Embed Size (px)
Citation preview

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 1/40

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 2/40
Funding the fight againstHIV/AIDS
A comparative report
of four African studies:Kenya, Mozambique, Namibia and South Africa

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 3/40
This report is part of a project carried out by African and Latin American organizations and
financed by the Swedish International Development Cooperation Agency. Please contact Idasa at
[email protected] for the African country studies and Fundar at finanzaspub [email protected] the Latin American country studies.
Editors: Teresa Guthrie and Alison Hickey
Design: Deikon.
Printed by: Mono comunicación, S.A. de C.V.
Octob er 2004, Fundar Centro de Análisis e InvestigaciónPopot la 96 5; Tizapán San Ángel; México, D.F.
Printed in Mexico

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 4/40
Funding t he fi ght against HIV/AIDS
A comparative report of four African studies:Kenya, Mozambique, Namibia and South Africa
Introduction ...................................................................................................................5
1. The Socioeconomic Environment ...................................................................................5
2. The Magnit ude of the HIV/AIDS Epidemic ....................................................................7
3. National Responses to HIV/AIDS...................................................................................8
3.1 Political Commitment
3.2 National Coordinating Structures
3.3 Tackling HIV/AIDS as a Development Issue
3.4 National HIV/AIDS Plans and Programmes
4. Reliance on Donor Aid .................................................................................................12
5. Funding and Budget Cont rol Mechanisms Used for HIV/AIDS Programmes..................13
6. Allocations Made to Public Health...............................................................................14
6.1 Public Health Allocations as a Share of GDP and Total Expenditure
6.2 Per Capita Public Health Allocations
7. Allocations Made to HIV/AIDS Programmes................................................................18
7.1 HIV/AIDS Nominal and Real Allocations
7.2 HIV/AIDS Allocationsas a Share of Total Expenditure and of Total Health Expenditure
7.3 HIV/AIDS Per Capita Al locations
8. Changing Priorit ies - Changing Types of Activit ies ......................................................26
9. Effi ciency and Equity in HIV/AIDS Spend ings ..............................................................29

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 5/40
4
10. Africa Regional Recomendations .................................................................................32
10.1 Policy Implications
10.2 Mainstreaming HIV/AIDS as a Development Issue
10.3 Institut ional Implications
10.4 Resource Implications
10.5 Funding and Budget Control Mechanisms
10.6 Coordinating Donor Funds
10.7 Monitoring Issues of Equity and Human Rights Promotion
References..........................................................................................................................37

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 6/40
5
Introduction
The African countries included in this study, Kenya, Mozambique, South Africa and Namibia,
presented differing scenarios in terms of socioeconomic indicators, HIV prevalence rates and
government response. All these factors, and many others, are intertwined and influence one other.
Thus an understanding of a government’s political commitment to the issue of HIV/AIDS is essential
when considering the policies and structures set in place to respond to the epidemic. These in turn
influence the amounts allocated and the funding mechanisms used to distribute funds. The degree
of reliance on donor funds to sustain national HIV/AIDS programmes is also a critical issue: the
fluctuating nature of donor funds can undermine a state’s ability t o determine and coordinate its own
response and to plan effectively over a medium-term expenditure period.
With escalating prevalence rates, increasing poverty and declining development in sub-Saharan
Africa, the pandemic has been identified as a development issue, and thus governments and donors
have been allocating increasing funds to the fight against it. These studies examine the trends in
real terms and consider the intervention priorities. However, it was beyond the scope of the research
to analyse the sufficiency of allocations, based on cost and needs analyses, or of the outcome and
impact of allocations.
This report gives an overview and comparison of the key issues as they relate to the four African
countries included here.
1. The Socioeconomic Environment
A ll four countries suffer, to varying degrees, from underdevelopment and socioeconomic
problems, such as slow or fluctuating economic growth, rising unemployment, increasing poverty andinequality, and generally limited state resources.
Table 1.1 sets out a few key socioeconomic and human development indicators in each country.
According to the human development index (HDI), South Africa is the highest ranked at 111th,
followed by Namibia at 124th, Kenya at 146th and Mozambique at 170th. The impact of HIV/AIDS has
been felt in declining life expectancy, causing countries to drop in their HDI ranking (UNDP, 2003).

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 7/40
6
Sources: World Bank, 2004. UNDP, 2003* The poverty rate given by the UNDP (2003) for South Africa is far lower than the in-country income and expendituresurveys show. Various analysts have indicated poverty levels around 50%, depending on the poverty line used (e.g.
Committee of Inquiry, 2002).
TABLE 1.1: Socioeconimic and d evelopment indicators
Indicator
Population density (peopleper km2) (World Bank, 2004)
Human development index(UNDP, 2003)
Human development rank(UNDP, 2003)
Life expentancy (yrs)(UNDP, 2003)
Adult literacy rate (%)(UNDP, 2003)
GDP per capit a (US$ PPP)(UNDP,2003)
GDP per capit a (US$)(UNDP,2003)
GDP per capita % grow th,2001-2002 (World Bank, 2004)
Human povert y index (%)(UNDP, 2003)
Population living below $2per day (%) (UNDP,2003)
Gini coefficient (UNDP, 2003)
Maternal mortalit y (per100,000) (UNDP, 2003)
Infant mor talit y (per 100,000live births) (UNDP, 2003)
Under-five mortality rate (per1000 live births) (UNDP, 2003)
36 ('02)
0.684 ('01)
111 ('01)
50.9 ('01)
85.6 ('01)
11.290 ('01)
2.620 ('01)
2.2
31.7 ('01)*
14.5 ('01)
0.59
340 ('95)
56 ('01)
71 ('01)
S. Af rica
2 ('02)
0.627 ('01)
124 ('01)
47.4 ('01)
82.7 ('01)
7.120 ('01)
1.730 ('01)
1.2
37.8 ('01)
55.8 ('01)
0.71
370 ('95)
55 ('01)
67 ('01)
Namibia
55 ('02)
0.489 ('01)
146 ('01)
46.4 ('01)
83.3 ('01)
980 ('01)
371 ('01)
-0.2
37.8 ('01)
58.6 ('01)
0.45
1300 ('95)
78 ('01)
122 ('01)
Kenya
24 ('02)
0.356 ('01)
170 ('01)
39.2 ('01)
45.2 ('01)
1.140 ('01)
200 ('01)
7.7
50.3 ('01)
78.4 ('01)
0.40
980 ('95)
125 ('01)
197 ('01)
Mozambique

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 8/40
7
HIV/AIDS has exacerbated the experience of poverty and hardship within households and
communities in these countries, causing declining life expectancies and decreasing household incomes.
The increasing numbers of orphans and vulnerable children have added to the burden of already
struggling households. The care of these children often falls on grandmothers and communities, and
increasingly on the state. Let us consider briefly the magnitude and scope of the HIV/AIDS problem in
each of the countries, as this relates to the sufficiency of allocated resources.
2. The Magnitude of t he HIV/AIDS Epidemic
Sub-Saharan Africa is the region that has been worst hit by the HIV/AIDS pandemic, with between25 million and 28 million people living with HIV/AIDS and an adult prevalence rate of between 7.5%
and 8.5% by the end of 2003, according to UNAIDS (2002).
Sources: UNAIDS, 2004
Sources: UNAIDS, 2004
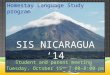
Figure 2.1: HIV prevalence among adults,ages 15-49, as at the end of 2003 Percentage
25
20
15
10
5
0
South Africa Namibia Kenya Mozambique
Percentage
TABLE 2.1: HIV/AIDS prevalence in the four African countriesas at the end of 2003 (UNAIDS, 2004)
Indicator - as at end 2003
Prevalence among adults(15-49 years)
Estimated number of personsliving with HIV
Estimated number of AIDS
deaths
21.5 %
5,300,000
370,000
S. Af rica
21.3 %
210,000
16,000
Namibia
6.7%
1,200,000
150,000
Kenya
12.2 %
1,300,000
110,000
Mozambique

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 9/40
8
In the African countries included in this study, drastic increases in prevalence rates were evident
in the 1990s. In Kenya, however, there was a gradual decline from 13.5% in 2000 to 10.2% in 2002
among adults (aged 15-49) (MoH, 2002). The recent estimates from the Kenyan Demographic and
Health Survey in 2003 found that the prevalence rate had dropped further to 6.7% (MoPND, 2003).
These decreases are indeed welcome. Mozambique’s adult (15-49 years) prevalence rate in 2002
was found to be 13.6% (Multisectorial Technical Group, 2003). In South Africa, 14.2% of the total
populat ion, and 24% of adults (15-49 years), were estimated to be infected with HIV in 2002, based on
the Antenatal Clinic Survey (Dorrington et al., 2002). The highest HIV/AIDS prevalence rates are found
in Namibia, with 23.3% of the to tal population found to be infected in 2002 (MoHSS, 2002).
HIV prevalence rates vary between provinces or regions within countries. The most notable
example in this study was Namibia, where the HIV prevalence among pregnant women varied
between 9% (Kunene Region in the north-west) and 43% (Caprivi Region, in the north-east). The
high rates in Caprivi could be related t o its being on a transport route with great human mobility
(via the Trans-Caprivi), and possibly due to an increased number o f defence forces (in 1999/2000)
along the Angolan/Namibian border. The evidence from all the African countries confirms that
females are more vulnerable to infection than males.
It is predicted that the effects of HIV/AIDS will have a negative impact on economic developmentin these countries. Per capita GDP will fall due to reduced productivity, reduced population growth,
reduced human capital accumulation and reduced physical capital accumulation (World Bank, 2003). It
is therefore imperative that national governments and the international community commit adequate
resources to mitigating the impact of HIV/AIDS on countries.
3. National Responses to HIV/AIDS
“ For the most part governments have been extremely slow to react to the potential impacts of
the epidemic,” note Barnett and Whiteside (2002:297). The African countries included in this study
displayed d iffering levels of polit ical commitment to the HIV/AIDS issue, and this was clearly reflected
in their policies and programmes, as well as in the power and authority given to the national AIDS
co-ordinating bodies. The location of these bodies also affected their effectiveness and scope of
influence. Another factor influencing response was whether governments viewed HIV/AIDS as a
development issue or purely as a public health problem, requiring a health-dominated response.

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 10/40
9
3.1 Political Commit ment
Best pract ice example - Polit ical Commitment
In Kenya, as early as the 1980s, HIV/AIDS was recognised as a development issue, rather than
merely a public health problem. In 1999, the Kenyan president declared HIV/AIDS a national
disaster and established the National AIDS Control Council (NACC). The NACC falls directly
under the Office of the President and has the authority to determine budgets and hold all
departments accountable in their HIV/AIDS activities. It also has district-level structures which
receive allocated funds for their HIV/AIDS activities. The NACC thus tracks all funding flows at
all levels of government, down to district level.
The government of South Africa was somewhat slower in acknowledging the scope of the
problem of HIV/AIDS and in committing its efforts to lessening the impact. Comparing South Africa’s
socioeconomic status to that of the other countries included in this study leads one to assume that
South Africa is best placed, in terms of financial resources and infrastructural capacity, to develop a
comprehensive response, which would include the provision of antiretroviral (ARV) treatment. The
cabinet finally approved ARV treatment in November 2003 – after extensive pressure from civil society
movements, primarily organised by the Treatment Action Campaign (TAC).
“ The most extreme manifestation of government ’s inabilit y to respond has been in South Africa.
President Thabo Mbeki appeared transfixed by the looming catastrophe...There was consensus that
this [dissident ] debate was confusing and damaging to South Africa’s response to AIDS” (Barnett and
Whiteside, 2002:297-298).
3.2 Nat ional Coordinating St ructures
The existence of a national coordinating body, and its position and power, reflect the degree ofseriousness of the state’s response. It is important to note that all the African countries in the study
had national coordinating bodies, although their roles, responsibilities and authority varied.
Best Practice Example - National Coord inating St ructures
In Mozambique, the National AIDS Council (NAC) is chaired by the Prime Minister and includes
all the relevant sectors. This high-powered body coordinates the multisectoral response, since
HIV/AIDS was recognised early as a development issue. These structures are replicated at
provincial level and at district level, where they incorporate representatives of civil society and
service provides, such as NGOs.

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 11/40
10
Soon after Namibia gained independence in 1990, the President launched the National AIDS
Control Programme (NACP), located within the Ministry of Health and Social Services and mandated
to coordinate patient care and preventative activities. Where the national coordinating body is
located within a country’s health ministry, its coordination of the HIV/AIDS activities in all the other
sectors becomes more difficult to ensure. Similarly, regional AIDS coordinators operating within
regional departments of health find it difficult to coordinate the HIV/AIDS activities of the other
departments, resulting in a health-dominated and fragmented response.
The South African National AIDS Council (SANAC) was formed in 2002 to combine government
and civil society efforts in fighting the HIV/AIDS epidemic. The sectors represented in the executive
management committee include health, labour, agriculture, transport, defence, government, women,youth, traditional healers, traditional leaders, the hospitality sector and people living with HIV/AIDS.
Although officially located in the Office of the Deputy President, SANAC has its secretariat within the
Department of Health (DoH), which limits its multisectoral coordination somewhat. SANAC has been
criticised for ineffectiveness and for excluding representatives of civil society. In November 2003,
SANAC was restructured with increased representation from additional sectors.
3.3 Tackling HIV/AIDS as a Development Issue
Most national responses reflect a shift from viewing and addressing HIV/AIDS as a health problem
to treating it as a development issue. This is reflected in a more mul t isectoral response, which requires
good coordination and commitment among sectors and ministries.
As early as 1985, the Kenyan government realised that the Ministry of Health alone could not
respond adequately to the HIV/AIDS situation, and thus initiated the development of a comprehensive
and intersectoral plan.
Until 1999, the Mozambican government viewed HIV/AIDS as primarily a health p roblem. It then
developed a Nation al Strategic Plan which emphasised a multisectoral approach. Unfortunately,
Mozambique has been negatively affected by years of civil war and by natural disasters such as
floods, which have decreased the resources available for HIV/AIDS. Nevertheless, HIV/AIDS is viewed
as a development issue, and is now included in development policies and efforts.
Similarly, HIV/AIDS is located as a critical issue in Namibia’s National Development Plan and is
central to the country’s Vision 2030. However, the NACP falls under the Ministry of Health and Social
Services (MoHSS), which therefore del ivers most of the government ’s HIV/AIDS programmes.

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 12/40

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 13/40
12
• Treatment: initially primarily treatment of sexually transmitted infections (STIs) and opportunistic
infections (OIs) and more recently the provision of ARVs;
• Mitigation of the socioeconomic impact of AIDS, for instance by providing social assistance and
other benefits, food parcels, etc;
• Monitoring and evaluation (sometimes including research); and
• Management and coordination.
With regard to ARV treatment, South Africa and Namibia announced in 2003 their intention to
provide free ARV treatment to public patients and in 2004, Mozambique and Kenya announced
their intentions. Namibia has reportedly already commenced distribution of the drugs to public
hospitals, while, at the t ime of writing, South Africa was lagging in implementation due to delays inthe accreditation1 and tender processes2, as well as other factors. Civil society has heavily criticised
the South Africa DoH for delaying the rollout o f the ARV programme.
4. Reliance on Donor A id
Our ability to include an analysis of donor aid was determined by the availability of a centralised
system of tracking or recording all donor funds coming into each country. The Kenyan National AIDSControl Council (NACC) had a detailed t racking mechanism, while South Africa did not have any such
system or database. The four countries relied on donor aid to differing degrees. Unlike the other
countries, the South African response to HIV/AIDS was primarily funded from state revenue, with some
additional donor funds. In comparison, the majority of the Mozambican response was funded by donor
aid. In 2002, for example, 62% of the health budget was funded by international aid (MISAU-DPC,
2003). Such heavy reliance on donor funds, which tend to fluctuate, influences the sustainability of
programmes and the state’s ability to plan its medium-term expenditure framework (MTEF) effectively.
Table 4.1 provides the donor-aid reliance indicators used in the World Development Report.
Source: World Bank, 2004:261.
TABLE 4.1: Country reliance on donor aid (2001)
Indicator
Aid per capita (US$)
Aid as % of GNI
Aid as % of government expedit ure
10.0
0.4
1.3
S. Af rica
61.0
3.4
12.3
Namibia
15.0
4.0
no data
Kenya
52.0
28.2
no data
Mozambique
1 Sites for distribution had to be screened and approved before provision could begin.2 The state followed a protracted tender procedure for purchasing drugs.

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 14/40
13
It is imperative that governments have some system for recording and coordinating donor aid
entering a country, in particular for HIV/AIDS activities. Donors could assist this process by reporting
on any of their funding which might not be channelled through the government. The development
budget system used by Namibia (described below) allows for some tracking of the donor aid to the
country.
5. Funding and Budget Control Mechanisms Used for HIV/AIDS Programmes
Funding sources and budget control systems for HIV/AIDS programmes varied from country to
country. The Namibian National Development Plan (NDP) pays specific attent ion to mainstreamingHIV/AIDS activities, sets targets and performance indicators and provides cost estimates for each
programme within each ministry. In theory the NDP was intended to guide ministries’ HIV/AIDS
plans and budgets, but in practice this does not happen to any large degree. The National Planning
Commission (NPC) prepares the three-year rolling development budget, which allocates donor
funds, either inside or outside the State Revenue Fund (SRF), and includes a sector classification
dedicated to HIV/AIDS. The Namibian country report was therefore able to present the donor
allocations going to the HIV/AIDS sector through the development budget. However, the
recurrent budget (primarily state revenue funded) does not have specific line it ems for HIV/AIDSprogrammes, which makes it d ifficult to capture all the state HIV/AIDS expenditure. While other
ministries implement HIV/AIDS programmes, their recurrent and development budgets do not
have sufficiently d isaggregated data to provide info rmation on the amounts allocated and spent
by those ministries on HIV/AIDS.
Kenya has proposed a new coordination and funding framework for the activities of the NACC,
which will use two key funding streams. The allocation for the NACC will flow directly from the
Office of the President. After retaining a proportion for its coordinating functions, the NACC willchannel the funds in two directions: some directly to the AIDS Control Units, which support the
implementation of the strategic plan through mainstreamed and integrated spending in all relevant
ministries, and the remainder to the constituency AIDS control committees, which coordinate HIV/
AIDS activities, including NGO projects, in constituencies and communities. These funding flows
would appear to support an integrated and grass-roots response.
The remainder of this chapter compares the allocations made to health and HIV/AIDS in the four
participating African countries. For further detail on individual health systems, budget processes and
allocations; please refer to the country-specific reports.

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 15/40
14
Best Pract ice Example - HIV/AIDS Funding and Budget Control Mechanisms
South Africa is fortunate to have detailed and easily accessible national and provinical budgets,
as well as national and provincial revenue and expenditure statements published regularly by
the National Treasury. These track mainly public funds channelled through the National Treasury,
making it easier to monitor and track national and provincial government budgets and spending.
South Africa’s national budget employs two key HIV/AIDS funding mechanisms. First there
are “ conditional grants,” ring-fenced amounts that have certain conditions attached and must
be spent on specific activities. National departments transfer such grants to their provincialcounterpart departments for spending on specific HIV/AIDS interventions in the health,
education and social development sectors. It is therefore easy to identify in the budget
ddocuments what has been allocated for HIV/AIDS through condit ional grants. In addit ion, the
mechanisms for reporting on the spending of these grants are well developed, and thus allow
for analysis of spending efficiency.
Secondly, in addition to the conditional grants, South Africa also uses a non-targeted funding
mechanism, referred to as the “ equitable share,” which allows discretionary spending by theprovinces. Funding from the equitable share can be used to mit igate the indirect consequences
of HIV/AIDS, for instance by strengthening health care systems, and supporting responses
across departments. It was particularly difficult to ascertain how much provinces were spend ing
on HIV/AIDS out of their equitable share allocations.
It appears that this mix of funding mechanisms, which allows both ensured delivery of specific
HIV/AIDS services and the “ untraceable spending” required to address the indirect impact of
HIV/AIDS, can produce a more integrated, multisectoral response.
6. Allocat ions Made t o Public Health
In April 2001, the Organisation of African Unity (OAU) committed itself to certain responses to the
HIV/AIDS pandemic, and these are contained in the Abuja Declaration (OAU, 2001). The declaration
called for African governments to allocate 15% of their national budgets to health spending, with
more emphasis on HIV/AIDS programmes. This commitment echoed that of the United Nations
General Assembly special session on HIV/AIDS (UNGASS), which called for spending on HIV/AIDS
programmes to be increased to US$7-10 billion by 2005. The declaration of commitment by the Africa

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 16/40
15
Union called for sufficient spending to provide coverage of essential prevention, care and mit igation
services in an effort to reduce the spread of the epidemic.
The analysis undert aken in each coun try at tempted to ascertain the state all ocations made to
public health, and the key sources of these funds – namely, state revenue or donor aid. It is important
to understand that this study d id not consider all public heath allocations, including private and out-
of-pocket expenditure. Therefore, the shares of state contributions presented here may be lower
than those calculated by either the national health accounts (NHA) or national AIDS accounts (NAA)
approach, both of which include all expenditures and include donor allocations in public health
expenditure. In order to consider the level of prioritisation of health spending, the allocations were
calculated as a proportion of each country’s gross domestic product (GDP) and total state expenditure.Where possible, per capita health allocations were also calculated.
The countries cannot be compared without qualification. For example, in the case of Mozambique,
it was difficult to distinguish state funds from donor funds as a large proportion of the health budget
was donor-funded (62% in 2002, according to MISAU-DPC, 2003), which may have contributed to the
slightly higher proportions reported here.
With regard to Namibia, health and social services both fall under one ministry (MoHSS) and theirrecurrent budgets are combined. It was therefore not useful to compare the full Namibian MoHSS
budget with the other countries’ MoH budgets, so the health-specific allocations within the MoHSS had
to be extracted and, where appropriate, compared with the health allocations of the other countries.
However, it was impossible to compare the Namibian development allocatio ns to HIV/AIDS with the
other countries’ state HIV/AIDS funding. Hence the Namibian HIV/AIDS allocations are omitted from
some of the comparative graphs below.
6.1 Public Health A llocations as a Share of GDP and Tot al Expend it ure
Consideration of the state-alone health allocations in the government budget as a share of GDP
shows that South Africa’s share remained fairly stable at around 3% over the study period (2000/01-
2005/06), while Kenya’s increased gradually, from 1.48% in 2000/01 to a proj ected 1.88% in 2004/05.
Mozambique’s health allocation as a share of GDP experienced a drastic increase from 2.9% in 2000/01
to 4.2% in 2002/03, which may have been due to injections of donor aid to alleviate the effects of the
floods in 2000 and 2001. The total budget for Namibia’s MoHSS remained around 12% to 13% of
total expenditure, while the health-specific allocations of that budget made up 9.65% in 2001/02 and
decreased to 9.24% in 2004/05, which would undermine the state’s commitment to health services.

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 17/40
16
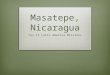
These trends are replicated when health allocations are viewed as a share of total state
expenditure, shown in figure 6.1. Only Mozambique appears to have met the 15% target of the Abuja
Declaration, with 15.4% in 2003/04. South Africa’s remains constant over the period at around 11.3%,
while Kenyapeaks at 6.33% in 2004/05. Again the Mozambique data included donor funds, which may
account for the higher apparent proportion there.
Sources: INE, 2003 (Mozambique); NT, 2003a and NT, 2003c (South Africa); GoK, 2003 and NACC, 2003b (Kenya).Republic of Namibia. 2001/02, 2002/03, 2003/04 (Namibia).
The Namibian MoHSS showed gradually increasing allocations – not adjusted for inflation, however
– but with a slight decrease projected for 2004/05. Health-specific spending makes up around three-
quarters of the total ministry expenditure.
6.2 Per Capit a Public Health A llocations
Comparing the real per capita health expenditure (state-only contributions) in the four countries
shows huge inequalities, with South Africa’s allocations being the highest at US$95 3 in 2005/06 (per
capita of the public population only4). Kenya and Mozambique’s health allocations remain fairly constant
at around US$8 and US$9 respectively, with a projected increase to almost US$10 for Kenya in 2004/05.
Figure 6.1Priorisation of health - public health allocations as ashare of tot al state expendi ture 2000/ 01 - 2005/06
Mozambique
Abuja target
Namibia - total MoHSS
South Africa
Namibia - health only
Kenya
18
16
14
12
10
8
6
4
2
0
2000/01 2001/02 2002/03 2003/04 2004/05 2005/06
Percentage
3 State-only contributions to public health.4 The population in South Africa using public health facilities is estimated at 85.7% of the total population, according to the Actuarial Society of South Africa
(ASSA). Thus it was considered appropriate to use only that port ion of the p opulati on (the “ publi c populati on” ) in these calculations. In comparison, a very high
proportion of Mozambique’s and Kenya’s population depend on the state health services. Per capita public calculations for South Africa gave a one-quarter
weighting to the 14.3% of the population who benefit from medical aid, while calculations for the other countries used their total populations.

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 18/40
17
Source: Republic of Namibia. 2001/02, 2002/03, 2003/04.
Sources: INE, 2003 (Mozambique); NT, 2003a and NT, 2003c (South Africa); GoK, 2003 and NACC, 2003b (Kenya).Dorrington et al., 2002.* The allocations for Mozambique could not be obt ained for after 2002/03.** The amounts have been adjusted for inflation and conver ted to US$ using the relevant exchange rate for each year.*** South Africa calculations use public population.
Figure 6.2Namibian MoHSS expenditure
2001/02 - 2003/04 (nominal) - millions of Namibian dollars
Total health-specificexpenditure
Social security andwelfare affairs and services
1,800
1,600
1,400
1,200
1,000
800
600
400
200
02001/02 2002/03 2003/04 2004/05
N$ millions
Figure 6.3Per capita public health allocations 2000/01 - 2005/06 - US dollars (real)
100
90
80
70
60
50
40
30
20
10
0
Mozambique Kenya South Africa
US $
2000/01
2001/02
2002/03
2003/04
2004/05
2005/06

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 19/40
18
7. Allocations Made to HIV/AIDS Programmes
The feasibili ty of analysing th e HIV/AIDS allocat ions with in each country was dependent upon
its budget process and structure, and on the degree of disaggregation of expenditure, and thus va-
ried f rom one country to an other. Some count ries, such as South Africa, h ad specific HIV/AIDS line
items in th eir budgets, while others did not. Namibia had a specific HIV/AIDS line item, but only
in it s development budget, so only the funds coming from development agencies and targeted
for HIV/AIDS activities could be tracked, but not the state allocations going through the SRF in the
recurrent budget. For all the countries it was difficult, if not impossible, to track what was being
spent on non-targeted, or “ mainstreamed” , HIV/AIDS activities. In addition, except for South Africa,
all the traceable HIV/AIDS allocations were within the MoH budgets. Therefore it was difficult toascertain the deg ree to which a multisectoral response was being funded. Where the national AIDS
coordinating bodies tracked all funds entering the country for HIV/AIDS activities, the analysis was
greatly facilitated. The research process highlighted the d ifficult ies in accessing such data, and thus
collecting and analysing the data took longer than was anticipated. Because of the different sources
and differing levels of “ totality of funds captured” , this study undertook cross-country comparisons
with caution, attempting to ensure common units of comparison and indicating any differences.
The Kenyan National Aids Resource Envelope – that is, the information collected by the MoHin their NHA process – made access to HIV/AIDS-specific spending relatively easy, and provided
disaggregated data by source, by service provider and by service provided. However, it must
be remembered that this was limited to health expenditure and did not consider multisectoral
spending. In South Africa, it was easier to track the HIV/AIDS-targeted conditional grants sent to
provinces (provincial health, education and social development departments) and the allocations to
the national programme. It proved more difficult to capture the indirect spending by provinces and
departments on HIV/AIDS activities, which were funded through the equitable share mechanism.
However, efforts were made to capture most of these, and they are presented here.
The Namibian development budget (both inside and outside the SRF) included identifiable
HIV/AIDS-related development projects, but it was not possible to determine the HIV/AIDS
amounts allocated in the recurrent budget, specifically in the budget of the MoHSS. Thus the
figures provided here could not include all the Namibian HIV/AIDS spending, and are therefore an
underestimation. Nevertheless they give an indication of the baseline spending on HIV/AIDS in the
country and should enable civil society to mobilise for increased state allocations and improved
reporting of these.

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 20/40
19
7.1 HIV/AIDS Nominal and Real Allocat ions
The countries’ nominal and real HIV/AIDS allocations are set out below, in the local currencies.
Each country’s funding mechanisms and the key policies and programmes being funded are described
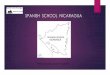
in the individual country reports. Figure 7.1 demonstrates that Kenya’s HIV/AIDS health-related
allocations are steadily rising, while South Africa’s show more drastic increases. The South African
figures include allocations within the three social sectors, as well as those provincial “ discretionary”
or additional allocations that could be ascertained. Mozambique’s allocations reflect fluctuations,
primarily due to influxes of donor aid, and only a small overall real increase. The Namibian HIV/AIDS
allocations made through the development budget, sourced primarily from donors, also show large
increases in funding to HIV/AIDS activities in that country.
Source: NACC, 2003b, b ased on NHA estimates.
The figure above shows the Kenyan state allocations directly to the ACUs, then public funds (made
up of state and some donor contributions), and finally from donors, the private sector and NGOs
committed to HIV/AIDS activities. Massive increases were experienced in 2001/02 (almost 400% in
state allocations in real terms). However these are slowing down, and declines are projected over the
MTEF period. The 51% decrease in state allocations in 2004/05 might be due, in part, to a limited
ability to project future state resources. Despite the forecasted decrease, the average annual real
Figure 7.1Kenyan HIV/AIDS allocations - state and donor funds2000/01 - 2005/06 (real) - billions of Kenya shillings
State (only)
Public sector -state an donor
Donors, private,
NGOs etc
16
14
12
10
8
6
4
2
0
2000/ 01 2001/ 02 2002/ 03 2003/ 04 2004/ 05 2005/ 06
Billions, Kenya shillings

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 21/40
20
growth rate in state-specific allocations to HIV/AIDS over the study period is almost 80%, strongly
indicative of the government’s commitment to the fight against HIV/AIDS.
Source: INE, 2003 (Mozambique).
The amounts allocated for the South African response include the national HIV/AIDS budget,the provincial health, education and social development allocations made through the HIV/AIDS
conditional grants to those three sectors, and the discretionary spending made from the provinces’
equitable shares. This indicates not only the targeted HIV/AIDS allocations to p rovide specific services,
but also non-targeted allocations from departments to support an integrated, mult isectoral response.
These two funding mechanisms are a useful model to support both forms of spending. The difficulty
inherent in the non-targeted allocations is that of tracking the funds which ministries or departments
might spend additionally on HIV/AIDS.
The figure above indicates what the Mozambican authors refer to as the “ lumpiness” of funding
due to fluctuations in the donor aid being directed to HIV/AIDS in Mozambique. This variability and
unpredictabil ity makes planning d ifficult and undermines the sustainabili ty of projects. When corrected
for inflation, an average annual real decrease of 11.3% is experienced in Mozambique between 2000/
01 and 2003/04. Such an erratic funding situation will seriously hamper the government’s HIV/AIDS
programmes, particularly its recently announced ARV treatment programme.
Figure 7.2Mozambique HIV/AIDS allocations 2000/01-2002/ 04
(nominal and real) - billions of meticals
Total HIV/AID
budget (nominal)
Total HIV/AIDS
budget (real)
250
200
150
100
50
0
2000/01 2001/02 2002/03 2003/04
Meticais billions

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 22/40
21
Source: Republic of Namibia (2001-2006).
The small proportion that goes through the SRF is the allocation to the NACP. The increasing
allocations to this programme will greatly enhance the government’s ability to coordinate a multisectoral
and integrated response to HIV/AIDS in Namibia.
7.2 HIV/AIDS Allocat ionsas a Share of Tot al Expend it ure and of Tot al Healt h Expendit ure
It is useful to compare the allocations to HIV/AIDS in each country as a share both of total stateexpenditure and of the state’s total public health expenditure. This gives a good indication of the
priority that states give the issue over other expenditure, and also assists in cross-country comparison.
Figure 7.4 shows the HIV/AIDS allocations as a share of total expenditure. Mozambique’s sharp
decline in 2002/03 may have been due, in part, to the fluctuating nature of donor funds. Thereafter
their allocations stabilise at around 0.4%.
Figure 7.3Namibian development budg et allocations to HIV/AIDS
2000/01 - 2005/ 06 - millions of Namibian dollars
Outide SRF
Inside SRF
90
80
70
60
50
40
30
20
10
0
2000/01 2001/02 2002/03 2003/04 2004/05 2005/06
N$ millions

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 23/40
22
Sources: INE, 2003 (Mozambique); Budget Review, 2003/04 and Estimates of National Expenditure, 2003 (south Africa);Estimates of Recurrent and Development Revenue, 2003, and National Aids Resource Envelope, 2003 (Kenya)
South Africa’s HIV/AIDS allocations as a share of total state expenditure have been steadily
increasing over the period of study and are projected to continue doing so, rising to 0.56% in 2005/
06. The recent increases have been due to the allocations specifically for the roll-out of the free ARV
treatment programme.
Out of the four countries studied, Kenya’s HIV/AIDS allocations form the largest share of total
state expenditure, jumping from under 0.1% to just over 0.85% of total state expenditure. Similar
patterns are revealed for HIV/AIDS allocations as a share of total state public health expenditure.
The HIV/AIDS line item in the Namibian development budget is absorbing an increasing amount
of the total donor funds captured in the MoHSS development budget. Figure 7.6 shows it as less
than 5% in 2000/02 and rising sharply to almost 38% in 2003/04. This certainly reflects the changing
priorities of donors towards HIV/AIDS, but also demands an analysis of whether the government’s
funding to HIV/AIDS has decreased in light o f these funding flows, or if the “ additionality” principle
of the Global Fund to Fight AIDS, Tuberculosis and Malaria is being honoured by recipient states.
Figure 7.4HIV/AIDS allocations as a share of t ot al expendit ure 2001/ 01 - 2005/ 06
South Africa - HIV/AIDSas % of total budget
Mozambique - HIV/AIDSas % of total budget
Kenya - HIV/AIDSas % of total budget
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
2000/01 2001/02 2002/03 2003/04 2004/05 2005/06
Percentage

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 24/40
23
Sources: INE, 2003 (Mozambique); NT, 2003a and NT, 2003c (South Africa); GoK, 2003 and NACC, 2003b (Kenya)
Sources: Namibian Rolling Development Budgets (2000/01, 2001/02-2003/04, 2003/04-2005/06).
Figure 7.6Namibian HIV/AIDS development allocations as a share
of t otal M oHSS development allocations 2000/01 - 2005/ 06
40
35
30
25
20
15
10
5
02000/01 2001/02 2002/03 2003/04 2004/05 2005/06
Percentage
Figure 7.5HIV/AIDS allocations as a share o f
the tot al public health budget 2000/01 - 2005/06
South Africa - HIV/AIDSas % of total health budget
Mozambique - HIV/AIDSas % of total health budget
Kenya - HIV/AIDSas % of total health budget
18
16
14
12
10
8
6
4
2
0
2000/01 2001/02 2002/03 2003/04 2004/05 2005/06
Percentage

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 25/40
24
The graphic presentation in the figures on the previous page are set out in tabular form in table 7.1.
Sources: INE, 2003 (Mozambique); NT, 2003a and NT, 2003c (South Africa); GoK, 2003 and NACC, 2003b (Kenya).
TABLE 7.1: State public health and HIV/AIDS prop ort ional shares
Health and HIV/AIDS shares (%)
SA: health as % of totalbudget
SA: healt h as % of GDP
SA: HIV/AIDS as % of to talbudget
SA: HIV/AIDS as % of to talhealth budget
MoZ: health as % of t ot albudget
MoZ: health as % of GDP
MoZ: HIV/AIDS as % of totalbudget
MoZ: HIV/AIDS as % of totalhealth budget
Ken: health as % of t otalbudget
Ken: health as % of GDP
Ken: HIV/AIDS as % of totalbudget
Ken: HIV/AIDS as % of total
health budgetNam: MoHSS as % of t ot alSRF budget
Nam: health only as % oftotal SRF budget
11.56%
2.96%
0.09%
0.67%
9.90%
2.90%
0.50%
5.20%
4.36%
1.48%
0.10%
2.24%
2000/1
11.60%
3.03%
0.13%
0.87%
12.60%
3.60%
0.80%
6.40%
4.80%
1.53%
0.147%
9.86%
13.37%
9.65%
2001/2
11.66%
3.04%
0.29%
1.88%
15.40%
4.20%
0.30%
1.60%
5.47%
1.69%
0.62%
11.41%
12.92%
9.45%
2002/3
11.35%
3.07%
0.39%
2.94%
15.40%
4.20%
0.40%
2.60%
5.12%
1.74%
0.88%
17.10%
13.55%
9.43%
2003/4
11.33%
3.06%
0.49%
3.86%
15.90%
4.30%
0.40%
2.60%
6.33%
1.88%
0.48%
7.63%
12.85%
9.24%
2004/5
11.16%
3.01%
0.56%
4.55%
15.90%
4.20%
0.40%
2.60%
5.85%
1.64%
0.46%
7.86%
2005/6

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 26/40
25
7.3 HIV/AIDS Per Capit a Allocations
For a cross-country comparison that takes into account the size of the population and the size ofthe epidemic in each country, it is useful to consider the HIV/AIDS allocations per capita, using public
populations as well as the HIVpositive populations (where possible). Amounts were converted in US$
equivalents, to allow comparison.
The per capita HIV/AIDS allocations varied greatly between the countries, and comparison
was problematic. Note the huge increases revealed in figure 7.7 with regard to the South African
allocations. In comparison, Kenya’s HIV/AIDS per capita allocat ion t ended to remain const ant over
the study period at around US $ 2.
Sources: NT, 2003a; NT, 2003c; NT, 2003d; NT, 2003g (South Africa); Dorrington, Bradshaw & Budlender, 2002;
Idasa calculations. NACC, 2003 (Kenya). Author’s pr ojections.Note: Kenya public HIV/AIDS allocations includes state and donor funds.
The use of calculations involving different target groups in South Africa adds detail that puts the
size of the allocations into the context of the severity of the epidemic in that country. The recent
increases in allocations have been primarily due to the policy decision to roll out free ARV treatment
to the population through the public health facilities. Figure 7.8 shows per capita figures based on
the total, HIV-positive and AIDS-sick population respectively. This cannot be interpreted as directly
indicating the amount of public resources allocated for each HIV-positive or AIDS-sick person, since
HIV/AIDS activities funded include preventative activities aimed at the HIV-negative population and
Figure 7.7South African and Kenyan annual per capita
HIV/AIDS allocations - 2000/01-2005/06 (real) - US dollars
SA state HIV/AIDS percapita (public population)
Kenya public HIV/AIDSper capita spending
6
5
4
3
2
1
0
US$
2000/01 2001/ 02 2002/03 2003/ 04 2004/05 2005/ 06
26

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 27/40
26
other responses that the HIV-positive population can benefit from, without necessarily being AIDS-
sick. Nevertheless, the figure gives a broad overview of the increasing allocations by beneficiary
group.
Sources: NT, 2003a; NT, 2003c; NT, 2003d; NT, 2003g; Dor rington, Bradshaw & Budlender, 2002; Idasa calculations.
8. Changing Priorit ies - Changing Types of Act ivit ies
The analysis of the composition of the HIV/AIDS allocations, (e.g. p revention versus treatment,multisectoral or health-dominated) relied heavily on the degree of disaggregation and codification
of budget documents and other sources within each country. For example, the Mozambican and
Namibian data did not disaggregate sufficiently to allow for this detailed analysis. The comparison
was further complicated by the differing categorisation and definitions used in the countries for
“ treatment” as opposed to “ preventative” activities. For purposes of this analysis, any action that
intends to prevent an HIV transmission is categorised as “ preventative” even where it involves
medical treatment. For example, PMTCT and the treatment of STIs are considered preventative.
“ Treatment” is defined narrowly as medical treatment fo r HIV-positive people, primarily ARV drugtreatment.
Figure 7.8Annual per capita HIV/AIDS expenditure in South Africa
2000/01 - 2005/06 (real) - rands
For public population
For HIV + population
For AIDS - sick population
2,000
1,800
1,600
1,400
1,200
1,000
800
600
400
200
02000/01 2001/02 2002/03 2003/04 2004/05 2005/06
Rand (real)
27

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 28/40
27
The best example of changes in policy being reflected in budget allocations is that of South Africa
and its recent commitment to providing free ARV treatment. Figure 8.1 on the following page shows
a rapid increase in the proport ion of the budget allocated for ARV treatment in South Africa, asopposed to the other HIV/AIDS activities. In addition, the actual allocations for ARVs (in both nominal
and real terms) are risin g dramatically. The figure demonstrates that allocations for prevention and
care and support activities are not increasing con currently. Figure 8.2 shows th e tot al HIV/AIDS-
earmarked budget in relation to the funds for the new ARV treatment programme. The figure also
includes the funds going to the departments of education (classified as preventative) and social
development (classified as care and support activities).
Sources: South Africa 2003/04 Budget . NT, 2003e. Idasa calculations.Note that the health conditional grant for HIV/AIDS (excluding ARV funds) is roughly divided as follows:50% for preventative measures, 40% for care and support and 10% for coordination.
These important shifts in policy, reflected in the budget allocations, came about because of
a number of factors, primarily the increasing need evident in rising mortality, morbidity and their
resultant hardship. Also critical was the effective pressure exerted by civil society organisations and,
importantly, accurate costing, which showed that providing free ARV treatment was within the state’s
financial capacity.
Figure 8.1Changing p riorit ies in HIV/AIDS spending in South Afr ica
according t o activity type 2000/02 - 2005/06 - millions of rands
1,800
1,600
1,400
1,200
1,000
800
600
400
200
0
Research
Management
Treatment
Care and support
Prevention
NGO transfers
2000/01 2001/02 2002/03 2003/04 2004/05 2005/06
28

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 29/40
28
Figure 8.2 shows the upward climb of the total HIV/AIDS allocations in real terms. The ARV
conditional grant funds will consume an increasing proportion of the health HIV/AIDS conditional
grant. In the first year of ARV rollout (2004/05), 38% of the funds transferred as conditional grantsto the provinces by the DoH will be intended for ARV treatment programmes. However, beginning
in 2005/06, national government will be sending more funds to provinces for ARV programmes
specifically than for all other HIV/AIDS interventions in the health sector. By 2006/07, 64% of the HIV/
AIDS conditional grant funds are intended for ARV treatment (Hickey, 2004).
Sources: NT, 2003c:407; NT,. 2003e:82. Idasa calculations.
Kenya’s total HIV/AIDS allocations (including donor funds) have remained relatively stable over
time in terms of service type (figure 8.3). The largest proportion goes to “ treatment and care” .However, since the Kenyan government does not provide free ARVs, much of this component would
be treatment of STIs and OIs funded by donor allocations and health care services offered by the
MoH.
Rough estimates for the composition of allocations in Mozambique were obtained through
interviews with the country’s National AIDS Council, which indicated that treatment activities receive
approximately 60% of the budget, while prevention receives approximately 40%.
Figure 8.2Contribution of ARV treatment funds to total
HIV/AIDS budgets in South A frica 2000/01 - 2005/ 06 - millions of rands
ARV treatment funds
HIV/AIDS budget excludingARV treatment funds
2,500
2,000
1,500
1,000
500
0
2000/ 01 2001/ 02 2002/ 03 2003/ 04 2004/ 05 2005/ 06
Billions, Kenya shillings
29

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 30/40
29
Sources: Estimates of Recurrent and Development Revenue, 2003, and National Aids Resource Envelope, 2003 (Kenya).* Incorporated under ‘prevention’ are: behaviour change, blood safety, PMTC and STI treatment. Incorporated under
" care" is mitigation of socioeconomic impact.
With regard to the Namibian data, compositional analysis was not possible based on data on
allocations and expenditure. However, based on the projected resource usage for the duration of
the country’s NDP (2001-2006), which provides targets and cost estimates for each programme and
ought to guide actual allocations, it was found that the majority of projected budgets (92%) were to
intended to be used for “ care and support” activities, primarily through the MoH.
9. Effi ciency and Equit y in HIV/ AIDS Spend ing
As noted above, this study has focused primarily on budget allocations. Analysis of actual
expenditure against allocated amounts is limited, largely due to the unavailability of expenditure
reports. Only South Africa has detailed quarterly expenditure reports published by the National
Treasury. Where spending data is available, it tends to indicate underspending of the actual
disbursements (such as the di screpancies between Mozambique’s allocated, disbursed and spent
health funds). Furthermore, there were cases of actual disbursements being lower than the amountsoriginally allocated in budget documents.
Figure 8.3Compositio n of tot al Kenyan HIV/AIDS allocations
by t ype of service 2000/01 - 2004/ 05 - billions of Kenya shillings
Policy developmentand managment
Care and suppor t(incl. IGAs)
Research and M&E
Treatment and care
(not i ncl. free ARVs)
Prevention activities(incl. PMTCT)
16
14
12
10
8
6
4
2
02000/01 2001/02 2002/03 2003/04 2004/05
K e
n y a
s h i l l i n g s b i l l i o n s
30

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 31/40
Best pract ice example – improving effi ciency in spending HIV/AIDS allocations
In South Africa, the increasing allocations to HIV/AIDS in recent years have placed extraordinarydemands on departments, requiring them to spend allocations that double or t riple from one
year to the next. For example, from 2000/01 to 2001/02 the National Treasury increased the
earmarked funds for HIV/AIDS sent to provinces by over 160%. In 2002/03, the amount national
government expected provinces to spend tripled in relation to the previous year. Including
expenditure on roll-overs , provincial HIV/AIDS managers succeeded in spending R109 million
in 2001/02 – six times the amount spent in the previous year. Moreover, in 2002/03 actual
spending increased again by over 250%, to R385 million (Hickey et al., 2003).
Despite these massive increases, the aggregate provincial spending records on the HIV/AIDS
conditional grants for the three years provide evidence of huge improvement. Overall, 85% of
HIV/AIDS conditional grant funds were spent in 2002/03, compared to a low 36.5% in 2000/01
(excluding the roll-over amounts indicated above). Beginning in 2001/02, aggregate spending
on HIV/AIDS conditional grants matched or exceeded average spending on conditional grants
generally, which indicates that the usual difficulties experienced with conditional grant spending
were surmounted by rapid improvement in HIV/AIDS programme structures and spending pro-
cedures (Hickey et al., 2003).
The lack of disaggregated data by region made it difficult to analyse whether HIV/AIDS resource
allocation was equitable, with respect to the burden of the disease carried in the different areas of
each country and according to the socioeconomic status, infrastructure and accessibi lity of health and
other state services in those areas.
In Kenya, the NACC ensures that the HIV/AIDS resources are allocated according to geographical
need. The new financing framework enables the NACC to allocate resources based on agreed priorit ies,
geographical targets set by the NACC and poverty reduction targets set by the government. It also
considers population size, prevalence rates and morb idit y rates, and well as the cost and effectiveness
of interventions and coverage rates. However, Kioko and Njeru, in the Kenyan report presented here,
indicate that this new “ resource allocation formula in enhancing regional equality has not funct ioned
as expected,” due in part to the incapacity of regions to prepare adequate funding proposals in order
to apply for HIV/AIDS allocations.
In South Africa it was possible to undertake a geographical comparison of HIV/AIDS allocations
based on provincial shares of the HIV-positive population. Figure 9.1 on the following page presents
31

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 32/40
the per capita amounts for the provincial health HIV/AIDS allocations as against the provincial HIV
positive population.
Figure 9.1 compares the provincial HIV/AIDS health-budgeted amounts per HIV-positive person
with the provincial share of the total HIV-positive population, according to 2000 model projections by
ASSA (Dorrington et al., 2002). Although the Western Cape is the province with the second lowest
number of HIV-positive people, its health department budgets the highest amount per HIV-infected
person (Hickey, 2003).
However, although this per capita analysis gives us some insight into sufficiency and equity
considerations in resource allocation across provinces, it should be treated with caution. Thisis because the graph does not take into account HIV/AIDS spending in sectors outside health,
nor does it include the indirect or “ hidden” HIV/AIDS-related expenditure in regular health care
services.
There is indeed a need for more detailed analysis of country HIV/AIDS allocations according to
indicators of equity, but this will require a significant degree of disaggregation and detail in budgets
and spending reporting mechanisms. The tracking of resources to different vulnerability groups and
beneficiary groups would be extremely useful, and a gendered perspective in tracking the resources
would be vital.
Sources: 2003 IGFR; 2003 Estimates of National Expenditure; 2003 Budget Review; 2003 Provincial Budget Statements;Dorrington et al ., 2002; Idasa calculations.
Figure 9.1Provincial HIV+population vs per capita HIV/AIDS
provincial health expenditure 2003/04
30
25
20
15
10
5
0
300
250
200
150
100
50
0
Percentage
Provincial share ofcountry's HIV +population 2003according to ASSAmodel projections
2003/4 provincialHIV/AIDS healthbudgeted amountper HIV + person(public population)
E a s t e
r n C a
p e
F r e e S
t a t e
G a u t e
n g
K w a Z u l u
N a t a l
N o r t h
W e s t
N o r t h
e r n C a p e
M p u m
a l a n g
a
L i m p o
p o
W e s t e r
n C a p e
32

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 33/40
10. Af rica Regional Recomendat ions
Each country report includes recommendations relevant to the specific country situation. Therecommendations pulled together here are those that are common to the countries and relevant to
the whole region, and that relate primarily to, or influence, budget allocations and processes. These
should inform a range of policy-makers, decision-makers, programme planners and implementers, as
well as civil society representatives and research agencies.
10.1 Policy Implicat ions
The International Guidelines on HIV/AIDS and Human Rights (1997) should guide and inform
countries’ National HIV/AIDS Strategic Plans (NSPs), and it is suggested that countries develop their
own charters of the rights of persons infected and affected by HIV/AIDS, emulating the Namibian HIV/
AIDS Charter of Rights. The UNGASS commitments and the Millennium Development Goals should
also influence NSPs and national development plans (NDPs).
Commitment to NSPs should be reflected in the adequate allocation of resources for their
implementation. Departments require increased capacity – infrastructurally and in terms of personnel,
financial systems and skills – in order to implement NSPs effectively. The implementation of all NSPs
should be monitored carefully.
NSPs should incorporate the provision of ARV treatment as a matter of urgency. In addition,
the delivery of PMTCT interventions, where missing or inadequate, should be incorporated or
strengthened. However, emphasis on the provision of ARV treatment should not be at the expense of
preventative, care and support activities.
10.2. Mainst reaming HIV/ AIDS as a Development Issue
HIV/AIDS should be incorporated into NDPs and poverty reduction strategy papers as a cross-sectoral,
goal-level priority. HIV/AIDS should also feature prominently in debt-relief negotiations and Heavily-
Indebted Poor Countries (HIPC) documents. Plans should have specific commitments and targets, linked
to actual budget allocations, which should be based on accurate costings (UNAIDS, 2003b:8).
33

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 34/40
Dealing with HIV/AIDS as a development issue requires an integrated and mult isectoral response.
However, the integration of HIV/AIDS into the activities of all ministries can only occur with adequate
budgetary allocations. Clear targets, performance indicators and cost estimates would assist ministriesto fund and execute their HIV/AIDS plans.
A mainstreamed response requires appropriate funding mechanisms: a combination of “ ring-
fenced” or condit ional amounts, which have clear directives for use, and “ non-allocated” or indirect
transfers that allow for ministries’ discretion in their HIV/AIDS activities. These mechanisms would
foster an integrated and flexible approach, while also ensuring the provision of certain essential
components.
Most of the country studies presented here could only capture health-related HIV/AIDS spending.
This emphasises the lack of data on multisectoral responses to HIV/AIDS. Therefore, all ministries
should allocate portions of their budgets to HIV/AIDS activities, and should provide regular and
detailed financial and performance reports to the national HIV/AIDS coordinating body.
10.3 Instit utional Implicat ions
A national AIDS coordinating body requires high-level authority to manage a multisectoral response
and should be composed of all key sectors, with both government and civil society representatives.
Therefore it is recommended that such bodies be situated in the highest office, preferably that of the
country ’s President or Prime Minister, and be autonomous of the MoH. Their powers , functions, and
lines of accountability should be clearly defined.
The national AIDS coordinating body should influence budget processes and allocations for
HIV/AIDS activities, and also coordinate and channel donor funds. This ensures that donor priorities
are in line with national priorities and reduces duplication, gaps and the fragmentation of services.
“ Mob ilising responses to HIV/AIDS and co-ordinating efforts should be the... core business” of
national co-ordinating structures (Strode and Barrett Grant, 2004:46). There should also be adequate
institut ional linkages between the national HIV/AIDS coordinating body and the Ministry of Finance or
Planning (UNAIDS, 2003b:8).
National coordinating bod ies require adequate funds and staff to ensure their efficiency and ability
to coordinate across all ministries and sectors, and should have a specific line item budget in the
national budget.
34

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 35/40
National AIDS coordinating bodies should have decentralised structures with representation at all
levels of government , throughout civil society and in every sector. The decentralised structures should
have adequate funds to support their activities.
Equally important, parliamentarians should be equipped and empowered to interrogate state
budgets and call for necessary changes. Members of parliament often do not have access to
information on HIV/AIDS spending, so efforts should be made to improve their access to, and
understanding of, such data (Lush et al., 2004). The national AIDS coordinating structure should rou-
tinely report on its activities to the cabinet.
10.4. Resource Implicat ions
Most countries in Africa are heavily dependent upon donor aid to support their HIV/AIDS activities.
The unpredictability of this source can undermine the state’s ability to plan and manage its response
to the epidemic and also has the potential to threaten the sustainability of programmes in the event
of decreasing funds. States should allocate increasing amounts to their HIV/AIDS programmes from
their own revenue, while continuing to work to improve the coordination of nationally sourced funds
with donor resources.
State allocations to health over the period of this study tended to be below the Abuja target
of 15%. There is a need for greater commitment by states to the achievement of this target. The
increasing allocations, from both states and donors, to HIV/AIDS activities are welcomed and
encouraged. In addition, funds must continue to be committed to general development, poverty
alleviation and the strengthening of the health sector, to ensure comprehensive efforts to mitigate the
impact of HIV/AIDS.
Massive injections of resources to strengthen financial, human, infrastructural and management
systems are required to ensure the efficient delivery of ARV and PMTCT treatment programmes.
These should be based on efforts to strengthen health systems generally. At the same time, resources
must continue to be directed to systems for prevention and for care and support. A balanced response
to HIV/AIDS, one which is not “ overmedicalised” , is imperative.
Increased resources are required for NGOs, CBOs and FBOs, which are the primary service
providers in many Africa countries. There is need for more efficient and robust transfer and
accountability systems for grant-making.
35

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 36/40
10.5. Funding and Budget Control Mechanisms
The mechanisms for the funding of HIV/AIDS activities should be improved, so as to allow foradequate funds and their efficient use. Two mechanisms have been suggested: ring-fenced funding
and unconditional fund transfers.
It is important for programmes to have specific HIV/AIDS budget line items to allow for improved
tracking and monitoring of HIV/AIDS expenditure. In addition departments should be required to
report on their discretionary spending on HIV/AIDS. Medium-term expenditure frameworks should
account for all HIV/AIDS-related expenditure, including resources expended by national AIDS
coordinating units (UNAIDS, 2003b.)
More comprehensive, accurate, timely and accessible data is required, from all relevant ministries
and departments, on disaggregated programme allocations and actual expenditure. Such information
should be made available to civil society and parliamentarians.
Bottlenecks in spending can be reduced with improved provincial and local financial management,
planning and accountability mechanisms.
10.6. Coordinating Donor Funds
As mentioned above, in order for governments to have increased control in planning and
managing their response to the epidemic, it is necessary for national coordinating bodies to have
greater control over, or at least greater knowledge of, all HIV/AIDS funds entering the country. To
assist this process, a centralised database should be established to which donors frequently submit
updated records of their funding activities, such as the Investment Budget in Mozambique, which
registers external funds.
Synchronisation of donor funding requirements and reporting mechanisms would greatly relieve
the burden on governments with regard to their reporting responsibilities to donors. At the moment,
duplication and excessively burdensome administrative procedures are crippling the ability of
governments to manage the expenditure of these funds effectively.
This study did not consider contributions from the private sector to HIV/AIDS activities. It is
recommended that a system for capturing and tracking these funds be developed in-country, andthat public-private partnerships be promoted.
36

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 37/40
10.7 Monitoring Issues of Equity and Human Rights Promotion
Increased efforts are required to develop performance indicators that measure the inputs, outputsand impact of budget allocations, particularly to the extent that they promote and protect the
achievements of the rights of citizens.
Such monitoring should measure allocations based on need (the disease burden, prevalence
rates and the demand for services). Geographical distribution, including the accessibility of health
services and other facilities and the capacity of regions to absorb, manage and utilise funds, should be
considered in the equitable distribution of resources. Allocations should also be analysed according
to beneficiary groups, ensuring that women, children and other vulnerable g roups are given priorityin resource distribution. It is important that such allocations translate into equal access to affordable
and quality services for all vulnerable persons.
There is a need to build the capacity of local civil society organisations to routinely monitor
government expenditure on HIV/AIDS and track donor funds, so that they can engage more actively
in the national budget process. Governments must be accountable to their citizens for their spending
of public funds, and should report on outputs and the achievement of their performance indicators.
This study has provided an effective capacity-building programme for NGOs in the countries
studied, in that their ability to monitor their government’s HIV/AIDS allocations has been enhanced.
The research process developed a valuable framework for comparative analysis, while also allowing
for countryspecific nuances in data collection and analysis. This project has been an important first
step in the empowerment of civil society to understand and interrogate budget processes and
allocations to HIV/AIDS. It has clearly identified gaps in budget allocation data, and therefore makes
an earnest appeal for greatly improved budget and spending records. It is hoped that this initiation
into budget analysis will lead to ongoing t racking of state and donor funds.
It is recommended that projects aiming to capacitate civil society to monitor HIV/AIDS allocations
should be supported, p romoted and expanded. The analysis should deepen to include an evaluation
of the outputs and impact of budgetary allocations. These allocations should also be evaluated
according to the estimated costs of required interventions, and in terms of the burden of disease.
37

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 38/40
References
• Barnett , T., & Whiteside, A., 2002. AIDS in the twenty-first century: disease and globalization. NewYork: Palgrave Macmillan.
• Commit tee of Inquiry into a Comprehensive Social Security System. 2002. “ Transforming the
present, Protecting the Future: Consolidated report” . Dept of Social Development. RSA.
• Dorrington, R., Bradshaw, D., & Budlender, D., 2002. HIV/AIDS profile in the provinces of South
Africa: indicators for 2002. CARE, MRC, ASSA.
• GoK, 2003. Printed Estimates of Recurrent and Development Expenditure, 2003/04. Govt. printers.
• Hickey, A. 2003. What are provincial health departments allocating for HIV/AIDS from their own
budgets? Ida sa Bud get Brie f No.135. Available: http ://www.idasact.org.za/bis/ [1 August 2004]
• Hickey, A., 2004. New allocations for ARV treatment: an analysis of the 2004/05 budget from an
HIV/AIDS perspective. Idasa Occasional Paper.
• Hickey, A., Ndlovu, N., & Guthrie, T., 2003. Budgeting for HIV/AIDS in South Africa: report
on intergovernmental funding flows for an integrated response in the social sector. Idasa-BIS.
Available: http :// www.idasact.org.za/pdf/1057- report.pdf [1 August 2004]
• INE, 2003. Database. Instituto Nacional de Estatística, Mozambique.
• International Guidelines on HIV/AIDS and Human Rights. 1997.
• Lush, D., Sherbourne, R., & Mbaindjikua, K., 2004. More questions than answers: the response of
the Namibian legislature to HIV and AIDS. Institute for Public Policy Research, Namibia. Pending.
• Martin, G., 2003. A comparative analysis of the financing of HIV/AIDS programmes in Botswana,
Lesotho, Mozambique, South Africa, Swaziland and Zimbabwe. Human Sciences Research Council:
Pretoria.
• MISAU-DPC, 2003: Donor Resource Survey 2001-2003. Directorate of Planning and Cooperation.
Ministry of Health, Mozambique.
38

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 39/40
• MoH, 2002. Financial performance of the cost sharing programme. Annual Report, 2001/02.
Division of Health Care Financing, Ministry of Health, Kenya.
• MoHSS, 2002. Epidemiological report on HIV/AIDS. Namibia: Ministry of Health and Social
Services.
• MoPND, 2003. Kenya demographic and health survey. Preliminary report. Nairobi: Ministry of
Planning and National Development.
• Multisectorial Technical Group, 2003. Official launch of new HIV prevalence rates. MISAU-PNC/
DTS/HIV-SIDA. November. Mozambique.
• NACC, 2003: The Kenya National HIV/AIDS Resource Envelope. Nai robi: National AIDS Control
Council, Office of the President.
• NT. 2003a. Budget Review. Pretoria: National Treasury. Available:
http:// www.treasury.gov.za/documents/budget /2003/review/ [17 August 2004]
• NT. 2003b. Division of Revenue Bill. Pretoria: National Treasury. Available:
http://www.finance.gov.za/document s/bu dge t/2003/drb/d rb.pdf [17 August 2004]
• NT. 2003c. Estimates of National Expenditure. Pretoria: National Treasury. Available:
http:// www.finance.gov.za/document s/budget/2003/en e/ [17 August 2004]
• NT. 2003d. Intergovernmental Fiscal Review. Pretoria: National Treasury. Available:
http:// www.finance.gov.za/document s/ifr/2003/ [17 August 2004]
• NT. 2003e. Medium-term bud get policy statement . Pretoria: National Treasury. Available:http:// www.finance.gov.za/documents/mtbps/2003/ [17 August 2004]
• OAU, 2001. Abuja declaration on HIV/AIDS, tuberculosis and other related infectious diseases.
Available: http://www.uneca.org/adf2000/Abuja%20Declaration.htm [15 July 2004]
• PHRplus. 2004. Harmonisation of methodologies: SIDALAC and PHR plus. Presentation made to
the UNAIDS Global Consort ium for Resource Tracking for HIV/AIDS. Geneva.
39

8/8/2019 HIV/AIDS and human rights: public budgets for the epidemic in Argentina, Chile, Ecuador, Mexico and Nicaragua
http://slidepdf.com/reader/full/hivaids-and-human-rights-public-budgets-for-the-epidemic-in-argentina-chile 40/40
• Republic of Namibia. 2001/02, 2002/03, 2003/04. Estimates of Revenue and Expenditure.
Windhoek: Ministry of Finance.
• Strode, A., & Barrett Grant, K., 2004. Understanding the institutional dynamics of South Africa’s
response to the HIV/AIDS pandemic. Cape Town: Idasa.
• UN, 2001. Declaration of Commitment on HIV/AIDS. UN Special Session on HIV/AIDS. 25-27 June
2001. United Nations. Available:
http://www.un.org/ga/aids/coverage/FinalDeclarationHIVAIDS.html [28 July 2004]
• UNAIDS, 2002. AIDS epidemic update. December 2003. UNAIDS & WHO.
• UNAIDS, 2003a. Monitoring the Declaration of Commitment on HIV/AIDS: guide-lines on
construction of core indicators. UNAIDS. http://www.unaids.org
• UNAIDS. 2003b. Planning, costing and budgeting framework. User’s manual.
• UNAIDS, 2003c. Progress report on the global response to the HIV/AIDS epidemic. UNAIDS.
http://www.unaids.org
• UNAIDS. 2004. 2004 Report on the g lobal AIDS epidemic: 4th g lobal report. UNAIDS.
http//www.unaids.org
• UNDP, 2003. Human development report, 2003.
• World Bank, 2002. HIV /AIDS: Impact on education intensifies downfall. Washington DC: World
Bank.
• World Bank, 2004. World development report, 2004 . Washington DC: World Bank.