Embed Size (px)
Citation preview

1
HMOBenefit Summaries 26 plans with office copays from $15 to $40
800.542.4218 www.calchoice.com
CalChoice®HMO152
Anthem Blue Cross*, Health Net*, Kaiser Permanente, Sharp, Western Health Advantage
No Deductible
$15Copay
$15 Copay
$100 Copay
$400Copay-100%
100%
$100 Copay (waived if admitted)
$10Copay
$20Copay
Covered
Covered as any illness
Not Covered
$2,000/$4,000
$15 Copay
$200 Copay
100%
$400 Copay – Max 100 days per year
$50 per trip
Covered
$30 Copay
20 visits per year
Not Covered
$400 Copay - 100% Acute detox only
CalChoiceHMO252
Anthem Blue Cross*
No Deductible
$25Copay
$25 Copay
$100 Copay
$450Copayperday-Max$1,800
100%
$150 Copay (waived if admitted)
$15Copay
$100Ded.-$30Copay
Covered
Covered as any illness
$25 Copay7
$3,000 / $6,000
$25 Copay
$400 Copay
$25 Copay
100%
$100 per trip
Covered
$25 Copay
No Maximum
$450 Copay per day - Max $1,800
$450 Copay per day – Max $1,800
CalChoiceHMO252
Health Net*
No Deductible
$25Copay
$25 Copay
$100 Copay
$450Copayperday-Max$1,800
100%
$150 Copay (waived if admitted)
$15Copay
$100Ded.-$30Copay
Covered
Covered as any illness
Not Covered
$3,000/$6,000
$25 Copay
$400 Copay
$45 Copay
$450 Copay per day – Max $1,800/100 days per year
$200 per trip
Covered
$40 Copay
20 visits per year
Not Covered
$450 Copay per day – Max $1,800, Acute detox only
CalChoiceHMO252
Kaiser Permanente
No Deductible
$25Copay
$5 Copay
$50 Copay
$400Copay-100%
100%
$150 Copay (waived if admitted)
$10Copay
$25Copay
Covered
Covered as any illness
Not Covered
$2,500/$5,000
$25 Copay
$300 Copay
100%
$100 Copay – Max 100 days per year
$100 per trip
Covered
$25 Copay
No Maximum
$400 Copay - 100%
$400 Copay - 100% Acute detox only
MedicalBenefits
Participating Health Plans
Deductible
DROFFICEVISITS
Lab and X-Ray
MRI, CT, and PET
HOSPITALSERVICES
Inpatient Physician Fees
Emergency Room
RxBENEFITS
Generic
Brand 3
Oral Contraceptives
Maternity
Chiropractic
Out-of-Pocket Max Ind/Fam
2nd Surgical Opinion
Outpatient Surgery
Home Health Care
Skilled Nursing Facility
Per Disability
Ambulance
Pre-Existing Conditions
Mental/Nervous Non-Severe 1,4,5
Doctor Fees
Annual Maximum
Hospital Fees
Drug/Alcohol 4,5
Hospital Fees
See footnotes on back page

800.542.4218 www.calchoice.com
2
HMOBenefit Summaries
CalChoiceHMO25 Value
Health Net*
No Deductible
$25Copay
$25 Copay
$100 Copay
75%
100%
$150 Copay (waived if admitted)
$15Copay
$100Ded.-$30Copay
Covered
Covered as any illness
Not Covered
$3,000/$6,000
$25 Copay
75%
$45 Copay
75% Max 100 days per year
$200 per trip
Covered
$40 Copay
20 visits per year
Not Covered
75% Acute detox only
CalChoiceHMO25 Value
Anthem Blue Cross*
$1,000 Sgl. $2,000 Fam. (applies to Max OOP)
$25Copay
$25 Copay
$100 Copay
80%afterdeductible
100%
$150 Copay after deductible (waived if admitted)
$15Copay
$200Ded.-$30Copay
Covered
Covered as any illness
$25 Copay7
$3,000/$6,000
$25 Copay
80% after deductible
$25 Copay
100% after deductible
$100 per trip
Covered
$25 Copay
No Maximum
80% after deductible
80% after deductible
MedicalBenefits
Participating Health Plans
Deductible
DROFFICEVISITS
Lab and X-Ray
MRI, CT, and PET
HOSPITALSERVICES
Inpatient Physician Fees
Emergency Room
RxBENEFITS
Generic
Brand 3
Oral Contraceptives
Maternity
Chiropractic
Out-of-Pocket Max Ind/Fam
2nd Surgical Opinion
Outpatient Surgery
Home Health Care
Skilled Nursing Facility
Per Disability
Ambulance
Pre-Existing Conditions
Mental/Nervous Non-Severe 1,4,5
Doctor Fees
Annual Maximum
Hospital Fees
Drug/Alcohol 4,5
Hospital Fees
CalChoiceHMO252
Western Health Advantage
No Deductible
$25Copay
$25 Copay
100%
$400Copayperday–Max$1,200
100%
$150 Copay (waived if admitted)
$15Copay
$100Ded.-$30Copay
Covered
Covered as any illness
Not Covered
$2,500/$5,000
$25 Copay
$300 Copay
$30 Copay
$400 Copay per day – Max $1,200/100 days per year
$100 per trip
Covered
$25 Copay
No Maximum
$400 Copay per day - Max $1,200
$400 Copay per day – Max $1,200, Acute detox only
CalChoice®HMO252
Sharp
No Deductible
$25Copay
$25 Copay
100%
$400CopayperdayMax$1,200
100%
$150 Copay (waived if admitted)
$15Copay
$100Ded.-$30Copay
Covered
Covered as any illness
Not Covered
$2,500/$5,000
$25 Copay
$300 Copay
$30 Copay
$400 Copay per day Max $1,200/100 days per year
$100 per trip
Covered
$40 Copay
20 visits per year
Not Covered
$400 Copay per day – Max $1,200, Acute detox only
See footnotes on back page

3
HMOBenefit Summaries Effective January 1, 2012
ElectOpenAccess
Health Net*
No Deductible
$25CopayHMO$40CopayPPO
$25 Copay
$100 Copay
75%
$25 Copay
$150 Copay (waived if admitted)
$15Copay
$100Ded.-$30Copay
Covered
Covered as any illness
Not Covered
$3,000 Ind/$6,000 Two Party/$7,000 Fam
$25 Copay
75%
100%
75% Max 100 days per year
100%
Covered
$30 Copay
20 visits per year
75% (30 days per year)
75% Acute detox only
ElectOpenAccess 25Plus
Health Net*
No Deductible
$25CopayHMO$40CopayPPO
$25 Copay
$100 Copay
$450Copayperday–Max$1,800
$25 Copay
$150 Copay (waived if admitted)
$15Copay
$100Ded.-$30Copay
Covered
Covered as any illness
Not Covered
$3,000 Ind/$6,000 Two Party/$7,000 Fam
$25 Copay
$400 Copay
100%
75% Max 100 days per year
100%
Covered
$30 Copay
20 visits per year
$450 Copay per day – Max $1,800, 30 Days per year
$450 Copay per day – Max $1,800, Acute detox only
SaludHMOyMás6
Health Net
No Deductible
$25Copay
100%
100%
$500Copayperday–Max$1,000
100%
$100 Copay (waived if admitted)
$15Copay
$25Copay
Covered
Covered as any illness
Not Covered
$2,500/$5,000
$25 Copay
$300 Copay
$30 Copay
$500 Copay per day – Max $1,000/100 days per year
$50 per trip
Covered
$40 Copay
20 visits per year
Not Covered
$500 Copay per day – Max $1,000, Acute detox only
MedicalBenefits
Participating Health Plans
Deductible
DROFFICEVISITS
Lab and X-Ray
MRI, CT, and PET
HOSPITALSERVICES
Inpatient Physician Fees
Emergency Room
RxBENEFITS
Generic
Brand 3
Oral Contraceptives
Maternity
Chiropractic
Out-of-Pocket Max Ind/Fam
2nd Surgical Opinion
Outpatient Surgery
Home Health Care
Skilled Nursing Facility
Per Disability
Ambulance
Pre-Existing Conditions
Mental/Nervous Non-Severe 1,4,5
Doctor Fees
Annual Maximum
Hospital Fees
Drug/Alcohol 4,5
Hospital Fees
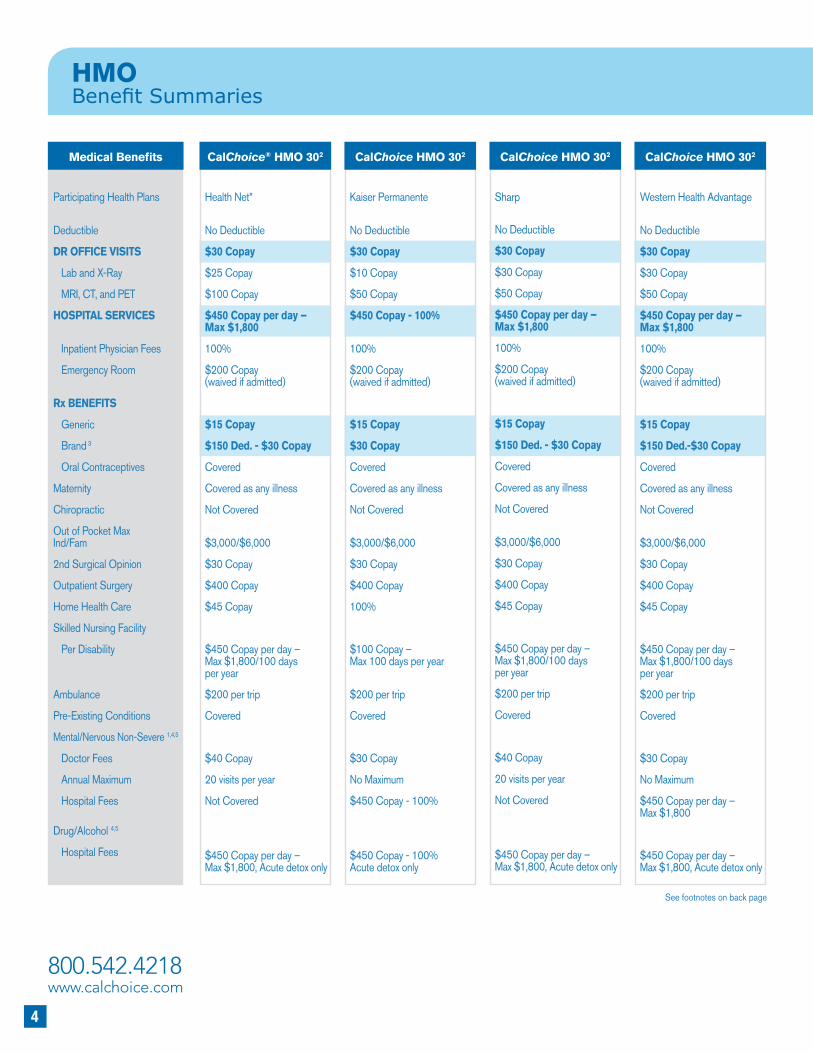
CalChoice®HMO302
Anthem Blue Cross*
No Deductible
$30Copay
$30 Copay
$100 Copay
$450Copayperday–Max$1,800
100%
$200 Copay (waived if admitted)
$15Copay
$150Ded.-$30Copay
Covered
Covered as any illness
$30 Copay7
$3,000/$6,000
$30 Copay
$400 Copay
$30 Copay
100%
$200 per trip
Covered
$30 Copay
No Maximum
$450 Copay per day – Max $1,800
$450 Copay per day – Max $1,800
See footnotes on back page
800.542.4218 www.calchoice.com
4
HMOBenefit Summaries
CalChoiceHMO302
Kaiser Permanente
No Deductible
$30Copay
$10 Copay
$50 Copay
$450Copay-100%
100%
$200 Copay
(waived if admitted)
$15Copay
$30Copay
Covered
Covered as any illness
Not Covered
$3,000/$6,000
$30 Copay
$400 Copay
100%
$100 Copay – Max 100 days per year
$200 per trip
Covered
$30 Copay
No Maximum
$450 Copay - 100%
$450 Copay - 100% Acute detox only
CalChoiceHMO302
Western Health Advantage
No Deductible
$30Copay
$30 Copay
$50 Copay
$450Copayperday–Max$1,800
100%
$200 Copay (waived if admitted)
$15Copay
$150Ded.-$30Copay
Covered
Covered as any illness
Not Covered
$3,000/$6,000
$30 Copay
$400 Copay
$45 Copay
$450 Copay per day – Max $1,800/100 days per year
$200 per trip
Covered
$30 Copay
No Maximum
$450 Copay per day – Max $1,800
$450 Copay per day – Max $1,800, Acute detox only
CalChoiceHMO302
Sharp
No Deductible
$30Copay
$30 Copay
$50 Copay
$450Copayperday–
Max$1,800
100%
$200 Copay
(waived if admitted)
$15Copay
$150Ded.-$30Copay
Covered
Covered as any illness
Not Covered
$3,000/$6,000
$30 Copay
$400 Copay
$45 Copay
$450 Copay per day – Max $1,800/100 days per year
$200 per trip
Covered
$40 Copay
20 visits per year
Not Covered
$450 Copay per day – Max $1,800, Acute detox only
CalChoice®HMO302
Health Net*
No Deductible
$30Copay
$25 Copay
$100 Copay
$450Copayperday–
Max$1,800
100%
$200 Copay
(waived if admitted)
$15Copay
$150Ded.-$30Copay
Covered
Covered as any illness
Not Covered
$3,000/$6,000
$30 Copay
$400 Copay
$45 Copay
$450 Copay per day – Max $1,800/100 days per year
$200 per trip
Covered
$40 Copay
20 visits per year
Not Covered
$450 Copay per day – Max $1,800, Acute detox only
MedicalBenefits
Participating Health Plans
Deductible
DROFFICEVISITS
Lab and X-Ray
MRI, CT, and PET
HOSPITALSERVICES
Inpatient Physician Fees
Emergency Room
RxBENEFITS
Generic
Brand 3
Oral Contraceptives
Maternity
Chiropractic
Out of Pocket Max Ind/Fam
2nd Surgical Opinion
Outpatient Surgery
Home Health Care
Skilled Nursing Facility
Per Disability
Ambulance
Pre-Existing Conditions
Mental/Nervous Non-Severe 1,4,5
Doctor Fees
Annual Maximum
Hospital Fees
Drug/Alcohol 4,5
Hospital Fees
See footnotes on back page

5
Effective January 1, 2012
CalChoice®HMO30 Value
Health Net*
No Deductible
$30Copay
$30 Copay
$100 Copay
70%
100%
$200 Copay
(waived if admitted)
$20Copay
$200Ded.-$30Copay
Covered
Covered as any illness
Not Covered
$3,500/$7,000
$30 Copay
70%
$45 Copay
70% Max 100 days per year
$200 per trip
Covered
$40 Copay
20 visits per year
Not Covered
70% Acute detox only
MedicalBenefits
Participating Health Plans
Deductible
DROFFICEVISITS
Lab and X-Ray
MRI, CT, and PET
HOSPITALSERVICES
Inpatient Physician Fees
Emergency Room
RxBENEFITS
Generic
Brand 3
Oral Contraceptives
Maternity
Chiropractic
Out of Pocket Max Ind/Fam
2nd Surgical Opinion
Outpatient Surgery
Home Health Care
Skilled Nursing Facility
Per Disability
Ambulance
Pre-Existing Conditions
Mental/Nervous Non-Severe 1,4,5
Doctor Fees
Annual Maximum
Hospital Fees
Drug/Alcohol 4,5
Hospital Fees
CalChoiceHMO402
Anthem Blue Cross*
No Deductible
$40Copay
$40 Copay
$100 Copay
$500Copayperday
100%
$250 Copay (waived if admitted)
$20Copay
$200Ded.-$30Copay
Covered
Covered as any illness
$40 Copay7
$3,500 / $7,000
$40 Copay
$500 Copay
$40 Copay
100%
$200 per trip
Covered
$40 Copay
No Maximum
$500 Copay per day
$500 Copay per day
CalChoiceHMO402
Kaiser Permanente
No Deductible
$40Copay
$10 Copay
$50 Copay
$500Copayperday
100%
$250 Copay (waived if admitted)
$15Copay
$30Copay
Covered
Covered as any illness
Not Covered
$3,500/$7,000
$40 Copay
$500 Copay
100%
$100 Copay – Max 100 days per year
$200 per trip
Covered
$40 Copay
No Maximum
$500 Copay per day
`
$500 Copay per day –
Acute detox only
CalChoiceHMO402
Health Net*
No Deductible
$40Copay
$25 Copay
$100 Copay
$500Copayperday
100%
$250 Copay
(waived if admitted)
$20Copay
$200Ded.-$30Copay
Covered
Covered as any illness
Not Covered
$3,500/$7,000
$40 Copay
$500 Copay
$50 Copay
$500 Copay per day – Max 100 days per year
$200 per trip
Covered
$50 Copay
20 visits per year
Not Covered
$500 Copay per day – Acute detox only
See footnotes on back page

800.542.4218 www.calchoice.com
6
HMOBenefit Summaries
See footnotes on back page
MedicalBenefits
Participating Health Plans
Deductible
DROFFICEVISITS
Lab and X-Ray
MRI, CT, and PET
HOSPITALSERVICES
Inpatient Physician Fees
Emergency Room
RxBENEFITS
Generic
Brand 3
Oral Contraceptives
Maternity
Chiropractic
Out of Pocket Max Ind/Fam
2nd Surgical Opinion
Outpatient Surgery
Home Health Care
Skilled Nursing Facility
Per Disability
Ambulance
Pre-Existing Conditions
Mental/Nervous Non-Severe 1,4,5
Doctor Fees
Annual Maximum
Hospital Fees
Drug/Alcohol 4,5
Hospital Fees
CalChoiceHMO40 Value
Anthem Blue Cross*
$1,500 Sgl. $3,000 Fam. (applies to Max OOP)
$40Copay
$40 Copay
$100 Copay
70%afterdeductible
100%
$250 Copay after deductible (waived if admitted)
$15Copay
$250Ded.-$30Copay
Covered
Covered as any illness
$40 Copay7
$4,000/$8,000
$40 Copay
70% after deductible
$40 Copay
100% after deductible
$200 per trip
Covered
$40 Copay
No Maximum
70% after deductible
70% after deductible
CalChoiceHMO402
Western Health Advantage
No Deductible
$40Copay
$40 Copay
$50 Copay
$500Copayperday
100%
$250 Copay (waived if admitted)
$20Copay
$200Ded.-$30Copay
Covered
Covered as any illness
Not Covered
$3,500/$7,000
$40 Copay
$500 Copay
$50 Copay
$500 Copay per day – Max 100 days per year
$200 per trip
Covered
$40 Copay
No Maximum
$500 Copay per day
$500 Copay per day – Acute detox only
CalChoice®HMO402
Sharp
No Deductible
$40Copay
$40 Copay
$50 Copay
$500Copayperday
100%
$250 Copay
(waived if admitted)
$20Copay
$200Ded.-$30Copay
Covered
Covered as any illness
Not Covered
$3,500/$7,000
$40 Copay
$500 Copay
$50 Copay
$500 Copay per day – Max 100 days per year
$200 per trip
Covered
$50 Copay
20 visits per year
Not Covered
$500 Copay per day – Acute detox only
CalChoiceHMO40 Value
Health Net*
No Deductible
$40Copay
$40 Copay
$100 Copay
60%
100%
$250 Copay (waived if admitted)
$20Copay
$200Ded.-$30Copay
Covered
Covered as any illness
Not Covered
$3,500/$7,000
$40 Copay
60%
$50 Copay
60% Max 100 days per year
$200 per trip
Covered
$50 Copay
20 visits per year
Not Covered
60%, Acute detox only

7
Effective January 1, 2012
See footnotes on back page
MedicalBenefits
Participating Health Plans
Deductible
DROFFICEVISITS
Lab and X-Ray
MRI, CT, and PET
HOSPITALSERVICES
Inpatient Physician Fees
Emergency Room
RxBENEFITS
Generic
Brand 3
Oral Contraceptives
Maternity
Chiropractic
Out of Pocket Max Ind/Fam
2nd Surgical Opinion
Outpatient Surgery
Home Health Care
Skilled Nursing Facility
Per Disability
Ambulance
Pre-Existing Conditions
Mental/Nervous Non-Severe 1,4,5
Doctor Fees
Annual Maximum
Hospital Fees
Drug/Alcohol 4,5
Hospital Fees
CalChoice®HMO40 Value
Western Health Advantage
$2,500 Sgl. $5,000 Fam.
$40Copay
100%
$50 Copay
$500Copayperday–afterdeductible(applies to Max OOP )
100%
$250 Copay after deductible (waived if admitted)
$20Copay
$250Ded.-$30Copay
Covered
Covered as any illness
Not Covered
$5,000/$10,000
$40 Copay
$250 Copay
100%
$500 Copay per day – Max 100 days per year
$50 per trip
Covered
$40 Copay
No Maximum
$500 Copay per day – after deductible
$500 Copay per day – after deductible, Acute detox only
ElectOpenAccess 40Plus
Health Net*
No Deductible
$40CopayHMO$55CopayPPO
$40 Copay
$100 Copay
$500Copayperday
$40 Copay
$250 Copay (waived if admitted)
$20Copay
$200Ded.-$30Copay
Covered
Covered as any illness
Not Covered
$3,500 Ind/$7,000 Two Party/$8,000 Fam
$40 Copay
$500 Copay
100%
60% Max 100 days per year
100%
Covered
$30 Copay
20 visits per year
$500 Copay per day – 30 Days per year
$500 Copay per day – Acute detox only

8
800.542.4218 www.calchoice.com
CC5234A.10.11
HMOMedical Benefit Notes
* Anthem Blue Cross and Health Net offer the option of an additional provider network. Those additional options are noted as: Anthem Blue Cross Select HMO and Health Net Silver HMO. Prior to enrollment, the employer may elect to offer the standard network OR these provider networks to their employees.
1 Health plans that provide hospital, medical or surgical coverage must provide coverage for the diagnosis and medically necessary treatment of severe mental illnesses of a person of any age, and serious emotional disturbances of a child, as specified, under the same terms and conditions applied to other medical conditions. These benefits will include inpatient, partial hospitalization and outpatient services and prescription drugs, if the plan includes drug coverage. The mental health benefits must be applied the same as any other medical benefit including, but not limited to, maximum lifetime benefits, copay and individual and family deductibles. “Severe mental illness” includes: schizophrenia, schizophrenic disorder, bipolar disorder (manic-depressive illness), major depressive disorders, panic disorders, obsessive-compulsive disorder, pervasive development disorder or autism, anorexia and bulimia nervosa.
2 Copayment shall be up to the designated amount, or 50% of provider’s contracted rate, whichever is less.
3 For Anthem Blue Cross - If a member selects a brand-name drug when a generic-equivalent is available, the member will be responsible for the generic copay plus the difference in cost between the brand-name drug and the generic-equivalent drug unless the physician writes “dispense as written” or “do not substitute”. The amount paid does not apply to the member’s brand-name deductible as applicable.
4 For Anthem Blue Cross - Pre-service review is required for the following mental or nervous disorders and substance abuse services: 1) Facility-based treatment or you will be required to pay a $250 copayment if pre-service review is not obtained; and 2) Outpatient professional services after twelve visits.
5 For complete information as to the mental health/substance abuse benefits and eligibility required under California and federal law, please see mental health/substance abuse benefit description provided by Plan/CHOICE Administrators® Insurance Services. Note: Certain small groups, depending on their size, may be eligible to receive mental health and substance abuse benefits in “parity” with (equivalent to) their medical benefits from Plan.
6 Salud HMO y Más benefits are shown for Salud Network. Please see Salud Application/Brochure for SIMNSA Network benefits.
7 In lieu of physical therapy visits. Must be approved by PMG/IPA.
This summary of benefits has been updated to comply with federal and state requirements, including applicable provisions of the recently enacted federal health care reform laws. As we receive additional guidance and clarification on the new health care reform laws from the U.S. Department of Health and Human Services, Department of Labor and Internal Revenue Service, we may be required to make additional changes to this summary of benefits. This summary of benefits, as updated, is subject to the approval of the California Department of Insurance and the California Department of Managed Health Care (as applicable).
800.542.4218 www.calchoice.com
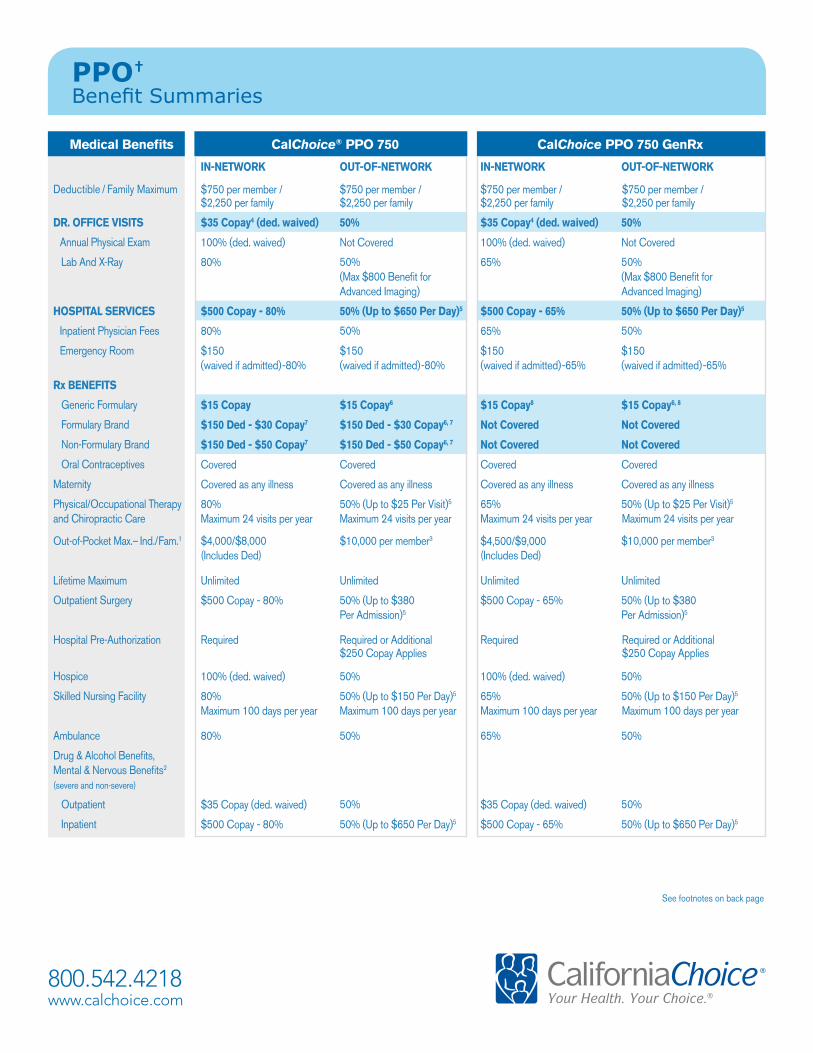
PPO† Benefit Summaries
Medical Benefits CalChoice® PPO 750 CalChoice PPO 750 GenRx
IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK
Deductible / Family Maximum $750 per member / $2,250 per family
$750 per member / $2,250 per family
$750 per member / $2,250 per family
$750 per member / $2,250 per family
DR. OFFICE VISITS $35 Copay4 (ded. waived) 50% $35 Copay4 (ded. waived) 50%
Annual Physical Exam 100% (ded. waived) Not Covered 100% (ded. waived) Not Covered
Lab And X-Ray 80% 50% 65% 50% (Max $800 Benefit for Advanced Imaging)
(Max $800 Benefit for Advanced Imaging)
HOSPITAL SERVICES $500 Copay - 80% 50% (Up to $650 Per Day)5 $500 Copay - 65% 50% (Up to $650 Per Day)5
Inpatient Physician Fees 80% 50% 65% 50%
Emergency Room $150 $150 $150 $150(waived if admitted)-80% (waived if admitted)-80% (waived if admitted)-65% (waived if admitted)-65%
Rx BENEFITS
Generic Formulary $ 15 Copay $ 15 Copay6 $ 15 Copay8 $ 15 Copay6, 8
Formulary Brand $150 Ded - $30 Copay7 $150 Ded - $30 Copay6, 7 Not Covered Not Covered
Non-Formulary Brand $150 Ded - $50 Copay7 $150 Ded - $50 Copay6, 7 Not Covered Not Covered
Oral Contraceptives Covered Covered Covered Covered
Maternity Covered as any illness Covered as any illness Covered as any illness Covered as any illness
Physical/Occupational Therapy and Chiropractic Care
80% 50% (Up to $25 Per Visit)5 65% 50% (Up to $25 Per Visit)5
Maximum 24 visits per year Maximum 24 visits per year Maximum 24 visits per year Maximum 24 visits per year
Out-of-Pocket Max.– Ind./Fam.1 $4,000/$8,000 $10,000 per member3 $4,500/$9,000 $10,000 per member3
(Includes Ded) (Includes Ded)
Lifetime Maximum Unlimited Unlimited Unlimited Unlimited
Outpatient Surgery $500 Copay - 80% 50% (Up to $380 $500 Copay - 65% 50% (Up to $380Per Admission)5 Per Admission)5
Hospital Pre-Authorization Required Required or Additional $250 Copay Applies
Required Required or Additional $250 Copay Applies
Hospice 100% (ded. waived) 50% 100% (ded. waived) 50%
Skilled Nursing Facility 80% 50% (Up to $150 Per Day)5 65% 50% (Up to $150 Per Day)5
Maximum 100 days per year Maximum 100 days per year Maximum 100 days per year Maximum 100 days per year
Ambulance 80% 50% 65% 50%
Drug & Alcohol Benefits, Mental & Nervous Benefits2
(severe and non-severe)
Outpatient $35 Copay (ded. waived) 50% $35 Copay (ded. waived) 50%
Inpatient $500 Copay - 80% 50% (Up to $650 Per Day)5 $500 Copay - 65% 50% (Up to $650 Per Day)5
See footnotes on back page
800.542.4218 www.calchoice.com
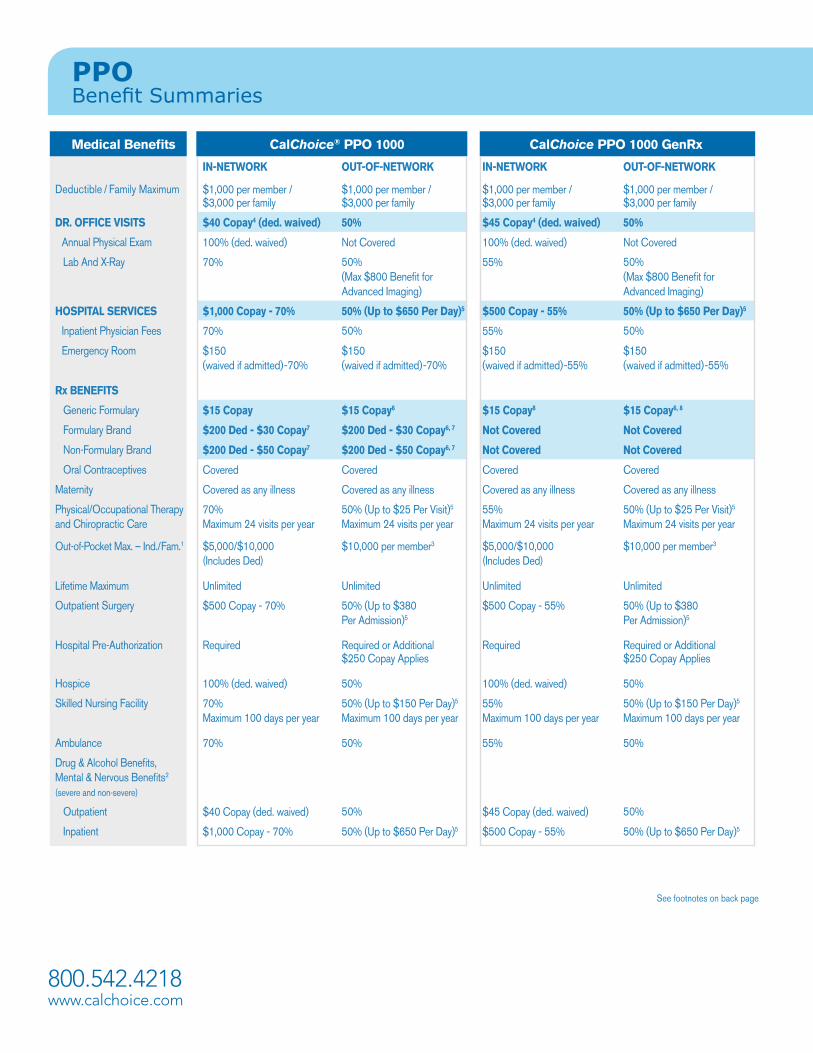
PPO Benefit Summaries
Medical Benefits CalChoice® PPO 1000 CalChoice PPO 1000 GenRx
IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK
Deductible / Family Maximum $1,000 per member / $3,000 per family
$1,000 per member / $3,000 per family
$1,000 per member / $3,000 per family
$1,000 per member / $3,000 per family
DR. OFFICE VISITS $40 Copay4 (ded. waived) 50% $45 Copay4 (ded. waived) 50%
Annual Physical Exam 100% (ded. waived) Not Covered 100% (ded. waived) Not Covered
Lab And X-Ray 70% 50% 55% 50% (Max $800 Benefit for Advanced Imaging)
(Max $800 Benefit for Advanced Imaging)
HOSPITAL SERVICES $1,000 Copay - 70% 50% (Up to $650 Per Day)5 $500 Copay - 55% 50% (Up to $650 Per Day)5
Inpatient Physician Fees 70% 50% 55% 50%
Emergency Room $150 $150 $150 $150(waived if admitted)-70% (waived if admitted)-70% (waived if admitted)-55% (waived if admitted)-55%
Rx BENEFITS
Generic Formulary $ 15 Copay $ 15 Copay6 $ 15 Copay8 $ 15 Copay6, 8
Formulary Brand $200 Ded - $30 Copay7 $200 Ded - $30 Copay6, 7 Not Covered Not Covered
Non-Formulary Brand $200 Ded - $50 Copay7 $200 Ded - $50 Copay6, 7 Not Covered Not Covered
Oral Contraceptives Covered Covered Covered Covered
Maternity Covered as any illness Covered as any illness Covered as any illness Covered as any illness
Physical/Occupational Therapy and Chiropractic Care
70% 50% (Up to $25 Per Visit)5 55% 50% (Up to $25 Per Visit)5
Maximum 24 visits per year Maximum 24 visits per year Maximum 24 visits per year Maximum 24 visits per year
Out-of-Pocket Max. – Ind./Fam.1 $5,000/$10,000 $10,000 per member3 $5,000/$10,000 $10,000 per member3
(Includes Ded) (Includes Ded)
Lifetime Maximum Unlimited Unlimited Unlimited Unlimited
Outpatient Surgery $500 Copay - 70% 50% (Up to $380 $500 Copay - 55% 50% (Up to $380Per Admission)5 Per Admission)5
Hospital Pre-Authorization Required Required or Additional $250 Copay Applies
Required Required or Additional $250 Copay Applies
Hospice 100% (ded. waived) 50% 100% (ded. waived) 50%
Skilled Nursing Facility 70% 50% (Up to $150 Per Day)5 55% 50% (Up to $150 Per Day)5
Maximum 100 days per year Maximum 100 days per year Maximum 100 days per year Maximum 100 days per year
Ambulance 70% 50% 55% 50%
Drug & Alcohol Benefits, Mental & Nervous Benefits2
(severe and non-severe)
Outpatient $40 Copay (ded. waived) 50% $45 Copay (ded. waived) 50%
Inpatient $1,000 Copay - 70% 50% (Up to $650 Per Day)5 $500 Copay - 55% 50% (Up to $650 Per Day)5
See footnotes on back page

Effective, January 1, 2012
Medical Benefits CalChoice® PPO 3000 CalChoice PPO 4000
IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK
Deductible / Family Maximum $3,000 per member / $9,000 per family
$3,000 per member / $9,000 per family
$4,000 per member / $10,000 per family
$4,000 per member / $10,000 per family
DR. OFFICE VISITS $30 Copay4 (ded. waived) 50% $40 Copay4 (ded. waived) 50%
Annual Physical Exam 100% (ded. waived) Not Covered 100% (ded. waived) Not Covered
Lab And X-Ray 70% 50% 60% 50% (Max $800 Benefit for Advanced Imaging)
(Max $800 Benefit for Advanced Imaging)
HOSPITAL SERVICES $500 Copay - 70% 50% (Up to $650 Per Day)5 $500 Copay - 60% 50% (Up to $650 Per Day)5
Inpatient Physician Fees 70% 50% 60% 50%
Emergency Room $150 $150 $150 $150(waived if admitted)-70% (waived if admitted)-70% (waived if admitted)-60% (waived if admitted)-60%
Rx BENEFITS
Generic Formulary $ 15 Copay $ 15 Copay6 $ 15 Copay $ 15 Copay6
Formulary Brand $250 Ded - $30 Copay7 $250 Ded - $30 Copay6, 7 $250 Ded - $30 Copay7 $250 Ded - $30 Copay6, 7
Non-Formulary Brand $250 Ded - $50 Copay7 $250 Ded - $50 Copay6, 7 $250 Ded - $50 Copay7 $250 Ded - $50 Copay6, 7
Oral Contraceptives Covered Covered Covered Covered
Maternity Covered as any illness Covered as any illness Covered as any illness Covered as any illness
Physical/Occupational Therapy and Chiropractic Care
70% 50% (Up to $25 Per Visit)5 60% 50% (Up to $25 Per Visit)5
Maximum 24 visits per year Maximum 24 visits per year Maximum 24 visits per year Maximum 24 visits per year
Out-of-Pocket Max. – Ind./Fam.1 $7,000/$14,000 $10,000 per member3 $7,000/$14,000 $10,000 per member3
(Includes Ded) (Includes Ded)
Lifetime Maximum Unlimited Unlimited Unlimited Unlimited
Outpatient Surgery $500 Copay - 70% 50% (Up to $380 $500 Copay - 60% 50% (Up to $380Per Admission)5 Per Admission)5
Hospital Pre-Authorization Required Required or Additional $250 Copay Applies
Required Required or Additional $250 Copay Applies
Hospice 100% (ded. waived) 50% 100% (ded. waived) 50%
Skilled Nursing Facility 70% 50% (Up to $150 Per Day)5 60% 50% (Up to $150 Per Day)5
Maximum 100 days per year Maximum 100 days per year Maximum 100 days per year Maximum 100 days per year
Ambulance 70% 50% 60% 50%
Drug & Alcohol Benefits, Mental & Nervous Benefits2
(severe and non-severe)
Outpatient $30 Copay (ded. waived) 50% $40 Copay (ded. waived) 50%
Inpatient $500 Copay - 70% 50% (Up to $650 Per Day)5 $500 Copay - 60% 50% (Up to $650 Per Day)5
See footnotes on back page
Note: For non-emergency care, out-of-network reimbursement amount is based on: an Anthem Blue Cross rate or fee schedule, a rate negotiated with the provider, information from a third party vendor, or billed charges. Members are responsible for the difference between the provider’s usual charges & the maximum allowed amount. Non-participating hospitals are covered at a reduced benefit but there are no benefits for care in non-contracting hospitals, except for medical emergencies. For medical emergency care rendered by a non-participating provider or non-contracting hospital, reimbursement is based on the reasonable and customary value. Members may be responsible for any amount in excess of the reasonable and customary value. Plans exclude coverage for pre-existing conditions (except for members under age 19, a child acquired through legal guardianship if the child is added within 31 days of final court decree or order, a child born to or newly adopted by an enrolled subscriber or spouse, or conditions of pregnancy) for the first six months of coverage unless replacing prior creditable coverage.
PPO† Medical Benefit Notes
† These plans are offered by Anthem Blue Cross Life and Health Insurance Company.
This summary of benefits has been updated to comply with federal and state requirements, including applicable provisions of the recently enacted federal health care reform laws. As we receive additional guidance and clarification on the new health care reform laws from the U.S. Department of Health and Human Services, Department of Labor and Internal Revenue Service, we may be required to make additional changes to this summary of benefits. This summary of benefits, as updated, is subject to the approval of the California Department of Insurance and the California Department of Managed Health Care (as applicable).
Please refer to the CaliforniaChoice® Program brochure for more detailed plan benefit information.
CC5234B.12.11
800.542.4218 www.calchoice.com
1 The following do not apply to the out-of-pocket maximum: inpatient, outpatient and ambulatory surgical facility copays, applicable pharmacy deductibles and copays for pharmacy benefits, copays for acupuncture/acupressure, copays for not obtaining pre-service review; infertility copay; and non-covered expenses. After a member reaches the out-of-pocket maximum in a calendar year, the member will no longer be required to pay a copay for the remainder of that year, except as stated in the Certificate. The insured remains responsible for these amounts even after the out-of-pocket maximum has been met.
2 Pre-service review is required for the following mental or nervous disorders and substance abuse services; 1) Facility-based treatment or you will be required to pay a $250 copayment if pre-service review is not obtained for non-participating providers; and 2) Outpatient professional services after twelve visits.
3 Once Anthem Blue Cross payments reach $10,000 per insured, the insured pays nothing for covered expenses for the remainder of the year.4 The dollar copay applies only to the visit itself. An additional copay applies for any services performed in office (i.e., x-ray, lab, surgery), after
any applicable deductible.5 The coverage amount listed is the maximum allowed charge for non-emergency services received from a non-participating hospital or
non-participating provider. Members are responsible for all charges in excess of the covered amount. Physician Services are covered separately at 50% of Allowable Amounts.
6 Benefits apply to prescriptions filled at participating pharmacies. Please see Health Plan & Formulary Comparison Guide for non-participating pharmacy benefits.
7 If a member selects a brand-name drug when a generic-equivalent is available, even if the physician writes a “dispense as written” or “do not substitute”, the member will be responsible for the generic copay plus the difference in cost between the brand-name drug and the generic equivalent drug. The amount paid does not apply to the member’s pharmacy deductible, if applicable.
8 This prescription drug plan includes coverage for drugs on the GenRx Prescription Drug Formulary only.
See footnotes on back page
800.542.4218 www.calchoice.com
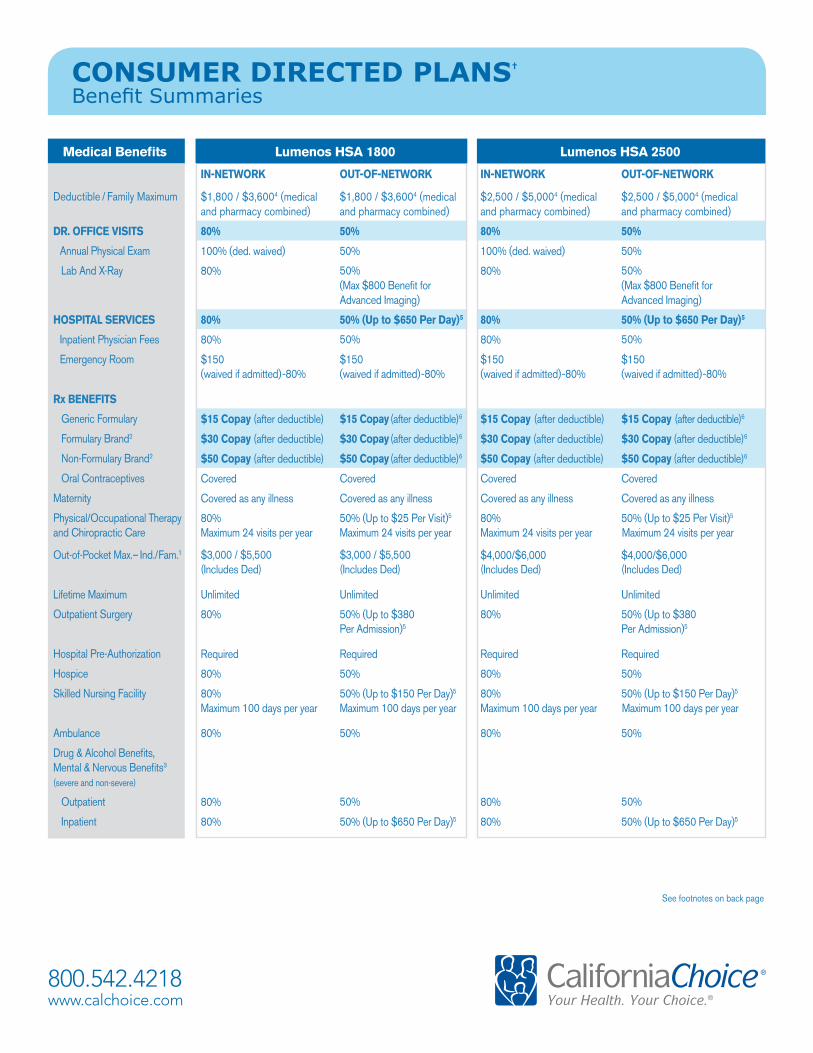
CONSUMER DIRECTED PLANS†
Benefit Summaries
Medical Benefits Lumenos HSA 1800 Lumenos HSA 2500
IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK
Deductible / Family Maximum $1,800 / $3,6004 (medical and pharmacy combined)
$1,800 / $3,6004 (medical and pharmacy combined)
$2,500 / $5,0004 (medical and pharmacy combined)
$2,500 / $5,0004 (medical and pharmacy combined)
DR. OFFICE VISITS 80% 50% 80% 50%
Annual Physical Exam 100% (ded. waived) 50% 100% (ded. waived) 50%
Lab And X-Ray 80% 50% 80% 50% (Max $800 Benefit for Advanced Imaging)
(Max $800 Benefit for Advanced Imaging)
HOSPITAL SERVICES 80% 50% (Up to $650 Per Day)5 80% 50% (Up to $650 Per Day)5
Inpatient Physician Fees 80% 50% 80% 50%
Emergency Room $150 $150 $150 $150(waived if admitted)-80% (waived if admitted)-80% (waived if admitted)-80% (waived if admitted)-80%
Rx BENEFITS
Generic Formulary $ 15 Copay (after deductible) $ 15 Copay (after deductible)6 $ 15 Copay (after deductible) $ 15 Copay (after deductible)6
Formulary Brand2 $30 Copay (after deductible) $30 Copay (after deductible)6 $30 Copay (after deductible) $30 Copay (after deductible)6
Non-Formulary Brand2 $50 Copay (after deductible) $50 Copay (after deductible)6 $50 Copay (after deductible) $50 Copay (after deductible)6
Oral Contraceptives Covered Covered Covered Covered
Maternity Covered as any illness Covered as any illness Covered as any illness Covered as any illness
Physical/Occupational Therapy and Chiropractic Care
80% 50% (Up to $25 Per Visit)5 80% 50% (Up to $25 Per Visit)5
Maximum 24 visits per year Maximum 24 visits per year Maximum 24 visits per year Maximum 24 visits per year
Out-of-Pocket Max.– Ind./Fam.1 $3,000 / $5,500 $3,000 / $5,500 $4,000/$6,000 $4,000/$6,000(Includes Ded) (Includes Ded) (Includes Ded) (Includes Ded)
Lifetime Maximum Unlimited Unlimited Unlimited Unlimited
Outpatient Surgery 80% 50% (Up to $380 80% 50% (Up to $380Per Admission)5 Per Admission)5
Hospital Pre-Authorization Required Required Required Required
Hospice 80% 50% 80% 50%
Skilled Nursing Facility 80% 50% (Up to $150 Per Day)5 80% 50% (Up to $150 Per Day)5
Maximum 100 days per year Maximum 100 days per year Maximum 100 days per year Maximum 100 days per year
Ambulance 80% 50% 80% 50%
Drug & Alcohol Benefits, Mental & Nervous Benefits3
(severe and non-severe)
Outpatient 80% 50% 80% 50%
Inpatient 80% 50% (Up to $650 Per Day)5 80% 50% (Up to $650 Per Day)5

800.542.4218 www.calchoice.comCC5234C.09.11
CONSUMER DIRECTED PLANSBenefit Summaries
Note: Fornon-emergencycare,out-of-networkreimbursementamountisbasedon:anAnthemBlueCrossrateorfeeschedule,aratenegotiatedwiththeprovider,informationfromathirdpartyvendor,orbilledcharges.Membersareresponsibleforthedifferencebetweentheprovider’susualcharges&themaximumallowedamount.Non-participatinghospitalsarecoveredatareducedbenefitbuttherearenobenefitsforcareinnon-contractinghospitals,exceptformedicalemergencies.Formedicalemergencycarerenderedbyanon-participatingproviderornon-contractinghospital,reimbursementisbasedonthereasonableandcustomaryvalue.Membersmayberesponsibleforanyamountinexcessofthereasonableandcustomaryvalue.Plansexcludecoverageforpre-existingconditions(exceptformembersunderage19,achildacquiredthroughlegalguardianshipifthechildisaddedwithin31daysoffinalcourtdecreeororder,achildborntoornewlyadoptedbyanenrolledsubscriberorspouse,orconditionsofpregnancy)forthefirstsixmonthsofcoverageunlessreplacingpriorcreditablecoverage.
† These plans are offered by Anthem Blue Cross Life and Health Insurance Company
1 The following do not apply to the out of pocket maximum: charges paid for acupuncture/acupressure by non-participating providers and non-covered expenses. The insured remains responsible for these amounts even after the out of pocket maximum has been met. In-network and out-of-network out-of-pocket maximums are exclusive of each other; includes calendar year deductible & prescription drug covered expense.
2 If a member selects a brand-name drug when a generic-equivalent is available, even if the physician writes a “dispense as written” or “do not substitute”, the member will be responsible for the generic copay plus the difference in cost between the brand-name drug and the generic-equivalent drug.
3 Pre-service review is required for the following mental or nervous disorders and substance abuse services: 1) Facility-based treatment; and 2) Outpatient professional services after twelve visits.
4 Employees enrolling for single coverage must satisfy the single deductible; for employees enrolling with Dependent coverage, the family deductible must be met before any member receives benefits. In-network and out-of-network deductibles are exclusive of each other; they are applicable to medical care & prescription drug benefits.
5 The coverage amount listed is the maximum allowed charge for non-emergency services received from a Non-Participating Hospital or Non-Participating Provider. Members are responsible for all charges in excess of the covered amount. Physician Services are covered separately at 50% of Allowable Amounts.
6 Benefits apply to prescriptions filled at participating pharmacies. Please see Health Plan & Formulary Comparison Guide for non-participating pharmacy benefits.
This summary of benefits has been updated to comply with federal and state requirements, including applicable provisions of the recently enacted federal health care reform laws. As we receive additional guidance and clarification on the new health care reform laws from the U.S. Department of Health and Human Services, Department of Labor and Internal Revenue Service, we may be required to make additional changes to this summary of benefits. This summary of benefits, as updated, is subject to the approval of the California Department of Insurance and the California Department of Managed Health Care (as applicable).
Please refer to the CaliforniaChoice® Program brochure for more detailed plan benefit information.
800.542.4218 www.calchoice.com
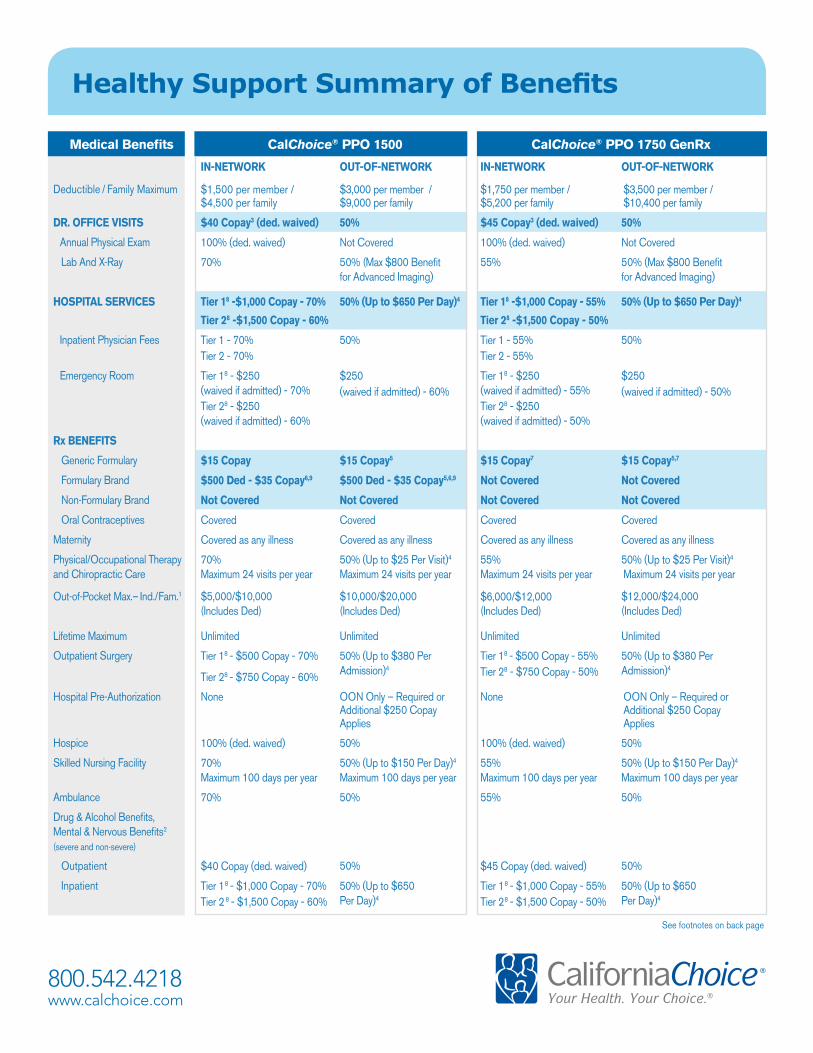
Healthy Support Summary of Benefits
Medical Benefits CalChoice® PPO 1500 CalChoice® PPO 1750 GenRx
IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK
Deductible / Family Maximum $1,500 per member / $4,500 per family
$3,000 per member / $9,000 per family
$1,750 per member / $5,200 per family
$3,500 per member / $10,400 per family
DR. OFFICE VISITS $40 Copay3 (ded. waived) 50% $45 Copay3 (ded. waived) 50%
Annual Physical Exam 100% (ded. waived) Not Covered 100% (ded. waived) Not Covered
Lab And X-Ray 70% 50% (Max $800 Benefit 55% 50% (Max $800 Benefitfor Advanced Imaging) for Advanced Imaging)
HOSPITAL SERVICES Tier 18 -$1,000 Copay - 70%
Tier 28 -$1,500 Copay - 60%
50% (Up to $650 Per Day)4 Tier 18 -$1,000 Copay - 55%
Tier 28 -$1,500 Copay - 50%
50% (Up to $650 Per Day)4
Inpatient Physician Fees Tier 1 - 70%Tier 2 - 70%
50% Tier 1 - 55%Tier 2 - 55%
50%
Emergency Room Tier 18 - $250 (waived if admitted) - 70%
$250(waived if admitted) - 60%
Tier 18 - $250 (waived if admitted) - 55%
$250 (waived if admitted) - 50%
Tier 28 - $250 (waived if admitted) - 60%
Tier 28 - $250 (waived if admitted) - 50%
Rx BENEFITS
Generic Formulary $ 15 Copay $ 15 Copay5 $ 15 Copay7 $ 15 Copay5,7
Formulary Brand $500 Ded - $35 Copay6,9 $500 Ded - $35 Copay5,6,9 Not Covered Not Covered
Non-Formulary Brand Not Covered Not Covered Not Covered Not Covered
Oral Contraceptives Covered Covered Covered Covered
Maternity Covered as any illness Covered as any illness Covered as any illness Covered as any illness
Physical/Occupational Therapy and Chiropractic Care
70% 50% (Up to $25 Per Visit)4 55% 50% (Up to $25 Per Visit)4
Maximum 24 visits per year Maximum 24 visits per year Maximum 24 visits per year Maximum 24 visits per year
Out-of-Pocket Max.– Ind./Fam.1 $5,000/$10,000 $10,000/$20,000 $6,000/$12,000 $12,000/$24,000(Includes Ded) (Includes Ded) (Includes Ded) (Includes Ded)
Lifetime Maximum Unlimited Unlimited Unlimited Unlimited
Outpatient Surgery Tier 18 - $500 Copay - 70%
Tier 28 - $750 Copay - 60%
50% (Up to $380 Per Admission)4
Tier 18 - $500 Copay - 55%Tier 28 - $750 Copay - 50%
50% (Up to $380 Per Admission)4
Hospital Pre-Authorization None OON Only – Required or Additional $250 Copay Applies
None OON Only – Required or Additional $250 Copay Applies
Hospice 100% (ded. waived) 50% 100% (ded. waived) 50%
Skilled Nursing Facility 70% Maximum 100 days per year
50% (Up to $150 Per Day)4
Maximum 100 days per year55% Maximum 100 days per year
50% (Up to $150 Per Day)4
Maximum 100 days per year
Ambulance 70% 50% 55% 50%
Drug & Alcohol Benefits, Mental & Nervous Benefits2
(severe and non-severe)
Outpatient $40 Copay (ded. waived) 50% $45 Copay (ded. waived) 50%
Inpatient Tier 1 8 - $1,000 Copay - 70%Tier 28 - $1,500 Copay - 60%
50% (Up to $650 Per Day)4
Tier 1 8 - $1,000 Copay - 55%Tier 28 - $1,500 Copay - 50%
50% (Up to $650 Per Day)4
See footnotes on back page
Note: For non-emergency care, out-of-network reimbursement amount is based on: an Anthem Blue Cross rate or fee schedule, a rate negotiated with the provider, information from a third party vendor, or billed charges. Members are responsible for the difference between the provider’s usual charges & the maximum allowed amount. Non-participating hospitals are covered at a reduced benefit. For medical emergency care rendered by a non-participating provider or non-contracting hospital, reimbursement is based on the reasonable and customary value. Members may be responsible for any amount in excess of the reasonable and customary value. Plans exclude coverage for pre-existing conditions (except for members under age 19, a child acquired through legal guardianship if the child is added within 31 days of final court decree or order, a child born to or newly adopted by an enrolled subscriber or spouse, or conditions of pregnancy) for the first six months of coverage unless replacing prior creditable coverage.
Healthy Support Summary of Benefits
Please refer to the CaliforniaChoice® Program brochure for more detailed plan benefit information.
CC5234D.5.12
800.542.4218 www.calchoice.com
1 The following do not apply to the out-of-pocket maximum: inpatient, outpatient and ambulatory surgical facility copays, applicable pharmacy deductibles and copays for pharmacy benefits, copays for acupuncture/acupressure, copays for not obtaining pre-service review; infertility copay; and non-covered expenses. After a member reaches the out-of-pocket maximum in a calendar year, the member will no longer be required to pay a copay for the remainder of that year, except as stated in the Certificate. The insured remains responsible for these amounts even after the out-of-pocket maximum has been met.
2 Pre-service review is required for the following mental or nervous disorders and substance abuse services; 1) Facility-based treatment (non-participating providers) or you will be required to pay a $250 copayment if pre-service review is not obtained; and 2) Outpatient professional services after twelve visits.
3 The dollar copay applies only to the visit itself. An additional copay applies for any services performed in office (i.e., x-ray, lab, surgery), after any applicable deductible.
4 The coverage amount listed is the maximum allowed charge for non-emergency services received from a non-participating hospital or non-participating provider. Members are responsible for all charges in excess of the covered amount. Physician Services are covered separately at 50% of Allowable Amounts.
5 Benefits apply to prescriptions filled at participating pharmacies. Please see Health Plan & Formulary Comparison Guide for non-participating pharmacy benefits.
6 If a member selects a brand-name drug when a generic-equivalent is available, even if the physician writes a “dispense as written” or “do not substitute”, the member will be responsible for the generic copay plus the difference in cost between the brand-name drug and the generic equivalent drug. The amount paid does not apply to the member’s pharmacy deductible, if applicable.
7 This prescription drug plan includes coverage for drugs on the GenRx Prescription Drug Formulary only.8 The hospital you choose will determine the benefit level payable under the plan. By choosing a Tier 1 Preferred Participating Hospital, you will
receive the highest level of benefits available under this plan. To view the Tier level of the participating hospitals go to www.calchoice.com and click on the Provider/Rx Search link.
9 This prescription drug plan includes coverage for drugs on the Generic Premium Prescription Drug Formulary only.





























