication between Provider and Patient
Overall Rating of Care Provided
• Outcomes Measures –• Improvement in
Ambulation
• Bed Transferring
• Bathing,
• Pain Interfering with Activity,
• Dyspnea
• Acute Care Hospitalization
Teamwork and Communication
•Care work is 1-on-1 with patient in home
•Team members connect/communicate by:
Periodic meetings (weekly, monthly, in home)
Phone calls – Text and Email if HIPAA secure
Electronic medical record if agency has this
Collaboration – proven to enhance outcomes
•Additional Communication also needed:
MD contacts and calls
Family contacts and calls
Community services & other referrals
Tips to Teamwork in the Home Care Setting
•Take time to MEET your team mates
•Learn everyone’s roles – so you can always answer questions like … what does the aide do? When is a social work referral needed?
•Find a mentor – huge plus to have someone helping us learn and grow
•Be prepared– be ready to summarize a case or a care issue concisely
Use SBAR - http://www.ihi.org/resources/pages/tools/sbartoolkit.aspx
•Identify when you need help – offer help to team mates
•Reap the benefit of experience – team members often know just the right equipment to order, how to handle an unmotivated patient and the best travel tips from roads to avoid, how to find parking, lowest cost for gas…
27
More Tips -Working in the home health setting
1. Wear comfortable clothing and secure footwear (cover your feet!)
2. Do not wear – jewelry, perfumes/colognes, smoke on your person
3. Take personal breaks – for hydration, nutrition, mental health
4. Schedule carefully – be prepared to handle downtime, delays…5. Pack your field bag or car trunk with key essentials
Healthy snacks, water, hand sanitizer, extra shirt/sweater/socks
6. Think like MacGyver! Carry painter’s tape, 10-25 foot measure, post-its, blanks sheets of paper… Be able to – measure distances & time, navigate to new geographical area
What to bring into the home on visits…
•Follow the bag policy/procedure for your Home Care agency
•Learn to be an EXPERT in infection control especially the basics Be prepared to clean equipment as well as hand wash
Community infections such as MRSA – will have agency policy/procedures
•Keep organized – paper/computer- treatment - hand washing items
•Most rehabilitation clinicians carry: Sphygmomanometer, stethoscope
Timer (watch, stop watch or phone app); Gait belt; goniometers
Resources to complete standardized tests/measures
Pain Scales, MOCA, Mini-mental, Barthel Index, Quick DASH, Clock draw, TUG…
Considerations for Home Safety
•Cognition
•Vision
•Medical Conditions
•Home Environment
•Community Access
•Support and Assist
•Education
•Equipment
28
Equipment (DME) Needs in the Home
•Be thoughtful! Most Insurances only cover ONE assistive device
•DME often has a co-pay requirement Try to be sure item is needed
•Home environment may dictate device
•Measure, especially items that need to be accurate Examples – walkers/doorways, tub seats/tub height, and more
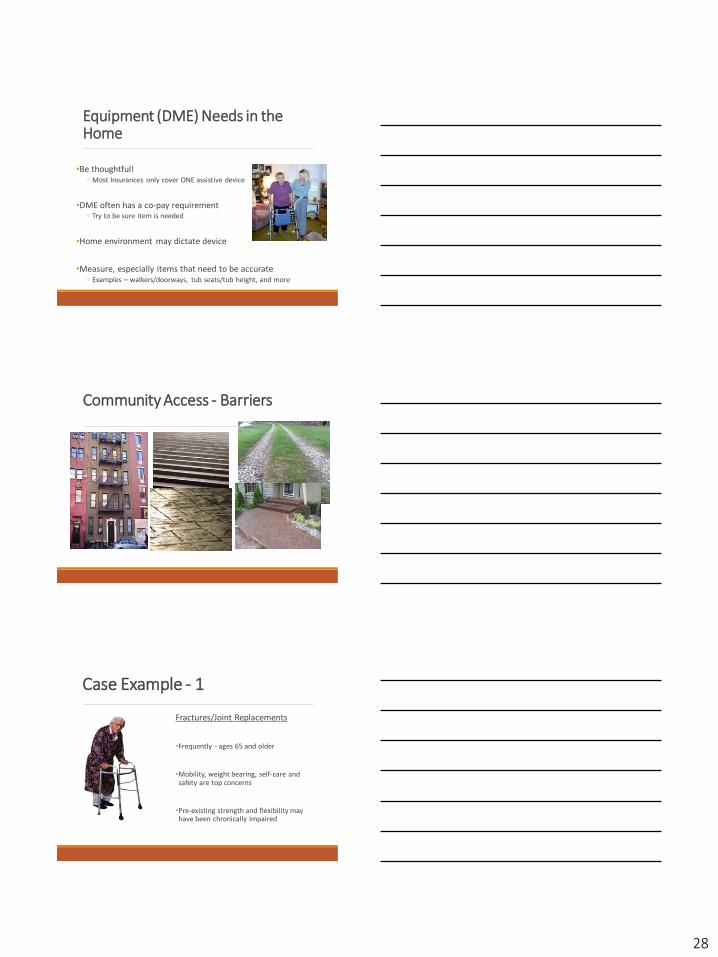
Community Access - Barriers
Case Example - 1
Fractures/Joint Replacements
•Frequently - ages 65 and older
•Mobility, weight bearing, self-care and safety are top concerns
•Pre-existing strength and flexibility may have been chronically impaired
29
Case Example - 2
Cardiopulmonary disease, i.e. HF, HTN,
COPD, post CABG
•Monitor Vital Signs and skilled observation
•Polypharmacy issues
•Environmental concerns
•Limited endurance, strength, flexibility issues
Case Example – 3
Geriatric and/or Chronic Comorbidities Concerns
•Posture
•Falls Risk
•Environmental safety
•Joint restrictions
•Adequate mobility & self-care
•Impact of Vision, Hearing
•Need for and/or use of assistive devices
Caregiver Burden
Mom is calling out and needs my help right now – the
babies are not fed yet….yikes!

30
Working in Home Care
PRO
•Individual sessions and creative care plans; true “1 on 1”
•Teamwork
•Involves families and caregivers
•“Real life” setting
CON
• Many work elements (visits, notes, phone calls, scheduling…)
• Treat/work alone
• Connecting with MD/team members
• Limited equipment/treatment areas
Home Care – Not for Everyone
Home Care – Expect the Unexpected!
31
Home Care is a Bridge to…
The Continuum of Health Care….
•Independence
•Outpatient Care
•Family Care
Thank You!
In addition to the links in the presentation, please see the reference list for this course for additional resources for working in the home health care setting…
As time permits on this webinar, Questions?
![Health Care Home Benchmarking Transcription · 2019. 1. 4. · Health Care Home Benchmarking – Transcription and PowerPoint Slides [Slide 1] Health Care Home Benchmarking Hello](https://img.pdfslide.us/doc/110x75/609e4a0651b2da0c18144707/health-care-home-benchmarking-transcription-2019-1-4-health-care-home-benchmarking.jpg)