Embed Size (px)
Citation preview

HIV-Related and Epstein-Barr Virus-Associated Anal Burkitt’s Lymphoma:
Report of a Case
S. Frentlenberg / P. Palma / R. Grobholz / L. Ngendahayo / S. Post
The incidences of anal carcinomas and malig- nant anal lym- phomas are in- creasing as a re- sult of the AIDS epidemic, but a case of HlV-re- lated anal Burkitt’s lymphoma (BL) has not been reported in the literature so far. Apart from the typical facial BL manifes- tation, atypical locations have been described in the ovaries, bladder, sto- mach, gallhladder, páncreas, and upper colon (1-4). The highest inci- dence of BL is in childhood and ado- lescence, and the prognosis is rapidly fatal without adequate treatment. Few cases have been found in the rectum, none of whicli was associated with HIV or Epstein-Barr virus (EBV) (5-7).
Report of a case
A 38-year-old African farmer from the Southern part of Rwanda presen- ted at the Surgi- cal Department of the Univer- sity Hospital of Butare with the symptoins of fecal incontinen- ce, perianal pain,
weight loss, and a rapidly growing anal tumor over six weeks. The clini- cal findings showed cachexia and an 8-cm x 13-cm anal tumor (Fig. 1). Be- cause of fecal incontinence and ne- crotization of the tumor, the odor was unbearable.Sphincter function was lost and rec- toscopy showed infiltration of the whole anal canal. Altliough the linea dentata was not distinguishable, only the very lowest part of the rectum se-
Se describe y comenta un caso de lin- foma primario de Burkitt localizado
en la región anal, eventualidad como se sabe extremadamente rara, en un paciente de 38 años de edad portador de HIV, al demostrar la histopatología y la innmnohistología la presencia de un Epstein-Barr, virus asociado al linfoma de Burkitt.Combinando la quimioterapia, la terapia virostática y el tratamiento quirúrgico, en tanto se le practicó al paciente ima resección abdomino-perineal del recto, o lo que es lo mismo, una amputación recto- anal abdomino-perineal, se ha conseguido un resultado satisfactorio.
Palabras clave: Región anal. Linfoma de Burkitt. AIDS. Epstein-Barr virus.
Fecha de recepción : Noviem bre 2 0 0 5 .
Seminario Médico Año 2006. Volumen 58, N.° 1. Págs. 79-84
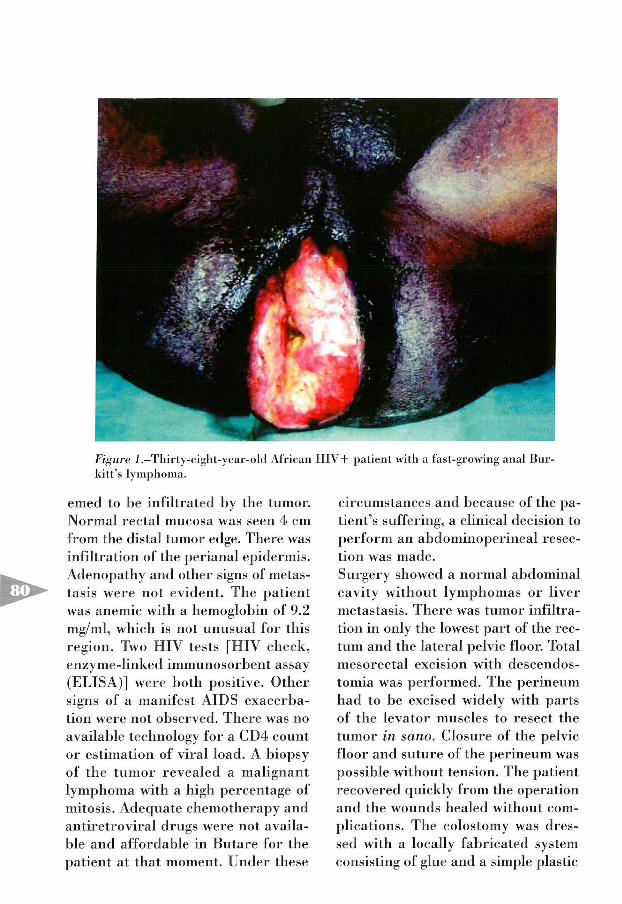
Figure 1.—Thirty-eight-year-old A lrican H IV + patient with a íast-growing anal Bur- kitt’ s lym phom a.
emed to be infiltrated by the tumor. Normal rectal mucosa was seen 4 cm from the distal tumor edge. There was infiltration oí the perianal epidermis. Adenopathy and other signs oí metástasis were not evident. The patient was anemic with a hemoglobin oí 9.2 mg/ml, which is not unusual for tliis región. Two HIV tests [HIV clieck, enzyme-linked immunosorbent assay (ELISA)] were both positive. Other signs of a manifest AIDS exacerba- lion were not observed. There was no availabie technology for a CD4 connt or estimation oí viral load. A biopsy of the tumor revealed a malignant lymphoma with a high percentage of mitosis. Adequate chemotherapy and antiretroviral drugs were not availa- hle and affordable in Bntare for the patient at that moment. Under these
circumstances and because of the pa- tient’s suffering, a clinical decisión to perfonn an abdominoperineal resec- tion was made.Surgery showed a normal abdominal cavity without lymphomas or liver metástasis. There was tumor infiltration in only the lowest part of the rec- tum and the lateral pelvic floor. Tolal mesorectal excisión with descendos- tomia was performed. The perineum had to be excised widely witli parts of the levator muscles to resect the tumor in sano. Closure of the pelvic floor and suture of the perineum was possible without tensión. The patient recovered quickly from the operation and the wounds healed without complica tions. The colostomy was dres- sed with a locally fabricated System consisting of glue and a simple plástic
bag. The patient was liappy to be able to eat and digest again without bot- hering bis family with the odor that had precluded normal social life.The histologic finding from light mi- croscopy performed by the Pathologic Institute oí the University of Bulare showed all the typical signs oí Bur- kitt’s lymphoma. Resection lines were free of tumor. The sphincter musele was completely destroyed and the lower rectum and the perineal skin were infiltrated. This diagnosis was verified by Butare’s academic part- ners at the University Hospital in Mannheim (Germany), which also
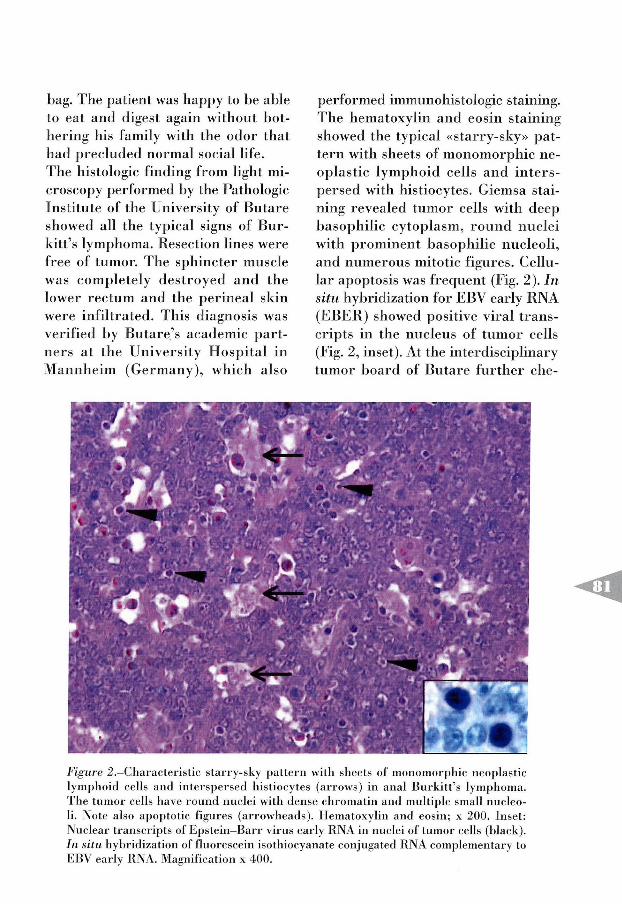
performed immunohistologic staining. The hematoxylin and eosin staining showed the typical «starry-sky» pat- tern with sheets of monomorphic ne- oplastic lymphoid cells and inters- persed with histiocytes. Giemsa staining revealed tumor cells with deep basophilic cytoplasm, round nuclei with prominent basophilic nucleoli, and numerous mitotic figures. Cellu- lar apoptosis was frequent (Fig. 2). In situ liybridization for EBV early RNA (EBER) showed positive viral trans- cripts in the nucleus of tumor cells (Fig. 2, inset). At the interdisciplinary tumor board of Butare further che-
Fig ure 2 .—Characteristic starry-sky pattern with sheets o f m onom orphic neoplastic lym phoid cells and interspersed histiocytes (arrow s) in anal Burkitt’ s lymphoma. The tum or cells llave round nuclei with dense chrom atin and múltiple small nucleoli. Note also apoptotic figures (arrowheads). Hematoxylin and eosin; x 200. Inset: Nuclear transcripts o f E pstein-B arr virus early RN A in nuclei o f tumor cells (black). In situ hybridizalion o f fluorescein isothiocyanate conjugated RN A com plem enlary to EBV early RNA. M agnification x 400.

motherapy was discussed, but becau- se the patient could not afford further chemotherapy or antiviral therapy, he was discharged without supple- mental treatment. Eight weeks after discharge the patient showed up with a generalized lymphadenopathy and progressing weakness. Within two days he fell into a coma and died.
D is c u s s io n
Burkitt’s lymphoma (BL) accounts for 1-2 percent of all cases of non-Hodg- kin’s lymphomas (NHL) in the general population but for as many as 35 per- cent among HlV-infected populations. One percent of African HIV + adults develop BL but most of the patients show cerebral or visceral BL. (8-12). The classic facial BL is not an AIDS- associated tumor in Africa (13). Although EBV is often associated with malignant lymphomas in HIV+ patients, this association seems to be less frequent in HIV+ patients with BL. (6, 14, 15). Nevertheless, in this case an association of EBV with the lymphoma was confirmed by in situ hy- bridization of EBV early RNA.The histologic and immunohistoche- mical results showed the characteris- tic signs of BL. Analysis of the typical translocations t(2;8) or t(8;22), ho- wever, was not possible under the cir- cumstances in rural Rwanda.An importan! differential diagnosis of BL ineludes a large-cell immuno- blastic lymphoma. The tumor cells in this entity, however, are larger with more abundant and less basophilic cytoplasm. Nuclei have one promi- nent, centrally located nucleolus. Also, nuclear pleomorphism is seen
and the starry-sky pattern is not ap- parent. Most of the visceral manifes- tations of BL are found in the sto- mach (2). A few cases of colonic BL are described, mostly in the upper colon and only in a single case in the rectum (1, 7). Primary anorectal lymphomas are rare and are usually found in immunocompromised patients (16, 17). Anal BL, as described here, is a rare event. In 12 major stu- dies that included a total of 1043 cases of primary gastrointestinal lymphomas, there was no reference to anal BL (6). In our opinión the term «anal Burkitt’s lymphoma» is justified in this case by the fact that more than three-fourths of the tumor grew below the lower rectum and liad infiltrated the whole anus.Treatment of visceral BL is the same as for other locations. Standard treatment is chemotherapy, in which se- veral combinations of drugs are con- sidered effective. Cyclophosphamide, doxorubicin, vindesine, bleomycin, and prednisone (ACVBP) (18) or cyclophosphamide, doxorubicin, vin- cristine, and prednisone (CHOP) (19, 20) are chemotherapeutic drug combinations with high response rates. Most patients with HlV-associated NHL benefit as well from low-dose as from standard or high-dose chemotherapy with less toxicity (11, 20). After a week of chemotherapy, tumor mass reduction of 75 percent can be expected (1). The response rate is lower in HIV+ patients compared with that in HIV- patients, with a median survival time for HIV + patients of approximately seven months, and
with a long-term survival rale of only 15 percent (8, 10).It is proven that antiretroviral the- rapy (ART) decreases the incidence of HlV-associated tumors, and ART is recommended in the treatment of ma- niíest BL as well (20-23).Surgery is inevitable in cases of BL complications or is used as palliative treatment when cliemotherapy is not available. In our case, the anal sp- hincter was completely destroyed. In addition, surgical reduction of the mass of the large abdominal BL befo- re chemotherapy seems to improve survival rate (24).In Bntare the cost of a major opera- tion is approximately $40 U.S. The cost of chemotherapy in comhination with the obligatory antiretroviral the- rapy is over $1,000 U.S. For our far- mer, like for most citizens of Rwanda for whom the average daily income is less than $1 U.S., chemotherapy and ART were not only unavailable but were also unaffordable. In spite of the poor prognosis, surgery was the only plausible intervention.With the persistence of the AIDS epi- demic, an increased incidence of anal malignant tumors can be expected. Especially in Africa, anal BL may be
a more common diagnosis in the fu- ture. Because of the high costs, ade- quate treatment will be reserved for only a small number of patients.
Acknowledgments
The authors thank the colleagues of Butare University Hospital for hel- ping with our patient’s care, the tech- nical support of Miriam Bierbaum, and the editorial input of Rachel Snow.
Sebastian Freudenbeg, M.D., E.B.S.Q.C.,Department o f Surgery, Universitary Hospital Mannheim, Ruprech-Kats-Uni- versity, Heidelberg, Germany. Pablo Palma, M.D., E.B.S.Q.C., Department of Surgery, Universitary Hospital Mannheim, Ruprech-Kats-University, Heidelberg, Germany. Rainer Grobholz, M.D., Department o f Patliology, University Hospital Mannheijn, Ruprecht-Karsl- University, Heidelberg, Germany. Louis Ngendahayo, M.D., Departament ofPat- hology. University o f Bulare, Butare, Rwanda. Stefan Post, M.D., Ph.D., Department o f Surgery, Universitary Hospital Mannlieim, Ruprech-Kats-University, Heidelberg, Germany.
R eferencias b ib liográficas
1. Balonga, C.; Lencina, R.; Reus, M.; Garre, C., De las Heras, M.: «Burkitt’s lymphoma: atypical localization». Rev Esp. E nferm . Dig., 1996; 88:439-41.
2. AjAYI, OO.: «Gastro-intestinal manifesta- tions o f Burkitt tum or». Ghana M ed. 1971; 10:30-3.
3. MEARINI, E.; Z u ccm , A .; COSTANTINI, E.; Fornetti, E; Tiacci, E., Mearini, L.: «Pri- mary Burkitt’ s lym phom a o f b ladder in patient with A ID S ». J. Urol., 2002; 167:1.397-8.
4. Neary, B.; Young, SB.; Reuter, KL.; Che- ESEMAN, S., SAVARESE, D.: «Ovarían Burkitt
lym phom a: pelvic pain in a woman with A ID S ». O bstet. G ynecol., 1996; 88:706-8.
5. Greif, E ; Burstein, Y., Hammer, B.: «Burkitt’ s lymphoma protruding through the anus: report o í an unusual case». Dis Colon Recturn., 1988; 31:629-31.
6. IOACHIM, HL.; ANTONESCU, C.; GlANCOTTI, F.; Dorsett, B., W einstein, M A.: «EBV-associated anorectal lym phom as in pa- tients with acquired immune deficiency syndrom e». Am. J. Surg. Pathol., 1997; 21:997-1.006.
7. Blanc, S.; Bertrand, Y.; Lorthois- Ninou, S.; Carlioz, R; Dijoud, F., Pra-CROS, JE: «Rectal localization oí’ Burkitt’s lym ph om a». A rch. Pediatr., 2002 ; 9:1.056-8.
8. Otieno, M I ; Remick, SC., W halen, C.: «A dult B urkitt’ s lym phom a in patients with and without hum an im m unodefi- ciency virus infection in Kenya». hit. J. Cáncer, 2 0 0 1 ;9 2 :6 8 7 -9 1 .
9. DlEBOLD, J.; RAPHAEL, M .; PREVOT, S., A.UDOUIN, J.: «Lymphomas associated with H IV in fection». C án cer Surv., 1997; 30: 263-93.
10. SPINA, M .; TtRELLI, U., ZAGONEL, Y., et al.: «B urkitt’ s lym phom a in adults with and without human im m unodeficiency virus in fection : a single-institution clinicopat- h ologic study o í 75 patients». Cáncer, 1998; 82:766-74.
11. STRAUS, DJ.: «Treatm ent o í B u rk itt ’ s lymphoma in H lVpositive patients». Bio- tned Pharm acother, 1996; 50:447-50.
12. ABOULAFIA, D.: «Epidem iology and pat- hogenesis o í AID S-related lym phom as». O ncology, 1998; 12:1.068-81.
13. Lucas, SB.; Diomande, M., Hounnou, A., et al.: «H IV associated lymphoma in A frica: an autopsy study in Cote d ’ Ivoire». Int. J. Cáncer, 1994; 59:20-4.
14. A mbinder, R E : «Epstein-Barr virus associa ted ly m ph oproliferation s in the AID S setting». Eur. J. Cáncer, 2001; 37: 1209-16.
15. Chan, JK .; Tsang, W Y.; Ng, CS.; W ong, CS., Lo, ES.: «A study o f the association o f E pstein -B arr virus with B u rk itt ’ s lym phom a occurring in a Chinese popu-
lation». H istopa th ology , 1995; 26:239- 45.
16. SMITH, D L., Cataldo, PA.: «P erianal lymphoma in a heterosexual and nonim- m unocom prom ised patient: report o f a case and review o f the literature». Dis Colon Recturn, 1999; 42:952-4.
17. Lee, MIL; Waxman, M., Gillooley, JE: «P rim a ry m alignant lym phom a o f the anoreetnm in hom osexual m en». Dis. C olon Recturn, 1986; 29:413-6.
18. Gisselbrecht, C.; Oksenhendler, E., Tirelli, U., et al.: «H um an im m unodefic ien cy v irus-related lym phom a treatm ent with intensive com bin ation ehe- m otherapy. French- Italian C ooperati- ve G rou p ». Am . J. M ed ., 1993; 95:188- 96.
19. Jones, SE.; Grozea, PN., Metz, EN., et al.: «Superiority o f adriam ycin-contai- ning com bination chem otherapy in the treatment o f diffuse lym phom a: a Southwest O ncology G roup study». Cáncer, 1979; 43:417-25.
20. E v e n s , AM ., G o rd o n , LL: «Burkitt’ s and Burkitt-like lymphoma». Curr. Treal. Op- tions O ncol., 2002; 3:291-305.
21. C o l e b u n d e r s , R .; D o h m e n , S.; V a n de VELDE, A . ; PELGROM, J ., H e RMANS, R : «B u rk itt ’ s lym phom a shortly after an acule H IV infection , treated with highly active retroviral treatment». A cta Clin. Belg., 2001; 56:321-2.
22. HOCQUELOUX, L .; AGBALIKA, F.; OKSEN- hendler, E., Molina, JM.: «Loug-term remission o f an AIDS-related prim ary ef- fusion lymphoma with antiviral therapy». AIDS 2001; 15:280-2.
23. Jones, JL.; Hanson, D L.; Dworkin, MS.; Ward, JW., Jaffe, HW.: «E ffect o f anti- retroviral therapy on recent trends in se- lected cáncers among H lV -infected per- sons. Adult/ Adolescent Spectrum o f H IV Disease P ro ject G rou p». J. Acquir. Im - m une D efic. Synclr., 1999; 21:11-7.
24. Magrati-i, IT.; Lwanga; S., Carswell, W., et al.: «Surgical reduction in management o f abdom inal B urkitt’ s L ym phom a». BMJ, 1974; 2:308-12.





























