Embed Size (px)
Citation preview

2400
Hodgkin’s Disease Associated with Human Immunodeficiency Virus Infection A Clinical Study of 46 Cases
Rafael Rubio, M.D., Ph.D., for the Cooperative Study Group of Malignancies Associated with HIV Infection of Madrid
Background. Hodgkin’s disease is not an acquired immunodeficiency syndrome (AIDS)-defining illness. However, Hodgkin’s disease associated with human im- munodeficiency virus (HIV) infection has a different nat- ural history and therapeutic outcome than in the general population of Hodgkin’s disease patients.
Methods. The authors studied the epidemiologic and clinicopathologic features and therapeutic outcomes of 46 patients with Hodgkin’s disease associated with HIV infection collected from a cooperative study of nine hos- pitals in Madrid, Spain.
Results. Forty-three (93.5%) of the subjects were men and three (6.5%) were women, with a mean age of 26.9 years. Thirty-nine (84.8%) were intravenous drug users and four (8.7%) were homosexuals. In 43 patients (93.5%), Hodgkin’s disease was the first manifestation of HIV in- fection. In 16 patients (34.8%), AIDS developed after the diagnosis of Hodgkin’s disease. Histologic subtypes were mixed cellularity (41.3%), lymphoid depletion (21.7%), nodular sclerosis (21.7%), and lymphocytic predomi- nance (4.3%). At diagnosis, 89.1% had advanced stages (III,IV), 82.6% had B symptoms, and 41.3% had bone mar-
From the Unidad lnfeccion HIV, Hospital ”12 de Octubre,” Ma- drid, Spain.
The following persons and institutions were participants in this study by the Cooperative Study Group of Malignancies Associated to HIV Infection of Madrid (Spain). Hospital ”12 de Octubre”: R. Rubio, 1. R. Costa, J . 1. Mayordomo, F. Pulido, J . J. Lahuerta, A. del Palacio; Hospital “Gregorio Maraiibn”: E. Flores, Y. Escobar; Hospital “Ra- m6n y Cajal”: M. Serrano, L. Buz6n. C. Bellas; Clinica ”Puerto de Hierro”: M. Yebra, P. Espafia; Hospital “Clhico San Carlos”: J. Diaz- Mediavilla, R. Martinez; Hospital “La Paz“: V. Pintado y A. Gil; Hos- pital “Prhcipe de Asturias” de Alcali de Henares: P. Ricard; Hospital de la Princesa: J. Verdejo; Hospital de M6stoles: C. Barros; Servicio de Epidemiologa de la Comunidad Aut6noma de Madrid: J. C. Alberdi y D. Lopez-Gay.
Address for reprints: Rafael Rubio, M.D., Ph.D., Unidad Infec- cion HIV, Hospital “12 de Octubre,” 28041-Madrid, Spain.
Accepted for publication November 29, 1993.
row involvement. Of 27 evaluable patients treated with chemotherapy, 44.4% had a complete response (16.7% re- lapsed) and 37% had a partial response. Median survival was 15 months (range, 1-44 months). Projected %year survival rate was 19%, and projected event-free survival rate was 22% at 30 months. Adverse prognostic factors for survival in univariate analysis were B symptoms, no response to chemotherapy, hemoglobin level less than 11 g/dl, leukocyte count less than 4500/mm3, total lympho- cyte count less than 1000/mm3, CD4 lymphocyte count less than 200/mm3, and alkaline phosphatase level greater than 300 IU/l.
Conclusions. Hodgkin’s disease associated with HIV infection is more frequent among intravenous drug ad- dicts, and the clinical course is different in these patients from that in the general population of Hodgkin’s disease patients, showing high frequency of advanced stages, un- favorable histologic subtypes, poor therapeutic response, and short survival time. Cancer 1994: 73:2400-7.
Key words: Hodgkin’s disease, non-Hodgkin’s lympho- mas, malignant lymphomas, human immunodeficiency virus infection, acquired immunodeficiency syndrome, CD4 lymphocytes.
Acquired immunodeficiency syndrome (AIDS) was first described in 1981 in the United States as a combined epidemic of Pneumocystis carinii pneumonia and Kaposi’s sarcoma.’ Subsequently, other disorders were accepted as criteria of AIDS, including primary lym- phoma of the central nervous system’ and high- and intermediate-grade non-Hodgkin’s lymphomas with B phenotype.3z4 In the last few years, small series of pa- tients with Hodgkin’s disease associated with human immunodeficiency virus (HIV) infection have been re- p ~ r t e d . ~ - ~ ~ However, Hodgkin’s disease is not consid- ered to be a diagnostic criteria of AIDS,4 although some authors have proposed that it should be in~luded.’,’~

Hodgkin’s Disease and HIV Infection/Rubio 2401
The purpose of our report was to study the epide- miologic and clinical features of Hodgkin’s disease as- sociated with HIV infection, response to therapy, and prognostic factors for survival in this setting.
Patients and Methods
Forty-six patients with Hodgkin‘s disease associated with HIV infection diagnosed in nine hospitals of the Autonomic Community of Madrid (Spain) from Janu- ary 1984 to January 1991 were studied retrospectively. Clinical and pathologic features of each patient were recorded by reviewing clinical charts and pathologic re- ports.
The Rye modification of the Lukes and Butler histo- pathologic classification was ~ s e d . ~ ~ , ~ ’ Each individual pathologist at each individual hospital reviewed his or her own material. For clinical staging, the Ann Arbor System49 was used. Staging procedures included clinical examination, thoracic and abdominal computed tomog- raphy scan, bone marrow biopsy, and renal and liver chemistries. In all cases, positive anti-HIV serology (en- zyme-linked immunosorbent assay plus Western blot) was required. Patients were considered evaluable for response if they received three or more cycles of che- motherapy. Response was defined as follows: complete response, complete disappearance of all detectable dis- ease with no new lesions developing for at least 4 weeks; partial response, more than 50% reduction of the area of measurable disease with no new lesions de- veloping for at least 4 weeks; no response, less than 50% reduction or increase of the area of measurable dis- ease or development of new lesions.
Survival time was measured from the day treat- ment was initiated to the day of death or the last day when the patient was known to be alive. Event-free sur- vival was measured from the day that complete re- sponse was first documented to the day of relapse, de- velopment of a disorder (infection or other disease) that is diagnostic of AIDS, death, or the last day when the patient was known to be in remission. The Kaplan- Meier method5’ was used for survival estimations. Comparison of survival curves was performed using the log-rank test.51 Cox’s regression models5’ were used to measure relative risk of death among different sub- groups within the cohort. The results were analyzed by standard chi-square contingency tables for categorical variables and by Student’s t test for continuous vari- ables. The level considered significant was established at P less than 0.05. Statistical analysis was performed using the computer programs R-SIGMA (Horus Hard- ware SA, Madrid, Spain) and EPILOG version 3.1 (Epi- center Software, Pasadena, CA).
Results
From January 1984 to January 1991, 46 cases of Hodg- kin‘s disease associated with HIV infection were diag- nosed in nine hospitals of the Autonomic Community of Madrid: 2 in 1984,4 in 1985,6 in 1986, 8 in 1987, 9 in 1988, 10 in 1989, 7 in 1990. Forty-three patients (93.5%) were men and 3 (6.5%) were women. Mean age at diagnosis of Hodgkin’s disease was 26.9 years (range, 18-55 years). All patients belonged to high-risk groups for AIDS: 39 (84.8%) were intravenous drugs users, 4 (8.7%) were homosexual, 2 (4.3%) were heterosexual partners of a high-risk person, and 1 (2.2%) had hemo- philia.
Three patients (6.5%) had a previous diagnosis of AIDS, and in 16 (34.8%) AIDS developed after the di- agnosis of Hodgkin’s disease (14 had opportunistic in- fections and 2 had Kaposi’s sarcoma). Overall, in 18 pa- tients (39. l YO), opportunistic infections developed. Ten patients (2 1.7%) had tuberculosis (before the diagnosis of Hodgkin’s disease in four patients and subsequently in six patients). In seven patients (15.2%), P. carinii pneumonia developed concomitantly or subsequently with the diagnosis of Hodgkin’s disease. Less frequent infections included esophageal candidiasis (13%), cyto- megalovirus disease (6.5%), disseminated disease due to Mycobacterium avium-intracellulare (4.3%), and Cyp- tosporidium diarrhea (2.1 YO).
The distribution of histologic subtypes was as fol- lows: 19 patients (41.3%) had mixed cellularity, 10 (21.7%) had lymphoid depletion, 10 (21.7%) had nod- ular sclerosis, 2 (4.3%) had lymphocytic predominance, and 5 (10.9%) had unknown histologic subtype. At first diagnosis, 2 patients (4.3%) had Stage IA disease; 3 (6.5%), Stage 11; 18, (39.1%), Stage 111; and 23 (50%), Stage IV. Thirty-eight patients (82.6%) had B symp- toms. Forty-five patients (97.8%) had nodal disease and 23 (50%) had extranodal disease. Nineteen (41.3%) had bone marrow involvement, and 6 (13%) had Hodgkin’s disease in the liver (Table 1).
At first diagnosis, 27 of 41 patients (51.2%) had anemia, 18 of 41 (43.9%) had leukopenia, 8 of 34 (23.5%) had neutropenia, and 10 of 33 (30.3%) had thrombocytopenia. Elevated serum lactic dehydro- genase level was recorded in 19 of 28 patients (67.9%) and elevated alkaline phosphatase level in 24 of 33 (72.3%). Lymphopenia was observed in 8 of 34 patients (23.5%). CD4 positive lymphocytes were below 500/ mm3 (<0.5 X 109/1) in 26 of 32 patients (81.2%) and below 200/mm3 (<0.2 X 109/1) in 14 (43.7%). The CD4: CD8 ratio was below 0.5 in 11 of 30 patients (36.7%).
Patients with bone marrow involvement had sig- nificantly lower hemoglobin levels, platelet count, and

2402 CANCER May I, 1994, Volume 73, No. 9
Table 1. Hodgkin’s Disease Associated With HIV Infection: Clinicopathological Features
Parameter patients Qh No. of
Risk group i.v. drug users Homosexual
Previous Subsequent
Histopathology Mixed cellularity Lymphoid depletion Nodular sclerosis Lymphocytic predominance
AIDS
Advanced stages (111-IV) B symptoms Extranodal involvement Bone marrow involvement CD4 lymphocytes
< 500/mm3 < 200/mm3
Response to chemotherapy Complete response Partial response
39 4
3 16
19 10 10 2
41 38 23 19
26/32 14/32
12/27 10/27
84.8 8.7
6.5 34.8
41.3 21.7 21.7 4 .3
89.1 82.6 50.0 41.3
81.2 43.7
44.4 37.0
HIV: human immunodeficiency virus; i.v.: intravenous; AIDS: acquired irnmu- nodeficiency syndrome.
CD8 positive lymphocyte count in addition to signifi- cantly elevated serum levels of alkaline phosphatase (Table 2).
Of 46 patients with Hodgkin’s disease associated with HIV infection, 40 were treated with combination chemotherapy, 3 received local radiation therapy, and 3 received no therapy (2 died before treatment could be initiated and 1 was lost to follow-up).
Two of three patients treated with local radiation therapy had Stage IA disease and one had Stage IIA disease. All of them had complete response. One of them relapsed 14 months later. Another died of dissem-
inated tuberculosis 4 months after achieving complete response, and the third patient remains alive and dis- ease-free 10 months after complete response was docu- mented.
This was not a prospective therapeutic trial, and pa- tients were not treated uniformly, which is why all in- formation regarding treatment results must be consid- ered accordingly. Of 40 patients treated with combina- tion chemotherapy, alternating mechlorethamine, vincristine, procarbazine, and prednisone (MOW)/ doxorubicin, bleomycin, vinblastine, dacarbazine (ABVD)53 was used in 16, MOPP-doxorubicin, bleomy- cin, vinblastine hybrid54 in 5, in 6, ABVD56 in 4, cyclophosphamide, vinblastine, procarbazine, pred- nisone (CVPP)57 in 5, and CVPP/ABVD in 4. Twenty- seven patients were evaluable for response to chemo- therapy. Thirteen patients were considered inevaluable (one third of the entire group) due to voluntary aban- donment of therapy (eight patients), death after first cy- cle (four patients), and short follow-up (one patient, still receiving therapy). Of 27 evaluable patients, 12 (44.4%) had a complete response (95% confidence interval, 26- 64%) and 10 (37%) had partial response (95% confi- dence interval, 20-57%), for an overall response rate of 81.4%. Five patients (18.5%) had no response (95% confidence interval, 6-38%). Two of 12 patientsin com- plete remission (1 6.7%) experienced relapse at 7 and 17 months. The percentage of complete responses was 66.6% for patients with mixed cellularity, 33.3% for lymphoid depletion, and 16.6% for nodular sclerosis (nonsignificant differences).
Concerning myelotoxicity of chemotherapy, 16 of 27 patients (59.3%) had leukopenia (<1500 leuko- cytes/mm3) and 15 of 27 (55.5%) had Grade 4 neutro- penia (<500 neutrophils/mm3) according to World Health Organization criteria.
Median follow-up was 10.5 months. Twenty-six of 46 patients with Hodgkin’s disease (56.5%) died. Twenty of them (76.9%) died with evidence of Hodg-
Table 2. Hodgkin’s Disease Associated With HIV Infection: Analytical Parameters Related to Bone Marrow Involvement
Bone marrow No bone marrow involvement involvement
Parameter (mean value) (mean value) P
Hemoglobin (g/dl) 9.9 12.3 < 0.01 Platelets (X 1o3/mm3) 151.5 268.3 < 0.05 Alkaline phosphatase (IU/1) 937.7 334.8 < 0.05 CD8 lymphocytes/mm3 341.6 928.6 < 0.05 CD4 lymphocytes/mm3 291.1 359.9 < 0.1 HIV human immunodeficiency virus.

Hodgkin’s Disease and HIV Infection/Rubio 2403
~
WPOFITIOW
0.8 -
0.7 -
0.6 -
0.5 -
0.4 -
0.3 -
0.2 -
Oul t I I I I I I I
0 6 I f I8 24 30 36 42 Q 0 1 I I(a(THS
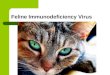
Figure 1. Survival time in 46 patients with Hodgkin’s disease associated with HIV infection.
kin’s disease, and in 14 cases (53.8%), infections con- tributed to death. Projected 3-year survival rate was 19%. Median survival time for the whole group was 15 months (range, 1-44 months) (Fig. 1). Projected event- free survival was 22% at 30 months (median, 17 months; range, 1-55 months) (Fig. 2).
Adverse prognostic factors for survival in univari- ate analysis were B symptoms (P < 0.01), no response to chemotherapy (P < 0.001), hemoglobin level less than 11 g/dl at diagnosis (P < 0.01), leukocyte count less than 4500/mm3 (P < 0.001), lymphocyte count less than 1000/mm3 (P < 0.001), CD4 positive lymphocyte counts less than 200/mm3 (P < 0.05), and alkaline phosphatase level greater than 300 UI/I (P < 0.01) (Ta- ble 3).
Median survival time for patients achieving com- plete response was 26 months; for those with partial response, 14 months; and for those with no response, 5 months.
Discussion
Since the beginning of the AIDS epidemic, isolated cases or small series of patients with Hodgkin’s disease
associated with HIV infection have been r e p ~ r t e d . ~ - ~ ~ However, Hodgkin’s disease has not been accepted as a criterion of AIDS.4 The incidence of Hodgkin’s disease in patients with HIV infection is lower than for non- Hodgkin’s lymphomas.8~’z~z0~29~30~40 In Ioachim et al.’s series,40 the non-Hodgkin’s 1ymphomas:Hodgkin’s dis- ease ratio is 9:l; in Knowles et al.’s reportz9 it is 7:l; in Lowenthal et al.’s report3’ it is 5:l; in Ahmed et al.’s series it is 4:lZ0; and in DiCarlo et al.’s series” there are 29 cases of non-Hodgkin’s lymphoma and only 1 case of Hodgkin’s disease. In Madrid, the ratio is 1.7: 1. This ratio is somewhat more balanced than the reported in Italy (2.7:l). The higher frequency of Hodgkin’s disease in Spain and Italy occurs in a similar epidemiologic context: the predominant high-risk group in both coun- tries is intravenous drug addicts. In our series, we ob- served a significantly higher Hodgkin’s disease:non Hodgkin’s lymphoma ratio in intravenous drug addicts than in homosexuals (0.81 versus 0.24; P < 0.01). A sig- nificantly higher ratio in intravenous drug addicts com- pared with homosexuals has also been reported in France45 and Italy.3zr34 In a study performed involving New York convicts from 1981 to 1984, Ahmed et a1.” did not find an increased incidence of Hodgkin’s disease compared with the general population. However,
PRopOArIW
I
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.1
O a 2 t I I I I I I 0 1 I mnm
0 6 I2 I8 24 30 36 42 Q
Figure 2. Event-free survival time in 12 complete responders.

2404 CANCER May I , 1994, Volume 73, No. 9
Table 3. Hodgkin’s Disease Associated With HIV Infection: Adverse Parameters for Survival (Univariate Analysis)
Parameter
B symptoms Yes No
No response Complete or partial response
AIDS Yes No
Hemoglobin < 1 lg/dl 2 l lg/dl
Total leukocytes < 4500/mm3 t 4500/mm3
Total lymphocytes
Response to therapy
< 1000/mm3 t
< 200/mm3 2 200/mm3
CD4 lymphocytes
Alkaline phosphatase 2 300 1U/1 < 300 IU/I
2 60mm < 60mm
Erythrocyte sedimentation rate
Median Relative No. of survival risk patients (rno)’ (95% cI)t P
38 14 6.4 (1.4-30.1) < 0.01 8 44
5 8 6.9 (1.8-27.0) < 0.001 23 24
19 11 1.9 (0.9-4.1) < 0.1 27 26
17 8 3.1 (1.3-7.6) < 0.01 24 26
18 4 4.4 (1.8-11.1) < 0.001 23 36
8 4 5.1 (1.8-14.0) < 0.001 26 36
14 1 1 3.1 (1.1-8.8) < 0.05 18 36
17 5 3.6 (1.3-9.7) < 0.01 16 26
12 8 2.9 (0.8-10.4) < 0.1 12 26
~ ~ _ _
HIV: human immunodeficiency virus; CI: confidence interval; AIDS: acquired immunodeficiency syndrome * Log-rank test t Cox’s proportional risk model (univariate analysis).
among convicts who were intravenous drug addicts, the incidence of Hodgkin’s disease was three times higher. In agreement with other authors,45 we think that avail- able data support the finding that Hodgkin’s disease as- sociated with HIV infection occurs preferentially in in- travenous drug addicts. Transmission of blood-borne infectious agents in patients with HIV-induced immu- nosuppression may be implied in the pathogenesis of Hodgkin’s disease in such patients. Recently, an in- creased incidence of Hodgkin’s disease in San Francisco homosexuals with HIV infection has also been re- ported.58
The natural history of Hodgkin’s disease in patients with HIV infection results in a more aggressive disease than in the general population, including higher fre- quency of advanced stages and unfavorable histologc
In the current se- ries, 89% of patients had advanced stages (111-IV) at di- findings at diagnosis. 10.13,15-17,32,38.41-44
agnosis, a percentage similar to other series of Hodg- kin’s disease associated with HIV infection (74-94%) and higher than the frequency reported in series of Hodgkin’s disease in the general population (approxi- mately 40?L0).~~ Most patients have B symptoms (70- 100 y0),29,38.41-43 in contrast to 57% in patients with Hodgkin’s disease without HIV infection.60 In the cur- rent series, 41.3% of patients had bone marrow in- volvement at first diagnosis versus 3.5% in 659 histori- cal controls with Hodgkin’s disease and no HIV infec- t i ~ n . ~ ~ The high frequency of bone marrow involvement has also been reported in other series of Hodgkin’s disease associated with HIV infection (50-
In our experience, the most frequent histologic sub- type was mixed cellularity (41.3%), followed by lym- phoid depletion (21.7%), nodular sclerosis (21.7%), and lymphocytic predominance (4.3%). Such distribution is
72y0).29,38.41.42

Hodgkin’s Disease and HIV Infection/Rubio 2405
similar in most series of Hodgkin‘s disease associated with HIV infection, mixed cellularity being most fre- quent (30-loo%), followed by nodular sclerosis (6- 54~0).27,29-31.38,41-43 I n some series, nodular sclerosis was the most frequent subtype.” Lymphoid depletion was observed in 8-20% of cases,29~31~38~42 although other au- thors have not reported such a s ~ b t y p e . ~ ’ , ~ ~ These data are in contrast with those observed in patients with Hodgkin’s disease without HIV infection, in whom nodular sclerosis is the most frequent histologic subtype (52-62%), followed by mixed cellularity (23-25%), lymphocytic predominance (6-7%), and lymphoid de- pletion (3-6Y0).~’
Active Hodgkin’s disease in patients without HIV infection is associated with functional alterations in the immune system,61’62 with no relevant alteration in the number of T-lymphocytes or CD4 or CD8 positive pop- ulations in peripheral In contrast, in patients with Hodgkin’s disease associated with HIV infection as well as in patients with AIDS,64 a severe depletion of CD4 lymphocytes has been ~ b s e r v e d . ~ ’ , ~ ~
The percentage of complete responses in patients with Hodgkin’s disease without HIV infection treated with MOPP/ABVD is 89%, and 8-year disease-free survival time is 73%.65 The percentage of complete responses in patients with Hodgkin’s disease associ- ated with HIV infection is markedly lower (53- 64~0).29,31,38,41.46 The percentage was 48% in the current series. Acknowledging the limitations of historic com- parisons, these results must be interpreted with caution.
The frequency of severe myelotoxicity due to che- motherapy is higher in patients with Hodgkin’s disease and HIV infection than in patients with Hodgkin’s dis- ease without HIV infection.53 This may be due to HIV- related depression of hematopoiesis.66
Infections described in patients with Hodgkin’s dis- ease without HIV infection are mostly due to gram-pos- itive cocci and bacilli and gram-negative bacilli (84% of microbiologically documented infection^).^' Opportu- nistic infections are infrequent in these patient^.^^,^^ In contrast, in patients with Hodgkin’s disease and HIV infection, opportunistic infections diagnostic of AIDS often develop, many of them concomitantly with com- bination ~hemotherapy.~~,~’,~’-~~ In 35-78 % of patients, AIDS develops eventually.
In the series of patients without HIV infection re- ported by Longo et al.,55 48% of patients with Hodg- kin’s disease treated with MOPP survived, with a me- dian follow-up time of 14 years (range, 9-21 years) after completion of therapy. In the current series, patients with Hodgkin’s disease associated with HIV infection had a median survival time of 15 months, similar to that reported by other^.^^,^^,^^,^^,^^ Adverse prognostic fac-
tors were presence of B symptoms, absence of complete response, anemia, leukopenia, lymphopenia, impair- ment of cellular immunity (CD4 lymphocyte count < 200/mm3), and high serum levels of alkaline phospha- tase.
In conclusion, Hodgkin’s disease associated with HIV infection is more frequent among intravenous drug addicts and behaves differently than in the general pop- ulation, including higher frequency of advanced-stage disease, B symptoms, unfavorable histologic subtypes, bone marrow involvement, decreased CD4 lympho- cytes, and development of opportunistic infections. Re- sponse to combination chemotherapy is poor, myelo- toxicity is frequent, and survival time is short.
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
Centers for Disease Control. Centers for Disease Control Task Force on Kaposi sarcoma and opportunistic infections: epidemi- ological aspects of the current outbreak of Kaposi Sarcoma and opportunistic infections. N Engl J M e d 1982; 306:248-52. Centers for Disease Control. Update: acquired immunodefi- ciency syndrome. United States. MMWR 1982; 31:507-14. Centers for Disease Control. Revision of the case definition of acquired immunodeficiency syndrome for national reporting United States. MMWR 1985; 34:373-5. Centers for Disease Control. Revision of the CDC surveillance case definition for acquired immunodeficiency syndrome,
Ioachim HL, Cooper MC, Hellman GC. Hodgkin’s disease and the acquired immunodeficiency syndrome. Ann Intern Med 1984;
Robert NJ, Schneidermn H. Hodgkin‘s disease and the acquired immunodeficiency syndrome. Ann Intern Med 1984; 101:142-3. Dancis A, Odajnyk C, Krigel RL, Raphael B, Laubenstein L, Goldberg A, et al. Association of Hodgkin’s and non-Hodgkin’s lymphomas with the acquired immunodeficiency syndrome (AIDS). Proceedings of the American Society of Clinical Oncol- ogy; May 1984; 3:61. Ioachim HL, Cooper MC, Hellman GG. Lymphomas in men at high risk for acquired immune deficiency syndrome (AIDS): a study of 21 cases. Cancer 1985; 56:2831-42. Scheib RG, Siege1 RS. Atypical Hodgkin’s disease and the ac- quired immunodeficiency syndrome. Ann Intern Med 1985; 102: 554-5. Schoeppel SL, Hoppe RT, Dorfman RF, Homing SJ, Chew TG, Weiss LM, et al. AIDS and Hodgkin‘s disease. Front Radiat Ther Oncol 1985; 19:66-73. Moore GE, Cook DD. AIDS in association with malignant mela- noma and Hodgkin’s disease. ] Clin Oncol 1985; 3:1437. DiCarlo EF, Amberson JB, Metroka CE, Ballard P, Moore A, Mouradian JA. Malignant lymphomas and the acquired immu- nodeficiency syndrome. Arch Pathol Lab Med 1986; 110:1012-6. Baer DM, Anderson ET, Wilkinson LE. Acquired immunodefi- ciency syndrome in homosexual men with Hodgkin’s disease. Am I M e d 1986; 80:738-40. Mitsuyasu RT, Colman MF, Sun NC. Simultaneous occurrence of Hodgkin’s disease and Kaposi’s sarcoma in a patient with ac- quired immunodeficiency syndrome. A m I Med 1986; 80:954-8.
MMWR 1987; 36(S~ppl):15-155.
101:876-7.

2406 CANCER May 2, 2994, Volume 73, No. 9
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
30.
31.
32
33
34
35
Temple JJ, Andes WA. AIDS and Hodgkin‘s disease. Lancet
Prior E, Goldberg AF, Conjalka MS, Chapman WE, Tay S, Ames ED. Hodgkin’s disease in homosexual men: an AIDS-related phenomenon. Am J M e d 1986; 81:1085-8. Unger PD, Strauche ]A. Hodgkin’s disease in AIDS complex pa- tients: report of four cases and tissue immunologic market stud- ies. Cancer 1986; 58:821-5. Groopman JE, Mayer K, Zipoli T, Wallach S, Fallon 8, Clark J. Unusual neoplasms associated with HTLV-111 infection. Pro- ceeding of the American Society of Clinical Oncology 1986; 5:4. Lopez-Herce Cid ]A, Lopez-Herce Cid J, Saiiudo EF, Menarquez J, Ochaita JL. AIDS and Hodgkin’s disease. Lancet 1986; 21104-5. Ahmed T, Wormser GP, Stahl RE, Mamtani R, Cimino J, Glasser M, et al. Malignant lymphomas in a population at risk for ac- quired immune deficiency syndrome. Cancer 1987; 60:719-23. Picard 0, Gramont A, Krulik M, Gonzalez G, Debray J, Caday J . Rectal Hodgkin’s disease and the acquired immunodeficiency syndrome. Ann Intern Med 1987; 106:775. Bello JL, Magallon M, Villar JM. Hodgkin‘s disease in hemophil- iacs. A n n Intern Med 1987; 107:257. Coulbourn D, Staszewsky H, Goldenberg S, Donovan V, Raio F. Fulminant lymphocyte depleted Hodgkin’s disease in a homo- sexual man with HIV infection. Ny State J Med 1987; 87:570-1. De Luca RR, Needleman SW, Schiffer CA. Hodgkin’s disease in HTLV-111 positive patients. Proceedings of the American Society of Clinical Oncology 1987; 6:3. G6ngora-Biachi RA, Gonzalez Martinez P, Bastarrachea Ortiz J . Hodgkin’s disease as the initial manifestation of acquired immu- nodeficiency syndrome. Ann Intern Med 1987; 107:112. Ioachim HL, Cooper MC, Hellman GC. Lymphomas associated with the acquired immune deficiency syndrome (AIDS): a study of 35 cases. Cancer Detect Prev 1987; 1:557-65. Kaplan LD, Abrams DI, Volberding PA. Clinical course and epi- demiology of Hodgkin’s disease in homosexual men in San Francisco. Third International Conference on Acquired Immu- nodeficiency Syndrome; 1987 Jun 1-5; Washington, DC; 3:9. Clavero C, Bailen A, Botello MC, Maldonado J. Complejo asoci- ado al shdrome de immunodeficiencia adquirida y enfermedad de Hodgkin. Med Clin (Bard 1987; 89:219-20. 29. Knowles DM, Chamulak GA, Subar M, Burke JS, Dugan M, Wernz J, et al. Lymphoid neoplasia associated with the acquired immunodeficiency syndrome (AIDS). Ann Intern Med 1988; 108: 744-53. Lowenthal DA, Straus DJ, Campbell SW, Gold JW, Clarkon BD, Koziner B. AIDS related lymphoid neoplasia. Cancer 1988; 61:
Andrieu JM, Tirelli V, Tourani JM, Vaccher E, Lazzarin A, Ra- phael M, et al. Areport of 53 patients with HIV-associated Hod- gkin’s disease in Europe. Second International Workshop on AIDS-related neoplasia; 1988 May 13-14, 1988; Toledo [ab- stract 261. Tirelli U, Vaccher E, Rezza G , Broccia G, Fassio PG, Gobbi M et al. Hodgkin’s disease and infection with the human immunode- ficiency virus (HIV) in Italy. Ann Intern Med 1988; 108:309-10. Devars de Mayne JF, Teillet-Thiebaud F, Pulik M, Courtois F. Seropositivity to HIV in Hodgkin’s disease. Lancet 1988; 2:1024. Italian Cooperative Group for AIDS related tumors. Malignant lymphomas in patients with or at risk for AIDS in Italy. J Natl Cancer lnst 1988; 802355-60. Keyserlingk HV, Ludwing WD, Seibt H, Ruhl H, Hoffken G. Atypical presentation of Hodgkin’s disease in a patient at risk for
1986; 2~454-5.
2325-37.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
the acquired immunodeficiency syndrome. Cancer Detect Prev
Rubio R, Yebra M, Alvarez de Mon M, Costa JR, Espafia P, Tor- roba L y cols. Enfermedad de Hodgkin en pacientes con infec- ci6n por el virus de la inmunodeficiencia humana. Estudio de 9 casos. Med Clin @arc) 1989; 93:l-4. De Mascarel A, Merlio JP, Laborie V, Lacut JY. Hodgkin’s disease in acquired immunodeficiency syndrome. Arch Pathol Lab Med 1989; 113:328. Serrano M, Bellas C, Campos E, Ribera J, Martin C, Rubio R, et al. Hodgkin’s disease in patients with antibodies to human immunodeficiency virus: a study of 19 patients. Cancer 1990; 65:
Rubio R, Serrano M, Flores E, Buz6n L, Yebra M, Escobar Y, et al. Hodgkin’s disease in intravenous drug users with HIV infec- tion: a report of 27 cases in Madrid. Sixth International Confer- ence on AIDS; 1990 Jun 20-24; San Francisco, vol. 3 [abstract 212 (SB 506)]. Ioachim HL, Dorsett B, Cronin W, Maya M, Wahls S. Acquired immunodeficiency syndrome-associated lymphomas: clinical, pathologic, immunologic and viral characteristics of 11 1 cases. Hum Patholl991; 22659-73. Ree HJ, Strauchen ]A, Khan AA, Gold JE, Crowley JP, Khan H, et al. Human immunodeficiency virus-associated Hodgkin‘s dis- ease. Cancer 1991; 67:1614-21. Ames ED, Conjalka MS, Golberg AF, Hirschman R, Jain S, Dis- tenfeld A, et al. Hodgkin’s disease and AIDS. Hematol Oncol Clin North Am 1991; 5:343-56. Gold JE, Altarac D, Ree HJ, Khan A, Sordillo PP, Zalusky R. HIV- associated Hodgkin’s disease: a clinical study of 18 cases and review of the literature. Am J Hematol 1991; 36:93-9. Pelstring RJ, Zellmer RB, Sulak LE, Baks PM, Clare N. Hodgkin’s disease in association with human immunodeficiency virus in- fection: pathologic and immunologic features. Cancer 1991; 6 7
Roithmann S, Tourani JM, Andrieu JM. Hodgkin‘s disease in HIV-infected intravenous drug abusers. N EnglJ Med 1990; 323:
Monfardmi S, Tirelli U, Vaccher E, Foa R, Gavosto F. Hodgkin’s disease in 63 intravenous drug users infected with human im- munodeficiency virus. Ann Oncoll991; Z(Suppl2):201-5. Lukes RJ, Craver LF, Hall TC, Rappaport H, Ruber P. Report of the nomenclature committee. Cancer Res 1966; 26:1311. Lukes RJ, Butler JJ. The pathology and nomenclature of Hodg- kin’s disease. Cancer Res 1966; 26:1063-83. Carbone PP, Kaplan HS, Musshoff K, Smithiers DW, Tubiana M. Report of the committee on Hodgkin’s disease staging. Cancer Res 1971; 31:1860-1. Kaplan EL, Meier P. Non-parametric estimation from incom- plete observations. ]Am Stat Assoc 1958; 53:457-81. Mantel N. Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother Rep 1966;
Cox DR. Regression models and life tables. J R Stat SOC B 1972;
Santoro A, Bonadonna G, Bonfante V, Valaggussa P. Alternating drug combinations in the treatment of advanced Hodgkin’s dis- ease. N Engl J Med 1982; 306:770-5. Klimo P, Connors JM. An update on the Vancouver experience in the management of advanced Hodgkin’s disease treated with the MOPP/ABV Hybrid program. Semin Hernatol 1988;
Longo DL, Young RC, Wesley M, Hubbard SM, Duffey PL, Jaffe
1988; 12~243-8.
2248-54.
1865-73.
275-6.
50:163-70.
34:187-220.
25(S~ppl2):34-40.

Hodgkin’s Disease and HIV Infection/Rubio
56.
5 7.
58.
59.
60.
61.
ES, et al. Twenty years of MOPP therapy for Hodgkin’s disease. J Clin Oncol 1986; 4:1295-306. Santoro A, Bonadona G, Valagussa P, Zucaldi R, Viviani S, Vil- lani F, et al. Long-term results of combined chemotherapy-ra- diotherapy approach in Hodgkin’s disease: superiority of ABVD plus radiotherapy versus MOPP plus radiotherapy. J Clin Oncol
Morgenfeld M, Somoza N, Magnasco J, Pavlovsky S , Bonesana AC, Bezares R, et al. Combined chemotherapy with cyclophos- phamide, vinblastine, procarbazine and prednisone (CVPP) vs CVPP plus CCNU (CCVPP) in Hodgkin‘s disease. Cancer 1979;
Hessol NA, Katz MH, Liu JY, Buchbinder SP, Rubino CJ, Holmberg SD. Increased incidence of Hodgkin‘s disease in ho- mosexual men with HIV infection. Ann Intern Med 1992; 117:
Colby TV, Hoppe RT, Warnke RA. Hodgkin’s disease: a clinico- pathologic study of 659 cases. Cancer 1981; 1848-58. David S, Dahlberg S, Myers MH, Chen A, Steinhom SC. Hodg- kin’s disease in the United States: a comparison of patient char- acteristics and survival in the Centralized Cancer Patient Data System and the Surveillance, Epidemiology and End Results Program. INCl 1987; 78:471-8. Ford RJ, Tsao J, Mehta S . Interleukin abnormality in Hodgkin‘s
1987; 5:27-37.
43: 1579-86.
309-1 1.
62.
63.
64.
65.
66.
67.
68.
2407
disease: its possible relationship to the T cell defect. Fed Proc 1984; 43:1920. Goodwin JS, Messner RP, Banfhurst AD, Peake GT, Saiki JH, Williams RC. Prostaglandin-producing supressor cells in Hodg- kin‘s disease. N Engl J M e d 1977; 297:963-8. Posner MR, Reinherz EL, Beard J, Nadler LM, Rosenthal DS, Scholssman SK. Lymphoid subpopulations of peripheral blood and spleen in untreated Hodgkin’s disease. Cancer 1987; 48:
Bowen-DL, Lane HC, Fauci AS. Immunopathogenesis of the ac- quired immunodeficiency syndrome. Ann Intern Med 1985; 103:
Bonadona G, Valagussa P, Santoro A. Alternating non-cross-re- sistant combination chemotherapy or MOPP in stage IV Hodg- kin’s disease: a report of 8-year results. Ann Intern Med 1986;
Scadden DT, Zon LI, Groopman JE. Pathophysiology and man- agement of HIV associated hematologic disorders. Blood 1989;
Coker DD, Moms DM, Coleman JJ, Schimpff SC, Wiernik PH, Elias EG. Infections among 210 patients with surgically staged Hodgkin’s disease. Am J M e d 1983; 75:97-109. Notter DT, Grossman PL, Rosenberg SA, Remington JS. Infec- tions in patients with Hodgkin’s disease: a clinical study of 300 consecutive adult patients. Rev Infect Dis 1980; 2:761-800.
11 70-6.
704-9.
104:739-46.
74~1455-63.