Embed Size (px)
Citation preview

HIV Drug Resistance in 2018
“How Can We Deal With It?”
Ghassan Wali, MDHead, Infectious Diseases section
HIV physicianKing Faisal specialist and research center, Jeddah

Objectives:
Review the prevalence of transmitted drug resistance locallyand internationally.
Go over the most important mutations and their clinicalimplications
Identify key points of managing antiretroviral drugs therapyin HIV patients who are treatment-experienced.
Apply evidence from recent clinical trials to managingpatients who are failing second and third line therapy.

Patient HAge 41
HIV Status Positive; 2 days ago
CD4 420
HIV RNA 100K per ml
eGFR 110
Co-infection HBsAg: positive
comorbidities hypertension
Metabolism hyperlipidemia
medications Amlor, lipitor
HIV genotype test pending
Patient is referred
from infertility
clinic

• What is your decision today at the clinic:
• 1- uphold ARV until genotype testing is back
• 2- start him on atazanavir/r plus TAF/FTC
• 3- Start him on Darunavir/r plus TAF/FTC
• 4- start him on raltegravir plus TAF/FTC
• 5- start him on dolutegravir plus TAF/FTC
• 6- I have a different answer

Recommendations for HIV resistance testing

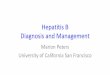
Prevalence of Drug Resistance Mutations in Treatment-Naive Patients, 2000-2013
Baseline plasma samples from 4 phase III trials (GS 903, 934, 104, 111)◦ 1617 samples analyzed for
integrase mutations◦ 2531 analyzed for protease or
RT mutations
Substantial in prevalence of NNRTI resistance, modest in PI resistance
Stable prevalence of NRTI resistance (mostly TAMs)◦ M184V/I 0.2%; K65R 0.2%
▪Little evidence of transmitted INSTI resistance over period◦ Mostly T97A polymorphism
Margot NA, et al. CROI 2014. Abstract 578.
2000 (GS-903)
2003 (GS-934)
2013 (GS-104/GS-111)
0Pts
With M
uta
tion
s a
t B
L (
%)
2
NNRTI
10
4
6
8
NRTI PI INSTI
0.5 1.0
0
4.2
8.7
3.22.6 2.6
1.2
2.4
2.9
1.4

Prevalence of Transmitted MDR HIV in the US: Selected Studies
Transmission of HIV resistant to a single class of ARV more common than HIV resistant to multiple classes[1,3]
◦ 13.6%, 2.1%, and 0.5% of transmitted HIV resistant to 1, 2, and 3 ARV classes, respectively[3]
1. Baxter JD, et al. HIV Med. 2015;16:77-87. 2. INSIGHT START Study Group.
N Engl J Med. 2015;373:795-807. 3. Kim D, et al. CROI 2013. Abstract 149.
Prevalence of Transmitted Drug-
Resistant HIV
(2009-2013), %[1-3]
Overall
▪ NRTI
▪ NNRTI
▪ PI
12.6-16.2
3.7-6.7
8.1-8.4
2.0-4.5

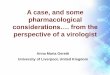
Decrease in Prevalence of MDR HIV in the US in Recent Era of HIV Treatment
• Assessment of phenotypic drug resistance patterns in US samples submitted to Monogram Biosciences for HIV resistance testing from 2003-2012 (N = 62,397)
Paquet AC, et al. Antivir Ther. 2014;19:435-441.
60
0
10
20
30
40
50
2-Class Resistance
PI and NRTIPI and NNRTINRTI and NNRTI
0
10
20
30
40
50
603-Class Resistance
1-Class Resistance
0
10
20
30
40
50
60
Resis
tant S
am
ple
s (
%)
PINRTINNRTI


Causes of Treatment Failure
DHHS Guidelines.
Poor adherence
Insufficient drug level
Viral replication in the presence of drug
Resistant virus
Social/personal issuesRegimen issues
Toxicities
Suboptimal potency
Wrong dose
Host genetics
Poor absorption
Rapid clearance
Poor activation
Drug interactions
Virologic failure
Transmitted or Acquired

• In case you need to start the patient on ARV before genotype test is readily available, use a PI-based ( boosted-darunavir) or high genetic barrier INSTI ( dolutegravir)
DHHS Guidelines.


• What is your decision today at the clinic:
• 1- uphold ARV until genotype testing is back
• 2- start him on atazanavir/r plus TAF/FTC
• 3- Start him on Darunavir/r plus TAF/FTC
• 4- start him on raltegravir plus TAF/FTC
• 5- start him on dolutegravir plus TAF/FTC
• 6- start him on dolutegravir plus darunavir/cobi

DHHS: Recommendations for Resistance Testing
• Results used to inform design of new ART regimens for pts experiencing VF
DHHS Guidelines.
Question Recommendation
Who should receive
resistance testing?
▪ Pts with VF and HIV-1 RNA levels > 1000 copies/mL
▪ May be considered for pts with 500-1000 copies/mL
When should testing be
conducted?
▪ While on failing ART regimen or < 4 wks from treatment end
▪ May still be considered after 4 wks
What types of testing
should be conducted?
▪ First-/second-line failure: genotypic testing
▪ Suspected MDR: genotypic plus phenotypic testing
▪ When considering CCR5 antagonist: tropism assay
▪ If prior failure on INSTI-containing regimen, test for INSTI
resistance
Other considerations ▪ Prior treatment history should be obtained

M184V
M = Methionine
184 = the codon #
V = Valine
A mutation at codon #184 in
the gene Reverse Transcriptase
codes for a Valine residue
where normally a Methionine
residue is found.


M184V
• Emerging first in a non suppressive regimen that contain 3TC or FTC.
• Give rise to resistance to 3TC,FTC but :
• No clinical implications.
• They should be still used for partial viral suppression and to decrease replication.
• Increased affinity to AZT, D4T & TNF.


K65R & L74V
• With initial use of TNF, ABC, DDI.
• TNF : K65R
• DDI : L74V
• ABC : L74V > K65R
• K65 reduces viral replication (VR) by 30 folds.
• It also causes hyper-susceptibility to AZT.

NNRTI Mutatations
• K103N is most common one, followed by C181Y
• Remember: they lead to cross resistance to all NNRTIs.


Patient R48 year old with diagnosed 5 years ago.
Started on AZT, 3TC and efaverenz 2 years ago.
Noncompliant, lost to follow up.
VL:200,000 c/ml CD4: 125 cells/mm3
Genotype:
NRTI
M184V, K219R
NNRTI
K103N, V108I
PI
None

DHHS: Management of First-line Failure
DHHS Guidelines.
*If RAL or EVG resistance detected, DTG + boosted PI can be used if DTG susceptible.
Failing Regimen (+ NRTIs)
▪ Boosted PI: Enforce adherenceModify for convenience or toxicity
▪ NNRTI: Boosted PI + NRTIsBoosted PI + INSTI
▪ INSTI: Boosted PI + NRTIsBoosted PI + active INSTI*

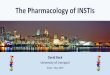
EARNEST: Second-line LPV/RTV ± RAL or 2-3 NRTIs in PI-Naive Pts
• Randomized, open-label, multicenter phase III trial in sub-Saharan Africa
LPV/RTV + RAL
(n = 433)
LPV/RTV + 2-3 NRTIs*
(n = 426)
HIV-infected pts
> 12 yrs of age
with confirmed VF on
NNRTI + 2 NRTIs
and no prior PIs
(N = 1277)
Wk 96
LPV/RTV 400/100 mg and RAL 400 mg dosed
BID.
*New or recycled NRTIs chosen WITHOUT
genotype by clinician.
Wk 12
LPV/RTV Monotherapy
(n = 418)
LPV/RTV + RAL
(n = 418)
Paton NI, et al. N Engl J Med. 2014;371:234-247.
Stratified by study
center, CD4+ cell
count (< 200 vs ≥
200 cells/mm3)

EARNEST: Boosted PI + RAL Comparable to Boosted PI + NRTIs
• SECOND-LINE[3] and ACTG 5273[4,5] showed similar results
LPV/RTV + RAL
(n = 433)
LPV/RTV + 2/3
NRTIs
(n = 426)
LPV/RTV
monotherapy
(n = 418)
10
0
8
0
6
0
4
02
0
0
Pts
(%)
HIV-1 RNA < 50
copies/mL,
Wk 96[1]
7473
44
P < .001
HIV-1 RNA < 400
copies/mL Through
Wk 144[2]
LPV/RTV + NRTI(Number of Active
NRTIs)
Pts
(%
)
88
0 LPV/RTV
+ RAL
7781
85
61
1 2-3
LPV/RTV

Virologic failuere with first line regimen
-DTG plus two NRTIs (at least one of which is active) can be
an option after failure of a first-line, NNRTI-based therapy (
based on DAWWNNG trial) (AI).
-Bictegravir (BIC) may have activity that is similar to that of
DTG; however, there are currently no data to support its use.
Adapted from DHHS Guidelines, October 25, 2018

PI Resistance
• PIs have high genetic barrier that is why Detectable virus in the face of boosted PI is rarely due to mutations. It is rather due to non-compliance . options:
• stress on adherence and repeat VL in 4 weeks.
• Switch to another PI.
• Switch to another class



The Role of Maraviroc
Highly effective in experienced pat. With R5 virus ( motivate trial).
Requires screening with tropism assay,
50% of experienced pat. Not candidates for MVC due to D/M or X4 virus.
D/M or X4 virus can be missed if present at less than 10%
Not approved as first line in naïve patients.

Raltegravir Resistance
• From BENCHMARK 1 & 2
• Partial analysis from 41 raltegravir failure: 32 with integrase changes, 9 with no consistent changes from baseline.
• N155H and Q148K/R/H are the recognized pathways.
• Unfortunately, they carry cross resistance to other elvitigravir.

Dolutegravir

Current Status of INSTI Resistance in the US
Transmitted INSTI resistance remains rare and rates of on-treatment INSTI resistance continue to be low[1-3]
1. Hernandez AL, et al. CROI 2017. Abstract 478. 2. Davy T, et al. CROI 2017. Abstract 483.
3. Koullias Y, et al. CROI 2017. Abstract 493.
Study Key Findings
CDC National HIV
Surveillance
System[1]
▪ Prevalence of INSTI resistance for HIV
diagnoses through 2014:
65/14,468 (0.4%)
▪ Pre-ART prevalence of INSTI resistance (ie,
transmitted): 2/4631 (0.04%)
UNC CFAR HIV
Clinical Cohort[2]
▪ 2015 INSTI resistance prevalence in 685 pts
who began ART in 2007 or later: 1%
Modeling study[3]
▪ Assuming 0.1% rate of transmitted INSTI
resistance and $250 cost per test: pre-ART
INSTI resistance testing correlated with worse
outcomes, higher costs vs no test

DHHS: Management of ART Failure Second-line ARV Failure
Goal: fully suppressive ARV regimen If susceptible to boosted PI, regimen
can be similar to those for first-line failure
If not susceptible to boosted PI, new regimen should have a minimum of 2 (preferably 3) fully active drugs if possible◦ Susceptibility to drug predicted from
pt treatment history, prior and current resistance and tropism testing, MoA of novel drug class
Not recommended to add single agent to failing regimen due to risk of developing resistance to entire regimen
DHHS Guidelines.
Boosted PI + NRTIs
Boosted PI + active
INSTI
2 and preferably
3 fully active
drugs
Yes No
PI
Susceptible

DHHS: Treatment of Pts With MDR HIV for Whom Optimal Virologic Suppression Is Not
Possible
Goals: minimize toxicity, preserve immunologic function,delay clinical progression, minimize further resistance
◦ Reduction of HIV-1 RNA > 0.5 log10 copies/mL correlated withclinical benefit
◦ If resistant, rarely a reason to continue NNRTIs, ENF, EVG, or RAL:no evidence of clinical benefit; may promote further resistance,limit future treatment options
DHHS Guidelines.

Emerging Investigational Agents for Pts With MDR HIV
1. Lalezari JP, et al. Lancet HIV. 2015;2:e427-437. 2. Granados-Reyes ER, et al. HIV
Glasgow 2016. Abstract O335A. 3. ClinicalTrials.gov. NCT02362503. 4. Lewis S, et al. CROI
2017. Abstract 449LB.
5. Lin H-H, et al. CROI 2017. Abstract 438. 6. Lalezari J, et al. CROI 2017. Abstract 437.
Investigational
AgentPhase MoA
Fostemsavir[1-3] III
Prodrug; when metabolized
binds gp120 to prevent CD4+
cell attachment, entry
Ibalizumab[4,5] IIIHumanized anti-CD4 receptor
mAb
PRO 140[6] IIb/III Humanized anti-CCR5 mAb

TMB-301: Ibalizumab in Pretreated Pts Infected With Multidrug-
Resistant HIV• Ibalizumab: humanized mAb to CD4 receptor that blocks HIV entry into
CD4+ T-cells
– FDA breakthrough and orphan drug designations
• Single-arm, open-label phase III trial
– Primary endpoint: ≥ 0.5 log10 HIV-1 RNA decrease at Day 14
Lewis S, et al. CROI 2017. Abstract 449LB.
Pts with HIV-1 RNA
> 1000 copies/mL;
on ART ≥ 6 mos, on
stable ART ≥ 8 wks;
resistant to
≥ 1 ARV from 3
classes, sensitive to ≥
1 ARV for OBR
(N = 40)
Wk 25
Ibalizumab
2000 mg IV Day 7
(loading dose)
Continue Failing ART
Days 0-14
Ibalizumab
800 mg IV Day 21, Q2W
(maintenance dose)
Switch to OBR
Day 14
Primary Endpoint:
Day 14Control Period:
Day 0-7

TMB-301: Efficacy
Lewis S, et al. CROI 2017. Abstract 449LB.
Virologic Outcome
Ibalizum
ab +
OBR
Day 14
≥ 0.5 log10 HIV-1 RNA decrease,
%
83*
≥ 1.0 log10 HIV-1 RNA decrease,
%
60
Mean HIV-1 RNA decrease, log10 1.1
Wk 24
≥ 1.0 log10 HIV-1 RNA decrease,
%
55
≥ 2.0 log10 HIV-1 RNA decrease,
%
48
HIV-1 RNA < 50 copies/mL, % 43
HIV-1 RNA < 200 copies/mL, % 50
Mean HIV-1 RNA decrease from
BL, log10
1.6
*Primary endpoint; P < .0001 vs 3% at end of control period.
Outcome,
cells/mm3
Baseline CD4+ Cell
Count (cells/mm3)
< 50
(n =
17)
50-200
(n =
10)
> 200
(n =
13)
Mean baseline
CD4+ cell
count
12 109 363
Mean increase
in CD4+ cell
count at Wk 24
▪ Missing
equals failure
analysis
9 75 78
▪ Per protocol
analysis15† 75 81‡
†n = 7. ‡n = 10.

Take-Home Points
Primary resistance continue to occur, do GT test before HAART
For pts with virologic failure and potential MDR HIV, genotypic andphenotypic resistance testing results and treatment history shouldinform the construction of new ART regimens
For pts with confirmed MDR, the goal of a new regimen is aminimum of 2 (preferably 3) active drugs if possible
◦ For pts with resistance to currently available agents, refer to aspecialized center for expanded access program
◦ Investigational agents with novel MoAs may provide options forpts with MDR HIV Fostemsavir (gp120 binder; prevents CD4+ cellattachment), ibalizumab (anti-CD4 receptor mAb), PRO 140 (anti-CCR5mAb)

The Goal of Therapy
The goal of therapy is virologicsuppression to < 50 c/ml in allpatients.
DHHS & IAS- USA Guidelines