Embed Size (px)
Citation preview
American Journal of Medical Genetics 53:46-51 (1994)
Holoprosencephaly Associated With Caudal Dysgenesis: A Clinical-Epidemiological Analysis
Maria Luisa Martinez-Frias, Eva Bermejo, Angel Garcia, Enrique Galan, and Luis Prieto ECEMC and Departamento de Farmacologia (M.L.M.-F.), ECEMC (E.B.), Departamento de Bioestadistica (L.P.), Facultad de Medicina, Universidad Complutense, Madrid, Servicio de Pediatria, Hospital General de la Seguridad Social de Guadalajara, Guadalajara (A.G.), and Servicio de Pediatria Badajoz, Hospital Materno-Infantil de Badajoz, Badajoz (E.G.), Spain
We have studied 9 cases with the combina- tion of some form of holoprosencephaly and any degree of caudal dysgenesis. The cases were identified through the Spanish Collab- orative Study of Congenital Malformations (ECEMC). Of the 9 cases, 6 infants had an aneuploidy syndrome, one had Meckel syn- drome, and 2 cases were of unknown etiol- ogy. We determined that the prevalence fig- ure for the association of both conditions in the same child was 0.08 per 10,000 livebirths, and 18.8 times higher for stillbirths (i.e., 1.50/10,000). This prevalence is significantly higher than what would be expected by chance. @ 1994 Wiley-Liss, Inc.
KEY WORDS: holoprosencephaly, cyclopia, caudal regression, caudal dysgenesis, midline blasto- genesis defects, clinical epi- demiology
INTRODUCTION Welch and Aterman [1984], in a review of the clinical
and etiological aspects of caudal dysgenesis, cited the sibship described by Rochet et al. [19661 and the family reported by Say and Coldwell [19751. These authors’ ar- ticles presented several relatives within the same fam- ily with some combination of cyclopia or cebocephaly with partial agenesis of the sacrum and coccygeal bones.
Although the combination of holoprosencephaly and caudal dysgenesis is common in the trisomy 13 syn- drome and other aneuploidy syndromes [Cohen, 19891, as far as we know there are no epidemiologic studies
Received for publication December 29, 1993; revision received May 23,1994.
Address reprint requests to Dr. M.L. Martinez-Frias, ECEMC, Facultad de Medicina, Universidad Complutense, 28040 Madrid, Spain.
0 1994 Wiley-Liss, Inc.
which document this association in any set of mal- formed babies.
Here we perform a clinical-epidemiological analysis of all of the cases with a combination of some form of holoprosencephaly with any degree of caudal dysgen- esis that have been identified among the 1,008,971 live- births and 6,687 stillbirths studied in the Spanish Col- laborative Study of Congenital Malformations (ECEMC).
MATERIAL AND METHODS The ECEMC is a hospital-based, case-control study
and surveillance system that began in April 1976, in- cluding only livebirths; stillbirths were included as of January 1980. All children born in hospitals from all over Spain are examined by physicians who, being in- terested in the problem of congenital anomalies, collab- orate with the ECEMC program and accept its uniform strict methodology. They examine the children during the first 3 days of life to identify major and minor de- fects. For each case, the next non-malformed baby of the same sex born in the same hospital is selected as a control subject. The collaborating physicians collect in- formation on approximately 250 data points on each child (whether case or control) and their mothers, using protocols specifically designed for this purpose. For ex- ample, there is a specific question about maternal dia- betes and an open-ended question on acute maternal diseases (including gestational diabetes) during preg- nancy. In many instances, karyotypes, photographs, imaging and laboratory studies, and necropsy reports are included in the records. All the collected informa- tion is sent on a monthly basis to the coordinating group of the ECEMC, which is located in Madrid. This group, which is constituted by experts in clinical genet- ics, dysmorphology, epidemiology, and statistics, per- form the clinical analysis of all the malformed infants, codify their congenital defects, and establish the differ- ent clinical group codes. Detailed descriptions of the ECEMC methodology have been published elsewhere [Martinez-Frias et al., 1990, 19911. The congenital anomaly coding system developed by the ECEMC has great flexibility and specificity for the retrieval and analysis of children with different types of multiple

Holoprosencephaly and Caudal Dysgenesis 47
found in 0.08, 1.50, and 0.09 per 10,000 liveborn, still- born, and total-born children, respectively. Table I also shows that the observed prevalence of this combination is significantly higher than what we would expect just by chance in all the groups (P < 0.0000, P = 0.0002, P < 0.0000, respectively). Furthermore, excluding those cases of known cause, we observed 2 of unknown cause with the combination of holoprosencephaly and caudal dysgenesis among the liveborn children (Table I), for a prevalence of 0.02 per 10,000 livebirths. The expected prevalence of the combination, multiplying the individual prevalences of holoprosencephaly and cau- dal dysgenesis, was 0.0001 per 10,000 liveborn infants. Thus, the observed figure (Table I) is 200 times higher than the expected one; this difference is statistically sig- nificant (Z = 19.9; P < 0.0000). Performing a more re- strictive estimation of the expected prevalence of the combination, multiplying the individual prevalences of holoprosencephaly and caudal dysgenesis of unknown cause (48 and 133 cases, for prevalence figures of 0.48 and 1.32 per 10,000 liveborn infants, respectively), the expected value is then 0.00006 per 10,000 livebirths, which is 333 times lower than the observed prevalence (Z = 25.7; P < 0.0000). In order to avoid the non-specific tendency for defects to cluster each other, we also used the method proposed by Khoury et al. [1990]. The re- sults are also statistically significant (P < 0.01); being the observed number was 7.96 times higher than the expected number. We excluded the syndromes from the analysis.
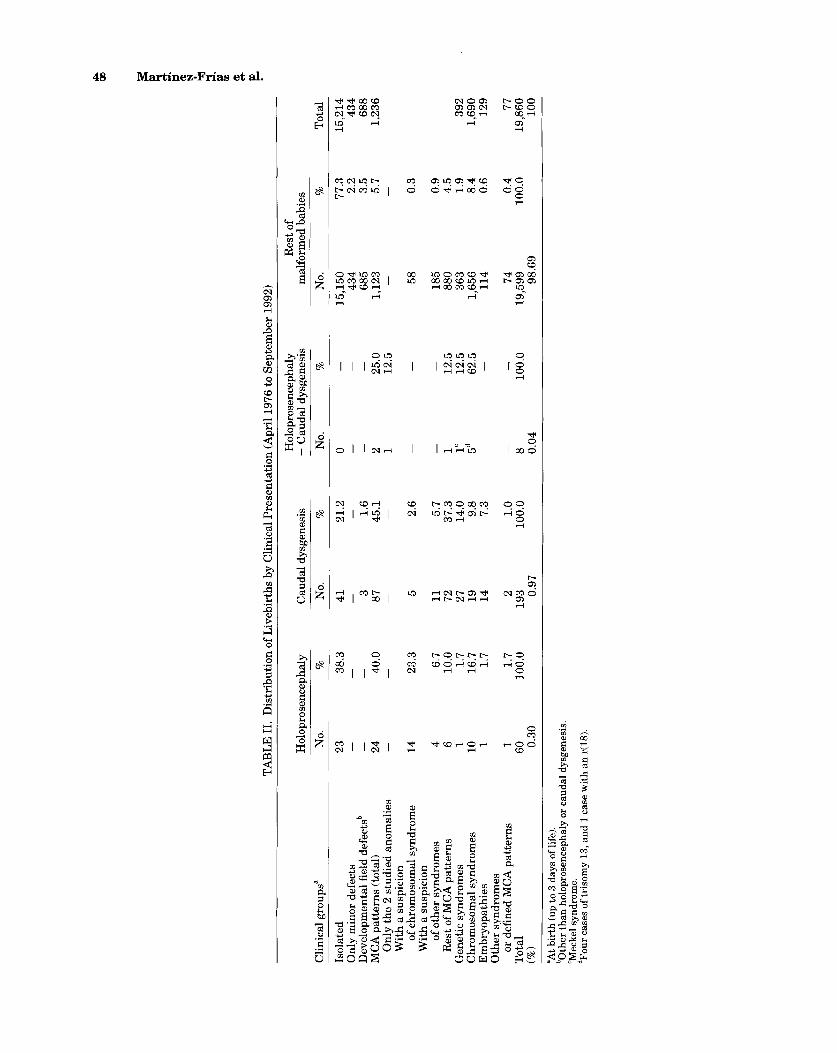
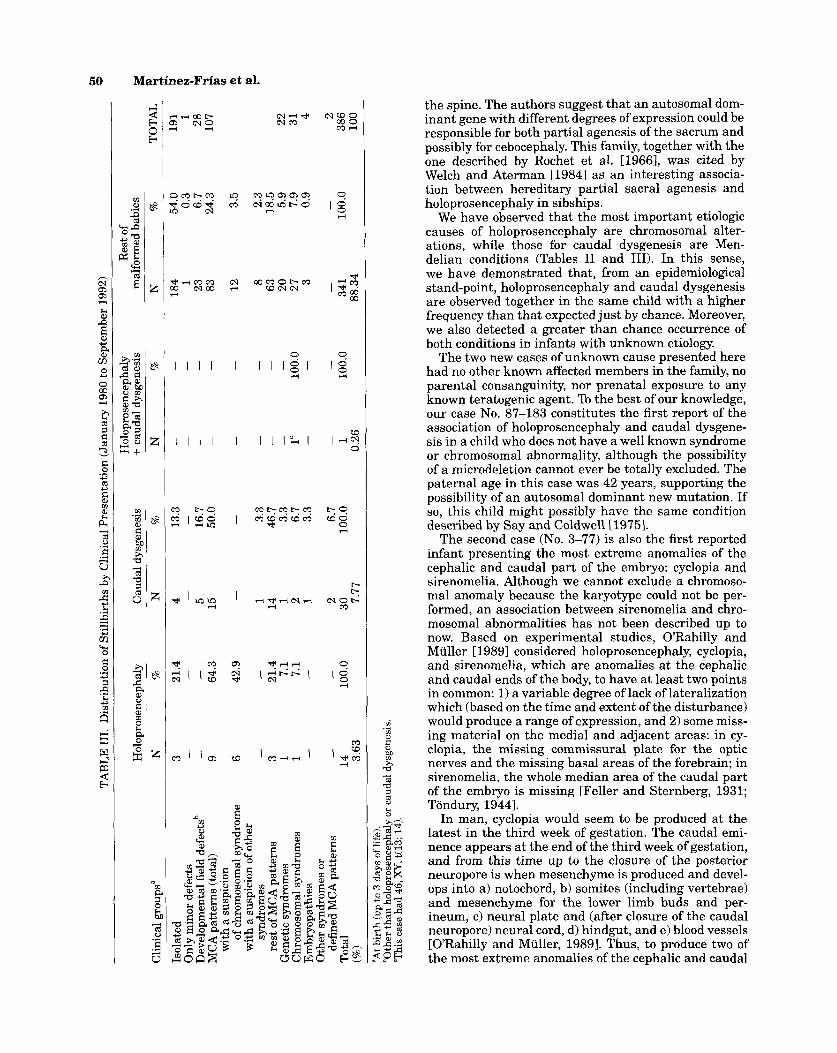
Table I1 shows the distribution of the 19,860 liveborn malformed children in the ECEMC register by clinical presentation into 4 groups: those who have only holo- prosencephaly with or without other congenital anom- alies excluding caudal dysgenesis, those with caudal dysgenesis with or without other congenital defects ex- cluding holoprosencephaly, the children who had both anomalies, and the children without any detected de- gree of holoprosencephaly o r caudal dysgenesis. Among the infants with an MCA pattern, we separate as sub- groups those cases whose clinical patterns were com- patible with a particular syndrome (whether chromoso- mal or monogenic) that we could not confirm because of
congenital anomalies (MCA) patterns through its two levels and different sublevels [Martinez-Frias, 1994a; Martinez-Frias and Urioste, 19941. Using this method- ology, we searched our data files for cases with any of the codes for holoprosencephaly and/or caudal dysgen- esis. For the purposes of this paper, not only the clini- cally confirmed cases of holoprosencephaly but also those patients whose phenotype strongly suggests the diagnosis have been included as holoprosencephalic. Children with an MCA pattern that affected the caudal eminence, such as those combining urinary, genital, and/or anal anomalies, and/or those with lumbosacral spine defects (including the most severe anomalies of the caudal region such as sirenomelia), were considered to have caudal dysgenesis. Some cases which lack the necropsy or radiological confirmation of the diagnosis have been included because, even if a classification bias existed, it would be the same for all the groups of cases that are considered in the study, and so would not affect the statistical reliability of the results.
RESULTS From April 1976 to September 1992 (Table I), the
ECEMC surveyed a total of 1,008,971 liveborn infants and identified 19,860 (1.97%) malformed babies. Among a total of 6,687 stillbirths from January 1980 to September 1992,386 (5.77%) were identified as having congenital anomalies.
Table I specifies the prevalence figures for holopros- encephaly, which are 0.59,20.94, and 0.75, respectively, per 10,000 livebirths, stillbirths, and total births (in- cluding livebirths and stillbirths, from January 1980 to September 1992). The figures for caudal dysgenesis are 1.91, 44.86, and 2.43 per 10,000, respectively. These prevalence figures are similar to the ones we gave in previous papers for holoprosencephaly [Urioste et al., 19881 and for caudal dysgenesis [Martinez-Frias and Gomar Morillo, 19941.
A computerized search of the 19,860 liveborn mal- formed infants identified 8 who had some degree of both holoprosencephaly and caudal dysgenesis, and one case from the 386 malformed stillbirths (Table I). Thus, the combination of these anomalies in the same child was
TABLE I. Prevalence Figures in the ECEMC*
Births
Pattern of anomalies
Livebirths Stillbirths Totalb No. Per 10,000 No. Per 10,000 No. Per 10,000
Holoprosencephaly (any degree) 60 0.59 14 20.94 65 0.75 Caudal dysgenesis (any degree) 193 1.91 30 44.86 212 2.43 Caudal dysgenesis + Holoprosencephaly” 8 0.08 1 1.50 8 0.09 - With known cause 6 0.06 1 1.50 7 0.08 - Unknown cause 2‘ 0.02 0 0 1 0.01 Total births 1,008,971 - 6,687 - 871,679 - Malformed infants 19,860 196.83 386 577.24 17,889 205.22
*Livebirths from April 1976 to September 1992; stillbirths from January 1980. “Observed’expected = Livebirths:8/0.01 = 800, Z = 79.9, P < 0.0000. Stillbirths: 1/0.06 = 16.7, Z = 3.8, P = 0.0002. Total: 8/0.02 = 400, Z = 56.4, P < 0.0000. bFigures on total births correspond to the period January 1980 to September 1992. W e have 2 “observed” cases versus an “expected” value of 0.01 cases (Z = 19.9; P < 0.0000).
TAB
LE 1
1. D
istr
ibut
ion
of L
iveb
irth
s by
Clin
ical
Pre
sent
atio
n (A
pril
1976
to S
epte
mbe
r 199
2)
Hol
opro
senc
epha
ly
Res
t of
Hol
opro
senc
epha
ly
Cau
dal d
ysge
nesi
s +
Cau
dal d
ysge
nesi
s m
alfo
rmed
bab
ies
No.
%
N
o.
%
No.
%
N
o.
%
Clin
ical
gro
ups"
Isol
ated
O
nly
min
or d
efec
ts
Dev
elop
men
tal
fiel
d de
fect
sb
MC
A p
atte
rns
(tot
al)
Onl
y th
e 2
stud
ied
anom
alie
s W
ith a
sus
pici
on
of c
hrom
osom
al s
yndr
ome
With
a s
uspi
cion
of
oth
er s
yndr
omes
R
est o
f MC
A p
atte
rns
Gen
etic
syn
drom
es
Chr
omos
omal
syn
drom
es
Em
bryo
path
ies
Oth
er s
yndr
omes
Tot
al
(%I or
def
ined
MC
A p
atte
rns
Tot
al
15,2
14
434
688
1,23
6
38.3
-
- 40.0
-
41
3 87
-
-
21.2
1.6
45.1
-
0 15
,150
43
4 68
5 1,
123
77.3
2.
2 3.
5 5.
7 -
2 1
-
25.0
12
.5
14
23.3
6.7
10.0
1.
7 16
.7
1.7
1.7
100.
0
2.6
5.7
37.3
14
.0
9.8
7.3
1.0
100.
0
58
0.3
5 11
72
27
19
14
2 19
3 0.97
4 6 1
10 1
1
60 0.30
185
880
363
1,65
6 11
4 74
19,5
99
98.6
9
0.9
4.5
1.9
8.4
0.6
0.4
100.
0
-
12.5
12
.5
62.5
1
1"
5d
392
1,69
0 12
9 77
19,8
60
100
-
8 0.04
-
100.
0
"At b
irth
(up
to 3
day
s of
life
).
'Mec
kel
synd
rom
e.
dFou
r cas
es o
f tri
som
y 13
, and
1 c
ase
wit
h an
r(18
).
than
hol
opro
senc
epha
ly o
r cau
dal d
ysge
nesi
s.
Holoprosencephaly and Caudal Dysgenesis 49
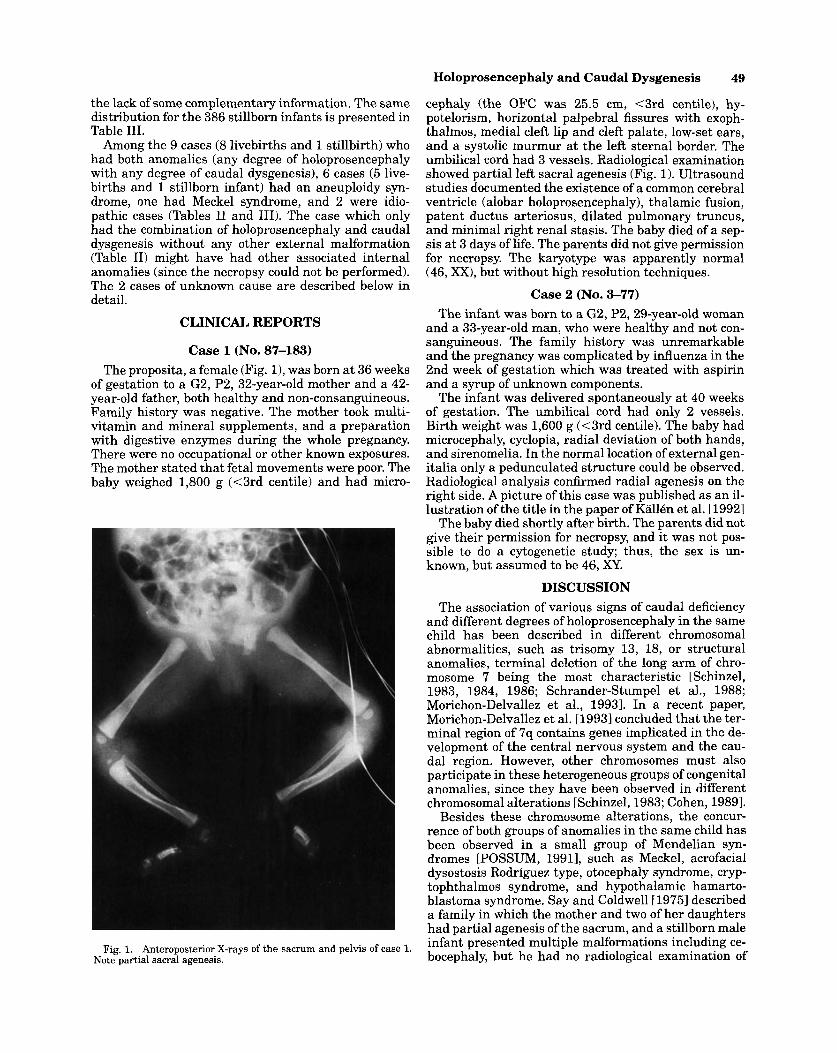
cephaly (the OFC was 25.5 cm, <3rd centile), hy- potelorism, horizontal palpebral fissures with exoph- thalmos, medial cleft lip and cleft palate, low-set ears, and a systolic murmur at the left sternal border. The umbilical cord had 3 vessels. Radiological examination showed partial left sacral agenesis (Fig. 1). Ultrasound studies documented the existence of a common cerebral ventricle (alobar holoprosencephaly), thalamic fusion, patent ductus arteriosus, dilated pulmonary truncus, and minimal right renal stasis. The baby died of a sep- sis at 3 days of life. The parents did not give permission for necropsy. The karyotype was apparently normal (46, XX), but without high resolution techniques.
Case 2 (No. 3-77) The infant was born to a G2, P2,29-year-o1d woman
and a 33-year-old man, who were healthy and not con- sanguineous. The family history was unremarkable and the pregnancy was complicated by influenza in the 2nd week of gestation which was treated with aspirin and a syrup of unknown components.
The infant was delivered spontaneously at 40 weeks of gestation. The umbilical cord had only 2 vessels. Birth weight was 1,600 g (<3rd centile). The baby had microcephaly, cyclopia, radial deviation of both hands, and sirenomelia. In the normal location of external gen- italia only a pedunculated structure could be observed. Radiological analysis confirmed radial agenesis on the right side. A picture of this case was published as an il- lustration of the title in the paper of Kallen et al. [19921
The baby died shortly after birth. The parents did not give their permission for necropsy, and it was not pos- sible to do a cytogenetic study; thus, the sex is un- known, but assumed t o be 46, XY.
DISCUSSION The association of various signs of caudal deficiency
and different degrees of holoprosencephaly in the same child has been described in different chromosomal abnormalities, such as trisomy 13, 18, or structural anomalies, terminal deletion of the long arm of chro- mosome 7 being the most characteristic [Schinzel, 1983, 1984, 1986; Schrander-Stumpel et al., 1988; Morichon-Delvallez et al., 19931. In a recent paper, Morichon-Delvallez et al. [1993] concluded that the ter- minal region of 7q contains genes implicated in the de- velopment of the central nervous system and the cau- dal region. However, other chromosomes must also participate in these heterogeneous groups of congenital anomalies, since they have been observed in different chromosomal alterations [Schinzel, 1983; Cohen, 19891.
Besides these chromosome alterations, the concur- rence of both groups of anomalies in the same child has been observed in a small group of Mendelian syn- dromes [POSSUM, 19911, such as Meckel, acrofacial dysostosis Rodriguez type, otocephaly syndrome, cryp- tophthalmos syndrome, and hypothalamic hamarto- blastoma syndrome. Say and Coldwell [1975] described a family in which the mother and two of her daughters had partial agenesis of the sacrum, and a stillborn male infant presented multiple malformations including ce- bocephaly, but he had no radiological examination of
the lack of some complementary information. The same distribution for the 386 stillborn infants is presented in Table 111.
Among the 9 cases (8 livebirths and 1 stillbirth) who had both anomalies (any degree of holoprosencephaly with any degree of caudal dysgenesis), 6 cases (5 live- births and 1 stillborn infant) had an aneuploidy syn- drome, one had Meckel syndrome, and 2 were idio- pathic cases (Tables I1 and 111). The case which only had the combination of holoprosencephaly and caudal dysgenesis without any other external malformation (Table 11) might have had other associated internal anomalies (since the necropsy could not be performed). The 2 cases of unknown cause are described below in detail.
CLINICAL REPORTS
Case 1 (No. 87-183) The proposita, a female (Fig. 11, was born at 36 weeks
of gestation to a G2, P2, 32-year-old mother and a 42- year-old father, both healthy and non-consanguineous. Family history was negative. The mother took multi- vitamin and mineral supplements, and a preparation with digestive enzymes during the whole pregnancy. There were no occupational or other known exposures. The mother stated that fetal movements were poor. The baby weighed 1,800 g (<3rd centile) and had micro-
Fig. 1. Anteroposterior X-rays of the sacrum and pelvis of case 1. Note partial sacral agenesis.
Martinez-Frias e t al.
9 I I I I I l l l g l
I l l I I I I ' r l I
the spine. The authors suggest that an autosomal dom- inant gene with different degrees of expression could be responsible for both partial agenesis of the sacrum and possibly for cebocephaly. This family, together with the one described by Rochet et al. [1966], was cited by Welch and Aterman [1984] as an interesting associa- tion between hereditary partial sacral agenesis and holoprosencephaly in sibships.
We have observed that the most important etiologic causes of holoprosencephaly are chromosomal alter- ations, while those for caudal dysgenesis are Men- delian conditions (Tables I1 and 111). In this sense, we have demonstrated that, from an epidemiological stand-point, holoprosencephaly and caudal dysgenesis are observed together in the same child with a higher frequency than that expected just by chance. Moreover, we also detected a greater than chance occurrence of both conditions in infants with unknown etiology.
The two new cases of unknown cause presented here had no other known affected members in the family, no parental consanguinity, nor prenatal exposure to any known teratogenic agent. To the best of our knowledge, our case No. 87-183 constitutes the first report of the association of holoprosencephaly and caudal dysgene- sis in a child who does not have a well known syndrome or chromosomal abnormality, although the possibility of a microdeletion cannot ever be totally excluded. The paternal age in this case was 42 years, supporting the possibility of an autosomal dominant new mutation. If so, this child might possibly have the same condition described by Say and Coldwell [1975].
The second case (No. 3-77) is also the first reported infant presenting the most extreme anomalies of the cephalic and caudal part of the embryo: cyclopia and sirenomelia. Although we cannot exclude a chromoso- mal anomaly because the karyotype could not be per- formed, an association between sirenomelia and chro- mosomal abnormalities has not been described up to now. Based on experimental studies, O'Rahilly and Muller [1989] considered holoprosencephaly, cyclopia, and sirenomelia, which are anomalies a t the cephalic and caudal ends of the body, to have at least two points in common: 1) a variable degree of lack of lateralization which (based on the time and extent of the disturbance) would produce a range of expression, and 2) some miss- ing material on the medial and adjacent areas: in cy- clopia, the missing commissural plate for the optic nerves and the missing basal areas of the forebrain; in sirenomelia, the whole median area of the caudal part of the embryo is missing [Feller and Sternberg, 1931; Tondury, 19441.
In man, cyclopia would seem to be produced at the latest in the third week of gestation. The caudal emi- nence appears at the end of the third week of gestation, and from this time up to the closure of the posterior neuropore is when mesenchyme is produced and devel- ops into a) notochord, b) somites (including vertebrae) and mesenchyme for the lower limb buds and per- ineum, c) neural plate and (after closure of the caudal neuropore) neural cord, d) hindgut, and e) blood vessels [O'Rahilly and Muller, 19891. Thus, to produce two of the most extreme anomalies of the cephalic and caudal

Holoprosencephaly and Caudal Dysgenesis 51
Kallen B, Castilla EE, Lancaster PAL, Mutchinick 0, Knudsen LB, Martinez-Frias ML, Mastroiacovo P, Robert E (1992): The cyclops and the mermaid: An epidemiological study of two types of rare malformation. J Med Genet 29:30-35.
Khoury MJ, James LM, Erickson J D (1990): On the measurement and interpretation of birth defect associations in epidemiologic studies. Am J Med Genet 37:229-236
KucQra J (1971): Rate and type of congenital anomalies among off- spring of diabetic mothers. J Reprod Med 7:61-70.
Martinez-Frias ML (1994a): Developmental field defects and associa- tions: Epidemiological evidence of their relationship. Am J Med Genet 49:45-51.
Martinez-Frias ML (1994b): Epidemiological analysis of mater- nal diabetes and outcome of pregnancies: Frequency and speci- ficity of different congenital anomalies. Am J Med Genet 51:108- 113.
Martinez-Frias ML, Frias JL, Salvador J (1990): Clinicallepidemio- logical analysis of malformations. Am J Med Genet 35121-125.
Martinez-Frias ML, Frias JL, Rodriguez-Pinilla E, Urioste M, Bermejo E, Cereijo A, Gaya F (1991): Value of clinical analysis in epidemiological research: The Spanish registry experience. Am J Med Genet 41:192-195.
Martinez-Frias ML, Gomar Morillo JL (1994): New case of axial meso- dermal dysplasia sequence: Epidemiologic evidence of a single en- tity. Am J Med Genet 49:74-76.
Martinez-Frias ML, Urioste M (1994): Segmentation anomalies of the vertebras and ribs: A developmental field defect. Epidemiologic ev- idence. Am J Med Genet 49:36-44.
Mills JL (1982): Malformations in infants of diabetic mothers. Tera- tology 25385-394.
Morichon-Delvallez N, Delezoide AL, Vekemans M (1993): Holopros- encephaly and sacral agenesis in a fetus with a terminal deletion 7q36-17qter. J Med Genet 30521-524.
Opitz JM (1993): Blastogenesis and the “primary field” in human de- velopment. In Opitz JM (ed): “Blastogenesis, Normal and Abnor- mal.” New York Wiley-Liss for the National Foundation-March of Dimes. BD:OAS 29 (1):3-37.
O’Rahilly R, Muller F (1989): Interpretation of some median anom- alies as illustrated by cyclopia and symmelia. Teratology 40:409- 421.
POSSUM (1991): “Pictures of Standard Syndromes and Undiag- nosed Malformations.” Version 3.0., 4th ed. Melbourne: Computer Power Group and The Murdoch Institute for Research into Birth Defects.
Rochet E, Gacon G, Robert JM, Grunthaler CH (1966): Dystocie os- seuse par agenesie sacrococcygienne. Observation familiale avec polylethalite dorigine malformative associee. Gynecol Obstet (Paris) 65115-124 (Cited by Welch and Aterman, 1984).
Say B, Coldwell J G (1975): Hereditary defect of the sacrum. Human- genetik 27:231-234.
Schinzel A (1983): “Catalogue of unbalanced chromosome aberrations in Man.” Berlin: de Gruyter.
Schinzel A (1984): Cyclopia and cebocephaly in two newborn infants with unbalanced segregation of a familial translocation t rcp (1;7) (q32;q34). Am J Med Genet 18:153-161.
Schinzel A (1986): A further case of cyclopia due to unbalanced segre- gation of a previously reported rcp (1;7) (q32;q34) familial translo- cation. Am J Med Genet 24:205-206.
Schrander-Stumpel C, Schrander J, Fryns JP, Hamers G (1988): Cau- dal deficiency sequence in 7q terminal deletion. Am J Med Genet
Tondury G (1944): Zur Kenntnis der Fehlbindungen mit Defekten des hinteren Korperendes. Arch J Klaus-Stiftung 19:225-264 (Cited by ORahilly and Miiller 1989).
Urioste M, Valcarcel E, Gdmez MA, Pine1 I, Garcia de Leon R, Diaz de Bustamante A, Tebar R, Martinez-Frias ML (1988): Holo- prosencephaly and trisomy 21 in a child born t o a nondiabetic mother. Am J Med Genet 30:925-928.
Welch JP, Aterman K (1984): The syndrome of caudal dysgenesis: A review, including etiologic considerations and evidence of het- erogeneity. Pediatr Pathol 2:313-327.
30757-761.
part of the midline (cyclopia and sirenomelia) in the same child, a cause must act in the third week of ges- tation at the latest. Consequently, both are severe de- fects of early blastogenesis (primary developmental field) and, thus, their concurrence should be considered as a sporadic association or due to a chromosomal al- teration [Opitz, 19931.
Several agents should interact with these two processes, and differences in their timing and intensity would explain the variability in the expression of these conditions. However, other factors must also be in- volved because the observation of both types of defects in the same child a t birth is very uncommon. We have estimated its frequency at about 7.9 per million live- births and 18.8 times higher than this in stillbirths. These prevalences should be considered minimal esti- mations, since there may be cases with less severe forms of holoprosencephaly and sacral agenesis who died without having X-ray and necropsy examinations and could not be counted. Moreover, the concurrence of the two conditions in the same child is extremely rare in those cases who were exposed to maternal diabetes mellitus, which has been demonstrated to be strongly associated to caudal dysgenesis and also, although to a lesser degree, to holoprosencephaly [Kucgra, 1971; Mills, 1982; Martinez-Frias, 1994131.
Both types of malformations of the cephalic and cau- dal part of the embryo are gross alterations of early blastogenesis, particularly those cases with both types of anomalies. Consequently, as Opitz [19931 pointed out, they are highly lethal and can produce early abor- tions. This may explain the low frequency of the con- currence in the same child of both anomalies a t birth, and also the fact that, in most cases in which the etio- logic factors are known, these are pre-zygotic (Le., chro- mosomal and genic syndromes). The early stage of de- velopment during which they are produced (when many women usually still do not know that they are preg- nant) makes it difficult to identify other causal agents.
It is very interesting the high frequency in which the combination of both defects is observed in syndromal cases (about 87.5% of the children). This makes it diffi- cult to know, for a given apparently sporadic case (even with normal chromosomes), whether this is a syndro- ma1 or an association with negligible recurrence risk [Opitz, 19931.
ACKNOWLEDGMENTS This work was supported in part by a Grant from the
Direccion General de Salud Publica del Ministerio de Sanidad y Consumo of Spain, and in part by Fundacidn ONCE.
We also gratefully acknowledge all the ECEMC col- laborators who collected the information, and C.F. War- ren for her linguistic assistance.
REFERENCES Cohen MM (1989): Perspectives on holoprosencephaly: Part I. epi-
demiology, genetics, and syndromology. Teratology 40:211-235. Feller A, Sternberg H (1931): Zur Kenntnis der Fehlbindungen der
Wirbelsaule. 111. Virchows Arch [A] 280549-692 (Cited by ORahilly and Muller, 1989).